
Abstract
Pectus excavatum is the most frequent anterior thoracic wall congenital malformation. Autologous fat tissue transfer represents a filling material with ideal properties for soft tissue augmentation. Stromal Enriched Lipograft (SEL) technique which was firstly described by the author and his team, is based on autologous fat grafting enriched with adipose derived stem cells and produces superior results without the need for repeat treatment sessions, which are usually necessary with the non stem cell enriched autologous fat transplantation. A total of 13 female and 27 male patients were operated from over a 2 year period with this technique. The total amount of SEL transplanted to the chest area varied from 25 to 145 ml. There were no major complications reported. The use of SEL technique for the treatment of mild pectus excavatum achieves satisfactory results with high patient satisfaction rates in a single surgical procedure.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
Technical Highlights
The authors have introduced a new method for transplantation of Stromal Enriched Lipograft (SEL) in order to restore the visible and non-functionally disturbing deformation of mild funnel chests.
The main technical highlights of this procedure are:
-
(a)
In Stromal Enriched Lipograft (SEL), freshly isolated Stromal Vascular Fraction (SVF) is attached to the aspirated fat, with the fat tissue acting as a living bioscaffold before transplantation.
-
(b)
The donor site for fat harvesting can be chosen according to the preference of the surgeon and the patient.
-
(c)
An important consideration for harvesting and refinement in preparation for grafting is to respect and maintain the tissue architecture of living fat.
-
(d)
Fat is aspirated using the syringe method.
-
(e)
The 2/3 of the aspirated fat is used in order to isolate the SVF containing Adipose Derived Stem Cells (ADSCs).
-
(f)
The remaining 1/3 of the aspirated fat is used for the ADSCs to be attached.
-
(g)
The SEL is inserted into tunnels beginning at the deep layer and working up into the more superficial. Different trajectories are created. The SEL is injected as the cannula is withdrawn.
Preoperative Considerations
-
1.
Candidates are patients over 18 years old with mild pectus excavatum (Fig. 42.1). Preoperative symptoms such as dyspnoea on exertion, shortness of breath at rest, chest pain, and palpitations are indications for further exams and possibly more complex surgical repairs.
Fig. 42.1 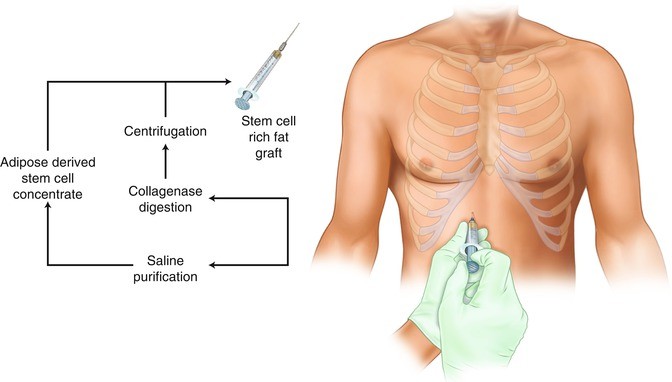
Overview of the process to obtain stem cell rich fat graft
-
2.
A full preoperative series of laboratory exams, CBC, coagulation tests, glucose, urea and creatinine tests are performed.
-
3.
Electrocardiograms are performed in order to diagnose or rule out cardiac pathologies.
-
4.
Chest X-Rays are performed in order to access the extent of the chest deformity.
-
5.
Lung function tests are performed in order to evaluate the pulmonary function.
-
6.
Chest perimeter plots to quantify the deformity at three different points: manubrium, sternum and xiphoid.
-
7.
Preoperative photographs of the deformity are taken.

