
Abstract
Summary
Osteoporosis, the most common metabolic bone disease, leads to increased susceptibility to fractures. In 2020, about 150,000 osteoporotic fractures occurred in Iran. Osteoporosis and related fractures cost the community US$ 393 million.
Introduction
The present study aimed at estimating the economic burden of osteoporosis in Iran in 2020.
Methods
We estimated the annual economic burden of osteoporosis in the above 50 years old population using a prevalence-based approach and from a societal perspective. The incidence of osteoporosis and related fractures were estimated based on meta-analysis reports in Iran and international comparisons. The direct medical and non-medical costs as well as the monetary value of quality-adjusted life-years (QALYs) lost because of fractures were estimated. Cost data were extracted from patient records, medical services prices, and previous literature.
Results
A total of 154,530 osteoporotic fractures were estimated in Iran in 2020. The shares of the hip, vertebral, forearm, and other fractures were 14%, 15%, 17%, and 54%, respectively. There were also 3554 deaths from osteoporotic fractures. The economic burden of osteoporosis in Iran was estimated at US$ 393.24 million (US$ 2165 million purchasing power parity 2020). Direct medical and non-medical cost (47.44%), QALY loss (29.65%), and long-term care for prior hip fracture costs (9.4%) were the main component of the economic burden of osteoporosis.
Conclusion
The economic burdens of osteoporosis are significant in Iran. Interventions to prevent osteoporosis and especially associated fractures, such as screening and prophylaxis, can reduce the cost of the disease and improve patients’ quality of life. Further studies are needed to identify cost-effective and feasible interventions in Iran.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is the most common metabolic bone disease, characterized by systemic abnormalities in bone mass and microstructures, leading to increased susceptibility to fractures [1,2,3]. According to the World Health Organization definition, “osteoporosis is defined as a value for bone mineral density (BMD) 2.5 standard deviations (SD) or more below the young female adult mean (T-score less than or equal to − 2.5 SD)” [4]. Osteoporosis, a major health problem, is associated with age-related fractures, especially in the hip, vertebrae, distal forearm, and humerus [5]. Fragility fractures are serious threats to patient’s health, quality of life, and health care sustainability [6].
In recent decades, the prevalence of osteoporosis increased dramatically worldwide [1, 7], and it became a global epidemic as a socio-economic threat associated with population aging [2]. According to the International Osteoporosis Foundation report, one-third of females and one-fifth of males aged above 50 experience osteoporotic fractures during their lives [8]. Based on the results of a systematic review and meta-analysis, the prevalence of osteoporosis in the above 50 years old population of Iran was estimated at 12% in males and 19% in females [9].
Osteoporotic fractures are associated with increased morbidity and mortality [5, 6, 10,11,12]. These fractures also cause heavy financial burdens for health care [1, 6, 12, 13]. The economic burden of osteoporotic fractures was estimated at € 37 billion in 2010, according to a study in 27 EU countries; and a 25% increase is projected by 2025 [4]. According to a study by Marcellusi et al., in Italy, osteoporosis imposes an annual economic burden of € 2.2 billion on average [14].
Since population aging is one of the most important factors affecting the osteoporosis incidence [1, 2] and Iran is moving toward population aging [15], being aware of the disease costs and economic dimensions of the disease is of great importance for policy-making and planning for its prevention and management; however, no comprehensive study was performed thus far on the economic aspects of osteoporosis in Iran. Therefore, the present study aimed at estimating the economic burden of osteoporosis in Iran in 2020 .
Methods
Study design
The present cross-sectional study estimated the economic burden of osteoporosis and its related fractures in Iran in 2020 from the perspective of society. Given that the risk of osteoporosis and its associated fractures is very low in individuals aged below 50 years and the related data are limited, only the individuals aged above 50 years were enrolled in the study. The costs of osteoporosis management and resulting fractures were estimated by the fracture type, including the hip, vertebrae, forearm, and other parts (including fractures of the femur, pelvis, humerus, rib, clavicle, scapula, and sternum), in the first year of the fracture. Since the economic consequences of fractures and their impact on patients’ quality of life (QoL) last more than a year, to estimate the economic burden of osteoporosis in the same duration, the fractures resulting from osteoporosis in previous years in a living individual should also be considered. Since such outcomes are greater in hip and vertebral fractures, the costs were calculated only for these two sites.
