
Abstract
The elevated serum undercarboxylated osteocalcin (ucOC) level is related to osteoporosis. In Japan, vitamin K intake is lower, and the incidence of hip fractures noticeably higher in northern Kyushu than in other areas. The study was done to determine the serum ucOC levels in a Japanese population and its association with diet and glucose metabolism. The data of 3,658 healthy adults aged 40–69 (1,373 men and 2,285 women) who lived in northern Kyushu area were analyzed. The data included anthropometric measurements and a self-reported personal interview on daily intake of foods. The serum ucOC level of each participant was measured by electrochemiluminescence immunoassay. Glycohemoglobin A1c (HbA1c), fasting plasma glucose, and serum insulin concentrations were measured. The median serum ucOC level of the women (4.65 ng/mL) was significantly higher than that of the men (3.04 ng/mL) (P = 0.0021). The age-specific ucOC levels of the men decreased significantly with age. In contrast, the ucOC levels of the women aged ≥50 were elevated, but the levels varied markedly within the other age groups. For both men and women, multivariate analysis identified a daily diet rich in vitamin K and HbA1c level as independently having a significant, negative relationship to serum ucOC level. Our study indicates that the serum ucOC decreases with age in men, increases postmenopausally in women, and correlates inversely with dietary consumption of certain foods and with fasting glucose and HbA1c level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a major public health problem worldwide due to the morbidity and mortality associated with osteoporotic fractures. Osteoporosis is characterized by a systemic impairment of bone mass and microarchitecture that results in fractures [1–4]. Osteoporosis is defined as a bone mineral density (BMD) ≥ 2.5 standard deviations below the mean peak bone mass of the average of young healthy adults as measured by X-ray absorptiometry.
Osteocalcin (OC), bone carboxylated protein, is a bone formation marker that contributes to mineral formation and maintenance of calcium ion homeostasis through a mechanism by which, in osteoblasts, vitamin K-dependent carboxylase adds carbonate ion to γ-glutamine residue, which allows incorporation into the bone matrix [5]. Vitamin K deficiency has been related to osteoporosis and identified as a risk factor for hip fracture [6]. Subclinical vitamin K deficiency in bone allows the transfer of under γ-carboxylated OC (ucOC), previously called non-carboxylated osteocalcin, to the blood; thus, a higher serum ucOC level reflects the nutritional state of vitamin K [7, 8]. Both BMD and ucOC, but not total OC, have been associated with the risk of hip fracture: odds ratio (OR) of 2.4 for low BMD, OR of 1.9 for high ucOC, and increased OR of 5.5 for both low BMD and high ucOC in elderly women, suggesting that ucOC predicts hip fracture risk independently of BMD [7].
Vitamin K naturally exists in two forms, phylloquinone (vitamin K1) and menaquinone (vitamin K2). Vitamin K1 is widely distributed in green and yellow leaf vegetables, whereas vitamin K2 exists preferentially in cheese, butter, and fermented soybeans. Soybean and soybean-derived foods contain isoflavones that affect bone metabolism [9].
The aims of this cross-sectional study were to determine the serum ucOC level in a large community-based population (n > 3,000) and to clarify the relationship between serum ucOC level and a diet rich in vitamin K. We also investigated the relationship between serum ucOC level and glucose metabolism in this large population.
Methods
Study population
The Kyushu and Okinawa Population Study (KOPS) was begun in 2007 as a survey of the incidence of vascular events associated with lifestyle-related diseases among the general population in Japan [10, 11]. In the present sub-study, we evaluated residents of Kasuya Town, a suburban area with about 35,500 residents and adjacent to Fukuoka City, Kyushu Island. The participants were residents notified by local newspaper and public announcements of a free annual health examination given by our department. Eligibility was limited to healthy residents aged 40–69 at the time of the investigation. Between June 2007 and November 2009, 6,348 residents took the examination, and 5,663 who agreed were enrolled for study (participation rate 89.2 %). Of these, 1,092 were excluded who self-reported currently as being under medical care for cardiovascular disease (n = 305), cerebrovascular disease (n = 169), cancer (n = 181), pulmonary and bronchial disease (n = 119), liver disease (n = 85), chronic renal disease (n = 21), or endocrine and metabolic disease including diabetes (n = 209) or who reported excessive alcohol consumption (n = 3). Also excluded were 522 who reported a history of cardiovascular (n = 76), cerebrovascular (n = 89), or endocrine and metabolic disease (n = 357). A further 275 were excluded for taking anti-osteoporosis drugs (bisphosphonate, selective estrogen receptor modulator, calcium, vitamin D, and vitamin K), estrogen analogs, multi-vitamin drugs, or systematic antiviral, antineoplastic, or immune-modulating drugs within the 12 months before enrollment. Of the remaining 3,774 residents, 116 with incomplete data were excluded, leaving the data of 3,658 healthy residents (1,373 men and 2,285 women) available for analysis. The study was approved by the Kyushu University Hospital Ethics Committee. Written informed consent was obtained from all participants prior to the examination. This study was carried out in accordance with the principles of the Declaration of Helsinki as revised in 2000.
