
Abstract
Purpose
The purpose of this study was to characterize the geometry of the proximal tibia in both genders in the Korean population. Anthropometric data on the medial and lateral tibial condyles of the osteoarthritic knees of 149 males and 814 females were obtained using three-dimensional magnetic resonance imaging.
Methods
In the medial and lateral proximal tibial condyles, the anteroposterior (AP) dimension, widest dimension (WD) at defined points, and condylar aspect ratio were evaluated. These measurements were compared with similar dimensions of the tibial components from five commonly used unicompartmental knee arthroplasty (UKA) designs in Korea.
Results
Both the AP dimension and WD in the medial and lateral tibial condyles of the male patients were significantly greater than those of the female patients (P < 0.05). In addition, the AP dimension and WD were greater in the medial than in the lateral tibial condyle (P < 0.05). There was WD overhang in three and two prostheses in the medial and lateral tibial condyles, respectively. A decrease in the condylar aspect ratio with an increasing AP dimension was found in the medial and lateral tibial condyles for both the male and female patients.
Conclusions
Smaller medial and lateral tibial condylar dimensions are more frequent in Korean women than in Korean men. This study highlights the finding that conventional UKA designs lead to size mismatch in the Korean population and may indicate an important guideline on proper gender-specific UKA tibial prostheses with different WD/AP dimension aspect ratios. In addition, this study suggests that the shape of the medial tibial plateau is different to that of the lateral plateau, which can lead to a mediolateral overhang for medial UKA in an attempt to optimize the AP coverage.
Level of evidence
III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Unicompartmental knee arthroplasty (UKA) is an appropriate treatment for patients with osteoarthritis (OA) of the single compartment of the knee [20]. The use of UKA is increasing three times faster than that of total knee arthroplasty (TKA) [24]. Excellent clinical results in the first decade have encouraged surgeons to expand the indication for UKA to younger and more active patients [30]. Furthermore, UKA is associated with better range of motion and function than TKA [25]. Although many studies have investigated the functional outcome and longevity of UKA [2, 6], information regarding UKA component designs that are suitable for different population groups is limited.
Some anatomical studies have shown a wide range of variability in the size and shape of the medial and lateral tibial compartments [14, 22, 27, 28]. In addition, the anthropometry of the resected proximal-medial tibial condyle in Korean cadavers was studied by Surendran et al., which we compared with the dimensions of the five conventionally used UKA tibial components [28]. Surendran et al. reported that most of the prostheses showed a tendency toward over-sizing in the mediolateral dimensions in the Korean population [28]. Despite the high degree of differentiation between individual patients, a range of five to six tibial tray sizes is provided by most UKA tibial component systems [5].
If the prosthesis is too large, it overhangs on the bone and impinges on the soft tissues. If it is too small, contact stress is increased and load transfer across its surface is poorer; this may also result in subsidence if the implant is not resting on the harder cortical bone rim [11, 16]. In addition, Asians have a smaller build and stature than Westerners; however, most prostheses in the market are produced to fit to the physique of Westerners [27]. Furthermore, most of the sizing arrays have been designed for the medial compartment owing to the frequent medial OA, as compared with the confined lateral OA [5]. Technically, lateral UKA is more challenging than medial UKA, owing to difficulties with exposure and limitations of traditional implants, which do not address the anatomical differences between the medial and lateral compartments [9, 31]. The lateral tibial plateau is rounder than the medial tibial plateau. The tibial components do not match the anterior–posterior and/or medial–lateral ratio of the tibial plateau.
