
Abstract
Anxiety and fear are evolutionary beneficial emotions that help an organism to avoid danger and threat, but anxiety becomes pathological when it significantly impairs daily functioning. Anxiety disorders are among the most prevalent psychiatric disorders, and both etiology (fear learning) and involved neural circuitry are relatively well understood. In this chapter, we discuss the potential of functional MRI in understanding and detecting pathological anxiety, with a specific focus on the role of fear conditioning and extinction as a prevailing experimental and etiological model. We first address the neural (and psychophysiological) correlates of fear conditioning and extinction, which include the amygdala, hippocampus, dorsal anterior cingulate, and medial prefrontal cortex, among others. Then, we compare the sensitivity and specificity of this functional approach by discussing overlap and differences between anxiety disorders such as specific phobias, social anxiety disorder, and posttraumatic stress disorder. Furthermore, a brief overview of emerging evidence on panic disorder and obsessive-compulsive disorder is provided, although the latter is technically not an anxiety disorder according to the DSM-5. Finally, we discuss potential implications of functional MRI for anxiety disorders, including but not limited to presymptomatic detection, treatment selection, and tracking of progress.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction: Structural and Functional Imaging Tools of Anxiety Disorders
Anxiety disorders are the most prevalent group of psychiatric disorders with a 12-month prevalence of 14 %, affecting roughly 60 million people in the 27 countries of the European Union (Wittchen et al. 2011). Although the direct healthcare and indirect costs are lower in anxiety disorders compared to mood or psychotic disorders, the sheer amount of patients makes it one of the top five costliest brain disorders in Europe, surpassing an estimated 70 billion Euro a year (Gustavsson et al. 2011). Furthermore, prevalence estimates in the United States are comparable or even higher (Kessler et al. 2012).
In this chapter, we will address the role of neuroimaging markers in anxiety disorders, with a specific focus on posttraumatic stress disorder (PTSD), panic disorder, specific phobias, and social anxiety disorder. Moreover, we will briefly discuss obsessive-compulsive disorder (OCD). The development of neuroimaging methodology for anxiety disorders can be illustrated by the progress made in PTSD, a disorder that may develop after exposure to a potentially traumatic event and is characterized by intrusive memories, avoidance behavior, numbing, and hyperarousal. Before the widespread availability of functional magnetic resonance imaging (fMRI), studies addressed structural differences between PTSD patients and controls and observed volumetric differences in hippocampus (Bremner et al. 1995, 1997). When fMRI was technically suited to assess functional parameters of brain activity, the attention shifted from hippocampus to amygdala and the role of the prefrontal cortex. Research started to address the functioning of brain regions in PTSD by means of combining functional neuroimaging with symptom provocation tasks (e.g., with trauma scripts or stimuli), general affective tasks, and functional connectivity during the so-called resting state (Francati et al. 2007; Liberzon and Sripada 2008). These studies revealed intriguing altered functional patterns of activity and connectivity in the amygdala, the hippocampus, and the medial prefrontal cortex (mPFC) in PTSD (Francati et al. 2007; Liberzon and Sripada 2008; Vermetten and Lanius 2012). In more recent years, functional neuroimaging studies have increasingly focused on the underlying processes proposed to be involved in the etiology of PTSD, such as fear conditioning and extinction (Pitman et al. 2012). Importantly, these neuroimaging findings are starting to be integrated with data from genetics, endocrinology, and immunology to provide an integrative biological framework for PTSD in which prefrontal cortex dysregulation in conjunction with fear-conditioned amygdala response may eventually come to play a key role (Vermetten and Lanius 2012).
In this chapter, we would like to stress the utility of functional imaging tools for anxiety disorders, given that anatomical markers have revealed rather limited effects in most anxiety disorders (with the exception of OCD). For instance, one meta-analysis on volumetric differences in PTSD observed effect sizes d of 0.07–0.14 for the amygdala and 0.28–0.29 for the hippocampus (Karl et al. 2006). Some methodological issues deserve mentioning: the amount of positive reports on reduced hippocampus sizes in PTSD (about half of all published volumetric studies in the meta-analysis by Karl et al.) is rather high given the small effect and sample sizes (Ioannidis 2011), suggesting that there may be an analysis or reporting bias in the literature. Reduced hippocampus size may not be specific to PTSD since it is also observed in depression – yet, it is interesting that the volumetric differences are predominantly found in depressive patients with early childhood trauma (Vythilingam et al. 2002). Furthermore, the relevance of reduced hippocampus size may lie in altered hippocampal functioning, i.e., hippocampus size is, for instance, relevant for declarative memory performance (Starkman et al. 2003). Impaired functioning of the hippocampus may therefore be more closely related to anxiety symptoms and behavior. Although its use as a biomarker for PTSD or other anxiety disorders may be limited, reduced hippocampus sizes are of basic scientific interest considering whether they constitute a premorbid risk factor for PTSD or are a consequence of PTSD, or both – as indicated by longitudinal studies (Pitman et al. 2012). The more sensitive and specific endophenotype is, however, dysfunctional neural circuitry that is directly correlated to anxiety symptoms and behavior.
Functional imaging tools are as effective as the task that elicits (or modulates) brain activity to probe for abnormal functioning in specific circuitry. In other words, functional imaging tools depend on customized tasks to challenge the brain, as this may constitute a primary marker for whether brain functioning “breaks down” during stress. For task optimization, the related field of psychophysiology can be informative as many of the primary readouts are closely related to relevant neural circuitry (e.g., limbic and more downstream regions). A meta-analysis of psychophysiological effects in PTSD concluded that effect sizes of relevant physiological measures were larger for tasks involving trauma cues than for tasks involving trauma-unrelated stimuli, such as presentation of unexpected acoustic startle sounds, and that any task showed better effects than resting-state measurements (Pole 2007). For anxiety disorders, where a stimulus, context, event, or memory elicits specific fear (e.g., phobias, panic disorder, PTSD), symptom provocation by presentation of reminder cues will likely probe the neural fear circuitry to a much larger extent (and with more experimental control) than resting-state tasks. A promising alternative is to directly examine the underlying process that has been proposed to be responsible for pathological anxiety: fear conditioning and extinction (see Lissek et al. 2005).
