
Abstract
Introduction and hypothesis
The aim of this study was to compare outcomes after uterosacral ligament suspension (USLS) or sacrocolpopexy for symptomatic stage IV apical pelvic organ prolapse (POP) and evaluate predictors of prolapse recurrence.
Methods
The medical records of patients managed surgically for stage IV apical POP from January 2002 to June 2012 were reviewed. A follow-up survey was sent to these patients. The primary outcome, prolapse recurrence, was defined as recurrence of prolapse symptoms measured by validated questionnaire or surgical retreatment. Survival time free of prolapse recurrence was estimated using the Kaplan–Meier method, and Cox proportional hazards models evaluated factors for an association with recurrence.
Results
Of 2633 women treated for POP, 399 (15.2%) had stage IV apical prolapse and were managed with either USLS (n = 355) or sacrocolpopexy (n = 44). Those managed with USLS were significantly older (p < 0.001) and less likely to have a prior hysterectomy (39.7 vs 86.4%; p < 0.001) or prior apical prolapse repair (8.2 38.6%; p < 0.001). Median follow-up was 4.3 years [interquartile range (IQR) 1.1–7.7]. Survival free of recurrence was similar between USLS and sacrocolpopexy (p = 0.43), with 5-year rates of 88.7 and 97.6%, respectively. Younger age [adjusted hazard ratio (aHR) 1.55, 95% confidence interval (CI) 1.12–2.13; p = 0.008] and prior hysterectomy (aHR 2.8, 95% CI 1.39–5.64; p = 0.004) were associated with the risk of prolapse recurrence, whereas type of surgery approached statistical significance (aHR 2.76, 95% CI 0.80–9.60; p = 0.11).
Conclusions
Younger age and history of prior hysterectomy were associated with an increased risk of recurrent prolapse symptoms. Notably, excellent survival free of prolapse recurrence were obtained with both surgical techniques.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pelvic organ prolapse (POP) is a prevalent issue in adult women that can have a large impact on quality of life (QoL), leading to discomfort, decreased energy, and increased social isolation [1]. Notably, the prevalence of prolapse increases with advancing age, and it is estimated that the lifetime risk of a woman undergoing surgery for bothersome prolapse is as high as 13% [2]. Given the present age distribution in the United States, the number of women seeking treatment for this issue in the future will continue to increase [2, 3]. Recurrence of prolapse after surgical repair is not uncommon, with as many as 17% of patients undergoing a repeat prolapse treatment [4,5,6,7]. However, conflicting data regarding risk factors for prolapse recurrence after a native tissue vaginal repair exist [6,7,8,9,10,11]. In fact, a recent systematic review identified preoperative stage as the only consistently reported risk factor for recurrence after prolapse surgery [12]. Additionally, while there are numerous studies evaluating the outcomes of various apical prolapse surgeries [13, 14], given the purported differences in success rates and risks, the optimal management of apical prolapse (native tissue vs sacrocolpopexy) remains unclear. Of note, these studies typically treat high-grade prolapse as a combined category, with stage-specific outcomes being uncommon [15]. This is an important consideration, as the stage of preoperative prolapse may impact surgical outcomes of both transvaginal repair and sacrocolpopexy [8, 12]. Understanding the predictors of prolapse recurrence after surgery, as well as stage-specific surgical outcomes, may better inform patient-specific surgical decision making, preoperative counseling, and—in turn—surgical outcomes. Thus, we sought to compare outcomes after uterosacral ligament suspension (USLS) or sacrocolpopexy for symptomatic stage IV apical POP, and evaluate predictors of prolapse recurrence.
Materials and methods
Following Institutional Review Board approval, we identified all women at least 21 years of age who underwent surgery for symptomatic POP at Mayo Clinic (Rochester, MN, USA) from 1 January 2002 through 30 June 2012. After exclusion of patients who did not authorize the use of their medical records for research, we identified patients with stage IV apical POP using the simplified Pelvic Organ Prolapse Quantification (POP-Q) system definition [16], which is a validated modification from the original POP-Q [17]. The simplified POP-Q is similar to the original except it measures four points only—anterior, posterior, apical, and cervix—instead of nine, which makes it more clinically accessible [16, 17]. In both versions, stage IV prolapse represents complete vaginal vault or uterine eversion. [16, 17].