Special Instruments
The following instruments and reagents are required for this surgical procedure:
-
1.
Celltibator (Medikan, Los Angeles, CA).
-
2.
Lipokit Centrifuge (Medikan, Los Angeles, CA)
-
3.
Collagenase (Sigma, St. Louis, MO)
-
4.
Syringe assisted liposuction tools (Tulip Medical, San Diego, CA)
Surgical Technique
The pectus excavatum area to be treated is marked with the patient standing up, sitting down and in supine position. The areas to be liposucked are also marked. Preoperative sedation in is administered at the surgical suite. Anesthesia consists of intravenous sedation and epidural anaesthesia. The patient is placed in supine position with the arms spread out.
After the injection of normal saline wetting solution containing 1 : 500,000 of adrenaline by a small bore cannula and waiting 15 min, a 10-cc syringe attached to a 2.5 mm blunt cannula is inserted through a small stab incision in the abdomen. Fat is aspirated by using the syringe method [12]. The 2/3 of the aspirated fat is used in order to isolate the SVF. Digestion is done with 0.075 % collagenase (Sigma, St. Louis, MO) in buffered saline and agitated for 30 min at 37 °C in Celltibator (Medikan, Los Angeles, CA). Separation of the SVF containing ADSCs is then done by using centrifugation at 1200 × g for 5 min [10, 13]. The Lipokit Centrifuge (Medikan, Los Angeles, CA), is used. The SVF is located in the pellet derived from the centrifuged fat at the bottom of the lipoaspirate.
The remaining 1/3 of the aspirated fat is treated in the following manner in which the syringe is held vertically with the open end down through which the fat and fluid are separated. Isotonic saline is added to the syringe, the fat and saline are separated and the exudate discarded. The procedure is repeated until the fat becomes yellow in colour, free of blood and other contaminants [2, 4, 5, 14]. In Stromal Enriched Lipograft (SEL), freshly isolated SVF is attached to the aspirated fat, with the fat tissue acting as a living bioscaffold before transplantation [11] (Fig. 42.4). This whole procedure is done manually inside the operating theatre by 2 experts in tissue engineering for which they require about 90 min.
A 10-cc syringe attached to a 2.5 mm blunt cannula filled with the prepared fat is used. The adipose tissue graft enriched with SVF is woven in to the targeted chest area, injecting only a tiny amount with each pass as in order to obtain the most reliable clinical outcome. Tissue planes are created by using specific cannulas in different trajectories, always from the deeper aspect to more superficial areas. The fat is injected as the cannula is withdrawn in order to avoid intravascular fat injection.
Procedure Overview (Figs. 42.1, 42.2, and 42.3)

After the injection of normal saline wetting solution containing 1:500,000 of adrenaline is administered by a small bore cannula and blunt cannula is inserted through a small stab incision in the abdomen. Fat is aspirated by using the syringe method

The adipose tissue graft enriched with SVF is woven in to the targeted chest area, injecting only a tiny amount with each pass
Postoperative Management
Intravenous antibiotics and analgesics are administered perioperatively and during the first 24 h. The patients are mobilized on the 1st day after surgery and discharged 24 h after the surgical procedure. At the time of discharge patients are advised to avoid lifting heavy objects and continue for 7 days antibiotics and analgesic treatment. The patients are followed-up at 1, 2, 6 and 12 months after the surgical procedure. Patients overall satisfaction with their appearance of the treated areas after undergoing SEL is rated on a scale of 1–5, whereas 1 is ‘poor’, 2 is ‘fair’, 3 is ‘good’, 4 is ‘very good’ and 5 is ‘excellent’. The patient satisfaction scale has been already used in published papers and has been peer reviewed [1, 7, 8]. Evaluation of patient satisfaction is done at least 24 months after the initial surgical procedure.
Results
A total of 13 female and 27 male patients were operated from January 2008 to January 2010. Age distribution of patients ranged from 19 to 52 years, with a mean of 22.3 years. The total amount of SEL transplanted to the chest area varied from 25 to 145 ml (mean, 62 ml). There were no intraoperative complications and no blood transfusions were required. There were no cases of liponecrosis and no liponecrotic lumps were palpated on postoperative evaluation. There were no cases of cellulitis of donor and grafted areas, no deep vein thrombosis and no pulmonary embolism. All the patients achieved satisfactory results undergoing just one session of SEL. At 24 months 70 % percent reported that their appearance after thoracic SEL contouring was ‘very good’ to ‘excellent’ (32 % ‘excellent’ and 38 % ‘very good’) and 23 % responded that their appearance was ‘good’. Only 7 % of patients thought their appearance was less than good, (6 % ‘fair’ and 1 % ‘poor’).
Autologous fat tissue transfer has recently become extremely popular in the field of plastic and reconstructive surgery. Stromal Enriched Lipograft technique which was firstly described by the author and his team is based on autologous fat grafting enriched with ADSCs and produces superior results without the need for repeat treatment sessions, which are usually necessary with the non-stem cell enriched autologous fat transplantation [13]. The presence of adipose-derived stem cells in adipose tissue transplantation may contribute to neoangiogenesis in the acute phase by acting as endothelial progenitor cells or angiogenic-factor-releasing cells [17]. The number of functional ADSCs is likely to be important for tissue repair and remodelling and ADSCs differentiate into vascular endothelial cells which contribute to neoangiogenesis in the acute phase of transplantation. ADSCs up regulate also their proneovascular activity in response to hypoxia, and may harbour the capacity to home to ischemic tissue and function cooperatively with existing vasculature to promote angiogenesis [3]. Successful SEL graft requires attention to patient preparation, meticulous planning, and optimizing the harvesting, storage, and transplantation of adipose tissue [16]. SEL graft is a living tissue that must be in close proximity to a nutritional and respiratory source to survive [15]. The SEL technique for mild pectus excavatum correction provides a safer alternative to allogenic implant use, resulting in the creation of a functional tissue which has a more natural look and carries fewer risks than currently available augmentation options. There were no major complications reported in this series of patients. In female patients, mild pectus excavatum can cause modified breast morphology, resulting in mammary asymmetry, which may be increased by placing mammary implants alone. Stromal Enriched lipograft is simultaneously applied for the correction of the pectus excavatum deformity. Fat transfer using the SEL technique for treatment of mild pectus excavatum achieves satisfactory aesthetic results with high patient satisfaction rates in just one surgical procedure.
Procedure Related Images (Figs. 42.4, 42.5, 42.6, 42.7, 42.8, 42.9, 42.10, 42.11, and 42.12)