It leads to a problem of mismatch with the resected bony surfaces in the Asian population and points towards the need for a study on the anthropometry of the resected bony surfaces in various population groups to achieve the best outcome of UKA. Some studies have shown differences in the bony anatomy of the knees between males and females [15, 18, 19, 21]. Differences based on gender were also found in the Korean population in our previous study [18, 19]. Previous studies only focused on the anthropometry of the resected proximal-medial tibial condyle, and the sample sizes were too small [8, 28]. However, no previous analyses were performed on the gender-related differences in UKA in the Korean population and evaluations for both the medial and lateral tibial plateaus. In addition, the tibial component size is made either preoperatively using templates [3], or more often intraoperatively by the surgeon’s measurement. However, the variety of UKA implants available may not perfectly fit the resected tibial plateau. Thus, obtaining anthropometric data on the medial and lateral tibial plateaus becomes important to achieve the best stability and longevity for UKA.
Therefore, the purpose of this study was to obtain morphometric data on the medial and lateral tibial condyles of 963 Korean patients with OA (814 females and 149 males) using magnetic resonance imaging (MRI). A gender-related difference in proximal medial–lateral tibial condyles and size mismatch were hypothesized to be associated with the kind of UKA used in Korea.
Materials and methods
A total of 1163 OA knees (185 in male patients and 978 in female patients) were investigated in this study.
Patients who had primary knee joint osteoarthritis and TKA were included. Patients with any history of previous surgery or trauma to the affected knee were excluded. Finally, 963 patients comprised of 814 female and 149 male were included in this study. The mean ages and body mass indexes (BMIs) of the female patients and male patients were 69.1 ± 6.6, and 70.3 ± 7.2 years, and 30.0 ± 3.0 kg/m2, and 29.6 ± 3.2 kg/m2, respectively. MRI scans were acquired using a 1.5-T MRI scanner (Achieva 1.5 T; Philips Healthcare, Best, The Netherlands), with a high-resolution slice thickness of 1 mm in the sagittal plane for the tibiofemoral knee joint and 5 mm in the axial plane for the hip and ankle joints. For the non-fat saturation condition, MRI consisted of an axial proton-density sequence. A high-resolution setting was used for the spectral presaturation inversion recovery sequence (echo time, 25.0 ms; repetition time, 3590.8 ms; acquisition matrix, 512 × 512 pixels; number of excitations, 2.0; and field of view, 140 × 140 mm). The MRI method used in patient-specific instruments made it possible to develop three-dimensional (3D) reconstructed models effectively [23]. The MRI scans were imported to a modelling software (Mimics version 17.0; Materialise, Leuven, Belgium) and segmented to construct 3D bony and cartilage models of the tibia. To measure the anteroposterior (AP) dimension and widest dimension (WD), a method similar to that in previous studies was used [8, 28].
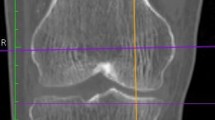
First, a line parallel and collinear to the clinical epicondylar axis of the femur mediolaterally (in the coronal plane) was drawn over the upper tibial surface, and was designated as mediolateral (ML) [28]. Second, the tibial mechanical axis was defined. We fitted the sphere on the ankle and defined the ankle centre as the sphere centre. For the tibial knee centre, the intercondylar eminence between the lateral and medial tubercles (spine) was chosen. The line connecting the centre of the ankle joint to the centre of the knee joint was created. The tibial transverse plane perpendicular to this line was then created. This axis was projected on the tibial transverse plane, and the projected line was defined as the tibial ML line (Fig. 1a). Line XY perpendicular to the ML line was created passing through the centre of the ML line. Line XZ was formed at a 6° angle with line XY, and cutting was performed along line AP parallel to line XZ, 3 mm away from the eminence. The thickness of the tibia cut was 6 mm, and the posterior slope was 7°. Cutting was performed on both the medial and lateral regions, and the same method was used. On the cutting plane, the maximum length in the direction parallel to line XZ was defined as the AP dimension, and the maximum length in the vertical direction was defined as the WD. To evaluate the variations with the conventional UKA tibial component designs, the WD and AP dimension of the resected medial and lateral tibial condyles with similar measurements obtained from the following five conventionally used unicondylar tibial prostheses were compared: Preservation (DePuy-Johnson and Johnson, Warsaw, IN, USA), ZUK (Zimmer, Warsaw, IN, USA), Miller-Galante (Zimmer, Warsaw, IN, USA), Accuris (Smith & Nephew Inc., Memphis, TN, USA), and Advance (Wright Medical Technology Inc., Arlington, TN, USA). All the measurements were obtained by an experienced observer. To test the intraobserver and interobserver variabilities, 100 of the 3D MRI scans from 50 female and 50 male patients were remeasured at > 1 week after the initial measurements by the same observer and by a second observer. The intraobserver error was 0.88 and the interobserver error was 0.92, calculated using the intraclass correlation method. The internal review board of our hospital (Yonsei Sarang Hospital Institutional Review Board No.: 18-DR-02, Protocol No.: 3D-MRI according to sex_1.0) approved the study.

