
Abstract
The last decade has witnessed a tremendous increase in rigorous intervention research in autism, particularly studies evaluating parent-mediated interventions. In 2011 and 2014, the Agency for Healthcare Research and Quality (AHRQ) published a pair of systematic literature reviews of studies evaluating the efficacy/effectiveness of behavioral interventions, including parent-mediated approaches. However, these reviews have not adequately incorporated articles published in 2013 and thereafter. Using the same methods and criteria to identify published articles providing adequate evidence as the original AHRQ reports, the current literature review update identified twenty additional studies, published between 2013 and 2015. All studies used controlled group designs to evaluate parent-mediated interventions for young children with autism. The current chapter reviews the results of these 20 studies and discusses whether the available evidence (defined broadly in terms of quality, quantity, and consistency) is sufficient to confidently determine that parent-mediated intervention approaches are effective for increasing children’s language/communication and cognitive abilities, reducing autism symptoms, and supporting the parents’ use of development-enhancing parenting practices.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
The last decade has witnessed a tremendous increase in rigorous intervention research in autism, particularly studies evaluating parent-mediated interventions. Efforts to systematically review this rapidly growing evidence base have been published by the Agency for Healthcare Research and Quality (Warren et al., 2011; Weitlauf et al., 2014), the Cochrane Database of Systematic Reviews (Oono, Honey, & McConachie, 2013), the National Standards Project (National Autism Center, 2015), the National Professional Development Center (Wong et al., 2013), as well as various academic journals (Beaudoin, Sébire, & Couture, 2014; Zwaigenbaum et al., 2015). Systematic literature reviews differ from each other in their methodology (e.g., study selection criteria related to children’s ages and characteristics of the research design) and the nature of the interventions being evaluated (e.g., parent-mediated approaches, behavioral intervention approaches). Further, one important limitation of any systematic effort to evaluate a highly active field of investigation is that new evidence emerges rapidly, and key conclusions can age rather quickly. In fact, the publication deadlines for studies to be included in the above-cited reviews ranged between June 2010 and December 2013. Given delayed indexing in bibliographic databases, available literature reviews have not adequately incorporated articles published in 2013 and thereafter.
The current chapter reports the results of a systematic review of intervention research published between 2012 and 2015. While the methodology of this literature review and key conclusions about the efficacy of parent-mediated interventions are summarized in this chapter, detailed methods and results are available upon request from the first author (M.S.).
Agency for Healthcare Research and Quality (AHRQ) Review of Behavioral Interventions for Children with Autism Spectrum Disorder
In 2011 and 2014, AHRQ published a pair of systematic literature reviews of studies evaluating the efficacy/effectiveness of behavioral interventions for children with autism spectrum disorder (ASD; Warren et al., 2011; Weitlauf et al., 2014). These literature reviews distinguished three kinds of behavioral intervention approaches : (1) ABA-Based Early Intensive Behavioral and Developmental Approaches, (2) Behavioral and Developmental Early Intervention-Parent Training, and (3) Play-/Interaction-Focused Intervention Approaches (Table 1.1). These three intervention approaches can be represented along two orthogonal dimensions:
-
1.
Whether the intervention is primarily implemented by a clinician or the child’s parent (i.e., clinician-mediated vs. parent-mediated)
-
2.
Whether the intervention is implemented during many hours per week, targeting multiple outcome domains, as compared to interventions that are implemented with relatively low intensity, focusing on a smaller number of outcomes (i.e., comprehensive vs. focused).
A graphical representation of these two dimensions, and how they relate to the three AHRQ categories of behavioral interventions, is presented in Fig. 1.1.

Graphical representation of two intervention dimensions (i.e., clinician-mediated vs. parent-mediated, and focused vs. comprehensive) and how they relate to the three categories of behavioral interventions included in the 2014 Report of the Agency for Healthcare Research and Quality (AHRQ)
Parent involvement, education, training, or coaching (i.e., parent-mediated interventions) plays an important role across all three kinds of behavioral intervention approaches. Although ABA-Based Early Intensive Behavioral and Developmental Approaches involve many hours of clinician-delivered intervention, parent involvement is considered to be a crucial component of most comprehensive intervention programs for young children with ASD. Examples include the UCLA/Lovaas Model (Lovaas, 1987), the Learning Experiences and Alternative Program (LEAP; Boyd et al., 2014), and the Early Start Denver Model (ESDM; Dawson et al., 2010). Similarly, many of the Play-/Interaction-Focused Intervention Approaches such as the Joint Attention Symbolic Play Emotion Regulation (JASPER; Kasari, Lawton et al., 2014) program, Focused Playtime Intervention (Siller, Hutman, & Sigman, 2013), or Reciprocal Imitation Training (Ingersoll & Gergans, 2007) have been implemented by training, educating, or coaching parents.
