
Abstract
Background
Preoperative nutritional status is considered to affect the short-term and long-term outcomes of cancer patients. The clinical value of the controlling nutritional status (CONUT) score in elderly patients undergoing gastrectomy for gastric cancer remains unknown.
Methods
This study reviewed 211 elderly patients aged 75 years or over who underwent curative resection for gastric cancer from 2000 to 2015. Patients were grouped according to the preoperative CONUT score into those with normal nutrition (75 patients), light malnutrition (100 patients) and moderate or severe malnutrition (36 patients). The predictive value of the CONUT score for postoperative morbidity and survival was assessed.
Results
Impaired nutrition was associated with cardiovascular disease (P = 0.012) and chronic kidney disease (P = 0.014), and worsened malnutrition was linked to advanced age (P = 0.004), decreased body mass index (P = 0.008) and advanced disease stage (P = 0.01). Multivariate analysis showed the CONUT score as an independent predictor of procedure-unrelated infectious morbidity (odds ratio, 2.36; 95% confidence interval [CI], 0.99–5.40; P = 0.046). Patients with a higher CONUT score had significantly shorter overall survival in both stage I and stage II/III gastric cancer (P = 0.044 and P = 0.007, respectively) and reduced cancer-specific survival in stage II/III (P = 0.003) The CONUT score was a strong predictors of overall survival (hazard ratio [HR], 2.12; 95% CI, 1.18–3.69; P = 0.012) and cancer-specific survival (HR, 3.75; 95% CI, 1.30–10.43; P = 0.015) independent of disease stage.
Conclusions
The preoperative CONUT score is a simple and promising predictor of postoperative procedure-unrelated infectious morbidity and prognosis in elderly gastric cancer patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer is one of the leading causes of cancer deaths globally and is expected to continue to increase as populations in developed countries age [1]. The number of elderly patients with gastric cancer in Japan has risen every year since records on it have been kept [2]. Gastrectomy is the main treatment for gastric cancer, but it can significantly diminish patients’ quality of life. Postoperative morbidities also seriously impair health condition and lead to poor prognosis in the elderly [3, 4]. Elderly patients generally have poor health condition that adversely affects surgical outcomes and prolongs disability after surgery [5, 6]. However, physical status varies greatly among elderly individuals. Therefore, it is essential to identify a practical tool that can predict postoperative morbidity and survival, and guide the development of therapeutic strategies for elderly gastric cancer patients.
Nutritional status is thought to be associated with prognosis after oncologic surgery [7, 8]. Gastric cancer causes debilitating malnutrition due to decreased oral intake and blood loss from the primary tumor. Furthermore, the elderly tend to develop malnutrition as a result of decreases in both physical function and food intake [9]. The controlling nutritional status (CONUT) score was developed to screen for nutritional impairment simply and objectively [10]. The CONUT score is calculated from serum albumin level, total lymphocyte count and total cholesterol level in the peripheral blood. Though the CONUT score has been reported to be useful as a prognostic indicator in patients with heart and liver disease [11, 12], few reports have studied the clinical value of CONUT score in cancer patients [13,14,15,16,17]. The value of the CONUT score in gastric cancer patients remains unknown.
The aim of this study was to investigate the predictive value of the preoperative CONUT score for postoperative morbidity and survival in elderly patients with gastric cancer.
