
Abstract
This study is a systematic literature review of outcomes following total knee arthroplasty with implants specifically designed to enable increased knee flexion. English language comparative studies without date restriction were identified through a computerised literature search and bibliography review. Nine studies met the inclusion criteria representing a total of 399 high-flexion knee arthroplasties in 370 patients. Five studies reported greater flexion or range of motion; however, the methodological rigour was questionable with inadequate blinding, flawed participant selection, short follow-up periods and functional outcomes which lacked sensitivity. There was insufficient evidence of improved range of motion or functional performance after high-flexion knee arthroplasty.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is common, successful and safe surgery for end-stage knee arthritis [1]. It achieves greater than 90% patient satisfaction [2] and has relatively low morbidity and mortality [3]. The increasing age of the population and improved survivorship enabling arthroplasty in younger more active age groups has seen the number of procedures double in the last decade [4, 5]. Demand for primary TKA is projected to grow in the USA by 673% to 3.48 million procedures by 2030 [3, 6].
Knee range of motion (ROM) and particularly knee flexion has traditionally been one of the most important factors used to determine success after TKA as many functional activities are dependent upon it. Ascending and descending stairs requires 90–120° of flexion, transferring into and out of a bath up to 135° [7] and cultural and religious activities such as squatting, kneeling and cross-legged sitting require up to 165° [8]. Following TKA however knee flexion seldom exceeds 110–115° [9–11] and while substantial functional improvements do occur post-operatively, they typically remain lower than age-matched population norms [12, 13]. Many patients are unable to return to more demanding activities such as kneeling and squatting [14, 15]. Implants designed to accommodate or even facilitate greater knee flexion and improve function whilst maintaining stability have recently emerged. These high-flexion prostheses include features such as reduced posterior femoral condylar radii with thickened posterior femoral condyles, modifications in tibial and femoral components to accommodate extensor mechanisms with deep flexion and facilitation of physiological posterior femoral rollback [16–20].
There are many factors other than prosthetic design however, which influence flexion after TKA [4, 5, 9, 11, 18, 20]. Female gender, higher body mass index, previous surgery and other co-morbidities are associated with reduced flexion [21] while intra-operative factors such as component malposition, ‘overstuffing’ the patellofemoral joint by inserting oversized components, inadequate flexion gap balancing, failure to remove posterior osteophytes and inattention to patellofemoral tracking and thickness have been reported to have a negative effect [5, 20, 22, 23]. Most consistently however, the literature reports pre-operative flexion as one of the most important predictors of flexion after TKA [9–11]. With so many variables influencing this outcome it is important to determine what effect, if any, high-flexion design has on ROM after TKA. This study is a systematic review of published trials designed to determine if there is a significant increase in ROM or function in patients who receive a high-flexion TKA compared to those who receive a standard TKA.
Materials and methods
The literature was accessed through computerised bibliographic medical and allied health databases [MEDLINE, EMBASE, Cochrane Library and Cumulative Index to Nursing & Allied Health Literature (CINAHL)]. All available English language literature was searched without date restriction. For the purposes of the review, high-flexion TKA was defined as a TKA involving a prosthesis specifically designed to achieve knee flexion greater than 120°.
The search string used for database querying was: “(arthroplasty or replacement) and knee and (flexion or (range of motion) or ROM) and (high or increased or high flexion or high flex) AND ((English[lang]))”. Meta-analyses, randomised controlled trials, retrospective and prospective studies with control groups were accepted while studies with less rigorous methodologies such as case series without control groups and anecdotal reports were excluded. Papers found by the searches were de-identified and reviewed by two authors to determine inclusion. If exclusion could not be determined easily by the title of the paper or the abstract content, full texts were obtained and reviewed.
Data abstraction
The following information was sought from all articles included in the review: study design (including randomisation methods and sample size calculation), patient characteristics such as age, gender, weight or body mass index, medical co-morbidities, surgical history, ROM, flexion and flexion contracture, duration of follow-up, inclusion and exclusion criteria, methods and blinding of assessment, functional outcome measures and patient satisfaction.
