
Abstract
Background
Aesthetic surgery of the thoracoabdominal region is one of the most frequently performed surgical procedures in plastic surgery.The combination of circumferential liposuction, autologous fat grafting of the buttocks and/or lower limbs, and the modified transverse abdominoplasty as an adjuvant procedure all done in a single surgical procedure is not very common. The authors present a prospective study of the surgical technique of composite body contouring, emphasizing the low rate of complications and the high overall patient satisfaction.
Methods
A total of 64 consecutive female patients were operated on between January 2004 and January 2007. All the patients who were included in the study were candidates for a classical abdominoplasty. Posterior and lateral syringe-assisted liposuction combined with fat insertion into the buttocks and/or lower limbs was performed. Autologous fat grafting was done in the gluteal area for buttocks enhancement and in the lower limbs to correct contour deformities. Anterolateral liposuction with modified transverse abdominoplasty was done as an adjuvant procedure. Overall satisfaction with body appearance after composite body contouring was rated on a scale of 1–5.
Results
From 1,500 to 4,600 ml of fat was obtained with liposuction (mean = 2,478 ml). Forty-five patients had fat grafting only to the buttocks area. Six patients had fat insertion into the lower limbs and 13 had fat injection into the buttocks and lower limbs. The amount of fat transplanted to the buttocks varied from 165 to 625 ml (mean = 346 ml) and to the lower limbs it varied from 75 to 270 ml (mean = 195 ml). Three patients (5%) suffered from early complications, including infection (3%) and hematoma formation (2%). Nine patients (14%) had late complications, including hypertophic scars (7.5%), dog ears (4.5%), and localized fat excess (2%). Nine patients (14%) underwent revision surgery. Sixty-three percent reported that their appearance after composite body contouring was “very good” (42%) or “excellent” (21%) and 27% responded that their appearance was “good.” Only 10% thought their appearance was less than good, (7% “fair” and 3% “poor”).The average follow-up time has been 3.2 years (range = 2–5 years).
Conclusion
Composite body contouring combines circumferential liposuction, fat grafting of the buttocks and lower limbs, and modified transverse abdominoplasty to accomplish very good aesthetic results in a single surgical procedure with a low rate of complications and high patient satisfaction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Abdominoplasty is the most frequently performed excisional body-contouring procedure in aesthetic surgery [1]. During the past decade, many combinations of operative techniques for abdominoplasty have evolved to suit the individual requirements of the patient. Body-contouring techniques were developed over the past few decades, before liposuction came on the scene. Classic abdominoplasty has become more common. It appears to be technically easy but nevertheless it is a source of potentially serious complications that can clearly affect the aesthetic results and the satisfaction rate of the patients [2–4].
Abdominoplasty and liposuction traditionally have been separate procedures. The problems that generate complaints and dissatisfaction with classic abdominoplasty surgery are fullness of the flanks and epigastric areas, lack of a posterior lumbar curve, hanging skin over the incision line, and visible scars over the flanks and beyond underwear or swimsuit coverage. Suction-assisted lipectomy (SAL) in association with classic abdominoplasty has been regarded with trepidation, with ischemia of the apron flap, skin loss, and open wounds among the potential dire consequences, especially in obese patients [5–7].
Truncal liposuction with modified abdominoplasty techniques has been used to treat patients with abdominal deformities marked by lower abdominal skin excess, abdominal muscle laxity, and excess adipose tissue on the abdominal wall and in adjacent contours [8–10]. A modified abdominoplasty technique with limited undermining and preservation of the flap perforator vessels makes it possible to reduce the complication rate attributable to flap necrosis and seroma in abdominoplasty [11]. The technique allows aggressive thinning and “sculpting” of full-thickness abdominal subcutaneous tissue and achieves a natural abdominal contour. It minimizes the creation of “dead space,” which often leads to postoperative complications, and preserves sensory nerve and blood supply to the abdominal skin.