Materials and methods
Patients
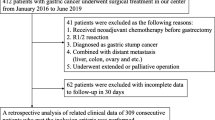
From January 2000 to December 2015, a total of 1149 patients underwent resection for gastric cancer at Kobe University Hospital. Of the 261 elderly patients defined as age 75 years or over, those who received preoperative chemotherapy or transfusion or had insufficient preoperative data or who were lost to follow-up were excluded. Two hundred and eleven patients who underwent curative resection were analyzed using clinicopathological and treatment data extracted from medical charts. Disease status was diagnosed according to the Japanese Classification of Gastric Carcinoma [18]. Surgical procedures were performed according to the Japanese Gastric Cancer Treatment Guideline [19]. Postoperative morbidities ≥ grade II on the Clavien–Dindo classification were defined as either infectious or noninfectious morbidities [20]. Infectious morbidities were divided into procedure-related and procedure-unrelated infectious morbidities. Procedure-related infectious morbidities included anastomotic leakage, pancreatic fistula, intra-abdominal abscess and wound infection. Procedure-unrelated infectious morbidities comprised organ infections such as pneumonia, enterocolitis, urinary tract infection, biliary tract infection and catheter-related infection. Noninfectious morbidities included anastomotic stricture, anastomotic hemorrhage, delayed gastric emptying, small bowel obstruction, arrhythmia, angina pectoris, venous thromboembolism and stroke. This study was approved by the Institutional Review Board of the Graduate School of Medicine, Kobe University. Written informed consent was received from all patients.
Preoperative nutritional assessment
The CONUT score is calculated as described in Table 1. Serum albumin level, total lymphocyte count and total cholesterol level in peripheral blood were each categorized into quartiles that were then assigned scores [10]. The total scores of three parameters represent four nutritional statuses: normal nutrition and light, moderate and severe malnutrition.
Statistical analysis
Statistical comparisons between groups were performed with the Mann–Whitney U test or Student’s t test for continuous variables and with the Chi-square test or Fisher’s exact test for categorical variables. Possible risk factors for postoperative morbidities were assessed using logistic regression analysis. Factors with a probability level ≤0.1 were adopted for subsequent multivariate analysis and were considered as independent risk factors at a probability level <0.05. The cumulative survival rate was calculated by the Kaplan–Meier method, and survival curves were compared using the log-rank test. A Cox proportional hazard regression model was constructed to identify independent prognostic factors. P values <0.05 were considered statistically significant. All statistical analyses were performed using JMP statistical software, version 11 (SAS institute Inc., Cary, NC, USA).
Results
Demographics and clinicopathologic characteristics
Based on their preoperative CONUT scores, there were 75 patients (36%) with normal nutrition, 100 (47%) with light malnutrition, 32 (15%) with moderate malnutrition and 4 (2%) with severe malnutrition. The patients were divided into three groups: normal nutrition, light malnutrition and moderate and severe malnutrition groups. A comparison of the clinicopathological characteristics of the three groups is summarized in Table 2. Cardiovascular disease (P = 0.012) and chronic kidney disease (P = 0.014) were more prevalent in the malnutrition groups than in the normal group. Compared with patients with normal nutrition and light malnutrition, those with moderate or severe malnutrition demonstrated significantly older age (P = 0.004), lower body mass index (P = 0.008) and advanced disease stage (P = 0.01).
Predictive value of the CONUT score for postoperative morbidity
Surgical procedures and outcomes are listed in Table 3. Open-approach surgery (P = 0.048) and intraoperative transfusion (P <0.001) were significantly more prevalent in moderate or severe malnutrition group, but there was no significant difference in the extent of gastrectomy or lymph node dissection, splenectomy or blood loss among the three groups. One patient with a high CONUT score died within 30 days of surgery. Postoperative morbidity developed in 83 patients (39%) after gastrectomy. Infectious morbidity developed in 61 patients (29%), and noninfectious morbidity occurred in 34 patients (16%). Patients with moderate or severe malnutrition experienced a higher tendency of any morbidity and infectious morbidity (P = 0.09 and P = 0.08, respectively) and suffered from procedure-unrelated infectious morbidity (P = 0.029) significantly more frequently. The incidence of postoperative pneumonia tended to increase with degree of impaired nutrition (P = 0.06).
The results of analysis for risk factors associated with procedure-unrelated infectious morbidities are shown in Table 4. Multivariate analysis showed that a high CONUT score was an independent risk factor for procedure-unrelated infectious morbidity (OR, 2.36; 95% CI, 0.99–5.40; P = 0.046).
