
Abstract
Summary
This meta-analysis aimed to investigate the associations between osteocalcin (Ocn) and fasting plasma glucose (FPG) and glycated hemoglobin A1c (HbA1c). It was revealed that both total Ocn and undercarboxylated Ocn (unOcn) were negatively related with FPG and HbA1c, and the association of unOcn with FPG was more pronounced in men.
Introduction
The aim of this study was to investigate the strength of associations between Ocn and FPG and HbA1c using a meta-analysis approach.
Methods
A search was carried out using the databases of PubMed, ISI Web of Science, and the Cochrane library from 2007 to 2014 to identify related studies. A pooled effect size with 95 % confidence intervals (CI) was derived.
Results
The meta-analysis included 39 studies involving 23,381 participants. The overall correlation was −0.16 (95 % CI, −0.19 to −0.14) between total Ocn (tOcn) and FPG and −0.15 (95 % CI, −0.20 to −0.11) between undercarboxylated Ocn (unOcn) and FPG. In the analysis of the association between Ocn and HbA1c, the pooled correlation was −0.16 (95 % CI, −0.18 to −0.14) for tOcn and −0.16 (95 % CI, −0.23 to −0.08) for unOcn. The magnitude of the correlation between unOcn and FPG is significantly higher in men than in women (r = −0.18, 95 % CI, −0.21 to −0.14; r = −0.09, 95 % CI, −0. 13 to −0.05, respectively; P for interaction < 0.05). Similar trend was also found between unOcn and HbA1c but without significance (for men, r = −0.19, 95 % CI, −0.24 to −0.14; for women, r = −0.09, 95 % CI, −0.22 to 0.04, respectively; P for interaction > 0.05). No indication of significant publication bias was found in any method.
Conclusions
This meta-analysis demonstrated that both unOcn and tOcn were similarly and negatively correlated with FPG and HbA1c in humans. The negative correlations between unOcn and glucose metabolism appear to be more pronounced in men than in women.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In recent years, the skeleton was believed to play a certain role in regulating whole body glucose homeostasis through endocrine pathways [1]. Accumulating evidence from mice studies has demonstrated that osteocalcin (Ocn), a bone protein synthesized and secreted by osteoblasts, especially in its undercarboxylated form, is generally acknowledged to fulfill this skeleton endocrine function [1]. It was shown that mice lacking Ocn (Ocn −/−) displayed glucose intolerance due to impaired insulin secretion and insulin resistance [1] while the metabolic phenotypes of mice lacking the gene Esp (Esp −/−), which had high circulating undercarboxylated Ocn (unOcn) but normal serum levels of total Ocn (tOcn), were just opposite to those observed in Ocn −/− mice [1]. What’s more, administration of unOcn to mice significantly improved glucose tolerance and protected both wild-type and high-fat diet mice from obesity and type 2 diabetes [2, 3].
Since the discovery of the hormonal properties of Ocn, many clinical studies have investigated the associations between serum tOcn and/or unOcn and biomarkers of glucose metabolism in humans [4–6]. However, the results are contradictory. Some studies have demonstrated higher serum levels of either tOcn or unOcn were correlated with lower fasting plasma glucose (FPG) or glycated hemoglobin A1c (HbA1c) [5, 7–9], whereas no such associations could be found in other studies [10–13]. It is also not clear in humans whether unOcn is more closely related with glucose-related parameters than tOcn as observed in mice studies. In addition, the study populations in human studies were heterogeneous; some studies were performed in normal adults, some in patients with different degrees of glucose tolerance, including type 2 diabetes, while some others in participants without defining diabetes status [6, 14–16]. The gender, ethnicities, and sample size of these human studies were also varied greatly. All these factors may contribute to the conflicting outcomes. In this circumstance, meta-analysis offers an effective approach to explore the overall estimate between Ocn and glucose metabolism. Therefore, we conducted a meta-analysis of the existing data sources to investigate the magnitude of associations between different subtypes of Ocn (tOcn and unOcn) and FPG or HbA1c. We also tried to give a comprehensive view of these relationships in different populations according to ethnicity and gender.