Estimation of the incidence and prevalence of osteoporosis, osteoporotic fractures, and associated deaths
In the present study, fractures associated with osteoporosis were categorized into four groups of the hip, vertebrae, forearm, and other parts (including fractures of the femur, pelvis, humerus, rib, clavicle, scapula, and sternum). Equation 1 was used to estimate the number of osteoporotic fractures in Iran.
where TFI is the total number of osteoporotic fractures, f is the type of fracture (including the hip, vertebrae, and forearm), g is the gender, i is the age, R is the incidence of fractures in the population, and N is the population above 50 years in Iran.
The age- and gender-specific incidences of hip fractures were estimated through a systematic review and meta-analysis in Iran [16]. Due to the lack of a study on the incidence of the forearm, vertebral, and other fractures in Iran, the approach used in the study by Hernlund et al. was utilized [4]. For this purpose, the incidences of the vertebral, forearm, and other fractures in Iran were estimated using the incidence of hip fractures to other fractures ratio in Sweden [17]. Data on the Iranian population by age and gender in 2020 were extracted from the Statistical Center of Iran website [18]. Data on the ratio of incidence of hip fractures to other fractures and other input parameters that we used to estimate the number of fractures and the economic burden of osteoporosis in Iran are shown in Supplementary Table S1.
Osteoporotic fractures increase the risk of mortality, but the size of this increase varies across fractures and the time elapsed since its occurrence [19, 20]. In the present study, the number of deaths from osteoporotic fractures in the first year of incidence was estimated using Eq. 2.
where TFM represents the total number of deaths from osteoporotic fractures, f is the type of fracture, g is the gender, i is the age, R is the incidence of fractures in the population, N is the total population, pM is the incidence of death in the general population, rrM is the risk of death from osteoporotic fractures in the first year of incidence, and A is the percent of mortality which are directly associated with osteoporotic fractures.
The osteoporosis-associated risk of death (rrM) in the first year of hip and vertebral fractures by type of fracture was extracted from previous studies [21] and accordingly, it was assumed that the risk of death does not increase after forearm fractures. In addition, the risk of death from other osteoporotic fractures was considered the same for all age groups as 1.22 [4]. Also, since a significant share of all deaths associated with osteoporotic fractures is attributed to other diseases [4], in the present research, like previous studies, it was assumed that 30% of deaths occurring after hip and vertebral fractures and 12% of deaths after other osteoporotic fractures are directly associated with these fractures [4, 22, 23].
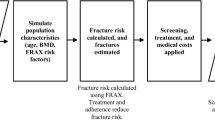
A Markov model was used to estimate the number of previous hip and vertebral fractures. Details of the Markov model are reported in previous studies [24, 25]. The structure of the model is shown in Supplementary Fig. S1. The model has four health states: healthy, hip fracture, vertebral fracture, and dead. The time horizon of the model was lifetime, and the length of each cycle was 1 year. With this model, we simulated the prevalence of prior hip and vertebral fractures using incidence data in the population over 50 years of age. The parameters of the Markov model included the incidence of age- and gender-specific fractures, age- and gender-specific deaths from other reasons, and risk of death from fractures. Age- and gender-specific deaths from other reasons were extracted from the Iran life table [26] and the risk of death associated with fractures from previous studies [4, 27]. We multiplied the sex- and age-specific prevalence of prior hip and prior clinical vertebral fractures by the sex- and age-specific population of Iran to estimate the number of prior fractures present in 2020.
Calculation of the cost of prevention and management of osteoporosis
For this purpose, three components of the cost of prevention and medication, the cost of visiting a doctor, and the cost of measuring bone density were considered.
Medication costs of prevention and management of osteoporosis were extracted from the Iranian Annual Pharma Statistics 2020. For this purpose, the drugs prescribed for osteoporosis management were identified, and their sales prices were extracted from the available statistics. Regarding medicines commonly prescribed for osteoporosis and other diseases, such as cancer, the share of osteoporosis in their sales amount was determined through consultation with experts. According to the osteoporosis guideline in Iran, to calculate the cost of physician visits, it was assumed that each patient is visited by a specialist once a year on average, and according to the distribution of ambulatory services in Iran, it was assumed that 70% of such patients refer to private offices. The average visit cost was determined according to the 2020 physician visit tariff for private and public sectors.
