
Abstract
Rationale
Substantial use of the plant kratom for psychoactive effects has driven interest in its abuse liability. Several place conditioning studies suggest abuse liability of the active ingredient mitragynine, though studies of its self-administration have not been published.
Methods
Binding of mitragynine to rat brain mu, kappa, and delta opioid receptors was compared to that for heroin and morphine. Self-administration of mitragynine, heroin, methamphetamine, or saline was assessed during single-session substitutions in rats trained to self-administer methamphetamine (0.022 mg/kg/injection, i.v.) during 1-h daily sessions.
Results
Mitragynine had > 2- or ~ 16-fold greater affinity for the mu opioid receptor than, respectively, for kappa or delta opioid receptors. Its affinity for the mu receptor was ~ 200-fold less than that for morphine. In rats trained to self-administer methamphetamine, saline substitutions significantly decreased the number of responses, whereas different doses of methamphetamine (0.002–0.068 mg/kg/injection) or heroin (0.001–0.03 mg/kg/injection) maintained self-administration with maximal responding at 0.022 or 0.01 mg/kg/injection, respectively. In contrast, no dose of mitragynine maintained response rates greater than those obtained with saline. Presession mitragynine treatment (0.1 to 3.0 mg/kg) decreased response rates maintained by heroin but had little effect on responding maintained by methamphetamine across the same range of doses.
Conclusions
These results suggest a limited abuse liability of mitragynine and potential for mitragynine treatment to specifically reduce opioid abuse. With the current prevalence of opioid abuse and misuse, it appears currently that mitragynine is deserving of more extensive exploration for its development or that of an analog as a medical treatment for opioid abuse.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Significant use of the plant kratom for its psychoactive effects has prompted interest by the United States Drug Enforcement Agency (DEA) to temporarily place the active ingredients of the plant, mitragynine, and 7-hydroxymitragynine, into Schedule I of the Controlled Substances Act as an abusable substance (US Drug Enforcement Administration 2016). The notice of that intent by DEA was met with responses from the public, commercial, and legislative sectors which included testimonials though little scientific evidentiary support for those various responses (Henningfield et al. 2018).
Kratom is the commonly used term for the leaves of Mitragyna speciosa, which contain a variety of constituents. Mitragynine accounts for 66% of total alkaloid content in some geographical variants of the plant with variations among species studied and interactions among the various kratom constituents (Takayama 2004). 7-OH-Mitragynine is also present at lower levels with a 5- to 10-fold higher affinity for μ-opioid receptors (Kruegel et al. 2016). As levels in brain tissue after intravenous injection of mitragynine indicate suitable brain penetration from plasma (Kong et al. 2017), it is likely that mitragynine is the main pharmacologically active alkaloid in kratom (Kruegel and Grundmann 2018), though see the description below of a study of kratom extracts (Sufka et al. 2014).
Several studies in animal subjects have examined various behavioral effects including the abuse potential of mitragynine (see Hassan et al. 2017; Kruegel and Grundmann 2018 for reviews). A study of place conditioning (Sufka et al. 2014) administered different doses of mitragynine or an extract of Mitragyna speciosa leaves over eight conditioning sessions, half of which were preceded with mitragynine injection and half with vehicle. Significant place conditioning was obtained in rats administered 5 or 30 mg/kg of mitragynine though the effect eluded statistical significance at 10 mg/kg. Though the kratom extract increased place conditioning, it was not to a statistically significant extent. The authors interpreted the diminished effect of the extract as possibly due to lower concentrations of mitragynine in the extract or the presence of other plant constituents with effects interfering with the effect of mitragynine. Yusoff et al. (2016), using a similar procedure, found significant place conditioning in rats administered 10 or 30 mg/kg of mitragynine over ten conditioning sessions. In a subsequent study (Yusoff et al. 2017), the place conditioning induced by 10 mg/kg of mitragynine was blocked by the co-administration of naloxone (0.3 or 1.0 mg/kg), indicating that the place conditioning was mediated by opioid receptors. However, there are studies suggesting non-opioid effects of mitragynine (Kruegel and Grundmann 2018), and a recent report of baclofen blockade of mitragynine-induced place conditioning suggests potential GABAB receptor involvement in that effect (Yusoff et al. 2018).
