
Abstract
Introduction and hypothesis
The aim of this study was to assess pelvic floor muscle (PFM) function using transabdominal ultrasound (TAUS) in women attending group exercise classes. Specific aims were to: (1) identify the ability to perform a correct elevating PFM contraction and (2) assess bladder-base movement during an abdominal curl exercise.
Methods
Ninety women participating in group exercise were recruited to complete a survey and TAUS assessment performed by two qualified Continence and Women’s Health physiotherapists with clinical experience in ultrasound scanning. The assessment comprised three attempts of a PFM contraction and an abdominal curl exercise in crook lying. Bladder-base displacement was measured to determine correct or incorrect activation patterns.
Results
Twenty-five percent (n = 23) of women were unable to demonstrate an elevating PFM contraction, and all women displayed bladder-base depression on abdominal curl (range 0.33–31.2 mm). Parous women displayed, on average, significantly more bladder-base depression than did nulliparous women [15.5 (7.3) mm vs 11.4 (5.8) mm, p < 0.009). Sixty percent (n = 54) reported stress urinary incontinence (SUI). There was no association between SUI and the inability to perform an elevating PFM contraction (p = 0.278) or the amount of bladder-base depression with abdominal curl [14.1 (7.6) mm SUI vs 14.2 (6.7) mm non-SUI].
Conclusions
TAUS identified that 25 % of women who participated in group exercise were unable to perform a correctly elevating PFM contraction, and all depressed the bladder-base on abdominal curl. Therefore, exercising women may be at risk of PFM dysfunction when performing abdominal curl activities.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The International Continence Society (ICS) defines urinary incontinence (UI) as the unwanted and involuntary leakage of urine [1]. It is a common problem that can affect women of all ages and may have a negative impact on quality of life (QoL) including, physical, psychological, sexual, emotional and social well-being [2]. UI is categorised into three types (stress, urge and mixed), with stress urinary incontinence (SUI) found to be the most frequent[1]. SUI is defined as the involuntary leakage of urine during an increase in intra-abdominal pressure (IAP), such as coughing, sneezing, effort or exertion (exercise). There are many well-researched risk factors for developing SUI, which include pregnancy, vaginal delivery, older age and menopause, obesity, lower back pain, chronic constipation, chronic coughing and heavy lifting [3]. Participation in physical activity and exercise has also frequently been suggested as a risk factor for SUI; however, it remains unclear if exercise is a risk factor or just unmasks the symptoms of SUI [4].
Studies investigating elite athletes have found a high prevalence of SUI, particularly in those engaging in high-impact exercises involving jumping [5]. However, in long-term follow-up studies, elite athletes were not found to have a higher prevalence of SUI compared with controls [6, 7]. Two studies investigated the prevalence of SUI within the general exercising population (14–51 years, 75 % nulliparous) and found a higher prevalence of SUI in women performing high-impact exercise compared with controls [8, 9]. In these studies, the most provocative activities for SUI included jumping, abdominal curl exercise and jogging. A recent study investigating women aged 18–83 years attending group exercise classes found that nearly half reported incidences of SUI [10]. Further research is needed to investigate exercise as a possible risk or contributing factor to SUI.
Abdominal curl exercises are often performed in group exercise classes and have been found to provoke SUI in up to 16 % of women [8, 9]. During abdominal exercises, there is potential for increases in IAP, as a study by Deeble et al. [11] found that women with UI and/or pelvic organ prolapse displayed wide variability in changes in IAP whilst performing an abdominal curl (range 4.00–81.67 cmH2O). This suggests that abdominal curl exercises may need to be restricted or modified in some women that generate high IAP, especially if performed repetitively whilst exercising.
As exercise is so important for general health and maintaining a healthy weight range, it is imperative to encourage women with UI to continue to participate in regular exercise. This is of particular importance, as increased body mass index (BMI) and obesity have been identified as significant risk factors for developing UI [3]. One study found that due to SUI, 10 % of women cease participation in their favourite sport and a further 20 % alter their participation to reduce leakage episodes [9]. Common preventative strategies that women use to reduce leakage during exercise are known to include limiting fluid intake; voiding prior to exercise; use of pads and modification of activity, often with the selection of lower-impact options [8–10, 12].
