
Abstract
Flexible ureterolithotripsy is a frequent urological procedure, usually used to remove stones from the kidney and upper ureter. Reusable uretero-scopes were the standard tool for that procedure, but recent concerns related to sterility and maintenance and repair costs created the opportunity to develop new technologies. In 2016, the first single-use digital flexible ureteroscope was introduced. Since then, other single-use ureteroscopes were developed, and studies compared them with the reusable ureteroscopes with conflicting results. The purpose of this study is to describe the literature that compares the performance of single-use and reusable flexible ureteroscopes in retrograde intrarenal surgery for urinary stones. A Systematic Review was performed in October 2022 in accordance with the Cochrane Handbook and the Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA). A search in MEDLINE, EMBASE, Web of Science, Google Scholar and LILACS retrieved 10,039 articles. After screening, 12 articles were selected for the Meta-Analysis. No differences were found in stone-free rate (OR 1.31, CI 95% [0.88, 1.97]), operative time (MD 0.12, CI 95% [−5.52, 5.76]), incidence of post-operative fever (OR 0.64, CI 95% [0.22, 1.89]), or incidence of post-operative urinary tract infection (OR 0.63 CI 95% [0.30, 1.32]). No differences were observed in the studied variables. Hence, the device choice should rely on the availability, cost analysis and surgeons’ preference.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
History
Urolithiasis incidence has been increasing worldwide [1]. Flexible ureteroscopy (fURS) is the main surgical treatment for calculi with less than 2 cm [2]. It presents higher stone-free rates(SFR), from 80 to 90% [3] than extracorporeal shock wave lithotripsy (ESWL) and per-cutaneous nephrolithotomy (PCNL) for calculi between 1 and 2 cm [4].
As with many great discoveries, the first ureteroscopy was performed by accident: in 1912, during a pediatric procedure for correction of congenital posterior urethral valves,
Hugh Hampton Young inadvertently passed a rigid pediatric cystoscope into the patient’s dilated ureter [5].
During a long time, the potential for ureteroscopy remained largely unrealized, until 1964, when Victor Marshall used the first fiber optic ureteroscope in humans to visualize a ureteral stone. This first, 9F, fURS was not capable of being directed and did not have a working channel, thus permitting only the most primitive diagnostic maneuvers [6].
In the next two decades, three major design changes were implemented. The addition of a working channel allowed irrigant and endoscopic accessories to be passed directly through the endoscope. Active tip deflection allowed the endoscope to be directed or steered to areas of interest. Finally, altering the stiffness of the endoscope shaft which increased its deflection capability and provided access to difficult regions as the lower renal pole. With those improvements, in 1986, Bagley et al [7] used an ureteroscope to perform the first fURS for the treatment of stone disease.
Since that time, two major advances happened: the use of digital technology to generate image and the use of single-use fURS. Lithovue TM , released in October 2015 in Europe, was the first fURS that combined these features [8]. And nowadays, despite being mainly used for kidney stone removal, fURS is also used for cancer treatment and upper urinary tract diagnosis.
Vision technology
The new digital fURS offer a better image quality than fiberoptic ones (which present image distortions as the Moiré pattern) [9]. Studies argue that poor visibility leads to impaired diagnosis and poorer outcomes [10], and one study [11] comparing digital and fiberoptic reusable fURS (rfURS) have shown a 9 min shorter fragmentation time with digital rfURS.
All the single-use fURS (sufURS) are digital, but some of the rfURS are fiberoptic and others are digital.
Reusable vs single-use
The rfURS have issues related to the high cost of purchase and maintenance (related to sterilization and repair), infection risk[12, 13] injury risk [13] and a higher carbon footprint [14]. Therefore, sufURS was developed to address those problems.
As sufURS are less expensive and have no need for sterilization or repair, cost comparisons demonstrate high initial investment and lower cost per procedure for rfURS and low initial investment and higher cost per procedure for suFURS. The exact cutoff depends on local reprocessing infrastructure and acquisition cost, but sufURS seems to be more cost effective for the majority (non-high volume) of stone centers [15].
It was observed that damage to rfURS that requires repair happens after 10 to 27 uses [16, 17] and once repaired a rfURS is more likely to be damaged again [16]. The rfURS also gradually loses its image quality and effectiveness [18].