For calculating the cost of bone density testing with DXA scan, the number of bone density testing centers by public and private sectors was estimated according to the total number of DXA machines available in Iran, and the number of active centers by public and private sectors was multiplied by the cost of each service.
Calculation of direct (medical and non-medical) costs of osteoporotic fractures
For calculating the direct costs of osteoporotic fractures, the Borgström et al. approach was utilized in the present study [28]. For this purpose, according to Eq. 3, the total number of fractures by type was multiplied by the average cost for each patient.
Total annual acute fracture-related costs
where f indicates the fracture type (i.e., hip, vertebrae, and forearm, etc.), g is the gender, i is the age, C is the average cost per patient in the first year of fracture, FI is the number of fractures, FM is the number of death cases in the first year of fracture, and X is the average number of days from the time of fracture to death in subjects who died in the first year of a fracture.
The average direct medical and non-medical costs were estimated by fracture type per patient in the first year of fracture in a survey; the details are provided in another article [29]. In brief, hospitalization expenses were calculated by evaluating the medical files of 300 patients admitted for osteoporotic fractures in the pelvis, vertebrae, and forearm. In addition, through interviews with patients, using the patient cost questionnaire, ambulatory and direct non-medical expenses, such as informal care, travel, and time, were calculated in a year after fracture occurrence.
Since all patients with osteoporotic fractures do not need a hospital stay, hospitalization costs were calculated only for those admitted. The percentage of patients admitted for hip, vertebral, and forearm fractures was estimated at 100, 35, and 25, respectively [28, 30]. Like the study by Hernlund et al. [4], due to difficulty in finding a sufficient sample size consisting of patients with other fractures associated with osteoporosis, it was assumed that the ratio of the cost of these fractures to the cost of hip fractures is identical across countries, and the hip fracture cost to other fractures ratio in Sweden was utilized [17]. Like the study by Borgström et al., costs were adjusted for patients who died in the first year of the fracture, and it was assumed that the average time of death was 140 days after the fracture occurrence [28]; hence, 35.38% of ambulatory care expenses were considered for such cases.
Calculation of long-term care expenses for patients with hip fractures
Since patients with hip fractures become significantly disabled and require long-term care, long-term expenses were calculated only for hip fractures. For this purpose, the number of live patients with hip fractures in need of long-term care in 2020 was estimated, and the number was multiplied by the average cost per patient. According to the results of a meta-analysis, 10–25% of patients with hip fracture require long-term care [31]; it was considered 10% in the present study. The average care cost per patient was also considered equal to the official minimum wage in 2020 (US$ 2,639 a year).
Calculation of the number and US dollar value of QALYs lost due to osteoporotic fractures in Iran
In the present study, the QALY was used to measure intangible costs (reduced QoL). As a cost, the QALYs lost due to osteoporotic fractures were measured for the current and previous cases based on the approach used by Borgström et al. [28]. In brief, the number of QALYs lost due to osteoporosis fractures was calculated by the fracture type, and the result was multiplied by the monetary value of each QALY (Eq. 4).
Total annual value of QALYs lost due to fractures=
where WPT is willingness to pay, Q1 and Q2 are the reduced QoL due to fractures in the first and following years, respectively, f is the type of fracture, g is the gender, i is the age, FI is the number of fractures, FM is the number of deaths in the first year of fracture, PF is the number of previous fractures (in previous years), X is the average number of days from the time of fracture to death in those died in the first year of fracture, and popQ is the QoL of the general population.
The size of reduction in QoL due to osteoporotic fractures by the fracture type and time elapsed since fracture occurrence (Q1 and Q2) were extracted from previous studies. In these studies, the impact of osteoporotic fractures on QoL was measured based on the EQ-5D questionnaire. It is a general preference-based instrument used to measure QoL in five dimensions, namely mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, and can be utilized to measure QALY [32].