Based on randomised controlled trials, pelvic floor muscle (PFM) training and use of “the knack” has been shown to be effective in managing SUI and is recommended by the International Continence Society (ICS) as first-line treatment [13–15]. The theoretical basis for this is that elevation of the PFM during activities that increase IAP assists urethral closure and ensures urethral and bladder-neck stabilisation by counteracting downwards movement [16]. However, if strength or timing of the PFM activation is inadequate or performed incorrectly, resultant SUI may occur with increases in IAP. Incorrect PFM activation in some people may result in depression of the levator plate and reduced ability for urethral closure and stabilisation. Previous studies on women with and without UI have used transabdominal (TAUS) and transperineal (TPUS) ultrasound to demonstrate that PFM exercises are often performed incorrectly [17–19]. Specifically, Thompson et al. [18] found that on PFM activation in crook lying, 17 % of women with SUI demonstrated bladder-base depression. Similar observations have been noted in other studies, in which 25–38 % of women with known SUI displayed Valsalva effort on verbal PFM instruction [20, 21]. Measuring PFM function in women who participate in group exercise is of interest to determine if they are able to demonstrate correct pelvic floor contraction. A previous study of women attending group exercise classes showed that despite 97 % having heard of PFM exercises, almost half still reported SUI [10]. Therefore, a proportion of these women may not have been performing PFM exercises correctly.
Real-time ultrasound (RTUS) has been used as an assessment and teaching tool to directly visualise PFM function by observing movement at the bladder-base [19, 22] and bladder-neck [23, 24]. TPUS has a higher reliability during functional manoeuvres but is more invasive than TAUS [18]. The advantages of using TAUS in the general exercising population are that the measures are quick to perform and the technique is totally non-invasive [17]. In determining PFM function during an abdominal curl, one study observed a strong trend for women with UI to have a greater amount of bladder-base depression compared wtih continent women [18]. Junginger et al. [25] observed the effect of abdominal curl on bladder-neck position and changes in IAP in an asymptomatic population. They found that bladder-neck depression was associated with an increase in IAP and that there was insufficient PFM activity to overcome the downward pressure exerted. The association between bladder-base mobility and SUI has not been extensively examined in the general exercising population.
The primary aims of this study were to assess the ability of women attending group exercise classes to perform a correctly elevating PFM contraction and to assess bladder-base movement during an abdominal curl exercise.
Materials and methods
In this cross-sectional exploratory study, a convenience sample of women participating in group exercise was recruited to complete a survey and non-invasive RTUS assessment. These women were engaging in a variety of low- and high-impact group exercise classes, which included Pilates, yoga, weight training, running, ball sports and aerobics classes. Recruitment took place between August and October 2014 from a total of 33 organised group exercise providers and advertisements on five community notice boards within the regions of Perth and Cairns, Australia. Recruited participants gave written, informed consent. Inclusion criteria were women aged ≥18 years and participation in at least one group exercise class per week. Those who were unable to read or understand English and reported current pregnancy were excluded. The study received ethical approval from the Human Research Ethics Committee, Curtin University.
Survey
All women completed an anonymous online survey that was modified from one used in a previous study approved by Curtin University, as per recommendations from the authors [10]. The survey contained questions related to four distinct topics:
-
1.
Participant characteristics
-
2.
Prevalence of known risk factors for SUI
-
3.
Characteristics of SUI including frequency, severity and concealment factors
-
4.
Knowledge of PFM exercises
Transabdominal real-time ultrasound
Prior to US assessment, the women were instructed to follow a standardised bladder-filling protocol, as per previous studies [22]. This required voiding 1 h prior to the assessment, then drinking 500 ml of water in preparation for the US. All assessments were conducted using a standardised technique by two qualified Continence and Women’s Health physiotherapists with clinical experience in US scanning. The participants were positioned in the crook-lying position with a pillow underneath their head. Hips and knees were flexed to 60°, with the lumbar spine positioned in neutral. An RTUS unit with a 3.5-MHz curved-array transducer (Chison 8300, Mindray DP-20, DP-6600 and DP-6900) was applied suprapubically in a transverse plane to measure bladder-base movement as an indicator of PFM function, as per standard clinical practice [18]. Participants were first instructed to draw in and lift their pelvic floor, as per previous studies investigating PFM function [18, 26]. They were then asked to perform a standardised abdominal curl procedure with instructions to place the arms across the chest and lift the head and shoulders until the edge of the shoulder blades just come off the bed [18]. The sequence of PFM contraction and abdominal curl was not randomised. Participants performed each task three times, with 10-s rest between. A marker placed at rest and at the end of both PFM contraction and abdominal curl was used to measure bladder-base displacement (in millimetres) to determine correct or incorrect activation patterns. The mean measure from all three attempts was recorded. Participants were not able to view the US screen, avoiding a biofeedback-training effect. Assessors were blinded to survey results and participant continence status.