Methods
Search strategy
We searched PubMed, ISI Web of Knowledge, and the Cochrane library from August 2007 to June 2014 to identify studies that evaluated the association between Ocn and FPG. We used the following keywords: “osteocalcin,” “bone Gla protein,” or “Bone gamma-carboxyglutamate protein” in combination with “glucose” or “glycated hemoglobin A1c” or “HbA1c” with no restriction. In addition, we read the reference lists of original articles and reviews in case of missing studies that were relevant to our current meta-analysis. The inclusion criteria of the studies were (1) original studies published in English language, investigating associations between Ocn and FPG or HbA1c; (2) observational studies conducted with adults; and (3) studies reporting a correlation coefficient r. We excluded review papers, letters, case-reports, studies with children, adolescents or pregnant women, diseases apparently affecting serum Ocn, as well as animal studies. If the same population was used in more than one study, only the study providing more information was included.
Quality assessment and data extraction
Two of the authors (Liu DM and Guo XZ) independently searched all of the related studies and identified eligible studies meeting the above criteria. The quality of the studies was assessed according to the Agency for Healthcare Research and Quality guidelines. Data extracted included the authors, year of publication, ethnicity, age, gender, sample size, and the r value between tOcn or unOcn and FPG or HbA1c. When the results were presented from various covariate analyses, we extracted the unadjusted ones because some of the studies over-adjusted for multiple confounders, which may influence the causal pathway between Ocn and glucose metabolism. Discrepancies were resolved upon discussion. We contacted the authors of the primary studies for detailed information when necessary.
The Spearman correlation coefficients were first transformed to Pearson correlation coefficients [17]. A Fisher transformation was used to convert each correlation coefficient into an approximately normal distribution for meta-analysis, and then back-transformed into the original correlation coefficients in the final results [18].
Statistical analysis
A pooled effect size of the included studies was determined using a random-effects model by the method of DerSimonian and Laird [19], and the results were presented as correlation coefficients with 95 % confidence intervals (CI). Analyses of the different populations were conducted according to ethnicity (East Asian and Caucasian) and gender (men and women) using a random-effects model or fixed-effects model to give further insight into the associations between Ocn, FPG and HbA1c in different populations.
The heterogeneity of correlations across the studies was assessed by the Cochran Q test, where P < 0.10 was considered statistically heterogeneous. An additional measure of heterogeneity was tested using the coefficient of inconsistency (I 2) statistic with 25, 50, and 75 % corresponding to cut-off points for low, moderate, and high degrees of heterogeneity, respectively [20, 21]. In addition, we performed subgroup analysis based on ethnicity and gender to investigate potential sources of heterogeneity.
For the sensitivity analysis, we repeated the calculations by omitting one study at one time to assess the stability of the estimates. Furthermore, we used the Begg’s adjusted rank correlation test and the Egger’s regression asymmetry test to detect publication bias, for both tests, P > 0.05 represented no significant publication bias [22, 23].
All of the statistical analyses were performed using STATA version 12.0 (Stata Corp, College Station, TX, USA).
Results
Characteristics of studies
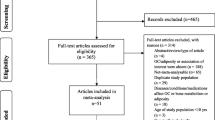
Briefly, 1370 references (716 from PubMed, 651 from ISI web of science, and 3 from the Cochrane library) were identified. Of those references, 1287 were excluded due to duplication and on a screening of the abstracts or titles. The full texts of the remaining 83 references were examined in detail, and 44 references were excluded according to the inclusion criteria. Finally, 39 citations involving 23,381 subjects were included in the meta-analysis [4–16, 24–49] (Fig. 1). The r values of the 15 studies included in this meta-analysis were transformed from Spearman correlation coefficients.

Flowchart of selected references
Thirty-four studies including 19,333 subjects were selected to analyze the association between tOcn and FPG, and 9 studies involving 6294 subjects were obtained to calculate the overall correlation coefficient between unOcn and FPG. Moreover, 21 studies containing 10,363 participants and 7 studies including 6145 participants were selected to analyze the relationships between tOcn or unOcn and HbA1c, respectively. The serum unOcn were all reported as absolute value quantified by electrochemiluminescence immunoassay (ECLIA) [14, 27, 28, 38, 40], or enzyme-linked immunosorbent assay (ELISA) [30, 33, 41, 43, 45]. The detailed information regarding the included studies is shown in Table 1. We included case-control or prospective studies that reported the correlation coefficients between Ocn and FPG or HbA1c at baseline.