Chart review (including preoperative consultation, operative reports, hospital summaries, follow-up office visits in gynecology or urology, and phone conversations) of patients with stage IV POP and the leading edge being the apical compartment was performed via electronic medical record review to identify pertinent clinical comorbidities, details of operative intervention, and documented follow-up. Patients were included in the study if they had undergone native tissue vaginal repair (at our institution, this is performed by USLS with Mayo–McMcall culdoplasty [18]) or sacrocolpopexy (abdominal or robotic). No patient during the study timeframe underwent laparoscopic sacrocolpopexy. Patients found to have a pouch of Douglas hernia were subsequently excluded [19]. Those known to be alive as of December 2012 were mailed a survey at that time containing validated questionnaires to evaluate prolapse-related urinary, bowel, and sexual symptoms. Surveys were the Pelvic Floor Distress Inventory-20 (PFDI-20) and the International Consensus on Incontinence Questionnaire Short Form (ICIQ-SF) [20,21,22]. A mailed reminder was sent 4 weeks after the initial survey to all recipients who had not returned a survey, followed by a phone call including a shorter form of the survey to increase the response rate.
The primary outcome—prolapse recurrence—was defined as the presence of symptomatic prolapse as assessed by answers to validated questions on the survey or interval surgical treatment for symptomatic prolapse recurrence [20,21,22]. A patient was considered to have symptomatic prolapse if she answered “Yes” to either of the following questions: “Do you usually have a sensation of bulging or protrusion from the vaginal area?” “Do you usually have a bulge or something falling out that you can see or feel in the vaginal area?” [20,21,22]. These questions discriminate between patients with and without prolapse [20,21,22]. Patient satisfaction was evaluated by response to the question: “How satisfied or dissatisfied are you with the result of your surgery for treatment of your pelvic floor condition?” with responses measured via a 5-point Likert scale, with options ranging from “completely satisfied” to “completely dissatisfied.” Patients reporting being completely satisfied or somewhat satisfied were considered satisfied in the analyses. Interval surgery was confirmed by review of the electronic medical record and patient questionnaire responses.
Continuous variables were summarized with mean and standard deviation (SD) or median and interquartile range (IQR); categorical variables are summarized by number count and percentage. Comparison of clinical and demographic patient characteristics between surgical approaches, and likewise between survey participants and nonparticipants, was performed using the chi-square or Fisher’s exact test for categorical variables and the Wilcoxon rank-sum test for continuous variables. Survival free of prolapse recurrence was estimated using the Kaplan–Meier method. For patients with prolapse recurrence, time to failure was calculated from the date of surgery to the earliest date of either symptomatic prolapse as reported on the survey or date of surgical retreatment. For patients without prolapse recurrence, duration of follow-up was censored at the latter of either the date of survey completion or date of last clinic visit. Patient characteristics were evaluated via univariate analyses for their association with prolapse recurrence based on fitting Cox proportional hazards models summarized using hazard ratios (HRs) and 95% confidence intervals (CIs). Two multivariate Cox models were fit using all the patients in the cohort, with Analysis A using time since surgery as the time scale and Analysis B using age as the time scale to allow for complete age adjustment. An additional Cox model (Analysis C) was fit to assess the association between surgical approach and prolapse recurrence using propensity score (PS)-matched pairs after establishing acceptable covariate balance between the two surgical approaches among matched pairs. PS was defined as the estimated probability of a patient having a sacrocolpopexy (vs USLS) given a set of measured baseline patient covariates and was derived from a multivariate logistic regression model that included the following covariates at the time of the surgery: age, diabetes, connective tissue disorder, menopausal status, prior hysterectomy, and prior apical prolapse repair. For each patient with a sacrocolpopexy, a patient was randomly selected from the potential pool of patients with a USLS who met the matching calipers using a greedy matching algorithm that matched on: (1) the logit of the PS values within 0.2 of the SD of the logit, and (2) surgery date within 2 years. The covariate balance between patients in the two surgical approaches was evaluated by calculating standardized differences for each covariate in both the original full cohort and the PS-matched cohort. Statistical analyses were performed using SAS version 9.3 (SAS Institute, Inc., Cary, NC, USA). All statistical analyses were two sided, and P values <0.05 were considered statistically significant.