Harun et al. (2015) compared the discriminative stimulus effects of mitragynine (15 mg/kg, i.p.) to those of morphine (5.0 mg/kg) in separate groups of rats each trained with one of the compounds. Both groups acquired discriminative control, though the morphine group acquired that control more rapidly. Each training drug produced a dose-related generalization to the training dose and each drug dose-dependently substituted for the other. Further 7-OH-mitragynine substituted for morphine more potently than did mitragynine. Interestingly, the discriminative effects of mitragynine were only incompletely antagonized by naloxone (Harun et al. 2015).
In a recent report (Hemby et al. 2018), rats were trained to reliably self-administer morphine (50 or 100 μg/infusion) under a fixed-ratio 3-response schedule, followed by replacement of drug with saline and extinction of responding. Following extinction, rats were allowed to self-administer different doses of mitragynine or 7-OH-mitragynine. No dose of mitragynine (25 to 150 μg/injection) maintained rates of responding significantly greater than those maintained by saline. In contrast, 7-OH-mitragynine maintained rates above those for saline at 2.5 to 20 μg/injection and also did so in a separate group of subjects without experience self-administering morphine. Both the μ-opioid receptor selective antagonist naloxonazine and the δ-opioid receptor antagonist naltrindole decreased self-administration of 7-OH-mitragynine but only naloxonazine decreased morphine self-administration.
The present study was designed to further assess the abuse liability of mitragynine using a self-administration procedure in rats. To confirm opioid activity, the displacement by mitragynine of opioid radioligands was studied using native rat tissue and compared to that produced by the standard opioids, morphine, and heroin. These binding affinities helped select doses tested to ensure that biologically active doses of mitragynine were studied.
Methods
Receptor binding assays
Whole rat brain tissue excluding the cerebellum was thawed on ice, then homogenized in 50 mM Tris HCl, pH 7.5 using a Brinkman Polytron (setting 6 for 20 s), and centrifuged at 30,000 × g for 10 min at 4 °C. The supernatant was discarded and the pellet was resuspended in fresh buffer and spun at 30,000×g for 10 min. The supernatant was discarded and the pellet was resuspended to give 100 mg/ml original wet weight. Ligand-binding experiments were conducted in polypropylene assay tubes containing 0.5 ml Tris HCl buffer for 60 min at room temperature. [3H]DADLE (final concentration 1 nM, PolyPeptide Laboratories, San Diego, CA), [3H]DAMGO (final concentration 1 nM, PolyPeptide Laboratories, San Diego, CA), or [3H]U-69,593 (final concentration 1 nM, Perkin Elmer Life Sciences, Waltham, MA) were used to determine binding at the delta, mu, and kappa opioid receptor sites, respectively. Unlabeled DAMGO (final concentration, 30 nM) was added to the delta receptor assay tubes to block the binding of the radioligand to mu opioid receptors. All assay tubes contained 100 μl homogenate suspension. Non-specific binding was determined using 0.01 mM naloxone for all assays. Incubations were terminated by rapid filtration through Whatman GF/B filters, presoaked in 0.1% PEI (polyethyleneimine), using a Brandel R48 filtering manifold (Brandel Instruments, Gaithersburg, MA). The filters were washed twice with 5 ml cold buffer and transferred to scintillation vials. Cytoscint (MP BioMedicals, Santa Ana, CA) (3.0 ml) was added and the vials were counted the next day using a Perkin Elmer TriCarb liquid scintillation counter.
Data were analyzed by using GraphPad Prism software (San Diego, CA). Inhibition constants (Ki values) were calculated using the Cheng-Prusoff equation (Cheng and Prusoff 1973), with IC50 value of inhibitors used in the assay and the Kd value of the radioligand previously determined in this laboratory.
Subjects for behavioral experiments
Six male Sprague-Dawley rats (obtained from the Animal Center of the Tongji Medical College of Hua Zhong University of Science & Technology, Wuhan, China) served as subjects and were acclimated to a temperature- and humidity-controlled room for at least 1 week before any procedures. Food and water were available at all times in their home cages. The housing room was under a 12:12-h light/dark cycle with lights on at 7:00 AM. After acclimation, body weights of subjects were maintained at approximately 320 g. The experimental protocol was approved by an Institutional Review Committee for the use of Animal Subjects. All procedures and facilities were operated in accordance with the Guide for the Care and Use of Laboratory Animals of Jianghan University.