Overall analysis and sensitivity analysis
For FPG, a random-effects meta-analysis revealed that the pooled estimate was −0.16 (95 % CI, −0.19 to −0.14) between tOcn and FPG with significant heterogeneity (I 2 = 66.2 %, P < 0.001) (Fig. 2a). The summary correlation between unOcn and FPG was −0.15 (95 % CI, −0.20 to −0.11), and clear heterogeneity was observed (I 2 = 52.5 %, P = 0.017) (Fig. 2b). For HbA1c, a fixed-effects model was used to calculate the correlation coefficient between tOcn and HbA1c (r = −0.16, 95 % CI, −0.18 to −0.14; I 2 = 43.1 %) (Fig. 3a), whereas a random-effects model was applied to obtain the overall estimate between unOcn and HbA1c (r = −0.16, 95 % CI, −0.23 to −0.08; I 2 = 84.5 %) (Fig. 3b).

Correlation (95 % CI) between tOcn (a) or unOcn (b) and FPG from a random-effects model

Correlation (95 % CI) between tOcn (a) or unOcn (b) and HbA1c from a fix-effects model and random-effects model
Due to significant heterogeneity, a sensitivity analysis was conducted to investigate the stability of the estimates and explore the potential sources of heterogeneity. No single study displayed a substantial influence on the summary effect size between tOcn and FPG or HbA1c. The combined association ranged from −0.16 (95 % CI, −0.19 to −0.13) to −0.17 (95 % CI, −0.19 to −0.14) for FPG and varied from −0.16 (95 % CI, −0.19 to −0.13) to −0.17 (95 % CI, −0.19 to −0.15) for HbA1c. However, after excluding the study of Furusyo et al. [38], which was conducted in a Japanese population living in northern Kyushu with low vitamin K intake (vitamin K is essential for the carboxylation of osteocalcin), the heterogeneity in the unOcn group disappeared both for FPG and HbA1c, although the results did not change, with the overall estimates fluctuating from a low of −0.14 (95 % CI, −0.18 to −0.09) to a high of −0.17 (95 % CI, −0.21 to −0.14) between unOcn and FPG, and −0.14 (95 % CI, −0.21 to −0.064) to −0.18 (95 % CI, −0.22 to −0.14) between unOcn and HbA1c.
Subgroup analysis
The populations were stratified according to ethnicity and gender and a subgroup analysis was conducted to explore whether either contributed to the heterogeneity. A fixed-effects model was performed in subgroups with I 2 lower than 50 %, while random-effects model was employed in subgroups with significant heterogeneity (I 2 ≥ 50 %) (Table 2). Significant negative associations were found in different subgroup populations between tOcn and FPG or HbA1c without significant differences between the groups (Table 2). While, the combined effect size between unOcn and FPG was statistically lower in women than that in men (r = −0.09, 95 % CI, −0.13 to −0.05; r = −0.18, 95 % CI, −0.21 to −0.14, respectively; P for interaction < 0.05) (Table 2). Regarding to the correlation of unOcn and HbA1c, our result showed that there was no statistical difference between men and women (P for interaction > 0.05), although a significant association was observed in men (r = −0.19, 95 % CI, −0.24 to −0.14) rather than women (r = −0.09, 95 % CI, −0.22 to 0.04) (Table 2). The association between unOcn and FPG was significant in East Asians with correlation coefficient −0.15 (95 % CI, −0.20 to −0.10), while in Caucasians, the r value was −0.34 (95 % CI, −0.67 to 0.13) (P for interaction > 0.05) (Table 2).
Publication bias
Both Begg’s and Egger’s test were used to evaluate the potential publication bias. No obvious publication bias was found regarding the included studies evaluating the relationship between total- or unOcn and FPG or HbA1c. For FPG, the Begg’s test P values for tOcn and unOcn were 0.257 and 0.837, respectively; For HbA1c, the Begg’s test P values for tOcn and unOcn were 0.785 and 0.858, respectively.
Discussion
The main findings of our current meta-analysis are that both circulating tOcn and unOcn are negatively correlated with FPG and HbA1c with similar potency, and the associations between unOcn and glucose metabolism appears to be more prominent in men than in women.
In recent years, genetic and pharmacological studies in mice models suggested that Ocn can promote insulin secretion, improve insulin sensitivity, and improve glucose tolerance [1]. In addition, mice lacking Ocn receptor Gprc6a specifically in the beta cell lineage displayed glucose intolerance resulting from reduced insulin production [50]. In mice studies, it was also repeatedly demonstrated that the favorable metabolic effects of Ocn on glucose metabolism are mediated through its undercaboxylated form unOcn [2, 3, 51]. Similarly, the majority of human cross-sectional investigations echo the findings in animal studies. In a recent meta-analysis, it also demonstrated that diabetic patients had a significant lower serum tOcn levels as compared with nondiabetes subjects [52], which was consistent with our findings that tOcn was in a negative association with FPG and HbA1c. As shown in this meta-analysis, both tOcn and unOcn were negatively associated with FPG and HbA1c levels in humans, showing possible involvement of Ocn in glucose homeostasis.