Questionnaire
All participants completed a self-administered questionnaire and, at the same time, underwent anthropometric measurements and venous blood drawing. The questionnaire inquired about the followings: daily dietary habits, smoking, alcohol consumption, diseases under current or previous treatment, use of drugs and vitamin supplements, and family history of selected diseases, and, for women only, menarche age and menopausal status. The postmenopausal status of each female participant was determined through the interview and was defined as the absence of menstrual bleeding during the preceding 12 months.
The food-frequency questionnaire (FFQ) was used to access average intake frequency at which the following foods and beverages were consumed over the past year. The questionnaire was primarily derived from the FFQ developed by Tokudome et al. [12], which was validated with 3D weighted diet records as the standard for energy and 26 nutrients, with most of the nutrients showing correlation coefficients of 0.4–0.6. Foods and beverages in our FFQ included fermented foods [(nattô; cooked soybeans fermented with Bacillus subtilis), miso soup, margarine, green and yellow leaf vegetables (green leaf vegetable, lettuce, spinach, broccoli, carrots, and cabbage), dairy products (cheese, butter, and yogurt), and drinks (coffee, Japanese green tea, and vegetable juice). For each item, the participant described consumption frequency over the past year by choosing 1 of 8 categories: rarely eat, eat 1–3 times a month, eat 1–2 times a week, eat 3–4 times a week, eat 5–6 times a week, eat once a day, eat twice a day, and eat three times a day.
Measurement of serum ucOC level and glucose metabolism test
Aliquots of whole blood and fresh serum and plasma samples from each participant were immediately sent at 4 °C to a clinical laboratory testing company (SRL, Fukuoka, Japan) for the measurement of the serum ucOC, fasting plasma glucose (FPG), fasting serum insulin, and glycohemoglobin A1c (HbA1c) levels.
The serum ucOC level of each participant was determined by a commercially available kit (Picolumi ucOC, Eidia Co., Ltd., Tokyo). It is a one-step sandwich electro-chemiluminescence immunoassay (electro-CLIA) that utilizes two mouse monoclonal undercarboxylated OC antibodies (Glu-OC4-5 and OC G3) (one of which is coated on the plate, and the other is ruthenium-labeled) for detection of ucOC. When used with an autoanalyzer, the kit achieved highly sensitive and rapid measurement over a range of 0.39–50 ng/mL. Assessment of reproducibility testing showed good results, with a coefficient of variation of ≤ 10 %, the recovery rate for spiked samples was 93–106 %, and there was no influence of interfering substances at normal levels [13].
FPG concentration was measured using a hexokinase-glucose-6-phosphate dehydrogenase method (Quick Auto Neo GLU-HK, Sinotest, Tokyo, Japan). Fasting serum insulin concentration was measured by chemiluminescent enzyme immunoassay (Lumipulse Presto Insulin, Fujirebio, Tokyo, Japan). The Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) was calculated using the following formula: FPG (mg/dL) × fasting serum insulin (μU/mL)/405. The HbA1c level was measured from fresh whole blood samples with an immune coherent method (RAPIDIA Auto HbA1c; Fujirebio). HbA1c levels are expressed as the US National Glycohemoglobin Standardization Program (NGSP) format level (%) [14].
Anthropometry measurement
Anthropometric measurements were performed with each participant wearing indoor clothing and without shoes. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Systolic blood pressure (BP) and diastolic BP were measured on the right arm in the sitting position with an automated sphygmomanometer after a 5-min rest.