Predictive value of the CONUT score for survival
Survival analysis after curative gastrectomy excluded one patient who died during hospitalization. The overall median follow-up period was 47 months (range 5–185 months). The survival curves stratified by preoperative nutritional status according to the CONUT score are demonstrated in Figs. 1 and 2. The overall survival (OS) in moderate or severe malnutrition group was significantly shorter than in normal nutrition and light malnutrition groups (P <0.001; Fig. 1a). In normal nutrition, light malnutrition and moderate and severe malnutrition groups, 5-year OS rates by disease status were as follows: stage I, 88, 76 and 51%; stage II/III, 64, 53 and 24%, respectively (Fig, 1b, c). A significant reduction in OS was also found for patients with moderate or severe malnutrition in both stage I and stage II/III groups (P = 0.044 and P = 0.007, respectively). The patients with moderate or severe malnutrition also significantly shortened cancer-specific survival (CSS) than those with normal nutrition and light malnutrition (P <0.001, Fig. 2a). CSS was significantly worse in patients with moderate or severe malnutrition than in those with normal nutrition and light malnutrition in stage II/III groups (5-year survival rates of 33% vs. 64% and 75%, P = 0.003; Fig, 2c), but not in stage I group (P = 0.56; Fig, 2b).

Kaplan–Meier overall survival curves of patients stratified according to CONUT score: a all stages; b stage I; c stage II/III

Kaplan–Meier cancer-specific curves of patients stratified according to CONUT score: a all stages; b stage I; c stage II/III
The results of the Cox regression hazard model for predictors of OS and CSS are shown in Tables 5 and 6. Multivariate analysis identified the CONUT score (hazard ratio [HR], 2.12; 95% CI, 1.18–3.69; P = 0.012) and procedure-unrelated infectious morbidities (HR, 2.53; 95% CI, 1.19–5.46; P = 0.016) as independent prognostic factors for OS as well as age (HR, 2.14; 95% CI, 1.31–3.45; P = 0.003), ASA score (HR, 1.90; 95% CI, 1.05–3.41; P = 0.035) and disease stage (HR, 2.27; 95% CI, 1.35–3.83; P = 0.002). High CONUT score (HR, 3.75; 95% CI, 1.30–10.43; P = 0.015), great age (HR, 3.46; 95% CI, 1.54–7.95; P = 0.003) and advanced disease stage (HR, 39.35; 95% CI, 7.32–73.3; P <0.001) were independently associated with worse CSS in multivariate analysis.
Discussion
Our results linked high CONUT scores in elderly patients undergoing curative resection for gastric cancer to a reduced OS, and a poor CSS in advanced stage. Moreover, a high CONUT score was an independent risk factor for procedure-unrelated infectious morbidities that worsened prognosis. These results imply that the preoperative CONUT score may be a potential prognostic predictor for elderly gastric cancer patients and aid in the clinical decision-making process.
The underlying mechanisms responsible for the adverse effect of preoperative malnutrition on survival after oncologic surgery have not yet been fully clarified. Possible explanations focus on physical status and oncological behavior, respectively. First, impaired nutrition status defined by CONUT score was associated with the prevalence of cardiovascular disease and chronic kidney disease, which both adversely affect survival. Second, malnutrition may increase postoperative morbidities due to impaired physical status, causing elderly patients to experience further physical decline, and may lead to cancer-unrelated deaths. Third, postoperative infectious morbidity has been reported to be associated with poor long-term survival [4, 21, 22]. Tumor progression is influenced not only by tumor behavior but also by host status such as nutrition, inflammation and immunity. Infectious morbidities may amplify systemic inflammatory responses and accelerate the suppression of tumor immunity, leading to tumor progression [23]. Malnutrition also facilitates prolongation of inflammation and immunological deterioration and may contribute to tumor recurrence especially for advanced stage [6, 24]. Considering these findings together, malnutrition may result in an unfavorable prognosis.