It is noteworthy that there is some controversy regarding the best assay to use for unOcn measurement [53, 54]. Serum unOcn can be measured either by hydroxyapatite (HAP) binding assay, in which the result is reported semi-quantitatively as a fraction of tOcn, or by ECLIA or ELISA methods directly as an absolute value [53, 55]. It was shown that serum unOcn is highly correlated with circulating tOcn concentrations [56, 57], while the serum percentage of unOcn does not correlate with tOcn that much [56]. In this meta-analysis, all the enrolled studies presented the absolute unOcn values. In addition to this technical issue, when analyzing the relations of unOcn with glucose- and obesity-related parameters, the potential confounders, such as age, gender, estrogen levels, food or vitamin K intake, and etc., should all be considered [54, 56, 58, 59].
In the current analysis, the association between tOcn and FPG or HbA1c was similar to unOcn and FPG or HbA1c. Indeed, tOcn and unOcn levels are highly correlated [53, 56, 57]; it is thus expected that at least under normal circumstances (i.e., vitamin K sufficiency), tOcn levels are a good indicator of unOcn concentrations. Therefore, although unOcn was regarded as a metabolically active form of Ocn in mice, in humans, as inferred from our current study, both tOcn and unOcn could be used as biomarkers related with glucose metabolism. The present results were further supported by a recent study that higher tOcn and unOcn were both related with lower diabetes risk [60].
In this meta-analysis, we also found that the magnitude of the correlation between unOcn and glucose metabolism appears to be greater in men than in women, which is consistent with several studies [8, 14, 38, 40]. The mechanism for such a finding is not clear. Ocn has been demonstrated to induce testosterone production by the testes in male mice [61], while in both rodents and human studies, it was shown that testosterone can protect against streptozotocin- or glucotoxicity-induced β cell apoptosis, especially in male rats [62, 63], and alleviate insulin resistance and improve glycemic control in hypogonadic type 2 diabetic men [64]. However, a most recent systematic review and meta-analysis of randomized controlled clinical trials failed to demonstrate the effects of testosterone treatment on glycemic control in male patients with type 2 diabetes and metabolic syndrome [65]. It is also not clear whether the correlation between unOcn and glucose metabolism observed only in males but not in females is overestimated. It was reported that serum unOcn concentrations were influenced by menopausal status [66], but the majority of studies involved in this meta-analysis did not distinguish the postmenopausal women from the total group. It is thus necessary to further investigate the underlying mechanism or the impacts of the interplay between tOcn, unOcn, and gonadal hormones on glucose metabolism in males and females separately.
In this study, we found that the correlation between unOcn and FPG appears to be significant in East Asians, but not in Caucasians. This result should be interpreted with caution. It should be noted that in the current analysis, only two studies with a very small number of Caucasian participants (n = 180) were included. In addition, a significant heterogeneity was observed, which further biased the summary effects. Therefore, confirming the association between unOcn and FPG in Caucasians will require additional studies with a larger sample size.
The current study shows no evidence of publication bias as measured by all of the methods (funnel plot, Begg’s and Egger’s tests). Whereas, significant heterogeneity was detected among the studies included; a random-effects model was applied to address this problem; subgroup analysis was further performed to deal with it. A possible reason for the heterogeneity among the studies may be due to the discrepancy of ethnicity and gender. In addition, the sample size, duration of diabetes mellitus, drugs taken for glycemic control, age, BMI, and statistic methods may also contribute to the heterogeneity in this meta-analysis.
Some limitations of our current study should be mentioned. First, we did not explore whether the associations between Ocn and FPG or HbA1c are different among nondiabetics, prediabetes, type 2 diabetes mellitus, and type 1 diabetes mellitus. Second, the studies with no significant results tend to be unpublished. This situation, to a certain extent, tends to overestimate the pooled estimate. Moreover, the inadequate inclusion of pertinent references threatens the validity of meta-analysis. Third, the present analysis was conducted entirely with cross-sectional studies reporting the correlation coefficients between Ocn and FPG or HbA1c, where association does not mean causation.