Results
Over the timeframe of the study 2633 women underwent surgery for POP—including 399 with stage IV prolapse with the most dependent compartment being the apical compartment—who were managed with either USLS (n = 355) or sacrocolpopexy (n = 44). No patient was treated with sacrospinous ligament fixation or transvaginal mesh placement. Clinical and demographic patient characteristics compared between those treated with USLS vs sacrocolpopexy for stage IV apical prolapse are shown in Table 1. Patients treated with sacrocolpopexy were younger (p < 0.001), less likely to be postmenopausal (p = 0.03), and more likely to have a prior hysterectomy (p < 0.001) as well as a prior apical prolapse repair (p < 0.001). There were no significant differences in body mass index (BMI) (p = 0.92) or smoking status (p = 0.66) between treatment groups.
At the time of the survey mailing, 309 of the 355 patients who underwent USLS were alive; 170 (55%) completed the survey (123 returned the full survey, and 46 responded to the shorter survey over the phone). Likewise, 40 of the 44 patients who underwent sacrocolpopexy were alive, and 19 (47.5%) completed the survey (17 returned the full survey, and two responded to the shorter survey over the phone). Survey participants were slightly younger than nonparticipants (mean age 70.3 vs. 68.7 years, p = 0.047). No differences in BMI, prior hysterectomy or hernia repair, menopausal status, or smoking status were observed between participants and nonparticipants (data not shown). Overall, 324 of the 399 patients (81.2%) either completed the survey (mailed or phone follow-up) or had follow-up at Mayo Clinic beyond their initial postoperative evaluation.
During the follow-up period, 18 of the 355 patients treated with USLS had a symptomatic prolapse recurrence by questionnaire criteria, and an additional 20 patients underwent a repeat prolapse surgery. Of those who underwent repeat surgery, all had a component of apical recurrence, which was addressed at the time of reoperation. Of these, nine were stage II, eight stage III, and three stage IV. Additionally, eight patients had recurrent anterior prolapse (stage ≥ II) and nine had recurrent posterior prolapse (stage ≥II). Among the 44 patients treated with sacrocolpopexy, there was one reoperation for posterior vaginal wall prolapse and two who met the questionnaire criteria for failure. Among those without prolapse recurrence, median length of follow-up after surgery was 4.3 years (IQR 1.1–7.7). Specifically, median length of follow-up for those without prolapse recurrence was 4.6 years (IQR 1.2–7.8) for the USLS and 3.7 years (IQR 1.1–7.1) for the sacrocolpopexy group.
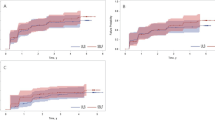
Survival free of prolapse recurrence was not significantly different between groups (p = 0.43), with 5-year rates of 88.7% and 97.6%, for the uterosacral and sacrocolpopexy cohorts, respectively (Fig. 1). Likewise, there was no significant difference in patient satisfaction among questionnaire participants between groups (87% (147/169) USLS patients vs 84.2% (16/19) sacrocolpopexy patients; p = 0.72).

Survival free of prolapse recurrence following surgery for those treated with uterosacral ligament suspension versus those treated with sacrocolpopexy
Univariate analysis revealed that younger age or premenopausal status at the time of surgery and prior hysterectomy were the only variables associated with an increased risk of prolapse recurrence (Table 2). After adjusting for age and prior hysterectomy in a multivariate Cox proportional hazards model, the association between type of surgery and prolapse recurrence approached statistical significance in models either using time since surgery as the time scale [adjusted hazard ratio (aHR) 3.18, 95% CI 0.94-10.80, p = 0.06) or age as the time scale (aHR 2.76, 95% CI 0.80-9.60, p = 0.11) Furthermore, the association was of similar magnitude based on a cohort of 38 PS-matched pairs (HR 2.96, 95% CI 0.80-10.96, p = 0.10) (Table 3). The standardized differences of covariates used to derive the PS was improved with all standardized differences among PS-matched pairs < 0.15 (Table 4).
Discussion
In a large, retrospective cohort study of women who had surgical correction of stage IV prolapse with the apical compartment as the leading edge, survival free of prolapse recurrence was not significantly different between the USLS and sacrocolpopexy cohorts, with 5-year survival free of prolapse recurrence rates of 88.7% and 97.6%, respectively. However, younger age at surgery and prior hysterectomy were associated with an increased risk of recurrent symptoms. After adjusting for these factors, the association between type of surgery and survival free of prolapse recurrence approached but did not reach statistical significance. Recognition of these factors can aid in preoperative patient counseling and setting appropriate expectations following surgery.
