
Abstract
Introduction
Pain is an unpleasant sensation triggered by noxious stimulation. It is one of the most prevalent conditions, limiting productivity and diminishing quality of life. Non steroidal anti inflammatory drugs (NSAIDs) are widely used as pain relievers in present day practice as pain is mostly initiated due to inflammation. However, due to potentially serious side effects, long term use of these antihyperalgesic drugs raises concern. Therefore there is a demand to search novel medicines with least side effects. Herbal products have been used for centuries to reduce pain and inflammation, and phytochemicals are known to cause fewer side effects. However, identification of active phytochemicals of herbal medicines and clear understanding of the molecular mechanism of their action is needed for clinical acceptance.
Materials and methods
In this review, we have briefly discussed the cellular and molecular changes during hyperalgesia via inflammatory mediators and neuro-modulatory action involved therein. The review includes 54 recently reported phytochemicals with antihyperalgesic action, as per the literature available with PubMed, Google Scholar and Scopus.
Conclusion
Compounds of high interest as potential antihyperalgesic agents are: curcumin, resveratrol, capsaicin, quercetin, eugenol, naringenin and epigallocatechin gallate (EGCG). Current knowledge about molecular targets of pain and their regulation by these phytochemicals is elaborated and the scope of further research is discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The ability to respond to noxious stimuli is vital for survival of an organism and can be considered as a protective mechanism against any damage due to that particular noxious stimulus. However, this response is associated with an unpleasant distressing feeling or pain. Pain is defined by the International Association for the Study of Pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. It is evoked as a defense mechanism against noxious stimuli which warns and instructs the individual to withdraw from damaging situations, to protect a damaged body part while it heals, and to avoid similar experiences in the future [1].
Perception of pain in response to noxious simulation is initiated with triggering of specialized peripheral sensory neurons known as nociceptors. Stimulated nociceptors are hyper sensitized to a mild painful stimulus giving perception of exaggerated pain or hyperalgesia. Hyperalgesia is defined as an augmented response to a noxious stimulus which manifests as an increased sensitivity to pain [2]. As the threshold for response also decreases, sometimes even innocuous stimuli may cause pain, a phenomenon called allodynia. Hyperalgesia is a hallmark of inflammatory pain triggered in response to different types of tissue insults.
The unpleasant feeling of pain is a terrible fear for mankind, even more than death itself. Therefore, relief from pain is a primary duty of a physician. Tremendous growth in pain therapy has improved the quality of life; however, selection of perfect pain relievers is still a challenge. Targeting inflammatory mediators by non steroidal anti inflammatory drugs (NSAIDs) is one of the strategies applied for treatment. However, partial success of NSAIDs guided the investigators to adopt new strategy, i.e. targeting multiple mediators and pathways simultaneously. Interestingly, most of the phytochemicals show multimode action, therefore fit better in contemporary idea. Further, long-term use of traditional drugs is dangerous due to their severe side effects [3]. In general, phytochemicals show lesser side effects, which further strengthens the idea of pain treatment using phytochemicals. Therefore, a large number of phytochemicals have been tested for their antihyperalgesic potential. Most recently used antihyperalgesic phytochemicals and their molecular mechanism are reviewed.
Nociceptive signaling
Nociceptors are afferent sensory neurons present in peripheral as well as visceral regions of the organism, and are activated by noxious stimulus. Nociceptors are unique neurons with pseudo-unipolar morphology. They have a cell body located in dorsal root ganglia (DRG) with a peripheral axon and terminal (ending) that responds to the stimulus, and a axonal branch originating from cell body is bifurcated and that transmits information to the central region (spinal cord dorsal horn or its trigeminal homologue) as well as the peripheral region. Nociceptors exhibit bidirectional signaling while transmitting noxious stimuli from the periphery to the spinal cord. The two branches are indistinguishable biochemically as most of the proteins synthesized by the cell body in DRG or trigeminal ganglion are distributed to both central and peripheral terminals [4]. This unique property contributes to hypersensitization of nociceptors (Fig. 1).

Activation of nociceptors by inflammatory mediators. Inflammatory mediators are released during tissue injury, leading to activation of several ion channels which results in depolarization of nociceptive neurons. The depolarized nociceptors up regulate the expression and secretion of inflammatory neuropeptides like SP and CGRP by DRG. These neuropeptides are distributed to both ends of nociceptors through peptidergic fibers (dotted arrows show transport of inflammatory mediators). Antidromic transport of neuropeptides to peripheral site further helps in sustained inflammation. On the other hand, transported inflammatory mediators reaching dorsal horn of spinal cord stimulate post synaptic spinal neurons as well as neighboring glial cells. Inflammatory mediators act as messengers to develop a cross talk between neurons and glial cells, immunocompetent cells, sympathetic terminals, etc. which leads to hypersensitivity of dorsal horn neuron
Nociceptive mediators of inflammatory soup stimulate and sensitize nociceptors via various receptors present at its peripheral terminal. The noxious stimuli are propagated as electrical impulses along the peripheral and central axon of the nociceptor upto the CNS (the spinal cord for the body and the trigeminal nucleus for the head). Environmental stimuli like heat, cold, and mechanical stimuli are responded by peripheral terminal, whereas endogenous stimuli like pH, lipids, and neurotransmitters trigger both the peripheral and central terminals [5]. Many of these molecules are targets for therapeutic intervention in clinical pain conditions. Both terminals are approached in pain targeting via spinal (intrathecal) delivery or via topical application of drugs.
Inflammatory mediators
Inflammatory mediators are released at peripheral site during tissue injury which may act via the surface receptors of nociceptors or by internalization, and in turn lead to activation of several ion channels resulting in depolarization of nociceptive neurons. This phenomenon is called inflammatory hyperalgesia. The depolarized nociceptors up-regulate the expression and secretion of inflammatory neuropeptides like substance-P (SP) and calcitonin gene- related peptide (CGRP) by DRG. These neuropeptides are distributed to both ends of nociceptors through peptidergic fibers. Antidromic transport of neuropeptides to peripheral site further helps in sustained inflammation. This phenomenon is called neurogenic inflammation [5]. On the other hand, transported inflammatory mediators reaching dorsal horn of spinal cord stimulate post synaptic spinal neurons as well as neighboring glial cells. Inflammatory mediators act as messengers to develop a cross talk between neurons and glial cells, immunocompetent cells, sympathetic terminals, etc. which leads to hypersensitivity of dorsal horn neurons [6].
Tissue damage or injury is accompanied by concomitant release of inflammatory mediators from local resident cells (endothelial cells, keratinocytes, and fibroblasts), infiltrated cells (neutrophils, mast cells, basophils, platelets, macrophages,) and from activated nociceptors. These mediators collectively constitute the inflammatory soup, which consists of wide range of signaling molecules including eicosinoids, cytokines, chemokines, neuropeptides, neurotrophins, as well as extracellular proteases and protons [5]. These pro-inflammatory agents act through the cell surface receptors expressed on nociceptors and initiate various signaling pathways leading to excitability and hypersensitivity of nociceptors. These inflammatory mediators are targets for development of pain relievers.
Pro-inflammatory cytokines
Pain modulation by pro-inflammatory cytokines has been studied in several animal models showing that tumor necrosis factor-alpha (TNF-α), interleukin (IL-1β and IL-6) induce and maintain hyperalgesia. Injury of peripheral nervous tissue leads to a rapid and sustained increase in cytokine secretion leading to pain behavior [7, 8].
Tumor necrosis factor-α (TNF-α)
Inflammatory cytokine TNF-α is known to play a well-established key role in several pain models [8,9,10,11,12]. TNF-α modulates both inflammatory and neuropathic hyperalgesia by initiating a cascade of inflammatory cytokines; therefore, its inhibitors show significant anti-hyperalgesic effects [13,14,15]. TNF-α receptors are expressed in both neurons and glial cells. TNF-α acts on different signaling pathways through cell surface receptors TNFR1 and TNFR2 to activate stress-activated protein kinases (SAPKs) and nuclear factor kappa B (NF-kB) during inflammation, which further activate cascade of other cytokines, notably IL-1β, IL-6, and IL-8 in the inflammatory models of carrageenan-induced and zymosan-induced hyperalgesic rats [16]. TNF-α activates tetrodotoxin-resistant voltage-gated sodium channels (TTX-r Na+ channels) via p38 MAPK pathway in cultured DRG cells [17]. Literature suggests that TNF-α mediates central mechanisms of neuropathic pain through glial systems [18]. In response to nerve injury and inflammation, microglia secrete pro-inflammatory cytokines including TNF-α [19], which mediate its effects via the p38-MAPK pathway [20]. TNF-α auto-stimulates its own production via G-protein coupled receptor (CXCR4) and TNF-α converting enzyme [21, 22].
Despite the significant role of TNF-α in neuropathic as well as inflammatory pain, the failure of TNF-α antagonists in clinical trials has guided research towards a collective role for glia-derived different mediators and their signaling pathways in the modulation of hyperalgesia [23, 24].
Interleukin-1β (IL -1β)
IL-1β is primarily released by monocytes, macrophages, fibroblasts, and endothelial cells during cell injury and inflammation. It is also reported to be expressed in nociceptive DRG neurons and spinal cord [25]. It is known to play a key role in several pain models [7, 10, 11, 26]. IL-1β signals through complex signaling cascades that lead to the release of other nociceptive molecules such as PGE2, IL-6, SP, and MMP9 in a number of neuronal and glial cells [27, 28]. Additionally, IL-1β has been shown to cause an increase in the heat-evoked release of CGRP from rat cutaneous nociceptors in vitro [29]. RT-PCR and in situ hybridization studies have demonstrated expression of IL-1R1 in sensory neurons [30], which suggests that IL-1β may directly act on nociceptors. Administration of IL-1ra is reported to reduce complete Freund’s adjuvant-induced (CFA-induced) upregulation of nerve growth factor (NGF), a neurotrophic factor known to play a crucial role in a variety of acute and chronic pain states [31]. Upregulation of NGF by IL-1β is known at both the transcriptional and post-transcriptional levels [32]. IL-1β is known to modulate neuronal excitability by affecting neuronal receptors such as transient receptor potential cation channel subfamily V member 1 (TRPV1), sodium channels, gamma-aminobutyric acid (GABA) receptors, and N-methyl-D-aspartate (NMDA) receptors [33].
Interleukin-6 (IL-6)
IL-6 contributes to the development of inflammatory and neuropathic pain after a peripheral nerve injury [8, 34] and in pathogenesis of rheumatoid arthritis [35]. IL-6 is secreted by activated microglia and astrocytes, and regulates neuropeptide expression in neurons [36]. In addition, intrathecal injection of IL-6 induces tactile allodynia and thermal hyperalgesia in intact and nerve-injured rats [34].
Prostaglandin PGE2 up-regulates expression of IL-6 via EP4 receptor, and activates PKC pathway in injured nerves in case of neuropathic pain model [37]. The role of PGE2 is also demonstrated in the synthesis of IL-6 in primary sensory neurons following nerve injury. In vitro studies suggest that prostaglandin E2 receptor 4 (EP4 receptor), PKA, PKC, ERK/MAPK, CREB, and NF-kB signaling pathways are involved in PGE2-induced IL-6 production in DRG neurons [38]. IL-6 mainly activates the JAK/STAT transduction pathway in microglia of spinal cord during neuropathic pain [39]. There is evidence of IL-6 induced microglial CX3C- chemokine receptor 1 (CX3CR1) expression in the spinal cord through p38 MAPK activation after peripheral nerve injury [40].
Inflammatory enzymes
The inflammatory enzymes COX and NOS, especially their inducible isozymes COX-2 and iNOS, are implicated in the development of hyperalgesia. There are important and complex interactions between these two mediator systems.
Cyclooxygenase (COX)
COX plays a key role in biosynthesis of prostaglandins from arachidonic acid. Prostaglandins have implication in promoting inflammation and hyperalgesia. Pro-inflammatory cytokines like TNF-α induce the expression of COX in cultured DRG neurons [41]. The inducible isozyme COX-2 is expressed in inflammatory cells and tissues after inflammation and causes hyperalgesia [42]; consequently, COX-2 selective inhibitors are potent antihyperalgesic agents. COX-2 specific inhibitor coxibs markedly reduce pain symptoms in rat models of carrageenan, zymosan or formalin-evoked hyperalgesia [43,44,45]. COX-2 plays an important role in central sensitization after peripheral inflammation in the mouse and rat models of inflammation [46, 47]. Recent findings show the activation of both COX-1 and COX-2 in DRG during inflammatory hyperalgesia leading to activation of TRPV1 ion channels as well as PKCε [48].
Nitric oxide synthase (NOS)
NO synthesized by nitric oxide synthase (NOS) has role in spinal nociceptive processing. Over activation of different isoforms of NOS plays important role in hyperalgesia by mediating neuronal excito-toxicity by activating the receptors and downstream MAPK signaling pathways [49]. iNOS is expressed in immune cells including glial cells and is involved in several signaling pathways of hyperalgesia [50]. Pro-inflammatory cytokines like TNF-α, IL-1β, and interferon-γ induce the expression of iNOS in microglia by activation of NF-κB causing peroxynitrite injury in peripheral nerve which plays a major role in peripheral nerve dysfunction and degeneration [51].
Nociceptive receptors
In response to inflammatory mediators, nociceptors are sensitized via a number of receptors present at peripheral terminals, e.g. TRPV, voltage-dependent and transient receptor potential ankyrin (TRPA), melastatin-related transient receptor potential (TRPM), acid-sensing ion channels (ASIC), GPCR, RTK, etc. At the central level, nociceptive pathways are modulated mainly by N-methyl-D-aspartate receptor (NMDAR), α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR), neurokinin 1 receptor (NK1R), and metabotropic glutamate receptors (mGluRs). Recent studies suggest a key role of NMDAR in central sensitization during chronic pain states. Therefore, blockers of many of these ion channels are being tested for their therapeutic potential by many investigators [51,52,53,54,55].