In general, our current meta-analysis agrees with rodent studies which demonstrated a beneficial effect of Ocn on glucose metabolism [1–3], and provided further evidence to demonstrate a negative association between Ocn and FPG and HbA1c in humans. This correlation appears to be more obvious in men than in women for unOcn; however, the causality between Ocn and glucose metabolism calls for prospective studies with larger sample sizes.
References
Lee NK, Sowa H, Hinoi E, Ferron M, Ahn JD, Confavreux C, Dacquin R, Mee PJ, McKee MD, Jung DY, Zhang Z, Kim JK, Mauvais-Jarvis F, Ducy P, Karsenty G (2007) Endocrine regulation of energy metabolism by the skeleton. Cell 130:456–469
Ferron M, McKee MD, Levine RL, Ducy P, Karsenty G (2012) Intermittent injections of osteocalcin improve glucose metabolism and prevent type 2 diabetes in mice. Bone 50:568–575
Ferron M, Hinoi E, Karsenty G, Ducy P (2008) Osteocalcin differentially regulates beta cell and adipocyte gene expression and affects the development of metabolic diseases in wild-type mice. Proc Natl Acad Sci U S A 105:5266–5270
Kindblom JM, Ohlsson C, Ljunggren O, Karlsson MK, Tivesten A, Smith U, Mellstrom D (2009) Plasma osteocalcin is inversely related to fat mass and plasma glucose in elderly Swedish men. J Bone Miner Res 24:785–791
Zhou M, Ma X, Li H, Pan X, Tang J, Gao Y, Hou X, Lu H, Bao Y, Jia W (2009) Serum osteocalcin concentrations in relation to glucose and lipid metabolism in Chinese individuals. Eur J Endocrinol 161:723–729
Saleem U, Mosley TH Jr, Kullo IJ (2010) Serum osteocalcin is associated with measures of insulin resistance, adipokine levels, and the presence of metabolic syndrome. Arterioscler Thromb Vasc Biol 30:1474–1478
Im JA, Yu BP, Jeon JY, Kim SH (2008) Relationship between osteocalcin and glucose metabolism in postmenopausal women. Clin Chim Acta 396:66–69
Bae SJ, Choe JW, Chung YE, Kim BJ, Lee SH, Kim HY, Koh JM, Kim HK, Kim GS (2011) The association between serum osteocalcin levels and metabolic syndrome in Koreans. Osteoporos Int 22:2837–2846
Bao Y, Zhou M, Lu Z, Li H, Wang Y, Sun L, Gao M, Wei M, Jia W (2011) Serum levels of osteocalcin are inversely associated with the metabolic syndrome and the severity of coronary artery disease in Chinese men. Clin Endocrinol (Oxf) 75:196–201
Kim SH, Lee JW, Im JA, Hwang HJ (2010) Serum osteocalcin is related to abdominal obesity in Korean obese and overweight men. Clin Chim Acta 411:2054–2057
Zhang Y, Qi L, Gu W, Yan Q, Dai M, Shi J, Zhai Y, Chen Y, Liu J, Wang W, Ning G, Hong J (2010) Relation of serum osteocalcin level to risk of coronary heart disease in Chinese adults. Am J Cardiol 106:1461–1465
Buday B, Pach FP, Literati-Nagy B, Vitai M, Vecsei Z, Koranyi L (2013) Serum osteocalcin is associated with improved metabolic state via adiponectin in females versus testosterone in males. Gender specific nature of the bone-energy homeostasis axis. Bone 57:98–104
Caglar GS, Ozdemir ED, Kiseli M, Demirtas S, Cengiz SD (2014) The association of osteocalcin and adiponectin with glucose metabolism in nondiabetic postmenopausal women. Gynecol Obstet Invest 77:255–260
Kanazawa I, Yamaguchi T, Yamauchi M, Yamamoto M, Kurioka S, Yano S, Sugimoto T (2011) Serum undercarboxylated osteocalcin was inversely associated with plasma glucose level and fat mass in type 2 diabetes mellitus. Osteoporos Int 22:187–194
Lee SW, Jo HH, Kim MR, You YO, Kim JH (2012) Association between obesity, metabolic risks and serum osteocalcin level in postmenopausal women. Gynecol Endocrinol 28:472–477
Liao M, Guo X, Yu X, Pang G, Zhang S, Li J, Tan A, Gao Y, Yang X, Zhang H, Qin X, Mo L, Lu Z, Wu C, Mo Z (2013) Role of metabolic factors in the association between osteocalcin and testosterone in Chinese men. J Clin Endocrinol Metab 98:3463–3469