Results
Literature description
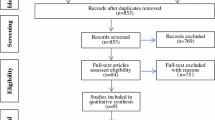
The initial search and bibliographic review returned 695 papers. Based on the title or abstract, 670 papers were excluded as they did not involve clinical outcomes of high-flexion TKA designs or were animal studies. Nine papers involving high-flexion designs were descriptive or anecdotal, or were case series without matched groups and were therefore excluded. Seven studies assessed high-flexion designs fluoroscopically but as with most studies of this nature recruited only “clinically successful” subjects and were excluded. Nine studies were included in this review for analysis (Table 1).
Overall, in the nine studies included in the review, 399 high-flex knees were implanted in 370 patients with a mean follow-up of 17.6 months. Subjects had a mean age of 67.3 years and 84.3% of the group were women. Osteoarthritis was the primary reason for TKA. Five of the nine studies were conducted in Asian populations reflecting the increased knee flexion demands in this region’s cultural and religious activities [24–28].
All studies reported ROM or knee flexion, or both, as their primary outcome (Table 2). Pre-operative ROM of an arthritic knee often comprises a measurable flexion contracture and elimination of this alone will contribute to greater post-operative ROM. This must be considered when calculating the contribution of high-flexion designs to overall ROM. One study which used ROM as their outcome did not report the flexion contracture [29].
Summary of findings
Four of the seven studies that reported flexion and two of the four studies that reported ROM found significant improvements with high-flexion designs when compared with controls (Table 2, p < 0.05). Three of the seven studies which investigated the LPS-Flex (Zimmer, Warsaw, IN, USA), the single studies involving the PFC Sigma RP-F (DePuy Orthopaedics, Inc., Warsaw, IN, USA) and the Genesis II High-flex PS (Smith & Nephew, Memphis, TN, USA) showed significant gains in their respective trials.
Functional outcome measures were reported in eight studies, the most common being the Knee Society Score (KSS) [30] in five studies [27, 29, 31–33] and the Hospital for Special Surgery (HSS) Knee Score [34] in two studies [24, 28] while one study used both [26] (Table 2). Nutton et al. [31] also used the WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) [35]. None of these studies showed any significant differences between the groups with these scores (p > 0.05). Culturally specific deep flexion activities were included in two trials. Seon et al. [28] found no difference between groups in the ability to comfortably kneel or sit in a cross-legged position. In contrast 80% of patients in the high-flexion group in the trial by Huang et al. [27] could squat at the final follow-up date compared with only 32% of those in the standard group. The significance of this difference was not reported. Interestingly 12 of the 28 patients from both groups who could squat could not get up without assistance or by pushing on their knees, and all of the 28 patients reported that they did not squat in their daily activities. The study by Nutton et al. [31] not only reported KSS but evaluated maximal functional knee flexion measured by electrogoniometry during various tasks. There were no significant differences between the high-flexion and conventional groups.
Discussion
Clinical knowledge is ideally developed through the outcomes of large, randomised controlled prospective trials. However, conducting high quality research in surgery presents obstacles such as difficulties with blinding, surgeon preference and inability to include adequate control groups [36, 37]. In the papers in this review, methodological quality and reporting was generally of a low standard. Only three of the nine trials involved randomisation [26, 31, 32], sample sizes were small with only one trial exceeding 50 [24] and only three trials revealed the detail of their sample size calculation [26, 29, 31]. Additionally, one trial involved a control group with a mobile bearing cruciate retaining device implanted with navigational assistance while the high-flexion design was a fixed bearing posterior stabilised design implanted in the conventional manner thus confounding meaningful comparison [28].