The molecular transducer TRPV1 is activated by noxious heat, reduced pH, and the chemical capsaicin, whereas TRPM8, TRPV2 channels respond to cold and methanol [56] and the pungent ingredients of mustard and garlic activate TRPA1 [57]. Triggering of mechanical pain involves TRPA1 receptors and potassium channel subfamily K (KCNK) channels [5].
Several ion channels are responsible for thermal and mechanical pain hypersensitivity; out of them TRPV1 is most studied. It is an ionotropic, Ca2+ permeable, non-selective cation channel which is suggested to be a key target of inflammatory mediators during generation of thermal hyperalgesia [58]. Studies have shown that TRPV1 functions as an integrator of multiple signals and its sensitivity for thermal stimuli can be greatly altered by several components of the inflammatory soup [59]. Few inflammatory mediators function as direct modulators of the channel, whereas others act through downstream signaling pathways. These interactions result in a decrease in activation threshold of these ion channels resulting in allodynia and hyperalgesia. However, there is a controversy regarding the intracellular signaling mechanisms which are most effective in TRPV1 modulation [60]. Nonetheless, TRPV1 modulation is suggested to be an important phenomenon in generation of pain hypersensitivity, particularly in the setting of tissue injury-evoked inflammation. Therefore, it may act as a therapeutic target in infections, osteoarthritis or rheumatoid arthritis, and inflammatory bowel disease.
Inflammatory pathways involved in initiation and maintenance of hyperalgesia
Nuclear factor kappa B (NF-kB) pathway
Nuclear factor-κB (NF-κB) belongs to the family of inducible transcription factors, which is known to regulate a variety of genes involved in different inflammatory and immune responses such as infection, tissue injury or ROS generation [61] via production of inflammatory cytokines [62]. Under normal conditions, NF-kB is localized in the cytoplasm of the cell and remains associated with inhibitory protein inhibitor of kB (IkB); but depending upon the type of stimulus, the activation of NF-κB follows two different signaling pathways. First, the canonical NF-κB pathway is known to be triggered by proinflammatory cytokines such as TNF-α and IL-1, members of TNF receptor super family, and T-cell receptor (TCR) and B-cell receptor [63]. The signaling pathway is initiated by IKK-mediated inducible degradation of IκB; and subsequent release and translocation of NF-kB into nucleus initiates transcription of inflammatory genes like TNFα, IL-1β, which further regulate down-stream mediators [64]. Second, the non-canonical NF-κB pathway or ‘alternative NF-kB pathway’ is activated selectively by specific stimuli which include ligands of a subset of TNFR super family members such as Lymphotoxin β Receptor (LTβR), B-cell activating factor receptor (BAFFR), CD40 and Receptor Activator of Nuclear Factor κ B (RANK) [65]. The activation of non-canonical NF-κB pathway does not involve IκBα degradation; rather it involves inducible phosphorylation of NF-κB2 precursor protein, p100 by IKKα leading to activation of RelB/p52 heterodimers [66]. Both the canonical and non-canonical pathways are involved in regulation of immune and inflammatory responses despite the differences in signaling mechanism [66, 67]. The activation of transcription factor NF-κB during hyperalgesia generally follows the canonical pathway [68] (Fig. 2).

Activation of NFκB pathway. NF-κB commonly refers to a p50-p65 heterodimer, which represents the major Rel/NF-κB complex in most cells. In basal conditions NF-κB is sequestered in the cytoplasm by inhibitor proteins, usually IκB. Upon stimulation, IκBα is rapidly phosphorylated by the IkB kinase complex (IKK). Phosphorylated IκB is substrate for ubiquitination and subsequent degradation by the 26S proteasome. The released NF-κB dimer is translocated to the nucleus leading to activation of target genes
NF-κB is widely recognized as a master switch that is essential for immune responses. Increased NF-κB activity in immune and nervous system cells is linked to several chronic pain conditions in humans like rheumatoid arthritis, migraine, nerve injury; as well as inflammation- and nerve injury-evoked pain in animals [69]. While NF-κB is ubiquitously expressed in a variety of cell types, its contribution is driven largely by signaling in the dorsal root ganglia and in astrocytes of spinal cord during inflammatory and neuropathic pain [70]. The activation of NF-κB in astrocytes may produce pain by decreasing the expression of catechol-o-methyltransferase (COMT), an enzyme that inactivates catecholamines and modulates pain [71]. Astrocytic NF-κB is reported to be upregulated in CFA-induced inflammation [72] as well as in nerve injury [70]. Likewise, loss of astrocytic NF-κB signaling attenuates pain following formalin administration [73].
NSAIDs are now believed to target both the NF-kB and COX pathways, to inhibit leukocyte recruitment [74]. Recent research indicates that natural compounds reduce the inflammation and hyperalgesia by blocking the activation of NF-kB and other inflammatory mediators.
MAPK pathways
Other than the classical role of MAPKs in cell death and survival, studies in the past decade revealed direct or indirect involvement of all the three MAPKs in neuropathic and inflammatory hyperalgesia. Role of MAPKs has been suggested to be specific in pain hypersensitivity with negligible effect on physiological pain perception [75]. Various inflammatory mediators are implicated in peripheral sensitization of nociceptors and initiation of hyperalgesia. However at central site, microglia and astrocytes contribute to the release of multiple inflammatory mediators, neuromodulators, and growth factors which enhance excitability within the dorsal horn of the spinal cord [76]. Central sensitization results from activation of different membrane receptors and channels via phosphorylation, leading to various intracellular kinase cascades. Several different intracellular signal transduction cascades converge on MAPK. Peripheral or spinal nerve injury activates p38 in spinal neurons, microglia, and Astrocytes, whereas ERK activity is reported to increase in microglia and Astrocytes [77]. Recent literature suggests a significant role of p38 in post-operative pain [78]. Increasing body of evidence indicates a crucial role of glial cells in the pathogenesis of pain [79].
ERK-MAPK activation is suggested as a master switch or gate for the regulation of central sensitization [80]. Activation of ERK is reported to be induced in spinal cord dorsal horn (SCDH) neurons by persistent noxious input, produced by various sources [81]. Stimulation of DRG neurons with TNF-α leads to ERK activation, and subsequent increase in expression of TRPV1 [82]; which is a major target of peripheral sensitization. Further, morphine-induced hyperalgesia involves activation of ERK in brain cortex [83]. Recent study reveals the role of ERK signaling in the periphery as it influences the transition from acute to chronic postoperative pain [84]. Therefore, activation of ERK has been considered as neuronal marker of pain [85]. Pharmacological intervention targeted specifically at the signal transduction pathways in nociceptive neurons may provide new therapeutic opportunities for pathological pain.
Recently, we have demonstrated that ROS produced during peripheral inflammation leads to activation of ERK in DRG as well as in spinal dorsal horn [86]. Therefore, we have suggested that antihyperalgesic property of natural polyphenols like resveratrol and curcumin may be attributed to their antioxidant property [87,88,89]. We have shown a functional correlation between down-regulation of ERK signaling in spinal cord by resveratrol with its antioxidant and antihyperalgesic potential [89]. The findings suggest that ERK-MAPK might be a major target of natural compounds used for hyperalgesia treatment.
Antihyperalgesic drugs
Clinical and molecular studies provide evidences that inflammation is responsible for acute inflammatory hyperalgesia as well as for maintenance of chronic pain. NSAIDs are most widely used antihyperalgesic drugs, especially in case of acute hyperalgesia although their long use leads to adverse effects like risk of elevated blood pressure, blood clots, platelet dysfunction, peptic ulcer, nephropathy and renal failure, inhibition of labor, cardiac failure, and sudden cardiac death [90, 91]. Opioids are used in case of chronic hyperalgesia. The major concern of long-term treatment of opioids includes increased risk of addiction, tolerance, and neuropsychological effects. The symptoms are nausea, vomiting, constipation, itching, dizziness, sweating, sedation, lethargy, CNS adverse events, and overdose leading to death [92]. Serious side effects of available antihyperalgesic or pain relieving drugs pose a challenge to scientist to search an alternative therapy with least side effects.
Antihyperalgesic phytochemicals
Recent studies show involvement of ROS in initiation and maintenance of hyperalgesia [93]. These are implicated in inflammatory as well as neuropathic pain [94, 95]. ROS is known to mediate development and maintenance of capsaicin-induced hyperalgesia in mice, primarily through central sensitization [96]. Recently, antioxidants have shown promising effect in elimination of pain. Polyphenols of dietary source like vegetables, fruits, and drinks (wine and tea) are being tested for their analgesic action [87, 88]. Scientists are engaged in search of antioxidant and anti inflammatory agent as pain relievers with minimum side effects.
A number of herbal products with antioxidant and anti inflammatory properties are known since ancient times which exhibit anti hyperalgesic potential. These products are used to treat pain and inflammation with almost no side effects. Although safe in most cases, ancient pain therapy using herbal medicines are ignored because neither their active components nor their molecular targets are well defined. However in the past decade, scientists have identified a number of targets which are manipulated by herbal products during intervening hyperalgesia. The active components are shown to inhibit the activation, release, and action of inflammatory mediators.
Here, we have reviewed more than 50 antihyperalgesic phytochemicals used in the studies conducted recently (Table 1). Three sources were used to search for appropriate papers. These included Medline-PubMed, Google Scholar, and Scopus using different combinations of keywords like pain, hyperalgesia, phytochemicals, herbal products, and phytotherapy. The databases were searched for studies published after 2010. Citations were limited to purified active constituents. Studies using crude or partially purified plant extracts were excluded. Additional papers were included by searching name of individual phytochemical in combination with above key words; and after the analysis of all references from the selected articles (some of them were published before 2010). Seven most cited phytochemicals; Curcumin, capsaicin, resveratrol, quercetin, eugenol, naringenin, and EGCG have been described in detail.
Curcumin
In India and other parts of Asia, turmeric is used to treat many health conditions. Curcumin, a substance in turmeric, may help to reduce inflammation. Both the ancient Indian and Chinese systems of medicine have recognized curcumin’s beneficial properties for thousands of years. Curcumin is considered as an excellent pain reliever [227,228,229,230]. It is believed to have anti-inflammatory, antioxidant, and anticancer properties [231,232,233]. Several studies suggest that it might ameliorate pain and inflammation in animal models and in case of human osteoarthritis and rheumatoid arthritis [234]. We have shown antihyperalgesic action of curcumin in rodents by modulation of antioxidant enzymes and down regulation of TNF-α, IL-1β and IL-6 [87]. Curcumin attenuates diabetic neuropathic pain in mouse, possibly through its inhibitory action on NO and TNF-α release [97, 98]. Curcumin has been shown to regulate numerous transcription factors [106, 110], cytokines [99], protein kinases [104, 105], adhesion molecules, redox status [87] and enzymes [102] that have been linked to hyperalgesia. It can inhibit the activity and the synthesis of COX-2 and 5-lipooxygenase (5-LOX), as well as other enzymes that have been implicated in inflammation and hyperalgesia [102, 108]. Curcumin is shown to be as effective as ibuprofen for the treatment of knee osteoarthritis with fewer gastrointestinal adverse effects [235]. It is believed to lead to a phase out of NSAID use, at least as a treatment for mild-to-moderate osteoarthritis. Now modern research is showing that curcumin may be one of nature’s most powerful potential healers.
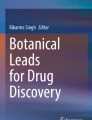
Curcumin contains vanilloid ring similar to that present in capsaicin, the main pungent ingredient in hot chili peppers (Fig. 3). The burning sensation of chili pepper is mediated via activation of capsaicin receptor (TRPV1). Recent studies demonstrate that pain relieving action of curcumin is due to antagonism of TRPV1 [100, 112]. In addition, antihyperalgesic action of curcumin is mediated by inhibition of other ion channels like TTXR-Na + channel and ASICs [103, 111]. Curcumin-induced antinociceptive action on neuropathic pain has also been reported via inhibition of TNF-α/NO release [97, 99], as well as by differential regulation of descending monoamine system and opioid receptors [101, 107, 113].

Structural similarity between curcumin and capsaicin
In spite of tremendous potential of curcumin in pain relief, its use is generally limited by its poor bioavailability. Therefore, research has been focused to increase its bioavailability by nano-encapsulation [109, 236, 237]. Nano-encapsulated curcumin shows better bioavailability and relieve pain by inhibiting brain-derived neurotrophic factor (BDNF) and P2X purinoceptor 3 (P2X3) [109, 237].
Capsaicin
Capsaicin is the main pungent ingredient in hot chili peppers has been used as a topical analgesic for centuries. Capsaicin is a highly selective agonist for TRPV1 receptors expressed in afferent neuronal C fibers and some Aδ fibers. Prolonged activation of TRPV1 by capsaicin through enzymatic or osmotic changes results in loss of receptor functionality, causing impaired local nociception for extended periods [156]. Capsaicin-induced local depletion of substance P was previously thought to be its mechanism for pain relief. However, this is no longer considered to be the case, rather other mechanisms may be involved [157]. For instance, Borbiro et al (2015) have demonstrated that activation of TRPV1 inhibits Piezo channels through a calcium-induced depletion of phosphoinositides [158]. This regulation could contribute to the cellular mechanisms by which the TRPV1 activation by capsaicin mitigates mechanical hypersensitivity. Recently capsaicin is demonstrated to alleviate inflammation by targeting MAPK-PGE2 pathway which has broadened our understanding for new avenues of therapy in neuro-inflammatory pain [160].
