
Abstract
Anxiety disorders have the highest lifetime prevalence rates (33.7%) and the youngest age of onset (median age, 11 years old) than any other mental illness in the United States. Further epidemiological research suggests that anxiety disorders often precede onset of other psychiatric conditions and worsen prognosis compared to individuals without anxiety. Current neuropsychiatric research exploring the biological underpinnings of anxiety and stress disorders such as generalized anxiety disorders (GAD), social anxiety disorder (SAD), specific phobia, panic disorder (PD), and posttraumatic stress disorder (PTSD) may be able to identify which structures can be targeted in treatment and interventions for said disorders.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Although the Diagnostic and Statistical Manual of Mental Disorders – 5 (DSM-5) has categorized each anxiety disorder based on its behavioral and subjective presentations, the neuroimaging literature suggests that biological mechanisms may be shared among the disorders [1, 2]. Generally, the neural activation of anxiety disorders can be categorized as either fear-driven activation or worry-driven activation [2, 3]. Fear-driven disorders are those that have a transient, fight-or-flight reaction coupled with hyperarousal to a distinct and immediate threat [2]. For example, specific phobia and social anxiety disorder (SAD) are fear-driven responses due to the clearly identified stimulus (e.g., spiders, snakes, crowds, etc.) accompanied by a disproportionately heightened state of arousal (e.g., racing heart, increased sweating, etc.) which dissipates once the stimulus is no longer present. On the other hand, worry- and stress-driven disorders are those which have more extensive periods of apprehension, worry, and despair over future or hypothetical situations that may not always be clearly defined [2]. In this chapter, we will first discuss the main experimental paradigms used to explore the neural mechanisms of anxiety disorders in both rodents and humans, discuss the basic functions of each structure implicated in these disorders, and then explore the role each structure is currently believed to play in specific disorders.
There are several experimental paradigms used to observe neural activity in anxiety disorders. Those paradigms usually fall under three categories: neutral-state paradigms, symptom-induction paradigms, and cognitive-activation paradigms. In neutral-state paradigms (e.g., resting-state fMRI), participants are often performing a continuous, idle task (e.g., staring at a white cross). Such paradigms are able to capture differences in brain activation between healthy individuals and individuals suffering for anxiety and stress disorders in the absence of triggering stimuli. Conversely, symptom-induced paradigms aim to measure brain function while an individual’s symptoms have been purposefully induced (e.g., showing an image of a spider to someone with arachnophobia). This allows for the comparison of healthy and anxious individuals in order to determine physiological differences in the induced state. Lastly, cognitive-activation paradigms aim to induce activation of a specific neuropathway through carefully designed tasks. All three paradigm types are used with neuroimaging techniques measuring blood flow or blood-glucose levels as indices of brain activity such as positron emission tomography (PET), trace-guided single-photon emission computed tomography (SPECT), and functional magnetic resonance imaging (fMRI [4]).
One important distinction to bear in mind when reading fMRI studies is the difference between regional activation and resting-state functional connectivity. “Activation” of a brain region indicates that this area is more (or less) active in one condition (e.g., when viewing a stimulus) versus another (e.g., when viewing a black screen). This is termed a “contrast,” and the quantity contrasted is the blood-oxygen level-dependent (BOLD) MR response that is proportional to the relative amounts of oxygenated and deoxygenated hemoglobin of the blood in that area. Activation can then be compared between groups (e.g., panic disorder vs. controls) by comparing their contrasts to the same pair of conditions. On the other hand, resting-state functional connectivity (rsFC) refers to networks of two or more regions of the brain whose BOLD signals fluctuate in synchrony at very low frequencies (e.g., 0.01 and 0.1 Hz) when a research subject is lying quietly awake looking at a fixation cross [5]. It is the degree of synchrony in such oscillations between two or more regions that is being compared when rsFC differences between different groups are being evaluated. Several studies have demonstrated that brain areas that are highly correlated in function will also have highly correlated BOLD signal changes during rsFC (for more details and clinical applications, see [5,6,7]). Of note, differing from both of these methods is “psychophysiological interaction” or PPI, an activational measure in which the degree to which different areas activate together during a particular contrast is assessed.
The fear-conditioning and extinction paradigms are among the most commonly used cognitive-activation paradigms in the neuroimaging of anxiety and stress disorders (see [8,9,10] for reviews). These paradigms rely on Pavlovian conditioning and extinction in order to experimentally mimic these processes. Fear conditioning involves the repetitive presentation of a stimulus which does not elicit an inherent fear response (e.g., a blue light), also known as the conditioned stimulus (CS), with an inherently fearful or unpleasant stimulus (e.g., electric shocks; an unconditioned stimulus or US). Over time, the previously neutral stimulus alone is able to elicit a fearful conditioned response (CR) from the subject (e.g., increased heart rate, skin conductance response). Fear extinction, in turn, is when the CS is repeatedly presented without the US, signaling that the US will no longer follow the CS. Over time, the CS will no longer elicit the CR. Of importance to the treatment of anxiety disorders is the fact that extinction represents a new, inhibitory memory that competes with the conditioned fear memory when the CS is again encountered [8, 11, 12]. Which memory prevails determines whether or not fear will be expressed [13, 14]. Fear-conditioning and extinction paradigms have demonstrated robust and reliable responses in laboratory settings and have been instrumental in mapping potential brain regions necessary for fear and extinction acquisition and memory in both animals and in humans [8, 15]. Some of the structures implicated in the fear-acquisition process are the amygdala, dorsal anterior cingulate cortex (dACC), insular cortex, and hippocampus [3, 16]. Extinction learning and memory on the other hand involve the ventromedial prefrontal cortex (vmPFC) in addition to the hippocampus [3, 8, 11, 17]. Although these findings have served as a foundation for exploring the neurocircuitry of anxiety disorders, the role of the aforementioned structures in individual disorders is still under investigation (e.g., [18,19,20]).
In anxiety disorders and mood disorders with anxious features, stressors may trigger an enhanced activation of the limbic-hypothalamic-pituitary-adrenal axis (LHPA), the sympathetic nervous system, and other central stress mechanisms [3]. Studies suggest that activation and inhibition of stress responses are governed by the same structures identified in fear-conditioning and extinction paradigms (e.g., vmPFC, dACC, dorsomedial prefrontal cortex, insular cortex, amygdala, and hippocampus) [2, 21]. However, activation of the LHPA does not always occur during fear conditioning, and fear is not normally reported at other times when the LHPA is activated (e.g., when eating a meal or feeling nauseated [22, 23]). Therefore, overlap in structural activation does not imply functional overlap, and it is important to note that the same brain structures may have different functions in the manifestation of different anxiety-related disorders [2, 3, 22]. In order to better understand how this may happen, we will look at how the main structures implicated in anxiety disorders (i.e., the amygdala, anterior cingulate cortex, insular cortex, hippocampus, and ventromedial prefrontal cortex) may predispose individuals to anxiety disorders.
Brain Structures Implicated Across Anxiety Disorders
Amygdala
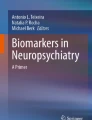
Several studies support the hypothesis that overactivation of the amygdala may be the primary culprit in anxiety disorders. As seen in Fig. 2.1, the amygdalae are located above the hippocampus in the ventromedial portion of the temporal lobe. Generally, the amygdala is involved in the processing of emotionally valanced stimuli, especially aversive stimuli. The amygdala has been shown to reliably activate during tasks requiring the perception of fearful stimuli and cues predicting aversive outcomes, as well as the encoding and expression of fear behaviors [22, 24]. This makes the amygdala not only critical for information processing but also makes it one of the brain’s key relay stations for anticipatory, avoidant, and fear-related behaviors. Several studies have shown that amygdala sensitivity to negative stimuli may be affected by the specific alleles of the 5-HTT-linked polymorphic region (5-HTTLPR) of the serotonin transporter gene carried by an individual [25]. The short and long alleles of 5-HTTLPR differentially affect amygdala sensitivity to dangerous environmental stimuli with individuals carrying the short allele being more reactive [26]. Another study found that those carrying at least one short allele showed greater amygdala reactivity when faced with social provocation (i.e., giving a speech to a public and private audience of study staff), with those homozygous for the short allele showing yet greater amygdala reactivity [27]. Interestingly, another study found that the short form of 5-HTTLPR is not only associated with hyperactivation of the amygdala but those carrying it also showed increased activation of the entire pathway implicated with threat anticipation [28]. These findings provide strong support for the genetic basis of psychopathology. Nonetheless, the 5-HTTLPR polymorphism may not be the only etiological factor leading to pathological functioning of the amygdala. During adolescence, an emotionally critical developmental period, the amygdala is naturally hypersensitive in order for humans to learn the social rules and emotional consequences of their environments [22, 29,30,31]. Studies show that pathological anxiety may arise when this hyperactivity fails to attenuate at the end of early adulthood [30]. Even individuals with non-pathological levels of anxiety, such as those who report higher state anxiety, demonstrate increased amygdala activation to fearful facial expressions compared to neutral facial expressions [32]. Together, these findings begin to elucidate how the non-pathological functions of the amygdala may predispose some individuals to the development of anxiety disorders.