The durability of rfURS is affected by stone location (usually low pole stones [19] and size, duration of use, use of other devices, surgeon’s experience and sterilization methods [20] (sterilizations seem to be the main cause of damage [21]). Considering those factors, a suggested strategy is to apply a hybrid method and use sufURS for procedures with a high risk of damage (as lower pole stones and for trainees) and rfURS for low-risk procedures [22], [23]. Reusable ureteroscopes have fine mechanics, thin working channels for laser fibers or baskets and are a challenge for sterilization [24]. Studies have observed 100% of protein contamination in rfURS, and various outbreaks of infection were reported related to contaminated ureteroscopes [13]. A sufURS can automatically eliminate the possibility of cross-contamination by bypassing the reprocessing and sterility steps.
Objective
As seen before sufURS seems to provide many benefits over rfURS, however, most of those studies are in vitro and studies in vivo present conflicting results. The purpose of this study is to perform a systematic review and meta-analysis comparing clinical outcomes of sufURS and rfURS in retrograde intrarenal surgery for nephrolithiasis.
Methods
In October 2022, our team performed a systematic review comparing single-use vs reusable ureteroscopy for nephrolithiasis, in accordance with the Cochrane Handbook and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Our review was registered at PROSPERO (CRD42022367287).
We considered inclusion studies with patients who underwent retrograde intrarenal surgery with flexible ureteroscopy (single-use ureteroscopes compared to reusable ureteroscopes) to treat urinary stones.
Our primary outcome is stone free rate. The secondary outcomes were operative time, postoperative fever and incidence of UTI.
We searched for all articles in MEDLINE, Embase, Google Scholar and LILACS. Selection of studies
For this review, two review authors (JA and MB) independently selected the trials to be included in accordance with the aforementioned criteria. We excluded trials from the review if they made comparisons other than specified above.
Studies were also excluded from if they met the following exclusion criteria: (I) the study examined previously published reviews; and/or (II) the study undertook a meta-analysis. Letters, comments, and conference abstracts were also excluded from the meta-analysis
Studies from non-English language journals were translated if necessary. If a trial was published more than once, we only included the most complete and up-to-date data.
Data extraction and management
For this review, two review authors (JA and MB) independently extracted the data, resolving any disagreements by recourse to a third party (CC). We used a data extraction form designed and piloted by the review authors. The data collected was either dichotomous or continuous. If studies had multiple publications, we included only the main trial report.
Assessment of risk of bias in included studies
We assessed the included trials for risk of bias, using the Cochrane Rob 2 tool. We evaluated the following seven domains for possible bias. We judged the different types of bias using the criteria from the Cochrane handbook. Two review authors checked these domains of bias independently and rated them as being at high, low, or unclear risk of bias. The assessments were compared, and any disagreements were resolved by consensus or by discussion with a third review author (CC).
Measures of treatment effect
Where dichotomous data measures were used, we have expressed the results in the reusable and disposable groups of each trial as odds ratios (ORs) with 95% confidence intervals (CIs). Where continuous data measures were used, we have expressed the results in the reusable and disposable groups of each trial as a mean difference with 95% confidence intervals (CIs).
Dealing with missing data
If data were missing from the included studies, we imputed individual values for the primary and secondary outcomes in accordance with the Cochrane Handbook.
Data synthesis
We used a random-effect model to combine data from primary studies. We conducted statistical analysis with Review Manager 5™ (Review Manager ™, version 5.4.3 2020, Cochrane), in accordance with the guidelines for statistical analysis developed by Cochrane, comparing disposable to reusable ureteroscopes for nephrolithiasis
Results
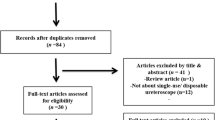
Our research retrieved 10039 studies from which 12 [15, 26,27,28] were included in the review as described in the PRISMA workflow (Table 1).