We performed a perspective study to evaluate the outcomes of a novel single-stage approach—composite body contouring—combining extensive liposuction, autologous fat transplantation, and modified transverse abdominoplasty as an adjuvant procedure.
Patients and Methods
A total of 64 consecutive female patients were operated on during 2004–2007. The age distribution of patients ranged from 30 to 67 years (mean = 48.3 years). All patients who were included in the study were candidates for a classical abdominoplasty. Overall satisfaction with body appearance after composite body contouring was rated on a scale of 1–5, where 1 is “poor,” 2 is “fair,” 3 is “good,” 4 is “very good,” and 5 is “excellent.” The evaluation was made at a minimal follow-up time of 6 months.
Surgical Technique
The steps of the surgical technique are as follows:
-
1.
The areas to be liposuctioned and fat grafted are marked while the patient is standing. The suprapubic incision mark and the infraumbilical flap mark are also made (Fig. 1).
Fig. 1 
a, b Marking of the patient in the standing position. c, d Marking of the suprapubic incision and of the infraumbilical flap
-
2.
Preoperative sedation in the surgical suite is administered. Anesthesia consists of an epidural block and intravenous sedation. The patient is placed in the prone position. Intermittent pneumatic compression is used in all our patients (Kendall Company, Boston, MA).
-
3.
After the injection of normal saline wetting solution, containing 1:500,000 of adrenaline, by a small bore cannula and waiting 15 min, a 60-cc syringe attached to a 4-mm blunt cannula is inserted through small incisions in the intergluteal fold as well as two incisions in the iliac crest and two more in the gluteal fold. Each incision is less than 1 cm long.
-
4.
Fat is aspirated using the syringe method. The donor sites include flank, thigh, and knee. Each individual area to be aspirated is treated separately.
-
5.
The aspirated fatty tissue is treated in the following manner. With the syringe held vertically with the open end down, the fat and fluid are separated. Isotonic saline is added to the syringe, the fat and saline are separated and the exudate discarded. The procedure is repeated until the fat becomes yellow in color and free of blood and other contaminants (Fig. 2) [12].
Fig. 2 
Fat preparation for autologous fat transplantation
-
6.
Upon completion of the liposuction procedure, access to the buttock region is gained through the incisions in the intergluteal fold.
-
7.
Initially, a deep plane to the gluteal muscles is created by the 4-mm cannula. Then other planes are created by the same cannula in different trajectories, always from the deeper aspect to the gluteal surface. The fat is inserted into these tunnels beginning at the deep layer and working up into the intermediate fat compartments. The fat is injected as the cannula is withdrawn. Care should be taken to avoid injecting more fat in the superficial fat compartment [13]. If necessary, separate incisions can be used to treat the whole gluteal region. The autologous fat transplantation is done by retrograde intramuscular and subcutaneous injection (Fig. 3).
Fig. 3 
a Intramuscular autologous fat transplantation to the gluteal area. b Subcutaneous fat grafting to the gluteal area
-
8.
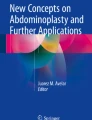
After placing the patient in the supine position, injection of normal saline wetting solution containing 1:500,000 of adrenaline by a small bore cannula is done in the whole abdomen. The 60-cc syringe attached to a 4-mm blunt cannula is inserted through a small incision in each of the groin areas and one incision in the umbilical crease. Fat is aspirated using the syringe method in the whole abdomen (Fig. 4). A diamond-shaped incision is made around the umbilicus. Incision of the premarked infraumbilical flap is done. The flap is undermined over the rectus and external oblique fascia in the infraumbilical area. Dissection above the umbilicus up to the xiphoid along the midline is done within a narrow tunnel less than 8 cm wide, just enough to plicate the recti muscles (Fig. 5).
Fig. 4 
Liposuction of the whole abdomen using the syringe method
Fig. 5 
a Incision of the premarked infraumbilical flap is done. b The flap is undermined over the rectus and external oblique fascia in the infraumbilical area. c Infraumbilical flap excision. d Dissection above the umbilicus up to xiphoid along the midline is done within a narrow tunnel less than 8 cm wide, just enough to plicate the recti muscles
-
9.