Rupinski MT, Dunlap WP (1996) Approximating Pearson Product-Moment Correlations from Kendall’s Tau and Spearman’s Rho. Educ Psychol Meas 56:419–429
Borenstein M, Hedges LV, Higgins JPT, Rothstein HR (2009) Introduction to meta-analysis. John Wiley & Sons, Ltd., United Kingdom
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Leeflang MM, Deeks JJ, Gatsonis C, Bossuyt PM, Cochrane Diagnostic Test Accuracy Working Group (2008) Systematic reviews of diagnostic test accuracy. Ann Intern Med 149:889–897
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539–1558
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50:1088–1101
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Aoki A, Muneyuki T, Yoshida M, Munakata H, Ishikawa SE, Sugawara H, Kawakami M, Kakei M (2011) Circulating osteocalcin is increased in early-stage diabetes. Diabetes Res Clin Pract 92:181–186
Bao YQ, Zhou M, Zhou J, Lu W, Gao YC, Pan XP, Tang JL, Lu HJ, Jia WP (2011) Relationship between serum osteocalcin and glycaemic variability in Type 2 diabetes. Clin Exp Pharmacol Physiol 38:50–54
Garcia-Martin A, Cortes-Berdonces M, Luque-Fernandez I, Rozas-Moreno P, Quesada-Charneco M, Munoz-Torres M (2011) Osteocalcin as a marker of metabolic risk in healthy postmenopausal women. Menopause 18:537–541
Levinger I, Zebaze R, Jerums G, Hare DL, Selig S, Seeman E (2011) The effect of acute exercise on undercarboxylated osteocalcin in obese men. Osteoporos Int 22:1621–1626
Iki M, Tamaki J, Fujita Y, Kouda K, Yura A, Kadowaki E, Sato Y, Moon JS, Tomioka K, Okamoto N, Kurumatani N (2012) Serum undercarboxylated osteocalcin levels are inversely associated with glycemic status and insulin resistance in an elderly Japanese male population: Fujiwara-kyo Osteoporosis Risk in Men (FORMEN) Study. Osteoporos Int 23:761–770
Movahed A, Larijani B, Nabipour I, Kalantarhormozi M, Asadipooya K, Vahdat K, Akbarzadeh S, Farrokhnia M, Assadi M, Amirinejad R, Bargahi A, Sanjdideh Z (2012) Reduced serum osteocalcin concentrations are associated with type 2 diabetes mellitus and the metabolic syndrome components in postmenopausal women: the crosstalk between bone and energy metabolism. J Bone Miner Metab 30:683–691
Ngarmukos C, Chailurkit LO, Chanprasertyothin S, Hengprasith B, Sritara P, Ongphiphadhanakul B (2012) A reduced serum level of total osteocalcin in men predicts the development of diabetes in a long-term follow-up cohort. Clin Endocrinol (Oxf) 77:42–46
Wieczorek-Baranowska A, Nowak A, Pilaczynska-Szczesniak L (2012) Osteocalcin and glucose metabolism in postmenopausal women subjected to aerobic training program for 8 weeks. Metabolism 61:542–545
Wiklund P, Nordstrom A, Hogstrom M, Alfredson H, Engstrom P, Gustafsson T, Franks PW, Nordstrom P (2012) High-impact loading on the skeleton is associated with a decrease in glucose levels in young men. Clin Endocrinol (Oxf) 77:823–827
Alfadda AA, Masood A, Shaik SA, Dekhil H, Goran M (2013) Association between osteocalcin, metabolic syndrome, and cardiovascular risk factors: role of total and undercarboxylated osteocalcin in patients with type 2 diabetes. Int J Endocrinol 2013:197519
Bao Y, Ma X, Yang R, Wang F, Hao Y, Dou J, He H, Jia W (2013) Inverse relationship between serum osteocalcin levels and visceral fat area in Chinese men. J Clin Endocrinol Metab 98:345–351
dos Santos B, Magalhaes K, Magalhaes MM, Diniz ET, Lucena CS, Griz L, Bandeira F (2013) Metabolic syndrome and central fat distribution are related to lower serum osteocalcin concentrations. Ann Nutr Metab 62:183–188