2 Experimental Tasks for Fear-Related Anxiety Disorders: Fear Conditioning and Extinction
As mentioned above, one major advantage of functional imaging tasks for anxiety disorders is that much can be learned from 80 years of experience in experimental psychology. Utilizing skin conductance response (SCR) or eyeblink startle electromyography (EMG) as physiological readouts, psychophysiological studies have provided a wealth of data on relevant functional tasks and dependent variables in anxiety disorders (Lissek et al. 2005). Although functional imaging can be viewed as adding a new dependent variable to the existing functional task and psychophysiological readouts, functional imaging research is only rarely tapping into this existing body of knowledge. In our opinion, functional imaging studies should be firmly rooted in experimental psycho(physio)logy, so that the neural correlates can be adequately labeled and interpreted.
Fear conditioning is a robust experimental task that has been studied over eighty years in human subjects, ever since pioneering studies observed that pairing an electric shock (unconditioned stimulus, US) with a light caused an SCR at subsequent light presentation (Steckle 1933; Switzer 1934; Rodnick 1937), which therefore became a conditioned stimulus (CS+) and the onset SCR an anticipatory, conditioned response (see Fig. 15.1, upper panel). This provided a well controllable translational model of classical conditioning, first reported in dogs by Pavlov (Pavlov 1927), and a template for further variations. The introduction of a safety stimulus (CS−) into the task allowed examination of the differential conditioned response, to control for individual variability in SCR intensity and frequency. After initial fear conditioning, the mere exposure of CS+ no longer followed by shocks constituted fear extinction, which as a laboratory model shares overlap with exposure-based therapy (Rauch et al. 2006). Variations in CS+ shapes provided a means to probe for fear generalization, which is a relevant process for several anxiety disorders (e.g., generalization of trauma- or panic-attack reminders is typically reported in PTSD and panic disorder, whereas a specific phobia may be characterized by a non-generalized fear to a specific object or context, Lissek 2012).

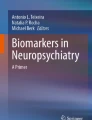
Upper panel: example of an early human fear-conditioning task describing anticipatory skin conductance responses (SCR) to a conditioned stimulus (CS+), in the figure at locations A and B (From Rodnick (1937)). Lower panels: activity correlated with a parametric modulation of the amplitude of anticipatory SCR to CS+ during the course of fear conditioning (decreasing slope), showing clusters of activity in the bilateral amygdala and thalamus (N = 34, pFDR < 0.025) (Reproduced by kind permission of Elsevier from Spoormaker et al. (2011))
Using fMRI, limbic and paralimbic regions such as the amygdala, hippocampus, dorsal anterior cingulate cortex (dACC), and ventromedial prefrontal cortex (vmPFC), as well as the insula and thalamus, have been repeatedly demonstrated to subserve fear conditioning and extinction in healthy individuals (for a systematic review, see Sehlmeyer et al. 2009). Already early fMRI studies on human fear conditioning revealed activity in the dACC and bilateral insula associated with CS+ (Büchel et al. 1998; LaBar et al. 1998), whereas the first human fMRI fear extinction study showed an increase in activity in the vmPFC during fear extinction (Phelps et al. 2004). In analyses addressing integration of SCR and fMRI data, the onset SCR to CS+ as described above appears specifically correlated to amygdala and thalamus activity to CS+ during fear conditioning (e.g., Spoormaker et al. 2011), see Fig. 15.1, lower panels. A quickly growing body of research has started to address the overlap in neurocognitive mechanisms underlying fear conditioning and extinction in preclinical and clinical studies, leading authoritative reviews to conclude that this is a successful model for translating data from animal models to human subjects and psychiatric patients (Milad and Quirk 2012; Pitman et al. 2012).
2.1 Functional Imaging of Fear Conditioning and Extinction: Relevance for PTSD
Fear conditioning and extinction has been increasingly recognized as a promising human and animal model for studying the neural circuitry involved in anxiety disorders, most notably PTSD (Rauch et al. 2006; Pape and Pare 2010). Besides forming the core of theoretical models on the etiology of normal and pathological anxiety (Lissek et al. 2005), multiple independent research groups have now provided the critical evidence for impaired extinction in PTSD and other anxiety disorders (Lissek et al. 2005; Blechert et al. 2007; Wessa and Flor 2007; Milad et al. 2009).
Crucially, the amygdala and dACC show abnormal fMRI activity in PTSD patients during extinction and at recall of extinction (Milad et al. 2009), whereas hypoactivity was observed in both the vmPFC and hippocampus. This pattern of activation and deactivation has also been reported by a recent meta-analysis of 26 functional neuroimaging studies of PTSD employing various tasks (from symptom provocation to fear extinction) that found that the dACC and amygdala were the most strongly activated regions in PTSD, whereas the vmPFC and the inferior frontal gyri were the most strongly deactivated regions in PTSD (Hayes et al. 2012). Moreover, a decrease in vmPFC activity was associated with increased amygdala activity (Hayes et al. 2012), in line with the inhibitory connections from the vmPFC to amygdala (LeDoux 2000). Neurocircuitry models of PTSD postulate that this failure of the vmPFC and hippocampus to downregulate a hyperactive amygdala is the core feature characterizing PTSD, which is postulated to be responsible for increased fear responses, impaired fear extinction learning and retrieval, and impairments in general emotion regulation and attentional biases towards threat (Rauch et al. 2006). In a recent comprehensive review on biological studies of PTSD (Pitman et al. 2012), a main conclusion was that the amygdala was hyperactive in PTSD in response to trauma-related stimuli as well as generic threat stimuli, and during fear conditioning, compared to control subjects. Here it is important to note, however, that amygdala deactivation has been observed in PTSD as well (Etkin and Wager 2007). Such amygdala deactivation has been proposed to be characteristic of dissociative subtype of PTSD, with limbic overmodulation rather than undermodulation as a core feature (Lanius et al. 2010a), which results in increased frontal cortical activity and decreased amygdala activity to traumatic script challenge. Patients responding with this pattern are typically characterized by early trauma histories (Lanius et al. 2010b). This would be an interesting area for further research on the use of neuroimaging tools in PTSD patient stratification.