After the 1-week acclimation to the facility, a chronic intravenous catheter (3.5 cm in length, 0.58 mm inner diameter, 0.91 mm outer diameter, BPU-T30, Instech, Plymouth Meeting, PA, USA) was surgically implanted in the subject and secured to the right jugular vein under sodium pentobarbital (50 mg/kg, i.p.) anesthesia, as per Kai et al. (2014). Catheters exited dorsally in the mid-scapular region through a back mount that was secured subcutaneously. Following surgery, rats were housed individually in home cages and allowed at least 7 days of recovery during which they received daily intravenous infusions of gentamicin (0.16 mg/kg) followed by 0.2 ml of a heparinized (1%) sterile saline solution to minimize the likelihood of infection and the formation of clots or fibroids.
Behavioral procedures
All self-administration experiments were conducted in operant-conditioning chambers (29 × 26 × 29 cm) enclosed in sound-attenuating and light-proof cubicles which were equipped with fans that provided ventilation (Anilab Software & Instruments Co., Ltd., China) (Zhang 2006). Two nose-poke operanda (ENV-114M; Med Associates, Fairfax, VT) were located 9 cm above the floor on the front panels of the chambers. A red stimulus light was mounted within each nose-poke hole and a white house light was mounted near the ceiling on the opposite wall. A syringe driver (model 22; Harvard Apparatus, Holliston, MA) containing a 10-ml syringe delivered injections. The syringe was connected by tubing to a fluid swivel (375 Series Single Channel Swivels, Instech Laboratories, Inc., Plymouth Meeting, PA) mounted on a balance arm above the chamber. Tubing, protected by a metal surrounding spring, connected the swivel to the subject’s catheter.
Subjects were placed in chambers during daily 1-h experimental sessions in which subjects were initially trained with responses producing methamphetamine injections under a FR 5-response schedule (each fifth response produced a 0.022 mg/kg/injection of methamphetamine). During these sessions, the white house light was illuminated when methamphetamine injections were available. A single nose poke in the left hole turned on the red stimulus light within that hole for 0.5 s. Completion of each FR 5 requirement turned off the house light, delivered the methamphetamine injection, and was followed by a 20-s timeout (TO) period during which all lights were off and responses were recorded but had no scheduled consequences. After the TO, the house light was illuminated and the FR schedule was again in effect. When response rates were sufficiently high to produce 25 injections per session and were reliable from one session to the next, training sessions with methamphetamine (M) and saline (S) injections were conducted in a double-alternation sequence (e.g., ...MMSSMMSS..., where M—methamphetamine and S—saline).
When the response rates were reliably higher during methamphetamine sessions than during saline sessions, tests (T) of substitutions with saline or various doses of methamphetamine, heroin, or mitragynine were assessed by inserting those tests between repeats of the double-alternation sequence [e.g., ...MSTSMTMST...]. Each dose was tested once in each of the six subjects. Subsequently, the effects of mitragynine on heroin or methamphetamine self-administration were assessed by administering various mitragynine doses [saline, 0.03, 0.1, 0.3, 1 and 3 mg/kg, i.p.] 5 min before test sessions as described above in which different doses of either heroin or methamphetamine were available for self-administration. The sequence of mitragynine dose testing was balanced among rats using a Latin square design.
Numbers of responses were tabulated for each subject and analyzed with one-way analyses of variance (ANOVA) with drug dose as a factor. Post hoc analyses were conducted to assess contributions to significant effects using Holm-Sidak Multiple Comparisons versus saline. The levels of inactive responses were separately analyzed using one-way ANOVAs.
Drugs
Mitragynine was obtained in “technical grade” from Carbosynth Limited (Compton, Berkshire, UK) and was dissolved in Tween 20 and DMSO, then diluted to the necessary concentration with 0.9% NaCl. Heroin HCl and methamphetamine HCl were obtained from the Hubei Public Security Bureau and were dissolved in 0.9% NaCl.
