
Abstract
Introduction and hypothesis
A presumed high failure rate of conventional procedures for prolapse has been part of the rationale for new surgical approaches. The aim of the present retrospective cohort study was to estimate the reoperation rate for prolapse within 10 years of primary surgery for prolapse.
Methods
We identified all patients who underwent primary surgery for prolapse at four large regional centers in Austria in 1997 and 1998. Hospital databases were searched to determine whether patients had been reoperated for prolapse through 2008.
Results
A total of 456 patients underwent a primary operation for prolapse in 1997 and 1998. The most common primary operation was vaginal hysterectomy with colporrhaphy (89 %). We identified 13 reoperations for prolapse, for a 10-year reoperation rate of (at least) 2.9 %. The median interval between primary and secondary surgery was 5.5 years (range 1.5–10 years).
Conclusion
The reoperation rate for prolapse after primary vaginal hysterectomy and colporrhaphy appears to be modest in this series of patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 1997 a large and widely cited study by Olsen et al. [1] reported that almost 30 % of women undergoing an operation for pelvic organ prolapse or incontinence had undergone a previous procedure for a similar problem. The 10-year follow-up of the cohort in the Olsen study reported a reoperation rate of 17 % [2]. These findings have been interpreted to imply that operations for pelvic floor disorders have high failure rates. In recent years, new surgical concepts and procedures for treatment of prolapse have been developed and brought to market. One justification for the new techniques is the assumption of poor long-term results with established operations, as in the Olsen study. However, results for incontinence and prolapse surgery are often lumped together, and few studies have addressed long-term reoperation rates for prolapse after primary surgery for prolapse [3, 4]. The aim of the present study was to determine the reoperation rate for recurrent prolapse 10 years after primary surgery for prolapse.
Materials and methods
We reviewed surgical logs and electronic records to identify all patients who underwent primary surgery for prolapse at four regional centers in the Austrian province of Styria in 1997 and 1998. Patients who had an index operation for urinary incontinence only and patients in whom it was unclear from the medical record whether she had undergone a previous procedure for prolapse were not counted. We recorded age at primary surgery, physical findings, indication for surgery, and type of prolapse surgery performed.
We then searched electronic databases at the hospitals to ascertain whether patients had undergone a second operation for prolapse through the end of 2008 (i.e., within 10 years). Patients undergoing a second procedure for incontinence only were not considered to have failed the prolapse operation and were not counted. The indication for repeat surgery and the type of operation performed were noted. The study protocol was approved by the Ethics Committee of the Medical University of Graz.
Results
A total of 456 patients who had a primary operation for prolapse in 1997 and 1998 were identified. A large majority (89 %) of these patients underwent vaginal hysterectomy with colporrhaphy (Table 1). This procedure included high closure of the peritoneum, but no explicit McCall sutures or sacrospinous fixation of the vault. Mean age at the time of the primary operation was 62 (31–93) years.
Through the end of 2008 we identified 13 women who underwent repeat surgery for prolapse, for a minimum reoperation rate of 2.9 % (Table 2). The median age of these 13 patients at the time of the primary operation was 50 years (range, 41–76). The most common reoperation was vaginal sacrospinous fixation (6/13, 46 %), 6 had colporrhaphies only and 1 received a posterior mesh. The median interval between primary surgery and reoperation was 5.6 years (1.5–10). We were not able to identify patients with recurrent symptomatic prolapse treated conservatively or not at all, patients reoperated in private hospitals or in other provinces of Austria, or patients who died in the interim.
Discussion
In this series of 456 patients undergoing fairly consistent primary surgery for pelvic organ prolapse we identified a minimum reoperation rate for prolapse of about 3 %. Although the true reoperation rate is certainly higher, this appears modest.
Defining the success or failure of surgery for pelvic organ prolapse is not straightforward. Strict anatomical criteria, such as those formulated by the NIH in 2001 [5], correlate poorly with symptoms and complaints. According to the NIH criteria 75 % of women undergoing routine gynecological examination with no symptoms of prolapse have a less than satisfactory result [6, 7]. Surgical studies based on such strict anatomical criteria will show high failure rates. For example, the randomized trial of three anterior colporrhaphy techniques by Weber et al. in 2001 [8] reported success rates between 30 % and 46 %. Chmielewski et al. [9] revisited and reevaluated this cohort and at 1 year found no prolapse beyond the hymen in 90 % of patients, 95 % of patients without prolapse symptoms, and a reoperation rate of 1 %. Similarly, Barber et al. [10] applied 18 definitions of success to the patients participating in the Colpopexy and Urinary Reduction Efforts (CARE) trial. Treatment success varied between 19 % and 97 % depending on the definition used [10]. For the purposes of the present study we decided to focus on one clear definition of failure, i.e. patients who require a second operation for the same problem. The reoperation rate for prolapse after prolapse is only a partial assessment, albeit a hard indicator, of anatomical failure.