Based on previous studies, the QoL in individuals with hip, vertebral, forearm, and other fractures corresponded to 0.7, 0.59, 0.96, and 0.85 of the age-specific QoL of healthy people, respectively, in the first year of fracture occurrence [33]. Hip and vertebral fractures also reduce the quality of life to 0.84 and 0.9 QoL of healthy people in the next years, respectively [33, 34]. Age- and gender-specific health-related quality of life for Iranian healthy people was extracted from the study by Emrani et al. [35]. The monetary value of each QALY was considered equal to per capita GDP, US$ 2422.5 in 2020 [36].
Calculation of the economic burden of osteoporosis in Iran
Finally, after calculating the different types of expenditure, including the direct cost of fractures, the cost of long-term care of patients with hip fractures, the cost of reducing QoL, and the costs of prevention and management of osteoporosis, the economic burden of osteoporosis in Iran in 2020 was calculated by adding all costs. All expenditures were expressed as US dollars using the official market exchange rate (US$ 1 = IR Rial 172,431) and purchasing power parity (PPP) exchange rate (US$ 1 = IR Rial 31,317) for 2020 [37]. Microsoft Excel, STATA, and TreeAge software were used to analyze the data.
Sensitivity analysis
The incidence rate of hip fracture is one of the most important parameters in our study. Because a large proportion of the economic burden of osteoporosis is attributable to hip fractures, we also estimated the incidence of other fractures based on the incidence of hip fractures. Thus, a change in the incidence of hip fractures implies a change in the incidence of other fractures. We performed a deterministic sensitivity analysis embedding the lower and upper 95% confidence intervals of the incidence rate of hip fracture in Iran to assess the impact of uncertainty in this parameter on the study results.
Results
According to Iran’s population in 2020, the number of osteoporosis cases was estimated to be 993,960 in males, 1,621,840 in females, and 2,615,800 in total. The number of incident and prior osteoporotic fracture cases by age and gender in Iran in 2020 is presented in Table 1. The total number of incident fractures was estimated at 154,530, of which 52.9% were males. The total number of the hip, vertebral, forearm, and other fractures was 21,136, 23,553, 26,183, and 83,658, respectively. The total number of prior hip and vertebral fractures was estimated at 337,635 in Iran in 2020, comprising 140,148 men and women with a prior hip fracture and 197,487 with a prior clinical vertebral fracture.
The results of the sensitivity analysis are presented in the supplementary file (Supplementary Tables S2 through S13). According to these results, the total number of osteoporotic fractures occurring was estimated to range from 114,652 to 209,734. The lower and upper limits of the hip, vertebral, forearm, and other fractures were estimated to be 15,821 to 28,432; 17,451 to 32,007; 20,217 to 34,106; and 61,162 to 115,188, respectively (Supplementary Tables S2 and S8).
According to Table 2, there were 3554 deaths associated with osteoporotic fractures, with an incidence of 21.13 per 100,000 people above 50 years. The numbers of deaths associated with hip, vertebral, and other fractures were 1334, 1157, and 1064, respectively. Based on the results of the sensitivity analysis, the lower and upper bounds of deaths related to osteoporotic fractures were 2656 and 4790, respectively (see Supplementary Tables S3 and S9).
Table 3 shows direct costs by hospitalization and ambulatory care services, including non-medical direct costs. Direct costs of other fractures (59.8%) accounted for the largest share, followed by hip (25.79%), vertebral (9.14%), and forearm (5.26%) fractures. Also, hip, vertebral, and other fractures had the highest number of deaths in the first year of occurrence. The share of the hip, vertebral, forearm and other fractures in the total direct costs was 25.79%, 9.14%, 5.26%, and 59.80%, respectively (see Table 3).
According to Table 4, with age increase, the number of people with previous hip fractures, the number of morbidities resulted from hip fractures, and, consequently, the long-term care costs increase so that the age group above 80 years had the highest share in expenses in both males and females. The total cost of long-term care for disabilities associated with hip fractures in 2020 was US$ 17,865,254, US$ 19,116,121, and US$ 36,981,375 for males, females, and in total, respectively.
According to Table 5, the total number of QALYs lost due to osteoporosis in Iran in 2020 was estimated at 48,129, of which approximately 56% were males. Of the total QALYs lost, 42.52% were due to fractures associated with osteoporosis and 55.28% to previous hip and vertebral fractures, and 2.20% of premature deaths were due to osteoporotic fractures.
Based on the results of the sensitivity analysis, the lower and upper limits of QALYs lost due to osteoporosis in Iran in 2020 were 35,652 and 65,325, respectively (see Supplementary Tables S6 and S12).