Results
Receptor binding assays
The Ki value for the displacement of [3H]DAMGO from the μ-opioid receptor by mitragynine was 502 nM, which indicated greater affinity for that receptor than that for κ- and δ-opioid receptors (Table 1). The Ki values for the displacement of [3H]U-69,593 and [3H]DADLE from κ- and δ-opioid receptors, respectively, were significantly greater than that for displacement of [3H]DAMGO. The affinity of mitragynine for the μ-opioid receptor was substantially lower than that for either heroin or morphine (Table 1). Values for heroin are likely due entirely to the affinity of its metabolite 6-acetylmorphine (Inturrisi et al. 1983).
Drug self-administration
The dose-effect curves for heroin and methamphetamine were biphasic for active responses (Fig. 1, center and right panels, filled symbols), with maximal effects at 0.01 and 0.022 mg/kg/injection, respectively. The ANOVA indicated that the differences in the mean values among heroin doses were greater than would be expected by chance (F4,20 = 8.32, P < 0.001). A similar result for dose was obtained with the ANOVA for methamphetamine (F4,20 = 76.2, P < 0.001). In contrast, no dose of mitragynine increased responding to levels greater than those obtained with saline (Fig. 1, left panel, filled symbols). However, the ANOVA indicated that the differences in the mean values among mitragynine doses were greater than would be expected by chance (F5,25 = 3.05, P = 0.028). Post hoc analysis indicated that the significance in the overall ANOVA was a result of the decreases in responding that were observed at the 3.0 mg/kg/injection dose (Holm-Sidak Multiple Comparisons versus saline (t = 3.49, P = 0.009). The levels of inactive responses (Fig. 1, open symbols) were uniformly low and were not different from saline with increases in dose per injection for any of the compounds.

Substitution of saline or a range of doses of mitragynine, heroin, or methamphetamine in rats trained to self-administer methamphetamine (0.022 mg/kg per i.v. injection) under an FR 5-response schedule of reinforcement. Ordinates: responses per session; abscissae: unit dose of substituted drug (mg/kg per i.v. injection), log scale. Filled points show active responses (left nose-poke hole); whereas, open points show inactive responses (right nose-poke hole). Each point represents the mean (± SEM) of six subjects. Note that both heroin and methamphetamine, but not mitragynine, maintained rates of response greater than those obtained with saline
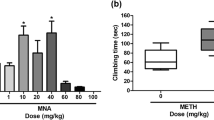
Treatment with mitragynine before sessions at 3.0 mg/kg decreased the maximal levels of active responses maintained by heroin (Fig. 2, left panel). Lower doses (0.1 to 1.0 mg/kg) of mitragynine generally had little effect. The ANOVA indicated significant differences in the mean values for the different doses of heroin (F3,32 = 13.7, P < 0.001) and mitragynine (F4,32 = 16.7, P < 0.001). Mitragynine had no significant effect on inactive responses (data not shown).

Effects of presession treatments with mitragynine on self-administration of heroin under an FR 5-response schedule of reinforcement. a The effects of mitragynine pretreatment on the heroin self-administration dose-effect curve. Ordinates: number of active responses per session; abscissae: heroin unit dose (mg/kg per i.v. injection), log scale. Each point represents the mean (±SEM) of six subjects. Note that data points are displaced horizontally a minimal amount in order to better distinguish error bars. Mitragynine pretreatment decreased self-administration of heroin at a dose of 3.0 mg/kg. b A comparison of the effects of pretreatments with mitragynine on the maximal rates of responses maintained by heroin (0.01 mg/kg/inj) or methamphetamine (0.022 mg/kg/inj). Ordinates: number of active responses (left nose-poke hole) per session as a percentage of that obtained after saline pretreatment; abscissae: mitragynine dose (mg/kg), log scale. The control rates of responding maintained were 2.42 and 1.49 responses per minute during the 1-h session for methamphetamine and heroin, respectively. Note that the dose of mitragynine (3.0 mg/kg) that decreased self-administration of heroin had little effect on responses maintained by methamphetamine injection
In contrast to the effects on heroin self-administration, mitragynine did not significantly affect responding maintained by methamphetamine injection. The ANOVA indicated that the effect of mitragynine dose (F3,15 = 1.69, P = 0.213) was not larger than random sampling variability. The right panel of Fig. 2 shows the lack of effect on the maximal rates of responding maintained by 0.022 mg/kg/injection of methamphetamine (triangles) across the range of doses of mitragynine from those having no effect to those decreasing rates of responding maintained by heroin (circles).