Statistical analysis
Statistical analysis of the data was performed using SPSS (version 22). Participant characteristics and descriptive data analysing PFM performance and bladder-base displacement on abdominal curl exercise are presented as frequencies, percentages and means with standard deviations (SD). Pearson’s chi-square test was used to assess associations between the presence of SUI and: (1) the ability to correctly elevate the PFM, (2) the presence of known risk factors for SUI and (3) known behavioural modification strategies for SUI. Statistical significance was inferred where p < 0.05.
Results
Demographics and participant characteristics
Ninety women with a mean (SD) age of 40 (10.6) years (range 22–69 years) were included in the trial. The mean BMI was 24.3 (3.7) kg/m2. Sixty-seven percent (n = 60) was parous. On average, participants completed three group exercise classes/week (range 1–6), with varied levels of exercise intensity. Sixty percent (n = 54) reported current SUI. Of them, 44 % (n = 40) experienced SUI on sneezing, 37 % (n = 33) on jumping, 19 % (n = 17) on running and 4 % (n = 4) on abdominal curl. Parity was found to be the only known risk factor associated with the presence of SUI (p = 0.022), with 76 % of women with SUI being parous (n = 41).
PFM performance
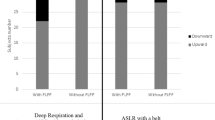
Twenty-five percent (n = 23) of the women were unable to demonstrate a correctly elevating PFM contraction. On abdominal curl, all women (n = 90) displayed bladder-base depression, with a mean descent of 14.2 (7.1) mm, (range 0.33–31.2 mm). There was no significant difference in the degree of descent between continent and incontinent women [14.2 (6.7) mm vs 14.1 (7.6) mm]. Parous women displayed, on average, significantly more bladder-base depression than did nulliparous women [15.5 (7.3) mm vs 11.4 (5.8) mm, p < 0.009], as displayed in Fig. 1.

Average bladder-base displacement of nulliparous and parous women during an abdominal curl
SUI and PFM function
The inability to correctly elevate the pelvic floor was not associated with SUI (p = 0.278) (Table 1). Seventy percent of women with SUI (n = 38) were able to demonstrate bladder-base elevation on PFM contraction. However, this was not associated with a reduced risk of SUI [odds ratio (OR) 0.57, 95 % confidence interval (CI) 0.197–1.66].
Behavioural modifications
Of the 54 women with SUI, 65 % (n = 35) urinated before exercise, 41 % (n = 22) altered or reduced their exercise participation and 31 % (n = 17) wore a pad to avoid or manage UI. Only 18 % of women from both groups (12 with and 4 without SUI) reduced their fluid intake prior to or during exercise. Women with SUI were significantly more likely to use strategies to help minimise or prevent leakage during exercise than those without SUI (chi-square 19.4, p value <0.001). Twenty-five percent of women without SUI used the behavioural modification strategies mentioned above, which may have prevented UI from occurring in this group.
Discussion
Urinary leakage during exercise is a common experience, with 60 % of women who participated in this study affected. The high prevalence of SUI reported in this study is not dissimilar to a recent study with comparable sample characteristics (age, parity and BMI), which reported SUI incidence of 49 % [10]. It is possible that potential sample bias was introduced in this study, as women experiencing symptoms of SUI may have been more likely to participate in order to increase their knowledge of PFM exercises. Previous studies with more rigorous inclusion criteria have reported a lower incidence of SUI (15–25 %) in predominantly nulliparous exercising women [8, 9]. In comparison, our study had greater variability in age, parity and menopausal status, which may account for the higher prevalence of UI. Even higher incidences of SUI (up to 80 %) have been reported; however, this was in samples of elite female athletes who engage in high-impact activity [5]. Unlike previous studies, the only risk factor that we found to be significantly correlated with SUI was parity [10]. There was no association with other well-known risk factors, likely due to the small sample size.