In total, osteoporosis had an economic burden of US$ 393.24 million (US$-PPP 2165 million) in Iran in 2020. Among these, direct medical and non-medical (47.44%), QALY loss (29.65%), and long-term care costs for people with previous hip fractures (9.40%) were the main determinants of the economic burden of osteoporotic fractures (see Table 6 and Fig. 1).

Economic burden of osteoporosis in Iran, 2020
According to the results of the sensitivity analysis, the total economic burden of osteoporosis in Iran in 2020 was estimated to be between US$ 305.11 million (US$-PPP 1680 million) and US$ 515.04 million (US$-PPP 2836 million) (Supplementary Tables S7 and S13).
Discussion
The present study was the first one to calculate the economic burden of osteoporosis in Iran. In the study, expenditures were calculated based on a prevalence-based approach from the community perspective in 2020. According to the findings, osteoporosis had an economic burden of US$ 393.24 million (US$-PPP 2165 million) in 2020 in Iran.
Osteoporotic fractures impose a heavy economic burden on health systems and society worldwide [4, 13, 38, 39]. Osteoporotic fractures imposed an economic burden of € 27 billion in 27 EU countries in 2010, projected to increase by 25% by 2025 [4]. The economic burden of osteoporotic fractures in Turkey in 2019 was estimated at US$ 455 million [40], and that of Austria in 2008 was € 685.2 million [38].
Osteoporosis imposes an economic burden of € 2.2 billion on average annually in Italy, € 8091 per patient on average [14]. The total cost of care for osteoporosis increased from US$ 3976 million to 5126 million in South Korea from 2008 to 2011, representing an annual increase of 9.2% [41]. According to a study by Svedbom et al., the economic burden of osteoporotic fractures in Switzerland was estimated at CHF 2.05 billion, projected to increase by 29% by 2025 compared to 2010 [42]. Also, the burden of hospitalization and hospital costs for osteoporotic fractures were higher than those of heart attack, stroke, and breast cancer among females aged 55 and above in the USA in 2000 and 2011; hence, osteoporotic fractures accounted for 40% of hospitalization and annual costs among mentioned diseases [43].
In the present study, direct medical and non-medical (47.44%), QALYs lost (29.65%), long-term care for people with previous hip fractures (9.40%), bone mineral density measurement (5.36%), prophylaxis (6.61%), and physician visit (1.54%) costs were the determinants of the economic burden of osteoporotic fractures in Iran. The main determinants of the economic burden of osteoporotic fractures varied across studies. Approximately 80% of the economic burden of osteoporosis in Italy was associated with hospitalization, 16% to medication, 3% to outpatient visits, and 0.6% to social security costs [14]. In the EU, 66% of the economic burden of fractures accounted for new fractures, 29% for long-term care of patients with fractures, and 5% for prophylaxis. Fractures also resulted in the loss of 1.18 million QALY units [4].
The largest share of osteoporotic fracture costs in Austria accounted for the opportunity cost of care provided by family members (30.2%) and inpatient care (26.6%) [38]. In Switzerland, 76% of the economic burden of osteoporotic fractures accounted for new fractures, 21% for long-term care of patients with fractures, and 3% for prophylaxis. Also, 24,000 QALYs are lost due to osteoporotic fractures [42]. In South Korea, of the total health care cost for osteoporosis, the share of hospitalization was 40%, ambulatory care 31%, and drug prescription 29% [41]. In Turkey, the highest economic burden of osteoporotic fractures accounted for hospitalization (47%), surgical (26%), and patient productivity (23%) costs [40].
Clinical outcomes of hip fractures are more than other fractures [1]. Hip fracture with a mortality rate of 20–24% in the first year of the fracture causes the most morbidity [39]. Also, since hip fracture requires hospitalization, it is the most costly outcome of osteoporosis. About 50% of the deaths associated with osteoporotic fractures in 2010 in Europe accounted for hip fractures [4]. The direct costs of hip fractures in Iran in 2010 were estimated at US$ 28 million, projected to increase to US$ 250 million by 2050 [44]. According to a study in Spain on a population above 65 years with hip fractures, the average direct cost was € 9690 for females and € 9019 for males [45]. In the present study, in addition to 25.79% of direct costs, hip fractures accounted for approximately 9.4% of the total economic burden directly due to the cost of long-term care of patients with hip fractures.