Discussion
In the present study, the self-administration of mitragynine was assessed and compared to that of heroin in rats trained to self-administer methamphetamine. In contrast to heroin, mitragynine did not maintain response rates greater than those obtained with saline injection. In addition, the effects of presession injections of mitragynine were assessed on responding maintained by heroin and methamphetamine. Mitragynine dose-dependently decreased rates of responding maintained by heroin but had little effect on responding maintained by methamphetamine across the same range of mitragynine doses. These results suggest a limited liability for abuse of mitragynine, perhaps due to its activity as a biased agonist (Kruegel et al. 2016; Váradi et al. 2016) and the possible specific reduction of opioid abuse by mitragynine treatment.
Hemby et al. (2018) also investigated mitragynine self-administration in rats. In that study, subjects trained to self-administer morphine did not self-administer mitragynine at doses approximating 0.07 to 0.43 mg/kg/injection (assuming 350-g rats). Those doses were at most 5.7-fold greater on a molar basis than the 50 μg/injection dose of morphine that maintained maximal response rates. The present study found an approximate 200-fold lower affinity of mitragynine than morphine at μ-opioid receptors in rat native tissue. Thus, the present study examined higher doses of mitragynine.
The comparison of mitragynine to heroin in the present study is complicated by the fact that heroin is a prodrug for morphine and 6-acetylmorphine (Inturrisi et al. 1983; Way et al. 1965) and is inactive in binding the μ-opioid receptor. The binding affinity obtained for heroin is likely entirely due to the affinity of the metabolite 6-acetylmorphine which can be detected in the binding assay tubes (Inturrisi et al. 1983). However, likely due to its lipophilicity (Way et al. 1960; Oldendorf et al. 1972), heroin is approximately 10-fold more potent than morphine (on a mg of the salt form basis) in a rat self-administration procedure (e.g., Hiranita et al. 2014). This potency difference renders the minimally effective dose of heroin the equivalent of morphine at 0.03 mg/kg/injection (or 0.04 μmol/kg/injection). The highest presently studied dose of mitragynine (3.0 mg or 7.53 μmol /kg/injection) approximates that necessary to ensure that a sufficient molar dose was studied. In addition, the highest tested dose per injection of mitragynine suppressed responding below levels obtained with saline, indicating that the range of mitragynine doses presently studied included those with biological activity.
There are several reasons to exercise caution in generalizing from the absence of mitragynine self-administration. First, the robust self-administration of several drugs of abuse occurs under some conditions but not others. Possibly the most pronounced example is nicotine for which there are numerous positive and negative outcomes (e.g., Caggiula et al. 2002; Kohut and Bergman 2016). Further, certain behavioral or pharmacological histories may predispose or mitigate robust self-administration (Young and Woods 1981; Hiranita et al. 2014). The use of an opioid rather than methamphetamine for training subjects may have facilitated mitragynine self-administration. However, a previous finding showed that several opioid agonists maintained responding comparably in subjects trained with methamphetamine or heroin (Hiranita et al. 2014). Nonetheless, it remains possible that circumstances may yet be found under which mitragynine is reliably self-administered. In addition, and as described above, there are several studies indicating place conditioning with mitragynine injections. Thus, while the present findings with a self-administration procedure suggest a relatively low abuse liability of mitragynine, further studies would add assurance to that conclusion.
