
Abstract
The fanlike extension fibers of the anterior cruciate ligament (ACL) adhere to the bone surface; regardless of the knee flexion angle, the fiber location and orientation do not change, in relation to the femoral surface. However, the ACL midsubstance fiber orientation related to the femur does change during knee motion.
The ACL femoral attachment was divided into a central area of dense fibers, with direct insertion into the femur, and anterior and posterior fanlike extension areas. The central area resisted 82–90 % of the anterior drawer force with the anterior and posterior fanlike areas at 2–3 % and 11–15 %, respectively. Among the 4 central areas, most load was carried close to the roof of the intercondylar notch.
An anatomic variation of the lateral intercondylar ridge (LIR) was identified in 94.0 % of 318 femora and the distal half of LIR was not visible in 18.4 % of these femora. The LIR was situated in the anteriormost part of the lateral condyle surface in 8.8 % and in the posteriormost part in 8.5 %. The ACL attachment anterior margin was typically located anterior to the middle and distal part of LIR.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The size and location of the femoral attachment of ACL are controversial points. Some studies have reported that ACL is attached to a narrow oval-shaped area on the lateral condyle [1–4], while other studies have described that ACL is attached to a wide area on the lateral condyle, and consequently, the posterior attachment margin abuts the articular cartilage margin [5–9]. We have thus performed a series of anatomic studies to clarify this discrepancy [10, 11]. In those studies, the femoral attachment of ACL fibers was found to be composed of two different shapes of fibers: (1) the main attachment of the midsubstance of ACL fibers and (2) the attachment of the thin fibrous tissue (from the midsubstance fibers and spread out like a fan on the posterior condyle). We termed these fibers “fanlike extension fibers” [10]. In addition, all fascicles which make up the midsubstance of ACL were found to attach to the relatively narrow oval area on the lateral condyle [11], although our previous study refers to these morphologies in a static phase, a knee extension position. The purpose of the 1st study was to evaluate the morphology of the midsubstance and fanlike extension fibers of ACL during knee motion with reference to the femoral attachment.
For ACL reconstruction, some have created femoral tunnels in the direct attachment of the midsubstance fibers [2, 12], whereas others have recommended that they should include as much as the whole area including the attachment of the fanlike extension fibers [13, 14]. This discrepancy can occur due to our lack of knowledge on the transmission of the load carried by the ACL to the femoral attachment. In some biomechanical studies in which the ACL was separated into 2 fiber bundles [15] or 3 fiber bundles [16], however, those did not use recent anatomic knowledge of the ACL attachment. The purpose of the second study was to clarify the load-bearing functions of the fibers of the femoral anterior cruciate ligament (ACL) attachment in the resistance of tibial anterior drawer and rotation.
Numerous studies have assessed the positional relationship of an osseous ridge (the resident’s ridge), on the lateral roof of the intercondylar notch with ACL femoral attachment [17–19]. Hutchinson and Ash showed its clinical relevance as a landmark during ACL reconstruction; they described that it was immediately anterior to the ACL attachment [17]. In their description of the “lateral intercondylar ridge” (LIR), Farrow et al. reported that it is distinct in all males but less constant and less distinct in females [18]. Purnell et al. reported that LIR passes from the roof within 3 mm of the articular cartilage edge together with anterior fibers of the ACL attached to the posterior aspect of the ridge [19]. Unfortunately, the focus of these studies was only on the proximal part of LIR. The purpose of the third study was to determine positional variations of LIR and to clarify relationships between both the proximal and distal parts of LIR and the anterior margin of the ACL attachment.
2 Static and Dynamic Observation of the Fanlike Extension Fibers
At full extension, both fiber types were aligned parallel to the intercondylar roof without deviation (Figs. 1.1a and 1.2a). The midsubstance fiber attachment area was observed to be slightly protuberant, compared with that of the fanlike extension fibers (Fig. 1.2a). The seemingly thin and coarse fanlike extension fibers came into contact with the margin of articular cartilage (Fig. 1.2b). In the application of tension to the midsubstance fibers, the tension appeared to be distributed to the fanlike extension fibers. It was impossible to define a distinct border between the midsubstance and fanlike extension fibers.