Previous research has shown that PFM training (to improve PFM function) is an effective strategy for treating SUI [13, 15]. The ability to perform a correct elevating PFM contraction on RTUS is used by physiotherapists to assess PFM function. It was hypothesised that within our study, a proportion of women with SUI would be unable to perform an elevating PFM contraction based on a similar trend observed in women with incontinence and prolapse, who were assessed lying supine [17]. Our study found that 25 % of participants demonstrated bladder-base depression on attempted PFM contraction. This percentage was smaller than the 43 % found in the study by Thompson and O’Sullivan [17], potentially due to the fact that women tested lying supine have been identified as having more difficulty elevating their bladder-base in comparison with lying in the crook position [27]. Our findings were similar to Thompson et al. [18] in that 17 % of women with SUI and 33 % with urinary urge incontinence depressed the bladder-base on attempted PFM contraction when lying in the crook position. Our study shows no association between the inability to perform an elevating PFM contraction and SUI. However, incorrect pelvic floor muscle activation with resultant bladder-base depression is not an optimal pattern for these women, who engage in three exercises classes/week on average. This repetitive strain could potentially be putting these women at risk of developing SUI.
Our study confirms previous research that high-impact exercise, particularly jumping and running, continues to be most provocative situation for SUI in women [8, 9]. Despite finding a lower incidence of SUI on abdominal curl in comparison with other studies [8, 9], it is still an activity that may be potentially harmful to women who exercise. This is due to the fact that all women in our study were known to be placing strain on their PFM by demonstrating bladder-base depression on abdominal curl. This is similar to findings by Junginger et al. [25], in which women who performed abdominal tasks were unable to demonstrate bladder-neck elevation. In symptomatic women or those at risk of pelvic floor dysfunction (parous women or women postgynaecological surgery), it would seem appropriate to recommend that they not participate in abdominal curl activities in order to minimise the risk of further PFM strain and incontinence. The repeated PFM strain with abdominal curl exercises could potentially be putting asymptomatic women at risk of developing incontinence, prolapse or other PFM dysfunction. The effect of repeated exercise on the pelvic floor has been studied by Ree et al. [28], where a small sample of women with mild SUI were found to have a lower maximal voluntary PFM contraction compared wtih controls after 90 min of intense exercise. A PFM-fatigue component may also contribute to SUI during exercise classes.
Whilst 70 % of the women with known SUI demonstrated bladder-base elevation on PFM contraction; it was found that performance of this correct technique does not necessarily protect against SUI. Assessing bladder-base mobility via TAUS does not investigate all aspects of PFM function. It lacks the ability to examine the specificity of the contraction in achieving urethral closure and stabilisation. TAUS is also unable to assess PFM strength or timing. Additionally, it does not examine anatomical features such as PFM tone, levator avulsion or pelvic organ prolapse - all of which may influence PFM function. In the clinical setting, TAUS is a quick, easy and noninvasive tool to assess if one can perform a correct PFM contraction. Despite its advantages, RTUS must be used with caution for this purpose, as it does not represent the complex nature of PFM function and dysfunction. A vaginal examination or TPUS may need to be performed to supplement RTUS results.
PFM endurance and repeatability are also key predictors of PFM function [29]. Our study did not assess endurance, preferring to measure the repeatability of three single attempts. We acknowledge that our measurements would not be representative of the usual pelvic floor requirements during a standard group exercise class, as fatigability was not taken into account. Given that a study found that maximal PFM contractions were reduced after strenuous physical activity [28], it is possible that the proportion of women who demonstrated a correct elevating PFM technique could have been lower if they had they been assessed after exercise participation.