Coronal rendering of the right amygdala
Bed Nucleus of the Stria Terminalis (BNST)
The BNST, located just above the amygdala, is part of a neural circuit termed the extended amygdala, and, like its neighbor, is implicated in the processing of negatively valanced emotional stimuli [33, 34]. There is increasing evidence that this structure is involved in the etiology and symptoms of anxiety disorders due to its prominent role in sustained and anticipatory fear and anxiety states [35]. The BNST projects directly to the hypothalamus and brainstem, mediating autonomic and behavioral responses to stress [36]. Lesion studies suggest that fear conditioning remains partially intact following bilateral damage to the amygdala suggesting a role for the BNST as a compensatory circuitry for fear processing [37, 38]. From these findings, researchers postulate that the BNST may be involved in anxious and avoidant responses that are slower in onset and longer-lasting in duration, making this structure a potentially key player in the maintenance of generalized anxiety disorder (GAD) symptoms [36]. Its role is often contrasted with that of the amygdala which generates acute fear responses, whereas the BNST generates sustained anxiety and threat apprehension [35].
Anterior Cingulate Cortex (ACC)
Although literature on the ACC is not as extensive as that on the amygdala, early research in cats and rodents has demonstrated that the ACC is involved in a large array of cognitive emotional and behavioral processes, including error detection, conflict monitoring, sensory and motor control, regulation of endocrine and autonomic functioning, processing of nociceptive stimuli, assessment of emotional content and valence, emotion regulation, and social cognition [39,40,41]. As one might expect, the anterior cingulate cortex is also strongly connected to the amygdala and medial prefrontal cortex (mPFC [3, 40]). In fact, due to the large and heterogeneous nature of the mPFC and the ACC, earlier studies may have characterized activation in these regions simply as mPFC activity. One meta-analysis exploring this issue in anatomical specificity indicated that most study results reporting PFC activation converged into two, specific subregions of the ACC, suggesting that these regions are also critical for emotion regulation [42]. The ACC can be divided into at least three distinct regions: the dorsal anterior cingulate cortex (dACC), the rostral anterior cingulate cortex (rACC), and the subgenual anterior cingulate cortex (sgACC).
Dorsal Anterior Cingulate Cortex (dACC)
Among its many functions, the dACC is involved in the modulation of attention (particularly to novel stimuli), sensory response selection, complex motor skills, and anticipation of taxing activities and nociception [41]. It has been argued that the function of the dACC is, in most general terms, the perception and processing of both physical and psychological distress in order to initiate survival-relevant behaviors [43]. Interestingly, the dACC has been reported to coincidentally activate in fear-conditioning studies designed to target the amygdala [44, 45]. Furthering these findings, Milad et al. [46] showed that healthy (non-anxious) individuals with greater thickness of the dACC had higher galvanic skin response (GSR) readings, during a fear-conditioning task. Furthermore, dACC activation was greater during presentation of the conditioned stimulus than of the innately fearful stimulus, suggesting that the dACC may play a role in the expression of psychophysiological fear responses [46]. In resting-state studies, the dACC is considered a major component of the “salience network,” a group of structures also including the amygdala and insula that function to direct attention toward goal-relevant and other salient stimuli, such as those that evoke fear [47], that also contains central regulators of autonomic arousal [48].
Rostral Anterior Cingulate Cortex (rACC)
In contrast to the dACC, the rACC has been shown to be involved in regulation and assessment of, as well as response to, emotionally valanced and motivational stimuli [41]. In two versions of a Stroop-type interference task, one with cognitive interference and the other with emotionally salient interference, greater activation of the rACC was seen in the task containing the emotionally salient interference task [49]. The rACC has been shown to be involved in the suppression of emotional responses (both pleasant and aversive [50]). As previously mentioned, activation of the ACC has been strongly correlated with activation of the amygdala since the early days of research in this region, which we now know is mostly accounted for by activation in the rACC [40]. Moreover, Etkin et al. [51] demonstrated that the rACC may directly inhibit amygdala activation, as shown by simultaneous decrease in amygdala action as activation of the rACC increases during resolution in an emotional-conflict task. Thus the rACC is considered a key structure participating in top-down control of amygdala activity and accompanying emotional arousal [52, 53].
Subgenual Anterior Cingulate Cortex (sgACC)
The sgACC, a region of the ACC lying below the genu of the corpus callosum (Fig. 2.4) and corresponding to Brodmann Area 25, plays a prominent role in anterior cingulate control of autonomic and homeostatic processes [54]. The sgACC is best known in psychiatry for well-documented abnormalities of this region in major depressive and bipolar disorders [55] and as a target for deep-brain stimulation to treat major depression [56]. Nonetheless, it has also been linked to symptoms of anxiety-related disorders [57] and anxious personality traits [58]. The sgACC is just caudal to but probably not functionally similar to the vmPFC, a structure key to extinction learning and memory (see below), although some studies have shown a degree of overlap [59]. Mayberg [60] demonstrated that greater activity of the posterior subgenual vmPFC is associated with greater MDD severity and where others have shown that posttreatment MDD patients have decreased posterior, subgenual vmPFC activity [60,61,62,63].
In summary, it appears the dACC (Fig. 2.2) may be implicated in fear acquisition through appraisal of threatening stimuli and arousal, while the rACC (Fig. 2.3) is implicated in regulation of fear through top-down inhibition of fear- and anxiety-related responses (e.g., arousal, avoidance, etc.) [64]. These structures, together with the vmPFC (and possibly portions of the sgACC; Fig. 2.4) are involved in the degree to which anxiety- and fear-related responses are expressed or inhibited.

Sagittal rendering of the dorsal anterior cingulate cortex

Sagittal rendering of the rostral anterior cingulate cortex

Sagittal rendering of the subgenual anterior cingulate cortex
Insular Cortex
The insular cortex (Fig. 2.5) is believed to play a key role in interoception—the perception of the internal state of the body from information conveyed to the cortex by afferent pathways from the body via brainstem and thalamic intermediaries [65,66,67,68]. Abnormalities in the perception of interoceptive information are believed to contribute to symptoms of multiple psychiatric conditions including anxiety disorders [69,70,71]. The insula shows a posteroanterior gradient in successive stages of interoceptive processing [66, 68]. Posterior regions receive interoceptive information from ascending inputs, middle regions integrate this information with other sensory modalities, and such integrated information is then re-represented in the anterior insula where it contributes to subjective feeling states in concert with prefrontal areas [66, 68]. Laboratory studies have shown insula activation during a wide array of processes in addition to interoception such as emotional and self-awareness, empathy and empathic pain, and time perception [66, 72,73,74]. Of clinical interest, the insula is implicated in threat anticipation and situational uncertainty [22, 66]. Studies with healthy individuals have demonstrated greater activation of the insula upon the presentation of an aversive stimulus when the stimulus followed an uncertain cue, such that at times the cue was followed by a neutral stimulus and at times was followed by the aversive stimulus [75]. Interestingly, almost 75% of this sample overestimated the presence of an aversive stimulus following the uncertain cue, and insular activation was positively correlated with this estimate. Considering its role in threat detection, it should come to no surprise that activity in the insular cortex is highly correlated with amygdala and rACC activation, such that rACC activation caused by anticipation of an aversive stimulus was negatively correlated with activation of the insula and amygdala [22, 66, 75]. In fMRI, comparisons between anxiety-disordered and healthy individuals presented with [1] or anticipating [76,77,78,79] aversive stimuli, greater insula activation in anxious individuals is ubiquitously seen. Researchers hypothesize that the insula may play a role in pathological anxiety by overestimating the frequency of aversive outcomes in ambiguous situations or by incorrectly categorizing the situation as being predictive of an aversive outcome due to hyperactivation of the amygdala [22, 80]. Notably, in PPI studies, co-activation of the insula and dACC is often seen during processing of threat or pain [81], and, in rsFC studies, the insula appears as a key node of the salience network [47].

Coronal rendering of the right and left insular cortex
Hippocampus
The hippocampus (Fig. 2.6) is most commonly known for its role in memory formation as seen in the famous case of the patient H.M., who was no longer able to encode new declarative memories but who had perfect cognitive functioning otherwise, including encoding of new procedural memories, following a lobectomy that removed a sizable portion of his hippocampus. A key memory-related function of the hippocampus, which may become impaired in anxiety and anxiety-related disorders such as PTSD, is the provision of contextual information to disambiguate whether a stimulus that could represent danger in fact does so [11, 82]. However, the hippocampus is also involved in autonomic functions and is part of the negative-feedback loop of the hypothalamic-adrenal-pituitary (HPA) axis stress-response pathway [3, 83]. Functionally, the hippocampus can be split into two regions: (1) the dorsal hippocampus, which has been historically implicated in the processing and encoding of memories and learning, and (2) the ventral hippocampus, which is implicated in anxiety and stress responses [84]. Although some have argued in favor of the functional dichotomy of the hippocampus with findings that lesions to the ventral hippocampus lead to inhibition of anxiety response (i.e., freezing) in contextual conditioned-freezing paradigms, Bannerman et al. [84] propose that the ventral hippocampus’ extensive and unique role in projection to the prefrontal cortex may be the pathway through which the hippocampus is able to regulate encoding of aversive and threatening memories [85, 86].

Coronal rendering of the right and left hippocampus
Inferior Prefrontal Cortex (PFC)
Broadly, the prefrontal cortex is involved in the processing and implementation of executive functions such as planning, decision-making, personality expression, behavioral inhibition, and emotion regulation. Here, we will take a closer look into the role of the inferior PFC in response inhibition and emotion regulation. Early research on the PFC demonstrated greater activation of the right inferior PFC (rIFC) during the inhibition phase of the go/no-go task (where participants are asked to inhibit a prepotent response following a seldom-occurring cue) in healthy adults [87, 88]. Further evidence in lesion studies demonstrate that damage to the right inferior PFC is associated with poorer no-go trial performance in both humans and primates [89]. Decreased activation in the rIFC may be the underlying cause for response-inhibition difficulties in persons with attention-deficit hyperactivity disorder (ADHD) who demonstrate both poorer inhibition on no-go trials and decreased right, inferior PFC activation [87]. Subsequently, the rIFG has been implicated in domain-general inhibition (e.g., of action, cognition, emotion) [87, 88, 90, 91], and impairment of its inhibitory function has been linked with anxiety-related syndromes such as posttraumatic stress disorder (PTSD) [92, 93]. Notably, to engage higher-level emotion-regulatory processes such as cognitive reappraisal, the lateral PFC may recruit more primitive paralimbic regions along with their associated functions such as fear extinction [94].