Midsubstance and fanlike extension fibers during flexion–extension of the knee (From [20] with permission)
(a) Full extension: Both fiber types were aligned parallel to the intercondylar roof without curving
(b) 15° flexion: The midsubstance fibers were found to curve slightly (arrowhead) at the postero-proximal edge of the direct attachment of the midsubstance fibers (according to 30° flexion with apparent fold).
(c) At 30° flexion: The midsubstance fiber degree of the curving was increased.
(d) At 45° flexion: The ACL fiber curving showed an obvious fold.
(e) At 60° flexion: The midsubstance fibers showed some twisting, and the fold deepened, particularly at the postero-distal portion.
(f) At 90° flexion: The whole fold was deeper in the thin space between the midsubstance fibers and the femoral condyle

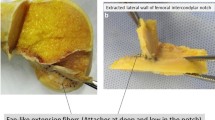
Static observation of the midsubstance and fanlike extension fibers at full extension and at 30° of knee flexion (From [20] with permission)
(a) Both fiber types were aligned parallel to the intercondylar roof without curving.
(b) High-magnification view of ACL fibers on the lateral condyle medial wall. The fanlike extension fibers extended to the margin of articular cartilage (arrowheads) and tended to adhere to the medial wall; they became relatively sparse as they approached the articular cartilage.
(c) The midsubstance fibers were curved (arrowhead) and changed direction from the fanlike extension fibers
(d) High-magnification view of ACL fibers on the lateral condyle medial wall. The fanlike extension fibers adhered to the bone surface, with no change in fiber location or orientation in relation to the bone surface, while the orientation of midsubstance fibers did change with knee flexion. Arrowheads indicate the articular margin
With knee flexion of 15 and 30°, the midsubstance fibers were slightly curved anterior to the articular cartilage of the lateral condyle (Fig. 1.1b, c). The border between the midsubstance fibers and the fanlike extension fibers was then distinct (Fig. 1.2c). The location and orientation of the fanlike extension fibers, in relation to the femoral condyle surface, did not change, due to adherence to the bone surface (Fig. 1.2d).
With knee flexion of 45 and 60°, the curved area of the ACL fibers became an obvious fold on the approximate line between the postero-proximal outlet point of the intercondylar edge and the postero-distal edge of the midsubstance attachment of the PL bundle (Fig. 1.1d, e). At 90°, the depth of the fold increased (Fig. 1.1f). Tension applied to the midsubstance fibers was not distributed to the fanlike extension fibers, due to the presence of the fold.
The attachment of the midsubstance fibers was significantly smaller than that of the fanlike extension fibers. The fold ratio (midsubstance attachment/whole ACL attachment) was 63.7 % (47.3–80.2 %). The attachment area of the fanlike extension fibers was approximately twofold the midsubstance fibers.
3 Histological Observation of Fiber Orientation
With the knee at full extension, the histological sections indicated that the AM bundle of the midsubstance fibers was attached adjacent to the proximal outlet of the intercondylar notch. The postero-proximal edge of the attachment made contact with the margin of the articular cartilage. The thin fanlike extension fibers extended from the midsubstance fibers of the PL bundle and attached to the postero-proximal aspect of the lateral condyle and extended to the articular cartilage of the lateral condyle.
With knee flexion at 120°, a fold in the midsubstance fibers was noted several millimeters from the bone surface (Fig. 1.3a–d). The thin fanlike extension fibers adhered to the bone surface in the same manner as that observed in the full extension position. The angle between the fanlike extension fibers and the midsubstance fibers was ≥90°. The area between the collagen fibers and the bone in the midsubstance fiber insertion comprised a cartilaginous zone, despite that almost all collagen fibers were directly attached to the bone in the fanlike extension fiber insertion and a cartilaginous tissue was rarely seen between them.

Histological observation of fiber orientation of the two fiber types at 120° flexion (From [20] with permission)
The left indicates 4 oblique-axial section planes parallel to the intercondylar roof.