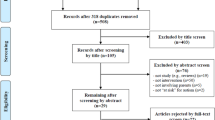
The methodology used to complete the AHRQ literature reviews (Warren et al., 2011; Weitlauf et al., 2014) involved three phases: (1) identification of published studies providing adequate evidence, (2) Study Quality Assessment, and (3) determination of Strength of Evidence grades. The first phase consisted of a sequence of bibliographic database searches, abstract review, and full-text review and identified 45 and 67 behavioral intervention studies for the 2011 and 2014 literature reviews, respectively. Criteria used to determine whether an article provided adequate evidence about the efficacy/effectiveness of an intervention approach included (a) participants ages 2–12 diagnosed with ASD or 0–2 at risk for ASD diagnosis, (b) at least 10 individuals with ASD (or at risk) in the target age range, and (c) the study used a controlled group design (e.g., randomized controlled trial, prospective and retrospective cohort study, and nonrandomized controlled trial). The latter criterion is particularly noteworthy, since studies using single-subject research designs did not meet the threshold for providing “adequate evidence” for this literature review.
Once studies providing adequate evidence about the efficacy/effectiveness of a behavioral intervention approach were identified, study quality was assessed by evaluating each studies’ methodological rigor. This assessment considered various study characteristics including the study design, diagnostic approach, participant ascertainment, intervention delivery, outcome measurement, and analysis approach. While the Study Quality Assessment was completed separately for each study, the Strength of Evidence grades were determined based on a qualitative synthesis of the entire body of research. Thus, Strength of Evidence was determined with regard to important, global questions. For example: Are Behavioral and Developmental Early Intervention-Parent Training approaches effective for increasing language/communication outcomes? How confident are we that these effects will be stable in light of future research? “Strength of evidence describes the adequacy of the current research, both in terms of quantity and quality, as well as the degree to which the entire body of current research provides a consistent and precise estimate of effect” (p.15, Weitlauf et al., 2014). For each global review question, four Strength of Evidence grades were assigned (Table 1.2).
A summary of the global questions evaluated, as well as the Strength of Evidence grades assigned in the 2014 AHRQ report, is provided in Table 1.3. For most of the evaluated global questions, the Strength of Evidence was graded as “low,” indicating “low confidence that the evidence reflects the true effect.” Only three intervention effects were graded as “moderate.” That is, the literature review revealed moderate confidence that ABA-Based Early Intensive Behavioral and Developmental Interventions are associated with improvements in IQ/cognitive abilities as well as language/communication skills. Similarly, the literature review revealed moderate confidence that Play-/Interaction-Based Interventions are associated with improvements in joint attention. With regard to Behavioral and Developmental Early Intervention-Parent Training, the AHRQ review revealed “low” confidence in positive treatment effects on symptom severity and language/communication outcomes, as well as no effect on IQ/cognitive outcomes.
Does Recent Evidence Change our Confidence in the Efficacy/Effectiveness of Parent-Mediated Interventions?
As emphasized above, all three categories of behavioral intervention approaches evaluated in the AHRQ reports (Warren et al., 2011; Weitlauf et al., 2014) include parent-mediated intervention strategies. However, for comprehensive, clinician-delivered intervention approaches (i.e., ABA-Based Early Intensive Behavioral and Developmental Interventions), the added value of including parent-mediated intervention components has not been fully quantified. Thus, the most direct evidence about the efficacy of parent-mediated interventions comes from Behavioral and Developmental Early Intervention-Parent Training, as well as parent-mediated focused interventions included among Play-/Interaction-Based Interventions.
To the largest extent possible, the current literature review update used the same methods and criteria to identify published articles providing adequate evidence as the original AHRQ reports (Warren et al., 2011; Weitlauf et al., 2014). One important exception is that the current literature review update was limited to interventions for younger children and only included samples of children with ASD (or at risk) who were 6 years or younger at baseline (the original AHRQ reports included samples of children who were 12 years or younger). Inter-rater reliability on the study selection process between the 2014 AHRQ review and the current review update was calculated based on articles published in 2012, revealing excellent agreement between the two reviews (kappa = 0.89). The review deadline for the current update was October 2015.
The current literature review update identified 49 articles that were published between 2012 and 2015 and were not included in the AHRQ 2014 review. These 49 articles reported on 47 unique research studies. For 6 of these 47 unique research studies, previous publications on the same research samples were identified (Carter et al., 2011; Casenhiser, Shanker, & Stieben, 2013; Dawson et al., 2010, 2012; Green et al., 2010; Kasari, Freeman, & Paparella, 2006; Kasari, Gulsrud, Freeman, Paparella, & Hellemann, 2012; Kasari, Paparella, Freeman, & Jahromi, 2008; Siller et al., 2013; Yoder & Stone, 2006a, 2006b).