There are conflicting data regarding risk factors for POP recurrence after surgical intervention; with five articles identifying 29 potential factors [6,7,8,9,10,11,12]. Only preoperative stage and patient age were consistently associated with recurrence in at least two articles [6,7,8,9,10,11,12]. Heterogeneity of these findings is likely due to differences in study populations and definitions of recurrence. Whereas we focused on a homogenous cohort of stage IV apical prolapse, others included patients with prolapse ranging from stage III to stage IV prolapse [6,7,8,9,10,11,12]. This is an important distinction, as it is likely that patients with the leading edge at +1.5 cm (and hence stage III) may have different natural histories and outcomes following surgical correction compared with women with complete eversion. In addition, we used a composite outcome for success, including symptom-based measures and surgical failure [20].
Others have reported an association between patient age and risk of prolapse recurrence [9,10,11]. Whiteside et al. reported a higher risk of anatomic recurrence among patients < 60 years [odds ratio (OR) 3.2, 95% CI 1.6-6.4, p = 0.001) at 1 year following vaginal prolapse repairs [11], Likewise, in a study of 134 patients evaluated 5 years after transvaginal prolapse repair, Diez–Itza et al. found an anatomic recurrence rate of 31% and that women < 60 years were at increased risk for both anatomic and functional recurrences [9].
Several hypothesized mechanisms may place younger patients at a higher risk of postoperative prolapse recurrence. First, younger patients may have weaker underlying connective tissue [23] or more severe pelvic floor trauma during deliveries [24], which contributes not only to their initial presentation with symptomatic prolapse but also their risk of recurrence. Second, younger patients may have a longer timeframe for follow-up and thus a longer time for symptom recurrence. Lastly, while not evaluated in this study, such patients may be more physically active, which could hypothetically impact surgical outcomes.
Although we identified history of prior hysterectomy as a risk factor for prolapse recurrence, two prior series found no association with the risk of postoperative prolapse recurrence [11, 25]. For instance, Salvatore et al. found only preoperative stage (≥ stage III) to be a risk factor for recurrence in an analysis of 360 women undergoing transvaginal prolapse surgery with a mean follow-up of 26 months [25]. However, both studies included women with stage III or IV prolapse at baseline and defined recurrence based on strict anatomic criteria (stage ≥2) that have limited correlation with patient perception of improvement or surgical success [20].
There are several reasons why hysterectomy may predispose to POP recurrence. Our group and others have shown that women who have concomitant prolapse at the time of the index hysterectomy, regardless of compartment, are at increased risk of prolapse recurrence [26,27,28]. In addition, it is likely that surgical technique (in particular, the use or lack thereof of prophylactic apical suspension) may place women at higher risk of prolapse recurrence following hysterectomy. In a large, population-based study from Sweden, vaginal hysterectomy was shown to increase the risk of prolapse in the first 5 years following the index surgery by sixfold [27]. Conversely, two other population-based cohorts found no association between route of hysterectomy and risk of prolapse recurrence [26, 28]. In fact, in a group of women with no baseline prolapse symptoms, the cumulative risk of requiring a subsequent prolapse repair after hysterectomy was 5% at the 30-year follow-up [26]. This increased to 12.2% in women with baseline prolapse undergoing no additional prolapse repairs [26]. It is important to understand that in that cohort, most participants underwent a prophylactic apical suspension at the time of hysterectomy [26].
The optimal surgical approach for symptomatic apical prolapse is widely debated. While several reports note higher anatomical success rates with a sacrocolpopexy compared with native tissue transvaginal repair, sacrocolpopexy is also associated with higher complication rates [13]. In a randomized trial evaluating uterosacral vault suspension and sacrocolpopexy for apical defects in 124 women, Rondini et al. found that anatomic (POP-Q point C of stage < 2) success rates were higher at 1-year follow-up for abdominal sacrocolpopexy than USLS (100 vs 82.5%; p = 0.0033) [29]. There was no difference in the degree of symptomatic improvement as measured by validated questionnaires [PFDI-20, Prolapse Quality of Life Questionnaire (P-QOL), Pelvic Organ Prolapse Urinary Incontinence Sexual Function Questionnaire (PISQ-12)] between groups [29]. In that study aggregate scores were used, with no subscores or individual prolapse-specific questions reported, which may favor detecting no difference. Additionally, a recent meta-analysis reported similar prolapse retreatment rates between the two approaches, though there were limited data available for analysis [14]. Similar to these findings, we did not identify a significant difference in prolapse-recurrence-free survival rates or patient satisfaction between USLS and sacrocolpopexy, though there was a trend toward higher reoperation rates among those treated with a vaginal approach (aHR 3.18 95% CI 0.94-10.80, p = 0.06), and this was consistent across the three analyses conducted. These findings may be secondary to differences in follow-up or insufficient power to detect a difference given the number of patients and events in the sacrocolpopexy cohort.