Chen L, Li Q, Yang Z, Ye Z, Huang Y, He M, Wen J, Wang X, Lu B, Hu J, Liu C, Ling C, Qu S, Hu R (2013) Osteocalcin, glucose metabolism, lipid profile and chronic low-grade inflammation in middle-aged and elderly Chinese. Diabet Med 30:309–317
Dou J, Ma X, Fang Q, Hao Y, Yang R, Wang F, Zhu J, Bao Y, Jia W (2013) Relationship between serum osteocalcin levels and non-alcoholic fatty liver disease in Chinese men. Clin Exp Pharmacol Physiol 40:282–288
Furusyo N, Ihara T, Hayashi T, Ikezaki H, Toyoda K, Ogawa E, Okada K, Kainuma M, Murata M, Hayashi J (2013) The serum undercarboxylated osteocalcin level and the diet of a Japanese population: results from the Kyushu and Okinawa Population Study (KOPS). Endocrine 43:635–642
Liu JM, Zhao HY, Zhao L, Chen Y, Zhang LZ, Tao B, Sun LH, Zhao YJ, Wang WQ, Xu MY, Chen JL, Ning G (2013) An independent positive relationship between the serum total osteocalcin level and fat-free mass in healthy premenopausal women. J Clin Endocrinol Metab 98:2146–2152
Ogawa-Furuya N, Yamaguchi T, Yamamoto M, Kanazawa I, Sugimoto T (2013) Serum osteocalcin levels are inversely associated with abdominal aortic calcification in men with type 2 diabetes mellitus. Osteoporos Int 24:2223–2230
Schwetz V, Gumpold R, Graupp M, Hacker N, Schweighofer N, Trummer O, Pieber TR, Ballon M, Lerchbaum E, Obermayer-Pietsch B (2013) Osteocalcin is not a strong determinant of serum testosterone and sperm count in men from infertile couples. Andrology 1:590–594
Sheng L, Cao W, Cha B, Chen Z, Wang F, Liu J (2013) Serum osteocalcin level and its association with carotid atherosclerosis in patients with type 2 diabetes. Cardiovasc Diabetol 12:22
Wang Q, Zhang B, Xu Y, Xu H, Zhang N (2013) The relationship between serum osteocalcin concentration and glucose metabolism in patients with type 2 diabetes mellitus. Int J Endocrinol 2013:842598
Weiler HA, Lowe J, Krahn J, Leslie WD (2013) Osteocalcin and vitamin D status are inversely associated with homeostatic model assessment of insulin resistance in Canadian Aboriginal and white women: the First Nations Bone Health Study. J Nutr Biochem 24:412–418
Chen X, Wu Y, Liu L, Tian H, Yu X (2014) Osteocalcin is inversely associated with glucose levels in middle-aged Tibetan men with different degrees of glucose tolerance. Diabetes Metab Res Rev 30:476–482
Choudhury AB, Sarkar PD, Sakalley DK, Petkar SB (2014) Role of adiponectin in mediating the association of osteocalcin with insulin resistance and type 2 diabetes: a cross sectional study in pre- and post-menopausal women. Arch Physiol Biochem 120:73–79
Cui R, Su B, Sheng C, Cheng X, Yang P, Bu L, Li H, Wang J, Sheng H, Qu S (2014) Total osteocalcin in serum predicts testosterone level in male type 2 diabetes mellitus. Int J Clin Exp Med 7:1145–1149
Maddaloni E, D'Onofrio L, Lauria A, Maurizi AR, Strollo R, Palermo A, Napoli N, Angeletti S, Pozzilli P, Manfrini S (2014) Osteocalcin levels are inversely associated with Hba1c and BMI in adult subjects with long-standing type 1 diabetes. J Endocrinol Invest 37:661–666
Rui X, Xu B, Su J, Pan C, Zhan C, Su B, Li H, Wang J, Sheng H, Qu S (2014) Differential pattern for regulating insulin secretion, insulin resistance, and lipid metabolism by osteocalcin in male and female T2DM patients. Med Sci Monit 20:711–719
Wei J, Hanna T, Suda N, Karsenty G, Ducy P (2014) Osteocalcin promotes beta-cell proliferation during development and adulthood through Gprc6a. Diabetes 63:1021–1031
Wei J, Ferron M, Clarke CJ, Hannun YA, Jiang H, Blaner WS, Karsenty G (2014) Bone-specific insulin resistance disrupts whole-body glucose homeostasis via decreased osteocalcin activation. J Clin Invest 124:1–13