The fold (black arrowheads) was observed at the border between the midsubstance fibers and the fanlike extension fibers, several millimeters away from the bone surface (a–d). The thin fanlike extension fibers adhered to the bone surface of the lateral condyle. The insertion of the midsubstance fibers tends to involve the cartilaginous zone between collagen fibers and bone surface. The fanlike extension fibers tend to insert into the bone without forming transitional cartilaginous zone
4 Fiber Function in the ACL Femoral Attachment
A sequential cutting study was performed on 8 fresh-frozen human knees. The femoral attachment of the ACL was divided into a central area of dense fibers which directly inserted into the femur and into the anterior and posterior fanlike extension areas (Fig. 1.4). The ACL fibers were cut sequentially from the bone in 2, 4, and 2 stages in the posterior fanlike area, the central dense area, and the anterior fanlike area, respectively. Each knee was mounted in a robotic joint testing system at 0–90 of flexion; tibial anteroposterior 6 mm translations and 10 or 15 of internal rotation were applied. The reduction in restraining force or moment was measured after each cut.

Femoral ACL attachment partition on lateral wall of intercondylar notch. The outer lines are tangent to the ACL attachment and oriented parallel to Blumensaat’s line or a line between the centers of the 2 fiber bundles of the ACL (anteromedial and posterolateral). Areas A, B, C, and D comprise the posterior fanlike extension; areas E, F, G, and H comprise the central direct attachment area; and areas I, J, K, and L comprise the anterior fanlike extension (From [26] with permission)
The midsubstance fibers of the ACL (the central attachment areas E, F, G, and H in Fig. 1.4) transmitted 82–90 % of the resistance to tibial displacement and that the large contribution of the central attachment fibers was biased strongly toward the roof of the femoral intercondylar notch. The fibers attached to areas G and H in Fig. 1.4, which corresponded to part of the AM bundle, provided from 66 to 84 % of the total resistance to anterior drawer across 0–90 of flexion (Fig. 1.5). The contribution of fiber attachment areas E and F in Fig. 1.4, which corresponded to part of the PL bundle, fell from 16 % at 0 to 9 % at 90. These changes reflected the slackening of the more posterior ACL fibers with knee flexion, which allowed more of the load to fall onto area H, which was “close to isometric.” Similarly, the posterior fanlike extension attachment fibers (areas A, B, C, and D in Fig. 1.4), which form a large part of the attachment area, contributed 15 % of the resistance to tibial anterior translation in the extended knee, falling to 11 % at 90 (Figs. 1.5 and 1.6).

The percentage contribution of each area to a 6 mm anterior tibial translation (force of the anterior cruciate ligament in intact knee was considered 100 %). The percentage contribution of zones E and F and zones G and H approximately shows that of the posterolateral and anteromedial bundle attachments, respectively. The percentage contribution of zones G and H was markedly greater at each angle of knee flexion (P < .05) compared with other angles (asterisks). # Significant differences (P < .05) compared with areas E and F (From [26] with permission)

Evaluation of the anterior margin of the ACL and LIR via micro-CT evaluation
(a) The medial femoral condyles and much of the notch roof have been removed. ACL is retracted posteriorly. A radiopaque silicon marker is on the anterior margin line of the femoral ACL attachment.
(b) In 15 of the 20 knees, the anterior margin line of the ACL, indicated by the marker, was straight (type 1) such that the marker–ridge distance was longest (mean, 4.5 mm) at the most distal part of the lateral intercondylar ridge (LIR). White arrow, resident’s ridge; white arrowheads, LIR; black arrow, intercondylar notch outlet.
(c) In the remaining 5 knees, the anterior margin line of the ACL was curved (type 2) such that the marker–ridge distance was greatest (mean, 2.8 mm) in the middle part of LIR (From [32] with permission)
5 Anatomic Variations of the Lateral Intercondylar Ridge
A total 318 feomora were examined to determine anatomic variations of the LIR. In addition, 20 cadavers knees, in which the anterior margin was marked by radiopaque silicon markers, were examined with micro-computed tomography to evaluate the positional relationship between LIR and the anterior margin of the ACL attachment.
Although LIR was identified in 94.0 % of the 318 femora (Table 1.1), the distal half of LIR was not visible in 18.4 % of these femora. LIR was single in 96.3 %, whereas 2 and 3 ridges were identified in 3.3 % and 0.3 %, respectively. Moreover, LIR was located in the anteriormost part of the lateral condyle surface in 8.8 % in comparison with the common location and in a markedly posterior part in 8.5 %. The length–height ratio (69.9 % in men, 63.6 % in women) and the length between the inlet of the notch roof and the proximal part of LIR (19.9 mm in men, 17.9 mm in women) were significantly greater in males than in females (P = .0028 and P < .0001, respectively) (Table 1.1). The anterior margin of the ACL attachment was commonly located anterior to the middle and distal part of LIR, having the mean marker–ridge distance of 4.2 mm.
