
Abstract
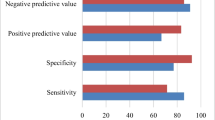
Small intestinal bacterial overgrowth (SIBO) is associated with a variety of gastrointestinal and hepatobilliary diseases. The hydrogen breath test can be used to diagnose malabsorption or intolerance of lactose or fructose, as well as to confirm SIBO. The hydrogen breath test used as a diagnostic tool for SIBO is simple and easy to perform. However, its sensitivity and specificity vary according to the materials used and the method of analysis. In the lactulose breath test, the diagnostic criterion using the early increase in the hydrogen concentration in the exhaled air may produce false positive results when the orocecal transit time is short. The other diagnostic criterion involving the assessment of the two peaks of hydrogen level has the disadvantage of low sensitivity and is not recommended. In the glucose breath test, a false negative result can be a problem when SIBO is present only in the distal small intestine. The choice of methodology may be affected by the suspected location of SIBO and intestinal transit time. Methane gas measurement is important, particularly in patients with constipation. The diagnostic criteria and test methodology to increase sensitivity, indications for use, and relationship of SIBO with patient’s symptoms need to be established.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Breath tests
- Hydrogen; Methane
- Small intestine
- Small intestinal bacterial overgrowth
- Gastrointestinal transit
-
There are many bacteria in the large intestine. In contrast, relatively few bacteria live in the small intestine, particularly in the proximal small intestine.
-
Bacterial overgrowth of the small intestine may occur in various conditions such as irritable bowel syndrome, inflammatory bowel diseases, gastrointestinal motility disorders, hypochlorhydria, immunosuppressed states, gastrointestinal structural abnormalities, liver cirrhosis, and chronic pancreatitis.
-
In the lactulose hydrogen breath test, the criterion that measures an early increase of hydrogen levels in the exhaled air is generally used but may produce false-positive results when the orocecal transit time is short. The glucose hydrogen breath test has the disadvantage that it is not able to diagnose bacterial overgrowth present only in the distal small intestine.
-
Lactose or fructose malabsorption can also be diagnosed using the hydrogen breath test.
Recently, many studies have suggested that many microorganisms are present in the gastrointestinal tract and that the gut microbiota is associated with diverse diseases. The upper gastrointestinal tract has a relatively small number of bacteria due to the influence of gastric acid, but the bacterial number increases when reaching the distal part [1, 2]. The small intestine has a relatively small number of bacteria compared to that in the large intestine. Small intestinal bacterial overgrowth (SIBO), in which the number of bacteria is abnormally increased in the small intestine, is associated with a variety of gastrointestinal and hepatobiliary diseases (Table 1) [3]. Invasive and noninvasive tests are used to diagnose SIBO. Culturing the jejunal aspirates is a relatively invasive method and cannot detect SIBO distal to the jejunum. Moreover, only a part of gut microbiota can be detected by culture. The hydrogen breath test is a simpler and noninvasive method and is commonly used.
The hydrogen breath test can be used to diagnose malabsorption or intolerance of lactose or fructose, as well as to confirm SIBO. This chapter reviews the principle, method, and clinical application of the hydrogen breath test.
Principles
When food materials are digested and fermented by intestinal bacteria, gases such as carbon dioxide, hydrogen, and methane are produced. Those gases diffuse into the systemic circulation and are expired through the lungs. Although carbon dioxide is produced during the metabolic processes of cells as well, hydrogen and methane gases are produced only by bacteria. The hydrogen breath test is a method of measuring the amount of hydrogen in the exhaled air by gas chromatography. Generally, anaerobic bacteria in the large intestine produce hydrogen when they encounter sugars or carbohydrates not absorbed in the small intestine. When the processes related to digestion or absorption of sugars or carbohydrates are disrupted in the small intestine, a large amount of hydrogen is generated in the large intestine. In SIBO, an increase in the number of bacteria in the small intestine, in turn, increases the amount of hydrogen produced in the small intestine. The hydrogen is absorbed through the wall of the small intestine or large intestine, enters the blood vessel, moves to the lungs, and is discharged through exhalation. Therefore, if there are excessive bacteria in the small intestine, the amount of hydrogen gas in the exhaled air increases before the gas reaches the large intestine. If there is absorption failure of a specific carbohydrate, a large amount of hydrogen is produced in the large intestine, causing an abnormal increase of hydrogen in the exhaled air.