Statistical analyses
Statistical analyses were conducted using SPSS Statistics 19.0 (IBM SPSS Inc., Chicago, IL, USA). Continuous data are expressed as median with first-third quartiles or interquartile range (IQR), and categorical variables are reported as frequencies and percentages. Univariate analyses were done using the Chi-square, Fisher’s Exact test, Mann–Whitney U test, or Spearman’s rank correlation coefficient, as appropriate. The Jonckheere–Terpstra trend test was used for ordered differences of serum ucOC level among aged-specific groups. One-way analysis of variance with the Games–Howell procedure was used for post hoc analysis of pairwise comparisons in serum ucOC level between age-specific groups. Variables with P value < 0.05 in univariate analysis were evaluated using stepwise multiple linear regression analysis with forward selection to identify variables significantly associated with serum ucOC level as a continuous variable. In general, all statistical tests were two-sided and the significance level was chosen as P value < 0.05.
Results
Clinical and lifestyle characteristic
Table 1 shows the clinical and lifestyle characteristics of the 3,658 residents who participated in the study. The medians of many of the parameters and the percentages of smokers and drinkers were significantly higher for men than for women. The FPG and HOMA-IR levels were significantly higher for men than for women, but there was no significant difference in the HbA1c levels of men and women. The percentage of men with HbA1c of 6.5 % or more (128 of 1,373, 9.3 %) was significantly higher than that of the women with HbA1c of 6.5 % or more (99 of 2,285, 4.3 %) (P < 0.0001). According to the self-administered questionnaire, 1,618 of 2,285 women (70.8 %) were postmenopausal, including 1,484 who were aged ≥50 (88.9 %). Very few (n = 13) reported a history of fractures.
Serum ucOC level
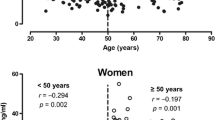
The median serum ucOC level (IQR) (ng/mL) of the women [4.65 (1.9)] was significantly higher than that of the men [3.04 (1.0)] (P = 0.0021). Figure 1 shows age-specific serum ucOC levels classified by sex. The age-specific median serum ucOC levels (IQR) (ng/mL) of the men decreased significantly with age: 40–44 years [3.3 (1.2)], 45–49 years [3.3 (1.3)], 50–54 years [3.0 (1.1)], 55–59 years [2.8 (1.0)], 60–64 years [2.9 (0.9)], and 65–69 years [3.0 (1.2)] (P ≤ 0.0001 for trend). The age-specific median serum ucOC levels (IQR) (ng/mL) of the women increased significantly with age: 40–44 years [2.9 (1.2)], 45–49 years [3.3 (1.4)], 50–54 years [4.8 (2.2)], 55–59 years [5.6 (2.1)], 60–64 years [5.1 (1.9)], and 65–69 years [5.3 (1.9)] (P ≤ 0.0001 for trend). The serum ucOC level of 40–44 year men was significantly higher than groups of men aged 50–54, 55–59, 60–64, and 65–69 (P = 0.006, P = 0.001, P ≤ 0.0001, and P = 0.014, respectively). The level of 45–49 year men was significantly higher than groups of men aged 50–54, 55–59, and 60–64 (P = 0.032, P = 0.009, and P = 0.007, respectively). The serum ucOC level of 40–44 year women was significantly lower than groups of women aged 45–49, 50–54, 55–59, 60–64, and 65–69 (P = 0.003, P ≤ 0.001, P ≤ 0.0001, P ≤ 0.001, and P ≤ 0.001, respectively). The level of 45–49 year women was significantly lower than groups of women aged 50–54, 55–59, 60–64, and 65–69 (all P ≤ 0.0001). The median serum ucOC level of the women aged 40–49 was similar to that of the men, in contrast with the level of the postmenopausal women aged ≥50, which was markedly increased. The median serum ucOC level of the women aged ≥50 was high, with the levels varying markedly within the other age groups (Table 2).