6 Discussion
6.1 Anatomy of the Midsubstance and Fanlike Extension Fibers
The most important finding of the present study [20] was that because the fanlike extension fibers adhered to the bone surface, the fiber location and orientation in relation to the femoral surface did not change, regardless of the knee flexion angle, while orientation of the midsubstance fibers in relation to the femur did change during knee motion. These two different structures formed a fold, observed in knee flexion, at the border between the midsubstance fibers and the fanlike extension.
There have been no reports in which fanlike extension fibers were observed in knee flexion positions, although a few anatomic studies histologically have observed fanlike extension fibers only at the full extension position [10, 21, 22]. The insertion of the midsubstance fibers involved cartilaginous zone, which is regarded as the direct insertion [23]. On the other hand, the fanlike extension fibers were directly attached to the bone without forming a transitional cartilaginous zone, which is regarded as the indirect insertion [24]. Sasaki et al. reported similar observations concerning the femoral attachment of the ACL [22]. This study performed at various flexion positions provided new information, which is critical to the understanding of the mechanism of the above-described fold formation, but also in consideration of the function of the fanlike extension fibers.
This study demonstrated the two types of attachment margins of ACL: (1) the relatively narrow oval attachment margin of the midsubstance fibers of ACL and (2) the broader attachment margin of the fanlike extension fibers. The previous studies were thus confirmed regarding the correct information on a part of the ACL attachment. Those previous studies might have observed one or both of these two attachment margins.
This study also showed that a deep fold was formed in the postero-proximal aspect of the midsubstance fibers several millimeters from the bone surface as the knee was flexed. To date, no other study has described this phenomenon or considered its functional significance. Interestingly, some previous studies report the fold formation can be noted in a few ACL photographs, taken at a knee flexion position [4, 5, 9, 25], although no discussion of this phenomenon was included. The above-described anatomic results suggested that the load distribution mechanism from the ACL midsubstance to the femur is more complex than previously thought. At the full extension position, some of the load is widely distributed to the fanlike extension fibers. As the knee is flexed, it is the midsubstance fibers that may play a more important role than the fanlike extension fibers.
6.2 Fiber Function in the Femoral Attachment
This biomechanical study [26], under the specific experimental conditions, yielded the following: the central area resisted 82–90 % of the anterior drawer force; the anterior fanlike area, 2–3 %; and the posterior fanlike area, 11–15 %. Among the 4 central areas with 0–90 of flexion, most load was carried close to the roof of the intercondylar notch: the anteromedial and posterolateral bundles resisted 66–84 % and 16–9 % of the force, respectively.
Our study suggests that in ACL reconstruction, the most important fibers to resist tibial anterior displacement attach to the central/proximal part of the femoral attachment; this would correspond to the AM fiber bundle [4]. With knee flexion, the contribution of the postero-distal ACL was reduced, thereby further concentrating the load onto the anteroproximal area. This behavior is in line with ACL isometry and fiber length change patterns [16, 27, 28].
The mechanical findings of this study are in agreement with observations of the higher-density collagen fibers in the more anterior area of ACL [29, 30], which matches the variation of tensile material properties [31] as well as the microscopic morphology of direct fiber insertions into the bone in the central band of the femoral attachment [10, 11, 20–22]. In contrast, these data pose the question of the function of the fanlike extension areas, since these areas seem to carry very little load though they occupy a considerable portion of the attachment area.
6.3 Anatomic Variations of LIR
This study [32] highlighted the great degree of variation (both positional and dimensional) in LIR. The distal half of LIR, when present, was not visible in 18.4 %. LIR was single in 96.3 %, whereas there were 2 and 3 ridges in 3.3 % and 0.3 %, respectively. Second, there were significant positional and dimensional LIR differences between male and female femora. Third, despite that the LIR proximal area showed relative correspondence with the ACL attachment anterior margin, micro-CT analysis showed that the ACL attachment anterior margin was commonly located anterior to the LIR middle and distal parts.