Diastasis repair and anterior sheath plication are performed, and the umbilicus is anchored to the fascia. Baroudi points between the undermined flap and the aponeurosis are used. Neo-omphaloplasty is done. The transverse suprapubic incision is closed in anatomical planes.
-
10.
No drains are used. Postoperative dressing is used in the area that was lipoaspirated, avoiding any pressure to the areas in which autologous fat transplantation was performed.
-
11.
The patient remains hospitalized for 24 h. Early mobilization, starting on the second postoperative day, is encouraged. Antibiotics, analgesics, and anti-inflammatory medications are prescribed for the following 7 postoperative days. Return to mild physical activities is allowed after the third postoperative week and lying down supine after 2 weeks. A nonzippered pullover female body vest (Yoga Ltda, Brazil) is placed on the second postoperative day and is kept on for 1 month.





Results
From 1,500 to 4,600 ml of fat was obtained with liposuction (mean = 2,478 ml). Forty-five patients had fat grafting to the buttocks area only. Six patients had fat insertion to the lower limbs and 13 had fat injection into the buttocks and lower limbs. The amount of clean adipose tissue transplanted to the buttocks ranged from 165 to 625 ml (mean = 346 ml) and to the lower limbs from 75 to 270 ml (mean = 195 ml). Three patients (5%) suffered from early complications, including infection (3%) and hematoma formation (2%). Nine patients (14%) had late complications, including hypertophic scars (7.5%), dog ears (4.5%), and localized fat excess (2%) (Fig. 6). Nine patients (14%) underwent revision surgery. Four patients requested further fat grafting of the gluteal area. Two received further fat grafting and two received gluteal silicone implants.

Schematic analysis of the type and percentage of complications
Sixty-three percent reported that their appearance after composite body contouring was “very good” (42%) to “excellent” (21%) and 27% responded that their appearance was “good.” Only 10% thought their appearance was less than good (7% “fair” and 3% “poor”) (Fig. 7). The average follow-up time was 3.2 years for all patients (range = 2–5 years).

Schematic presentation of the degree of satisfaction after the composite body contouring procedure
Patient 1
This 41-year-old woman presented for treatment of her abdominal flaccidity and local fat lipodystrophy and for buttock enhancement (Fig. 8a–c). Liposuction of the back, flanks, and abdomen as part of the composite body-contouring procedure was done and complemented by modified transverse abdominoplasty. Gluteal fat injection was performed. The following volumes were placed in one procedure: right gluteal area, 270 ml; left gluteal area, 260 ml; right subgluteal fold, 35 ml; and left subgluteal fold, 30 ml. Postoperative photos were taken 4 years after the procedure (Fig. 8d–f).

a–c Preoperative front, lateral, and posterior views of a 41-year-old woman. d–f Postoperative front, lateral, and posterior views 4 years after composite body contouring
Patient 2
This 49-year-old woman complained about her “floppy tummy,” generalized excess fat, and “loose buttocks” (Fig. 9a–c). Liposuction of the back, flanks, and abdomen was done along with a modified transverse abdominoplasty. Gluteal autologous fat transfer was performed. The following volumes were placed in one procedure: right gluteal area, 320 ml; left gluteal area, 340 ml; right subgluteal fold, 55 ml; and left subgluteal fold, 50 ml. Breast reduction was also performed. The patient is shown two years after the procedure (Fig. 9d–f).