There was little consensus in selection criteria and in the matched series by Huang et al. [27] patients receiving the high-flexion prosthesis were included according to their desire for high-flexion activities post-operatively and those with significant co-morbidities were excluded from this group. This non-randomised selection may bias the high-flexion group toward a more active and motivated population, which could have contributed to the significantly higher flexion achieved in that group. Several studies included patients who received bilateral TKA [24–26, 29]. Two studies specifically recruited bilateral cases implanting a high-flexion device in one knee and a standard device in the other [25, 26]. Ng et al. [25] argue that this is the ideal methodology to compare different prostheses as it eliminates the influence of an individual’s motivation. However, though this is convenient, it seems plausible that a subject who has bilateral TKA would compare the progress of the two knees and whether voluntarily through their rehabilitation, or incidentally with the demands of their daily activities, would achieve similar results in both knee’s function and ROM. Neither of these studies showed any significant difference between groups.
Five of the nine studies showed significantly improved flexion or ROM with the high-flexion compared with the standard design [24, 27, 29, 32, 33]. However, only one of these papers involved a prospective design with randomisation [32]. The study in this review with the most robust methodology did not show significant benefits of high-flexion design [31]. Only two trials revealed their blinding method [26, 31], though in the study by Kim et al. [26] both the surgeon and a blinded assistant measured the knee ROM without clarification of how these two measurements were then used. Additionally, the method of measurement of ROM was generally underreported and lacked uniformity. Six of the studies revealed their means of measurement: the universal goniometer [24–26, 28, 29, 31] with only four of these reporting basic detail on technique [24, 26, 31, 33]. Gupta et al. [29] used a combination of goniometer measurement and visual estimation. Conclusions made on the basis of differing or unknown measurement modalities may be misleading and should be made with caution [38].
Results from studies investigating the same design were inconsistent. Four of seven trials investigating the LPS-F design failed to reveal a significant difference in flexion or ROM between the high-flexion and the standard design and showed substantial variability (Table 2). This inconsistency was demonstrated in a fluoroscopic study of several high-flexion designs [LPS-F mobile bearing and fixed bearing designs (Zimmer, Warsaw, IN, USA), PFC Sigma RP-F mobile bearing (DePuy Orthopaedics, Inc., Warsaw, IN, USA), Scorpio Super-Flex Fixed Bearing (Stryker, Inc., Mahwah, NJ, USA)]. ROM was assessed in subgroups according to surgeon and prosthesis type and marked differences were achieved by different surgeons with the same prosthesis (PFC Sigma RP-F; 102–124.8°) [5].
There is growing uncertainty whether ROM is in fact as clinically relevant as functional improvement. Myles et al. [39] evaluated the ROM of subjects after standard design TKA (LCS, DePuy International, Leeds, UK) during various functional activities and compared these with a normal age-matched population [39]. Despite subjects achieving 100° ROM post-operatively none used more than 76° of that available range during the activities whilst the control group used up to 135°. Meneghini et al. [40] compared patients after standard TKA and found subjects who had achieved 125° knee flexion or greater had improved stair climbing ability compared to those with over 115°. However there was no improvement in any other functional activity or KSS. Park et al. [41] reported knee flexion after TKA was only weakly correlated to pain, function and quality of life, and in a trial by Miner et al. [42] WOMAC function was found to be a much stronger determinant of patient satisfaction following TKA than knee flexion and only significantly deteriorated when maximum flexion was less than 95°.
Additionally, studies from both Western and Asian populations report patients undergoing TKA may consider deeper flexion activities to be less important, suggesting that they had attenuated their activity to suit their functional ability [14, 43]. A combination of the effects of aging and degenerative arthritis with subsequent muscle weakness may prevent patients from being able to control the very large quadriceps moments evident in deep weight-bearing flexion [23, 44]. It is conceivable therefore that as evident in the trial by Huang et al. [27] patients may avoid deep flexion activities post-operatively regardless of any extra available ROM.