The costs and consequences of fractures are drastically high for public health [1]. The massive global burden of osteoporosis suggests that fracture risk assessment should be considered by health policy-makers [5]. According to the IOF recommendation, to support the effective management of osteoporotic fractures, health systems should prioritize prevention, provision of standard care, and financing [39]. Likewise, prioritizing bone health and supporting programs, such as fracture liaison services, are necessary to reduce this burden [43].
Fracture liaison service (FLS) is an accepted approach to reduce the incidence of osteoporotic fractures [46]. FLS care, in addition to cost-efficiency, significantly reduces the risk of subsequent fracture and post fracture mortality, especially in patients with hip fractures [12]. Although cost-efficacy studies report that the implementation of FLS is beneficial to patients and health care systems [47], further research is still needed to evaluate the clinical efficacy and cost-effectiveness of strategies for finding osteoporotic cases and assessment of risk worldwide [5].
According to the available evidence, population aging is one of the most important factors affecting the incidence of osteoporosis, so with an increase in the elderly population, the medical and socio-economic consequences of osteoporosis drastically increase [1, 2]. Iran is also moving toward population aging due to reduced fertility, reduced mortality, and increased life expectancy [15]; therefore, osteoporosis and its outcomes would be a critical public health problem in Iran shortly. It should seriously be considered by policy-makers who plan for the disease prevention and control programs [9].
In this study, we attempted for the first time to provide a comprehensive estimate of the economic impact of osteoporosis in Iran, a middle-income country. However, to do so, we had to make several assumptions due to data limitations. To estimate the incidence of osteoporotic fractures (excluding hip), the ratio of the incidence of osteoporotic fractures (including vertebral, forearm, and “other” fractures) to hip fractures in Iran was assumed to be similar to that in Sweden for each age and sex. In addition, because the incidence of the femur, pelvis, humerus, rib, clavicle, scapula, and sternum fractures was only available in complete form for Sweden, it was not possible to estimate the incidence of these fractures by fracture type for Iran. However, these fractures accounted for more than 50% of all estimated fractures and were responsible for a significant proportion of the economic burden of osteoporosis.
In some cases, vertebral fractures may be asymptomatic or not be correctly diagnosed. Although asymptomatic vertebral fractures can reduce QoL and impose costs, the study did not consider asymptomatic cases, so the estimates of vertebral fractures may be undercounted.
Conclusion
According to the results of the study, osteoporosis is an important health problem in Iran, and its economic burden is significant. Interventions to prevent osteoporosis and especially associated fractures, such as screening and prophylaxis, can reduce the cost of the disease and improve patients’ quality of life. Further studies are needed to identify cost-effective and feasible interventions in Iran.
References
Tootee A, Larijani B (2019) World osteoporosis day: celebrating two decades of progress in preventing osteoporotic fractures in Iran. J Diabetes Metab Disord 18(2):725–727
Rachner TD, Khosla S, Hofbauer LC (2011) Osteoporosis: now and the future. The Lancet 377(9773):1276–1287
International osteoporosis foundation (IOF). What is osteoporosis. https://www.osteoporosis.foundation. Accessed 2021
Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J et al (2013) Osteoporosis in the European Union: medical management, epidemiology and economic burden. Arch Osteoporos 8(1):1–115
Curtis EM, Moon RJ, Harvey NC, Cooper C (2017) Reprint of: The impact of fragility fracture and approaches to osteoporosis risk assessment worldwide. Int J Orthop Trauma Nurs 26:7–17