Resveratrol
Resveratrol is a natural polyphenol and a phytoalexin produced by several plants in response to injury or when the plant is under attack by pathogens such as bacteria or fungi (Fig. 4). Sources of resveratrol in food include the skin of grapes, blueberries, raspberries, mulberries. Richest sources of resveratrol are grapes and red wine. It has no known toxic side-effects [238]. The anti-inflammatory activity of resveratrol has been well documented and can be ascribed to inhibition of pro-inflammatory cytokines, chemokines and promotion of anti-inflammatory cytokine IL-10 [88, 114, 120]. It is reported to suppress the nociceptive neuronal activity [239, 240]. Resveratrol could be a complementary and alternative medicine to clinical pain management approaches, especially in patients with chronic severe pain being treated with morphine for long time through action on the NMDA receptors and neuroinflammatory responses [115, 241, 242].

Structure of resveratrol and quercetin
Previous reports indicate anti-nociceptive action of resveratrol by inhibition of COX-1 and COX-2 activity during inflammation-induced hyperalgesia [121, 122]. But now it is almost established that resveratrol decreases the production of prostaglandin E2 (PGE2) by inhibiting the cyclooxygenase (COX)-2 cascades [121]. Inhibitory action of resveratrol on spinal COX-2 expression has also been demonstrated in our lab [87].
In addition to anti-inflammatory mechanism, anti-hyperalgesic action of resveratrol is also supported by modulation of the activity of voltage’-gated and ligand-gated ion channels at peripheral and central levels. Resveratrol has been reported to modulate the excitability of neurons in the peripheral nervous system by activating voltage-dependent and transient receptor potential (TRP) channels [123,124,125,126]. Inhibition of TRP ankyrin 1 (TRPA1), a mechano-sensitive channel by resveratrol [126], suggests that it inhibits action potential firing via the mechanical transduction process. Moreover, Na+ and K+ ion channels of DRG are also modulated by resveratrol [124, 127]. Furthermore, antinociceptive effect of resveratrol after systemic administration appears to be mediated via an opioidergic mechanism [243]. Interestingly, opioidergic and inflammatory pathways are linked with concomitant ROS generation [244]. ROS is now considered as an essential component of hyperalgesia development. Therefore, anti-oxidant property of resveratrol is supposed to a key property which might be employed in most of its anti-hyperalgesic mechanisms [245, 246]. In this context, we recently analyzed the effect of resveratrol treatment on modulation of endogenous antioxidant defense system in peripheral and central nervous system. We found a correlation between modulation of antioxidant enzymes and anti-hyperalgesic effect of resveratrol. Furthermore, ROS scavenging property of resveratrol was also manifested in modulation of ROS sensitive signaling pathway such as TNFR1-ERK signaling [89]. ERK activation in spinal dorsal horn is now considered as hallmark of hyperalgesia which serves as a single convergence point for several signaling pathways; therefore, inhibition of ERK signaling in spinal cord further strengthens the candidature of resveratrol as a potent anti-hyperalgesic agent [85]. Resveratrol potently inhibits IL-6-mediated signaling to ERK in sensory neurons, blocking the perception of pain. Resveratrol administered at the time of incision is capable of completely blocking the development of persistent pain sensitization by upregulating the N-methyl-D-aspartate receptor (NMDAR) which is thought to be significant in morphine tolerance. Blocking NMDAR function effectively weakens tolerance to morphine and increases morphine’s analgesic properties [115]. Inhibition of microglial activation via AMPK signaling by resveratrol further contributes to reduce morphine’s tolerance [128, 247]. Other targets of resveratrol during hyperalgesia are P2X purinoceptor 7 (P2X7) and Sirtuin 1 (Sirt1) [116, 117, 119, 129]. Recent reports suggest its antihyperalgesic action by inhibiting glial activation [248].
Quercetin
Quercetin, a plant polyphenol is one of the most abundant dietary flavonoids, found in many fruits, vegetables, leaves, and grains (Fig. 4). Quercetin is classified as an antioxidant and is reported to exhibit a wide range of pharmacological properties, for example, anti-inflammatory and anticancerous [249], anti-hepatic fibrosis [250], anti-hyperalgesic [131], and neuroprotective in different animal models of neuropathy [132, 133, 251].
Quercetin is a non-specific protein kinase enzyme inhibitor [252]. The analgesic effects of quercetin observed in models of nociception were described to be dependent on many mechanisms, including NO production, activation of GABA and serotonin receptors, opioid like effects, inhibition of TRPV1 and NMDAR, inhibition of inflammatory cytokines (TNF-α and IL-1β) and inflammatory enzyme (COX-2) as well as by reducing oxidative stress [130, 253]. Quercetin is reported to elucidate its neuroprotective effect in diabetic neuropathy [251], alcohol-induced neuropathy [133], arthritic pain [138, 139, 254,255,256], adenomyosis-induced hyperalgesia [136], cancer-evoked pain [137] and paclitaxel-induced nuropathic pain [134]. Quercetin is a potential molecule for the treatment of muscle pain conditions. It reduces muscle mechanical hyperalgesia by inhibiting myeloperoxidase (MPO) and NAG activities, cytokine production, oxidative stress, COX-2 and NFκB activation; and by inducing Nrf2 and HO-1 and glial cells’ activation [135, 257]. Recently, Nie et al. (2017) have reported that quercetin decreases hyperalgesia by decreasing the expression levels of TRPV1, pp38, and pERK in DRG neurons suggesting that potential mechanism of action of quercetin is through reduced central sensitization [136].
Eugenol
Eugenol is a colorless to pale yellow, aromatic oily liquid extracted from certain essential oils especially from clove oil (80–95%), nutmeg, cinnamon, basil, and bay leaf. Eugenol (4-allyl-2-methoxyphenol) a methoxyphenol with a short hydrocarbon chain is a member of the phenylpropanoids class of chemical compounds (Fig. 5).

Structure of eugenol, EGCG, and naringenin
Pharmacologic studies have demonstrated that eugenol has anticonvulsant [258], local anesthetic [259], antistress [260], and anti-oxidation activity because of its ability to reduce superoxide to H2O2 [261] or to scavenge the free radicals through chelation of metal ions [262]. It shows anti-bacterial [263], antifungal [140], and anti-inflammatory activity by inhibiting inflammatory mediators such as COX-2, IL-1β, and TNF-α in LPS-activated macrophages and analgesic activity due to selective binding at the capsaicin receptor [264]. In pre-clinical studies, eugenol shows its antihyperalgesic action in neuropathic and arthritic hyperalgesia [142, 265, 266]. Eugenol is used as a local anesthetic. Reversible inhibition of nerve impulse and compound action potentials by eugenol was recorded in various nerves including tooth pulp nerve, sciatic nerve, and superior cervical ganglion neurons of rats [267]. It has been extensively used as a therapeutic agent in dentistry for sedation in patients with toothache, pulpitis, and dental hyperalgesia.
Eugenol successfully inhibited voltage-gated sodium channels when tested in dental primary afferent neurons [144] and DRG neurons [145] of rats, suggesting that eugenol might block action potentials in both nociceptive afferent fibers. Supporting evidence is yet to be found whether eugenol binds directly to voltage-gated sodium channels and modulate; however, it is clear that modulation of voltage-gated sodium channels is a mechanism that contributes to the analgesic action of eugenol. Voltage-gated potassium channels play roles in repolarization of cell membrane after action potential firing. Eugenol has been found to inhibit voltage-gated potassium channels in both capsaicin-sensitive and capsaicin-insensitive neurons [141]. Eugenol exerts its anesthetic action via antagonism of NMDAR, an NMDA-sensitive ionotropic glutamate receptor [268] that plays an important role in synaptic modulation and memory function.
Naringenin
Naringenin is a bitter and colorless flavonoid, predominantly found in grapefruit (Fig. 5). It has shown several biological activities like antioxidant, anti-inflammatory, anti-cancerous, and neuroprotective effects in several studies. Likewise, its antihyperalgesic potential has been revealed during past 5 years. Till date, its antihyperalgesic potential could be attributed to its antioxidant property. The anti-hyperalgesic potential of naringenin in diabetic neuropathy is shown by modulation of oxidative and inflammatory markers [149] and by improvement in the activity of antioxidant enzyme superoxide dismutase (SOD) [150]. Further studies revealed its effect on ROS-dependant downstream signaling pathways in inflammatory hyperalgesia. Recently, naringenin has been demonstrated to show its effect on superoxide anion-induced as well as CFA-induced hyperalgesia via modulation of oxidative stress, cytokines, nuclear factor erythroid 2-related factor 2 (Nrf-2), and NO − cGMP − PKG pathway [147, 148]. Furthermore, naringenin treatment is also effective in neuropathic pain by inhibition of microglial activation in spinal cord [146]. However, use of naringenin as antihyperalgesic agent is limited due to its poor bioavailability. Attempts should be made to increase its bioavailability either by structural modification or by nano-conjugation in order to attain final development.
Epigallocatechin gallate (EGCG)
Epigallocatechin gallate (EGCG), also known as epigallocatechin-3-gallate, is the most abundant catechin in tea, found in high content in the dried leaves of green tea (Fig. 5). It is a polyphenol which has recently attracted several scientists across the globe due to its tremendous potential to affect human health and disease. EGCG is known to have neuroprotective effects in various pathological states in the nervous system [269], which is generally attributed to its antioxidant property. Initial studies have shown that its antioxidant property may also be exploited for relief in neuropathic pain. The antihyperalgesic action of EGCG is suggested to be brought by inhibition of spinal nNOS which has encouraged researchers to exploit the antioxidant property of EGCG for relief in neuropathic patient [153]. Similarly, its potential to decrease diabetes-induced neuropathic pain is demonstrated by reduction in spinal ROS [151]. Further studies suggest the involvement of other inflammatory mediators in its antihyperalgesic action. For instance, intrathecal injection of EGCG is reported to improve the pain behaviors in CCI-induced neuropathic pain which is accompanied by decreased expression of TLR4, NF-κB, HMGB1, TNF-α, and IL-1β and increased content of IL-10 in the spinal cord [152]. Recent reports suggest a new role of EGCG during alleviation of neuropathic pain, i.e. inhibition of neuronal–microglial communication. It is attained by inhibition of chemokine CX3CL1 and RhoA expression in spinal cord [154, 155].
In general high doses of EGCG are required for treatment of neuropathic pain. Therefore, administration of pure EGCG in pills or capsule forms may be appropriate for alleviating neuropathic pain [154]. However, further research evidences are required before implementation of this mode of treatment.
Summary and future scope
A number of inflammatory mediators like pro-inflammatory cytokines TNF-α, IL -1β, IL-6, and inflammatory enzymes COX, NOS; nociceptive receptors TRPV, TRPA, TRPM, NMDAR, AMPAR, and channels ASIC, KCNK; and inflammatory pathways like NF-kB pathways and MAPK pathways provide specific molecular targets for pain therapy. We have reviewed the mechanism of action of herbal products of recent interest and the target points which are being intervened in treating inflammation and hyperalgesia.
An antihyperalgesic drug should be able to act at peripheral level or central level or at both levels simultaneously, depending upon different etiologies of different pain conditions. Therefore, pharmacognocy and pharmacokinetics of herb-derived phytochemicals is needed before therapeutical use. Another concern is the poor absorption and, therefore, low bioavailability of most of the phytochemicals. Their tissue availability may be improved by some structural modifications or by targeted nano-delivery. Furthermore, toxicological parameters must be checked in this course. The scientific development in this direction is not satisfactory. Future research should focus on pharmacokinetics, targeted nano- delivery, and toxicological parameters of phytochemicals.
References
Doleys DM. Chronic pain as a hypothetical construct: a practical and philosophical consideration. Front Psychol. 2017;8:664.
Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron. 2006;52:77–92.
Cho Y, Lee S, Kim J, Kang JW, Lee JD. Thread embedding acupuncture for musculoskeletal pain: a systematic review and meta-analysis protocol. BMJ Open. 2018;8(1):e015461.
Vardeh D, Naranjo JF. Anatomy and physiology: mechanisms of nociceptive transmission. In: Yong R, Nguyen M, Nelson E, Urman R, editors. Pain medicine. Cham: Springer; 2017.
Basbaum AI, Bautista DM, Scherrer G, Julius D. Cellular and molecular mechanisms of pain. Cell. 2009;137:267–84.
Hossain MZ, Unno S, Ando H, Masuda Y, Kitagawa J. Neuron-glia crosstalk and neuropathic pain: involvement in the modulation of motor activity in the orofacial region. Int J Mol Sci. 2017;18(10):2051.
Wang C, Song S, Zhang Y, Ge Y, Fang X, Huang T, Du J, Gao J. Inhibition of the Rho/Rho kinase pathway prevents lipopolysaccharide-induced hyperalgesia and the release of TNF-α and IL-1β in the mouse spinal cord. Sci Rep. 2015;5:145–53.
Huang PC, Tsai KL, Chen YW, Lin HT, Hung CH. Exercise combined with ultrasound attenuates neuropathic pain in rats associated with downregulation of IL-6 and TNF-α, but with upregulation of IL-10. Anesth Analg. 2017;124(6):2038–44.
Wu Y, Na X, Zang Y, Cui Y, Xin W, Pang R, Zhou L, Wei X, Li Y, Liu X. Upregulation of tumor necrosis factor-alpha in nucleus accumbens attenuates morphine-induced rewarding in a neuropathic pain model. Biochem Biophys Res Commun. 2014;449(4):502–7.
Ferraz CR, Calixto-Campos C, Manchope MF, Casagrande R, Clissa PB, Baldo C, Verri WA Jr. Jararhagin-induced mechanical hyperalgesia depends on TNF-α, IL-1β and NFκB in mice. Toxicon. 2015;103:119–28.
Carvalho TT, Borghi SM, Pinho-Ribeiro FA, Mizokami SS, Cunha TM, Ferreira SH, Cunha FQ, Casagrande R, Verri WA Jr.. Granulocyte-colony stimulating factor (G-CSF)-induced mechanical hyperalgesia in mice: role for peripheral TNFα, IL-1β and IL-10. Eur J Pharmacol. 2015;749:62–72.