Schematic representation of medial tibial condylar cuts and measurement methods using 3D magnetic resonance imaging analysis. a An anteroposterior cut was made parallel to line XZ, 3 mm apart. b The thickness of the tibia cut is 6 mm, and the posterior slope is 7°
Statistical analysis
A post hoc power analysis was performed in the medial AP dimension between the two groups using G power 3.1. The alpha value was 0.05 and the statistical power calculated was 100%. Statistical analyses were performed using SPSS for Windows version 12.0 (SPSS, Chicago, IL, USA), and the Student t test was used to evaluate the significance of the differences in data between the genders among the 963 patients. In addition, paired t tests were used to test for differences between the medial and lateral sides in the same gender. A P value of < 0.05 was considered significant.
Results
No significant differences were found in the demographics in each group, including age and BMI (Table 1). The morphological measurements of the knees are summarised in Table 2. The mean AP dimension and WD in the medial condyle were found to be 50.5 ± 4.0 and 28.1 ± 3.4 mm, respectively. The mean AP dimension and WD in the lateral condyle were 44.3 ± 3.6 and 27.2 ± 3.1 mm, respectively. The AP dimension and WD showed a significant difference between the medial and lateral condyles (P < 0.05) in both genders.
The medial tibial condyle for the male patients was significantly greater than that for the female patients (P < 0.05). Such a trend was also found in the lateral tibial condyle (P < 0.05). In the comparison of the AP dimension and WD with the respective measurements in five medial tibial components currently used in Korea, we found that three prostheses in male patients and two prostheses in female patients showed WD, a overhang for all the AP dimension ranges (Fig. 2). WD underhang and overhang for the smaller and larger AP dimensions, respectively, were observed in the Preservation design, irrespective of the gender. Conversely, WD underhang for the entire measured AP dimension range in the medial tibial components was observed in the Accuris design. The ZUK design was found to follow the morphological data closer than others in the medial tibial component.

Comparison of anteroposterior (AP) and mediolateral dimensions (WD) between the five conventional UKA designs and the tibia medial compartments of a female and b male patients
In addition, two prostheses in female patients and three prostheses in male patients showed WD underhang for all AP dimension ranges in the lateral tibial component (Fig. 3). The Advance design was found to follow the morphological data closer than the other designs in the female patients. By contrast, the M/G design was found to follow the morphological data closer than the other designs in the male patients. To determine whether the medial and lateral tibial components of UKA are suitable for the Korean population, the aspect ratio (WD/AP%) of the medial and lateral tibial condyles was evaluated (Fig. 4). A progressive decrease in the medial and lateral condylar aspect ratios was seen in the morphologic data, as the AP dimension increased, irrespective of gender (Fig. 4).

Comparison of anteroposterior (AP) and mediolateral dimensions (WD) between the five conventional UKA designs and tibia lateral compartments of the a female and b male patients

Comparison of aspect ratio (WD/AP%) between the five conventional UKA designs and measured values of a tibia medial and b tibia lateral compartments
None of the five tibial medial components had a declining change in the aspect ratio as the AP dimension increased. The aspect ratio in the lateral tibial condyle was significantly greater than that in the medial tibial condyle (P < 0.05). In addition, the aspect ratio among the male subjects was significantly greater than that among the female subjects (P < 0.05).