Age-specific serum undercarboxylated osteocalcin (ucOC) level, classified by sex. The boxes are shown as median [first-quartile (Q1), third-quartile (Q3)] due to the skewed distribution. The bottom and top of the box are the Q1 and Q3, and the band near the middle of the box is the median. The ends of the whiskers represent the 2nd percentile and the 98th percentile. The age-specific serum ucOC levels of the men decreased significantly with age (P ≤ 0.0001 for trend), whereas those of the women increased significantly with age (P ≤ 0.0001 for trend). The serum ucOC level of 40–44 year men (*) was significantly higher than groups of men aged 50–54, 55–59, 60–64, and 65–69 (P = 0.006, P = 0.001, P ≤ 0.0001, and P = 0.014, respectively). The level of 45–49 year men (#) was significantly higher than groups of men aged 50–54, 55–59, and 60–64 (P = 0.032, P = 0.009, and P = 0.007, respectively). The serum ucOC level of 40–44 year women (*) was significantly lower than groups of women aged 45–49, 50–54, 55–59, 60–64, and 65–69 (P = 0.003, P ≤ 0.001, P ≤ 0.0001, P ≤ 0.001, and P ≤ 0.001, respectively). The level of 45–49 year women (#) was significantly lower than groups of women aged 50–54, 55–59, 60–64, and 65–69 (all P ≤ 0.0001)
Relationship between serum ucOC level and clinical and dietary factors
Age (r = 0.179) and systolic and diastolic BPs (r = 0.072 and 0.067) had significant, positive correlations with the serum ucOC level of the women, but not for the men. The FPG (r = −0.146 and −0.079) and HbA1c (r = −0.142 and −0.069) levels had significant, negative correlations with the serum ucOC level of both for men and women.
Factors contributing to serum ucOC level
Factors possibly related to the serum ucOC level were evaluated by multivariate analysis (Tables 3, 4). From the FFQ, we chose foods and dinks rich in vitamin K (Nattô, Miso soup, Margarine, Green and yellow leaf vegetables, cheese, butter, and yogurt) to analyze their relationship with the serum ucOC level. Daily intake of Nattô or yogurt and HbA1c level were significant negative factors both for the men and women, suggesting that vitamin K intake and glucose metabolism cause the serum ucOC level of women to decrease. The percentages of the men and women who eat nattô everyday were 11.1 % and 13.1 %, respectively. The percentages of the men and women who eat yogurt everyday were 10.7 % and 21.3 %, respectively.
Discussion
To the best of our knowledge, this is the first large-scale, cross-sectional, population study to focus on serum ucOC level as a marker indicating vitamin K deficiency. The age-specific analysis of serum ucOC level revealed a difference between men and women. The influence of age on the serum ucOC level of women, especially those aged ≥50, was predictable as most of them were post-menopause.
It has been suggested that circulating OC fragments are generated by proteolysis in the circulation or during sample processing and storage [15]. Unfortunately, we have no information on overestimation of OC fragments by the electro-CLIA kit used in the present study. This assay kit is based on the same monoclonal undercarboxylated OC antibodies (OC 4-5 and OC G3) as those of a commercially available kit for measuring ucOC level (Takara Bio Inc. Otsu, Japan). Gundberg et al. [16] reported that this antibody might overestimate the quantity of ucOC fragments, and that it would be not known if the CLIA similarly does or does not overestimate ucOC. However, the Takara kit assay is specific for either carboxylated or undercarboxylated OC, and these values must be normalized to total intact OC in the sample.
Increasing ucOC concentrations can be related to either increased production of the carboxylation substrate OC, which leads to higher ucOC concentration in the case of unchanged carboxylation capacity, or to reduced carboxylation capacity. Therefore, the ratio of ucOC to total intact osteocalcin (ucOC/intact OC) seems to be a more accurate measure of carboxylation status, as previously reported [17]. However, Vergnaud et al. [7] reported that serum ucOC, but not total OC, was associated with the risk of hip fracture. We believe that measurement of ucOC can, only to a certain extent, evaluate the carboxylation status.
Large geographic differences in serum vitamin K level have been demonstrated between Japan and Europe [18]. Regarding vitamin K-rich food intake, the important findings of this study are that daily consumption of nattô and yogurt leads to a low serum ucOC level, but that of green and yellow leaf vegetables, margarine, or foods, such as cheese and butter, does not. Both nattô and yogurt are produced by bacterial fermentation and are rich in vitamin K. Although there is no difference in yogurt consumption in Japan, Nattô consumption is higher in the northern and the central Japan than in the west and south, and its consumption in Kyushu, in the far southwest, is comparatively low. The intake of vitamin K has been reported to be low, and the incidence of hip fractures is noticeably high in northern Kyushu [19], where fewer people regularly eat nattô. The area studied is a suburb of Fukuoka City in the northwestern Kyushu. Nattô is unappetizing to some people because of its powerful smell, strong flavor, and slimy texture; thus, a vitamin K2 preparation would be a viable substitute. Vitamin K2 treatment has been reported to be effective for the prevention of fractures in patients with osteoporosis [20].
