
Abstract
Meniscus root tears are disruptions in the ligamentous portion connecting the meniscus to the tibia. Its clinical presentation, pathophysiology, and treatment have only been explored fairly recently, compared to other meniscus tear types. Meniscus root tears are a unique clinical entity in that tears in this region disrupt the circumferential hoop tension of the whole meniscus, possibly leading to total meniscectomy-like consequences in the knee joint. Recent findings regarding pathophysiology and prognosis suggest that degenerative root tears follow a different clinical course compared to acute tears. A clear understanding of tear pathophysiology is required to accurately diagnose and choose patients that would benefit from surgical repair.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Meniscus root tears are defined as disruptions in the ligament tissue connecting the meniscus to the tibia. Meniscus root tears are a unique clinical entity in that tears in this region disrupt the circumferential hoop tension of the whole meniscus, possibly leading to total meniscectomy-like consequences in the knee joint. Unlike other meniscus tear types, it is only recently that meniscus root tears have been extensively characterized. In this chapter, we will explore recent findings in epidemiology, pathophysiology, and prognosis of meniscus root tears.
Epidemiology
Meniscus root tears most commonly present as medial meniscus posterior root tears, as chronic, degenerative tears associated with knee osteoarthritis. Reports find these tears during 10–21% of arthroscopic meniscus procedures [1,2,3]. The actual incidence of degenerative medial meniscus posterior root tears presenting with other osteoarthritis associated intra-articular pathologies are expected to be much higher, considering that root tears are a common finding in advanced osteoarthritis during total knee arthroplasty. Lateral meniscus posterior root tears on the other hand are less prevalent, found in approximately 3–7% of patients who undergo arthroscopic surgery. The occurrence of these tears increases up to 15% in anterior cruciate ligament deficient knees [1, 4,5,6]. The exact incidence of anterior root tears is unknown, as they are rarely described in the literature.
Anatomy
Grossly, each meniscus has two roots: anterior and posterior root. Each root connects the meniscus body to the tibial plateau. The anterior roots of the medial and lateral menisci are flat and have relatively planar insertions to the tibia. The anterior root of the medial meniscus inserts in line with the medial tibial eminence at an average of 7 mm anterior to the anterior cruciate ligament tibial insertion [7]. The anterior root of the lateral meniscus, on the other hand, inserts anterior to the lateral tibial eminence and adjacent to the insertion of the anterior cruciate ligament [7]. The posterior root of the lateral meniscus inserts posteromedial to the lateral tibial eminence apex and anterior to the posterior cruciate ligament tibial attachment [7]. The posterior root of the medial meniscus inserts posterior to the apex of the medial tibial plateau and anteromedial to the posterior cruciate ligament tibial attachment. The medial meniscus posterior root runs obliquely through its course with its tibial attachment sloping down the tibial edge where posterior cruciate ligament insertion occurs [8]. The posterior, sheet-like fibers of the medial meniscus posterior root have been termed “shiny white fibers” due to their appearance during arthroscopy via posterior portals [9].
Microstructure-wise, the normal meniscus root is a ligament-like structure that differs from fibrocartilage tissue of the meniscus body [10]. Collagen bundles of the meniscal roots mostly run parallel to its longitudinal axis [10]. Meniscus roots are mostly composed of collagen type 3 and collagen type 1 extracellular matrix. The tibial insertions sites exhibit classic enthesis characteristics, with tissue transitioning from ligament tissue to uncalcified and calcified fibrocartilage, and ultimately bone (Fig. 1) [8].

From (Park et al., American Journal of Sports medicine, 2015)
Function of Meniscus Roots
Meniscus roots act to stabilize the meniscus and transmit loads from femoral condyles to tibia [5]. The meniscus contains circumferential collagen fibers that resist extrusion during load bearing from femoral condyles. This resistance toward extrusion is also known as “hoop stress.” Meniscus roots in turn complete the circumferential collagen structure of the meniscus. Consequently, a tear in the posterior root results in a 25% increase in femur-tibia peak contact pressure on the knee, compared to knees with intact roots, similar to a total meniscectomy [5]. This increase in peak contact pressure returns to normal values upon root repair. Root tears also increase external rotation and lateral translation of the tibia relative to the femur and result in varus alignment [11].
Pathophysiology
Root tears occur in two different types of settings, one as a result of an acute traumatic event, and the other as a result of a degenerative process within the knee joint such as osteoarthritis.
