
Abstract
Background
Adrenocortical carcinoma (ACC) is rare but often fatal. Surgery offers the only chance of cure. As minimally invasive (MI) procedures for cancer become common, their role for ACC is still debated. We reviewed usage of MI approaches for ACC over time and risk factors for conversion using a large national database.
Methods
ACC patients with localized disease were identified in the National Cancer Data Base from 2010 to 2014. A retrospective review examined trends in the surgical approach over time. Patient demographics, surgical approach, and tumor characteristics between MI, open, and converted procedures were compared.
Results
588 patients underwent adrenalectomy for ACC, of which 200 were minimally invasive. From 2010 to 2014, MI operations increased from 26 to 44% with robotic procedures increasing from 5 to 16%. The use of MI operations compared to open was not different based on facility type (p = 0.40) or location (p = 0.63). MI tumors were more likely to be confined to the adrenal (p < 0.001) but final margin status was not different (p = 0.56). Conversion was performed in 38/200 (19%). Average tumor size was 10.2 cm in the converted group compared to 8.6 cm in the MI group (p = 0.09). There was no difference in extent of disease (p = 0.33), margin status (p = 0.12), or lymphovascular invasion (p = 0.59) between MI and converted procedures. Tumor size > 5 cm was the only significant predictor of conversion (p = 0.04). No patients with pathologic stage I disease required conversion (0/19).
Conclusions
The frequency of MI approaches for ACC is increasing. In the final year of the study, 44% of adrenalectomies were MI. Size > 5 cm was the only significant predictor of conversion.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adrenocortical carcinoma is a rare disease affecting less than one person per million. The prognosis is poor and five-year overall survival ranges from 38 to 46% [1]. Open adrenalectomy has traditionally been recommended due to the large size of these tumors, tendency for local invasion, and high propensity for implantation. Surgeons have been deterred from adopting a MI approach by previously published reports of poor outcomes after laparoscopic resection including positive margins, earlier time to recurrence, and development of peritoneal carcinomatosis. A complete oncologic resection is critical for ACC because of the lack of effective adjuvant therapy. MI surgery has multiple advantages that are well described for benign adrenal tumors, but evidence to support the safety and efficacy for ACC is lacking. In order to evaluate whether minimally invasive techniques are being used for adrenocortical cancer, we examined the trends in operative approaches for this tumor using the National Cancer Data Base (NCDB). We examined differences in outcomes between MI and open, as well as possible risk factors for conversion to an open procedure.
Methods
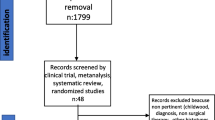
The NCDB was queried for cases of adrenocortical carcinoma from 2010 to 2014. The earliest year of 2010 was chosen because surgical approach data became available then. 1459 patients with adrenocortical carcinoma were identified using histology code 8370 within the NCDB. Patients with more than one malignant diagnosis, metastatic disease, and undefined operative approach were excluded. Using these inclusion and exclusion criteria, 588 patients were included in the study (Fig. 1). Of these, 151 were treated with laparoscopic adrenalectomy, 49 with robotic adrenalectomy, and 388 with an open procedure. The frequency of each surgical approach during the study period was compared to identify utilization trends over time.

Selection map
Characteristics of the MI group and the open group were compared using an intent-to-treat model (all MI cases were included regardless of conversion status). To evaluate differences between the MI and converted group, the patients having a successful MI surgery were compared to the patients requiring conversion to open. Chi-square test was used for categorical variables and t test for continuous variables. Both univariate and multivariable analyses were performed to identify predictors of conversion. Characteristics analyzed included age at diagnosis, gender, ethnicity, primary tumor size > 5 cm, laterality, insurance status, Charlson–Deyo comorbidity index, presence of lymphovascular invasion, adjuvant chemotherapy and/or radiation, and American Joint Committee on Cancer (AJCC) pathologic stage. Facility type was categorized using the NCDB definitions of academic center, community cancer program, comprehensive community cancer program, or integrated network cancer program. Facility location was analyzed by the nine NCDB geographic designations throughout the USA. Margin status was categorized as negative (R0) or positive (R1 or R2). Data on nodal status were missing for the majority of patients (92%) and were consequently excluded from analysis. Extent of disease was categorized as localized or extra-adrenal with any extension beyond the capsule including into adjacent organs. Postoperative outcomes were evaluated using 30-day mortality, 30-day hospital readmission, and length of stay. A Kaplan–Meier survival curve was created to evaluate overall survival, and Cox regression analysis was used to identify independent predictors of a worse outcome. All data analyses were performed using SAS 9.4 (Cary, NC), and a p < 0.05 was considered statistically significant.