The dACC showed increased activity during fear conditioning and recall of extinction in PTSD compared to trauma-exposed healthy controls; the vmPFC, in contrast, was concluded to have decreased activity during both trauma-related and trauma-unrelated affective stimuli. Hippocampus involvement may be task dependent and is likely related to “deficits in recognizing safe contexts” (Pitman et al. 2012). Context dependencies of CS+ (e.g., fear conditioning in context A and fear extinction in context B, manipulated by presenting different background colors during both phases) involve the hippocampus (Milad et al. 2007) and are impaired in PTSD patients compared to trauma-exposed controls (Milad et al. 2009). The hippocampus is involved at a more basic level in pattern completion or separation to CS+, which would activate the vmPFC in turn (Lissek 2012). The emotional circuitry sensitive to PTSD extends to other regions involved in affective processing, such as the insula, but this has also been observed in other anxiety disorders and may not be specific to PTSD (Etkin and Wager 2007).
2.2 Comparison of PTSD with Other Anxiety Disorders
Which brain activity is specific to PTSD? This question was addressed by Etkin and Wager (2007) in a meta-analysis of imaging studies that compares PTSD with specific phobias, social anxiety disorder, and fear conditioning in healthy subjects. Most functional imaging (positron emission tomography, PET; and functional magnetic resonance imaging, fMRI) studies included in the meta-analysis used symptom provocation: i.e., 10 out of 15 imaging studies on PTSD used visual- or script-based trauma cues, five out of eight imaging studies on social phobia used negative facial expressions (the other addressing public speaking and speech anticipation), and six out of seven imaging studies on specific phobias used images, words, or videos of the phobic object/animal/situation.
Results revealed that all disorders (patients > control subjects) showed hyperactivity in the amygdala and insula and that this pattern of activity was analogous to fear conditioning in healthy subjects. This suggests overlapping fear circuitry involved in both symptom provocation in patients and fear conditioning in controls, relevant across disorders. However, only PTSD further showed hypoactivity in the ventro- and dorsomedial prefrontal cortex (dmPFC), anterior hippocampus, and parahippocampal gyrus, among others, that was specific to this disorder. According to the meta-analysis, results of social and specific phobias were strongly overlapping, whereas the pattern of activation and deactivation in PTSD showed more deviation and complexity. In PTSD, hypoactivity in medial prefrontal regions tended to co-occur, whereas a pattern of hypoactivity in the medial prefrontal and hyperactivity in the amygdala was also observed in this meta-analysis. Interestingly, hyperactivity in the amygdala tended to occur more frequently in phobias than in PTSD (Etkin and Wager 2007), with potential relevance for PTSD subtype stratification (Lanius et al. 2010a, b) as mentioned above.
Due to this specificity, hypoactivity in medial prefrontal and hippocampal areas in PTSD may be of special interest. A logical prediction is that hypoactivity in these regions is correlated with extinction and/or generalization impairments. Future research has yet to address this question; however, studies have already shown that mPFC activity correlates with subjectively reported PTSD symptom severity (Shin et al. 2005). Intriguingly and consistent with this, symptom severity improvements after cognitive-behavioral therapy for PTSD have been found to be related to an increase in mPFC and a decrease in amygdala activity (Felmingham et al. 2007). Although the hypoactivity of the vmPFC and hyperactivity of the amygdala in PTSD are unequivocal, there is some lack of clarity regarding whether or not the dmPFC (dACC) is hyper- or hypoactivated in PTSD: Etkin and Wager (2007) found clear hypoactivity in PTSD, while other studies have shown hyperactivity of the dACC during fear conditioning in PTSD (Milad et al. 2009) and positive correlations between dACC and amygdala activity (Pitman et al. 2012). It is possible though that hyperactivity is confined to the more posterior dACC (middle cingulate cortex) that extends into the supplementary motor area, which has been found to consistently activate during fear conditioning (Sehlmeyer et al. 2009). More rostral portions of the dACC and ACC extending into the ventral parts may then be more hypoactivated in PTSD and involved in extinction learning and recall (Phelps et al. 2004; Etkin and Wager 2007; Milad et al. 2009). For a brief summary, see Fig. 15.2.

Functional interactions among fear circuitry regions. A recent review on the biology of PTSD described the relevance of dACC excitatory connections to the basolateral amygdala (BLA), vmPFC inhibitory connections to the central nucleus of the amygdala (CEA) through intercalated cells (ITC), and a high vmPFC/dACC activity ratio for successful fear memory encoding and retrieval (left). As compared to stronger inhibitory influence of the vmPFC and lower excitatory input of the dACC over the amygdala under healthy conditions (middle), excess dACC activity during fear conditioning and extinction results in hyperactivity in the amygdala and reduced vmPFC activity (right), which further implies a failure to downregulate the amygdala, causing functional impairments in extinction memory encoding and/or retrieval (Reproduced by kind permission of Macmillan Publishers from Pitman et al. (2012))
2.3 Fear Conditioning: Functional and Imaging Limitations
Although fear conditioning and extinction constitutes one of the most robust paradigms in experimental psychophysiology, allowing disturbing symptom provocation tasks to be replaced by less stressful and better controlled experimental stimuli, the task has too received critique for exclusively focusing on physiological (and subjective) components of emotion while not addressing the behavioral component of (pathological) anxiety, i.e., avoidance and safety behavior (Beckers et al. 2013). New tasks combining fear conditioning with exploration and avoidance behavior in virtual reality environments are a promising start into this understudied dimension (Grillon et al. 2006). Moreover, PTSD is primarily characterized by distressing intrusive memories in the form of flashbacks and nightmares, and electrical shocks as US do not tap into (dys)function of such memory aspects. Tasks exploiting conditioning with highly intrusive movie scenes as US (Wegerer et al. 2013) may provide a promising and clinically useful extension of the typical fear-conditioning task. Furthermore, stimuli in fear-conditioning tasks are typically visual or auditory; more research attention could be devoted to alternative stimuli given the promise of olfactory trauma reminders in neuroimaging studies of PTSD (Vermetten et al. 2007).