The HSS Knee Score and/or the KSS were used in eight of the nine papers reviewed. No significant differences were found in these scores between high-flexion and standard groups, though five of the studies showed significant improvements in flexion or ROM. Critics of these scores argue that ceiling effects prevent adequate assessment of higher functioning patients [14, 45]. For example, no further points are scored after 125° of flexion. To compensate for such limitations in existing scores, the addition of functional tests such as stair climbing or rising from sitting which specifically target higher flexion activities may be required for research of high-flexion designs [40, 46]. In this review only two of the papers used functional tests [27, 28], both involving dichotomous scores of achievement of different tasks. Huang et al. [27] revealed significantly better knee flexion and clinical squatting ability with the LPS-F device; however, none of their patients squatted in their daily activities [27]. In contrast Seon et al. [28] found no difference in flexion, cross-legged sitting or kneeling between the LPS-F and a mobile bearing design. Both studies however had significant methodological flaws.
In the modern health care environment patient satisfaction is becoming increasingly important [47]. These scores correlate strongly to function and pain but vary depending on the domain which is assessed and are influenced by patient expectation and a willingness of patients to please their surgeon [1, 42, 48]. Two studies in this review included assessed satisfaction, both involving the patient’s satisfaction with outcome. Kim et al. [26] found patients in both high-flexion and standard groups were equally satisfied, but both groups did not differ in any other primary outcome. Similarly, both groups in the study by Huang et al. [27] were equally satisfied despite the high-flexion group achieving significantly higher flexion and squatting ability. Whilst it may be valuable for surgeons and researchers to ascertain a patient’s perception of the outcome of the surgery, these results clearly demonstrate the lack of sensitivity when the domain is non-specific. Future research in high-flexion TKA using satisfaction scores should separate domains such as pain and function.
High-flexion TKA is a relatively new development in knee arthroplasty and as such long-term outcome is unknown. None of the comparative studies in this review have follow-up periods longer than 35 months. Some designs require extra resection of bone to accommodate the femoral component which could lead to instability and more problematic revision surgery [19]. A recent study revealed 38% of patients in a cohort implanted with the LPS Flex showed femoral component loosening at 32 months [17] and 20% of a series of over 200 patients implanted with the Bisurface knee prosthesis (Kyocera, Kyoto, Japan) reported ‘looseness’ [49].
Conclusion
Methodological limitations and inconsistent results in high-flexion TKA research along with uncertain long-term survivorship ensure there is currently no established benefit in post-operative knee ROM or physical function when using these implants. Improvement in functional performance was not demonstrated by the papers in this review perhaps due in part to the use of knee scores which, though widely used in orthopaedic research, may not be sufficiently sensitive to detect differences, if any, in higher functioning patients. Additionally, there is growing evidence that increased knee flexion post-operatively is not sought by TKA candidates and any increase is underused. Patients are most often primarily concerned with relief of their chronic arthritic pain. Well-designed, longer term randomised controlled studies with accurate, blinded ROM measurement are therefore required to investigate the proposed benefits of these implants and should involve validated functional tests which assess higher levels of functional knee flexion such as stair climbing or rising from sitting.