Our study included 5 types of single-use flexible ureteroscopes: LithoVue TM (Boston Scientific, Marlborough USA), Wiscope TM (OTU Medical Inc., Union City, US), PU3022 TM (Zhuhai Pusen Medical Technology Company Limited, China), US31B-12 TM (Innovex Anqing Medical Instrument CO. LTD, Shangai, China), Zebrascope TM (Happiness Workshop, Beijing, China) and 8 types of reusable ureteroscopes URF-V TM, URF-V2 TM, URF-P6 TM, URF-P7 TM (Olympus, Tokyo, Japan), Flex-X2 TM, Flex-XC TM, Flex- X2S TM (Karl Storz SE & Co. KG, Tuttligen, Germany), Cobra TM (Richard Wolf, Knit- tlingen, Germany) as described in Table 2.
While all the single-use ureteroscopes are digital, some of the reusable ureteroscopes are digital and others use optic fiber to generate the image (Table 3).
Five studies compared the stone-free rate. In this analysis, we only included articles that defined stone-free rate (SFR) as the absence of stones greater than 1 to 4 mm depending on the study. Evaluation of residual stones was done with a CT scan or X-ray a month after the procedure. As we see in Fig. 1, no significant difference was found when comparing the ureteroscopes (OR 1.31 CI 95% [0.88, 1.97]).

Stone free rate plot
Twelve articles display information comparing the operative time between the two types of devices. As we see in Fig. 2, no significant difference was found when comparing the ureteroscopes (MD 0.12, CI 95% [−5.52, 5.76]).

Operative time plot
Regarding infectious complications, we compared both the incidence of postoperative fever (6 studies resulted in OR 0.64, CI 95% [0.22, 1.89], Fig. 3) and postoperative urinary tract infection(UTI), (6 studies resulted in OR 0.63 CI 95% [0.30, 1.32] Fig. 4) and no significant differences were observed.

Postoperative fever

Postoperative UTI
Our risk of bias analysis showed that only 3 articles have a low risk of bias. The areas with higher bias are the randomization process as most of the studies are non-randomized retrospective trials and it is important to consider that it is impossible to blind the surgeon about the equipment that he is using. (Fig. 5)

Risk of bias
Discussion
As exposed before, single-use ureteroscopes have many benefits: no need for sterilization, no maintenance costs, better image quality, and lower weight [16]. Previous studies assessed whether those improvements affect surgical outcomes with conflicting results.
All the studies presented the same demographics and preoperative characteristics. In two studies [28, 29] authors were able to make the baseline of the two groups equivalent by doing a propensity-score matching analysis. In the first study, the single-use group initially presented greater stone diameter and stone volume. In the second study, the single-use group had a significantly higher stone burden and lower mean age.
Stone free rate
Regarding SFR, we included only outcomes measured with a CT scan done after surgery. Some studies [15, 26, 30] measured SFR intraoperatively using surgeon’s endoscopic and fluoroscopic views. As the error of this method to evaluate SFR is unavoidable those studies were excluded during the assessment of SFR.
Studies that did not specify how the SFR was measured and were also excluded from our analysis.
Operative time
The theoretical discussion on whether single-use ureteroscopes increase or decrease operative time has good arguments on both sides. On one hand, the advances of the new technology could allow faster surgeries. On the other, single-use ureteroscopes freed surgeons from anxieties about breaking the scope. This could allow the surgeon to perform more meticulous and longer operations [4, 31].
Empirically, most of the studies agree that there is no significant difference in operative time. However, two authors [26, 32] observed shorter operative time with single use uretero- scopes while two authors [33, 34] observed the opposite.
Mourmouris et al. [26] used differences are different proportions of the size of laser fiber between the groups (270 µm and 365 µm). Usawachintachit et al. [32] had high levels of bias, probably due to the originality of his work, being one of the first comparisons of single-use vs reusable fURS.
Kam et al. [34] observed that rfURS outperformed sufURS in visibility and maneuverability.
However, because of missing standard deviation information we imputed standard deviation values according to Cochrane Handbook. In the study itself, the statistical comparison used three groups (2 single-use and one reusable) and no differences were observed. To fit the purpose of our study we combined the first two groups and as we see, the difference in operative time has become statistically significant.
Salman et al. [33] analyzed exclusively patients with lower pole stones and it was a surprise to see shorter operative time with reusable ureteroscopes. A factor to bear in mind is that the not observed differences in stone density could impact those results.