Farrow et al. reported that LIR was present in 194 of 200 human femora (97 %). However, they also described that LIR was visible in only 95 of the 194 femora, whereas the remaining 99 (51 %) did not have a visibly elevated ridge [33]. Further, they revealed a significant variation in the anatomy of LIR. Thus, their 2 studies indicated that LIR, particularly the distal part, has a great degree of positional and dimensional variation [18].
Considering LIR and ACL attachments, it has been believed that LIR completely corresponds to the anterior margin line of the ACL attachment [7, 17, 19, 21]. Hutchinson and Ash, in canted cross-sectional sagittal section observations of distal femur specimens, described that the resident’s ridge is located just anterior to the ACL femoral attachment [17]. However, they did not report any measurements or observe the distal part of LIR. Ferretti et al., in 3-D laser camera assessment of osseous landmarks, reported no ACL attachment anterior to LIR [7], although they did not observe LIR and the ACL attachment in the anterior border simultaneously. Purnell et al. used high-resolution CT scan simultaneous observation of LIR and the ACL attachment by Hounsfield unit scale control [19]. However, this method may incorrectly identify the anterior margin of the ACL because the ACL attaches to the femur by “direct” insertion (4 layers of bone, calcified cartilage, noncalcified cartilage, and fibrous tissues) [20–22]. Therefore, it is often difficult to simultaneously visualize the ACL attachment and LIR via control of the Hounsfield unit scale of CT. In the present study, micro-CT (a well-recognized scientific tool) was used to simultaneously visualize both LIR and ACL attachment. In addition, the radiopaque line marker (anterior margin of the ACL attachment) confirmed the relationship between the micro-CT image and the surgeon’s observation. Therefore, this is the first study to employ simultaneous observation of the whole LIR and the complete ACL attachment anterior margin.
7 Clinical Relevance Based on These Studies
This anatomic study [20] on the fanlike extension fibers and midsubstance fibers indicated the difficulty to reconstruct the natural function of the fanlike extension fibers by creating a tunnel at the ends of each fiber bundle, although the midsubstance fibers can be reconstructed in such a fashion. It also provided critical biomechanical study data [26] which clarified fanlike extension fiber biomechanics and also facilitated the creation of mathematical models of ACL. Our biomechanical study [26] also did not support the method of covering the entire ACL attachment area with a graft [34]. Second, considering anterior laxity, the results suggest that the femoral tunnel of single-bundle ACL reconstruction in the central/proximal area would most closely mimic the natural restraint. Data do not confirm reconstruction of a central “anatomic single bundle” [35, 36]. As for double-bundle ACL reconstruction, this study indicated the creation of two femoral tunnels in the central/proximal and central/distal areas, where the ACL attachment is most dense.
Recently, though some studies recommend creation of a femoral tunnel to reconstruct the AM bundle of the ACL [13, 37], such a method may not achieve reconstruction of the normal ACL in terms of function and morphology for the following reasons. The fanlike extension fibers contributed only 15 % of the resistance to tibial anterior translation in the extended knee, and 11 % at 90. Further, it would be difficult to reconstruct the natural morphology. However, it is the midsubstance fibers of the ACL that transmitted 82–90 % of the resistance to tibial displacement; they can be reconstructed by such tunnel creation.
Regarding LIR variations, LIR may be useful as an osseous landmark for conventional single-bundle reconstruction, as previously reported [17, 18, 33]. However, even the proximal part of LIR has great variations, and thus, knowledge and skills are critical to determine the appropriate tunnel location when encountering a knee with an invisible ridge or a ridge in an untypical position. Most noteworthy is that the present study indicates that use of LIR as an osseous landmark is limited in femoral tunnel creation for anatomic single- and double-bundle reconstructions, and due to the great variations, it is often difficult for surgeons to determine an appropriate tunnel position using LIR as a bony landmark in these reconstruction procedures.