Strengths of our study include evaluation of a large homogenous cohort of women with stage IV prolapse who underwent native tissue and sacrocolpopexy correction of prolapse and had long-term, robust follow-up. Furthermore, secondary analysis using matching via propensity scoring was employed to evaluate our initial findings. Additionally, we used a composite endpoint (surgical retreatment or symptomatic recurrence) shown to be correlated with patient perception of improvement and success. This provides a useful clinical endpoint of symptomatic recurrences rather than strictly anatomic outcomes [20]. Additionally, all procedures were performed at a single institution, decreasing heterogeneity in the surgical approaches and follow-up.
Limitations of our study should be noted: During the study timeframe, a relatively small cohort meeting study inclusion criteria was managed with a sacrocolpopexy (n = 44), which may limit our ability to detect differences in outcomes between groups. Additionally, while we had a limited survey response, our composite outcome included follow-up for 81.2% of the cohort, and there were limited differences between respondents and nonrespondents. Furthermore, our study endpoint does not include anatomic criteria for failure, as we did not perform clinical examinations. Nevertheless, we used two questions that correlate with clinical exam findings and used the hard endpoint of reoperation for prolapse recurrence [20,21,22]. Lastly, our results represent a single institutional series with surgeons who completed fellowship training. Although this greatly improved our internal validity, it may limit generalizability of our findings.
Conclusions
Younger age and history of prior hysterectomy were associated with an increased risk of recurrent prolapse symptoms. Notably, excellent survival free of prolapse recurrence and patient satisfaction can be obtained with both USLS and sacrocolpopexy in patients with stage IV POP.
References
Fritel X, Varnoux N, Zins M, Breart G, Ringa V. Symptomatic pelvic organ prolapse at midlife, quality of life, and risk factors. Obstet Gynecol. 2009;113(3):609–16.
Wu JM, Matthews CA, Conover MM, Pate V, Jonsson FM. Lifetime risk of stress urinary incontinence or pelvic organ prolapse surgery. Obstet Gynecol. 2014;123(6):1201–6.
Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in U.S. women: 2010 to 2050. Obstet Gynecol. 2009;114(6):1278–83.
Gotthart PT, Aigmueller T, Lang PF, Ralph G, Bjelic-Radisic V, Tamussino K. Reoperation for pelvic organ prolapse within 10 years of primary surgery for prolapse. Int Urogynecol J. 2012;23(9):1221–4.
Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89(4):501–6.
Salvatore S, Siesto G, Serati M. Risk factors for recurrence of genital prolapse. Curr Opin Obstet Gynecol. 2010;22(5):420–4.
Denman MA, Gregory WT, Boyles SH, Smith V, Edwards SR, Clark AL. Reoperation 10 years after surgically managed pelvic organ prolapse and urinary incontinence. Am J Obstet Gynecol. 2008;198(5):555):e551–5.
Aslam MF, Osmundsen B, Edwards SR, Matthews C, Gregory WT. Preoperative Prolapse Stage as Predictor of Failure of Sacrocolpopexy. Female Pelvic Med Reconstr Surg. 2015.
Diez-Itza I, Aizpitarte I, Becerro A. Risk factors for the recurrence of pelvic organ prolapse after vaginal surgery: a review at 5 years after surgery. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(11):1317–24.
Nieminen K, Huhtala H, Heinonen PK. Anatomic and functional assessment and risk factors of recurrent prolapse after vaginal sacrospinous fixation. Acta Obstet Gynecol Scand. 2003;82(5):471–8.
Whiteside JL, Weber AM, Meyn LA, Walters MD. Risk factors for prolapse recurrence after vaginal repair. Am J Obstet Gynecol. 2004;191(5):1533–8.
Vergeldt TF, Weemhoff M, IntHout J, Kluivers KB. Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecol J. 2015;26(11):1559–73.