It is possibly one of the great paradoxes in functional MR imaging of anxiety disorders that the brain regions that are most relevant, such as the amygdala, vmPFC, subgenual ACC, and orbitofrontal cortex, are among the regions that are most strongly affected by magnetic susceptibility-induced artifacts and consequently signal loss (Schwarzbauer et al. 2010). Such artifacts are caused by inhomogeneities of the magnetic field and arise especially at and in proximity of brain/air borders, due to the anatomy itself. fMRI is especially sensitive to local variations of field homogeneity, as the primary source of the image contrast is its sensitivity to small changes in the magnetic properties of hemoglobin, depending on the blood oxygenation (leading to the so-called blood oxygen level dependent – BOLD – effect, which is reflected by changes of the T2* relaxation rates of neighboring nuclear spins). As a result, fMRI image acquisition optimization is desirable to recover signal from these essential regions.
2.4 Panic Disorder
Panic disorder is arguably an anxiety disorder most closely related to the specific phobias and PTSD since in panic disorder, patients have learned to fear upcoming panic attacks (US) often triggered by interoceptive stimuli (CS+) thought to prequel a following attack. Agoraphobia, a fear of open or public spaces, is a frequent comorbid disorder in panic disorder. Psychophysiological research has shown impairments in extinction learning (Michael et al. 2007) and overgeneralization in panic disorder patients to various deviating versions of CS+ (Lissek et al. 2010). No imaging data have yet been published on these tasks; however, clear predictions of neural correlates of overgeneralization would point to the hippocampus given its role in pattern completion versus separation and the mPFC in relation to impaired extinction learning (Lissek 2012). Interestingly, an initial study showed increased midbrain activity in panic patients during fear conditioning (Lueken et al. 2013), which was paralleled by impaired differential learning in panic disorder patients (manifest in subjective ratings); however, no psychophysiological measures were recorded. Another fear conditioning study without psychophysiological measures also observed increased midbrain activity in panic disorder patients in response to safety cues, coactivating with clusters of activity in the ventral striatum, the anterior medial temporal lobe, and the subgenual ACC (Tuescher et al. 2011).
In general, it is of note that panic disorder has been studied to a lesser degree than PTSD, and the imaging studies that have been conducted to date, employing general affective tasks (e.g., emotional stroop, facial recognition, negative pictures), have shown mixed results (see Dresler et al. 2013, for a review). fMRI studies of affective tasks (N = 9) were inconclusive, but abnormal activity in the ACC (either increased or decreased) occurred across tasks (Dresler et al. 2013). Hyperactivity of the amygdala has not been consistently found during these tasks; however, a few case studies of spontaneous panic attacks during functional imaging sessions reported increased amygdala and insula activity (Dresler et al. 2013). Another review has implicated the amygdala, insula, mPFC and hippocampus in panic disorder (de Carvalho et al. 2010); yet as no meta-analyses have yet been conducted, a formal statistical evaluation of such potentially relevant effects is precluded.
For panic disorder, promising alternative models have been tested that may eventually be combined with fear conditioning to achieve a comprehensive view on this disorder. Hyper- and hypocapnia (elevated and reduced CO2 levels in the blood) have been experimentally induced in panic disorder (Martinez et al. 1998). This resulted in differences in heart rate and blood pressure between panic disorder patients and controls (Martinez et al. 1998), the correlates of which in fMRI need to be more closely examined. Pharmacological models of panic attacks have also been reported, such as with panicogenic neuropeptide cholecystokinin tetrapeptide (CCK-4), showing increased amygdala activation compared to placebo after CCK-4 administration in healthy subjects, as well as in the vmPFC, lateral prefrontal regions, brainstem, and cerebellum, among others (Eser et al. 2009). The reported anticipatory anxiety associated with the dACC in this study is also worth mentioning. CCK-4 led to an increase in subjective panic symptoms and heart rate, which may interfere with the experimental readout in fMRI studies – also here closer examination of potential interference of autonomic responses to panicogenic stimuli with the BOLD signal appears of interest, although the specific, localized increase in limbic and paralimbic areas after CKK-4 seems to go beyond potential unspecific baseline differences.
One methodological issue that is relevant for panic disorder but also for other anxiety disorders is that anxiety typically correlates with respiratory alterations that may produce significant changes in cerebral blood flow independent of task-related neural activation (Giardino et al. 2007). Measuring arterial carbon dioxide tension (or at the very least, breathing patterns) may be a useful way to control for variance in fMRI data of nonneuronal origin.
2.5 Specific Phobias, Social Anxiety Disorder, and Generalized Anxiety Disorder
A recent meta-analysis on specific phobias has confirmed the initial conclusions by Etkin and Wager (2007) and reported that phobic stimuli were associated with increased activity in the amygdala, insula, and pallidum and that these regions and the cerebellum and thalamus were also more activated in phobic patients relative to healthy controls in response to phobic stimuli (Ipser et al. 2013). Differences between patients and controls in the ACC were related to general affective processing. Noteworthy is that this meta-analysis also observed reduced activity in the dACC, thalamus, insula, and more lateral prefrontal regions after cognitive-behavioral treatment (N = 3) (Ipser et al. 2013). The same group performed a meta-analysis on social anxiety disorder as a distinct and epidemiologically relevant anxiety disorder, which also revealed increased activity in the amygdala, pallidum, and ACC in response to social stimuli (e.g., faces, linguistic stimuli), as well as in the hippocampal complex (perirhinal cortex). These conclusions are still tentative as the amount of included fMRI studies was rather small (N = 7); however, the reported regions fit well with the regions activated in fear-conditioning tasks (Sehlmeyer et al. 2009), and the absence of hypoactivity in the mPFC could have functional relevance for the specificity of the phobic fear (Lissek 2012) versus the overgeneralization in, for instance, PTSD.