a–c Preoperative front, lateral, and posterior views of a 49-year-old woman. d–f Postoperative front, lateral, and posterior views 2 years after composite body contouring
Patient 3
This 70-year-old woman complained about her abdominal flaccidity and generalized fat lipodystrophy and expressed the desire for buttock enhancement (Fig. 10a–c). Liposuction of the back, flanks, and abdomen as part of the composite body-contouring procedure was done and complemented by a modified transverse abdominoplasty. Autologous fat transplantation to the gluteal area was performed. The following volumes were placed in one procedure: right gluteal area, 330 ml; left gluteal area, 310 ml; right subgluteal fold, 55 ml; and left subgluteal fold, 60 ml. Breast reduction had been performed at a different time. Postoperative photos were taken 2 years after the procedure (Fig. 10d–f).

a–c Preoperative front, lateral, and posterior views of a 70-year-old woman. d–f Postoperative front, lateral, and posterior views 2 years after composite body contouring
Discussion
The shape, volume, and size of the body vary greatly. These variations can be observed in the same person during his/her life span. Ethnic background, sex, genetics, hormones, physical exercise, and diet are some of the factors that influence body contour [14]. The principle of composite body contouring offers a more ample selection to patients and addresses their requests. The procedure is based on liposuction and autologous fat transplantation. The modified transverse abdominoplasty is an adjunctive procedure that complements the contouring effects of the liposuction and the lipografting.
As in every surgical procedure, the success of liposuction and gluteal and lower-limb fat grafting is dependent on many factors: the techniques and instruments used to harvest the fat tissue, the fat processing, the volume of fat implanted, and the sites to be liposuctioned and implanted, the levels of placement, and even the individual patient. Because of these variables and perhaps because of other factors that are not yet understood, the results of liposuction and fat grafting via some techniques, in some patients, and in some areas can be unpredictable. Although there is no universal agreement on what constitutes an ideal methodology for liposuction and gluteal and lower-limb fat grafting, there are some proven points that should be taken into account. No statistical differences in adipocyte viability of abdominal fat, thigh fat, flank fat, or knee fat donor sites have been demonstrated [15]. The donor site can be chosen according to the preference of the surgeon and the patient. Recent reports have shown that mechanical centrifugation does not appear to enhance immediate fat tissue viability before implantation [16]. An important consideration for harvesting and refinement in preparation for grafting is to respect and maintain the tissue architecture of living fat. Any mechanical or chemical insult that damages the fragile tissue architecture of fat will result in eventual necrosis of the injected fat. Guerrerosantos has performed numerous successful autologous fat transfers, advocating injection into the muscle as well as deep into the fat [17]. The transplanted fat must have access to blood supply [18]. The creation of multiple tunnels ensures adequate blood supply of the grafted fat. Grafting of the superficial fat compartment must not exceed 20 ml per tunnel because of low vascularity and excessive compression of the area that can result in liponecrosis [19]. Intramuscular fat grafting should also be done in tunnels and retrograde injection should be performed to avoid intravascular fat injection. Pressure should not be applied in the grafted gluteal area [20]. Excess fat should not be injected at one spot. For predictable results, the surgeon should refine the fat into relatively pure living tissue using sterile conditions and avoiding external contact to prevent contamination. Transplantation of a high percentage of nonviable components such as blood and local factors reduces the potential for accurate volume estimation. The average tissue loss due to reabsorption after lipoinjection in the buttock varies between 24 and 36% [21]. Surgeons have come to realize that transplanted fat can create not only satisfying changes in contour but also long-lasting results [22].
Initial attempts at lipoabdominoplasty ranged on one extreme from timid addition of liposuction to some areas while avoiding “danger zones” to the other extreme of adding only lower abdominal dermolipectomy and minimal midline plication to extensive liposuction [5, 23]. It has been reported in the literature that full or modified abdominoplasty procedures, combined with extensive liposuction in all areas of the abdomen and hips, can be performed without local complications such as flap necrosis and seroma when progressive tension suturing is included [24, 25]. On the other hand, the reduced undermining in the upper quadrants has been proven to preserve the perforator arteries, minimize the creation of extra “dead space,” and preserve the sensory nerve and blood supply to the abdominal skin [9, 11]. In this series we have limited the undermining of the abdominal flap in the supraumbilical region just by performing extensive liposuction, limited central undermining, and plication of the rectus muscles. We realized that extensive liposuction achieves a satisfactory contour and mobilizes enough of the flap to allow the requisite skin excision and closure, without the need to perform wide undermining of the abdominal flap. The use of the Baroudi points plays an important role in the decrease of the dead space created after the abdominal undermining, making the use of drains unnecessary and contributing significantly in the prevention of seroma [26].