References
Girgis FG, Marshall JL, Monajem A (1975) The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res 106:216–231
Yasuda K, Kondo E, Ichiyama H, Kitamura N, Tanabe Y, Tohyama H, Minami A (2004) Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy 20(10):1015–1025. doi:10.1016/j.arthro.2004.08.010
Takahashi M, Doi M, Abe M, Suzuki D, Nagano A (2006) Anatomical study of the femoral and tibial insertions of the anteromedial and posterolateral bundles of human anterior cruciate ligament. Am J Sports Med 34(5):787–792
Edwards A, Bull AMJ, Amis AA (2008) The attachments of the anteromedial and posterolateral fibre bundles of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 16(1):29–36
Odensten M, Gillquist J (1985) Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. J Bone Joint Surg Am 67(2):257–262
Harner CD, Baek GH, Vogrin TM, Carlin GJ, Kashiwaguchi S, Woo SLY (1999) Quantitative analysis of human cruciate ligament insertions. Arthroscopy 15(7):741–749
Ferretti M, Ekdahl M, Shen W, Fu FH (2007) Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthroscopy 23(11):1218–1225
Zantop T, Wellmann M, Fu FH, Petersen W (2008) Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction. Am J Sports Med 36(1):65–72
Otsubo H, Shino K, Suzuki D, Kamiya T, Suzuki T, Watanabe K, Fujimiya M, Iwahashi T, Yamashita T (2012) The arrangement and the attachment areas of three ACL bundles. Knee Surg Sports Traumatol Arthrosc 20(1):127–134. doi:10.1007/s00167-011-1576-z
Mochizuki T, Muneta T, Nagase T, Shirasawa S, Akita K, Sekiya I (2006) Cadaveric knee observation study for describing anatomic femoral tunnel placement for two-bundle anterior cruciate ligament reconstruction. Arthroscopy 22(4):356–361
Hara K, Mochizuki T, Sekiya I, Yamaguchi K, Akita K, Muneta T (2009) Anatomy of normal human anterior cruciate ligament attachments evaluated by divided small bundles. Am J Sports Med 37(12):2386–2391
Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL (2002) Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med 30(5):660–666
Shino K, Nakata K, Nakamura N, Toritsuka Y, Horibe S, Nakagawa S, Suzuki T (2008) Rectangular tunnel double-bundle anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft to mimic natural fiber arrangement. Arthroscopy 24(10):1178–1183. doi:10.1016/j.arthro.2008.06.010
Forsythe B, Kopf S, Wong AK, Martins CA, Anderst W, Tashman S, Fu FH (2010) The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am 92(6):1418–1426. doi:10.2106/JBJS.I.00654
Sakane M, Fox RJ, Woo SL, Livesay GA, Li G, Fu FH (1997) In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. J Orthop Res 15(2):285–293. doi:10.1002/jor.1100150219
Amis A, Dawkins G (1991) Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries. J Bone Joint Surg Br 73(2):260–267
Hutchinson MR, Ash SA (2003) Resident’s ridge: assessing the cortical thickness of the lateral wall and roof of the intercondylar notch. Arthroscopy 19(9):931–935
Farrow LD, Gillespie RJ, Victoroff BN, Cooperman DR (2008) Radiographic location of the lateral intercondylar ridge: its relationship to Blumensaat’s line. Am J Sports Med 36(10):2002–2006. doi:10.1177/0363546508317413
Purnell ML, Larson AI, Clancy W (2008) Anterior cruciate ligament insertions on the tibia and femur and their relationships to critical bony landmarks using high-resolution volume-rendering computed tomography. Am J Sports Med 36(11):2083–2090
Mochizuki T, Fujishiro H, Nimura A, Mahakkanukrauh P, Yasuda K, Muneta T, Akita K (2014) Anatomic and histologic analysis of the mid-substance and fan-like extension fibers of the anterior cruciate ligament during knee motion, with special reference to the femoral attachment. Knee Surg Sports Traumatol Arthrosc 22(2):336–344
Iwahashi T, Shino K, Nakata K, Otsubo H, Suzuki T, Amano H, Nakamura N (2010) Direct anterior cruciate ligament insertion to the femur assessed by histology and 3-dimensional volume-rendered computed tomography. Arthroscopy 26(9):S13–S20