Discussion
The most important finding of this study was the gender-related difference in the medial–lateral tibial condyles.
The AP dimension and WD were significantly greater in male than in the female patients. The medial tibial condyle was significantly greater than the lateral tibial condyle in both the male and female patients. In addition, some prosthetic designs had morphologic data specifically well-matched with each gender and medial or lateral side. To design a unicompartmental tibial component suitable for most Korean populations, morphological data on the medial and lateral tibial condyles were evaluated. In the medial and lateral condyles, the AP dimension and WD were measured on the resected surface.
The variability of the tibial plateau anatomy may result in difficult optimization for coverage and preventing significant implant overhang or undercoverage with the conventional UKA [5]. Proper selection of patients and implants to provide the best fit to the resected surface plays a significant role in obtaining successful long-term UKA outcomes. In UKA, the geometry of the tibial component should match the resected surface as closely as possible to obtain the best stability and load transfer [21]. Previous studies have shown that overhang of the tibial component can lead to significant clinical issues with pain and impingement. Chau et al. demonstrated that in partial knees, patients with significant overhang have an increased risk for worse knee and pain scores post-operatively [7]. In addition, a previous study showed that the medial collateral ligament load was twice greater when overhang was > 2 mm; this further suggests that the excess strain may lead to chronic pain issues, which ultimately can cause revision [13]. Thus, the anthropometric data of the resected medial and lateral tibial condyles must be collected to design the proper tibial component in specific populations. The Asian population is known to have a smaller build and stature than the Western population [29]. However, most of the conventional UKA prostheses currently used are designed to match the build of Westerners.
In addition, no studies have investigated the design of the tibial component in the Asian population based on the anthropometry of the resected medial and lateral tibial condyles.
Both the AP dimension and WD were larger in the male patients than in the female patients. In our study, the AP dimension and WD were 50.5 ± 4.0 and 28.0 ± 3.3 mm, respectively, which were slightly larger than those obtained by Surendran et al. [28] (47.1 ± 4.1 and 24.8 ± 2.5 mm, respectively) and Cheng et al. [8] (49.8 ± 3.7 and 28.2 ± 2.2 mm, respectively), but smaller than those obtained by Servien et al. [27] (50.8 ± 3 and 28.8 ± 3 mm, respectively for the WD) in the medial tibial condyle. However, the AP dimension and WD are similar to those in previous studies. In addition, a previous study [11] showed that an asymmetric UKA design with varied sizes and shapes can make the implant edge lay well on the cortical bone. Our results showed that the medial and lateral tibial condyles were asymmetrical. The AP dimension and WD in the medial tibial condyle were greater than those in the lateral tibial condyle, except for the WD in the male patients. Such a trend was also found in the previous study [27]. To investigate whether the medial tibial component of UKA is suitable for the Korean population, the aspect ratio of the tibia; the medial and lateral tibial condylar aspect ratio (WD/AP%) progressively decreased as the AP dimension increased, were evaluated, and similar data were obtained as those in previous studies [8, 28]. None of the five currently used prostheses had a declining change in the aspect ratio as the AP dimension increased. It was suggested that redesigning the UKA for the Korean population based on their unique morphological properties may lead to a better outcome. The aspect ratios (WD/AP%) in the female and male patients in our study were 56.0 ± 6.1 and 5.3 ± 4.7, respectively. In the previous study [8], the aspect ratio was 57.5 ± 5.9 and 56.1 ± 5.6, respectively. A gender-related difference in aspect ratio was found in the present study as well as in previous studies [8]. Anatomically, the shape of the medial tibial plateau is different from that of the lateral tibial plateau. Owing to the difference in aspect ratio (AP/WD%) between the medial and lateral plateaus at the resection level, some implant designs may lead to WD overhang while obtaining good AP coverage. The aspect ratios (AP/WD%) of the medial and lateral tibial condyles were 1.8 ± 0.2 and 1.6 ± 0.3, respectively. In the study by Sevien et al., the ratios were 1.8 ± 0.1 and 1.6 ± 0.1, respectively. Bare et al. [1] recommended the use of different components on the lateral side. In a previous study, the results of lateral UKA are as good and reliable as those of medial UKA [26]. When the population data were compared with those obtained using the conventional design for the tibial components, WD overhang was found in three products for males and two products for females, for all the comparative AP dimensions in the medial tibial condyle. The need for smaller-sized UKA tibial components was demonstrated in the medial tibial condyle in our population group. Such results are similar to those of previous studies that showed that the medial tibial component UKA is suitable for the Asian population [8, 28]. The Preservation design followed the morphological data closer, although it showed WD undersizing for the smaller AP dimensions and WD overhang for the larger AP dimensions in the medial tibial condyle [28].