(a, b) Preoperative views of a female patient with mild pectus excavatum

Lipoaspirated fat using the syringe method

Schematic representation of the stromal enriched lipograft technique

Stromal enriched lipograft in 1 ml syringes for injection

(a,b) Intraoperative photos of mild pectus excavatum in a female patient after breast augmentation has been performed. (c, d) Intraoperative photos of stromal enriched lipograft for the correction of the mild pectus excavatum

(a) Intraoperative photo of Stromal Enriched Lipograft to the breast. (b–d) Intraoperative photos of the corrected mild pectus excavatum in a female patient

(a, b) Preoperative photos of a female patient with mild pectus excavatum. (c, d) Postoperative photos of a female patient who underwent bilateral breast augmentation and Stromal Enriched Lipograft for the correction of mild pectus excavatum

(a, b) Preoperative photos of a male patient with mild pectus excavatum. (c, d) Postoperative photos of a male patient who underwent Stromal Enriched Lipograft for the correction of mild pectus excavatum

(a, b) Preoperative photos of a female patient with mild pectus excavatum. (c, d) Postoperative photos of a female patient who underwent bilateral breast augmentation and Stromal Enriched Lipograft for the correction of mild pectus excavatum
Patient 1
A 33 year old woman with mild pectus excavatum requested aesthetic correction, combined with breast augmentation (Fig. 42.10a, b). Initially bilateral breast augmentation by insertion of silicone implants was performed (Fig. 42.8a, b). SEL chest contouring was performed with insertion of 65 ml of fat (Fig. 42.8c, d). SEL breast contouring of 35 ml was also performed in order to complement the breast augmentation (Fig. 42.9a). The follow-up for the patient has been 32 months with no complications and an excellent aesthetic result (Fig. 42.10c, d).
Patient 2
A 29 year old male was referred to our clinic because he was highly concerned about the aesthetic appearance of his pectoral area (Fig. 42.11a, b). The patient expressed the desire to undergo the least invasive intervention that could produce an aesthetically acceptable result. It was decided to perform the SEL chest contouring. A total of 110 ml was injected and the follow-up for the patient has been 35 months with no complications and a very good aesthetic result (Fig. 42.11c, d).
Patient 3
A 33 year old woman with mild pectus excavatum requested aesthetic correction and simultaneous breast augmentation (Fig. 42.12a, b). Bilateral breast augmentation and SEL chest contouring was performed with insertion of 35 ml of fat. The follow-up for the patient has been 32 months with no complications and an excellent aesthetic result (Fig. 42.12c, d).
Suggested Reading
Citarella ER, Sterodimas A, Condé-Green A. Endoscopically assisted limited-incision rhytidectomy: a 10-year prospective study. Plast Reconstr Aesthet Surg. 2010;63(11):1842–8.
Haroldo Pereira L, Sterodimas A. Aesthetic restoration of axillary contour deformity after lymph node dissection. J Plast Reconstr Aesthet Surg. 2008;61(2):231–2.