Results
During the study period, 1459 patients with ACC were identified, of whom 588 met inclusion criteria (Fig. 1). A MI approach was used in 200 (34%) patients and an open approach in 388 (66%). Between 2010 and 2014, the use of MI surgery increased almost twofold from 26 to 44%, while robotic adrenalectomy increased more than threefold from 5 to 16%. Open adrenalectomy accounted for 74% of the procedures in 2010 and 56% in 2014 (Fig. 2). Among patients undergoing MI surgery, there was no difference in overall conversion rate between laparoscopic adrenalectomy and robotic adrenalectomy (21 vs. 12%, p = 0.17). Although the numbers of robotic adrenalectomy grew at a faster rate during the study period, it was trending toward to a lower conversion rate compared to laparoscopic adrenalectomy. However, this was not statistically significant (Table 1).

Frequency of surgical approach by year (%)
Characteristics of patients having MI and open adrenalectomy were compared (Table 2). When considering known preoperative variables, there was no difference in the use of MI surgery based on tumor laterality, insurance status, facility type, or geographic location. Only tumor size > 5 cm was significantly different between the two groups (p > 0.001). Average tumor size was greater in the open group as compared to the MI group (12.4 ± 6.9 vs. 8.9 ± 6.2 cm, p < 0.001). The MI group was more likely to have disease confined to the adrenal and present with earlier stage disease; however, there was no difference in final margin status. The open group was more likely to have adjuvant chemotherapy.
To determine factors associated with conversion, the MI surgery group was compared to the converted group (Table 3). There was no difference in age, gender, race, insurance status, Charlson–Deyo comorbidity index, extent of disease, laterality, margin positivity, AJCC pathologic stage, or lymphovascular invasion between the two groups. None of the patients with pathologic stage I disease required conversion (0/19). Twenty-five percent of stage II (13/52), 16% of stage III (5/31), and 30% of stage IV patients (3/10) were converted to open, but the difference was not statistically significant. Size greater than 5 cm was the only predictor of conversion on multivariable analysis (p = 0.04). The overall conversion rate for tumors > 5 cm was 22%, while the conversion rate for tumors ≤ 5 cm was 7%. The average tumor size was 8.6 cm (± 6.3 SD) for the MI group and 10.2 cm (± 5.1 SD) for the converted group, respectively.
Table 4 summarizes the short-term outcomes between the MI and the converted groups. There were no deaths within 30 days in either group but the data were missing in 27% of the MI group and 32% of the converted group. No difference was seen between the groups for 30-day readmission (p = 0.77). Average length of stay was shorter for the MI group compared to the converted group (3.7 vs. 6.3 days, p = 0.02).
Overall survival for the converted group was worse compared to the MI group in both unadjusted and adjusted analyses (Fig. 3). The median survival for the MI group was twice that of the converted group (4.7 vs. 2.3 years, p = 0.005). In multivariable Cox analysis, MI converted to open (HR 2.1, 95% CI 1.1–3.9), tumor size > 5 cm (HR 1.02, 95% CI 1.01–1.02) and positive margin (HR 2.4, 95% CI 1.2–4.7) were the independent predictors of worse overall survival among patients undergoing MI adrenalectomy.

Overall survival for patients with ACC with a minimally invasive procedure versus converted to an open operation
Despite the worse survival seen in the converted group, there was no difference in overall survival between the MI and open groups in both unadjusted and adjusted analyses (Fig. 4). Median survival for the MI group was 4.4 years compared to 4.6 years in the open group. In multivariable Cox analysis, positive margin (HR 2.08, 95% CI 1.35–3.20) and lymphovascular invasion (HR 1.60, 95% CI 1.07–2.38) were the independent predictors of worse overall survival.