Both anatomical and clinically meaningful functional outcomes are important, and long-term outcomes are essential to evaluate both established and new surgical procedures [11–13]. More than half the reoperations in our series occurred between 5 and 10 years after the index operation. Few studies have focused on long-term reoperation rates for prolapse after primary prolapse surgery. The landmark study from Kaiser Permanente Northwest (KPNW) by Olsen et al. [1] reported that 29 % of patients undergoing surgery for prolapse or incontinence had had a previous procedure for a pelvic floor disorder (but not necessarily prolapse). In the 10-year follow-up of 374 women undergoing surgery in the KPNW cohort, the reoperation rate was 17 % [2]. However, only 65 % of the initial procedures were for prolapse (the others were for incontinence only) and 61 % of reoperations in patients with no surgery before the 1995 index surgery were at a different site. Thus, the results reported from the KPNW cohort appear subject to misinterpretation because they are not entirely clear on how many patients undergo reoperations for the same problem [1, 2, 13]. For example, the reoperation rates in the KPNW cohort include patients who have an operation for prolapse and a second operation for incontinence. In our view this is not necessarily a failure of the prolapse operation.
Like us, Fialkow et al. [3] looked at recurrent prolapse 10 years after primary surgical management in a series of 142 patients. They report a 25 % rate of recurrence, weakly defined as a description of prolapse at clinical examination. However, only 6 women (4.2 %) of the initial group were reoperated [3]. In a 5-year prospective follow-up study of 185 women undergoing vaginal surgery for prolapse in Sweden, the reoperation rate for prolapse was 9.7 % [4]. In another Swedish series Crafoord et al. found a reoperation rate of 5.3 % within 6 years of primary prolapse surgery in a cohort of 542 patients [14]. Kapoor et al. [15] followed 207 women for a mean of 50 months after primary anterior colporrhaphy and found a 3.4 % reoperation rate for recurrent cystocele. In stark contrast, Benson et al. [16] reoperated for prolapse on 14 out of 42 (33 %) patients randomized to vaginal reconstructive surgery within a mean of only 2.5 years.
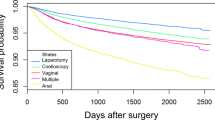
Our study permits no conclusions as to which anatomical compartment is most likely to fail. The large majority of patients underwent primary surgery in all three compartments and the most common reoperation was vaginal sacrospinous fixation, which is performed with colporrhaphy and addresses all compartments. The median age at primary surgery of the 13 reoperated patients in our series was 50 years, compared with 62 years for the overall collective. This is consistent with the conclusion by Whiteside et al. [17] that younger women are more likely to experience recurrent prolapse after vaginal repair. Salvatore et al. identified stage ≥ III prolapse as the only significant risk factor for recurrent prolapse after vaginal reconstructive surgery [18].
The strengths of our study are the comparatively large number of patients undergoing fairly consistent primary surgery (vaginal hysterectomy with colporrhaphy in the premesh era) and the 10-year follow-up. The major limitation of our study is that we could not identify patients with recurrent and symptomatic prolapse who were treated conservatively (for example, with pessaries by their primary care physicians) or not at all. Nor could we identify patients reoperated outside of our system (although in the Austrian setting patients travelling to other provinces for care is unlikely). The descriptions of the physical findings before the primary surgery were often imprecise. We were not able to identify patients who died. Lastly, we have no data on clinical examinations or functional outcomes.
Surgery for pelvic floor disorders is common, but it remains difficult to determine the long-term efficacy of these procedures and even to define efficacy. Composite outcomes are required. Prolapse is a complex entity occurring in a wide range of patients with different expectations. Assessment of results will have to take these different aspects into account.