Generalized anxiety disorder, an anxiety disorder characterized by excessive and diffuse anxiety and worrying rather than specific fear, has shown less consistent neural correlates than the fear-related anxiety disorders. An increased amygdala response to all – aversive and neutral – stimuli has been observed in generalized anxiety disorder (Nitschke et al. 2009), although another study reported decreased amygdala activity in response to fearful faces in patients compared to healthy volunteers (Blair et al. 2008), and further studies did not observe any group differences between patients and controls during affective stimulus processing (Whalen et al. 2008; Etkin et al. 2010). It may be that diffuse anxiety may be associated with different neural correlates than amygdala-mediated fear and a role for the involvement of the bed nucleus of the stria terminalis has been proposed (Davis 1998) and observed in generalized anxiety disorder patients in response to uncertainty (Yassa et al. 2012). Moreover, a few studies point to abnormal patterns of (de)activation in the dorsomedial and dorsolateral prefrontal cortices associated with emotional (dys)regulation (Blair et al. 2012; Ball et al. 2012), which differed from healthy controls but not from patients with generalized social phobia (Blair et al. 2012). Further research is necessary to replicate these promising observations.
3 Obsessive-Compulsive Disorder
The situation is different in obsessive-compulsive disorder (OCD), which has received much attention in neuroimaging and is rather discrepant from the other anxiety disorders, both in symptomatology and imaging findings. OCD is characterized by obsessive thoughts and images, with which persons cope by means of ritualistic and stereotyped overt or covert behavior. The disorder has been removed from the section of anxiety disorders in the fifth version of the diagnostic and statistical manual of mental disorders (DSM-5) and now has a separate chapter: Obsessive-Compulsive and Related Disorders. This also makes sense from an imaging perspective: instead of dysfunctional neural circuitry primarily in limbic and medial prefrontal areas, both anatomical (Radua and Mataix-Cols 2009; Peng et al. 2012) and functional (Menzies et al. 2008; Rotge et al. 2008) meta-analyses have implicated the striatum and particularly cortico-striato-thalamic loops in OCD, with additional differential activity in the orbito- and prefrontal cortices (Menzies et al. 2008; Rotge et al. 2008). Changes in striatal volumes have not always been found (Rotge et al. 2009), although heterogeneity in the meta-analyses may be due to methodological differences (Ferreira and Busatto 2010).
The meta-analysis by Menzies et al. (2008) on a variety of functional tasks in OCD revealed increased activity in the orbitofrontal cortex and caudate nucleus and medial and lateral prefrontal cortex. Lateral orbitofrontal and medial prefrontal cortex abnormalities were proposed to be related to the intrusive obsessions, whereas striatal abnormalities have been proposed to be related to the stereotyped behavior. A recent meta-analysis on brain structure abnormalities has pointed out that the dmPFC and vmPFC/orbitofrontal cortex have reduced volumes in OCD, whereas the caudate nucleus shows increased volumes (Peng et al. 2012); see Fig. 15.3.

Gray matter differences between patients with obsessive-compulsive disorder and healthy controls, with decreased gray matter volumes in patients depicted in blue (a) and increased volumes in red (b) (Reproduced by kind permission from Elsevier from Peng et al. (2012))
4 Outlook: Imaging Markers for Prediction of Treatment Outcome and Tracking of Treatment Success
A promising application for functional imaging may be to stratify patients and track treatment progress in an objective manner. Exposure-based cognitive-behavioral therapy is one of the most successful treatments for anxiety disorders and shows effects in a majority of patients. However, a minority does not respond to this therapeutic approach and would possibly benefit more from pharmacological treatment. Imaging tasks related to fear conditioning and extinction could help to predict who might benefit from exposure- (and self-regulation) based therapies and who may better start with pharmacological or combined treatment. Research into this field has started to develop, with a recent fMRI study of 39 social anxiety disorder patients as a timely example: this study observed that activity in the occipitotemporal cortex before treatment was positively correlated to cognitive-behavioral treatment outcome 12 weeks later (Doehrmann et al. 2013). Other studies with a similar setup focused on treatment response in generalized anxiety disorder and noted that dACC activity predicted response to the serotonin-norepinephrine reuptake inhibitor (SNRI) venlafaxine (Whalen et al. 2008; Nitschke et al. 2009). Intriguingly, an early study reported that long-term treatment with the selective serotonin reuptake inhibitor (SSRI) paroxetine resulted in an increase in hippocampal volumes – and verbal declarative memory performance – in PTSD patients (Vermetten et al. 2003).
Moreover, a study in PTSD patients found amygdala and vmPFC activity to be predictive of treatment response to cognitive-behavioral therapy (Bryant et al. 2008). This relates to the previously described finding that symptom severity improvements after cognitive-behavioral therapy for PTSD were related to an increase in the mPFC and a decrease in amygdala activity (Felmingham et al. 2007). Analogous findings were observed in a meta-analysis on specific phobia, with reduced activity in the dACC, thalamus, insula, and more lateral prefrontal regions after cognitive-behavioral treatment (Ipser et al. 2013). However, findings of this meta-analysis are tentative due to small group sizes, typical noninclusion of patient control groups, not reporting the group × time interactions, or employing no or inadequate multiple test corrections in the included studies.
5 Conclusion
Functional neuroimaging has proved to be a relevant tool for anxiety disorders, including PTSD, specific phobias, social anxiety disorder, and panic disorder. Fear conditioning and extinction tasks have become the dominant paradigm for the etiology (and treatment) of these anxiety disorders and have been successfully combined with functional neuroimaging tools, extending decades of psychophysiological research. Most neuroimaging attention to date has been devoted to PTSD, where hypoactivity in the vmPFC, dmPFC, and hippocampal complex may be a specific feature compared to phobias. In contrast, hyperactivity in amygdala seems to be a general feature shared by most anxiety disorders. Particularly for specific phobias, generalized anxiety disorder, and panic disorder, more replications are required. In contrast, the literature on OCD is more mature and converges towards both functional and structural abnormalities in cortico-striato-thalamic circuitry including the orbitofrontal cortex, albeit with considerable heterogeneity. Methodological challenges lie in the optimization of fMRI acquisition protocols for limbic and medial prefrontal circuitry, the control for respiration-induced vascular changes, and the expansion of fear-conditioning tasks with intrusion-relevant unconditioned stimuli and measurable avoidance behavior. Potential applications seem promising for treatment outcome prediction and patient stratification.