Overall survival for patients with ACC with a minimally invasive procedure versus open operation
Discussion
As the use of minimally invasive surgery for cancer becomes more widespread, the oncologic outcomes of these techniques compared to the open approach continue to be scrutinized. Minimally invasive adrenalectomy for small, benign lesions has become standard, while there is mixed evidence about the outcomes of these techniques for adrenocortical carcinoma. Adjuvant treatments offer limited benefit for this disease, and therefore a complete oncologic resection is critical. Due to reports of shorter time to recurrence and peritoneal carcinomatosis, the clinical impression has been that prolonged disease-free and overall survival can be best achieved with an open operation [2,3,4,5]. Despite these observations, we found in our study that the use of MI techniques in ACC is increasing. This contrasts with the most recently published 2017 recommendation by the National Comprehensive Cancer Network that states open adrenalectomy is the preferred approach for preoperatively suspected adrenal cancer. These recommendations specifically state that there is an increased risk of peritoneal spread and local recurrence with laparoscopic resection [2]. In our data, the use of MI adrenalectomy accounted for almost half (44%) of procedures in the final year of study.
Characteristics of patients having a MI adrenalectomy were compared to those having an open operation. Smaller tumor size was predictive of having a minimally invasive procedure (p < 0.001) (Table 2). MI procedures were more likely to have tumors confined to the adrenal, but there was no difference in pathologic margin status between MI and open groups. In our data, despite smaller tumor size predicting the use of MI surgery, large tumor size was not a clear deterrent to the use of a MI approach. The average tumor size was 8.9 cm in the MI group and 12.4 cm in the open group. There were no differences in the use of MI procedures based on facility type or location throughout the USA. In one of the largest studies to date comparing MI to open adrenalectomy, including 13 tertiary care facilities and 201 patients, smaller tumor size was the only preoperative predictor of MI surgery. Similar to our study, they did not identify any differences in utilization based on institution [6].
Although ACC may not always be diagnosed preoperatively, large tumor size is well known to be associated with an increased risk of cancer [5, 7, 8]. Specifically, a study performed by Sturgeon et al. from Northwestern University comparing data from the Surveillance, Epidemiology, and End Results Program (SEER) to retrospective single institution data found that the size of the primary tumor was highly predictive of the presence of ACC. Tumors > 8 cm had a likelihood ratio of 16.9 of being ACC compared with tumors < 8 cm [8]. Similarly, in an institutional prospective series from Oxford University Hospitals in the UK reviewing adrenal tumors > 8 cm seen from 2000 to 2013, Abdel-Aziz et al. found that 81% (31/37) were ACC on final pathology [7]. With the average tumor size in our study > 8 cm, it can be inferred that the majority of MI cases were done with the suspicion for malignancy.
The advantages of laparoscopic and robotic adrenalectomy are well described. These include decreased postoperative pain, decreased hospital length of stay, less blood loss, and earlier return to normal activity when compared to open surgery [9]. Our data showed an average length of stay of 3.7 days for MI surgery compared to 6.3 days for converted procedures (Table 4). Compared to laparoscopy, robotic adrenalectomy offers additional technical advantages. Three-dimensional camera magnification of the operative field and wristed instruments aid in difficult dissection, careful handling of delicate adrenal tissue and vascular structures during adrenalectomy. Although most series describing robotic adrenalectomy are small and were performed for benign tumors, based on our data it does appear that this technique is being used for ACC more frequently [10,11,12]. The largest review series at this time for robotic adrenalectomy was a review of technique and outcomes in 26 studies published in 2016 by Xin et al. from Singapore. Most patients included had benign disease. However, they concluded that robotic adrenalectomy in general is safe and effective when compared to laparoscopy [10]. There is a paucity of literature describing outcomes of robotic adrenalectomy for ACC. More data are needed to evaluate this practice as it becomes more common.