Heneidi S, Simerman AA, Keller E, Singh P, Li X, Dumesic DA, Chazenbalk G. Awakened by cellular stress: isolation and characterization of a novel population of pluripotent stem cells derived from human adipose tissue. PLoS One. 2013;8(6):e64752.
Nicareta B, Pereira LH, Sterodimas A, Illouz YG. Autologous gluteal lipograft. Aesthetic Plast Surg. 2011;35(2):216–24.
Pereira LH, Nicaretta B, Sterodimas A. Correction of liposuction sequelae by autologous fat transplantation. Aesthetic Plast Surg. 2011;35(6):1000–8.
Pereira LH, Sterodimas A. Free fat transplantation for the aesthetic correction of mild pectus excavatum. Aesthetic Plast Surg. 2008;32(2):393–6.
Pereira LH, Sterodimas A. Composite body contouring. Aesthetic Plast Surg. 2009;33(4):616–24. Epub 2009 May 12.
Pereira LH, Sterodimas A. Transaxillary breast augmentation: a prospective comparison of subglandular, subfascial, and submuscular implant insertion. Aesthetic Plast Surg. 2009;33(5):752–9. Epub 2009 Jul 14.
Pereira LH, Sterodimas A. Fat transfer for mild pectus excavatum. In: Melvin.A. Shiffman editor. Autologous fat transfer: art, science, and practice. Berlin Heidenberg: Springer; 2009. p. 322–29.
Sterodimas A. Adipose stem cell engineering: clinical applications in plastic and reconstructive surgery. In: Illouz YG, Sterodimas A, editors. Adipose derived stem cells and regenerative medicine. Heidelberg: Springer; 2011. p. 165–80.
Sterodimas A. Stromal enriched lipograft for rhinoplasty refinement. Aesthet Surg J. 2013;33(4):612–4.
Sterodimas A, Boriani F, Magarakis E, Nicaretta B, Pereira LH, Illouz YG. Thirtyfour years of liposuction: past, present and future. Eur Rev Med Pharmacol Sci. 2012;16(3):393–406.
Sterodimas A, de Faria J, Nicaretta B, Boriani F. Autologous fat transplantation versus adipose-derived stem cell-enriched lipografts: a study. Aesthet Surg J. 2011;31(6):682–93.
Sterodimas A, Huanquipaco JC, de Souza FS, Bornia FA, Pitanguy I. Autologous fat transplantation for the treatment of Parry-Romberg syndrome. J Plast Reconstr Aesthet Surg. 2009;62(11):e424–6.
Sterodimas A, Illouz YG. Conclusions and future directions. In: Illouz YG, Sterodimas A, editors. Adipose derived stem cells and regenerative medicine. Heidelberg: Springer; 2011. p. 273–6.
Sterodimas A, Pereira LH. Liposuction of the abdomen and trunk. In: Rubin JP, Jewell ML, Richter D, Uebel CO, editors. Body contouring & liposuction. New York: W.B. Saunders Elsevier; 2012. p. 311–20.
Yuan Y, Gao J, Liu L, Lu F. Role of adipose-derived stem cells in enhancing angiogenesis early after aspirated fat transplantation: induction or differentiation? Cell Biol Int. 2013;37(6):547–50.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Sterodimas, A., Pereira, L.H. (2017). Free Fat Transplantation for the Aesthetic Correction of Mild Pectus Excavatum. In: Saxena, A. (eds) Chest Wall Deformities. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-53088-7_42
Download citation
DOI: https://doi.org/10.1007/978-3-662-53088-7_42
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-53086-3
Online ISBN: 978-3-662-53088-7
eBook Packages: MedicineMedicine (R0)