Ventromedial Prefrontal Cortex (vmPFC)
The vmPFC (Fig. 2.7) is often implicated in neuroimaging studies of anxiety disorders [63] most often suggesting that the vmPFC suppresses negative affect through the inhibition of amygdala activation [59, 95,96,97]. For example, studies have demonstrated decreased activity in the vmPFC during trauma reminders as well as fear-conditioning paradigms with PTSD patients compared to trauma-exposed controls [97,98,99,100]. However, there also exist controversies. In a lesion study with war veterans which suggested that veterans with damage to the vmPFC were actually less likely to develop PTSD than those with intact vmPFC. [63, 101] note that several other studies have found a negative relationship between vmPFC activity and reported anxiety symptoms. Therefore, Myers-Schulz et al. [63] propose that the vmPFC as a whole is involved in the general modulation of amygdala activity, including both inhibitory and excitatory functions, and that each of these is modulated by subregions of the vmPFC: the posterior vmPFC (corresponding to the sgACC) and the perigenual PFC. Together, these studies suggest that the perigenual area of the vmPFC may be modulating positive affect, while the posterior vmPFC/sgACC may be modulating negative affect [63].

Sagittal rendering of the left vmPFC
Integrative Models
As one can see, deviances from each of these structures’ non-pathological, and often evolutionarily adaptive, functions may lead to exacerbated fear encoding, anxiety, and excitatory responses. Basic research using animal models in combination with fear-acquisition paradigms have been able to identify some of the macro-circuitry involved in anxiety disorders. Such models begin to elucidate the pathways associated with threat interpretation, evaluation, and response loops. The literature suggests that initial threat interpretation starts in the amygdala, projects to the BNST, and then follows to the hippocampus and medial prefrontal cortex (mPFC [102]). In this pathway, the amygdala’s major nucleus of information processing (basolateral amygdala or BLA) not only assigns emotional valance to a stimulus but also creates connections indicating the predictive value of a stimulus (Fig. 2.8 [102, 103]). In other words, this step determines whether neutral stimuli predict positive or negative outcomes, in addition to evaluating the valence of the outcome itself. The assigned valence to emotional content is then processed in the mPFC and hippocampus, which determine whether or not it is worthy of enhanced vigilance based on previous experiences, and then projects the signal back to the BNST and the amygdala [102]. An interesting concomitant to more extended processing networks LeDoux’s [104] concept of a “high” and “low” road to fear responses whereby sensory cues indicative of danger can bypass more extensive processing in sensory cortices and instead trigger motor responses via a low road proceeding from the sensory thalamus directly to the BLA and, thence, via the central nucleus (CeA, the main amygdala output nucleus) to rapid defensive responses mediated by the hypothalamus, autonomic nervous system, and brainstem. In addition to sensory cues alone, such responses in the amygdala can be modified by the evaluation of contextual information in the hippocampus [104]. Considering how these structures are some of the brain’s main information-processing and relay centers, it is no surprise that changes in one region may trigger a cascade of events that go on to cause neurochemical and anatomical deviances. Although each anxiety disorder may not implicate all of these brain regions due to distinct features of their behavioral and cognitive manifestations, these structures serve as the main foundation for fear acquisition, extinction, and maintenance. Below, we will explore current hypotheses for the neural mechanisms behind specific phobia, generalized anxiety disorders (GAD), social anxiety disorder (SAD), panic disorder (PD), and posttraumatic stress disorder (PTSD).

Representative structures engaged in normal and pathological anxiety and the behavioral responses subserved. Connectivity illustrated is highly simplified and does not show extensive interconnections among structures depicted (e.g., BNST and vmPFC) and not depicted (e.g., sgACC, ventral striatum). BNST bed nucleus of the stria terminalis, dACC dorsal anterior cingulate cortex, HPA hypothalamic-pituitary-adrenal, LC locus coeruleus, LPFC-lateral prefrontal cortex, PAG periaqueductal gray, PVN paraventricular nucleus, vmPFC ventromedial prefrontal cortex, Red structures: fear and anxiety promoting. Blue structures: fear and anxiety regulatory
Neural Mechanisms Implicated in Specific Anxiety Disorders
Specific Phobia
Specific phobia is perhaps one of the disorders most closely modeled by the fear paradigm due to having a clearly identified stimulus and a fear response that dissipates upon the removal of the stimulus. There is also a clearer body of literature detailing the neural pathway of specific phobias than that of other anxiety disorders. Studies exploring the neurocircuitry of specific phobia have reported increased activation and connectivity of the amygdala, with the degree of amygdala hyperactivation predicting symptom severity [2, 3, 105]. However, findings are mixed, and results consistently show hyperactivation of other fear-processing and fear-response regions such as the insula and dACC suggesting an overall exacerbated fear response throughout the salience network in individuals with specific phobia [2, 3]. Furthermore, other studies have also shown decreased activation of the vmPFC when participants were presented with phobic stimuli, suggesting less regulation of the amygdala by the PFC [106]. Cognitive behavioral therapy as well as the habituation and extinction resulting from exposure to phobic stimuli has been demonstrated to decrease activation of the dACC and the insula in individuals with specific phobia, but not to increase activation of the vmPFC [3]. These results suggest that there is a greater dysfunction in the threat-processing and threat-response regions than in emotion-regulatory regions for individuals with specific phobia. It is important to note, however, that neural activation in individuals with specific phobia will differ slightly depending on the phobic stimuli. For example, Hilbert et al. [107] found increased white matter volume in the left PFC in individuals with dental phobia, but not in individuals with snake phobia. An interesting ongoing controversy is whether some of the most common phobic stimuli (e.g., spiders, snakes, heights) are “biologically prepared” or potentiated by brain mechanisms that evolved in response to environmental threats in ancestral humans [108, 109]. Like specific phobia, we also see unique patterns of activation in SAD, which are discussed next.
Social Anxiety Disorder (SAD)
The general pathophysiology of SAD is similar to that of other fear- and worry-driven disorders in that there is an abnormality in the threat interpretation, evaluation, and response circuits of the brain. However, as we mentioned in earlier sections, the disorder’s hallmark feature of anxiety surrounding social situations leads to somewhat different activation patterns than those of strictly fear- or worry-driven disorders. SAD differs from other anxiety disorders as it encompasses worry, constant self-evaluation, and out-of-proportion fear reactions to specific stimuli [110]. Much like in GAD, SAD neurobiology has implicated abnormalities in emotion-regulation structures such as the amygdala, insula, ACC, hippocampus, and mPFC [111]. Uniquely, studies with SAD patients have demonstrated elevated activity in the fusiform gyrus’ face area and occipital lobe when patients were presented with images of fearful faces (compared to healthy controls [112]). These findings suggest greater processing of social stimuli for SAD patients than for healthy controls and are convergent with literature verifying that the fusiform face area is dedicated exclusively to the processing of facial features and face-like arrangements [113]. The fusiform face area also had greater connectivity to the amygdala in tasks where participants were shown fearful faces, but not in tasks involving symptom provocation (e.g., anticipation of public speaking) [112, 114,115,116,117]. Further studies have demonstrated greater rsFC of the amygdala with the rACC and insula [3, 117]. Although some studies report decreased activation in the mPFC and vmPFC in individuals with SAD, which would be consistent with findings suggesting decreased top-down regulation of the amygdala by these prefrontal structures, other studies have observed increased activation and connectivity between the amygdala and these regions [2, 3]. According to Shin and Liberzon [3], the heterogeneity in the results could be explained by a study that found delayed responses of the mPFC in SAD during the presentation of fearful faces. Nonetheless, cognitive behavioral interventions targeting cognitive reframing, or reappraisal, of negative emotions and events have demonstrated decreased activation of the amygdala following treatment [118]. These studies have also demonstrated that differences in symptom severity (namely, decreases) were negatively correlated with connectivity between the amygdala and inferior PFC regions (i.e., vmPFC and ventrolateral PFC) [116, 118]. The discordance across these results could be due to the diverse functions associated with the different subregions of the vmPFC in threat processing. Further studies are needed in order to determine the exact connectivity between the prefrontal cortex and the amygdala in SAD.