In the present study, pretreatment with mitragynine dose-dependently decreased heroin self-administration, and those decreases were more profound than those for the self-administration of methamphetamine. As methamphetamine has psychomotor stimulant effects, accumulation over the course of the session may have mitigated the response rate decreasing effects of mitragynine that were obtained with heroin self-administration. The total intake of methamphetamine within a session from the present study averaged about 0.054 mg/kg, distributed across a 1-h session. A single bolus dose of 0.1 mg/kg (i.p.) of methamphetamine has reliable direct behavioral effects on rats responding under ratio-type schedules (e.g., Mechner and Latranyi 1963), suggesting that accumulated methamphetamine did not offset the effects of mitragynine on response rates. Nonetheless, a comparison of effects of mitragynine on heroin self-administration with those on food-reinforced responding would add clarification to the selectivity of mitragynine.
Mitragynine at an active dose decreased the maximal self-administration of heroin rather than shifting the dose-effect curve rightward as is typically obtained by treatment with opioid antagonists (Bertalmio and Woods 1989; Harrigan and Downs 1978). The contrast among these effects along with the documented opioid-agonist effects of mitragynine indicates that the mechanism of mitragynine-induced decreases in heroin self-administration is not due to an antagonism of heroin effects. Previous studies of opioid pretreatments have produced similar decreases in maximal self-administration of opioid agonists (e.g., Hiranita et al. 2014; Winger et al. 1992). Noting the similarity of these downward shifts to the effects of food prefeeding on responding maintained by food reinforcement, Hiranita et al. (2014) suggested this outcome could reflect a satiating effect of the drug pretreatment on opioid self-administration (see also Zanettini et al. 2018). Satiation was suggested previously as explanation for the clinical efficacy of methadone in treating opioid abuse (Dole and Nyswander 1965).
Several reports have provided information that human self-administration of mitragynine is maintained by alleviation of opioid withdrawal symptoms (e.g., Grundmann 2017; Smith and Lawson 2017; Swogger and Walsh 2018). For example, Vicknasingam et al. (2010) reported that treatment of opioid withdrawal was self-reported by 62.5% and 46.9%, respectively, of short- and long-term kratom users in Malaysia. In addition, Cheaha et al. (2017) reported that an extract of Mitragyna speciosa suppressed naloxone-precipitated fecal excretions; however, it did not suppress naloxone-precipitated jumping in mice. Those results suggest some direct effects of mitragynine on opioid withdrawal, which has been historically used as evidence of its own potential to produce dependence (Himmelsbach 1941). However, the differences between the effects of mitragynine on the two different withdrawal signs in the Cheaha et al. (2017) study suggest some reservations regarding too extensive a conclusion. Further studies should examine the effects of the various pure alkaloids of the plant, both on precipitated withdrawal and that unfolding after cessation of agonist treatment. Studies over a range of doses, and with a wider variety of withdrawal signs and time frames would add substantially to consideration of kratom physiological dependence liability.
The present study suggests that mitragynine has limited abuse liability from the perspective of self-administration procedures. Those results should prompt other studies to further examine mitragynine self-administration across a broader range of conditions to assess the generality of the findings. Further mitragynine produced a decrease in self-administration of heroin at doses that did not affect self-administration of methamphetamine. These outcomes suggest potential for use of mitragynine in treating opioid abuse though it should be noted that mitragynine has a variety of other behavioral effects that may limit that potential (Hassan et al. 2017). Nonetheless, the current prevalence of opioid abuse and its consequent and multiple impacts on public health, it appears at present that mitragynine is deserving of more extensive exploration for the development of a therapeutic used for treating opioid abuse.