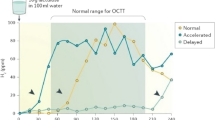
To diagnose SIBO in the small intestine, substances such as lactulose, which are not digested or absorbed in the small intestine, are generally used. In the case of SIBO, the increase in the hydrogen level in the exhaled air can be observed before the gas reaches the large intestine or produces two peaks, one in the small intestine and one in the large intestine. However, when the intestinal transit time is short, the increase in hydrogen level can also be observed early after the ingestion of lactulose, causing a false-positive diagnosis of SIBO.
Approximately 15–30% of people have intestinal flora including Methanobrevibacter smithii. Because this type of bacteria converts hydrogen gas into methane gas, the presence of SIBO or carbohydrate malabsorption does not increase the amount of hydrogen gas in the exhaled air. Instead, the amount of methane gas increases [4]. Therefore, it is recommended to measure methane gas in addition to hydrogen gas to reduce the false-negative diagnosis rate.
Methods
Slowly absorbed carbohydrates and fiber, such as those in bread, vegetables, fruits, pasta, and soybeans, should be avoided from the evening of the day before the test. Drinking water is generally acceptable, but it is recommended to fast for 8–12 h. Sleep, smoking, and exercise are not permitted for at least 1 h before the test, because they affect respiration and may change the amount of hydrogen in the exhaled air. Antibiotics should be avoided for 4 weeks before the breath test. Prokinetics and laxatives should be stopped at least 1 week prior to the breath test. Conclusive data on the discontinuation or continuation of probiotics, motility-reducing agents, and acid inhibitory agents before the test are lacking.
To prevent the early increase in hydrogen concentration owing to the bacteria present in the mouth, brushing the teeth and rinsing the mouth with mouthwash and tap water are recommended before the breath test. After measuring the basal hydrogen concentration in exhalation, patients are asked to orally ingest 10 g of lactulose, 75 g or 1 g/kg of glucose, 25 g of lactose, or 25 g of fructose mixed with 200–250 mL of water as a test material. Exhalation gas is collected in 15 min intervals for 2 h after the ingestion of glucose and for 2–4 h after the ingestion of lactulose. Subsequently, the amount of hydrogen and methane is measured by a commercially available machine (Fig. 1). Samples are collected for at least 3 h after the ingestion of lactose or fructose. The assessment of symptoms during the test is recommended as well. In the lactose tolerance test, the blood glucose level is generally measured in a fasting state and 30 min after the intake of lactose together with the hydrogen breath test [5].

Principles of the hydrogen breath test to diagnose small intestinal bacterial overgrowth
Results
An average basal hydrogen level in the exhaled air above 16 ppm is considered abnormally high, wherein the test should not be carried out. In that situation, pre-treatment should be performed again before the start of the hydrogen breath test. In the hydrogen breath test, SIBO is diagnosed when the hydrogen level is above 20 ppm from the baseline [6]. In the lactulose breath test, the presence of two peaks above 20 ppm from the baseline value may lead to the diagnosis of SIBO. However, the data on the validity of a double peak are lacking [6]. The sensitivity of the glucose hydrogen breath test is 20–93%, indicating a large difference between the reports. Furthermore, SIBO in the distal small intestine that is not accompanied by SIBO in the proximal small intestine cannot be detected by the glucose hydrogen breath test. The lactulose hydrogen breath test also has a low diagnostic sensitivity for SIBO (31–68%) [7, 8]. The diagnostic criteria for the lactulose hydrogen breath test is a result of 20 ppm or higher above the baseline value within 90 min. However, when the orocecal transit time is less than 90 min, those criteria are not suitable. Patients exhibiting the diarrhea subtype of irritable bowel syndrome are considered to have a shorter orocecal transit time due to increased intestinal motility. Asian people are also known to have a shorter orocecal transit time than Western populations. Therefore, the diagnostic criteria using the early increase in the hydrogen level are not likely to be appropriate, particularly in Asia, unless the orocecal transit time is measured simultaneously by a radioisotope-labeled scintigraphic method [9, 10]. A level of 10 ppm or higher over the baseline can be considered positive for the methane breath test [6].