The CONUT score is computed from three peripheral blood parameters. The serum albumin level is considered to be a dependable indicator of nutrition condition and systematic inflammation [25]. Although serum albumin concentration is associated with prognosis in gastric cancer, the prognostic value of albumin is considered to be secondary to systemic inflammatory response [26]. The predictive value of albumin was of debatable even among physically impaired elderly without inflammation [27]. The total lymphocyte count is known to reflect the host’s immune responsiveness to a tumor [28]. The total cholesterol concentration has been reported to be associated with tumor progression and patient prognosis in various cancers [29, 30]. Low serum cholesterol level was correlated with worse survival possibly due to hypocholesterolemia resulting from depletion of cholesterol by tumor growth [31]. The CONUT score could therefore reflect not only nutritional status, but also systemic inflammation and an immune responsiveness, and may provide a more balanced assessment than other candidates such as prognostic nutritional index and the Glasgow prognostic score [13, 32].
The elderly population is a heterogeneous cohort with various physical statuses. Frailty represents a physical vulnerability of the elderly to surgical stressors and leads to increase adverse outcomes. The association between frailty and adverse surgical outcomes has been demonstrated in patients undergoing various type of surgery [33, 34]. Frailty assessment is essential for surgical risk assessment. Physical status is commonly assessed by chronological age and performance status (PS). However, chronological age does not necessarily reflect age-related physical changes in the elderly [35]. PS is a useful predictor of surgical outcomes, but can differ from one evaluator to the next. Elderly patients may be divided into three categories for cancer treatment. Some patients have sufficiently healthy status to enable them to receive the same treatment as nonelderly patients; some patients are vulnerable enough to indicate something less aggressive than standard treatment, and the remainders are too frail to be treated aggressively. Health status stratified according to the CONUT scoring system may conform to this category. A CONUT score of 0 or 1 represents healthy condition, a CONUT score of 3 or 4 represents some vulnerability and a CONUT score ≥5 represents frailty. Hence, the CONUT score may serve to identify those frail patients who require intensive perioperative care to gastric cancer surgery. For elderly patients with high CONUT score, we have to plan the therapeutic strategy not to worsen postoperative outcome with meticulous care. Limited lymph node dissection should be considered to be adopted to prevent procedure-unrelated infectious morbidity. Aggressive perioperative nutritional therapies such as preoperative immunomodulating nutrition need to be offered to reduce postoperative morbidity [36,37,38], and these nutritional supports should be collaborated closely with ERAS program [39, 40]. Moreover, prehabilitation consisting of preoperatively correcting the declined nutritional, physical and neurophysiological function of patients may contribute to improved postoperative outcome [41, 42].
This study has several potential limitations because of its retrospective nature and enrollment of a limited number of patients at a single institution. The median follow-up period of only 47 months may be too short to form valid conclusions about long-term survival. Prospective studies of perioperative nutritional support based on the preoperative CONUT score are therefore required to better clarify the clinical value of the CONUT score in gastric cancer.
In conclusion, our results implied that the CONUT score was associated with prognosis after curative gastrectomy in elderly gastric cancer patients. Assessment of preoperative nutrition status according to the CONUT score may be of benefit in developing effective therapeutic strategies for gastric cancer.