Generalized Anxiety Disorder (GAD)
There is somewhat of a dearth of literature on the neural pathways of GAD, despite its high lifetime prevalence (5%) around the world [119, 120]. Currently, the literature proposes two models for the potential pathophysiology of GAD. The first is the “emotional dysregulation model,” which proposes that individuals with GAD turn to worry due to difficulties with emotion regulation [121]. Although there is competing evidence, a large portion of studies supporting this model report hypoactivation of the mPFC and ACC in individuals diagnosed with GAD, suggesting that there may be a lack top-down regulation of amygdala activity. For example, an rsFC study showed reduced connectivity between the amygdala and frontal regions such as the dorsolateral PFC [122]. The other is the “conditioned fear generalization theory” which, as Mochcovitch et al. [121] point out, is only supported by a handful of studies. This theory postulates that conditioned fear is overgeneralized to nonthreatening, perceptually similar cues, increasing the probability that those events will also trigger fear- and anxiety-type responses [123]. Greenberg [124] found that healthy individuals seemed to recruit the insula, rACC, vmPFC, and amygdala during a fear generalization task, where we see increased activity in the insula, rACC, and amygdala activation during initial stimuli presentation which decreases as the brain determines the threat is specific to one stimulus. As this specificity occurs, we see increases in vmPFC activation and decreases in the aforementioned areas, which further supports the theory that vmPFC function is involved in amygdala regulation. When the same task was conducted with GAD participants, there appeared to be a lack of increased vmPFC activation during generalization and prolonged activation of fear evaluation, interpretation, and response loops (e.g., amygdala, dACC, and insula [124]). Although the two models propose different paths through which symptoms may develop and be maintained in GAD, they both provide compelling evidence for a deficit in regulation of responses to aversive stimuli. These findings in functional connectivity are congruent with other findings suggesting generally decreases in activation of emotion-modulation regions in GAD (i.e., hippocampus, mPFC, rACC) and increases in activation of slow- and prolonged-onset fear-response structures such as the BNST [2, 125]. In GAD, we see decreased connectivity between the amygdala and the mPFC, as well as decreased connectivity among the inferior PFC, amygdala, and rACC [126]. A recent review found that PFC hypoactivation with abnormal PFC-amygdala connectivity was the most typical finding in fMRI studies of GAD [121]. Furthermore, some studies have also found increased connectivity between the insula and the amygdala in GAD patients, suggesting hyperactivity of the salience network [2]. However, in another rsFC study, amygdala connectivity was reduced to areas of the salience network including the anterior insula and dorsal anterior cingulate cortex (dACC) but increased to areas of the central executive network—a finding interpreted as a compensatory effort to self-regulate anxiety [127]. Despite their variability, these findings together suggest that increasing emotion regulation in GAD patients may be an effective treatment target. Fortunately, studies that collected rsFC data pre- and post-CBT treatment for GAD have demonstrated not only attenuated activity of the amygdala, rACC, and mPFC during exposure to negative stimuli, but also increased activation of those areas during presentation of positively valanced stimuli (e.g., happy faces), as well as increased connectivity between the amygdala and insula [128].
Panic Disorder (PD)
Panic disorder is marked by sudden or unexpected panic attacks, along with frequent worrying about future attacks or changes in behavior related to the attacks including agoraphobia [110]. Current literature supports a pathophysiological model of PD suggesting hyperactivation of the amygdala, hippocampus, thalamus, and brainstem structures [129]. In agreement with this model, studies have demonstrated greater activation in fear network regions such as the striatum and the dACC [57, 130]. Heightened interoceptive sensitivity has also been widely documented in PD [131,132,133], while interoceptive conditioning is implicated in its etiology [134] and interoceptive exposure therapy is employed in its treatment [135]. Accordingly, in persons with PD, there are reports of heightened reactivity of insular cortex to emotional tasks [136, 137] as well as reduced numbers of insula benzodiazepine binding sites [138]. Although the exact function of the dACC in PD has yet to be determined, case studies reporting both immediate and delayed onset of panic attacks following surgical removal of the dACC in humans suggest it plays a key role in the disorder [139]. Unlike other anxiety disorders, there have been inconsistent findings regarding amygdala activation in PD patients, with studies suggesting both hypo- and hyperactivation of this structure [137, 140,141,142]. Despite the lack of evidence for amygdala hyperactivation, several structural MRI studies have found volumetric deficits in the amygdala of individuals with PD [141, 143,144,145]. Gorman et al.’s [129] model of PD also points to the role of the hippocampus in contextualizing fearful situations. Generally, phobic avoidance arises from people with PD associating their fearful state (a panic attack) with the situation or scenes that were present at the time of their panic. Even with successful treatment, patients may still avoid situations contextually similar to those in which they had a panic attack due to this conditioning. Since the hippocampus is necessary for contextualization, Gorman and colleagues suggested that the hippocampus may be a treatment target for deconditioning contextual fear learning. A review by Shin and Liberzon [3] has also implicated abnormal hippocampal activity within PD. While there is little evidence from fMRI research, structural MRI studies have found a decrease in hippocampal volumes and density of persons with panic disorder, suggesting decreased consolidation of extinction and generalization memories for these individuals [141, 144, 145].
Posttraumatic Stress Disorder (PTSD)
Although not a perfect model, fear- conditioning studies have also been used to study PTSD and its neurocircuitry (see [146]). In general, it appears that individuals with PTSD are better at fear learning (conditioning) and worse at learning extinction and later recalling these extinction memories due to abnormalities in their fear network [147, 148]. Imaging studies of PTSD tend to report hyperactivation in the amygdala both at rest [149, 150] and during task-based experiments [99, 151] (reviewed in [152]), which may lead to an exaggerated fear response. Individuals with PTSD demonstrate exacerbated activation of the amygdala and dACC as well as increased skin conductance response (SCR), suggesting increased processing of threatening stimuli [153, 154]. Furthermore, several imaging studies have reported hypoactivation of the mPFC, vmPFC, and rACC in individuals with PTSD, suggesting deficits in regulation of fear-processing structures, e.g., amygdala, insula, and dACC, as seen in GAD, SAD, and PD [155, 156] (reviewed in [3]). Additionally, the vmPFC and hippocampus are important for fear-conditioning generalization. Studies with healthy controls demonstrate activation in both regions when subjects were presented with stimuli that only resembled the conditioned stimulus and successfully generalized previous extinction learning [157]. Both increases and decreases in hippocampal activity have been correlated with PTSD severity (reviewed in [3] and [2]). While activation patterns are unclear, abnormal hippocampal function may play a role in the tendency of PTSD patients to generalize their fear response to situations and contexts that differ from the trauma. Convergent with this hypothesis, studies have shown decreased hippocampal and vmPFC volumes in patients with PTSD [158,159,160,161,162,163]. Some researchers even suggest that smaller hippocampal volume may be a precursor to PTSD development. In a twin study of combat-exposed individuals, the twin sibling of veterans with PTSD had smaller hippocampal volume than that of twins of veterans without PTSD, independent of trauma exposure [164] reviewed in [100]. Sleep deficiencies are also a potential precursor and target for PTSD. Objective and subjective sleep abnormalities, including subjective insomnia reports, either preceding or following traumatic experiences, predict later development of PTSD (reviewed in [165,166,167]). Such findings suggest that sleep disturbances may be a precursor to, in addition to a consequence of, PTSD development and may play a key role in the etiology of this disorder [165,166,167,168,169,170,171,172,173,174]
Conclusion
In summary, the pathophysiology of anxiety disorders is marked by abnormalities in emotion-processing structures, particularly the amygdala, BNST, rACC, and insula as well as in emotion-regulation structures such as the vmPFC, dACC, mPFC, and hippocampus. Although studies suggest that fear-driven disorders (e.g., SAD and specific phobia) have greater deficits in emotion-processing structures, while worry-driven disorders (e.g., GAD and PD) are categorized by deficits in emotion-regulation pathways, disturbances occur across all points of the threat interpretation, evaluation, and response loops which is more clearly defined in the neurocircuitry of PTSD. Further studies and greater homogeneity across study methodology are needed to advance greater understanding of these disorders and avoid potential misunderstandings in anatomical specificity. Studies exploring the effects of well-validated interventions for anxiety disorders may be of particular benefit in untangling the connection between behavior, cognition, and functional neuroimaging for the development of future treatment targets.
References
Etkin A, Wager TD. Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am J Psychiatry. 2007;164(10):1476–88.
Duval ER, Javanbakht A, Liberzon I. Neural circuits in anxiety and stress disorders: a focused review. Ther Clin Risk Manag. 2015;11:115–26. https://doi.org/10.2147/TCRM.S48528.
Shin LM, Liberzon I. The neurocircuitry of fear, stress, and anxiety disorders. Neuropsychopharmacology. 2010;35(1):169–91. https://doi.org/10.1038/npp.2009.83.
Rauch SL, Shin LM, Wright CI. Neuroimaging studies of amygdala function in anxiety disorders. Ann N Y Acad Sci. 2003;985(1):389–410.
Raichle ME. The restless brain. Brain Connect. 2011;1(1):3–12. https://doi.org/10.1089/brain.2011.0019.
Greicius MD, Supekar K, Menon V, Dougherty RF. Resting-state functional connectivity reflects structural connectivity in the default mode network. Cereb Cortex. 2009;19(1):72–8. https://doi.org/10.1093/cercor/bhn059.
Fox MD, Greicius M. Clinical applications of resting state functional connectivity. Front Syst Neurosci. 2010;4:19.
Milad MR, Quirk GJ. Fear extinction as a model for translational neuroscience: ten years of progress. Annu Rev Psychol. 2012;63:129–51. https://doi.org/10.1146/annurev.psych.121208.131631.
Lonsdorf TB, Menz MM, Andreatta M, Fullana MA, Golkar A, Haaker J, et al. Don’t fear ‘fear conditioning’: Methodological considerations for the design and analysis of studies on human fear acquisition, extinction, and return of fear. Neurosci Biobehav Rev. 2017;77:247–85. https://doi.org/10.1016/j.neubiorev.2017.02.026.
Lonsdorf TB, Merz CJ. More than just noise: Inter-individual differences in fear acquisition, extinction and return of fear in humans – Biological, experiential, temperamental factors, and methodological pitfalls. Neurosci Biobehav Rev. 2017;80:703–28. https://doi.org/10.1016/j.neubiorev.2017.07.007.