Infections
As described before, the infectious complications analysis was done assessing two outcomes: fever and UTI. Considering biological plausibility, we expected that single-use ureteroscopes would have lower infection rates, but overall that was not observed. We believe that the routine use of preoperative antibiotics, done in all the studies, may play an important role in that.
The only study that observed higher infection rates (both fever and UTI) in the reusable group was Bozzini et al [35]. It also presented higher levels of positive blood culture (0 vs 1 patient p < 0.05) and urosepsis (0 vs 1 patient p < 0.05). It is important to consider that there was no difference in the operative time, neither in demographic characteristics between the groups and that the incidence of fever in this study was higher than in others.
Limitations
Overall, the included studies had non-low levels of bias due to randomization issues and the impossibility to blind the surgeon. It is also worth noting that we grouped different available options of ureteroscopes under the categories of single-use and reusable and due to scarce literature, we could not compare each model to each other.
Our analysis is also limited to ordinary patients and does not address special situations such as pregnant women, infants, and horseshoe kidney patients.
We did not consider the cost-effectiveness of each type of ureteroscope. This kind of analysis is a complex process that involves acquisition, repair, and reprocessing costs of fURS. In general, it is demonstrated lower investments and higher cost per procedure for sufURS and higher initial investments and lower cost per procedure for rfURS, resulting in a point of intersection where total investments for single-use instruments exceed the costs for reusable ureteroscopes.
Conclusion
We conclude that flexible ureteroscope choice between single-use and reusable for retrograde intrarenal surgery should be based on surgeon’s preference and local cost-effective analysis.
Data availability
Data can be available upon request to the corresponding author.
References
Sorokin I, Mamoulakis C, Miyazawa K et al (2017) Epidemiology of stone disease across the world. World J Urol 35(9):1301–1320
Assimos D (2016) Surgical management of stones: american urological association/endourological society guideline. PART I J Urol 196(4):1153–1160
Skolarikos A (2015) Outcomes of flexible ureterorenoscopy for solitary renal stones in the croes urs global study. J Urol 194(1):137–143
Bozzini G (2017) A prospective randomized comparison among SWL, PCNL and RIRS for lower calyceal stones less than 2 cm: a multicenter experience : a better understanding on the treatment options for lower pole stones. World J Urol 35:1967–1975
Fuchs GJ (2006) Milestones in endoscope design for minimally invasive urologic surgery: the sentinel role of a pioneer. Surg Endosc. https://doi.org/10.1007/s00464-006-0078-4
Marshall VF (1964) Fiber optics in urology. J Urol 91(1):64066–64073
Bagley DH, Rittenberg MH (1986) Percutaneous antegrade flexible ureteroscopy. Urology 27(4):331–334
Butticè S, Sener TE, Netsch C et al (2016) LithoVueTM: a new single-use digital flexible ureteroscope. Cent European J Urol 69(3):302–305
Lusch A (2013) In vitro and in vivo comparison of optics and performance of a distal sensor ureteroscope versus a standard fiberoptic ureteroscope. J Endourol 27(7):896–902
Monga M, Hendlin K, Skenazy J et al (2004) A novel dual-diameter ureteroscope working channel: impact on irrigant flow. Urol 64(5):892–894
Isaacson D (2017) Defining the costs of reusable flexible ureteroscope reprocessing using time-driven activity-based costing. J Endourol 31(10):1026–1031
Monga M (2006) Durability of flexible ureteroscopes: a randomized, prospective study. J Urol. https://doi.org/10.1016/S0022-5347(06)00575-1
Chang CL, Su LH, Lu CM et al (2013) Outbreak of ertapenem-resistant Enterobacter cloacae urinary tract infections due to a contaminated ureteroscope. J Hosp Infect 85(2):118–124
Davis NF, Mcgrath S, Quinlan M et al (2018) Carbon footprint in flexible ureteroscopy: a compar-ative study on the environmental impact of reusable and single-use ureteroscopes. J Endourol 32(3):214–217