Forty-one percent of women with SUI either modified exercise participation or avoided specific activities in order to prevent or reduce leakage. This is similar to previous studies that reported rates between 30 and 47 % of women modifying exercise behaviour [9, 10]. Whilst it is not recommended to cease participation in exercise completely, it is important for those who experience SUI on exercise to consider selecting lower-impact and/or lower-intensity options. This will not only reduce the amount of strain on the pelvic floor but also give muscles a chance to overcome the amount of IAP generated during exercise tasks. In doing so, women will still be able to receive the benefits of exercise whilst ensuring their risk of experiencing UI is reduced. It was noted that few women employed fluid restriction prior to exercise, regardless of continence status. This may be indicative of the warm climate in Perth and Cairns and the well-publicised health promotion encouraging adequate hydration. Interestingly, 25 % of women from this study who did not experience SUI employed behavioural modification strategies such as pre-emptive voiding or restricting fluids to avoid urinary leakage with exercise. These habits not only indicate that the prevalence of SUI may in fact be higher than reported in this group but also highlights that a proportion of women may unknowingly be participating in inappropriate exercise that is placing strain on their vulnerable pelvic floor. Without modifying their exercise participation (which only one of these non-SUI women reported doing) the severity of UI and future cost associated with it may be increased.
In our study there is potential for sample bias towards a more symptomatic population given the selective recruitment process, unknown response rate and small sample size. It is acknowledged that there are some potential limitations to this study pertaining to the US technique employed, similar to those in an earlier study that included measurement error due to probe placement and inability to have a fixed reference point, as compared wtih TPUS [18]. The two qualified Continence and Women’s Health physiotherapists who performed the assessments paid close attention to holding the probe securely to minimise this measurement error. Despite their clinical skill, with each physiotherapist having >5 years’ experience in TAUS scanning, inter-rater reliability may have been affected.
Our study, along with previous research, found that PFM function, when assessed via RTUS, is not sensitive in predicting continence status. As SUI has been identified as a significant barrier to exercise participation, further research is needed to investigate the relationship between PFM function and SUI in this population of exercising women. Additional pelvic floor assessments conducted with women in functional positions and using TPUS or vaginal examination would further add to the profile of PFM function and assist in gaining a better understanding of this relationship. Research that takes into account fatigability by assessing PFM endurance and repeatability is also needed, as this would be more representative of PFM requirements during exercise.
Conclusion
Through the use of TAUS, it was identified that 25 % of women participating in group exercise were unable to perform a correctly elevating PFM contraction. All women displayed bladder-base depression on an abdominal curl. Parous women displayed, on average, significantly more bladder-base depression than did nulliparous women. Sixty percent of these exercising women reported current SUI. There was no correlation between continence status and the ability to perform a correct PFM contraction or the amount of bladder-base depression on an abdominal curl exercise. This study emphasises that exercising women may be at risk of PFM dysfunction when performing abdominal curl activities.
References
Milsom I, Altman D, Cartwright R, Lapitan MC, Nelson R, Sillen U, Tikkinen K (2013) Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ prolapse (POP) and anal incontinence (AI). In: Abrams P, Cardozo L, Khoury S, Wein A (eds) Fifth international consultation on incontinence. Health Publications, Paris
Avery JC, Gill TK, MacLennan AH, Chittleborough CR, Grant JF, Taylor AW (2004) The impact of incontinence on health-related quality of life in a South Australian population sample. Aust N Z J Public Health 28:173–179
Koelbl H, Igawa T, Salvatore S, Laterza RM, Lowry A, Sievert K-D, Sultan A (2013) Pathophysiology of urinary incontinence, faecal incontinence and pelvic organ prolapse. In: Abrams P, Cardozo L, Khoury S, Wein A (eds) Fifth International consultation on incontinence. Health Publications, Paris
Bo K (2004) Urinary incontinence, pelvic floor dysfunction, exercise and sport. Sports Med 34:451–464