References
Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL (1997) Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 89:501–506
Denman MA, Gregory T, Boyles SH, Smith V, Edwards SR, Clark AL (2008) Reoperation 10 years after surgically managed pelvic organ prolapse and incontinence. Am J Obstet Gynecol 198:555.e1–555.e5
Fialkow MF, Newton KM, Weiss NS (2008) Incidence of recurrent pelvic organ prolapse 10 years following primary surgical management: a retrospective cohort study. Int Urogynecol J 19:1483–1487
Miedel A, Tegerstedt G, Mörlin B, Hammarström M (2008) A 5-year prospective follow-up study of vaginal surgery for pelvic organ prolapse. Int Urogynecol J 19:1593–1601
Weber AM, Abrams P, Brubaker L, Cundiff G, Davis G, Dmochowski R et al (2001) The standardization of terminology for researchers in female pelvic floor disorders. Int Urogynecol J 12:178–186
Swift S, Woodman P, O’Boyle A, Kahn M, Valley M, Bland D, Wang W, Schaffer J (2005) Pelvic organ support study (POSST): the distribution, clinical definition, and epidemiologic condition of pelvic support defects. Am J Obstet Gynecol 192:795–806
Swift SE, Tate SB, Nicholas J (2003) Correlation of symptoms with degree of pelvic organ support in a general population of women: what is pelvic organ prolapse? Am J Obstet Gynecol 189:372–377
Weber AM, Walters MD, Piedmonte MR, Ballard LA (2001) Anterior colporrhaphy: a randomized trial of three surgical techniques. Am J Obstet Gynecol 185:1299–1306
Chmielewski L, Walters MD, Weber AM, Barber MD (2011) Reanalysis of a randomized trial of 3 techniques of anterior colporrhaphy using clinically relevant definitions of success. Am J Obstet Gynecol 205:69.e1–69.e8
Barber MD, Brubaker L, Nygaard I, for the Pelvic Floor Disorders Network et al (2009) Defining success after surgery for pelvic organ prolapse. Obstet Gynecol 114:600–609
Hilton P (2008) Long-term follow-up studies in pelvic floor dysfunction: the Holy Grail or a realistic aim? BJOG 115:135–143
Wall LL, Versi E, Norton P, Bump R (1998) Evaluating the outcome of surgery for pelvic organ prolapse. Am J Obstet Gynecol 178:877–879
Clark AL, Gregory T, Smith VJ, Edwards R (2003) Epidemiologic evaluation of reoperation for surgically treated pelvic organ prolapse and urinary incontinence. Am J Obstet Gynecol 189:1261–1267
Crafoord K, Sydsjö A, Kjolhede P (2008) Genital prolapse surgery after a shift in treatment tradition: an analysis of subsequent prolapse surgery. Acta Obstet Gynecol Scand 87:449–456
Kapoor DS, Nemcova M, Pantazis K, Brockman P, Bombieri L, Freeman RM (2010) Reoperation rate for traditional anterior vaginal repair: analysis of 207 cases with a median 4-year follow-up. Int Urogynecol J 21:27–31
Benson JT, Lucente V, McClellan E (1996) Vaginal versus abdominal reconstructive surgery for the treatment of pelvic support defects: a prospective randomized study with long-term outcome evaluation. Am J Obstet Gynecol 175:1418–1422
Whiteside JL, Weber AM, Meyn LA, Walters MD (2004) Risk factors for prolapse recurrence after vaginal repair. Am J Obstet Gynecol 191:1533–1538
Salvatore S, Athanasiou S, Digesu GA et al (2010) Identification of risk factors for genital prolapse recurrence. Neurourol Urodyn 28:301–304
Conflicts of interest
Dr. Gotthart: none
Dr. Aigmueller: speaker, Ethicon Women’s Health Female Urology/Gynecare; travel support, Astellas and Pfizer
Dr. Lang: none
Dr. Ralph: speaker and consultant, Ethicon Women’s Health Female Urology/Gynecare
Dr. Bjelic-Radisic: none
Dr. Tamussino: speaker and consultant, Ethicon Women’s Health Female Urology/Gynecare; speaker and clinical studies, Astellas (departmental); speaker, Covidien (departmental)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gotthart, P.T., Aigmueller, T., Lang, P.F.J. et al. Reoperation for pelvic organ prolapse within 10 years of primary surgery for prolapse. Int Urogynecol J 23, 1221–1224 (2012). https://doi.org/10.1007/s00192-012-1736-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-012-1736-9