Previous reports have identified MI surgical approach as a risk factor for the development of peritoneal carcinomatosis (PC) in ACC. Leboullex et al. reported a single institution retrospective cohort study of 64 French patients with ACC having surgery from 2003 to 2009 [3]. Only six patients in this group had laparoscopic surgery. However, they did find an association with development of PC during the follow-up period since 67% of the laparoscopic operations developed PC compared to 27% of the open operations. Gonzalez et al. from MD Anderson Cancer Center reported an 8% risk of PC in patients treated with open adrenalectomy and a startling 83% risk of PC in patients having a laparoscopic adrenalectomy [4]. A retrospective series from the University of Michigan of 17 patients undergoing laparoscopic adrenalectomy also found earlier time to recurrence (9.6 vs. 19.2 months for open) and recommended against MI adrenalectomy [5]. Although there is no consensus about the ideal approach for resection of an adrenal cancer, R0 resection is associated with a recurrence rate of 23% versus 51% for R1 and R2 resections [13]. Further study is needed to determine if there is an independent relationship between the surgical approach, time to recurrence, and disease-specific survival.
Tumor size is frequently discussed in adrenal surgery concerning both the feasibility of minimally invasive approaches and rates of conversion. The tumor size threshold for surgeons to attempt MI resection has increased over time with individual and institutional experience, as well as improving laparoscopic and robotic technologies [11, 14]. In addition to size, the tendency for local invasion is frequently but not always suspected based on preoperative imaging and may alter the surgical approach if suspected preoperatively or encountered during the operation. Previous reports cite bleeding, tumor size, local tumor invasion, adhesions, and body habitus as contributing factors for conversion to open adrenalectomy [10, 13, 15, 16]. Our analysis showed that tumor size greater than 5 cm was associated with conversion (p = 0.04). All patients with stage I tumors had a successful minimally invasive procedure. The overall conversion rate for tumors > 5 cm was 22 versus 7% for tumors less than 5 cm. Interestingly, tumor extension outside the adrenal gland was not more common in the converted group (p = 0.33). In the MI group, 27% (44/162) had locally invasive tumors compared to 24% (9/38) in the converted group.
To evaluate perioperative morbidity, we used data points available through the NCDB as surrogate markers including 30-day mortality, 30-day readmission, and length of hospital stay. Mortality and readmission rates were not different. However, 30-day mortality must be interpreted with caution due to a large amount of missing data (28% of patients). Length of stay for MI adrenalectomy was 3.7 days (range 0–38) and 6.3 days (range 1–56) for converted procedures (p = 0.02). Surgery-specific factors that may have contributed to conversion cannot be identified such as surgeon experience or volume, intra-operative blood loss, operative time, or patient body mass index. Based on our findings of an increased conversion rate, we suggest that tumor size > 5 cm should warrant caution when choosing a MI resection for a suspected ACC.
In our study, we saw a decreased overall survival for the converted group. This was present in both the unadjusted and adjusted analysis when controlling for multiple factors, including positive margin and tumor size. Previous studies have reported that complete surgical resection confers a five-year survival of 32 to 50% in patients with localized ACC. The risk of recurrence after surgical resection for ACC can be as high as 50 to 85% [16]. In our data, overall survival for the converted group was 60% at one year versus 80% for the minimally invasive group. There was no difference in positive margins, 30-day readmission, or mortality. The converted group did have a larger tumor size, which has been associated with worse disease-free survival [16]. However, when controlling for these factors, overall survival was still worse in the converted group, indicating there are other factors influencing this outcome.
When the MI group was compared to open, we did not see a difference in overall survival on unadjusted or adjusted analysis (Fig. 4). The MI group had smaller tumors on average, and more disease confined to the adrenal. Positive margin status and presence of lymphovascular invasion did not differ between groups (Table 2). In multivariable Cox analysis, positive margin (HR 2.08, 95% CI 1.35–3.20) and lymphovascular invasion (HR 1.60, 95% CI 1.07–2.38) were the independent predictors of worse overall survival.