Liposuction of the flanks does not increase the complication rate of the lipoabdominoplasty procedures, and a tendency toward shorter scars in patients who underwent abdominoplasty combined with liposuction of the flanks has been observed [27]. With the combination of suction-assisted lipectomy, autologous fat transplantation, and modified abdominoplasty, the majority of patients treated will be highly satisfied with the results. This has been confirmed by the high satisfaction rate observed in this series of patients. The complication rate of this study is similar to that of other studies, although in our series the autologous fat transplantation was performed in all patients [6, 28].
With experience, the surgeon can predict the amount of volume needed to be grafted to produce the desired result. Although the aim of every surgeon is to produce the desired augmentation of the gluteal region and lower limb by autologous fat grafting in one stage, the patient should be advised that a secondary procedure may be needed to accomplish the desired result.
The composite body-contouring principle can also be used for secondary body-contouring cases where the combination of liposuction, autologous fat transplantation, and modified transverse abdominoplasty can correct iatrogenic deformities [29, 30].
With the overall acceptance of aesthetic surgery increasing, the number of patients undergoing body-contouring procedures increasing, and an aging population, it is likely that plastic surgeons will see more patients requesting composite body-contouring surgery in the future.
Conclusion
The combination of circumferential liposuction, autologous fat transplantation, and modified transverse abdominoplasty permits excellent body contouring in a single surgical procedure with minimal complications and a high satisfaction rate.
References
Cormenzana PS, Samprón NM, Escudero-Nafs FJ (2008) Secondary abdominoplasty. Aesthetic Plast Surg 32(3):503–508
Mayr M, Holm C, Höfter E, Becker A, Pfeiffer U, Mühlbauer W (2004) Effects of aesthetic abdominoplasty on abdominal wall perfusion: a quantitative evaluation. Plast Reconstr Surg 114(6):1586–1594
Momeni A, Heier M, Bannasch H, Stark GB (2008) Complications in abdominoplasty: a risk factor analysis. J Plast Reconstr Aesthet Surg [Epub ahead of the print]
Gliksman J, Himy S, Ringenbach P, Andreoletti JB (2006) [Abdominoplasty: towards a two procedure surgery? Retrospective study of postoperative complications about 100 cases]. Ann Chir Plast Esthet 51(2):151–156
Illouz YG (1992) A new safe and aesthetic approach to suction abdominoplasty. Aesthetic Plast Surg 16(3):237–245
Matarasso A, Swift RW, Rankin M (2006) Abdominoplasty and abdominal contour surgery: a national plastic surgery survey. Plast Reconstr Surg 117(6):1797–1808
Kolker AR (2008) Improving esthetics and safety in abdominoplasty with broad lateral subcostal perforator preservation and contouring with liposuction. Ann Plast Surg 60(5):491–497
Matarasso A (1991) Abdominoplasty: a system of classification and treatment for combined abdominoplasty and suction-assisted lipectomy. Aesthetic Plast Surg 15:111
Saldanha OR, De Souza Pinto EB, Mattos WN Jr, Pazetti CE, Lopes Bello EM, Rojas Y, dos Santos MR, de Carvalho AC, Filho OR (2003) Lipoabdominoplasty with selective and safe undermining. Aesthetic Plast Surg 27(4):322–327
Avelar JM (2006) Abdominoplasty combined with lipoplasty without panniculus undermining: abdominolipoplasty—a safe technique. Clin Plast Surg 33(1):79–90, vii