In the study by Surendran et al. [28], the Preservation design followed the population anatomy more closely for the medial plateau. In another study, Oxford and ZUK showed a shape closest to that of the tibial cut on the medial plateau [27]. An interesting finding was obtained from the lateral tibial condyle. Unlike in the medial tibial condyle, WD underhang was found in two products for male and three products for females, for all the comparative AP dimensions in the lateral tibial condyle. In addition, the Advance design was found to follow the morphological data closer than did the other designs in the lateral tibial condyle in the females, while the M/G design followed data closer in the males. Accordingly, some implant designs can be more suitable for the lateral compartment or a specific gender.
This implies that for a given increase in the AP dimension of the resected medial and lateral tibial condyles, the corresponding increase in the WD dimension is lesser in the Korean population, unlike the relatively equal increase in the AP dimension and WD of the conventional UKA tibial component designs that lead to size mismatch. In other words, the size mismatch between the conventional designs and population data was due to their relatively constant condylar aspect ratio as compared with its declining ratio in the population data.
In terms of clinical relevance, the present study findings could help surgeons understand some cases of failure. In some patients, the tibial component may have WD overlapping in medial UKA. This may be a cause of pain due to soft tissue impingement. Subsidence and aseptic loosening of the tibial tray are the most common reasons for revision with UKA as some reports show a failure rate as high as 25% attributed to aseptic tibial loosening [4, 10, 12]. In addition, this study suggests that the shape of the medial tibial plateau is different to the shape of lateral plateau, which can lead to mediolateral overhang for medial UKA in attempting to optimize AP coverage.
To the best of our knowledge, a direct causal link between undercoverage, which could lead to tibial implant fixation on softer cancellous bones, and tibial loosening or subsidence was not shown in any study; it has been suggested as a contributing factor to aseptic loosening in both UKAs [7, 11] as the cancellous bone is less able to support the loads placed on the implant [16]. Some reports have shown gender-related differences in the morphology of the knees [8, 18, 19]. In this study, the male patients had larger aspect ratios than the female patients. These results suggest that a gender-specific prosthetic design may be able to achieve a better outcome in UKA. Thus, whether to design gender-specific knee prostheses remains controversial. Theoretically, a gender-specific design could improve the anatomical match between the bone and the prostheses and avoid medial soft tissue impingement, but the clinical outcome of a gender-specific design requires further study. In addition, medial and lateral UKAs were suggested to be developed separately.
This study has some limitations. First, MRI was used to develop the 3D representation of the proximal tibia in this study, which may have led to errors in the computation model. Nevertheless, MRI allows for the reconstruction of the soft tissues, such as the articular cartilage and the inaccuracy of the 3D reconstruction could be reduced using a protocol described in a previous study [17]. Second, only one resected surface in the medial and lateral tibial condyles was measured in this study. However, this study emphasized that the basic anthropometric data for the resected medial tibial condyle were based on the commonly performed proximal tibial resection thickness and inclination values. Further studies are needed to achieve detailed analyses of UKA-related anthropometry at different levels of the cutting thickness in the medial and lateral condyles. Third, this study does not report post-operative clinical outcomes, as patients with UKA implants were not examined. Nevertheless, our findings provide valuable information for the development of UKA that are clinically well-matched to the Korean morphology and for the establishment of preoperative guidelines related to the choice of prosthesis.