McInnes IB, Schett G. Pathogenetic insights from the treatment of rheumatoid Arthritis: Targeted treatments for rheumatoid arthritis 1. Lancet. 2017;389:2328–37.
Lima CK, Silva RM, Lacerda RB, Santos BL, Silva RV, Amaral LS, Quintas LE, Fraga CA, Barreiro EJ, Guimaraes MZ, Miranda AL. LASSBio-1135: a dual TRPV1 antagonist and anti-TNF-alpha compound orally effective in models of inflammatory and neuropathic pain. PLoS One. 2014;9(6):e99510.
Nascimento FP, Macedo-Júnior SJ, Borges FR, Cremonese RP, da Silva MD, Luiz-Cerutti M, Martins DF, Rodrigues AL, Santos AR. Thalidomide reduces mechanical hyperalgesia and depressive-like behavior induced by peripheral nerve crush in mice. Neuroscience. 2015;303:51–8.
Yang Y, Zhang J, Gao Q, Bo J, Ma Z. Etanercept attenuates thermal and mechanical hyperalgesia induced by bone cancer. Exp Ther Med. 2017;13(5):2565–69.
Xu T, Li D, Zhou X, Ouyang HD, Zhou LJ, Zhou H, Zhang HM, Wei XH, Liu G, Liu XG. Oral application of magnesium-l-threonate attenuates vincristine-induced allodynia and hyperalgesia by normalization of tumor necrosis factor-α/nuclear factor-κB signaling. Anesthesiology. 2017;126(6):1151–68.
Jin X, Gereau RW. Acute p38-mediated modulation of tetrodotoxin-resistant sodium channels in mouse sensory neurons by tumor necrosis factor-α. J Neurosci. 2006;26:246–55.
Gruber-Schoffnegger D, Drdla-Schutting R, Hönigsperger C, Wunderbaldinger G, Gassner M, Sandkühler J. Induction of thermal hyperalgesia and synaptic long-term potentiation in the spinal cord lamina I by TNF-α and IL-1β is mediated by glial cells. J Neurosci. 2013;33(15):6540–51.
Ren K, Dubner R. Neuron-glia crosstalk gets serious, role in pain hypersensitivity. Curr Opin Anaesthesiol. 2008;21: 570–79.
Schäfers M, Sorkin LS, Geis C, Shubayev VI. Spinal nerve ligation induces transient upregulation of tumor necrosis factor receptors 1 and 2 in injured and adjacent uninjured dorsal root ganglia in the rat. Neurosci Lett. 2003;347:179–82.
Watkins LR, Maier SF. Glia, a novel drug discovery target for clinical pain. Nat Rev Drug Discov. 2003;2:973–85.
Watkins LR, Hutchinson MR, Milligan ED, Maier SF. “Listening” and “talking” to neurons, implications of immune activation for pain control and increasing the efficacy of opioids. Brain Res Rev. 2007;56:148–69.
Korhonen T, Karppinen J, Paimela L, Malmivaara A, Lindgren KA, Bowman C, Hammond A, Kirkham B, Järvinen S, Niinimäki J, Veeger N, Haapea M, Torkki M, Tervonen O, Seitsalo S, Hurri H. The treatment of disc-herniation-induced sciatica with infliximab, one-year follow-up results of FIRST II, a randomized controlled trial. Spine.2006;31:2759–66.
Cohen SP, Bogduk N, Dragovich A, Buckenmaier CC III, Griffith S, Kurihara C, Raymond J, Richter PJ, Williams N, Yaksh TL. Randomized, double-blind, placebo-controlled, dose-response, and preclinical safety study of transforaminal epidural etanercept for the treatment of sciatica. Anesthesiology. 2009;110:1116–26.
Piccinelli AC, Morato PN, Dos Santos Barbosa M, Croda J, Sampson J, Kong X, Konkiewitz EC, Ziff EB, Amaya-Farfan J, Kassuya CA. Limonene reduces hyperalgesia induced by gp120 and cytokines by modulation of IL-1 β and protein expression in spinal cord of mice. Life Sci. 2017;174:28–34.
Nieto FR, Clark AK, Grist J, Hathway GJ, Chapman V, Malcangio M. Neuron-immune mechanisms contribute to pain in early stages of arthritis. J Neuroinflamm. 2016;13:96.
Economides AN, Carpenter LR, Rudge JS, Wong V, Koehler-Stec EM, Hartnett C, Pyles EA, Xu X, Daly TJ, Young MR, Fandl JP, Lee F, Carver S, McNay J, Bailey K, Ramakanth S, Hutabarat R, Huang TT, Radziejewski C, Yancopoulos GD, Stahl N. Cytokine traps, multi-component, high affinity blockers of cytokine action. Nat Med. 2003;9(1):47–52.
Kawasaki Y, Xu ZZ, Wang X, Park JY, Zhuang ZY, Tan PH, Gao YJ, Roy K, Corfas G, Lo EH, Ji RR. Distinct roles of matrix metalloproteases in the early- and late-phase development of neuropathic pain. Nat Med. 2008;14:331–36.
Opree A, Kress M. Involvement of the protoinflammatory cytokines Tumor Necrosis Factor-α, IL-1β, and IL-6 but not IL-8 in the development of heat hyperalgesia, effects on heat-evoked Calcitonin Gene-Related Peptide release from rat skin. J Neurosci. 2000;20(16):6289–93.
Obreja O, Rathee PK, Lips KS, Distler C, Kress M. IL-1β potentiates heat-activated currents in rat sensory neurons, involvement of IL-1R1, tyrosine kinase, and protein kinase C. FASEB. 2002;16:1497–502.
Safieh-Garabedian B, Poole S, Allchorne A, Winter J, Woolf CJ. Contribution of interleukin-1β to the inflammation-induced increase in nerve growth factor levels and inflammatory hyperalgesia. Br J Pharmacol. 1995;115:1265–75.
Teh DBL, Prasad A, Jiang W, Ariffin MZ, Khanna S, Belorkar A, Wong L, Liu X, All AH. Transcriptome analysis reveals neuroprotective aspects of human reactive astrocytes induced by interleukin 1β. Sci Rep. 2017;7(1):139–88.
Schäfers M, Sorkin L. Effect of cytokines on neuronal excitability. Neurosci Lett. 2008;437:188–93.
Zhou YQ, Liu Z, Liu ZH, Chen SP, Li M, Shahveranov A, Ye DW, Tian YK. Interleukin-6: an emerging regulator of pathological pain. J Neuroinflammation. 2016;13(1):141.
Sanayama Y, Ikeda K, Saito Y, Kagami S, Yamagata M, Furuta S, Kashiwakuma D, Iwamoto I, Umibe T, Nawata Y, Matsumura R, Sugiyama T, Sueishi M, Hiraguri M, Nonaka K, Ohara O, Nakajima H. Prediction of therapeutic responses to tocilizumab in patients with rheumatoid arthritis: biomarkers identified by analysis of gene expression in peripheral blood mononuclear cells using genome-wide DNA microarray. Arthritis Rheumatol. 2014;66:1421–31.
Klein MA, Moller JC, Jones LL. Impaired neuroglial activation in interleukin-6 deficient mice. Glia. 1997;19:227–33.
Ma W, Quirion R. Up-regulation of interleukin-6 induced by prostaglandin E from invading macrophages following nerve injury: an in vivo and in vitro study. J Neurochem. 2005;93:664–73.
St-Jacques B, Ma W. Role of prostaglandin E2 in the synthesis of the proinflammatory cytokine interleukin-6 in primary sensory neurons: an in vivo and in vitro study. J Neurochem. 2011;118:841–54.
Dominguez E, Rivat C, Pommier B, Mauborgne A, Pohl M. JAK/STAT3 pathway is activated in spinal cord microglia after peripheral nerve injury and contributes to neuropathic pain development in rat. J Neurochem. 2008;107:50–60.
Lee KM, Jeon SM, Cho HJ. Interleukin-6 induces microglial CX3CR1 expression in the spinal cord after peripheral nerve injury through the activation of p38 MAPK. Eur J Pain. 2010;14:682.
Fehrenbacher JC, Burkey TH, Nicol GD, Vasko MR. Tumor necrosis factor α and interleukin-1β stimulate the expression of cyclooxygenase II but do not alter prostaglandin E2 receptor mRNA levels in cultured dorsal root ganglion cells. Pain. 2006;113:113–22.
Guay J, Bateman K, Gordon R, Mancini J, Riendeau D. Carrageenan-induced paw edema in rat elicits a predominant prostaglandin E2 (PGE2) response in the central nervous system associated with the induction of microsomal PGE2 synthase-1. J Biol Chem. 2004;279:24866–72.
Veiga AP, Duarte ID, Avila MN, da Motta PG, Tatsuo MA, Francischi JN. Prevention by celecoxib of secondary hyperalgesia induced by formalin in rats. Life Sci. 2004;75:2807–17.
Svensson CI, Yaksh TL. The spinal phospholipasecyclooxygenase- prostanoid cascade in nociceptive processing. Annu Rev Pharmacol Toxicol. 2002;42:553–83.
Popp L, Häussler A, Olliges A, Nüsing R, Narumiya S, Geisslinger G, Tegeder I. Comparison of nociceptive behavior in prostaglandin E, F, D, prostacyclin and thromboxane receptor knockout mice. Eur J Pain. 2009;13(7):691–703.
Seybold VS, Jia YP, Abrahams LG. Cyclooxygenase-2 contributes to central sensitization in rats with peripheral inflammation. Pain. 2003;105:47–55.
Ghilardi JR, Svensson CI, Rogers SD, Yaksh TL, Mantyh PW. Constitutive spinal cyclooxygenase-2 participates in the initiation of tissue injury-induced hyperalgesia. J Neurosci. 2004;24:2727–32.
Araldi D, Ferrari LF, Lotufo CM, Vieira AS, Athié MC, Figueiredo JG, Duarte DB, Tambeli CH, Ferreira SH, Parada CA. Peripheral inflammatory hyperalgesia depends on the COX increase in the dorsal root ganglion. Proc Natl Acad Sci USA. 2013;110(9):3603–8.
Lee WH, Li LL, Chawla A, Hudmon A, Lai YY, Courtney MJ, Hohmann AG. Disruption of nNOS-NOS1AP protein-protein interactions suppresses neuropathic pain in mice. Pain. 2018. https://doi.org/10.1097/j.pain.0000000000001152.
Sun JS, Yang YJ, Zhang YZ, Huang W, Li ZS, Zhang Y. Minocycline attenuates pain by inhibiting spinal microglia activation in diabetic rats. Mol Med Rep. 2015;12(2):2677–82.
Kakita H, Aoyama M, Nagaya Y, Asai H, Hussein MH, Suzuki M, Kato S, Saitoh S, Asai K. Diclofenac enhances proinflammatory cytokine induced phagocytosis of cultured microglia via nitric oxide production. Toxicol Appl Pharmacol. 2013;268:99–105.
Zhou HY, Chen SR, Pan HL. Targeting N-methyl-D-aspartate receptors for treatment of neuropathic pain. Expert Rev Clin Pharmacol. 2011;4(3):379–88.
Wallace MS, Lam V, Schettler J. NGX426, an oral AMPA-kainate antagonist, is effective in human capsaicin-induced pain and hyperalgesia. Pain Med. 2012;13(12):1601–10.
Weyer AD, Lehto SG. Development of TRPM8 Antagonists to Treat Chronic Pain and Migraine. Pharmaceuticals (Basel). 2017;10(2):37.
Chen J, Hackos DH. TRPA1 as a drug target—promise and challenges. Naunyn Schmiedebergs Arch Pharmacol. 2015;388(4):451–63.
Julius D, Basbaum AI. Molecular mechanisms of nociception. Nature. 2001;413: 203–10.
Bautista DM, Movahed P, Hinman A, Axelsson HE, Sterner O, Högestätt ED, Julius D, Jordt SE, Zygmunt PM. Pungent products from garlic activate the sensory ion channel TRPA1. Proc Natl Acad Sci. 2005;102(34):12248–52.
Caterina MJ, Leffler A, Malmberg AB, Martin WJ, Trafton J, Petersen-Zeitz KR, Koltzenburg M, Basbaum AI, Julius D. Impaired nociception and pain sensation in mice lacking the capsaicin receptor. Science. 2000;288(5464):306–13.
Julius D. TRP Channels and Pain. Annu Rev Cell Dev Biol. 2013;29:355–84.
Lumpkin EA, Caterina MJ. Mechanisms of sensory transduction in the skin. Nature. 2007;445(7130):858–65.
Oeckinghaus A, Ghosh S. The NF-kappaB family of transcription factors and its regulation. Cold Spring Harb Perspect Biol. 2009;1:a000034.
Lawrence T. The Nuclear Factor NF-κB Pathway in Inflammation. Cold Spring Harb Perspect Biol. 2009;1(6):a001651.
Karin M, Delhase M. The I kappa B kinase (IKK) and NF-kappa B: key elements of proinflammatory signalling. Semin Immunol. 2000;12:85–98.
Israel A. The IKK complex, a central regulator of NF-kappaB activation. Cold Spring Harb Perspect Biol. 2010;2:a000158.
Sun SC, Liu ZG. A special issue on NF-kappaB signaling and function. Cell Res. 2011;21:1–2.
Sun SC. Non-canonical NF-kappaB signaling pathway. Cell Res. 2011;21:71–85.
Noort AR, Tak PP, Tas SW. Non-canonical NF-κB signaling in rheumatoid arthritis: Dr Jekyll and Mr Hyde? Arthritis Res Ther. 2015;17(1):15.
Yamamoto Y, Gaynor RB. IkappaB kinases: key regulators of the NF-kappaB pathway. Trends Biochem Sci. 2004;29:72–9.
Ma W, Bisby MA. Increased activation of nuclear factor kappa B in rat lumbar dorsal root ganglion neurons following partial sciatic nerve injuries. Brain Res. 1998;797:243–54.