Sasaki N, Ishibashi Y, Tsuda E, Yamamoto Y, Maeda S, Mizukami H, Toh S, Yagihashi S, Tonosaki Y (2012) The femoral insertion of the anterior cruciate ligament: discrepancy between macroscopic and histological observations. Arthroscopy 28(8):1135–1146. doi:10.1016/j.arthro.2011.12.021
Schneider H (1956) Structure of tendon attachments. Z Anat Entwicklungsgesch 119:431–456 (in German)
Benjamin M, Evans EJ, Copp L (1986) The histology of tendon attachments to bone in man. J Anat 149:89–100
Ziegler CG, Pietrini SD, Westerhaus BD, Anderson CJ, Wijdicks CA, Johansen S, Engebretsen L, LaPrade RF (2011) Arthroscopically pertinent landmarks for tunnel positioning in single-bundle and double-bundle anterior cruciate ligament reconstructions. Am J Sports Med 39(4):743–752
Kawaguchi Y, Kondo E, Takeda R, Akita K, Yasuda K, Amis AA (2015) The role of fibers in the femoral attachment of the anterior cruciate ligament in resisting tibial displacement. Arthroscopy 31(3):435–444. doi:10.1016/j.arthro.2014.08.033
Hefzy MS, Grood ES, Noyes FR (1989) Factors affecting the region of most isometric femoral attachments. Part II: the anterior cruciate ligament. Am J Sports Med 17(2):208–216
Sidles JA, Larson RV, Garbini JL, Downey DJ, Matsen FA 3rd (1988) Ligament length relationships in the moving knee. J Orthop Res 6(4):593–610. doi:10.1002/jor.1100060418
Mommersteeg TJ, Blankevoort L, Kooloos JG, Hendriks JC, Kauer JM, Huiskes R (1994) Nonuniform distribution of collagen density in human knee ligaments. J Orthop Res 12(2):238–245. doi:10.1002/jor.1100120213
Petersen W, Tillmann B (1999) Structure and vascularization of the cruciate ligaments of the human knee joint. Anat Embryol (Berl) 200(3):325–334
Butler DL, Guan Y, Kay MD, Cummings JF, Feder SM, Levy MS (1992) Location-dependent variations in the material properties of the anterior cruciate ligament. J Biomech 25(5):511–518
Tsukada S, Fujishiro H, Watanabe K, Nimura A, Mochizuki T, Mahakkanukrauh P, Yasuda K, Akita K (2014) Anatomic variations of the lateral intercondylar ridge: relationship to the anterior margin of the anterior cruciate ligament. Am J Sports Med 42(5):1110–1117. doi:10.1177/0363546514524527
Farrow LD, Chen MR, Cooperman DR, Victoroff BN, Goodfellow DB (2007) Morphology of the femoral intercondylar notch. J Bone Joint Surg Am 89(10):2150
van Eck CF, Lesniak BP, Schreiber VM, Fu FH (2010) Anatomic single- and double-bundle anterior cruciate ligament reconstruction flowchart. Arthroscopy 26(2):258–268. doi:10.1016/j.arthro.2009.07.027
Vaiyapuri S, Vaiyapuri R, Ashokan R, Ramasamy K, Nattamaisundar K, Jeyaraj A, Chandran V, Gajjeraman P, Baksh MF, Gibbins JM, Hutchinson EG (2013) Snakebite and its socio-economic impact on the rural population of Tamil Nadu, India. PLoS ONE 8(11), e80090. doi:10.1371/journal.pone.0080090
Kondo E, Merican AM, Yasuda K, Amis AA (2011) Biomechanical comparison of anatomic double-bundle, anatomic single-bundle, and nonanatomic single-bundle anterior cruciate ligament reconstructions. Am J Sports Med 39(2):279–288. doi:10.1177/0363546510392350
Suzuki T, Shino K, Nakagawa S, Nakata K, Iwahashi T, Kinugasa K, Otsubo H, Yamashita T (2011) Early integration of a bone plug in the femoral tunnel in rectangular tunnel ACL reconstruction with a bone-patellar tendon-bone graft: a prospective computed tomography analysis. Knee Surg Sports Traumatol Arthrosc 19:S29–S35. doi:10.1007/s00167-011-1481-5
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Japan
About this chapter
Cite this chapter
Mochizuki, T., Akita, K. (2016). Functional Anatomy of the ACL Fibers on the Femoral Attachment. In: Ochi, M., Shino, K., Yasuda, K., Kurosaka, M. (eds) ACL Injury and Its Treatment. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55858-3_1
Download citation
DOI: https://doi.org/10.1007/978-4-431-55858-3_1
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55856-9
Online ISBN: 978-4-431-55858-3
eBook Packages: MedicineMedicine (R0)