Quirk GJ, Mueller D. Neural mechanisms of extinction learning and retrieval. Neuropsychopharmacology. 2008;33(1):56–72.
Hermans D, Craske MG, Mineka S, Lovibond PF. Extinction in human fear conditioning. Biol Psychiatry. 2006;60(4):361–8.
Craske MG, Kircanski K, Zelikowsky M, Mystkowski J, Chowdhury N, Baker A. Optimizing inhibitory learning during exposure therapy. Behav Res Ther. 2008;46(1):5–27.
McNally RJ. Mechanisms of exposure therapy: how neuroscience can improve psychological treatments for anxiety disorders. Clin Psychol Rev. 2007;27(6):750–9.
Beckers T, Krypotos A-M, Boddez Y, Effting M, Kindt M. What’s wrong with fear conditioning? Biol Psychol. 2013;92(1):90–6.
Milad MR, Wright CI, Orr SP, Pitman RK, Quirk GJ, Rauch SL. Recall of fear extinction in humans activates the ventromedial prefrontal cortex and hippocampus in concert. Biol Psychiatry. 2007;62(5):446–54.
Quirk GJ, Garcia R, Gonzalez-Lima F. Prefrontal mechanisms in extinction of conditioned fear. Biol Psychiatry. 2006;60(4):337–43.
Marin JM, Agusti A, Villar I, Forner M, Nieto D, Carrizo SJ, et al. Association between treated and untreated obstructive sleep apnea and risk of hypertension. JAMA. 2012;307(20):2169–76. https://doi.org/10.1001/jama.2012.3418.
Duits P, Cath DC, Lissek S, Hox JJ, Hamm AO, Engelhard IM, et al. Updated meta-analysis of classical fear conditioning in the anxiety disorders. Depress Anxiety. 2015;32(4):239–53. https://doi.org/10.1002/da.22353.
Milad MR, Rauch SL. Obsessive-compulsive disorder: beyond segregated cortico-striatal pathways. Trends Cogn Sci. 2012;16(1):43–51. https://doi.org/10.1016/j.tics.2011.11.003.
Liberzon I, Martis B. Neuroimaging studies of emotional responses in PTSD. Ann N Y Acad Sci. 2006;1071:87–109. https://doi.org/10.1196/annals.1364.009.
Taylor JM, Whalen PJ. Neuroimaging and anxiety: The neural substrates of pathological and non-pathological anxiety. Curr Psychiatry Rep. 2015;17(6):49.
Abelson JL, Khan S, Liberzon I, Young EA. HPA axis activity in patients with panic disorder: review and synthesis of four studies. Depress Anxiety. 2007;24(1):66–76.
Knight DC, Nguyen HT, Bandettini PA. The role of the human amygdala in the production of conditioned fear responses. NeuroImage. 2005;26(4):1193–200.
Hariri AR, Holmes A. Genetics of emotional regulation: the role of the serotonin transporter in neural function. Trends Cogn Sci. 2006;10(4):182–91. https://doi.org/10.1016/j.tics.2006.02.011.
Hariri AR, Drabant EM, Munoz KE, Kolachana BS, Mattay VS, Egan MF, et al. A susceptibility gene for affective disorders and the response of the human amygdala. Arch Gen Psychiatry. 2005;62(2):146–52. https://doi.org/10.1001/archpsyc.62.2.146.
Furmark T, Tillfors M, Garpenstrand H, Marteinsdottir I, Langstrom B, Oreland L, et al. Serotonin transporter polymorphism related to amygdala excitability and symptom severity in patients with social phobia. Neurosci Lett. 2004;362(3):189–92.
Drabant EM, Ramel W, Edge MD, Hyde LW, Kuo JR, Goldin PR, et al. Neural mechanisms underlying 5-HTTLPR-related sensitivity to acute stress. Am J Psychiatry. 2012;169(4):397–405.
Spear LP. The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev. 2000;24(4):417–63.
Casey B, Jones RM, Somerville LH. Braking and Accelerating of the Adolescent Brain. J Res Adolesc. 2011;21(1):21–33. https://doi.org/10.1111/j.1532-7795.2010.00712.x.
Casey B, Ruberry EJ, Libby V, Glatt CE, Hare T, Soliman F, et al. Transitional and translational studies of risk for anxiety. Depress Anxiety. 2011;28(1):18–28.
Bishop SJ, Duncan J, Lawrence AD. State anxiety modulation of the amygdala response to unattended threat-related stimuli. J Neurosci. 2004;24(46):10364–8.
Davis M, Walker DL, Miles L, Grillon C. Phasic vs sustained fear in rats and humans: role of the extended amygdala in fear vs anxiety. Neuropsychopharmacology. 2010;35(1):105–35. https://doi.org/10.1038/npp.2009.109.
Walker DL, Ressler KJ, Lu KT, Davis M. Facilitation of conditioned fear extinction by systemic administration or intra-amygdala infusions of D-cycloserine as assessed with fear-potentiated startle in rats. J Neurosci. 2002;22(6):2343–51.
Lebow MA, Chen A. Overshadowed by the amygdala: the bed nucleus of the stria terminalis emerges as key to psychiatric disorders. Mol Psychiatry. 2016;21(4):450–63. https://doi.org/10.1038/mp.2016.1.
Walker DL, Toufexis DJ, Davis M. Role of the bed nucleus of the stria terminalis versus the amygdala in fear, stress, and anxiety. Eur J Pharmacol. 2003;463(1-3):199–216.
Kazama AM, Heuer E, Davis M, Bachevalier J. Effects of neonatal amygdala lesions on fear learning, conditioned inhibition, and extinction in adult macaques. Behav Neurosci. 2012;126(3):392–403. https://doi.org/10.1037/a0028241.
Poulos AM, Ponnusamy R, Dong HW, Fanselow MS. Compensation in the neural circuitry of fear conditioning awakens learning circuits in the bed nuclei of the stria terminalis. Proc Natl Acad Sci U S A. 2010;107(33):14881–6. https://doi.org/10.1073/pnas.1005754107.
Lockwood PL, Wittmann MK. Ventral anterior cingulate cortex and social decision-making. Neurosci Biobehav Rev. 2018;92:187–91. https://doi.org/10.1016/j.neubiorev.2018.05.030.
Devinsky O, Morrell MJ, Vogt BA. Contributions of anterior cingulate cortex to behaviour. Brain. 1995;118(Pt 1):279–306.
Bush G, Luu P, Posner MI. Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn Sci. 2000;4(6):215–22.
Marusak H, Thomason M, Peters C, Zundel C, Elrahal F, Rabinak C. You say ‘prefrontal cortex’ and I say ‘anterior cingulate’: meta-analysis of spatial overlap in amygdala-to-prefrontal connectivity and internalizing symptomology. Transl Psychiatry. 2016;6(11):e944.
Lieberman MD, Eisenberger NI. The dorsal anterior cingulate cortex is selective for pain: Results from large-scale reverse inference. Proc Natl Acad Sci U S A. 2015;112(49):15250–5. https://doi.org/10.1073/pnas.1515083112.
Cheng DT, Knight DC, Smith CN, Helmstetter FJ. Human amygdala activity during the expression of fear responses. Behav Neurosci. 2006;120(6):1187.
Cheng DT, Knight DC, Smith CN, Stein EA, Helmstetter FJ. Functional MRI of human amygdala activity during Pavlovian fear conditioning: stimulus processing versus response expression. Behav Neurosci. 2003;117(1):3.
Milad MR, Quirk GJ, Pitman RK, Orr SP, Fischl B, Rauch SL. A role for the human dorsal anterior cingulate cortex in fear expression. Biol Psychiatry. 2007;62(10):1191–4.
Chen T, Cai W, Ryali S, Supekar K, Menon V. Distinct global brain dynamics and spatiotemporal organization of the salience network. PLoS Biol. 2016;14(6):e1002469. https://doi.org/10.1371/journal.pbio.1002469.
Critchley HD. Electrodermal responses: what happens in the brain. Neuroscientist. 2002;8(2):132–42.
Whalen PJ, Bush G, McNally RJ, Wilhelm S, McInerney SC, Jenike MA, et al. The emotional counting Stroop paradigm: a functional magnetic resonance imaging probe of the anterior cingulate affective division. Biol Psychiatry. 1998;44(12):1219–28.
Phillips ML, Ladouceur CD, Drevets WC. A neural model of voluntary and automatic emotion regulation: Implications for understanding the pathophysiology and neurodevelopment of bipolar disorder. Mol Psychiatry. 2008;13:833–57.
Etkin A, Egner T, Peraza DM, Kandel ER, Hirsch J. Resolving emotional conflict: a role for the rostral anterior cingulate cortex in modulating activity in the amygdala. Neuron. 2006;51(6):871–82. https://doi.org/10.1016/j.neuron.2006.07.029.
Dodhia S, Hosanagar A, Fitzgerald DA, Labuschagne I, Wood AG, Nathan PJ, et al. Modulation of resting-state amygdala-frontal functional connectivity by oxytocin in generalized social anxiety disorder. Neuropsychopharmacology. 2014;39(9):2061–9. https://doi.org/10.1038/npp.2014.53.
Pizzagalli DA. Frontocingulate dysfunction in depression: toward biomarkers of treatment response. Neuropsychopharmacology. 2011;36(1):183–206. https://doi.org/10.1038/npp.2010.166.
Ongur D, Price JL. The organization of networks within the orbital and medial prefrontal cortex of rats, monkeys and humans. Cereb Cortex. 2000;10(3):206–19.