Tsugawa et al. [17] measured the circulating concentrations of phylloquinone (K1), and menaquinone 4 (MK-4) and 7 (MK-7) in women of Nagano prefecture, near Tokyo, and determined if each form of vitamin K is significantly associated with bone metabolism. Nagano prefecture is located in the middle of the main island (Honshu) of Japan, whereas the area of our study is a town in the northwestern part of Kyushu. The fact of the studied area being much different from that of Tsugawa et al. may have had an impact on the results, but, for the relationship between the intake of vitamin K (Nattô) and the incidence of hip fractures, we believe that the studied area is of clinical significance.
Reports of the association between age and serum ucOC level have been inconsistent. Sokoll et al. [8] reported ucOC concentrations decreasing with age in men and women, while other reports have shown no difference by the age of men and women [21]. Other studies have shown ucOC concentrations increasing with the age of women [17, 22]. Osteoblastic activity is age dependent, and osteocalcin synthesis changes with age [23]. Similar to the present study, ucOC increased with the age of women but decreased with the age of men, which could be interpreted as an association of ucOC with estrogen [24]. Our findings showed an especially high serum ucOC level for women aged ≥50, 88.9 % of whom were postmenopausal. The underlying mechanism of osteoporosis is an imbalance between bone resorption and bone formation. In normal bone, there is constant matrix remodeling; up to 10 % of all bone mass may be undergoing remodeling at any point in time. Hormonal factors strongly determine the rate of bone resorption; the post-menopause lack of estrogen increases bone resorption as well as decreasing the deposition of new bone that normally takes place in weight-bearing bones [3].
Similar to another study [25], the serum ucOC levels of the older men in this study were low because of impaired glucose tolerance. Numerous epidemiologic studies have revealed that age, male sex, and obesity are risk factors for diabetes and insulin resistance. Impaired glucose tolerance affects the insulin receptors of osteoblasts and decreases OC production [26]. Obesity, insulin resistance, and diabetes are related disorders of energy metabolism. Lee et al. [27] demonstrated in mice that bone regulates the insulin/glucose axis and energy metabolism, providing a new framework for approaching common disorders of bioenergetics. Osteoblast can alter energy metabolism. The rat osteotesticular phosphatase (OST-PTPase) gene, Esp, encodes the osteoblast protein tyrosine phosphatase OST-PTP. The inactivation of Esp expression in bone is relevant to increased osteocalcin metabolic bioactivity, which leads to numerous metabolically desirable characteristics: increased proliferation of pancreatic beta cells, increased insulin secretion, lower blood glucose, increased insulin sensitivity, decreased visceral fat, and increased energy expenditure. Related to the mechanism by which osteoblasts promote bone resorption, impaired glucose tolerance weakens bones, causing osteoporosis in a vitamin K-independent manner. Moreover, new insights in the molecular pathways of bone remodeling have clarified the mechanisms responsible for skeletal fragility in several forms of secondary osteoporosis, such as that occurring in type 2 diabetes [28]. The current study demonstrated that daily consumption of nattô and yogurt leads to a low serum ucOC level. Both nattô and yogurt are produced by bacterial fermentation and are rich in vitamin K, leading to an association with glucose metabolism.
A limitation of this study is that it was cross-sectional and included only Japanese participants. The causality of our findings cannot be inferred. Both ucOC and glucose metabolism could be related to a common underlying factor, and the association could be coincidental. We have no data on other bone turnover markers such as serum procollagen type 1 amino-terminal propeptide, urinary/serum collagen type 1 cross-linked C-telopeptide, or vitamin D level. Also, this study did not include BMD measurement. However, the findings from this study of over 3,000 participants of both sexes aged ≥40 would seem to be of general interest.
In conclusion, this study indicates that the serum ucOC decreases with age in men, increases postmenopausally in women, and correlates inversely with dietary consumption of certain foods and with fasting glucose and HbA1c level.