References
Cutsem EV, Sagaert X, Topal B et al (2016) Gastric cancer. Lancet 388:2654–2664
Cancer Information Survice CANCER STATISTICS in JAPAN http://ganjoho.jp/en/professional/statistics/brochure/index.html
Takeuchi D, Koide N, Suzuki A et al (2015) Postoperative complications in elderly patients with gastric cancer. J Surg Res 198:317–326
Suzuki S, Kanaji S, Matsuda Y et al (2017) Long-term impact of postoperative pneumonia after curative gastrectomy for elderly gastric cancer patients. Ann Gatroenterol Surg 2:72–78
Damhuis RA, Tilanus HW (1995) The influence of age on resection rates and postoperative mortality in 2773 patients with gastric cancer. Eur J Cancer 31A:928–931
Kitamura K, Sugimachi K, Saku M (1999) Evaluation of surgical treatment for patients with gastric cancer who are over 80 years of age. Hepatogastroenterology 46:2074–2080
Kanda M, Mizuno A, Tanaka C et al (2016) Nutritional predictors for postoperative short-term and long-term outcomes of patients with gastric cancer. Medicine 95:e3781
Song GM, Tian X, Liang H et al (2015) Role of enteral immunonutrition in patients undergoing surgery for gastric cancer. Medicine 94:e1311
Ahmed T, Haboubi N (2010) Assessment and management of nutrition in older people and its importance to health. Clin Interv Aging 5:207–216
Ignacio de Ulíbarri J, González-Madroño A, de Villar NG et al (2005) CONUT score: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp 20:38–45
Iwasaki I, Nagai T, Furukawa TA et al (2017) Prognostic value of malnutrition assessed by controlling nutritional status score for long-term mortality in patients with acute heart failure. Int J Cardiol 230:529–536
Fukushima K, Ueno Y, Kawagishi N et al (2011) The nutritional index ‘CONUT’ is useful for predicting long-term prognosis of patients with end-stage liver disease. Tohoku J Exp Med 224:215–219
Iseki Y, Shibutani M, Maeda K et al (2015) Impact of the preoperative controlling nutritional status (CONUT) score on the survival after curative surgery for colorectal cancer. PLoS ONE 10:e0132488
Hirahara N, Matsubara T, Hayashi H et al (2016) Prognostic importance of controlling nutritional status in patients undergoing curative thoracoscopic esophagectomy for esophageal cancer. Am J Ther. https://doi.org/10.1097/mut.0000000000000414
Shoji F, Haratake N, Akamine T et al (2017) The preoperative controlling nutritional status score predicts survival after curative surgery in patients with pathological stage I non-small cell lung cancer. Anticancer Res 37:741–747
Yoshida N, Baba Y, Shigaki H et al (2016) Preoperative nutritional assessment by controlling nutritional status (CONUT) is useful to estimate postoperative morbidity after esophagectomy for esophageal cancer. World J Surg 40:1910–1917. https://doi.org/10.1007/s00268-016-3549-3
Yoshida N, Harada K, Baba Y et al (2017) Preoperative controlling nutritional status (CONUT) is useful to estimate the prognosis after esophagectomy for esophageal cancer. Langenbecks Arch Surg 402:333–341
Japanese Gastric Cancer Association (2011) Japanese classification of gastric carcinoma, 3rd English edition. Gastric Cancer 14:101–112
Japanese Gastric Cancer Association (2017) Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 20:1–19
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Tokunaga M, Tanizawa Y, Bando E et al (2013) Poor survival rate in patients with postoperative intra-abdominal infectious complications following curative gastrectomy for gastric cancer. Ann Surg Oncol 20:1575–1583
Hayashi T, Yoshikawa T, Aoyama T et al (2015) Impact of infectious complications on gastric cancer recurrence. Gastric Cancer 18:368–374
Hu WH, Cajas-Monson LC, Eisenstein S et al (2015) Preoperative malnutrition assessments as predictors of postoperative mortality and morbidity in colorectal cancer: as analysis of ACS-NSQIP. Nutr J. https://doi.org/10.1186/s12937-015-0081-5