Graf R, de Araujo LR, Rippel R, Neto LG, Pace DT, Cruz GA (2006) Lipoabdominoplasty: liposuction with reduced undermining and traditional abdominal skin flap resection. Aesthetic Plast Surg 30(1):1–8
Pereira LH, Sterodimas A (2008) Free fat transplantation for the aesthetic correction of mild pectus excavatum. Aesthetic Plast Surg 32(2):393–396
Pereira LH, Sterodimas A (2008) Aesthetic restoration of axillary contour deformity after lymph node dissection. J Plast Reconstr Aesthet Surg 61(2):231–232
Baroudi R, Moraes M (1991) Philosophy, technical principles, selection, and indication in body contouring surgery. Aesthetic Plast Surg 15(1):1–18 (review)
Ullmann Y, Shoshani O, Fodor A, Ramon Y, Carmi N, Eldor L, Gilhar A (2005) Searching for the favorable donor site for fat injection: in vivo study using the nude mice model. Dermatol Surg 31(10):1304–1307
Rohrich RJ, Sorokin ES, Brown SA (2004) In search of improved fat transfer viability: a quantitative analysis of the role of centrifugation and harvest site. Plast Reconstr Surg 113(1):391–395 (discussion 396–397)
Guerrerosantos J (1996) Autologous fat grafting for body contouring. Clin Plast Surg 23(4):619–631
Lewis CM (1991) Transplantation of autologous fat. Plast Reconstr Surg 88(6):1110–1111
Pereira LH, Radwanski HN (1996) Fat grafting of the buttocks and lower limbs. Aesthetic Plast Surg 20(5):409–416
Lewis CM (1992) Correction of deep gluteal depression by autologous fat grafting. Aesthetic Plast Surg 16(3):247–250
Wolf GA, Gallego S, Patrón AS, Ramírez F, de Delgado JA, Echeverri A, García MM (2006) Magnetic resonance imaging assessment of gluteal fat grafts. Aesthetic Plast Surg 30(4):460–468
Coleman SR (1995) Long-term survival of fat transplants: controlled demonstrations. Aesthetic Plast Surg 19(5):421–425
Matarasso A (1995) Abdominolipoplasty: a system of classification and treatment for combined abdominoplasty and suction-assisted lipectomy. Plast Reconstr Surg 95:829–836
Pollock H, Pollock T (2000) Progressive tension sutures: a technique to reduce local complications in abdominoplasty. Plast Reconstr Surg 105(7):2583–2586 (discussion 2587–2588)
Khan UD (2008) Risk of seroma with simultaneous liposuction and abdominoplasty and the role of progressive tension sutures. Aesthetic Plast Surg 32(1):93–99 (discussion 100)
Baroudi R, Ferreira CA (1996) Contouring the hip and the abdomen. Clin Plast Surg 23(4):551–572 (discussion 572–573)
Rieger UM, Erba P, Wettstein R, Schumacher R, Schwenzer-Zimmerer K, Haug M, Pierer G, Kalbermatten DF (2008) Does abdominoplasty with liposuction of the love handles yield a shorter scar? An analysis with abdominal 3D laser scanning. Ann Plast Surg 61(4):359–363
Stewart KJ, Stewart DA, Coghlan B, Harrison DH, Jones BM, Waterhouse N (2006) Complications of 278 consecutive abdominoplasties. J Plast Reconstr Aesthet Surg 59(11):1152–1155
Pereira LH, Sterodimas A (2008) Correction for the iatrogenic form of banana fold and sensuous triangle deformity. Aesthetic Plast Surg 32(6):923–927
Pereira LH, Sterodimas A (2008) Treatment of iatrogenic abdominal contour irregularities. Aesthetic Plast Surg [Epub ahead of print]
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pereira, L.H., Sterodimas, A. Composite Body Contouring. Aesth Plast Surg 33, 616–624 (2009). https://doi.org/10.1007/s00266-009-9348-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-009-9348-6