Conclusions
The present study highlights the finding that conventional UKA designs lead to size mismatch in the Korean population. This study may show important references on proper gender-specific UKA tibial prostheses with different aspect ratios (WD/AP%) for the Korean population. In addition, the AP dimension and WD in the lateral and medial tibial condyles are significantly different; thus, lateral UKA is specifically necessary.
References
Bare JV, Gill HS, Beard DJ, Murray DW (2006) A convex lateral tibial plateau for knee replacement. Knee 13:122–126
Berger RA, Nedeff DD, Barden RM, Sheinkop MM, Jacobs JJ, Rosenberg AG, Galante JO (1999) Unicompartmental knee arthroplasty. Clinical experience at 6- to 10-year followup. Clin Orthop Relat Res 367:50–60
Bothra V, Lemon G, Lang D, Smith DM, Ali AM (2003) Reliability of templating in estimating the size of uni-condylar knee arthroplasty. J Arthroplasty 18:780–783
Bruni D, Zaffagnini S, Iacono F, Bragonzoni L, Lo Presti M, Neri MP, Muccioli GM, Nitri M, Raspugli G, Marcacci M (2016) High rate of implant loosening for uncemented resurfacing-type medial unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 24:3175–3182
Carpenter DP, Holmberg RR, Quartulli MJ, Barnes CL (2014) Tibial plateau coverage in UKA: a comparison of patient specific and off-the-shelf implants. J Arthroplasty 29:1694–1698
Carr A, Keyes G, Miller R, O’Connor J, Goodfellow J (1993) Medial unicompartmental arthroplasty. A survival study of the Oxford meniscal knee. Clin Orthop Relat Res 295:205–213
Chau R, Gulati A, Pandit H, Beard DJ, Price AJ, Dodd CA, Gill HS, Murray DW (2009) Tibial component overhang following unicompartmental knee replacement—does it matter? Knee 16:310–313
Cheng FB, Ji XF, Zheng WX, Lai Y, Cheng KL, Feng JC, Li YQ (2010) Use of anthropometric data from the medial tibial and femoral condyles to design unicondylar knee prostheses in the Chinese population. Knee Surg Sports Traumatol Arthrosc 18:352–358
Demange MK, Von Keudell A, Probst C, Yoshioka H, Gomoll AH (2015) Patient-specific implants for lateral unicompartmental knee arthroplasty. Int Orthop 39:1519–1526
Fehring TK, Odum SM, Masonis JL, Springer BD (2010) Early failures in unicondylar arthroplasty. Orthopedics 33:11
Fitzpatrick C, FitzPatrick D, Lee J, Auger D (2007) Statistical design of unicompartmental tibial implants and comparison with current devices. Knee 14:138–144
Furnes O, Espehaug B, Lie SA, Vollset SE, Engesaeter LB, Havelin LI (2007) Failure mechanisms after unicompartmental and tricompartmental primary knee replacement with cement. J Bone Joint Surg Am 89:519–525
Gudena R, Pilambaraei MA, Werle J, Shrive NG, Frank CB (2013) A safe overhang limit for unicompartmental knee arthroplasties based on medial collateral ligament strains: an in vitro study. J Arthroplasty 28:227–233
Hashemi J, Chandrashekar N, Gill B, Beynnon BD, Slauterbeck JR, Schutt RC Jr, Mansouri H, Dabezies E (2008) The geometry of the tibial plateau and its influence on the biomechanics of the tibiofemoral joint. J Bone Joint Surg Am 90:2724–2734
Hitt K, Shurman JR 2nd, Greene K, McCarthy J, Moskal J, Hoeman T, Mont MA (2003) Anthropometric measurements of the human knee: correlation to the sizing of current knee arthroplasty systems. J Bone Joint Surg Am 85-A(Suppl 4):115–122
Hofmann AA, Bachus KN, Wyatt RW (1991) Effect of the tibial cut on subsidence following total knee arthroplasty. Clin Orthop Relat Res 269:63–69