Drevets WC, Savitz J, Trimble M. The subgenual anterior cingulate cortex in mood disorders. CNS Spectr. 2008;13(8):663–81.
Johansen-Berg H, Gutman DA, Behrens TE, Matthews PM, Rushworth MF, Katz E, et al. Anatomical connectivity of the subgenual cingulate region targeted with deep brain stimulation for treatment-resistant depression. Cereb Cortex. 2008;18(6):1374–83.
Tuescher O, Protopopescu X, Pan H, Cloitre M, Butler T, Goldstein M, et al. Differential activity of subgenual cingulate and brainstem in panic disorder and PTSD. J Anxiety Disord. 2011;25(2):251–7. https://doi.org/10.1016/j.janxdis.2010.09.010.
Haas BW, Omura K, Constable RT, Canli T. Emotional conflict and neuroticism: personality-dependent activation in the amygdala and subgenual anterior cingulate. Behav Neurosci. 2007;121(2):249–56. https://doi.org/10.1037/0735-7044.121.2.249.
Phelps EA, Delgado MR, Nearing KI, LeDoux JE. Extinction learning in humans: role of the amygdala and vmPFC. Neuron. 2004;43(6):897–905.
Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C, et al. Deep brain stimulation for treatment-resistant depression. Neuron. 2005;45(5):651–60.
Mayberg HS, Brannan SK, Tekell JL, Silva JA, Mahurin RK, McGinnis S, et al. Regional metabolic effects of fluoxetine in major depression: serial changes and relationship to clinical response. Biol Psychiatry. 2000;48(8):830–43.
Drevets WC, Bogers W, Raichle ME. Functional anatomical correlates of antidepressant drug treatment assessed using PET measures of regional glucose metabolism. Eur Neuropsychopharmacol. 2002;12(6):527–44.
Myers-Schulz B, Koenigs M. Functional anatomy of ventromedial prefrontal cortex: implications for mood and anxiety disorders. Mol Psychiatry. 2012;17(2):132–41. https://doi.org/10.1038/mp.2011.88.
Etkin A, Egner T, Kalisch R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cogn Sci. 2011;15(2):85–93. https://doi.org/10.1016/j.tics.2010.11.004.
Craig AD. How do you feel? interoception: the sense of the physiological condition of the body. Nat Rev. 2002;3(8):655–66.
Craig AD. How do you feel – now? The anterior insula and human awareness. Nature reviews. 2009;10(1):59–70.
Craig AD. Significance of the insula for the evolution of human awareness of feelings from the body. Ann N Y Acad Sci. 2011;1225:72–82. https://doi.org/10.1111/j.1749-6632.2011.05990.x.
Namkung H, Kim SH, Sawa A. The insula: an underestimated brain area in clinical neuroscience, psychiatry, and neurology. Trends Neurosci. 2017;40(4):200–7. https://doi.org/10.1016/j.tins.2017.02.002.
Khalsa SS, Adolphs R, Cameron OG, Critchley HD, Davenport PW, Feinstein JS, et al. Interoception and mental health: a roadmap. Biol Psychiatry. 2018; https://doi.org/10.1016/j.bpsc.2017.12.004.
Murphy J, Brewer R, Catmur C, Bird G. Interoception and psychopathology: a developmental neuroscience perspective. Dev Cogn Neurosci. 2017;23:45–56. https://doi.org/10.1016/j.dcn.2016.12.006.
Seth AK, Friston KJ. Active interoceptive inference and the emotional brain. Philos Trans R Soc Lond Ser B Biol Sci. 2016;371(1708) https://doi.org/10.1098/rstb.2016.0007.
Bernhardt BC, Singer T. The neural basis of empathy. Annu Rev Neurosci. 2012;35:1–23. https://doi.org/10.1146/annurev-neuro-062111-150536.
Zaki J, Wager TD, Singer T, Keysers C, Gazzola V. The anatomy of suffering: understanding the relationship between nociceptive and empathic pain. Trends Cogn Sci. 2016;20(4):249–59. https://doi.org/10.1016/j.tics.2016.02.003.
Craig AD. How do you feel? an interoceptive moment with your neurobiological self. Princeton: Princeton University Press; 2016.
Sarinopoulos I, Grupe D, Mackiewicz K, Herrington J, Lor M, Steege E, et al. Uncertainty during anticipation modulates neural responses to aversion in human insula and amygdala. Cereb Cortex. 2009;20(4):929–40.
Chua P, Krams M, Toni I, Passingham R, Dolan R. A functional anatomy of anticipatory anxiety. NeuroImage. 1999;9(6 Pt 1):563–71. https://doi.org/10.1006/nimg.1999.0407.
Ploghaus A, Tracey I, Gati JS, Clare S, Menon RS, Matthews PM, et al. Dissociating pain from its anticipation in the human brain. Science. 1999;284(5422):1979–81.
Simmons A, Matthews SC, Stein MB, Paulus MP. Anticipation of emotionally aversive visual stimuli activates right insula. Neuroreport. 2004;15(14):2261–5.
Simmons A, Strigo I, Matthews SC, Paulus MP, Stein MB. Anticipation of aversive visual stimuli is associated with increased insula activation in anxiety-prone subjects. Biol Psychiatry. 2006;60(4):402–9. https://doi.org/10.1016/j.biopsych.2006.04.038.
Paulus MP. The role of neuroimaging for the diagnosis and treatment of anxiety disorders. Depress Anxiety. 2008;25(4):348–56.
Klumpp H, Angstadt M, Phan KL. Insula reactivity and connectivity to anterior cingulate cortex when processing threat in generalized social anxiety disorder. Biol Psychol. 2012;89(1):273–6. https://doi.org/10.1016/j.biopsycho.2011.10.010.
Ji J, Maren S. Hippocampal involvement in contextual modulation of fear extinction. Hippocampus. 2007;17(9):749–58.
Martin EI, Ressler KJ, Binder E, Nemeroff CBJPC. The neurobiology of anxiety disorders: brain imaging, genetics, and psychoneuroendocrinology. Psychiatr Clin. 2009;32(3):549–75.
Bannerman D, Rawlins J, McHugh S, Deacon R, Yee B, Bast T, et al. Regional dissociations within the hippocampus – memory and anxiety. Neurosci Biobehav Rev. 2004;28(3):273–83.
Richmond M, Yee B, Pouzet B, Veenman L, Rawlins J, Feldon J, et al. Dissociating context and space within the hippocampus: effects of complete, dorsal, and ventral excitotoxic hippocampal lesions on conditioned freezing and spatial learning. Behav Neurosci. 1999;113(6):1189.
Kjelstrup KG, Tuvnes FA, Steffenach H-A, Murison R, Moser EI, Moser M-B. Reduced fear expression after lesions of the ventral hippocampus. Proc Natl Acad Sci. 2002;99(16):10825–30.
Aron AR, Robbins TW, Poldrack RA. Inhibition and the right inferior frontal cortex. Trends Cogn Sci. 2004;8(4):170–7.
Aron AR, Robbins TW, Poldrack RA. Inhibition and the right inferior frontal cortex: one decade on. Trends Cogn Sci. 2014;18(4):177–85. https://doi.org/10.1016/j.tics.2013.12.003.
Iversen SD, Mishkin M. Perseverative interference in monkeys following selective lesions of the inferior prefrontal convexity. Exp Brain Res. 1970;11(4):376–86.
Aron AR, Robbins TW, Poldrack RA. Right inferior frontal cortex: addressing the rebuttals. Front Hum Neurosci. 2014;8:905. https://doi.org/10.3389/fnhum.2014.00905.
Dillon DG, Pizzagalli DA. Inhibition of Action, Thought, and Emotion: A Selective Neurobiological Review. Appl Prev Psychol. 2007;12(3):99–114.
van Rooij SJ, Rademaker AR, Kennis M, Vink M, Kahn RS, Geuze E. Impaired right inferior frontal gyrus response to contextual cues in male veterans with PTSD during response inhibition. J Psychiatry Neurosci. 2014;39(5):330–8.
Falconer E, Bryant R, Felmingham KL, Kemp AH, Gordon E, Peduto A, et al. The neural networks of inhibitory control in posttraumatic stress disorder. J Psychiatry Neurosci. 2008;33(5):413–22.
Delgado MR, Nearing KI, Ledoux JE, Phelps EA. Neural circuitry underlying the regulation of conditioned fear and its relation to extinction. Neuron. 2008;59(5):829–38.
Milad MR, Rauch SL. The role of the orbitofrontal cortex in anxiety disorders. Ann N Y Acad Sci. 2007;1121(1):546–61.
Milad MR, Rauch SL, Pitman RK, Quirk GJ. Fear extinction in rats: implications for human brain imaging and anxiety disorders. Biol Psychol. 2006;73(1):61–71.
Jovanovic T, Ressler KJ. How the neurocircuitry and genetics of fear inhibition may inform our understanding of PTSD. Am J Psychiatry. 2010;167(6):648–62. https://doi.org/10.1176/appi.ajp.2009.09071074.
Rauch SL, Shin LM, Phelps EA. Neurocircuitry models of posttraumatic stress disorder and extinction: human neuroimaging research – past, present, and future. Biol Psychiatry. 2006;60(4):376–82.
Milad MR, Pitman RK, Ellis CB, Gold AL, Shin LM, Lasko NB, et al. Neurobiological basis of failure to recall extinction memory in posttraumatic stress disorder. Biol Psychiatry. 2009;66(12):1075–82. https://doi.org/10.1016/j.biopsych.2009.06.026.