Abbreviations
- BOLD:
-
Blood oxygen level dependent
- CCK-4:
-
Cholecystokinin tetrapeptide
- CS−:
-
Safety stimulus
- CS+:
-
Conditioned stimulus
- dACC:
-
Dorsal anterior cingulate cortex
- dmPFC:
-
Dorsomedial prefrontal cortex
- EMG:
-
Electromyography
- ITC:
-
Intercalated cells
- OCD:
-
Obsessive-compulsive disorder
- vmPFC:
-
Ventromedial prefrontal cortex
- PTSD:
-
Posttraumatic stress disorder
- SCR:
-
Skin conductance response
- SNRI:
-
Serotonin-norepinephrine reuptake inhibitor
References
Ball TM, Ramsawh HJ, Campbell-Sills L, Paulus MP, Stein MB (2012) Prefrontal dysfunction during emotion regulation in generalized anxiety and panic disorders. Psychol Med 31:1–12
Beckers T, Krypotos AM, Boddez Y, Effting M, Kindt M (2013) What’s wrong with fear conditioning? Biol Psychol 92:90–96
Blair K, Shaywitz J, Smith BW, Rhodes R, Geraci M, Jones M, McCaffrey D, Vythilingam M, Finger E, Mondillo K, Jacobs M, Charney DS, Blair RJ, Drevets WC, Pine DS (2008) Response to emotional expressions in generalized social phobia and generalized anxiety disorder: evidence for separate disorders. Am J Psychiatry 165:1193–1202
Blair KS, Geraci M, Smith BW, Hollon N, DeVido J, Otero M, Blair JR, Pine DS (2012) Reduced dorsal anterior cingulate cortical activity during emotional regulation and top-down attentional control in generalized social phobia, generalized anxiety disorder, and comorbid generalized social phobia/generalized anxiety disorder. Biol Psychiatry 72:476–482
Blechert J, Michael T, Vriends N, Margraf J, Wilhelm FH (2007) Fear conditioning in posttraumatic stress disorder: evidence for delayed extinction of autonomic, experiential, and behavioural responses. Behav Res Ther 45(9):2019–2033
Bremner JD, Randall P, Scott TM, Bronen RA, Seibyl JP, Southwick SM, Delaney RC, McCarthy G, Charney DS, Innis RB (1995) MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 152:973–981
Bremner JD, Randall P, Vermetten E, Staib L, Bronen RA, Mazure C, Capelli S, McCarthy G, Innis RB, Charney DS (1997) Magnetic resonance imaging-based measurement of hippocampal volume in posttraumatic stress disorder related to childhood physical and sexual abuse–a preliminary report. Biol Psychiatry 41:23–32
Bryant RA, Felmingham K, Kemp A, Das P, Hughes G, Peduto A, Williams L (2008) Amygdala and ventral anterior cingulate activation predicts treatment response to cognitive behaviour therapy for post-traumatic stress disorder. Psychol Med 38:555–561
Büchel C, Morris J, Dolan RJ, Friston KJ (1998) Brain systems mediating aversive conditioning: an event-related fMRI study. Neuron 20:947–957
Davis M (1998) Are different parts of the extended amygdala involved in fear versus anxiety? Biol Psychiatry 44:1239–1247
de Carvalho MR, Dias GP, Cosci F, de-Melo-Neto VL, Bevilaqua MC, Gardino PF, Nardi AE (2010) Current findings of fMRI in panic disorder: contributions for the fear neurocircuitry and CBT effects. Expert Rev Neurother 10:291–303
Doehrmann O, Ghosh SS, Polli FE, Reynolds GO, Horn F, Keshavan A, Triantafyllou C, Saygin ZM, Whitfield-Gabrieli S, Hofmann SG, Pollack M, Gabrieli JD (2013) Predicting treatment response in social anxiety disorder from functional magnetic resonance imaging. JAMA Psychiatry 70:87–97
Dresler T, Guhn A, Tupak SV, Ehlis AC, Herrmann MJ, Fallgatter AJ, Deckert J, Domschke K (2013) Revise the revised? New dimensions of the neuroanatomical hypothesis of panic disorder. J Neural Transm 120:3–29
Eser D, Leicht G, Lutz J, Wenninger S, Kirsch V, Schüle C, Karch S, Baghai T, Pogarell O, Born C, Rupprecht R, Mulert C (2009) Functional neuroanatomy of CCK-4-induced panic attacks in healthy volunteers. Hum Brain Mapp 30:511–522
Etkin A, Wager TD (2007) Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am J Psychiatry 164:1476–1488
Etkin A, Prater KE, Hoeft F, Menon V, Schatzberg AF (2010) Failure of anterior cingulate activation and connectivity with the amygdala during implicit regulation of emotional processing in generalized anxiety disorder. Am J Psychiatry 167:545–554
Felmingham K, Kemp A, Williams L, Das P, Hughes G, Peduto A, Bryant R (2007) Changes in anterior cingulate and amygdala after cognitive behavior therapy of posttraumatic stress disorder. Psychol Sci 18:127–129
Ferreira LK, Busatto GF (2010) Heterogeneity of coordinate-based meta-analyses of neuroimaging data: an example from studies in OCD. Br J Psychiatry 197:76–77
Francati V, Vermetten E, Bremner JD (2007) Functional neuroimaging studies in posttraumatic stress disorder: review of current methods and findings. Depress Anxiety 24:202–218
Giardino ND, Friedman SD, Dager SR (2007) Anxiety, respiration, and cerebral blood flow: implications for functional brain imaging. Compr Psychiatry 48:103–112
Grillon C, Baas JMP, Cornwell B, Johnson L (2006) Context conditioning and behavioral avoidance in a virtual reality environment: effect of predictability. Biol Psychiatry 60:752–759