References
NIH Consensus Development Panel on Osteoporosis Prevention Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA 285, 785–795 (2001)
H. Hagino, K. Sakamoto, A. Harada, T. Nakamura, Y. Mutoh, S. Mori et al., Committee on osteoporosis of the Japanese Orthopedic Association. Nationwide one-decade survey of hip fractures in Japan. J. Orthop. Sci. 15, 737–745 (2010)
L.G. Raisz, Pathogenesis of osteoporosis: concepts, conflicts, and prospects. J. Clin. Invest. 115, 3318–3325 (2005)
D. Bliuc, N.D. Nguyen, V.E. Milch, T.V. Nguyen, J.A. Eisman, J.R. Center, Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA 301, 513–521 (2009)
Y. Koshihara, K. Hoshi, Vitamin K2 enhances osteocalcin accumulation in the extracellular matrix of human osteoblasts in vitro. J. Bone Miner. Res. 12, 431–438 (1997)
S.L. Booth, K.L. Tucker, H. Chen, M.T. Hannan, D.R. Gagnon, L.A. Cupples et al., Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density in elderly men and women. Am. J. Clin. Nutr. 71, 1201–1208 (2000)
P. Vergnaud, P. Garnero, P.J. Meunier, G. Bréart, K. Kamihagi, P.D. Delmas, Undercarboxylated osteocalcin measured with a specific immunoassay predicts hip fracture in elderly women: the EPIDOS study. J. Clin. Endocrinol. Metab. 82, 719–724 (1997)
L.J. Sokoll, S.L. Booth, M.E. O’Brien, K.W. Davidson, K.I. Tsaioun, J.A. Sadowski, Changes in serum osteocalcin, plasma phylloquinone, and urinary gamma-carboxyglutamic acid in response to altered intakes of dietary phylloquinone in human subjects. Am. J. Clin. Nutr. 65, 779–784 (1997)
B.H. Arjmandi, M.J. Getlinger, N.V. Goyal, L. Alekel, C.M. Hasler, S. Juma et al., Role of soy protein with normal or reduced isoflavone content in reversing bone loss induced by ovarian hormone deficiency in rats. Am. J. Clin. Nutr. 68, 1358S–1363S (1998)
N. Furusyo, T. Koga, M. Ai, S. Otokozawa, T. Kohzuma, H. Ikezaki et al., Utility of glycated albumin for the diagnosis of diabetes mellitus in a Japanese population study: results from the Kyushu and Okinawa Population Study (KOPS). Diabetologia 54, 3028–3036 (2011)
N. Furusyo, T. Koga, M. Ai, S. Otokozawa, T. Kohzuma, H. Ikezaki, et al. Plasma glycated albumin level and atherosclerosis: results from the Kyushu and Okinawa Population Study (KOPS). Int. J. Cardiol. (2012) (doi: 10.1016/j.ijcard.2012.05.045
Y. Tokudome, C. Goto, N. Imaeda, T. Hasegawa, R. Kato, K. Hirose et al., Relative validity of a short food frequency questionnaire for assessing nutrient intake versus three-day weighed diet records in middle-aged Japanese. J. Epidemiol. 15, 135–145 (2005)
J. Nishimura, N. Arai, J. Tohmatsu. Measurement of serum undercarboxylated osteocalcin by ECLIA with the “Picolumi ucOC” kit. Clin. Calcium. 17, 1702–1708 (2007) (Japanese)
A. Geistanger, S. Arends, C. Berding, T. Hoshino, J.O. Jeppsson, R. Little et al., IFCC Working Group on Standardization of Hemoglobin A1c. Statistical methods for monitoring the relationship between the IFCC reference measurement procedure for hemoglobin A1c and the designated comparison methods in the United States, Japan, and Sweden. Clin. Chem. 54, 1379–1385 (2008)
P. Garnero, M. Grimaux, P. Seguin, P.D. Delmas, Characterization of immunoreactive forms of human osteocalcin generated in vivo and in vitro. J. Bone Miner. Res. 9, 255–264 (1994)
C.M. Gundberg, S.D. Nieman, S. Abrams, H. Rosen, Vitamin K status and bone health: an analysis of methods for determination of undercarboxylated osteocalcin. J. Clin. Endocrinol. Metab. 83, 3258–3266 (1998)