Pennestrì F, Corbetta S, Favero V, Banfi G (2019) Fragility fracture prevention—implementing a fracture liaison service in a high volume orthopedic hospital. Int J Environ Res Public Health 16(24):4902
Salari N, Ghasemi H, Mohammadi L, Rabieenia E, Shohaimi S, Mohammadi M (2021) The global prevalence of osteoporosis in the world: a comprehensive systematic review and meta-analysis. J Orthop Surg Res 16(1):1–20
International osteoporosis foundation (IOF). About osteoporosis. https://www.osteoporosis.foundation/patients/about-osteoporosis. Accessed July 2019
Irani AD, Poorolajal J, Khalilian A, Esmailnasab N, Cheraghi Z (2013) Prevalence of osteoporosis in Iran: a meta-analysis. J Res Med Sci 18(9):759–766
Wong RM, Law S, Lee K, Chow SK, Cheung W (2019) Secondary prevention of fragility fractures: instrumental role of a fracture liaison service to tackle the risk of imminent fracture. Hong Kong Med J 25(3):235–242
Clynes MA, Harvey NC, Curtis EM, Fuggle NR, Dennison EM, Cooper C. The epidemiology of osteoporosis. British medical bulletin. 2020
Briot K (2017) Fracture liaison services. Curr Opin Rheumatol 29(4):416–421
Tarride J-É, Adachi J, Brown J, Schemitsch E, Slatkovska L, Burke N. Incremental costs of fragility fractures: a population-based matched-cohort study from Ontario, Canada. Osteoporosis International. 2021:1–9
Marcellusi A, Rotundo MA, Nardone C, Sciattella P, Gazzillo S, Rossini M et al (2020) Osteoporosis: economic burden of disease in Italy. Clin Drug Investig 1–10
Mosadeghrad AM, Mousavi A (2021) The futurology of aging population in Iran: Letter to the Editor. Tehran Univ Med J 68(3):66–71
Tanha K, Fahimfar N, Nematollahi S, Sajjadi-Jazi SM, Gharibzadeh S, Sanjari M et al (2021) Annual incidence of osteoporotic hip fractures in Iran: a systematic review and meta-analysis. BMC Geriatr 21(1):1–8
Kanis J, Johnell O, Oden A, Sernbo I, Redlund-Johnell I, Dawson A et al (2000) Long-term risk of osteoporotic fracture in Malmö. Osteoporos Int 11(8):669–674
Iranian Statistics Center. Statistics-by-Topic/Population: definitions, concepts and statistical survey. https://www.amar.org.ir/english/Statistics-by-Topic/Population. Accessed 2022
Center JR, Nguyen TV, Schneider D, Sambrook PN, Eisman JA (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. The Lancet 353(9156):878–882
Johnell O, Kanis J, Odén A, Sernbo I, Redlund-Johnell I, Petterson C et al (2004) Fracture risk following an osteoporotic fracture. Osteoporos Int 15(3):175–179
Johnell O, Kanis J, Oden A, Sernbo I, Redlund-Johnell I, Petterson C et al (2004) Mortality after osteoporotic fractures. Osteoporos Int 15(1):38–42
Kanis JA, Oden A, Johnell O, De Laet C, Jonsson B (2004) Excess mortality after hospitalisation for vertebral fracture. Osteoporos Int 15(2):108–112
Gauthier A, Kanis JA, Jiang Y, Martin M, Compston JE, Borgström F, et al (2011) Gauthier, A., et al., Epidemiological burden of postmenopausal osteoporosis in the UK from 2010 to 2021: estimations from a disease model. Arch Osteoporos 6(1):179–88
Tosteson A, Jönsson B, Grima D, O’Brien B, Black D, Adachi J (2001) Challenges for model-based economic evaluations of postmenopausal osteoporosis interventions. Osteoporos Int 12(10):849–857
Zethraeus N, Borgström F, Ström O, Kanis J, Jönsson B (2007) Cost-effectiveness of the treatment and prevention of osteoporosis—a review of the literature and a reference model. Osteoporos Int 18(1):9–23
World Health Organization, Global Health Observatory data repository, Life tables by country. http://apps.who.int/gho/data/node.main.LIFECOUNTRY?lang=en. Accessed 2017
Jönsson B, Ström O, Eisman JA, Papaioannou A, Siris ES, Tosteson A et al (2011) Cost-effectiveness of denosumab for the treatment of postmenopausal osteoporosis. Osteoporos Int 22(3):967–982
Borgström F, Sobocki P, Ström O, Jönsson B (2007) The societal burden of osteoporosis in Sweden. Bone 40(6):1602–1609