Lee MK, Han SR, Park MK, Kim MJ, Bae YC, Kim SK, Park JS, Ahn DK. Behavioral evidence for the differential regulation of p-p38 MAPK and p-NF-kappaB in rats with trigeminal neuropathic pain. Mol Pain. 2011;7:57.
Hartung JE, Eskew O, Wong T, Tchivileva IE, Oladosu FA, O’Buckley SC, Nackley AG. Nuclear factor-kappa B regulates pain and COMT expression in a rodent model of inflammation. Brain Behav Immun. 2015;50:196–202.
Luo JG, Zhao XL, Xu WC, Zhao XJ, Wang JN, Lin XW, Sun T, Fu ZJ. Activation of spinal NF-kappaB/p65 contributes to peripheral inflammation and hyperalgesia in rat adjuvant-induced arthritis. Arthritis Rheumatol. 2014;66:896–906.
Fu ES, Zhang YP, Sagen J, Yang ZQ, Bethea JR. Transgenic glial nuclear factor-kappa B inhibition decreases formalin pain in mice. Neuroreport. 2008;18:713–7.
Ostenfeld T, Krishen A, Lai RY, Bullman J, Green J, Anand P, Scholz J, Kelly M. A randomized, placebo-controlled trial of the analgesic efficacy and safety of the p38 MAP kinase inhibitor, losmapimod, in patients with neuropathic pain from lumbosacral radiculopathy. Clin J Pain. 2015;31(4):283–93.
Ellis A, Bennett DLH. Neuroinflammation and the generation of neuropathic pain. Br J Anaesth. 2013;111(1):26–37.
Chen NF, Chen WF, Sung CS, Lu CH, Chen CL, Hung HC, Feng CW, Chen CH, Tsui KH, Kuo HM, Wang HM, Wen ZH, Huang SY. Contributions of p38 and ERK to the antinociceptive effects of TGF-β1 in chronic constriction injury-induced neuropathic rats. J Headache Pain. 2016;17(1):72.
Luo X, Fitzsimmons B, Mohan A, Zhang L, Terrando N, Kordasiewicz H, Ji RR. Intrathecal administration of antisense oligonucleotide against p38α but not p38β MAP kinase isoform reduces neuropathic and postoperative pain and TLR4-induced pain in male mice. Brain Behav Immun. 2017;30508(17):889–1591.
Donnerer J, Liebmann I. Upregulation of BDNF and Interleukin-1ß in rat spinal cord following noxious hind paw stimulation. Neurosci Lett. 2017;665:152–5.
Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10(9):895–926.
Zhang X, Zhang H, Shao H, Xue Q, Yu B. ERK MAPK activation in spinal cord regulates phosphorylation of Cdk5 at Serine 159 and contributes to peripheral inflammation induced pain hypersensitivity. PLoS One. 2014;9(1):e87788.
Hensellek S, Brell P, Schaible HG, Bräuer R, Segond von Banchet G. The cytokine TNF-α increases the proportion of DRG neurons expressing the TRPV1 receptor via the TNFR1 receptor and ERK activation. Mol Cell Neurosci. 2007;36: 381–91.
Sanna MD, Ghelardini C, Galeeotti N. Regionally selective activation of ERK and JNK in morphine paradoxical hyperalgesia, A step towards improving opioid pain therapy. Neuropharmacology. 2014;86:67–77.
Skopelja-Gardner S, Saha M, Alvarado-Vazquez PA, Liponis BS, Martinez E, Romero-Sandoval EA. Mitogen-activated protein kinase phosphatase-3 (MKP-3) in the surgical wound is necessary for the resolution of postoperative pain in mice. J Pain Res. 2017;10:763–74.
Gao YJ, Ji RR. c-Fos or pERK, which is a better marker for neuronal activation and central sensitization after noxious stimulation and tissue injury? Open Pain J. 2009;2:11–7.
Singh AK, Vinayak M. Activation of ERK signaling by Src family kinases (SFKs) in DRG neurons contributes to hydrogen peroxide (H2O2) induced thermal hyperalgesia. Free Radic Res. 2017; 51(9–10):838–50.
Singh AK, Vinayak M. Curcumin attenuates CFA induced thermal hyperalgesia by modulation of antioxidant enzymes and down regulation of TNF-α, IL-1β and IL-6. Neurochem Res. 2015;40:463–72.
Singh AK, Vinayak M. Anti-nociceptive effect of resveratrol during inflammatory hyperalgesia via differential regulation of pro-inflammatory mediators. Phytother Res. 2016;30(7):1164–71.
Singh AK, Vinayak M. Resveratrol alleviates inflammatory hyperalgesia by modulation of reactive oxygen species (ROS), antioxidant enzymes and ERK activation. Inflamm Res. 2017. https://doi.org/10.1007/s00011-017-1072-0.
Fosbøl EL, Folke F, Jacobsen S, Rasmussen JN, Sørensen R, Schramm TK, Andersen SS, Rasmussen S, Poulsen HE, Køber L, Torp-Pedersen C, Gislason GH. Cause specific cardiovascular risk associated with nonsteroidal anti-inflammatory drugs among healthy individuals. Circ Cardiovasc Qual Outcomes. 2010;3(4):395–405.
Möller B, Pruijm M, Adler S, Scherer A, Villiger PM, Finckh A. Chronic NSAID use and long term decline of renal function in a prospective rheumatoid arthritis cohort study. Ann Rheum Dis. 2015;74(4):718–23.
Mallick-Searle T, Fillman M. The pathophysiology, incidence, impact, and treatment of opioid-induced nausea and vomiting. J Am Assoc Nurse Pract. 2017;29(11):704–10.
La JH, Wang J, Bittar A, Shim HS, Bae C, Chung JM. Differential involvement of reactive oxygen species in a mouse model of capsaicin-induced secondary mechanical hyperalgesia and allodynia. Mol Pain. 2017. https://doi.org/10.1177/1744806917713907.
Lochhead JJ, McCaffrey G, Sanchez-Covarrubias L, Finch JD, Demarco KM, Quigley CE, Davis TP, Ronaldson PT. Tempol modulates changes in xenobiotic permeability and occludin oligomeric assemblies at the blood-brain barrier during inflammatory pain. Am J Physiol Heart Circ Physiol. 2012;302(3):582–93.
Xu YQ, Jin SJ, Liu N, Li YX, Zheng J, Ma L, Du J, Zhou R, Zhao CJ, Niu Y, Sun T, Yu JQ. Aloperine attenuated neuropathic pain induced by chronic constriction injury via anti-oxidation activity and suppression of the nuclear factor kappa B pathway. Biochem Biophys Res Commun. 2014;451(4):568–73.
Schwartz ES, Lee I, Chung K, Chung JM. Oxidative stress in the spinal cord is an important contributor in capsaicin-induced mechanical secondary hyperalgesia in mice. Pain. 2008;138:514–24.
Di YX, Hong C, Jun L, Renshan G, Qinquan L. Curcumin attenuates mechanical and thermal hyperalgesia in chronic constrictive injury model of neuropathic pain. Pain Ther. 2014;3(1):59–69.
Sharma S, Kulkarni SK, Chopra K. Curcumin, the active principle of turmeric (Curcuma longa), ameliorates diabetic nephropathy in rats. Clin Exp Pharmacol Physiol. 2006;33:940–45.
Cao H, Zheng JW, Li JJ, Meng B, Li J, Ge RS. Effects of curcumin on pain threshold and on the expression of nuclear factor κ B and CX3C receptor 1 after sciatic nerve chronic constrictive injury in rats. Chin J Integr Med. 2014;20(11):850–56.
Li X, Liu RH, Cao H, Li J. Effects of curcumin on behavior and p-ERK, p-CREB, c-fos expression in dorsal root ganglion in chronic constrictive injury rats. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2009;25(3):418–22.
Yeon KY, Kim SA, Kim YH, Lee MK, Ahn DK, Kim HJ, Kim JS, Jung SJ, Oh SB. Curcumin produces an anti- hyperalgesic effect via antagonism of TRPV1. J Dent Res. 2010;89:170–4.
Banafshe HR, Hamidi GA, Noureddini M, Mirhashemi SM, Mokhtari R, Shoferpour M. Effect of curcumin on diabetic peripheral neuropathic pain: possible involvement of opioid system. Eur J Pharmacol. 2014;723:202–6.
Zhu X, Li Q, Chang R, Yang D, Song Z, Guo Q, Huang C. Curcumin alleviates neuropathic pain by inhibiting p300/CBP histone acetyltransferase activity-regulated expression of BDNF and cox-2 in a rat model. PLoS One. 2014;9(3):e91303.
Meng B, Shen LL, Shi XT, Gong YS, Fan XF, Li J, Cao H. Effects of curcumin on TTX-R sodium currents of dorsal root ganglion neurons in type 2 diabetic rats with diabetic neuropathic pain. Neurosci Lett. 2015;605:59–64.
Ji FT, Liang JJ, Liu L, Cao MH, Li F. Curcumin exerts antinociceptive effects by inhibiting the activation of astrocytes in spinal dorsal horn and the intracellular extracellular signal-regulated kinase signaling pathway in rat model of chronic constriction injury. Chin Med J (Engl). 2013;126(6):1125–31.
Zhao WC, Zhang B, Liao MJ, Zhang WX, He WY, Wang HB, Yang CX. Curcumin ameliorated diabetic neuropathy partially by inhibition of NADPH oxidase mediating oxidative stress in the spinal cord. Neurosci Lett. 2014;560:81–5.
Fattori V, Pinho-Ribeiro FA, Borghi SM, Alves-Filho JC, Cunha TM, Cunha FQ, Casagrande R, Verri WA Jr. Curcumin inhibits superoxide anion-induced pain-like behavior and leukocyte recruitment by increasing Nrf2 expression and reducing NF-κB activation. Inflamm Res. 2015;64(12):993–1003.
Zhao X, Xu Y, Zhao Q, Chen CR, Liu AM, Huang ZL. Curcumin exerts antinociceptive effects in a mouse model of neuropathic pain: Descending monoamine system and opioid receptors are differentially involved. Neuropharmacology. 2012;62(2):843–54.
Murakami Y, Ishii H, Takada N, Tanaka S, Machin M, Ito S, Fujisawa S. Comparative anti-inflammatory activities of curcumin and tetrahydrocurcumin based on the phenolic O-H bond dissociation enthalpy, ionization potential and quantum chemical descriptor. Anticancer Res. 2008;28:699–707.
Zhao S, Yang J, Han X, Gong Y, Rao S, Wu B, Yi Z, Zou L, Jia T, Li L, Yuan H, Shi L, Zhang C, Gao Y, Li G, Liu S, Xu H, Liu H, Liang S. Effects of nanoparticle-encapsulated curcumin on HIV-gp120-associated neuropathic pain induced by the P2 × 3 receptor in dorsal root ganglia. Brain Res Bull. 2017;135:53–61.
Li Y, Zhang Y, Liu DB, Liu HY, Hou WG, Dong YS. Curcumin attenuates diabetic neuropathic pain by downregulating TNF-α in a rat model. Int J Med Sci. 2013;10(4):377–81.
Wu Y, Qin D, Yang H, Fu H. Evidence for the Participation of Acid-Sensing Ion Channels (ASICs) in the Antinociceptive Effect of Curcumin in a Formalin-Induced Orofacial Inflammatory Model. Cell Mol Neurobiol. 2017;37(4):635–42.
Yang M, Wang J, Yang C, Han H, Rong W, Zhang G. Oral administration of curcumin attenuates visceral hyperalgesia through inhibiting phosphorylation of TRPV1 in rat model of ulcerative colitis. Mol Pain. 2017;13. https://doi.org/10.1177/1744806917726416.
Hu X, Huang F, Szymusiak M, Tian X, Liu Y, Wang ZJ. PLGA -Curcumin Attenuates Opioid-Induced Hyperalgesia and Inhibits Spinal CaMKIIα. PLoS One. 2016;11(1):e0146393.
Tao L, Ding Q, Gao C, Sun X. Resveratrol attenuates neuropathic pain through balancing pro-inflammatory and anti-inflammatory cytokines release in mice. Int Immunopharmacol. 2016;34:165–72.
Tsai RY, Chou KY, Shen CH, Chien CC, Tsai WY, Huang YN, Tao PL, Lin YS, Wong CS. Resveratrol regulates N-Methyl-D-aspartate receptor expression and suppresses neuroinflammation in morphine-tolerant rats. Anesth Analg. 2012;115(4):944–52.
Shao H, Xue Q, Zhang F, Luo Y, Zhu H, Zhang X, Zhang H, Ding W, Yu B. Spinal SIRT1 activation attenuates neuropathic pain in mice. PLoS One. 2014;9(6):e100938.
Yin Q, Lu FF, Zhao Y, Cheng MY, Fan Q, Cui J, Liu L, Cheng W, Yan CD. Resveratrol facilitates pain attenuation in a rat model of neuropathic pain through the activation of spinal Sirt1. Reg Anesth Pain Med. 2013;38(2):93–9.
Zhao X, Yu C, Wang C, Zhang JF, Zhou WH, Cui WG, Ye F, Xu Y. Chronic resveratrol treatment exerts antihyperalgesic effect and corrects co-morbid depressive like behaviors in mice with mononeuropathy: involvement of serotonergic system. Neuropharmacology. 2014;85:131–41.
Xie J, Liu S, Wu B, Li G, Rao S, Zou L, Yi Z, Zhang C, Jia T, Zhao S, Schmalzing G, Hausmann R, Nie H, Li G, Liang S. The protective effect of resveratrol in the transmission of neuropathic pain mediated by the P2 × 7 receptor in the dorsal root ganglia. Neurochem Int. 2017;103:24–35.
Cheng W, Zhao Y, Liu H, Fan Q, Lu FF, Li J, Yin Q, Yan CD. Resveratrol attenuates bone cancer pain through the inhibition of spinal glial activation and CX3CR1 upregulation. Fundam Clin Pharmacol. 2014;28(6):661–70.