Starup-Linde J, Eriksen SA, Lykkeboe S, Handberg A, Vestergaard P (2014) Biochemical markers of bone turnover in diabetes patients–a meta-analysis, and a methodological study on the effects of glucose on bone markers. Osteoporos Int 25:1697–1708
Gundberg CM, Lian JB, Booth SL (2012) Vitamin K-dependent carboxylation of osteocalcin: friend or foe? Adv Nutr 3:149–157
Ferron M, Wei J, Yoshizawa T, Ducy P, Karsenty G (2010) An ELISA-based method to quantify osteocalcin carboxylation in mice. Biochem Biophys Res Commun 397:691–696
Nishimura J, Arai N, Tohmatsu J (2007) Measurement of serum undercarboxylated osteocalcin by ECLIA with the “Picolumi ucOC” kit. Clin Calcium 17:1702–1708
Booth SL, Centi A, Smith SR, Gundberg C (2013) The role of osteocalcin in human glucose metabolism: marker or mediator? Nat Rev Endocrinol 9:43–55
Kirmani S, Atkinson EJ, Melton LJ 3rd, Riggs BL, Amin S, Khosla S (2011) Relationship of testosterone and osteocalcin levels during growth. J Bone Miner Res 26:2212–2216
Kumar R, Vella A (2011) Carbohydrate metabolism and the skeleton: picking a bone with the beta-cell. J Clin Endocrinol Metab 96:1269–1271
Binkley NC, Krueger DC, Engelke JA, Foley AL, Suttie JW (2000) Vitamin K supplementation reduces serum concentrations of under-gamma-carboxylated osteocalcin in healthy young and elderly adults. Am J Clin Nutr 72:1523–1528
Yeap BB, Alfonso H, Chubb SA, Gauci R, Byrnes E, Beilby JP, Ebeling PR, Handelsman DJ, Allan CA, Grossmann M, Norman PE, Flicker L (2015) Higher serum undercarboxylated osteocalcin and other bone turnover markers are associated with reduced diabetes risk and lower estradiol concentrations in older men. J Clin Endocrinol Metab 100:63–71
Oury F, Sumara G, Sumara O, Ferron M, Chang H, Smith CE, Hermo L, Suarez S, Roth BL, Ducy P, Karsenty G (2011) Endocrine regulation of male fertility by the skeleton. Cell 144:796–809
Kooptiwut S, Hanchang W, Semprasert N, Junking M, Limjindaporn T, Yenchitsomanus PT (2015) Testosterone reduces AGTR1 expression to prevent beta-cell and islet apoptosis from glucotoxicity. J Endocrinol 224:215–224
Palomar-Morales M, Morimoto S, Mendoza-Rodriguez CA, Cerbon MA (2010) The protective effect of testosterone on streptozotocin-induced apoptosis in beta cells is sex specific. Pancreas 39:193–200
Kapoor D, Goodwin E, Channer KS, Jones TH (2006) Testosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with type 2 diabetes. Eur J Endocrinol 154:899–906
Grossmann M, Hoermann R, Wittert G, Yeap BB (2014) Effects of testosterone treatment on glucose metabolism and symptoms in men with type 2 diabetes and the metabolic syndrome: a systematic review and meta-analysis of randomized controlled clinical trials. Clin Endocrinol (Oxf). doi:10.1111/cen.12664
Yasui T, Uemura H, Tomita J, Miyatani Y, Yamada M, Miura M, Irahara M (2006) Association of serum undercarboxylated osteocalcin with serum estradiol in pre-, peri- and early post-menopausal women. J Endocrinol Invest 29:913–918
Funding
This work was supported by the National Nature Science Foundation of China (grants 81370977 and 81170804) and Doctoral Innovation Fund Projects from Shanghai Jiao Tong University School of Medicine (BXJ201410).
Conflicts of interest
Dong-mei Liu, Xing-zhi Guo, Hai-jun Tong, Bei Tao, Li-hao Sun, Hong-Yan Zhao, Guang Ning, and Jian-min Liu declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding authors
Additional information
D.-M. Liu and X.-Z. Guo contributed equally to this work.
Rights and permissions
About this article

Cite this article
Liu, DM., Guo, XZ., Tong, HJ. et al. Association between osteocalcin and glucose metabolism: a meta-analysis. Osteoporos Int 26, 2823–2833 (2015). https://doi.org/10.1007/s00198-015-3197-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-015-3197-8