Sakurai K, Ohira M, Tamura T et al (2016) Predictive potential of preoperative nutritional status in long-term outcome projections for patients with gastric cancer. Ann Surg Oncol 23:525–533
McMilan DC, Elahi MM, Sattar N et al (2001) Measurement of the systemic inflammation response predicts cancer-specific and non-cancer survival in patients with cancer. Nutr Cancer 41:64–69
Crumley ABC, Stuart RC, McKeranan M et al (2010) Is Hypoalbuminemia an independent prognostic factor in patients with gastric cancer? World J Surg 34:2393–2398. https://doi.org/10.1007/s00268-010-0641-y
Kuzuya M, Izawa S, Enoki H et al (2007) Is serum albumin a good marker for malnutrition in the physically impaired elderly? Clin Nutr 26:84–90
Hoffmann TK, Dworacki G, Tsukihiro T et al (2002) Spontaneuos apotosis of circulating T lymphocytes in patients with head and neck cancer and its clinical importance. Clin Cancer Res 8:2553–2562
Strasak AM, Pfeiffer RM, Brant LJ et al (2009) Time-dependent association of total serum cholesterol and cancer incidence in a cohort of 172210 men and women: a prospective 19-year follow-up study. Ann Oncol 20:1113–1120
Wang Q, Lau WY, Zhang B et al (2016) Preoperative total cholesterol predicts postoperative outcomes after partial hepatectomy in patients with chronic hepatitis B- or C-related hepatocellular carcinoma. Surgery 155:263–270
Cengiz O, Kocer B, Süemeil S et al (2006) Are pretreatment serum albumin and cholesterol levels prognostic tools in patients with colorectal carcinoma? Med Sci Monit 12:CR240–CR247
Toyokawa T, Kubo N, Tamura T et al (2016) The pretreatment controlling nutritional status (CONUT) score is an independent prognostic factor in patients with resectable thoracic esophageal squamous cell carcinoma: results from a retrospective study. BMC Cancer 16:722–732
Makary MA, Segev DL, Pronovost PJ et al (2010) Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg 210:901–908
Revenig LM, Canter DJ, Taylor MD et al (2013) Too frail for surgery? initial results of a large multidisciplinary prospective study examining preoperative variables predictive of poor surgical outcomes. J Am Coll Surg 217:665–670
Nashimoto A (2013) Current status of treatment strategy for elderly patients with gastric cancer. Int J Clin Oncol 18:969–970
Weimann A, Braga M, Carli F et al (2017) ESPEN guideline: clinical nutrition in surgery. Clin Nutr 36:623–650
Jie B, Jiang ZM, Nolan MT et al (2012) Impact of preoperative nutritional support on clinical outcome in abdominal surgical patients at nutritional risk. Nutrition 28:1022–2017
Mazaki T, Ishii Y, Murai I (2015) Immunoenhancing enteral and parental nutrition for gastrointestinal surgery a multiple-treatments meta-analysis. Ann Surg 261:662–669
MortensenK Nilsson M, Slim L et al (2014) Consensus guidelines for enhanced recovery after gastrectomy: enhanced recovery after surgery (ERAS(R)) society recommendations. Br J Surg 101:1209–1229
Tanaka R, Lee SW, Kawai M et al (2017) Protocol for enhanced recovery after surgery improves short-term outcomes for patients with gastric cancer: a randomized clinical trial. Gastric Cancer 20:861–871
Morgan J, Guinan E, McCormic P et al (2014) The ability of prehabilitation to influence postoperative outcome after intra-abdominal operation: a systemic review and meta-analysis. Surgery 155:124–133
Silver JK, Baima J (2013) Cancer prehabilitation: an opportunity to decrease treatment-related morbidity, increase cancer treatment options, and improve physical and psychological health outcomes. Am J Phys Med Rehabil 92:715–727
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have no conflicts of interest or financial to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Suzuki, S., Kanaji, S., Yamamoto, M. et al. Controlling Nutritional Status (CONUT) Score Predicts Outcomes of Curative Resection for Gastric Cancer in the Elderly. World J Surg 43, 1076–1084 (2019). https://doi.org/10.1007/s00268-018-04889-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-018-04889-6