Pham-Marcou TA, Beloeil H, Sun X, Gentili M, Yaici D, Benoit G, Benhamou D, Mazoit JX. Antinociceptive effect of resveratrol in carrageenan-evoked hyperalgesia in rats: Prolonged effect related to COX-2 expression impairment. Pain. 2008;140:274–83.
Torres-López JE, Ortiz MI, Castañeda-Hernández G, Alonso-López R, Asomoza-Espinosa R, Granados-Soto V. Comparison of the antinociceptive effect of celecoxib, diclofenac and resveratrol in the formalin test. Life Sci. 2002;70:1669–76.
Gao ZB, Hu GY. Trans-resveratrol, a red wine ingredient, inhibits voltage-activated potassium current in rat hippocampal neurons. Brain Res. 2005;1056:68–75.
Granados-Soto V, Argüelles C, Ortiz M. The peripheral antinociceptive effect of resveratrol is associated with activation of potassium channels. Neuropharmacology. 2002;43:917–23.
Liew R, Stagg MA, MacLeod KT, Collins P. The red wine polyphenol, resveratrol, exerts acute direct actions on guinea-pig ventricular myocytes. Eur J Pharmacol. 2005;519:1–8.
Yu L, Wang S, Kogure Y, Yamamoto S, Noguchi K, Dai Y. Modulation of TRP channels by resveratrol and other stilbenoids. Mol Pain. 2013;9:1.
Im KH, Kim TH, Song JH. Resveratrol inhibits Na + currents in rat dorsal root ganglion neurons. Brain Res. 2005;1045:134–41.
Tillu DV, Melemedjian OK, Asiedu MN, Qu N, De Felice M, Dussor G, Price TJ. Resveratrol engages AMPK to attenuate ERK and mTOR signaling in sensory neurons and inhibits incision-induced acute and chronic pain. Mol Pain. 2012;8:5.
Wu B, Ma Y, Yi Z, Liu S, Rao S, Zou L, Wang S, Xue Y, Jia T, Zhao S, Shi L, Li L, Yuan H, Liang S. Resveratrol-decreased hyperalgesia mediated by the P2 × 7 receptor in gp120-treated rats. Mol Pain. 2017;13:1744806917707667.
Valério DA, Georgetti SR, Magro DA, Casagrande R, Cunha TM, Vicentini FT, Vieira SM, Fonseca MJ, Ferreira SH, Cunha FQ, Verri WA Jr. Quercetin reduces inflammatory pain: inhibition of oxidative stress and cytokine production. J Nat Prod. 2009;72:1975–9.
Ji C, Xu Y, Han F, Sun D, Zhang H, Li X, Yao X, Wang H. Quercetin alleviates thermal and cold hyperalgesia in a rat neuropathic pain model by inhibiting toll-like receptor signaling. Biomed Pharmacother. 2017;94:652–8.
Azevedo MI, Pereira AF, Nogueira RB, Rolim FE, Brito GA, Wong DV, Lima-Júnior RC, de Albuquerque Ribeiro R, Vale ML. The antioxidant effects of the flavonoids rutin and quercetin inhibit oxaliplatin-induced chronic painful peripheral neuropathy. Mol Pain. 2013;9:53.
Raygude KS1, Kandhare AD, Ghosh P, Ghule AE, Bodhankar SL. Evaluation of ameliorative effect of quercetin in experimental model of alcoholic neuropathy in rats. Inflammopharmacol. 2012;20:331–41.
Gao W, Zan Y, Wang ZJ, Hu XY, Huang F. Quercetin ameliorates paclitaxel-induced neuropathic pain by stabilizing mast cells, and subsequently blocking PKCε-dependent activation of TRPV1. Acta Pharmacol Sin. 2016;37(9):1166–77.
Borghi SM, Pinho-Ribeiro FA, Fattori V, et al. Quercetin inhibits peripheral and spinal cord nociceptive mechanisms to reduce intense acute swimming-induced muscle pain in mice. PLoS One. 2016;11(9):e0162267.
Nie J, Liu X. Quercetin alleviates generalized hyperalgesia in mice with induced adenomyosis. Mol Med Repo. 2017;16(4):5370–76.
Calixto-Campos C, Corrêa MP, Carvalho TT, Zarpelon AC, Hohmann MS, Rossaneis AC, Coelho-Silva L, Pavanelli WR, Pinge-Filho P, Crespigio J1, Bernardy CC, Casagrande R, Verri WA Jr. Quercetin reduces Ehrlich tumor-induced cancer pain in mice. Anal Cell Pathol (Amst). 2015;2015:285708.
Guazelli CFS, Staurengo-Ferrari L, Zarpelon AC, Pinho-Ribeiro FA, Ruiz-Miyazawa KW, Vicentini FTMC., Vignoli JA, Camilios-Neto D, Georgetti SR, Baracat MM, Casagrande R, Verri WA Jr. Quercetin attenuates zymosan-induced arthritis in mice. Biomed Pharmacother. 2018;102:175–84.
Ji JJ, Lin Y, Huang SS, Zhang HL, Diao YP, Li K. Quercetin: a potential natural drug for adjuvant treatment of rheumatoid arthritis. Afr J Tradit Complement Altern Med. 2013;10(3):418–21.
Lee SJ, Han JI, Lee GS, Park MJ, Choi IG, Na KJ, Jeung EB. Antifungal effect of eugenol and nerolidol against Microsporum gypseum in a guinea pig model. Biol Pharm Bull. 2007;30:184–8.
Li HY, Park CK, Jung SJ, Choi SY, Lee SJ, Park K, Kim JS, Oh SB. Eugenol inhibits K + currents in trigeminal ganglion neurons. J Dent Res. 2007;86:898–902.
Yeon KY, Chung G, Kim YH, Hwang JH, Davies AJ, Park MK, Ahn DK, Kim JS, Jung SJ, Oh SB. Eugenol reverses mechanical allodynia after peripheral nerve injury by inhibiting hyperpolarization-activated cyclic nucleotide-gated (HCN) channels. Pain. 2011;152(9):2108–16.
Park CK, Kim K, Jung SJ, Kim MJ, Ahn DK, Hong SD, Kim JS, Oh SB. Molecular mechanism for local anesthetic action of eugenol in the rat trigeminal system. Pain. 2009;144(1–2):84–94.
Park CK, Li HY, Yeon KY, Jung SJ, Choi SY, Lee SJ, Lee S, Park K, Kim JS, Oh SB. Eugenol inhibits sodium currents in dental afferent neurons. J Dent Res. 2006;85:900–4.
Cho JS, Kim TH, Lim JM, Song JH. Effects of eugenol on Na + currents in rat dorsal root ganglion neurons. Brain Res. 2008;1243:53–62.
Hu CY, Zhao YT. Analgesic effects of naringenin in rats with spinal nerve ligation-induced neuropathic pain. Biomed Rep. 2014;2(4):569–73.
Pinho-Ribeiro FA, Zarpelon AC, Fattori V, Manchope MF, Mizokami SS, Casagrande R, Verri WA Jr. Naringenin reduces inflammatory pain in mice. Neuropharmacology. 2016;105:508–19.
Manchope MF, Calixto-Campos C, Coelho-Silva L, Zarpelon AC, Pinho-Ribeiro FA, Georgetti SR, Baracat MM, Casagrande R, Verri WA Jr. Naringenin inhibits superoxide anion-induced inflammatory pain: role of oxidative stress, cytokines, Nrf-2 and the NO-cGMP-PKG-KATP channel signaling pathway. PLoS One. 2016;11(4):e0153015.
Kandhare AD, Raygude KS, Ghosh P, Ghule AE, Bodhankar SL. Neuroprotective effect of naringin by modulation of endogenous biomarkers in streptozotocin induced painful diabetic neuropathy. Fitoterapia. 2012;83(4):650–9.
Hasanein P, Fazeli F. Role of naringenin in protection against diabetic hyperalgesia and tactile allodynia in male Wistar rats. J Physiol Biochem. 2014;70(4):997–1006.
Raposo D, Morgado C, Pereira-Terra P, Tavares I. Nociceptive spinal cord neurons of laminae I-III exhibit oxidative stress damage during diabetic neuropathy which is prevented by early antioxidant treatment with epigallocatechin-gallate (EGCG). Brain Res Bull. 2015;110:68–75.
Kuang X, Huang Y, Gu HF, Zu XY, Zou WY, Song ZB, Guo QL. Effects of intrathecal epigallocatechin gallate, an inhibitor of Toll-like receptor 4, on chronic neuropathic pain in rats. Eur J Pharmacol. 2012;676(1–3):51–6.
Choi JI, Kim WM, Lee HG, Kim YO, Yoon MH. Role of neuronal nitric oxide synthase in the antiallodynic effects of intrathecal EGCG in a neuropathic pain rat model. Neurosci Lett. 2012;510(1):53–7.
Álvarez-Pérez B, Homs J, Bosch-Mola M, Puig T, Reina F, Verdú E, Boadas-Vaello P. Epigallocatechin-3-gallate treatment reduces thermal hyperalgesia after spinal cord injury by down-regulating RhoA expression in mice. Eur J Pain. 2016;20(3):341–52.
Bosch-Mola M, Homs J, Álvarez-Pérez B, Puig T, Reina F, Verdú E, Boadas-Vaello P. (-)-Epigallocatechin-3-gallate antihyperalgesic effect associates with reduced CX3CL1 chemokine expression in spinal cord. Phytother Res. 2017;31(2):340–4.
Groninger H, Schisler RE. Topical Capsaicin for Neuropathic Pain. J Palliat Med. 2012; (8): 946–7.
Anand P, Bley K. Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high concentration capsaicin 8% patch. Br J Anaesthesia. 2011;107(4):490–502.
Borbiro I, Badheka D, Rohacs T. Activation of TRPV1 channels inhibits mechanosensitive Piezo channel activity by depleting membrane phosphoinositides. Sci Signal. 2015;8(363):ra15.
Altier C. Spicing up the sensation of stretch: TRPV1 controls mechanosensitive Piezo channels. Sci Signal. 2015;8(363):fs3.
Bhatia HS, Roelofs N, Muñoz E, Fiebich BL. Alleviation of Microglial Activation Induced by p38 MAPK/MK2/PGE2 Axis by Capsaicin: Potential Involvement of other than TRPV1 Mechanism/s. Sci Rep. 2017;7:116.
de Santana MF, Guimarães AG, Chaves DO, Silva JC, Bonjardim LR, de Lucca Júnior W, Ferro JN, Barreto Ede O, dos Santos FE, Soares MB, Villarreal CF, Quintans Jde S. Quintans-Júnior LJ.The anti-hyperalgesic and anti-inflammatory profiles of p-cymene: Evidence for the involvement of opioid system and cytokines. Pharm Biol. 2015;53(11):1583–90.
Brito RG, Dos Santos PL, Quintans JS, de Lucca Júnior W, Araújo AA, Saravanan S, Menezes IR, Coutinho HD, Quintans-Júnior LJ. Citronellol, a natural acyclic monoterpene, attenuates mechanical hyperalgesia response in mice: evidence of the spinal cord lamina I inhibition. Chem Biol Interact. 2015;239:111–7.
Guimarães AG, Oliveira GF, Melo MS, Cavalcanti SC, Antoniolli AR, Bon-jardim LR, Silva FA, Santos JP, Rocha RF, Moreira JC, Araújo AA, Gelain DP, Quintans-Júnior LJ. Bioassay-guided evaluation of antioxidantand antinociceptive activities of carvacrol. Basic Clin Pharmacol Toxicol. 2010;107:949–57.
Guimarães AG, Scotti L, Scotti MT, Mendonça Júnior FJ, Melo NS, Alves RS, De Lucca Júnior W, Bezerra DP, Gelain DP, Quintans Júnior LJ. Evidence for the involvement of descending pain-inhibitory mechanisms in the attenuation of cancer pain by carvacrol aided through a docking study. Life Sci. 2014;116(1):8–15.
Paula-Freire LI, Andersen ML, Gama VS, Molska GR, Carlini EL. The oral administration of trans-caryophyllene attenuates acute and chronic pain in mice. Phytomedicine. 2014;21(3):356–62.
Trevisan G, Rossato MF, Walker CI, Klafke JZ, Rosa F, Oliveira SM, Tonello R, Guerra GP, Boligon AA, Zanon RB, Athayde ML, Ferreira J. Identification of the plant steroid α-spinasterol as a novel transient receptor potential vanilloid 1 antagonist with antinociceptive properties. J Pharmacol Exp Ther. 2012;343(2):258–69.
Zhang FF, Morioka N, Kitamura T, Fujii S, Miyauchi K, Nakamura Y, Hisaoka-Nakashima K, Nakata Y. Lycopene ameliorates neuropathic pain by upregulating spinal astrocytic connexin 43 expression. Life Sci. 2016;155:116–22.
Goel R, Tyagi N. Potential contribution of antioxidant mechanism in the defensive effect of lycopene against partial sciatic nerve ligation induced behavioral, biochemical and histopathological modification in wistar rats. Drug Res (Stuttg). 2016;66(12):633–8.
Kuhad A, Sharma S, Chopra K. Lycopene attenuates thermal hyperalgesia in a diabetic mouse model of neuropathic pain. Eur J Pain. 2008;12(5):624–32.
Veloso Cde C, Rodrigues VG, Ferreira RC, Duarte LP, Klein A, Duarte ID, Romero TR. Perez Ade C. Tingenone, a pentacyclic triterpene, induces peripheral antinociception due to opioidergic activation. Planta Med. 2014;80(17):1615–21.
de Carvalho Veloso C, Rodrigues VG, Ferreira RC, Duarte LP, Klein A, Duarte ID, Romero TR, de Castro Perez A. Tingenone, a pentacyclic triterpene, induces peripheral antinociception due to NO/cGMP and ATP-sensitive K(+) channels pathway activation in mice. Eur J Pharmacol. 2015;755:1–5.