N. Tsugawa, M. Shiraki, Y. Suhara, M. Kamao, K. Tanaka, T. Okano, Vitamin K status of healthy Japanese women: age-related vitamin K requirement for gamma-carboxylation of osteocalcin. Am. J. Clin. Nutr. 83, 380–386 (2006)
M. Kaneki, S.J. Hodges, T. Hosoi, S. Fujiwara, A. Lyons, S.J. Crean et al., Japanese fermented soybean food as the major determinant of the large geographic difference in circulating levels of vitamin K2: possible implications for hip-fracture risk. Nutrition 17, 315–321 (2001)
Y. Yaegashi, T. Onoda, K. Tanno, T. Kuribayashi, K. Sakata, H. Orimo, Association of hip fracture incidence and intake of calcium, magnesium, vitamin D, and vitamin K. Eur. J. Epidemiol. 23, 219–225 (2008)
M. Shiraki, Y. Shiraki, C. Aoki, M. Miura, Vitamin K2 (menatetrenone) effectively prevents fractures and sustains lumbar bone mineral density in osteoporosis. J. Bone Miner. Res. 15, 515–521 (2000)
N.M. McKeown, P.F. Jacques, C.M. Gundberg, J.W. Peterson, K.L. Tucker, D.P. Kiel et al., Dietary and nondietary determinants of vitamin K biochemical measures in men and women. J. Nutr. 132, 1329–1334 (2002)
S.R. Beavan, A. Prentice, D.M. Stirling, B. Dibba, L. Yan, D.J. Harrington et al., Ethnic differences in osteocalcin gamma-carboxylation, plasma phylloquinone (vitamin K1) and apolipoprotein E genotype. Eur. J. Clin. Nutr. 59, 72–81 (2005)
P.D. Delmas, D. Stenner, H.W. Wahner, K.G. Mann, B.L. Riggs, Increase in serum bone gamma-carboxyglutamic acid protein with aging in women. Implications for the mechanism of age-related bone loss. J. Clin. Invest. 71, 1316–1321 (1983)
T. Yasui, H. Uemura, J. Tomita, Y. Miyatani, M. Yamada, M. Miura et al., Association of serum undercarboxylated osteocalcin with serum estradiol in pre-, peri- and early post-menopausal women. J. Endocrinol. Invest. 29, 913–918 (2006)
M. Iki, J. Tamaki, Y. Fujita, K. Kouda, A. Yura, E. Kadowaki et al., Serum undercarboxylated osteocalcin levels are inversely associated with glycemic status and insulin resistance in an elderly Japanese male population: Fujiwara-kyo Osteoporosis Risk in Men (FORMEN) study. Osteoporos. Int. 23, 761–770 (2012)
M. Ferron, J. Wei, T. Yoshizawa, A. Del Fattore, R.A. DePinho, A. Teti et al., Insulin signaling in osteoblasts integrates bone remodeling and energy metabolism. Cell 142, 296–308 (2010)
N.K. Lee, H. Sowa, E. Hinoi, M. Ferron, J.D. Ahn, C. Confavreux, R. Dacquin, P.J. Mee, M.D. McKee, D.Y. Jung, Z. Zhang, J.K. Kim, F. Mauvais-Jarvis, P. Ducy, G. Karsenty, Endocrine regulation of energy metabolism by the skeleton. Cell 130, 456–469 (2007)
G. Mazziotti, J. Bilezikian, E. Canalis, D. Cocchi, A. Giustina, New understanding and treatments for osteoporosis. Endocrine 41, 58–69 (2012)
Acknowledgments
The authors thank H. Ohnishi, H. Mukae, M. Unno, K. Eiraku, F. Mistumotro, and S. Hiramine of our department for helping with the study. The authors also thank Miss S. Nagata, Mr. K. Tozawa, and Miss K. Nakao for their helpful assistance. The study was supported by the Japan Multi-institutional Collaborative Cohort Study (J-MICC Study), Scientific Support Programs for Cancer Research Grant-in-Aid for Scientific Research on Innovative Areas (no. 221 S001), and a Grant-in-Aid for Comprehensive Research of the 21st Century COE Program from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Furusyo, N., Ihara, T., Hayashi, T. et al. The serum undercarboxylated osteocalcin level and the diet of a Japanese population: results from the Kyushu and Okinawa Population Study (KOPS). Endocrine 43, 635–642 (2013). https://doi.org/10.1007/s12020-012-9803-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-012-9803-z