References
Wylde V, Dieppe P, Hewlett S, Learmonth ID (2007) Total knee replacement: is it really an effective procedure for all? Knee 14:417–423
Robertsson O, Dunbar M, Pehrsson T et al (2000) Patient satisfaction after knee arthroplasty: a report on 27,372 knees operated on between 1981 and 1995 in Sweden. Acta Orthop Scand 71:262–267
Katz JN (2006) Total joint replacement in osteoarthritis. Best Pract Res Clin Rheumatol 20:145–153
Jones CA, Beaupre LA Johnston DW, Suarez-Almazor ME (2007) Total joint arthroplasties: current concepts of patient outcomes after surgery. Rheum Dis Clin North Am 33:71–86
Dennis DA, Komistek RD, Scuderi GR, Zingde S (2007) Factors affecting flexion after total knee arthroplasty. Clin Orthop Relat Res 464:53–60
Kurtz S, Ong K, Lau E et al (2007) Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 89:780–785
Rowe PJ, Myles CM, Walker C, Nutton R (2000) Knee joint kinematics in gait and other functional activities measured using flexible electrogoniometry: how much knee motion is sufficient for normal daily life? Gait Posture 12:143–155
Mulholland SJ, Wyss UP (2001) Activities of daily living in non-Western cultures: range of motion requirements for hip and knee joint implants. Int J Rehabil Res 24:191–198
Ritter MA, Harty LD, Davis KE et al (2003) Predicting range of motion after total knee arthroplasty. Clustering, log-linear regression, and regression tree analysis. J Bone Joint Surg Am 85:1278–1285
Anouchi YS, McShane M, Kelly F Jr et al (1996) Range of motion in total knee replacement. Clin Orthop Relat Res 331:87–92
Schurman DJ, Rojer DE (2005) Total knee arthroplasty: range of motion across five systems. Clin Orthop Relat Res 430:132–137
Finch E, Walsh M, Thomas SG, Woodhouse LJ (1998) Functional ability perceived by individuals following total knee arthroplasty compared to age-matched individuals without knee disability. J Orthop Sports Phys Ther 27:255–263
March LM, Cross MJ, Lapsley H et al (1999) Outcomes after hip or knee replacement surgery for osteoarthritis. A prospective cohort study comparing patients’ quality of life before and after surgery with age-related population norms. Med J Aust 171:235–238
Noble PC, Gordon MJ, Weiss JM et al (2005) Does total knee replacement restore normal knee function? Clin Orthop Relat Res 431:157–165
Weiss JM, Noble PC, Conditt MA et al (2002) What functional activities are important to patients with knee replacements? Clin Orthop Relat Res 404:172–188
Coughlin KM, Incavo SJ, Doohen RR et al (2007) Kneeling kinematics after total knee arthroplasty: anterior-posterior contact position of a standard and a high-flex tibial insert design. J Arthroplasty 22:160–165
Han HS, Kang SB, Yoon KS (2007) High incidence of loosening of the femoral component in legacy posterior stabilised-flex total knee replacement. J Bone Joint Surg Br 89:1457–1461
Argenson JN, Scuderi GR, Komistek RD et al (2005) In vivo kinematic evaluation and design considerations related to high flexion in total knee arthroplasty. J Biomech 38:277–284
Ranawat CS (2003) Design may be counterproductive for optimizing flexion after TKR. Clin Orthop Relat Res 416:174–176
Sultan PG, Most E, Schule S et al (2003) Optimizing flexion after total knee arthroplasty: advances in prosthetic design. Clin Orthop Relat Res 416:167–173
Fisher DA, Dierckman B, Watts MR, Davis K (2007) Looks good but feels bad: factors that contribute to poor results after total knee arthroplasty. J Arthroplasty 22(6 Suppl 2):39–42
Laskin RS, Beksac B (2004) Stiffness after total knee arthroplasty. J Arthroplasty 19(4 Suppl 1):41–46
Kurosaka M, Yoshiya S, Mizuno K, Yamomoto T (2002) Maximizing flexion after total knee arthroplasty: the need and the pitfalls. J Arthroplasty 17:59–62
Bin SI, Nam TS (2007) Early results of high-flex total knee arthroplasty: comparison study at 1 year after surgery. Knee Surg Sports Traumatol Arthrosc 15:350–355
Ng FY, Wong HL, Yau WP et al (2008) Comparison of range of motion after standard and high-flexion posterior stabilised total knee replacement. Int Orthop 32:795–798