Pitman RK, Rasmusson AM, Koenen KC, Shin LM, Orr SP, Gilbertson MW, et al. Biological studies of post-traumatic stress disorder. Nature reviews. 2012;13(11):769–87. https://doi.org/10.1038/nrn3339.
Koenigs M, Huey ED, Calamia M, Raymont V, Tranel D, Grafman J. Distinct regions of prefrontal cortex mediate resistance and vulnerability to depression. J Neurosci. 2008;28(47):12341–8.
Calhoon GG, Tye KM. Resolving the neural circuits of anxiety. Nat Neurosci. 2015;18(10):1394.
McDonald AJ. Cortical pathways to the mammalian amygdala. Prog Neurobiol. 1998;55(3):257–332.
LeDoux JE. Emotion circuits in the brain. Annu Rev Neurosci. 2000;23:155–84. https://doi.org/10.1146/annurev.neuro.23.1.155.
Lipka J, Miltner WH, Straube T. Vigilance for threat interacts with amygdala responses to subliminal threat cues in specific phobia. Biol Psychiatry. 2011;70(5):472–8. https://doi.org/10.1016/j.biopsych.2011.04.005.
Killgore WD, Britton JC, Schwab ZJ, Price LM, Weiner MR, Gold AL, et al. Cortico-limbic responses to masked affective faces across PTSD, panic disorder, and specific phobia. Depress Anxiety. 2014;31(2):150–9.
Hilbert K, Pine DS, Muehlhan M, Lueken U, Steudte-Schmiedgen S, Beesdo-Baum K. Gray and white matter volume abnormalities in generalized anxiety disorder by categorical and dimensional characterization. Psychiatry Res. 2015;234(3):314–20. https://doi.org/10.1016/j.pscychresns.2015.10.009.
Seligman MEP. Phobias and preparedness. Behav Ther. 1971;2:307–20.
Ohman A, Mineka S. Fears, phobias, and preparedness: toward an evolved module of fear and fear learning. Psychol Rev. 2001;108(3):483–522.
APA. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington: American Psychiatric Publishing; 2013.
Hattingh CJ, Ipser J, Tromp S, Syal S, Lochner C, SJB B, et al. Functional magnetic resonance imaging during emotion recognition in social anxiety disorder: an activation likelihood meta-analysis. Front Hum Neurosci. 2013;6:347.
Frick A, Howner K, Fischer H, Kristiansson M, Furmark T. Altered fusiform connectivity during processing of fearful faces in social anxiety disorder. Transl Psychiatry. 2013;3:e312. https://doi.org/10.1038/tp.2013.85.
Kanwisher N, McDermott J, Chun MM. The fusiform face area: a module in human extrastriate cortex specialized for face perception. J Neurosci. 1997;17(11):4302–11.
Tillfors M, Furmark T, Marteinsdottir I, Fischer H, Pissiota A, Langstrom B, et al. Cerebral blood flow in subjects with social phobia during stressful speaking tasks: a PET study. Am J Psychiatry. 2001;158(8):1220–6.
Lorberbaum JP, Kose S, Johnson MR, Arana GW, Sullivan LK, Hamner MB, et al. Neural correlates of speech anticipatory anxiety in generalized social phobia. Neuroreport. 2004;15(18):2701–5.
Danti S, Ricciardi E, Gentili C, Gobbini MI, Pietrini P, Guazzelli M. Is social phobia a “mis-communication” disorder? brain functional connectivity during face perception differs between patients with social phobia and healthy control subjects. Front Syst Neurosci. 2010;4:152. https://doi.org/10.3389/fnsys.2010.00152.
Klumpp H, Fitzgerald JM. Neuroimaging predictors and mechanisms of treatment response in social anxiety disorder: an overview of the Amygdala. Curr Psychiatry Rep. 2018;20(10):89. https://doi.org/10.1007/s11920-018-0948-1.
Young KS, Burklund LJ, Torre JB, Saxbe D, Lieberman MD, Craske MG. Treatment for social anxiety disorder alters functional connectivity in emotion regulation neural circuitry. Psychiatry Res Neuroimaging. 2017;261:44–51. https://doi.org/10.1016/j.pscychresns.2017.01.005.
Bandelow B, Michaelis S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin Neurosci. 2015;17(3):327–35.
Ruscio AM, Brown TA, Chiu WT, Sareen J, Stein MB, Kessler RC. Social fears and social phobia in the USA: results from the National Comorbidity Survey Replication. Psychol Med. 2008;38(1):15–28. https://doi.org/10.1017/S0033291707001699.
Mochcovitch MD, da Rocha Freire RC, Garcia RF, Nardi AE. A systematic review of fMRI studies in generalized anxiety disorder: evaluating its neural and cognitive basis. J Affect Disord. 2014;167:336–42. https://doi.org/10.1016/j.jad.2014.06.041.
Liu WJ, Yin DZ, Cheng WH, Fan MX, You MN, Men WW, et al. Abnormal functional connectivity of the amygdala-based network in resting-state FMRI in adolescents with generalized anxiety disorder. Med Sci Monit. 2015;21:459–67. https://doi.org/10.12659/MSM.893373.
Lissek S. Toward an account of clinical anxiety predicated on basic, neurally mapped mechanisms of Pavlovian fear-learning: the case for conditioned overgeneralization. Depress Anxiety. 2012;29(4):257–63. https://doi.org/10.1002/da.21922.
Greenberg T, Carlson JM, Cha J, Hajcak G, Mujica-Parodi LR. Neural reactivity tracks fear generalization gradients. Biol Psychol. 2013;92(1):2–8. https://doi.org/10.1016/j.biopsycho.2011.12.007.
Yassa MA, Hazlett RL, Stark CE, Hoehn-Saric R. Functional MRI of the amygdala and bed nucleus of the stria terminalis during conditions of uncertainty in generalized anxiety disorder. J Psychiatr Res. 2012;46(8):1045–52. https://doi.org/10.1016/j.jpsychires.2012.04.013.
Roy AK, Fudge JL, Kelly C, Perry JS, Daniele T, Carlisi C, et al. Intrinsic functional connectivity of amygdala-based networks in adolescent generalized anxiety disorder. J Am Acad Child Adolesc Psychiatry. 2013;52(3):290–9. e2. https://doi.org/10.1016/j.jaac.2012.12.010.
Etkin A, Prater KE, Schatzberg AF, Menon V, Greicius MD. Disrupted amygdalar subregion functional connectivity and evidence of a compensatory network in generalized anxiety disorder. Arch Gen Psychiatry. 2009;66(12):1361–72. https://doi.org/10.1001/archgenpsychiatry.2009.104.
Brooks SJ, Stein DJ. A systematic review of the neural bases of psychotherapy for anxiety and related disorders. Dialogues Clin Neurosci. 2015;17(3):261–79.
Gorman JM, Kent JM, Sullivan GM, Coplan JD. Neuroanatomical hypothesis of panic disorder, revised. Am J Psychiatry. 2000;157(4):493–505. https://doi.org/10.1176/appi.ajp.157.4.493.
de Carvalho MR, Dias GP, Cosci F, de-Melo-Neto VL, Bevilaqua MC, Gardino PF, et al. Current findings of fMRI in panic disorder: contributions for the fear neurocircuitry and CBT effects. Expert Rev Neurother. 2010;10(2):291–303. https://doi.org/10.1586/ern.09.161.
Yoris A, Esteves S, Couto B, Melloni M, Kichic R, Cetkovich M, et al. The roles of interoceptive sensitivity and metacognitive interoception in panic. Behav Brain Funct. 2015;11:14. https://doi.org/10.1186/s12993-015-0058-8.
Limmer J, Kornhuber J, Martin A. Panic and comorbid depression and their associations with stress reactivity, interoceptive awareness and interoceptive accuracy of various bioparameters. J Affect Disord. 2015;185:170–9. https://doi.org/10.1016/j.jad.2015.07.010.
Domschke K, Stevens S, Pfleiderer B, Gerlach AL. Interoceptive sensitivity in anxiety and anxiety disorders: an overview and integration of neurobiological findings. Clin Psychol Rev. 2010;30(1):1–11. https://doi.org/10.1016/j.cpr.2009.08.008.
De Cort K, Schroijen M, Hurlemann R, Claassen S, Hoogenhout J, Van den Bergh O, et al. Modeling the development of panic disorder with interoceptive conditioning. Eur Neuropsychopharmacol. 2017;27(1):59–69. https://doi.org/10.1016/j.euroneuro.2016.11.001.
Boettcher H, Brake CA, Barlow DH. Origins and outlook of interoceptive exposure. J Behav Ther Exp Psychiatry. 2016;53:41–51. https://doi.org/10.1016/j.jbtep.2015.10.009.
Gorka SM, Nelson BD, Phan KL, Shankman SA. Insula response to unpredictable and predictable aversiveness in individuals with panic disorder and comorbid depression. Biology of mood & anxiety disorders. 2014;4:9. https://doi.org/10.1186/2045-5380-4-9.
Sobanski T, Wagner G. Functional neuroanatomy in panic disorder: Status quo of the research. World J Psychiatry. 2017;7(1):12–33. https://doi.org/10.5498/wjp.v7.i1.12.
Cameron OG, Huang GC, Nichols T, Koeppe RA, Minoshima S, Rose D, et al. Reduced gamma-aminobutyric acid(A)-benzodiazepine binding sites in insular cortex of individuals with panic disorder. Arch Gen Psychiatry. 2007;64(7):793–800. https://doi.org/10.1001/archpsyc.64.7.793.