Dolatshahi M, Farbood Y, Sarkaki A, Mansouri SM, Khodadadi A. Ellagic acid improves hyperalgesia and cognitive deficiency in 6-hydroxidopamine induced rat model of Parkinson’s disease. Iran J Basic Med Sci. 2015;18(1):38–46.
Gauthier ML, Beaudry F, Vachon P. Intrathecal [6]-gingerol administration alleviates peripherally induced neuropathic pain in male Sprague-Dawley rats. Phytother Res. 2013;27(8):1251–4.
Gao Y, Liu H, Deng L, Zhu G, Xu C, Li G, Liu S, Xie J, Liu J, Kong F, Wu R, Li G, Liang S. Effect of emodin on neuropathic pain transmission mediated by P2 × 2/3 receptor of primary sensory neurons. Brain Res Bull. 2011;84(6):406–13.
Sui F, Huo HR, Zhang CB, Yang N, Guo JY, Du XL, Zhao BS, Liu HB, Li LF, Guo SY, Jiang TL. Emodin down-regulates expression of TRPV1 mRNA and its function in DRG neurons in vitro. Am J Chin Med. 2010;38(4):789–800.
Zhao X, Li XL, Liu X, Wang C, Zhou DS, Ma Q, Zhou WH, Hu ZY. Antinociceptive effects of fisetin against diabetic neuropathic pain in mice: Engagement of antioxidant mechanisms and spinal GABAA receptors. Pharmacol Res. 2015;102:286–97.
Zhao X, Wang C, Cui WG, Ma Q, Zhou WH. Fisetin exerts antihyperalgesic effect in a mouse model of neuropathic pain: engagement of spinal serotonergic system. Sci Rep. 2015;5:9043.
Hernandez-Leon A, Fernández-Guasti A, González-Trujano ME. Rutin antinociception involves opioidergic mechanism and descending modulation of ventrolateral periaqueductal grey matter in rats. Eur J Pain. 2016;20(2):274–83.
Cherng CH, Lee KC, Chien CC, Chou KY, Cheng YC, Hsin ST, Lee SO, Shen CH, Tsai RY, Wong CS. Baicalin ameliorates neuropathic pain by suppressing HDAC1 expression in the spinal cord of spinal nerve ligation rats. J Formos Med Assoc. 2014;113(8):513–20.
Valsecchi AE, Franchi S, Panerai AE, Rossi A, Sacerdote P, Colleoni M. The soy isoflavone genistein reverses oxidative and inflammatory state, neuropathic pain, neurotrophic and vasculature deficits in diabetes mouse model. Eur J Pharmacol. 2011;650(2–3):694–702.
Bertozzi MM, Rossaneis AC, Fattori V, Longhi-Balbinot DT, Freitas A, Cunha FQ, Alves-Filho JC, Cunha TM, Casagrande R, Verri WA Jr. Diosmin reduces chronic constriction injury-induced neuropathic pain in mice. Chem Biol Interact. 2017;273:180–9.
Carballo-Villalobos AI, González-Trujano ME, Pellicer F, Alvarado-Vásquez N, López-Muñoz FJ. Central and peripheral anti-hyperalgesic effects of diosmin in a neuropathic pain model in rats. Biomed Pharmacother. 2018;97:310–20.
Meotti FC, Luiz AP, Pizzolatti MG, Kassuya CA, Calixto JB, Santos AR. Analysis of the antinociceptive effect of the flavonoid myricitrin: evidence for a role of the L-arginine-nitric oxide and protein kinase C pathways. J Pharmacol Exp Ther. 2006;316(2):789–96.
Córdova MM, Werner MF, Silva MD, Ruani AP, Pizzolatti MG, Santos AR. Further antinociceptive effects of myricitrin in chemical models of overt nociception in mice. Neurosci Lett. 2011;495(3):173–7.
Zhu Q, Mao LN, Liu CP, Sun YH, Jiang B, Zhang W, Li JX. Antinociceptive effects of vitexin in a mouse model of postoperative pain. Sci Rep. 2016;6:19266.
Borghi SM, Carvalho TT, Staurengo-Ferrari L, Hohmann MS, Pinge-Filho P, Casagrande R, Verri WA Jr. Vitexin inhibits inflammatory pain in mice by targeting TRPV1, oxidative stress, and cytokines. J Nat Prod. 2013;76(6):1141–9.
Visnagri A, Kandhare AD, Chakravarty S, Ghosh P, Bodhankar SL. Hesperidin, a flavanoglycone attenuates experimental diabetic neuropathy via modulation of cellular and biochemical marker to improve nerve functions. Pharm Biol. 2014;52(7):814–28.
Carballo-Villalobos AI, González-Trujano ME, Alvarado-Vázquez N, López-Muñoz FJ. Pro-inflammatory cytokines involvement in the hesperidin antihyperalgesic effects at peripheral and central levels in a neuropathic pain model. Inflammopharmacology. 2017;25(2):265–9.
Hara K, Haranishi Y, Terada T, Takahashi Y, Nakamura M, Sata T. Effects of intrathecal and intracerebroventricular administration of luteolin in a rat neuropathic pain model. Pharmacol Biochem Behav. 2014;125:78–84.
Liu M, Liao K, Yu C, Li X, Liu S, Yang S. Puerarin alleviates neuropathic pain by inhibiting neuroinflammation in spinal cord. Mediators Inflamm. 2014;2014:485927.
Chen L, Chen W, Qian X, Fang Y, Zhu N. Liquiritigenin alleviates mechanical and cold hyperalgesia in a rat neuropathic pain model. Sci Rep. 2014;4:5676.
Aswar M, Kute P, Mahajan S, Mahajan U, Nerurkar G, Aswar U. Protective effect of hesperetin in rat model of partial sciatic nerve ligation induced painful neuropathic pain: an evidence of anti-inflammatory and anti-oxidative activity. Pharmacol Biochem Behav. 2014;124:101–7.
Park MK, Lee HJ, Choi JK, Kim HJ, Kang JH, Lee EJ, Kim YR, Kang JH, Yoo JK, Cho HY, Kim JK, Kim CH, Park JH, Lee CH. Novel anti-nociceptive effects of cardamonin via blocking expression of cyclooxygenase-2 and transglutaminase-2. Pharmacol Biochem Behav. 2014;118:10–5.
Voon FL, Sulaiman MR, Akhtar MN, Idris MF, Akira A, Perimal EK, Israf DA, Ming-Tatt L. Cardamonin (2′,4′-dihydroxy-6′-methoxychalcone) isolated from Boesenbergia rotunda (L.) Mansf. inhibits CFA-induced rheumatoid arthritis in rats. Eur J Pharmacol. 2017;794:127–34.
Sambasevam Y, Omar Farouk AA, Tengku Mohamad TA, Sulaiman MR, Bharatham BH, Perimal EK. Cardamonin attenuates hyperalgesia and allodynia in a mouse model of chronic constriction injury-induced neuropathic pain: Possible involvement of the opioid system. Eur J Pharmacol. 2017;796:32–8.
Wang S, Zhai C, Zhang Y, Yu Y, Zhang Y, Ma L, Li S, Qiao Y. Cardamonin, a novel antagonist of hTRPA1 cation channel, reveals therapeutic mechanism of pathological pain. Molecules. 2016;21(9):E1145.
Jiang W, Wang Y, Sun W, Zhang M. Morin suppresses astrocyte activation and regulates cytokine release in bone cancer pain rat models. Phytother Res. 2017;31(9):1298–304.
Cao FL, Xu M, Wang Y, Gong KR, Zhang JT. Tanshinone IIA attenuates neuropathic pain via inhibiting glial activation and immune response. Pharmacol Biochem Behav. 2015;128:1–7.
Sun S, Yin Y, Yin X, Cao F, Luo D, Zhang T, Li Y, Ni L. Anti-nociceptive effects of Tanshinone IIA (TIIA) in a rat model of complete Freund’s adjuvant (CFA)-induced inflammatory pain. Brain Res Bull. 2012;88(6):581–8.
Ren BX, Ji Y, Tang JC, Sun DP, Hui X, Yang DQ, Zhu XL. Effect of Tanshinone IIA intrathecal injections on pain and spinal inflammation in mice with bone tumors. Genet Mol Res. 2015;14(1):2133–8.
Jiang J, Shen YY, Li J, Lin YH, Luo CX, Zhu DY. (+)-Borneol alleviates mechanical hyperalgesia in models of chronic inflammatory and neuropathic pain in mice. Eur J Pharmacol. 2015;757:53–8.
Zhou HH, Zhang L, Zhou QG, Fang Y, Ge WH. (+)-Borneol attenuates oxaliplatin-induced neuropathic hyperalgesia in mice. Neuroreport. 2016;27(3):160–5.
Nishijima CM, Ganev EG, Mazzardo-Martins L, Martins DF, Rocha LR, Santos AR, Hiruma-Lima CA. Citral: a monoterpene with prophylactic and therapeutic anti-nociceptive effects in experimental models of acute and chronic pain. Eur J Pharmacol. 2014;736:16–25.
Yang L, Li Y, Ren J, Zhu C, Fu J, Lin D, Qiu Y. Celastrol attenuates inflammatory and neuropathic pain mediated by cannabinoid receptor type 2. Int J Mol Sci. 2014;15(8):13637–48.
Popiolek-Barczyk K, Kolosowska N, Piotrowska A, Makuch W, Rojewska E, Jurga AM, Pilat D, Mika J. Parthenolide relieves pain and promotes M2 microglia/macrophage polarization in rat model of neuropathy. Neural Plast. 2015;2015:676473.
Dutra RC, Simão da Silva KA, Bento AF, Marcon R, Paszcuk AF, Meotti FC, Pianowski LF, Calixto JB. Euphol, a tetracyclic triterpene produces antinociceptive effects in inflammatory and neuropathic pain: the involvement of cannabinoid system. Neuropharmacology. 2012;63(4):593–605.
Nieto FR, Cobos EJ, Entrena JM, Parra A, García-Granados A, Baeyens JM. Antiallodynic and analgesic effects of maslinic acid, a pentacyclic triterpenoid from Olea europaea. J Nat Prod. 2013;76(4):737–40.
de Lima FO, Alves V, Barbosa Filho JM, Almeida JR, Rodrigues LC, Soares MB, Villarreal CF. Antinociceptive effect of lupeol: evidence for a role of cytokines inhibition. Phytother Res. 2013;27(10):1557–63.
Goldie M, Dolan S. Bilobalide, a unique constituent of Ginkgo biloba, inhibits inflammatory pain in rats. Behav Pharmacol. 2013;24(4):298–306.
Katsuyama S, Kuwahata H, Yagi T, Kishikawa Y, Komatsu T, Sakurada T, Nakamura H. Intraplantar injection of linalool reduces paclitaxel-induced acute pain in mice. Biomed Res. 2012;33(3):175–81.
Zulazmi NA, Gopalsamy B, Farouk AA, Sulaiman MR, Bharatham BH, Perimal EK. Antiallodynic and antihyperalgesic effects of zerumbone on a mouse model of chronic constriction injury-induced neuropathic pain. Fitoterapia. 2015;105:215–21.
Zulazmi NA, Gopalsamy B, Min JC, Farouk AA, Sulaiman MR, Bharatham BH, Perimal EK. Zerumbone alleviates neuropathic pain through the involvement of l-arginine-nitric oxide-cGMP-K ATP channel pathways in chronic constriction injury in mice model. Molecules. 2017;22(4):E555.
Chia JSM, Omar Farouk AA, Mohamad AS, Sulaiman MR, Perimal EK. Zerumbone alleviates chronic constriction injury-induced allodynia and hyperalgesia through serotonin 5-HT receptors. Biomed Pharmacother. 2016;83:1303–10.
Huang SY, Chen NF, Chen WF, Hung HC, Lee HP, Lin YY, Wang HM, Sung PJ, Sheu JH, Wen ZH. Sinularin from indigenous soft coral attenuates nociceptive responses and spinal neuroinflammation in carrageenan-induced inflammatory rat model. Mar Drugs. 2012;10(9):1899–919.
Huang Q, Mao XF, Wu HY, Li TF, Sun ML, Liu H, Wang YX. Bullatine A stimulates spinal microglial dynorphin A expression to produce anti-hypersensitivity in a variety of rat pain models. J Neuroinflammation. 2016;13(1):214.
Lin YC, Huang SY, Jean YH, Chen WF, Sung CS, Kao ES, Wang HM, Chakraborty C, Duh CY, Wen ZH. Intrathecal lemnalol, a natural marine compound obtained from Formosan soft coral, attenuates nociceptive responses and the activity of spinal glial cells in neuropathic rats. Behav Pharmacol. 2011;22(8):739–50.
Guida F, Luongo L, Aviello G, Palazzo E, De Chiaro M, Gatta L, Boccella S, Marabese I, Zjawiony JK, Capasso R, Izzo AA, de Novellis V, Maione S. Salvinorin A reduces mechanical allodynia and spinal neuronal hyperexcitability induced by peripheral formalin injection. Mol Pain. 2012;8:60.
Wang ML, Yu G, Yi SP, Zhang FY, Wang ZT, Huang B, Su RB, Jia YX, Gong ZH. Antinociceptive effects of incarvillateine, a monoterpene alkaloid from Incarvillea sinensis, and possible involvement of the adenosine system. Sci Rep. 2015;5:16107.
Bhat RA, Lingaraju MC, Pathak NN, Kalra J, Kumar D, Kumar D, Tandan SK. Effect of ursolic acid in attenuating chronic constriction injury-induced neuropathic pain in rats. Fundam Clin Pharmacol. 2016;30(6):517–28.