Goldstick O, Constantini N (2014) Urinary incontinence in physically active women and female athletes. Br J Sports Med 48:296–298
Bo K, Sundgot Borgen J (2010) Are former female elite athletes more likely to experience urinary incontinence later in life than non-athletes? Scand J Med Sci Sports 20:100–104
Nygaard IE (1997) Does prolonged high-impact activity contribute to later urinary incontinence? A retrospective cohort study of female olympians. Obstet Gynecol 90:718–722
Fozzatti C, Riccetto C, Herrmann V, Brancalion MF, Raimondi M, Nascif CH, Marques LR, Palma PP (2012) Prevalence study of stress urinary incontinence in women who perform high-impact exercises. Int Urogynecol J 23:1687–1691
Salvatore S, Serati M, Laterza R, Uccella S, Torella M, Bolis PF (2009) The impact of urinary stress incontinence in young and middle-age women practising recreational sports activity: an epidemiological study. Br J Sports Med 43:1115–1118
McKenzie S, Preedy T, Thompson J, Briffa K (2014) Women who attend group exercise classes or gymnasiums have a high prevalence of stress urinary incontinence. 23rd National Conference on Incontinence 12th September; Cairns
Deeble M, French S, Thompson J, Andrews A, Briffa K (2012) Should women with pelvic floor dysfunction do sit-ups? Australian and New Zealand Continence Journal 19: ISSN 1448-0131
Jácome C, Oliveira D, Marques A, Sá-Couto P (2011) Prevalence and impact of urinary incontinence among female athletes. Int J Gynecol Obstet 114:60–63
Dumoulin C, Hay-Smith J (2010) Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. doi:10.1002/14651858.CD005654.pub2
Miller J, Ashton-Miller J, Delancey J (1998) A pelvic muscle precontraction can reduce cough-related urine loss in selected women with mild SUI. J Am Geriatr Soc 46:870–874
Moore K, Dumoulin C, Bradley C, Burgio K, Chambers T, Hagen S, Hunter K, Imamura M, Thakar R, Williams K, Vale L (2013) Adult conservative management. In: Abrams P, Cardozo L, Khoury S, Wein A (eds) Fifth international consultation on incontinence. Health Publications, Paris
Delancey J, Ashton-Miller J (2004) Pathophysiology of adult urinary incontinence. Gastroenterology 126:S23–S32
Thompson JA, O’Sullivan PB (2003) Levator plate movement during voluntary pelvic floor muscle contraction in subjects with incontinence and prolapse: a cross-sectional study and review. Int Urogynecol J 14:84–88
Thompson JA, O’Sullivan PB, Briffa NK, Neumann P (2007) Comparison of transperineal and transabdominal ultrasound in the assessment of voluntary pelvic floor muscle contractions and functional manoeuvres in continent and incontinent women. Int Urogynecol J 18:779–786
Thompson J, O’Sullivan P, Briffa K, Neumann P (2006) Altered muscle activation patterns in symptomatic women during pelvic floor muscle contraction and Valsalva manouevre. Neurourol Urodyn 25:268–276
Theofrastous J, Wyman J, Bump R, McClish D, Elser D, Robinson D, Fantl J (1997) Relationship between urethral and vaginal pressures during pelvic muscle contraction. Neurourol Urodyn 16:553–558
Bump R, Hurt W, Fantl J, Wyman J (1991) Assessment of Kegel pelvic muscle exercise performance after brief verbal instruction. Am J Obstet Gynecol 165:322–329
Thompson JA, O’Sullivan PB, Briffa K, Neumann P, Court S (2005) Assessment of pelvic floor movement using transabdominal and transperineal ultrasound. Int Urogynecol J 16:285–292
Dietz H, Wilson P, Clarke B (2001) The use of perineal ultrasound to quantify levator activity and teach pelvic floor muscle exercises. Int Urogynecol J 12:166–169
Dietz H, Steensma A, Vancaillie T (2003) Levator function in nulliparous women. Int Urogynecol J 14:24–26
Junginger B, Baessler L, Sapsford R, Hodges P (2010) Effect of abdominal pressure and pelvic floor tasks on muscle activity, abdominal pressure and bladder neck. Int Urogynecol J 21:69–77
Chehrehrazi M, Arab AM, Karimi N, Zargham M (2009) Assessment of pelvic floor muscle contraction in stress urinary incontinent women: comparison between transabdominal ultrasound and perineometry. Int Urogynecol J 20:1491–1496
Frawley HC, Galea MP, Phillips BA, Sherburn M, Bø K (2006) Effect of test position on pelvic floor muscle assessment. Int Urogynecol J 17:365–371
Ree M, Nygaard I, Bo K (2007) Muscular fatigue in the pelvic floor muscles after strenuous physical activity. Acta Obstet Gynecol Scand 87:870–876
Laycock J, Jerwood D (2001) Pelvic floor muscle assessment. The PERFECT scheme. Physiotherapy 87:631–642
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Barton, A., Serrao, C., Thompson, J. et al. Transabdominal ultrasound to assess pelvic floor muscle performance during abdominal curl in exercising women. Int Urogynecol J 26, 1789–1795 (2015). https://doi.org/10.1007/s00192-015-2791-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-015-2791-9