In addition to the retrospective nature of this study, there are several limitations. We cannot examine contributing factors such as surgeon experience, tumor capsule rupture or spillage of tumor, perioperative blood loss, operative time, tumor functionality, development of local recurrence, or metastatic disease. The NCDB does not identify time to recurrence or disease-specific survival. Caution should be used when interpreting the survival data, especially the worse overall survival in the converted group, due to the limitations mentioned above. Further study is needed to compare disease-specific outcomes for MI versus open adrenalectomy for ACC.
Conclusion
The frequency of minimally invasive surgery for adrenocortical carcinoma is increasing. Up to 44% of all adrenalectomies were performed using a MI approach in the final study year. Smaller tumor size predicted the use of minimally invasive surgery. Size > 5 cm was the only significant predictor of conversion to open.
References
Bilimoria K, Shen W, Elaraj D et al (2008) Adrenocortical carcinoma in the United States: treatment utilization and prognostic factors. Cancer 113:3130–3136
National Comprehensive Cancer Network. Neuroendocrine Tumors (Version 2.2017) http://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf. Accessed May 18, 2017
Leboulleux S, Deandreis D, Al Ghuzlan A et al (2010) Adrenocortical carcinoma: is the surgical approach a risk factor of peritoneal carcinomatosis? Eur J Endocrinol 162:1147–1153
Gonzalez R, Shapiro S, Sarlis N et al (2005) Laparoscopic resection of adrenal cortical carcinoma: a cautionary note. Surgery 138:1078–1085
Miller B, Ammori J, Broome J et al (2010) Laparoscopic resection is inappropriate for known or suspected adrenocortical carcinoma. World J Surg 34:1380–1385. doi:10.1007/s00268-010-0532-2
Lee C, Salem A, Schneider D et al (2017) Minimally invasive resection of adrenocortical carcinoma: a multi-institutional study of 201 patients. J Gastrointest Surg 21:352–362
Abdel-Aziz T, Rajeev P, Sadler G et al (2015) Risk of adrenocortical carcinoma in adrenal tumors > 8cm. World J Surg 39:1268–1273. doi:10.1007/s00268-014-2912-5
Sturgeon C, Shen W, Clark O et al (2006) Risk assessment in 457 adrenal cortical carcinomas: how much does tumor size predict the likelihood of malignancy? J Am Coll Surg 202:423–430
Dovirak O, Mao J, Taylor K et al (2016) How to quantify recovery after laparoscopic adrenalectomy: an assessment of patient-reported health-related quality of life. Surg Laparosc Endosc Percutan Tech 26:290–294
Xin L, Sey K (2016) Robotic assisted adrenalectomy: is it ready for prime time? Investig Clinc Urol 57:S130–S146
Carnaille B (2012) Adrenocortical carcinoma: which surgical approach? Langenbecks Arch Surg 397:195–199
Park J, Kim S, Lee C et al (2013) Robot-assisted posterior retroperitoneoscopic adrenalectomy using single-port access: technical feasibility and preliminary results. Ann Surg Oncol 20:2741–2745
Crucitti F, Bellantone R, Ferrante A et al (1996) The italian registry for adrenal cortical carcinoma: analysis of a multi-institutional series of 129 patients. Surgery 119:161–170
Sautter A, Cunningham S, Kowdley G et al (2016) Laparoscopic adrenalectomy for adrenal cancer-a systematic review. Am Surg 82:420–426
Gaujoux S, Bonnet S, Leconte M et al (2011) Risk factors for conversion and complications after unilateral laparoscopic adrenalectomy. Br J Surg 10:1292–1299
Kim Y, Margonis G, Prescott J et al (2017) Curative surgical resection of adrenocortical carcinoma: determining long-term outcome based on conditional disease-free probability. Ann of Surg 265:197–204
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Calcatera, N.A., Hsiung-Wang, C., Suss, N.R. et al. Minimally Invasive Adrenalectomy for Adrenocortical Carcinoma: Five-Year Trends and Predictors of Conversion. World J Surg 42, 473–481 (2018). https://doi.org/10.1007/s00268-017-4290-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-017-4290-2