Shinoura N, Yamada R, Tabei Y, Otani R, Itoi C, Saito S, et al. Damage to the right dorsal anterior cingulate cortex induces panic disorder. J Affect Disord. 2011;133(3):569–72. https://doi.org/10.1016/j.jad.2011.04.029.
Dresler T, Guhn A, Tupak SV, Ehlis AC, Herrmann MJ, Fallgatter AJ, et al. Revise the revised? New dimensions of the neuroanatomical hypothesis of panic disorder. J Neural Transm (Vienna). 2013;120(1):3–29. https://doi.org/10.1007/s00702-012-0811-1.
Kim JE, Dager SR, Lyoo IK. The role of the amygdala in the pathophysiology of panic disorder: evidence from neuroimaging studies. Biology of mood & anxiety disorders. 2012;2:20. https://doi.org/10.1186/2045-5380-2-20.
Ottaviani C, Cevolani D, Nucifora V, Borlimi R, Agati R, Leonardi M, et al. Amygdala responses to masked and low spatial frequency fearful faces: a preliminary fMRI study in panic disorder. Psychiatry Res. 2012;203(2-3):159–65. https://doi.org/10.1016/j.pscychresns.2011.12.010.
Massana G, Serra-Grabulosa JM, Salgado-Pineda P, Gasto C, Junque C, Massana J, et al. Amygdalar atrophy in panic disorder patients detected by volumetric magnetic resonance imaging. NeuroImage. 2003;19(1):80–90.
Del Casale A, Serata D, Rapinesi C, Kotzalidis GD, Angeletti G, Tatarelli R, et al. Structural neuroimaging in patients with panic disorder: findings and limitations of recent studies. Psychiatr Danub. 2013;25(2):108–14.
Pannekoek JN, van der Werff SJ, Stein DJ, van der Wee NJ. Advances in the neuroimaging of panic disorder. Hum Psychopharmacol. 2013;28(6):608–11. https://doi.org/10.1002/hup.2349.
VanElzakker MB, Dahlgren MK, Davis FC, Dubois S, Shin LM. From Pavlov to PTSD: the extinction of conditioned fear in rodents, humans, and anxiety disorders. Neurobiol Learn Mem. 2014;113:3–18. https://doi.org/10.1016/j.nlm.2013.11.014.
VanElzakker MB. Posttraumatic Stress Disorder. In: Neuroscience in the 21st Century: From Basic to Clinical; 2016. p. 4055–84.
Garfinkel SN, Abelson JL, King AP, Sripada RK, Wang X, Gaines LM, et al. Impaired contextual modulation of memories in PTSD: an fMRI and psychophysiological study of extinction retention and fear renewal. J Neurosci. 2014;34(40):13435–43. https://doi.org/10.1523/JNEUROSCI.4287-13.2014.
Chung YA, Kim SH, Chung SK, Chae J-H, Yang DW, Sohn HS, et al. Alterations in cerebral perfusion in posttraumatic stress disorder patients without re-exposure to accident-related stimuli. Clin Neurophysiol. 2006;117(3):637–42.
Semple WE, Goyer PF, McCormick R, Donovan B, Muzic RF Jr, Rugle L, et al. Higher brain blood flow at amygdala and lower frontal cortex blood flow in PTSD patients with comorbid cocaine and alcohol abuse compared with normals. Psychiatry. 2000;63(1):65–74.
Bryant RA, Kemp AH, Felmingham KL, Liddell B, Olivieri G, Peduto A, et al. Enhanced amygdala and medial prefrontal activation during nonconscious processing of fear in posttraumatic stress disorder: an fMRI study. Hum Brain Mapp. 2008;29(5):517–23. https://doi.org/10.1002/hbm.20415.
Shvil E, Rusch HL, Sullivan GM, Neria Y. Neural, psychophysiological, and behavioral markers of fear processing in PTSD: a review of the literature. Curr Psychiatry Rep. 2013;15(5):358.
Bremner JD, Vermetten E, Schmahl C, Vaccarino V, Vythilingam M, Afzal N, et al. Positron emission tomographic imaging of neural correlates of a fear acquisition and extinction paradigm in women with childhood sexual-abuse-related post-traumatic stress disorder. Psychol Med. 2005;35(6):791–806.
Linnman C, Zeffiro TA, Pitman RK, Milad MR. An fMRI study of unconditioned responses in post-traumatic stress disorder. Biol Mood Anxiety Disord. 2011;1(1):8.
Rougemont-Bucking A, Linnman C, Zeffiro TA, Zeidan MA, Lebron-Milad K, Rodriguez-Romaguera J, et al. Altered processing of contextual information during fear extinction in PTSD: an fMRI study. CNS Neurosci Ther. 2011;17(4):227–36. https://doi.org/10.1111/j.1755-5949.2010.00152.x.
Gold AL, Shin LM, Orr S, Carson M, Rauch S, Macklin M, et al. Decreased regional cerebral blood flow in medial prefrontal cortex during trauma-unrelated stressful imagery in Vietnam veterans with post-traumatic stress disorder. Psychol Med. 2011;41(12):2563–72.
Lissek S, Bradford DE, Alvarez RP, Burton P, Espensen-Sturges T, Reynolds RC, et al. Neural substrates of classically conditioned fear-generalization in humans: a parametric fMRI study. Soc Cogn Affect Neurosci. 2013;9(8):1134–42.
Bremner JD, Randall P, Scott TM, Bronen RA, Seibyl JP, Southwick SM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry. 1995;152(7):973.
Bremner JD, Randall P, Vermetten E, Staib L, Bronen RA, Mazure C, et al. Magnetic resonance imaging-based measurement of hippocampal volume in posttraumatic stress disorder related to childhood physical and sexual abuse – a preliminary report. Biol Psychiatry. 1997;41(1):23–32.
Bremner JD, Vythilingam M, Vermetten E, Southwick SM, McGlashan T, Nazeer A, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry. 2003;160(5):924–32.
Kitayama N, Vaccarino V, Kutner M, Weiss P, Bremner JD. Magnetic resonance imaging (MRI) measurement of hippocampal volume in posttraumatic stress disorder: a meta-analysis. J Affect Disord. 2005;88(1):79–86.
Kühn S, Gallinat J. Gray matter correlates of posttraumatic stress disorder: a quantitative meta-analysis. Biol Psychiatry. 2013;73(1):70–4.
Woon FL, Sood S, Hedges DW. Hippocampal volume deficits associated with exposure to psychological trauma and posttraumatic stress disorder in adults: a meta-analysis. Prog Neuro-Psychopharmacol Biol Psychiatry. 2010;34(7):1181–8.
Gilbertson MW, Shenton ME, Ciszewski A, Kasai K, Lasko NB, Orr SP, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci. 2002;5(11):1242–7. https://doi.org/10.1038/nn958.
Babson KA, Feldner MT. Temporal relations between sleep problems and both traumatic event exposure and PTSD: a critical review of the empirical literature. J Anxiety Disord. 2010;24(1):1–15. https://doi.org/10.1016/j.janxdis.2009.08.002.
Wright KM, Britt TW, Bliese PD, Adler AB, Picchioni D, Moore D. Insomnia as predictor versus outcome of PTSD and depression among Iraq combat veterans. J Clin Psychol. 2011;67(12):1240–58. https://doi.org/10.1002/jclp.20845.
Pace-Schott EF, Germain A, Milad MR. Sleep and REM sleep disturbance in the pathophysiology of PTSD: the role of extinction memory. Biol Mood Anxiety Disord. 2015;5:3. https://doi.org/10.1186/s13587-015-0018-9.
Germain A, Buysse DJ, Nofzinger E. Sleep-specific mechanisms underlying posttraumatic stress disorder: integrative review and neurobiological hypotheses. Sleep Med Rev. 2008;12(3):185–95.
Mellman TA. Sleep and post-traumatic stress disorder: a roadmap for clinicians and researchers. Sleep Med Rev. 2008;12(3):165–7.
Spoormaker VI, Montgomery P. Disturbed sleep in post-traumatic stress disorder: secondary symptom or core feature? Sleep Med Rev. 2008;12(3):169–84.
Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. 2013;36(7):1059–68. https://doi.org/10.5665/sleep.2810.
Babson KA, Badour CL, Feldner MT, Bunaciu L. The relationship of sleep quality and PTSD to anxious reactivity from idiographic traumatic event script-driven imagery. J Trauma Stress. 2012;25(5):503–10. https://doi.org/10.1002/jts.21739.
Babson KA, Blonigen DM, Boden MT, Drescher KD, Bonn-Miller MO. Sleep quality among U.S. military veterans with PTSD: a factor analysis and structural model of symptoms. J Trauma Stress. 2012;25(6):665–74. https://doi.org/10.1002/jts.21757.
Germain A. Sleep disturbances as the hallmark of PTSD: where are we now? Am J Psychiatry. 2013;170(4):372–82. https://doi.org/10.1176/appi.ajp.2012.12040432.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Daffre, C., Oliver, K.I., Pace-Schott, E.F. (2020). Neurocircuitry of Anxiety Disorders. In: Bui, E., Charney, M., Baker, A. (eds) Clinical Handbook of Anxiety Disorders. Current Clinical Psychiatry. Humana, Cham. https://doi.org/10.1007/978-3-030-30687-8_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-30687-8_2
Published:
Publisher Name: Humana, Cham
Print ISBN: 978-3-030-30686-1
Online ISBN: 978-3-030-30687-8
eBook Packages: MedicineMedicine (R0)