Among the 47 studies with newly published data, 30 reported on intervention approaches that were exclusively parent-mediated. Of these, nine evaluated comprehensive intervention approaches (i.e., Behavioral and Developmental Early Intervention-Parent Training) and eleven evaluated play−/interaction-based, focused, parent-mediated approaches (i.e., Play-/Interaction-Based Interventions). Finally, the literature review update identified ten parent-mediated intervention studies that did not fit into either of these two categories and will not be discussed in the current chapter. Of these ten studies, four evaluated interventions for high-risk infants (Baranek et al., 2015; Green et al., 2013; Green et al., 2015; Rogers et al., 2014), three evaluated interventions targeting challenging behaviors or sleep (Bearss et al., 2015; Grahame et al., 2015; Johnson et al., 2013), and three evaluated interventions that did not directly address child outcomes and focused instead on improving parent knowledge and well-being (Feinberg et al., 2014; Suzuki et al., 2014; Zhang, Yan, Du, & Liu, 2014). While these studies do not fit into the scope of the current chapter, some of these topics are examined in-depth elsewhere in this volume including Part I (Chaps. 2, 3, and 4 discuss interventions for infants at high risk for autism) and Part IV (Chap. 18 discusses self-help for parents of children with autism). The following sections of this introductory chapter provide a summary of evidence from this updated review of the literature specific to parent-mediated interventions, both comprehensive and focused.
Newer Evidence About Comprehensive, Parent-Mediated Intervention Approaches
Improvements in language/communication
Siller and Sigman (2002, 2008) published the first pair of prospective longitudinal studies to show that responsive parental behaviors reliably predict long-term (16-year!) language gains in children with ASD. This finding, which has since been replicated by several research groups (e.g., Adamson, Bakeman, Deckner, & Romski, 2009; Baker, Messinger, Lyons, & Gantz, 2010; McDuffie & Yoder, 2010; Perryman et al., 2013; Warren, Brady, Sterling, Fleming, & Marquis, 2010), provided an important impetus to research evaluating parent-mediated interventions in ASD. Despite this correlational evidence, the 2014 AHRQ review (Weitlauf et al., 2014) failed to demonstrate a consistent treatment effect of comprehensive parent-mediated interventions (i.e., Behavioral and Developmental Early Intervention-Parent Training) on children’s communication/language outcomes. Although the 2014 AHRQ review identified several studies that reported significant treatment effects on communication/language outcomes (e.g., Aldred, Green, Emsley, & McConachie, 2012; Roberts et al., 2011; Strauss et al., 2012), it was concluded that the studies’ methodology (e.g., intervention approach, nature of the control group, outcome measure) was too variable to conclude with confidence that the evidence reflects a true and consistent treatment effect (i.e., Strength of Evidence grade: low for positive effect).
Of the nine comprehensive, parent-mediated intervention studies identified in the current literature update (Table 1.4), only one study (Wetherby et al., 2014) reported a significant treatment effect on a standardized, clinician-administered measure of children’s language abilities. In this study, the treatment effect was evident for children’s receptive, but not expressive language abilities. In addition, two studies showed significant treatment effects on measures derived from language samples collected during parent-child interaction (Casenhiser, Binns, McGill, Morderer, & Shanker, 2015; Hardan et al., 2015), and three studies showed significant treatment effects on parent-reported communication/language abilities (Green et al., 2010; Hardan et al., 2015; Pickles et al., 2015; Stadnick, Stahmer, & Bookman-Frazee, 2015).
Conclusions:
-
Standardized, clinician-administered measures of language/communication evidence two important strengths, when used in research evaluating parent-mediated interventions. First, compared to the intervention context, standardized measures capture children’s language/communication abilities at a fairly high level of generalization (i.e., different setting, materials, interactive partner). Second, when used in the context of a randomized clinical trial, clinician-administered measures allow the concealment of children’s group assignment. However, given characteristic difficulties with generalization, standardized, clinician-administered outcome measures set a very high bar when evaluating the impact of parent-mediated interventions on language/communication outcomes in children with autism. Moreover, standardized language measures typically focus on gains in vocabulary and language structure, rather than spontaneous, communicative, and functional language use typically targeted in parent-mediated interventions.