Zhang Y, Song C, Li H, Hou J, Li D. Ursolic acid prevents augmented peripheral inflammation and inflammatory hyperalgesia in high-fat diet-induced obese rats by restoring downregulated spinal PPARα. Mol Med Rep. 2016;13(6):5309–16.
Gill N, Bijjem KR, Sharma PL. Anti-inflammatory and anti-hyperalgesic effect of all-trans retinoic acid in carrageenan-induced paw edema in Wistar rats: involvement of peroxisome proliferator-activated receptor-β/δ receptors. Indian J Pharmacol. 2013;45(3):278–82.
Maione F, Cantone V, Pace S, Chini MG, Bisio A, Romussi G, Pieretti S, Werz O, Koeberle A, Mascolo N, Bifulco G. Anti-inflammatory and analgesic activity of carnosol and carnosic acid in vivo and in vitro and in silico analysis of their target interactions. Br J Pharmacol. 2017;174(11):1497–508.
Wang YW, Zhang X, Chen CL, Liu QZ, Xu JW, Qian QQ, Li WY, Qian YN. Protective effects of Garcinol against neuropathic pain - Evidence from in vivo and in vitro studies. Neurosci Lett. 2017;647:85–90.
Ahn EJ, Choi GJ, Kang H, Baek CW, Jung YH, Woo YC, Bang SR. Antinociceptive Effects of Ginsenoside Rg3 in a Rat Model of Incisional Pain. Eur Surg Res. 2016;57(3–4):211–23.
Chen SD, Ji BB, Yan YX, He X, Han KY, Dai QX, Zhang MX, Mo YC, Wang JL. Carnosic acid attenuates neuropathic pain in rat through the activation of spinal sirtuin1 and down-regulation of p66shc expression. Neurochem Int. 2016;93:95–102.
Andoh T, Kobayashi N, Uta D, Kuraishi Y. Prophylactic topical paeoniflorin prevents mechanical allodynia caused by paclitaxel in mice through adenosine A1 receptors. Phytomedicine. 2017;25:1–7.
Zhu Q, Sun Y, Yun X, Ou Y, Zhang W, Li JX. Antinociceptive effects of curcumin in a rat model of postoperative pain. Sci Rep. 2014;4:4932.
Xiao L, Ding M, Fernandez A, Zhao P, Jin L, Li X. Curcumin alleviates lumbar radiculopathy by reducing neuroinflammation, oxidative stress and nociceptive factors. Eur Cell Mater. 2017;33:279–93.
Ceyhan D, Kocman AE, Yildirim E, Ozatik O, Aydin S, Aydan K. Comparison of the effects of curcumin, tramadol and surgical treatments on neuropathic pain induced by chronic constriction injury in rat. Turk Neurosurg. 2017. https://doi.org/10.5137/1019-5149.JTN.19824-17.0.
Das L, Vinayak M. Anti-carcinogenic action of curcumin by activation of antioxidant defense system and inhibition of NF -κB signaling in lymphoma-bearing mice. Bioscience Rep. 2012;32:161–70.
Das L, Vinayak M. Curcumin attenuates carcinogenesis by down regulating proinflammatory cytokine interleukin-1 (IL-1α and IL-1β) via modulation of AP-1 and NF-IL6 in lymphoma bearing mice. Int Immunopharmacol. 2014;20(1):141–7.
Das L, Vinayak M. Long term effect of curcumin in restoration of tumour suppressor p53 and phase-II antioxidant enzymes via activation of Nrf2 signalling and modulation of inflammation in prevention of cancer. PLoS One. 2015;10(4):e0124000.
Chen JJ, Dai L, Zhao LX, Zhu X, Cao S, Gao YJ. Intrathecal curcumin attenuates pain hypersensitivity and decreases spinal neuroinflammation in rat model of monoarthritis. Sci Rep. 2015;5:10278.
Sharma S, Kulkarni SK, Agrewala JN, Chopra K. Curcumin attenuates thermal hyperalgesia in a diabetic mouse model of neuropathic pain. Eur J Pharmacol. 2006; 536:256–61.
Kuptniratsaikul V, Dajpratham P, Taechaarpornkul W, Buntragulpoontawee M, Lukkanapichonchut P, Chootip C, Saengsuwan J, Tantayakom K, Laongpech S. Efficacy and safety of Curcuma domestica extracts compared with ibuprofen in patients with knee osteoarthritis: a multicenter study. Clin Interv Aging. 2014;9:451–8.
Arora R, Kuhad A, Kaur IP, Chopra K. Curcumin loaded solid lipid nanoparticles ameliorate adjuvant-induced arthritis in rats. Eur J Pain. 2015;19(7):940–52.
Pieretti S, Ranjan AP, Di Giannuario A, Mukerjee A, Marzoli F, Di Giovannandrea R, Vishwanatha JK. Curcumin-loaded Poly (d, l-lactide-co-glycolide) nanovesicles induce antinociceptive effects and reduce pronociceptive cytokine and BDNF release in spinal cord after acute administration in mice”. Colloids Surf B Biointerfaces. 2017;158:379–86.
Russo GL. Ins and outs of dietary phytochemicals in cancer chemoprevention. Biochem Pharmacol. 2007;74:533–44.
Takeda M, Takehana S, Sekiguchi K, Kubota Y, Shimazu Y. Modulatory mechanism of nociceptive neuronal activity by dietary constituent resveratrol. Int J Mol Sci 2016;17(10):E1702.
Takehana S, Sekiguchi K, Inoue M, Kubota Y, Ito Y, Yui K, Shimazu Y, Takeda M. Systemic administration of resveratrol suppress the nociceptive neuronal activity of spinal trigeminal nucleus caudalis in rats. Brain Res Bull. 2016;120:117–22.
Takehana S, Kubota Y, Uotsu N, Yui K, Iwata K, Shimazu Y, Takeda M. The dietary constituent resveratrol suppresses nociceptive neurotransmission via the NMDA receptor. Mol Pain. 2017;13:1744806917697010.
Sekiguchi K, Takehana S, Shibuya E, Matsuzawa N, Hidaka S, Kanai Y, Inoue M, Kubota Y, Shimazu Y, Takeda M. Resveratrol attenuates inflammation-induced hyperexcitability of trigeminal spinal nucleus caudalis neurons associated with hyperalgesia in rats. Mol Pain. 2016;12:1744806916643082.
Gupta Y, Sharma M, Briyal S. Antinociceptive effect of trans-resveratrol in rats: Involvement of an opioidergic mechanism. Methods Find Exp Clin Pharmacol. 2004;26:667–72.
Doyle T, Bryant L, Muscoli C, Cuzzocrea S, Esposito E, Chen Z, Salvemini D. Spinal NADPH oxidase is a source of superoxide in the development of morphine-induced hyperalgesia and antinociceptive tolerance. Neurosci lett. 2010;483(2):85–9.
Peres Klein C, Rodrigues Cintra M, Binda N, Montijo Diniz D, Gomez MV, Souto AA, de Souza AH. Coadministration of resveratrol and rice oil mitigates nociception and oxidative state in a mouse fibromyalgia-like model. Pain Res Treat. 2016;2016:3191638.
Wang ZM, Chen YC, Wang DP. Resveratrol, a natural antioxidant, protects monosodium iodoacetate-induced osteoarthritic pain in rats. Biomed Pharmacother. 2016;83:763–70.
Han Y, Jiang C, Tang J, Wang C, Wu P, Zhang G, Liu W, Jamangulova N, Wu X, Song X. Resveratrol reduces morphine tolerance by inhibiting microglial activation via AMPK signalling. Eur J Pain. 2014;18(10):1458–70.
Wang LL, Shi DL, Gu HY, Zheng MZ, Hu J, Song XH, Shen YL, Chen YY. Resveratrol attenuates inflammatory hyperalgesia by inhibiting glial activation in mice spinal cords. Mol Med Rep. 2016;13(5):4051–7.
Maurya AK, Vinayak M. Quercetin attenuates cell survival, inflammation, and angiogenesis via modulation of AKT signaling in murine T-Cell lymphoma. Nutr Cancer. 2017;69(3):470–80.
Lee ES, Lee HE, Shin JY, Yoon S, Moon JO. The flavonoid quercetin inhibits dimethylnitrosamine-induced liver damage in rats. J Pharm Pharmacol. 2003;55:1169–74.
Narenjkar J, Roghani M, Alambeygi H, Sedaghati F. The effect of the flavonoid quercetin on pain sensation in diabetic rats. Basic clin neurosci. 2011;2(3):51–7.
Russo GL, Russo M, Spagnuolo C, Tedesco I, Bilotto S, Iannitti R, Palumbo R. Quercetin: a pleiotropic kinase inhibitor against cancer. Cancer Treat Res. 2014;159:185–205.
Filho AW, Filho VC, Olinger L, de Souza MM. Quercetin: further investigation of its antinociceptive properties and mechanisms of action. Arch Pharm Res. 2008;31:713–21.
Borghi SM, Mizokami SS, Pinho-Ribeiro FA, Fattori V, Crespigio J, Clemente-Napimoga JT, Napimoga MH, Pitol DL, Issa JPM, Fukada SY, Casagrande R, Verri WA Jr. The flavonoid quercetin inhibits titanium dioxide (TiO2)-induced chronic arthritis in mice. J Nutr Biochem. 2017;53:81–95.
Britti D, Crupi R, Impellizzeri D, Gugliandolo E, Fusco R, Schievano C, Morittu VM, Evangelista M, Di Paola R, Cuzzocrea. S.A novel composite formulation of palmitoylethanolamide and quercetin decreases inflammation and relieves pain in inflammatory and osteoarthritic pain models. BMC Vet Res. 2017;13(1):229.
Ruiz-Miyazawa KW, Staurengo-Ferrari L, Mizokami SS, Domiciano TP, Vicentini FTMC., Camilios-Neto D, Pavanelli WR, Pinge-Filho P, Amaral FA, Teixeira MM, Casagrande R, Verri WA Jr. Quercetin inhibits gout arthritis in mice: induction of an opioid-dependent regulation of inflammasome. Inflammopharmacology. 2017. https://doi.org/10.1007/s10787-017-0356-x.
Maioli NA, Zarpelon AC, Mizokami SS, Calixto-Campos C, Guazelli CF, Hohmann MS, Pinho-Ribeiro FA, Carvalho TT, Manchope MF, Ferraz CR, Casagrande R, Verri WA Jr. The superoxide anion donor, potassium superoxide, induces pain and inflammation in mice through production of reactive oxygen species and cyclooxygenase-2. Braz J Med Biol Res. 2015;48(4):321–31.
Jeong KH, Lee DS, Kim SR. Effects of eugenol on granule cell dispersion in a mouse model of temporal lobe epilepsy. Epilepsy Res. 2015;115:73–6.
Wang ZJ, Tabakoff B, Levinson SR, Heinbockel T. Inhibition of Nav1.7 channels by methyl eugenol as a mechanism underlying its antinociceptive and anesthetic actions. Acta Pharmacol Sin. 2015;36(7):791–9.
Garabadu D, Shah A, Ahmad A, Joshi VB, Saxena B, Palit G, Krishnamurthy S. Eugenol as an anti-stress agent: modulation of hypothalamic-pituitary-adrenal axis and brain monoaminergic systems in a rat model of stress. Stress. 2011;14(2):145–55.
Gülçin İ. Antioxidant activity of eugenol: a structure-activity relationship study. J Med Food. 2011;14(9):975–85.
Fujisawa S, Atsumi T, Kadoma Y, Sakagami H. Antioxidant and prooxidant action of eugenol-related compounds and their cytotoxicity. Toxicology. 2002;177:39–54.
Walsh SE, Maillard JY, Russell AD, Catrenich CE, Charbonneau DL, Bartolo RG. Activity and mechanisms of action of selected biocidal agents on grampositive and negative bacteria. J Appl Microbiol. 2003;94:240–7.
Lee I, Kim HK, Kim JH, Chung K, Chung JM. The role of reactive oxygen species in capsaicin-induced mechanical hyperalgesia and in the activities of dorsal horn neurons. Pain. 2007;13:9–17.
Lionnet L, Beaudry F, Vachon P. Intrathecal eugenol administration alleviates neuropathic pain in male Sprague-Dawley rats. Phytother Res. 2010;24(11):1645–53.
Ferland CE, Beaudry F, Vachon P. Antinociceptive effects of eugenol evaluated in a monoiodoacetate-induced osteoarthritis rat model. Phytother Res. 2012;26(9):1278–85.
Moreira-Lobo DC, Linhares-Siqueira ED, Cruz GM, Cruz JS, Carvalho-de-Souza JL, Lahlou S, Coelho-de-Souza AN, Barbosa R, Magalhães PJ, Leal-Cardoso JH. Eugenol modifies the excitability of rat sciatic nerve and superior cervical ganglion neurons. Neurosci Lett. 2010;472:220–4.
Wie MB, Won MH, Lee KH, Shin JH, Lee JC, Suh HW, Song DK, Kim YH. Eugenol protects neuronal cells from excitotoxic and oxidative injury in primary cortical cultures. Neurosci Lett. 1997;225:93–6.
Zaveri NT. Green tea and its polyphenolic catechins: medicinal uses in cancer and noncancer applications. Life Sci. 2006;78:2073–80.
Acknowledgements
Authors are thankful to DRDO, India for financial support (Grant no. ERIP/ER/1003851/M/01/1336). Partial financial support by DST-FIST and UGC-CAS program to Department of Zoology, BHU; and UGC-UPE to BHU are also acknowledged.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that there is no conflict of interest.
Additional information
Responsible Editor: John Di Battista.
Rights and permissions
About this article

Cite this article
Singh, A.K., Kumar, S. & Vinayak, M. Recent development in antihyperalgesic effect of phytochemicals: anti-inflammatory and neuro-modulatory actions. Inflamm. Res. 67, 633–654 (2018). https://doi.org/10.1007/s00011-018-1156-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-018-1156-5