Injury resulting in an acute meniscus root tear usually occurs with the knee in hyperflexion, such as during squatting [12]. Medial meniscus posterior root tears have also been associated with multi-ligament knee injuries [13]. Anterior roots and lateral meniscus posterior roots are relatively more mobile compared to medial meniscus posterior roots [14]. Consequently, root tears other than medial meniscus posterior roots are much less commonly encountered [15].
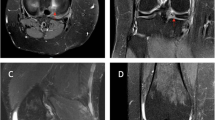
Degenerative root tears, overwhelmingly occurring in the medial meniscus posterior root, have a different pathophysiology compared to acute tears. Risk factors for degenerative root tears of the medial meniscus overlap with those of knee osteoarthritis, including increased age, female sex, increased BMI, varus alignment, and decreased sports activity levels [1,2,3]. Medial meniscus posterior roots also receive more compressive stress and are relatively less mobile compared to other roots due to the root’s firm adhesion with the medial collateral ligament and posterior capsule, making this region more susceptible to chronic tears [14, 16,17,18]. Our recent study characterizing medial meniscus posterior root changes in normal, and untorn, partially torn, and completely torn roots from osteoarthritic knees suggest that the pathophysiology of degenerative medial meniscus roots closely resembles that of degenerative rotator cuff tears [8]. The normal root is devoid of fibrocartilage except in areas of root-to-bone interface. We have found fibrocartilage formation along with other degeneration related markers within the roots correlating with the degree of tear (Fig. 2). Repetitive, compressive stress resulting from osteoarthritic changes may cause ectopic fibrocartilage formation in the root, a known adaptive change in tendons suffering from pathologic compression and impingement. Fibrocartilage formation makes the tissue more resistant to compressive stress, yet less resistant to tensile stress. While the medial meniscus root resists compression stress, the main function is to resist tensile stress from the hoop tension of the meniscus body. The degenerated, fibrocartilage region of the root may, therefore, be more susceptible to tear, usually in a radial direction (Fig. 3). This unique pathophysiology of degenerative root tears is clinically important as the tissue of tear margins differ from acute tears and may not be suitable for repair.

From (Park et al., American Journal of Sports medicine, 2015)

From (Park et al., American Journal of Sports medicine, 2015)
Prognosis
The natural history of root tears is not well-defined. Theoretically, non-operative treatment of meniscus root tears may exacerbate meniscus extrusion and joint space narrowing of the involved compartment. Such prognosis, however, is not always clear. In one study involving patients with degenerative medial meniscus tears, the degree of meniscus extrusion was similar in knees with and without root tears [12]. Another study evaluating subjective knee scores and degree of joint space narrowing in lateral meniscus posterior root tears left untreated during anterior cruciate ligament reconstruction found that there was progression of joint space narrowing of about 1 mm compared to control knees at 10 years follow-up but no difference in subjective scores [19].
Operative treatment for meniscal root tears includes meniscectomy and meniscus root repair. Partial meniscectomy may be indicated in symptomatic patients with chronic root tears and concomitant grade 3–4 cartilage lesions who do not respond to non-operative treatment. In a previous retrospective study assessing 67 patients with a mean follow-up of 56.7 months, partial meniscectomy for medial meniscus posterior root tears resulted in improvement of subjective knee scores but also resulted in progression of radiographic arthritis [3] Another retrospective study comparing 58 patients with medial meniscus root tears who received either partial meniscectomy or root repair showed that although both procedures resulted in subjective knee score improvements, the repair group showed less progression of osteoarthritis at 4 years follow-up [20]. Meniscal root repair, on the other hand, may be indicated in symptomatic patients with acute tears, or with chronic tears that are without severe concomitant cartilage lesions (< grade 3). Several studies have shown subjective knee score improvements, reduction of extrusion, and cessation of degeneration progression in the short term [20,21,22,23,24]. Controversy exists, however, in regard to patient selection, timing of surgery, and method of repair. Not all root repairs heal, as demonstrated in previous studies assessing the repair efficacy by MRI or second look arthroscopy [22, 23]. Further understanding of tear pathogenesis, healing mechanism, and natural history of root tears should improve the overall prognosis of root tear treatment.
References
Bin SI, Kim JM, Shin SJ. Radial tears of the posterior horn of the medial meniscus. Arthroscopy. 2004;20(4):373–8.