Mager R, Kurosch M, Höfner T et al (2018) Clinical outcomes and costs of reusable and single-use flexible ureterorenoscopes: a prospective cohort study. Urolithiasis 46(6):587–593
Hennessey DB, Fojecki GL, Papa NP et al (2018) Single-use disposable digital flexible ureteroscopes: an ex vivo assessment and cost analysis. BJU Int 121:55–61
Legemate JD (2019) Durability of flexible ureteroscopes: a prospective evaluation of longevity, the factors that affect it, and damage mechanisms. Eur Urol Focus 5(6):1105–1111
Mrkobrada M (2015) CUA guidelines on antibiotic prophylaxis for urologic procedures. Can Urol Assoc J 9(1–2):13–22
Moore B, Proietti S, Giusti G et al (2019) Single-use ureteroscopes. Urol Clin North Am 46(2):165–174
Carey RI, Martin CJ, Knego JR (2014) Prospective evaluation of refurbished flexible ureteroscope durability seen in a large public tertiary care center with multiple surgeons. Urology 84(1):42–45
Abraham JBA (2007) Rapid communication: effects of Steris 1 sterilization and Cidex ortho-phthalaldehyde high-level disinfection on durability of new-generation flexible ureteroscopes. J Endourol 21(9):985–992
Martin CJ (2017) The economic implications of a reusable flexible digital ureteroscope: a cost-benefit analysis. J Urol 197(3):730–735
Taguchi K (2018) Micro-costing analysis demonstrates comparable costs for lithovue compared to reusable flexible fiberoptic ureteroscopes. J Endourol 32(4):267–273
Ofstead CL, Heymann OL, Quick MR et al (2017) The effectiveness of sterilization for flexible ureteroscopes: a real-world study. Am J Infect Control 45(8):888–895
Carey RI, Gomez CS, Maurici G et al (2006) Frequency of ureteroscope damage seen at a tertiary care center. J Urol. https://doi.org/10.1016/j.juro.2006.03.059
Wendt-Nordahl G, Mut T, Krombach P et al (2011) Do new generation flexible ureterorenoscopes offer a higher treatment success than their predecessors? Urol Res 39(3):185–188
Mourmouris P (2021) Comparison of a single-use, digital flexible ureteroscope with a reusable, fiberoptic ureteroscope for management of patients with urolithiasis. Arch Ital Urol Androl 93(3):326–329
José A, Salvadó JM et al (2019) Endoscopic treatment of lower pole stones: is a disposable ureteroscope preferable? results of a prospective case-control study. Cent Eur J Urol 72(3):280
Takazawa R (2022) development of microscopy apparatus switchable between fluorescence and ultralow-frequency raman modes. J Anal Methods Chem. https://doi.org/10.1155/2022/2694545
Huang F (2022) Reusable digital flexible ureteroscope to treat upper urinary calculi: a propensity-score matching analysis. Front Surg. https://doi.org/10.3389/fsurg.2021.778157
Baboudjian MBM (2021) Single use versus reusable flexible ureteroscopy for the treatment of urolithiasis: a comparative study of perioperative complications. Urology 1:66–69
Li Y (2021) Comparison of single-use and reusable flexible ureteroscope for renal stone management: a pooled analysis of 772 patients. Transl Androl Urol 10(1):483–493
Usawachintachit M (2017) A prospective case-control study comparing lithovue, a single-use, flexible dis- posable ureteroscope, with flexible reusable fiber-optic ureteroscopes. J Endourol 31(5):468–475
Salman MY, Bayar G, Dincer HR et al (2021) Comparison of reusable and single-use ureteroscopes for the treatment of medium-sized stones in the lower calyx: a prospective randomized study. Ann Clin Anal Med. https://doi.org/10.4328/ACAM.20446
Kam J (2019) Single use versus reusable digital flexible ureteroscopes: a prospective comparative study. Int J Urol 26(10):999–1005
Author information
Authors and Affiliations
Contributions
MB and JPO wrote the main manuscript text, MB JA and CC worked on data analysis, ELAA and LSM prepared figures and tables. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interests
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Belkovsky, M., Passerotti, C.C., Maia, R.S. et al. Comparing outcomes of single-use vs reusable ureteroscopes: a systematic review and meta analysis. Urolithiasis 52, 37 (2024). https://doi.org/10.1007/s00240-024-01537-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00240-024-01537-8