References
Bertalmio AJ, Woods JH (1989) Reinforcing effect of alfentanil is mediated by mu opioid receptors: apparent pA2 analysis. J Pharmacol Exp Ther 251:455–460
Caggiula AR, Donny EC, Chaudhri N, Perkins KA, Evans-Martin FF, Sved AF (2002) Importance of nonpharmacological factors in nicotine self-administration. Physiol Behav 77:683–687
Cheaha D, Reakkamnuan C, Nukitram J, Chittrakarn S, Phukpattaranont P, Keawpradub N, Kumarnsit E (2017) Effects of alkaloid-rich extract from Mitragyna speciosa (Korth) Havil on naloxone-precipitated morphine withdrawal symptoms and local field potential in the nucleus accumbens of mice. J Ethnopharmacol 208:129–137
Cheng Y, Prusoff WH (1973) Relationship between the inhibition constant (KI) and the concentration which causes 50% inhibition of an enzymatic reaction. Biochem Pharmacol 22:403–411
Dole VP, Nyswander M (1965) A medical treatment for diacetylmorphine (heroin) addiction: a clinical trial with methadone hydrochloride. JAMA 193: 646–650
Grundmann O (2017) Patterns of kratom use and health impact in the US — results from an online survey. Drug Alcohol Depend 176:63–70
Harrigan SE, Downs DA (1978) Continuous intravenous naltrexone effects on morphine selfadministration in rhesus monkeys. J Pharmacol Exp Ther 204: 481–486
Harun N, Hassan Z, Navaratnam V, Mansor SM, Shoaib M (2015) Discriminative stimulus properties of mitragynine (kratom) in rats. Psychopharmacol 232:2227–2238
Hassan Z, Bosch OG, Singh D, Narayanan S, Kasinather BV, Seifritz E, Kornhuber J, Quednow BB, Müller CP (2017) Novel psychoactive substances — recent progress on neuropharmacological mechanisms of action for selected drugs. Front Psychiatry 8:152
Hemby SE, Mcintosh S, Cutler SJ, McCurdy CR (2018) Abuse liability of mitragynine and 7-hydroxymitragynine putative primary alkaloids of Mitragyna speciosa (kratom). Soc Neurosci Abstr 794:21
Henningfield JE, Fant RV, Wang DW (2018) The abuse potential of kratom according the 8 factors of the controlled substances act: implications for regulation and research. Psychopharmacol 235:573–589
Himmelsbach CK (1941) The effects of certain chemical changes on the addiction characteristics of drugs of the morphine, codeine series. J Pharmacol Exp Ther 71:41–48
Hiranita T, Kohut SJ, Soto PL, Tanda G, Kopajtic TA, Katz JL (2014) Preclinical efficacy of N-substituted benztropine analogs as antagonists of methamphetamine self-administration in rats. J Pharmacol Exp Ther 348:174–191
Inturrisi CE, Schultz M, Shin S, Umans JG, Angel L, Simon EJ (1983) Evidence from opiate binding studies that heroin acts through its metabolites. Life Sci 33(Suppl 1):773–776
Kai Y, Ma B, Chen L, Tian X, Ru Q, Gan Y, Wang D, Jin G, Li C (2014) l-Stepholidine, a naturally occurring dopamine D1 receptor agonist and D2 receptor antagonist, attenuates heroin self-administration and cue-induced reinstatement in rats. Neuroreport 25:7–11
Kohut SJ, Bergman J (2016) Reinforcing effectiveness of nicotine in nonhuman primates: effects of nicotine dose and history of nicotine self-administration. Psychopharmacol 233:2451–2458
Kong WM, Mohamed Z, Alshawsh MA, Chik Z (2017) Evaluation of pharmacokinetics and blood-brain barrier permeability of mitragynine using in vivo microdialysis technique. J Pharm Biomed Anal 143:43–47
Kruegel AC, Grundmann O (2018) The medicinal chemistry and neuropharmacology of kratom: a preliminary discussion of a promising medicinal plant and analysis of its potential for abuse. Neuropharmacol 134:108–120
Kruegel AC, Gassaway MM, Kapoor A, Váradi A, Majumdar S, Filizola M, Javitch JA, Sames D (2016) Synthetic and receptor signaling explorations of the Mitragyna alkaloids: mitragynine as an atypical molecular framework for opioid receptor modulators. J Am Chem Soc 138:6754–6764
Mechner F, Latranyi M (1963) Behavioral effects of caffeine, methamphetamine, and methylphenidate in the rat. J Exp Anal Behav 6:331–342
Oldendorf WH, Hyman S, Braun L, Oldendorf SZ (1972) Blood-brain barrier: penetration of morphine, codeine, heroin, and methadone after carotid injection. Science 178:984–986