When the hydrogen level in the exhaled air is increased above 20 ppm from the baseline, or the methane level is increased above 10 ppm from the baseline in the lactose or fructose hydrogen breath test, it is considered to indicate malabsorption or intolerance. When the blood glucose level is not increased above 20 mg/dL at 30 min after lactose intake, it is also regarded as malabsorption or intolerance. However, a false-negative result is common [5].
Limitations
There are some limitations in diagnosing SIBO using the hydrogen breath test. The lactulose hydrogen breath test shows different diagnostic sensitivity depending on the diagnostic criteria [7, 8]. In addition, the culture test of the jejunal aspiration is not suitable as a standard test, because only 30% of the gut microorganisms can be cultured and the test site is limited to the proximal small intestine. Because glucose is completely absorbed in the proximal small intestine, bacterial overgrowth of the distal small intestine cannot be diagnosed by the glucose hydrogen breath test. Therefore, the glucose hydrogen breath test may underestimate SIBO prevalence. The lactulose hydrogen breath test is affected by the orocecal transit time. If the transit time is long, the increase of hydrogen level in the exhaled air appears late because it requires a long time to reach the cecum. On the contrary, if the transit time is short, the increase of hydrogen concentration in the exhaled air appears early, which is misdiagnosed as SIBO. Therefore, a combination of the hydrogen breath test with the measurement of the orocecal transit time is desirable. It is suggested that SIBO be diagnosed when the hydrogen level in the exhaled air increases above 5 ppm from the baseline at least 15 min before the radioisotope reaches the cecum when the combination of the lactulose hydrogen breath test and 99mTc-DTPA small intestine transit time test is performed simultaneously [11]. SIBO cannot be detected through the hydrogen breath test if bacteria in the small intestine produce other gases such as methane or hydrogen sulfide without producing hydrogen. The level of methane gas can be measured, but that of the hydrogen sulfide cannot be measured yet. Methane is known to be associated with constipation [12]. The diagnosis of SIBO by the hydrogen breath test does not always guarantee that the symptoms of the patients are caused by SIBO. If symptoms are improved by the treatment of SIBO, the diagnosis is confirmed.
Clinical Applications
Symptoms associated with SIBO are non-specific and the presence of SIBO can be suspected when symptoms are accompanied by conditions that may cause SIBO. The hydrogen breath test is recommended for patients with chronic abdominal symptoms including bloating, gas, and diarrhea, and particularly in those with conditions such as irritable bowel syndrome, inflammatory bowel diseases, gastrointestinal motility disorders, hypochlorhydria, immunosuppressed states, gastrointestinal structural abnormalities, cirrhosis, and chronic pancreatitis.