Rajabi M, Ostovar A, Sari AA, Sajjadi-Jazi SM, Fahimfar N, Larijani B et al (2021) Direct costs of common osteoporotic fractures (hip, vertebral and forearm) in Iran. BMC Musculoskelet Disord 22(1):1–7
Stevenson M, Davis S, Kanis J (2006) The hospitalisation costs and out-patient costs of fragility fractures. Women’s Health Med 3(4):149–151
Dyer SM, Crotty M, Fairhall N, Magaziner J, Beaupre LA, Cameron ID, et al (2016) A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr 16(1):1–18
Brooks R, Group E (1996) EuroQol: the current state of play. Health Policy 37(1):53–72
Peasgood T, Herrmann K, Kanis J, Brazier J (2009) An updated systematic review of Health State Utility Values for osteoporosis related conditions. Osteoporos Int 20(6):853–868
Borgström F, Johnell O, Kanis JA, Oden A, Sykes D, Jönsson B (2004) Cost effectiveness of raloxifene in the treatment of osteoporosis in Sweden. Pharmacoeconomics 22(17):1153–1165
Emrani Z, Sari AA, Zeraati H, Olyaeemanesh A, Daroudi R (2020) Health-related quality of life measured using the EQ-5D–5 L: population norms for the capital of Iran. Health Qual Life Outcomes 18(1):1–8
World Bank Open Data. https://data.worldbank.org/country/iran-islamic-rep. Accessed 2022
World Bank Open Data. https://data.worldbank.org/indicator/PA.NUS.ATLS?locations=IR. Accessed 2022
Dimai HP, Redlich K, Peretz M, Borgström F, Siebert U, Mahlich J (2012) Economic burden of osteoporotic fractures in Austria. Heal Econ Rev 2(1):1–10
International osteoporosis foundation (IOF). Burden of osteoporosis. https://www.osteoporosis.foundation/policy-makers/burden-osteoporosis. Accessed 2020
Aziziyeh R, Perlaza JG, Saleem N, Kirazlı Y, Akalın E, McTavish RK et al (2020) The burden of osteoporosis in Turkey: a scorecard and economic model. Arch Osteoporos 15(1):1–9
Ha Y-C, Kim H-Y, Jang S, Lee Y-K, Kim T-Y (2017) Economic burden of osteoporosis in South Korea: claim data of the national health insurance service from 2008 to 2011. Calcif Tissue Int 101(6):623–630
Svedbom A, Ivergård M, Hernlund E, Rizzoli R, Kanis JA (2014) Epidemiology and economic burden of osteoporosis in Switzerland. Arch Osteoporos 9(1):1–8
Singer A, Exuzides A, Spangler L, O’Malley C, Colby C, Johnston K et al (2015) Burden of illness for osteoporotic fractures compared with other serious diseases among postmenopausal women in the United States. Mayo Clin Proc 90(1):53–62
Ahmadi-Abhari S, Moayyeri A, Abolhassani F (2007) Burden of hip fracture in Iran. Calcif Tissue Int 80(3):147–153
Caeiro JR, Bartra A, Mesa-Ramos M, Etxebarría Í, Montejo J, Carpintero P et al (2017) Burden of first osteoporotic hip fracture in Spain: a prospective, 12-month, observational study. Calcif Tissue Int 100(1):29–39
Major G, Ling R, Searles A, Niddrie F, Kelly A, Holliday E et al (2019) The costs of confronting osteoporosis: cost study of an Australian fracture liaison service. JBMR plus 3(1):56–63
Hoang-Kim A, Kanengisser D (2020) Developing registries and effective care models for the management of hip fractures: aligning political, organizational drivers with clinical outcomes. Curr Osteoporos Rep 18(3):180–188
Funding
This study was funded by the Tehran University of Medical Sciences (grant number 9611119004).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the Deputy of Research and Technology of the Tehran University of Medical Sciences (IR.TUMS.EMRI.REC.1396.0016). All authors confirm and declare that this study was conducted in compliance with the Declaration of Helsinki. The participants were assured that their information would remain confidential. Informed consent was obtained from all individual participants included in the study.
Conflicts of interest
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 101 kb)
Rights and permissions
About this article

Cite this article
Ostovar, A., Mousavi, A., Sajjadi-Jazi, S.M. et al. The economic burden of osteoporosis in Iran in 2020. Osteoporos Int 33, 2337–2346 (2022). https://doi.org/10.1007/s00198-022-06484-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-022-06484-x