Maher C, Feiner B, Baessler K, Schmid C. Surgical management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2013;4:CD004014.
Siddiqui NY, Grimes CL, Casiano ER, et al. Mesh sacrocolpopexy compared with native tissue vaginal repair: a systematic review and meta-analysis. Obstet Gynecol. 2015;125(1):44–55.
Kolusari A, Yildizhan R, Adali E, et al. Short-term results of posterior intravaginal slingplasty in grade 4 uterine prolapse. Arch Gynecol Obstet. 2010;281(1):55–8.
Parekh M, Swift S, Lemos N, et al. Multicenter inter-examiner agreement trial for the validation of simplified POPQ system. Int Urogynecol J. 2011;22(6):645–50.
Bump RC, Mattiasson A, Bo K, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996;175(1):10–7.
Webb MJ, Aronson MP, Ferguson LK, Lee RA. Posthysterectomy vaginal vault prolapse: primary repair in 693 patients. Obstet Gynecol. 1998;92(2):281–5.
Klingele CJ, Bharucha AE, Fletcher JG, Gebhart JB, Riederer SG, Zinsmeister AR. Pelvic organ prolapse in defecatory disorders. Obstet Gynecol. 2005;106(2):315–20.
Barber MD, Brubaker L, Nygaard I, et al. Defining success after surgery for pelvic organ prolapse. Obstet Gynecol. 2009;114(3):600–9.
Barber MD, Kuchibhatla MN, Pieper CF, Bump RC. Psychometric evaluation of 2 comprehensive condition-specific quality of life instruments for women with pelvic floor disorders. Am J Obstet Gynecol. 2001;185(6):1388–95.
Barber MD, Spino C, Janz NK, et al. The minimum important differences for the urinary scales of the Pelvic Floor Distress Inventory and Pelvic Floor Impact Questionnaire. Am j obstet gynecol. 2009;200(5):580. e581-587
Connell KA, Guess MK, Chen H, Andikyan V, Bercik R, Taylor HS. HOXA11 Is critical for development and maintenance of uterosacral ligaments and deficient in pelvic prolapse. J Clin Invest. 2008;118(3):1050–5.
DeLancey JO, Morgan DM, Fenner DE, et al. Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol. 2007;109(2 Pt 1):295–302.
Salvatore S, Athanasiou S, Digesu GA, et al. Identification of risk factors for genital prolapse recurrence. Neurourol Urodyn. 2009;28(4):301–4.
Blandon RE, Bharucha AE, Melton LJ 3rd, et al. Incidence of pelvic floor repair after hysterectomy: A population-based cohort study. Am J Obstet Gynecol. 2007;197(6):664. e661-667
Altman D, Falconer C, Cnattingius S, Granath F. Pelvic organ prolapse surgery following hysterectomy on benign indications. Am J Obstet Gynecol. 2008;198(5):572. e571-576
Dallenbach P, Kaelin-Gambirasio I, Dubuisson JB, Boulvain M. Risk factors for pelvic organ prolapse repair after hysterectomy. Obstet Gynecol. 2007;110(3):625–32.
Rondini C, Braun H, Alvarez J, et al. High uterosacral vault suspension vs Sacrocolpopexy for treating apical defects: a randomized controlled trial with twelve months follow-up. Int Urogynecol J. 2015;26(8):1131–8.
Funding
Mayo Clinic Department of Obstetrics and Gynecology.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
BJL, SAE, AAM, ALW, MEM, DJR, CJK, JAO, ECT- none.
JBG- UpTo Date, Elsevier, Astora.
Author participation
BJL: Project development, Manuscript writing, Data collection.
SAE: Project development, Manuscript editing, Data collection.
AAM: Project development, Manuscript editing.
ALW: Project development, Manuscript editing, Statistical analysis.
MEM: Project development, Manuscript editing, Statistical analysis.
DJR: Project development, Manuscript editing.
JBG: Project development, Manuscript editing.
CJK: Project development, Manuscript editing.
JAO: Project development, Manuscript editing.
ECT: Project development, Manuscript editing.
Rights and permissions
About this article

Cite this article
Linder, B.J., El-Nashar, S.A., Mukwege, A.A. et al. Long-term outcomes and predictors of failure after surgery for stage IV apical pelvic organ prolapse. Int Urogynecol J 29, 803–810 (2018). https://doi.org/10.1007/s00192-017-3482-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-017-3482-5