Hwang BY, et al. Risk factors for medial meniscus posterior root tear. Am J Sports Med. 2012;40(7):1606–10.
Ozkoc G, et al. Radial tears in the root of the posterior horn of the medial meniscus. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):849–54.
Ahn JH, et al. Double transosseous pull out suture technique for transection of posterior horn of medial meniscus. Arch Orthop Trauma Surg. 2009;129(3):387–92.
Allaire R, et al. Biomechanical consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. J Bone Joint Surg Am. 2008;90(9):1922–31.
Choi CJ, et al. Magnetic resonance imaging evidence of meniscal extrusion in medial meniscus posterior root tear. Arthroscopy. 2010;26(12):1602–6.
Johnson DL, Swenson TM, Livesay GA, Aizawa H, Fu FH, Harner CD. Insertion-site anatomy of the human menisci: gross, arthroscopic, and topographical anatomy as a basis for meniscal transplantation. Arthroscopy. 1995;11(4):386–94.
Park DY, et al. The degeneration of meniscus roots is accompanied by fibrocartilage formation, which may precede meniscus root tears in osteoarthritic knees. Am J Sports Med. 2015;43(12):3034–44.
Anderson CJ, et al. Arthroscopically pertinent anatomy of the anterolateral and posteromedial bundles of the posterior cruciate ligament. J Bone Joint Surg Am. 2012;94(21):1936–45.
Villegas DF, Donahue TL. Collagen morphology in human meniscal attachments: a SEM study. Connect Tissue Res. 2010;51(5):327–36.
Papalia R, et al. Meniscal root tears: from basic science to ultimate surgery. Br Med Bull. 2013;106:91–115.
Lee DH, et al. Predictors of degenerative medial meniscus extrusion: radial component and knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2011;19(2):222–9.
Kim YJ, et al. Posterior root tear of the medial meniscus in multiple knee ligament injuries. Knee. 2010;17(5):324–8.
Bhatia S, et al. Meniscal root tears. Am J Sports Med. 2014;42(12):3016–30.
De Smet AA, et al. MR diagnosis of posterior root tears of the lateral meniscus using arthroscopy as the reference standard. AJR Am J Roentgenol. 2009;192(2):480–6.
Lerer DB, et al. The role of meniscal root pathology and radial meniscal tear in medial meniscal extrusion. Skeletal Radiol. 2004;33(10):569–74.
Vedi, V., et al. Meniscal movement. An in-vivo study using dynamic MRI. J Bone Joint Surg Br. 1999;81(1):37–41.
Tibial meniscal dynamics using three-dimensional reconstruction of magnetic resonance images.pdf.
Shelbourne KD, Roberson TA, Gray T. Long-term evaluation of posterior lateral meniscus root tears left in situ at the time of anterior cruciate ligament reconstruction. Am J Sports Med. 2011;39(7):1439–43.
Kim SB, et al. Medial meniscus root tear refixation: comparison of clinical, radiologic, and arthroscopic findings with medial meniscectomy. Arthroscopy. 2011;27(3):346–54.
Ahn JH, et al. Results of arthroscopic all-inside repair for lateral meniscus root tear in patients undergoing concomitant anterior cruciate ligament reconstruction. Arthroscopy. 2010;26(1):67–75.
Jung YH, et al. All-inside repair for a root tear of the medial meniscus using a suture anchor. Am J Sports Med. 2012;40(6):1406–11.
Kim JH, et al. Arthroscopic suture anchor repair versus pullout suture repair in posterior root tear of the medial meniscus: a prospective comparison study. Arthroscopy. 2011;27(12):1644–53.
Lee JH, et al. Arthroscopic pullout suture repair of posterior root tear of the medial meniscus: radiographic and clinical results with a 2-year follow-up. Arthroscopy. 2009;25(9):951–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Min, B., Park, D.Y. (2021). Root Tear: Epidemiology, Pathophysiology, and Prognosis . In: Kim, J.G. (eds) Knee Arthroscopy. Springer, Singapore. https://doi.org/10.1007/978-981-15-8191-5_19
Download citation
DOI: https://doi.org/10.1007/978-981-15-8191-5_19
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-8190-8
Online ISBN: 978-981-15-8191-5
eBook Packages: MedicineMedicine (R0)