Smith KE, Lawson T (2017) Prevalence and motivations for kratom use in a sample of substance users enrolled in a residential treatment program. Drug Alcohol Depend 180:340–348
Sufka KJ, Loria MJ, Lewellyn K, Zjawiony JK, Ali Z, Abe N, Khan IA (2014) The effect of Salvia divinorum and Mitragyna speciosa extracts, fraction and major constituents on place aversion and place preference in rats. J Ethnopharmacol 151:361–364
Swogger MT, Walsh Z (2018) Kratom use and mental health: a systematic review. Drug Alcohol Depend 183:134–140
Takayama H (2004) Chemistry and pharmacology of analgesic indole alkaloids from the rubiaceous plant, Mitragyna speciosa. Chem Pharm Bull (Tokyo) 52:916–928
US Drug Enforcement Administration (2016) Schedules of controlled substances: placement of mitragynine and 7-Hydroxymitragynine into schedule I. Federal Register. https://www.federalregister.gov/documents/2016/08/31/2016-20803/schedules-of-controlledsubstances-temporary-placement-of-mitragynine-and-7-hydroxymitragynine-into. Accessed 10 April 2017
Váradi A, Marrone GF, Palmer TC, Narayan A, Szabó MR, Le Rouzic V, Grinnell SG, Subrath JJ, Warner E, Kalra S, Hunkele A (2016) Mitragynine/Corynantheidine pseudoindoxyls as opioid analgesics with mu agonism and delta antagonism, which do not recruit β-Arrestin-2. J Med Chem 59:8381–8397
Vicknasingam B, Narayanan S, Beng GT, Mansor SM (2010) The informal use of ketum (Mitragyna speciosa) for opioid withdrawal in the northern states of peninsular Malaysia and implications for drug substitution therapy. Int J Drug Policy 21:283–288
Way EL, Kemp JW, Young JM, Grassetti DR (1960) The pharmacologic effects of heroin in relationship to its rate of biotransformation. J Pharmacol Exp Ther 129:144–154
Way EL, Young JM, Kemp JW (1965) Metabolism of heroin and its pharmacologic implications. Bull Narc 17:25–33
Winger G, Skjoldager P, Woods JH (1992) Effects of buprenorphine and other opioid agonists and antagonists on alfentanil- and cocaine-reinforced responding in rhesus monkeys. J Pharmacol Exp Ther 261:311–317
Young AM, Woods JH (1981) Maintenance of behavior by ketamine and related compounds in rhesus monkeys with different self-administration histories. J Pharmacol Exp Ther 218:720–727
Yusoff NHM, Suhaimi FW, Vadivelu RK, Hassan Z, Rümler A, Rotter A, Amato D, Dringenberg HC, Mansor SM, Navaratnam V, Müller CP (2016) Abuse potential and adverse cognitive effects of mitragynine (kratom). Addict Biol 21:98–110
Yusoff NHM, Mansor SM, Müller CP, Hassan Z (2017) Opioid receptors mediate the acquisition, but not the expression of mitragynine-induced conditioned place preference in rats. Behav Brain Res 332:1–6
Yusoff NHM, Mansor SM, Müller CP, Hassan Z (2018) Baclofen blocks the acquisition and expression of mitragynine-induced conditioned place preference in rats. Behav Brain Res 345:65–71
Zanettini C, Wilkinson DS, Katz JL (2018) Behavioral economic analysis of the effects of N-substituted benztropine analogs on cocaine self-administration in rats. Psychopharmacol 235: 47–58
Zhang F (2006) SuperState: a computer program for the control of operant behavioral experimentation. J Neurosci Methods 155:194–201
Acknowledgments
We thank Drs. Christopher R. McCurdy for the initial advice on mitragynine and James H. Woods for the advice on the writing of this report.
Funding
This project was funded by the National Natural Science Foundation of China (81302762) and the National Institute on Drug Abuse, Intramural Research Program. These studies were initiated at NIDA when Kai Yue was funded by a scholarship from the China Scholarship Council (CSC), a non-profit institution affiliated with the Ministry of Education of the P.R. China, Level 13, Building A3, No. 9 Chegongzhuang Avenue, Beijing 100044, P. R. China.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Yue, K., Kopajtic, T.A. & Katz, J.L. Abuse liability of mitragynine assessed with a self-administration procedure in rats. Psychopharmacology 235, 2823–2829 (2018). https://doi.org/10.1007/s00213-018-4974-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-018-4974-9