Gustavsson A, Svensson M, Jacobi F, Allgulander C, Alonso J, Beghi E, Dodel R, Ekman M, Faravelli C, Fratiglioni L, Gannon B, Jones DH, Jennum P, Jordanova A, Jönsson L, Karampampa K, Knapp M, Kobelt G, Kurth T, Lieb R, Linde M, Ljungcrantz C, Maercker A, Melin B, Moscarelli M, Musayev A, Norwood F, Preisig M, Pugliatti M, Rehm J, Salvador-Carulla L, Schlehofer B, Simon R, Steinhausen HC, Stovner LJ, Vallat JM, Van den Bergh P, van Os J, Vos P, Xu W, Wittchen HU, Jönsson B, Olesen J, CDBE2010Study Group (2011) Cost of disorders of the brain in Europe 2010. Eur Neuropsychopharmacol 21:718–779
Hayes JP, Hayes SM, Mikedis AM (2012) Quantitative meta-analysis of neural activity in posttraumatic stress disorder. Biol Mood Anxiety Disord 2:9
Ioannidis JP (2011) Excess significance bias in the literature on brain volume abnormalities. Arch Gen Psychiatry 68:773–780
Ipser JC, Singh L, Stein DJ (2013) Meta-analysis of functional brain imaging in specific phobia. Psychiatry Clin Neurosci 67:311–322
Karl A, Schaefer M, Malta LS, Dörfel D, Rohleder N, Werner A (2006) A meta-analysis of structural brain abnormalities in PTSD. Neurosci Biobehav Rev 30:1004–1031
Kessler RC, Petukhova M, Sampson NA, Zaslavsky AM, Wittchen HU (2012) Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res 21:169–184
LaBar KS, Gatenby JC, Gore JC, LeDoux JE, Phelps EA (1998) Human amygdala activation during conditioned fear acquisition and extinction: a mixed-trial fMRI study. Neuron 20:937–945
Lanius RA, Vermetten E, Loewenstein RJ, Brand B, Schmahl C, Bremner JD, Spiegel D (2010a) Emotion modulation in PTSD: clinical and neurobiological evidence for a dissociative subtype. Am J Psychiatry 167:640–647
Lanius RA, Frewen PA, Vermetten E, Yehuda R (2010b) Fear conditioning and early life vulnerabilities: two distinct pathways of emotional dysregulation and brain dysfunction in PTSD. Eur J Psychotraumatol 1:5467
LeDoux JE (2000) Emotion circuits in the brain. Ann Rev Neurosci 23:155–184
Liberzon I, Sripada CS (2008) The functional neuroanatomy of PTSD: a critical review. Prog Brain Res 167:151–169
Lissek S (2012) Toward an account of clinical anxiety predicated on basic, neurally mapped mechanisms of Pavlovian fear-learning: the case for conditioned overgeneralization. Depress Anxiety 29:257–263
Lissek S, Powers AS, McClure EB, Phelps EA, Woldehawariat G, Grillon C, Pine DS (2005) Classical fear conditioning in the anxiety disorders: a meta-analysis. Behav Res Ther 43:1391–1424
Lissek S, Rabin S, Heller RE, Lukenbaugh D, Geraci M, Pine DS, Grillon C (2010) Overgeneralization of conditioned fear as a pathogenic marker of panic disorder. Am J Psychiatry 167:47–55
Lueken U, Straube B, Reinhardt I, Maslowski NI, Wittchen HU, Ströhle A, Wittmann A, Pfleiderer B, Konrad C, Ewert A, Uhlmann C, Arolt V, Jansen A, Kircher T (2013) Altered top-down and bottom-up processing of fear conditioning in panic disorder with agoraphobia. Psychol Med 23:1–14
Martinez JM, Coplan JD, Browne ST, Goetz R, Welkowitz LA, Papp LA, Klein DF, Gorman JM (1998) Hemodynamic response to respiratory challenges in panic disorder. J Psychosom Res 44:153–161
Menzies L, Chamberlain SR, Laird AR, Thelen SM, Sahakian BJ, Bullmore ET (2008) Integrating evidence from neuroimaging and neuropsychological studies of obsessive-compulsive disorder: the orbitofronto-striatal model revisited. Neurosci Biobehav Rev 32:525–549
Michael T, Blechert J, Vriends N, Margraf J, Wilhelm FH (2007) Fear conditioning in panic disorder: enhanced resistance to extinction. J Abnorm Psychol 116:612–617
Milad MR, Quirk GJ (2012) Fear extinction as a model for translational neuroscience: ten years of progress. Annu Rev Psychol 63:129–151
Milad MR, Wright CI, Orr SP, Pitman RK, Quirk GJ, Rauch SL (2007) Recall of fear extinction in humans activates the ventromedial prefrontal cortex and hippocampus in concert. Biol Psychiatry 62:446–454
Milad MR, Pitman RK, Ellis CB, Gold AL, Shin LM, Lasko NB, Zeidan MA, Handwerger K, Orr SP, Rauch SL (2009) Neurobiological basis of failure to recall extinction memory in posttraumatic stress disorder. Biol Psychiatry 66:1075–1082
Nitschke JB, Sarinopoulos I, Oathes DJ, Johnstone T, Whalen PJ, Davidson RJ, Kalin NH (2009) Anticipatory activation in the amygdala and anterior cingulate in generalized anxiety disorder and prediction of treatment response. Am J Psychiatry 166:302–310
Pape HC, Pare D (2010) Plastic synaptic networks of the amygdala for the acquisition, expression, and extinction of conditioned fear. Physiol Rev 90:419–463
Pavlov IP (1927) Conditioned reflexes. Oxford University Press, London
Peng Z, Lui SS, Cheung EF, Jin Z, Miao G, Jing J, Chan RC (2012) Brain structural abnormalities in obsessive-compulsive disorder: converging evidence from white matter and grey matter. Asian J Psychiatry 5:290–296
Phelps EA, Delgado MR, Nearing KI, LeDoux JE (2004) Extinction learning in humans: role of the amygdala and vmPFC. Neuron 43:897–905
Pitman RK, Rasmusson AM, Koenen KC, Shin LM, Orr SP, Gilbertson MW, Milad MR, Liberzon I (2012) Biological studies of post-traumatic stress disorder. Nat Rev Neurosci 13:769–787
Pole N (2007) The psychophysiology of posttraumatic stress disorder: a meta-analysis. Psychol Bull 133:725–746