Conclusion
The hydrogen breath test is a diagnostic tool for SIBO and is simple and easy to perform. However, its sensitivity and specificity vary according to the materials used and the method of analysis. In the lactulose breath test, the diagnostic criterion using the early increase in the hydrogen concentration in the exhaled air is commonly used but may produce false-positive results when the orocecal transit time is short. The other diagnostic criterion involving the assessment of the two peaks of hydrogen level has the disadvantage of low sensitivity and is not recommended. Simultaneous measurement of small intestinal transit time using the radioisotope with the lactulose breath hydrogen test appears to be ideal. In the glucose breath test, a false-negative result can be a problem when SIBO is present only in the distal small intestine. Each methodology has its own advantages and disadvantages. The choice of methodology may be affected by the suspected location of SIBO and intestinal transit time. If SIBO is suspected to be in the proximal small intestine, the glucose hydrogen breath test is recommended. If SIBO is suspected to be in the distal small intestine, the lactulose breath hydrogen test appears to be more appropriate than the glucose hydrogen breath test; however, in that case, consideration of small intestinal transit time may be necessary. Methane gas measurement is important, particularly in patients with constipation. The diagnostic criteria and test methodology to increase sensitivity, indications for use, and relationship of SIBO with patient’s symptoms need to be established.
References
Mackie RI, Sghir A, Gaskins HR. Developmental microbial ecology of the neonatal gastrointestinal tract. Am J Clin Nutr. 1999;69:1035S–45S.
Gabrielli M, D’Angelo G, Di Rienzo T, et al. Diagnosis of small intestinal bacterial overgrowth in the clinical practice. Eur Rev Med Pharmacol Sci. 2013;17(Suppl 2):30–5.
Ghoshal UC, Ghoshal U. Small intestinal bacterial overgrowth and other intestinal disorders. Gastroenterol Clin N Am. 2017;46:103–20.
Levitt MD, Furne JK, Kuskowski M, Ruddy J. Stability of human methanogenic flora over 35 years and a review of insights obtained from breath methane measurements. Clin Gastroenterol Hepatol. 2006;4:123–9.
Babu J, Kumar S, Babu P, Prasad JH, Ghoshal UC. Frequency of lactose malabsorption among healthy southern and northern Indian populations by genetic analysis and lactose hydrogen breath and tolerance tests. Am J Clin Nutr. 2009;91:140–6.
Rezaie A, Buresi M, Lembo A, et al. Hydrogen and methane-based breath testing in gastrointestinal disorders: the north American consensus. Am J Gastroenterol. 2017;112:775–84.
Ghoshal UC, Srivastava D, Ghoshal U, et al. Breath tests in the diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome in comparison with quantitative upper gut aspirate culture. Eur J Gastroenterol Hepatol. 2014;26:753–60.
Khoshini R, Dai SC, Lezcano S, Pimentel M. A systematic review of diagnostic tests for small intestinal bacterial overgrowth. Dig Dis Sci. 2008;53:1443–54.
Ghoshal UC, Ghoshal U, Ayyagari A, et al. Tropical sprue is associated with contamination of small bowel with aerobic bacteria and reversible prolongation of orocecal transit time. J Gastroenterol Hepatol. 2003;18:540–7.
Lu CL, Chen CY, Chang FY, Lee SD. Characteristics of small bowel motility in patients with irritable bowel syndrome and normal humans: an oriental study. Clin Sci (Lond). 1998;95:165–9.
Zhao J, Zheng X, Chu H, et al. A study of the methodological and clinical validity of the combined lactulose hydrogen breath test with scintigraphic oro-cecal transit test for diagnosing small intestinal bacterial overgrowth in IBS patients. Neurogastroenterol Motil. 2014;26:794–802.
Ghoshal UC, Srivastava D, Verma A, Misra A. Slow transit constipation associated with excess methane production and its improvement following rifaximin therapy: a case report. J Neurogastroenterol Motil. 2011;17:48–51.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Lee, K.J. (2022). Principle and Clinical Application of the Hydrogen Breath Test. In: Chun, H.J., Seol, SY., Choi, MG., Cho, J.Y. (eds) Small Intestine Disease. Springer, Singapore. https://doi.org/10.1007/978-981-16-7239-2_31
Download citation
DOI: https://doi.org/10.1007/978-981-16-7239-2_31
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-7238-5
Online ISBN: 978-981-16-7239-2
eBook Packages: MedicineMedicine (R0)