Kang KT, Kim SH, Son J, Lee YH, Kim S, Chun HJ (2017) Probabilistic evaluation of the material properties of the in vivo subject-specific articular surface using a computational model. J Biomed Mater Res B Appl Biomater 105:1390–1400
Kang KT, Son J, Kwon OR, Baek C, Heo DB, Park KM, Kim HJ, Koh YG (2017) Effects of measurement methods for tibial rotation axis on the morphometry in Korean populations by gender. Knee 24:23–30
Koh YG, Nam JH, Chung HS, Kim HJ, Chun HJ, Kang KT (2018) Gender differences in morphology exist in posterior condylar offsets of the knee in Korean population. Knee Surg Sports Traumatol Arthrosc 27:1628–1634
Koskinen E, Paavolainen P, Eskelinen A, Pulkkinen P, Remes V (2007) Unicondylar knee replacement for primary osteoarthritis: a prospective follow-up study of 1,819 patients from the Finnish Arthroplasty Register. Acta Orthop 78:128–135
Lonner JH, Jasko JG, Thomas BS (2008) Anthropomorphic differences between the distal femora of men and women. Clin Orthop Relat Res 466:2724–2729
Mensch JS, Amstutz HC (1975) Knee morphology as a guide to knee replacement. Clin Orthop Relat Res 112:231–241
Nunley RM, Ellison BS, Zhu J, Ruh EL, Howell SM, Barrack RL (2012) Do patient-specific guides improve coronal alignment in total knee arthroplasty? Clin Orthop Relat Res 470:895–902
Riddle DL, Jiranek WA, McGlynn FJ (2008) Yearly incidence of unicompartmental knee arthroplasty in the United States. J Arthroplasty 23:408–412
Rougraff BT, Heck DA, Gibson AE (1991) A comparison of tricompartmental and unicompartmental arthroplasty for the treatment of gonarthrosis. Clin Orthop Relat Res 273:157–164
Servien E, Aitsiselmi T, Neyret P, Verdonk P (2007) How to select candidates for lateral unicompartmental prosthesis. Techn Knee Surg 6:51–59
Servien E, Saffarini M, Lustig S, Chomel S, Neyret P (2008) Lateral versus medial tibial plateau: morphometric analysis and adaptability with current tibial component design. Knee Surg Sports Traumatol Arthrosc 16:1141–1145
Surendran S, Kwak DS, Lee UY, Park SE, Gopinathan P, Han SH, Han CW (2007) Anthropometry of the medial tibial condyle to design the tibial component for unicondylar knee arthroplasty for the Korean population. Knee Surg Sports Traumatol Arthrosc 15:436–442
Vaidya SV, Ranawat CS, Aroojis A, Laud NS (2000) Anthropometric measurements to design total knee prostheses for the Indian population. J Arthroplasty 15:79–85
Vince KG, Cyran LT (2004) Unicompartmental knee arthroplasty: new indications, more complications? J Arthroplasty 19:9–16
Wada K, Hamada D, Takasago T, Nitta A, Goto T, Tonogai I, Tsuruo Y, Sairyo K (2018) Native rotational knee kinematics is restored after lateral UKA but not after medial UKA. Knee Surg Sports Traumatol Arthrosc 26:3438–3443
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
Approval was obtained from the institutional review board of the authors’ hospital.
Informed consent
Consent was obtained from patient.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Koh, YG., Nam, JH., Chung, HS. et al. Morphologic difference and size mismatch in the medial and lateral tibial condyles exist with respect to gender for unicompartmental knee arthroplasty in the Korean population. Knee Surg Sports Traumatol Arthrosc 28, 1789–1796 (2020). https://doi.org/10.1007/s00167-019-05600-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05600-5