Radua J, Mataix-Cols D (2009) Voxel-wise meta-analysis of grey matter changes in obsessive-compulsive disorder. Br J Psychiatry 195:393–402
Rauch SL, Shin LM, Phelps EA (2006) Neurocircuitry models of posttraumatic stress disorder and extinction: human neuroimaging research–past, present, and future. Biol Psychiatry 60:376–382
Rodnick EH (1937) Characteristics of delayed and trace conditioned responses. J Exp Psychol 20:409–425
Rotge JY, Guehl D, Dilharreguy B, Cuny E, Tignol J, Bioulac B, Allard M, Burbaud P, Aouizerate B (2008) Provocation of obsessive-compulsive symptoms: a quantitative voxel-based meta-analysis of functional neuroimaging studies. J Psychiatry Neurosci 33:405–412
Rotge JY, Guehl D, Dilharreguy B, Tignol J, Bioulac B, Allard M, Burbaud P, Aouizerate B (2009) Meta-analysis of brain volume changes in obsessive-compulsive disorder. Biol Psychiatry 65:75–83
Schwarzbauer C, Mildner T, Heinke W, Brett M, Deichmann R (2010) Dual echo EPI–the method of choice for fMRI in the presence of magnetic field inhomogeneities? Neuroimage 49:316–326
Sehlmeyer C, Schöning S, Zwitserlood P, Pfleiderer B, Kircher T, Arolt V, Konrad C (2009) Human fear conditioning and extinction in neuroimaging: a systematic review. PLoS One 4:e5865
Shin LM, Wright CI, Cannistraro PA, Wedig MM, McMullin K, Martis B, Macklin ML, Lasko NB, Cavanagh SR, Krangel TS, Orr SP, Pitman RK, Whalen PJ, Rauch SL (2005) A functional magnetic resonance imaging study of amygdala and medial prefrontal cortex responses to overtly presented fearful faces in posttraumatic stress disorder. Arch Gen Psychiatry 62:273–281
Spoormaker VI, Andrade KC, Schröter MS, Sturm A, Goya-Maldonado R, Sämann PG, Czisch M (2011) The neural correlates of negative prediction error signaling in human fear conditioning. Neuroimage 54:2250–2256
Starkman MN, Giordani B, Gebarski SS, Schteingart DE (2003) Improvement in learning associated with increase in hippocampal formation volume. Biol Psychiatry 53(3):233–238
Steckle LC (1933) A trace conditioning of the galvanic reflex. Gen Psychol 9:475–480
Switzer SA (1934) Anticipatory and inhibitory characteristics of delayed conditioned reactions. J Exp Psychol 17:603–620
Tuescher O, Protopopescu X, Pan H, Cloitre M, Butler T, Goldstein M, Root JC, Engelien A, Furman D, Silverman M, Yang Y, Gorman J, LeDoux J, Silbersweig D, Stern E (2011) Differential activity of subgenual cingulate and brainstem in panic disorder and PTSD. J Anxiety Disord 25:251–257
Vermetten E, Lanius RA (2012) Biological and clinical framework for posttraumatic stress disorder. In: Schlaepfer TE, Nemeroff CB (eds) Neurobiology of psychiatric disorders, vol 106 (3rd series), Handbook of clinical neurology. Elsevier, London, pp 291–342
Vermetten E, Vythilingam M, Southwick SM, Charney DS, Bremner JD (2003) Long-term treatment with paroxetine increases verbal declarative memory and hippocampal volume in posttraumatic stress disorder. Biol Psychiatry 54:693–702
Vermetten E, Schmahl C, Southwick SM, Bremner JD (2007) Positron tomographic emission study of olfactory induced emotional recall in veterans with and without combat-related posttraumatic stress disorder. Psychopharmacol Bull 40:8–30
Vythilingam M, Heim C, Newport J, Miller AH, Anderson E, Bronen R, Brummer M, Staib L, Vermetten E, Charney DS, Nemeroff CB, Bremner JD (2002) Childhood trauma associated with smaller hippocampal volume in women with major depression. Am J Psychiatry 159:2072–2080
Wegerer M, Blechert J, Kerschbaum H, Wilhelm FH (2013) Relationship between fear conditionability and aversive memories: evidence from a novel conditioned-intrusion paradigm. PLoS ONE 8:e79025. doi:10.1371/journal.pone.0079025
Wessa M, Flor H (2007) Failure of extinction of fear responses in posttraumatic stress disorder: evidence from second-order conditioning. Am J Psychiatry 164:1684–1692
Whalen PJ, Johnstone T, Somerville LH, Nitschke JB, Polis S, Alexander AL, Davidson RJ, Kalin NH (2008) A functional magnetic resonance imaging predictor of treatment response to venlafaxine in generalized anxiety disorder. Biol Psychiatry 63:858–863
Wittchen HU, Jacobi F, Rehm J, Gustavsson A, Svensson M, Jönsson B, Olesen J, Allgulander C, Alonso J, Faravelli C, Fratiglioni L, Jennum P, Lieb R, Maercker A, van Os J, Preisig M, Salvador-Carulla L, Simon R, Steinhausen HC (2011) The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol 21:655–679
Yassa MA, Hazlett RL, Stark CE, Hoehn-Saric R (2012) Functional MRI of the amygdala and bed nucleus of the stria terminalis during conditions of uncertainty in generalized anxiety disorder. J Psychiatr Res 46:1045–1052
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Berlin Heidelberg
About this chapter
Cite this chapter
Spoormaker, V.I., Vermetten, E., Czisch, M., Wilhelm, F.H. (2014). Functional Neuroimaging of Anxiety Disorders. In: Mulert, C., Shenton, M. (eds) MRI in Psychiatry. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-54542-9_15
Download citation
DOI: https://doi.org/10.1007/978-3-642-54542-9_15
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-54541-2
Online ISBN: 978-3-642-54542-9
eBook Packages: MedicineMedicine (R0)