Kim YH, Sohn KS, Kim JS (2005) Range of motion of standard and high-flexion posterior stabilized total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am 87:1470–1475
Huang HT, Su JY, Wang GJ (2005) The early results of high-flex total knee arthroplasty: a minimum of 2 years of follow-up. J Arthroplasty 20:674–679
Seon JK, Song EK, Lee JY (2005) Comparison of range of motion of high-flexion prosthesis and mobile-bearing prosthesis in total knee arthroplasty. Orthopedics 28(10 Suppl):s1247–s1250
Gupta SK, Ranawat AS, Shah V et al (2006) The P.F.C. sigma RP-F TKA designed for improved performance: A matched-pair study. Orthopedics 29(9 Suppl):S49–S52
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res 248:13–14
Nutton RW, van der Linden ML, Rowe PJ et al (2008) A prospective randomised double-blind study of functional outcome and range of flexion following total knee replacement with the NexGen standard and high flexion components. J Bone Joint Surg Br 90:37–42
Weeden SH, Schmidt R (2007) A randomized, prospective study of primary total knee components designed for increased flexion. J Arthroplasty 22:349–352
Laskin RS (2007) The effect of a high-flex implant on postoperative flexion after primary total knee arthroplasty. Orthopedics 30(8 Suppl):86–88
Insall JN, Ranawat CS, Aglietti P, Shine J (1976) A comparison of four models of total knee-replacement prostheses. J Bone Joint Surg Am 58:754–765
Bellamy N, Buchanan WW, Goldsmith CH et al (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 15:1833–1840
Fairbank JCT (2004) Randomised controlled trials. In: Pynsent PB, Fairbank JCT, Carr AJ (eds) Outcome measures in orthopaedics and orthopaedic trauma, 2nd edn. Arnold, London, pp 31–40
Boutron I, Ravaud P, Nizard R (2007) The design and assessment of prospective randomised, controlled trials in orthopaedic surgery. J Bone Joint Surg Br 89:858–863
Edwards JZ, Greene KA, Davis RS et al (2004) Measuring flexion in knee arthroplasty patients. J Arthroplasty 19:369–372
Myles CM, Rowe PJ, Walker CR, Nutton RW (2002) Knee joint functional range of movement prior to and following total knee arthroplasty measured using flexible electrogoniometry. Gait Posture 16:46–54
Meneghini RM, Pierson JL, Bagsby D et al (2007) Is there a functional benefit to obtaining high flexion after total knee arthroplasty? J Arthroplasty 22(6 Suppl 2):43–46
Park KK, Chang CB, Kang YG et al (2007) Correlation of maximum flexion with clinical outcome after total knee replacement in Asian patients. J Bone Joint Surg Br 89:604–608
Miner AL, Lingard EA, Wright EA et al (2003) Knee range of motion after total knee arthroplasty: how important is this as an outcome measure? J Arthroplasty 18:286–294
Park KK, Shin KS, Chang CB et al (2007) Functional disabilities and issues of concern in female Asian patients before TKA. Clin Orthop Relat Res 461:143–152
Nagura T, Dyrby CO, Alexander EJ, Andriacchi TP (2002) Mechanical loads at the knee joint during deep flexion. J Orthop Res 20:881–886
Victor J, Bellemans J (2006) Physiologic kinematics as a concept for better flexion in TKA. Clin Orthop Relat Res 452:53–58
Boonstra MC, De Waal Malefijt MC, Verdonschot N (2008) How to quantify knee function after total knee arthroplasty? Knee 15:390–395
Wylde V, Blom AW, Whitehouse SL et al (2009) Patient-reported outcomes after total hip and knee arthroplasty: comparison of midterm results. J Arthroplasty 24:210–216
Noble PC, Conditt MA, Cook KF, Mathis KB (2006) The John Insall Award: Patient expectations affect satisfaction with total knee arthroplasty. Clin Orthop Relat Res 452:35–43
Akagi M, Nakamura T, Matsusue Y et al (2000) The Bisurface total knee replacement: a unique design for flexion. Four-to-nine-year follow-up study. J Bone Joint Surg Am 82:1626–1633
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Murphy, M., Journeaux, S. & Russell, T. High-flexion total knee arthroplasty: a systematic review. International Orthopaedics (SICOT) 33, 887–893 (2009). https://doi.org/10.1007/s00264-009-0774-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-009-0774-5