-
Although responsive parental behaviors are commonly observed in the context of parent-child play interactions, language learning occurs across many daily routines including caretaking, the completion of household chores, and community outings. Arguably, Wetherby et al. (2014) revealed the strongest treatment effects on language/communication because parents were provided with the supports necessary to embed intervention strategies across different kinds of daily routines.
-
Responsiveness-based intervention strategies may be most effective in promoting children’s early language milestones. That is, Carter et al. (2011) reported that children with relatively low object interest at baseline showed larger treatment-related gains in communication/language in response to a responsiveness-based intervention, compared to children with higher object interest.
Improvements in autism symptoms
The AHRQ 2014 review also identified several studies evaluating comprehensive parent-mediated intervention approaches that report significant treatment-related reductions in ASD symptoms (Aldred et al., 2012; Landa & Kalb, 2012; Strauss et al., 2012). Again, it is the studies’ heterogeneity of intervention approaches, sample characteristics, outcome measures, and findings that “makes it difficult to meaningfully compare outcomes across studies” (p. 85; Weitlauf et al., 2014). Overall, the AHRQ 2014 report concluded that there was “low” confidence that the evidence in support of a treatment effect of comprehensive, parent-mediated interventions on ASD symptom severity reveals a true (e.g., consistent) treatment effect.
None of the nine comprehensive, parent-mediated intervention studies identified in the current literature update (Table 1.4) reported adequate evidence to show significant treatment-related reductions on symptom severity scores derived from a standardized diagnostic measure (e.g., Autism Diagnostic Observation Schedule, ADOS, Lord et al., 2012). Preliminary evidence suggesting a treatment effect on ADOS classifications was reported by Solomon, VanEgeren, Mahoney, Huber, and Zimmerman (2014); however, due to methodological concerns, the authors state that “the improvements in autism symptomatology (…) must be viewed very cautiously” (p. 483). Short of changes on measures derived from standardized diagnostic measures, several studies revealed treatment effects on observational measures of specific symptom domains. For example, Wetherby et al. (2014) reported a significant treatment effect on the Social Composite of the Communication and Symbolic Behavior Scales (CSBS, Wetherby & Prizant, 2002). Similarly, several authors reported significant treatment-related gains on social communication behaviors observed during parent-child interaction (Green et al., 2010; Casenhiser et al., 2013, 2015; Solomon et al., 2014). Importantly, Pickles et al. (2015) reported that 61–80% of the (nonsignificant) treatment effect on ADOS social communication scores was mediated by gains in child initiations observed during parent-child interaction. Finally, two studies reported significant treatment effects on parent-reported measures of social communication and socialization (Green et al., 2010; Wetherby et al., 2014).
Conclusions:
-
Studies identified in the current literature review update provide little evidence to suggest that comprehensive , parent-mediated interventions have a true and consistent treatment effect on global measures of symptom severity, derived from standardized diagnostic instruments (e.g., ADOS).
-
Several studies have revealed significant treatment effects on symptom levels in the social domain. Measures to capture social outcomes vary across studies, both in content (e.g., social initiation, social communication, socialization) and method of data collection (i.e., clinical assessment, observation of parent-child interaction, parent report). This methodological heterogeneity limits the general conclusions that can be drawn.
-
Future research would benefit greatly from behavioral measures of children’s social symptoms that can feasibly be administered to diverse samples; that effectively capture aspects of children’s social attention, comprehension, and motivation; and that are related to the etiology of autism (i.e., endophenotypes). Current advances in eye-tracking of dynamic social stimuli bear great promise in this regard (Rice, Moriuchi, Jones, & Klin, 2012; Swanson & Siller, 2013).
Improvements in cognitive abilities/IQ
The AHRQ 2014 review (Weitlauf et al., 2014) found that most studies evaluating comprehensive, parent-mediated interventions do not find a significant treatment effect on children’s cognitive abilities/IQ. Of the nine studies evaluated for the current literature review update, at least four studies evaluated treatment outcomes using a standardized assessment of cognitive abilities (e.g., the Mullen Scales of Early Learning; Psychoeducation Profile-Revised), and no evidence was provided to suggest that comprehensive, parent-mediated interventions are associated with treatment effects in cognitive abilities/IQ (Solomon et al., 2014; Tonge, Brereton, Kiomall, Mackinnon, & Rinehart, 2014; Welterlin, Turner-Brown, Harris, Mesibov, & Delmolino, 2012; Wetherby et al., 2014).
Conclusions:
-
Although it is not unreasonable to assume that shorter-term gains in language/communication abilities and reductions in autism symptoms will increase children’s access to learning opportunities, leading to longer-term increases in cognitive abilities/IQ, this cascade of treatment effects has little empirical evidence to date.
Improvements in patterns of parent-child interaction
One outcome domain that was not addressed in the AHRQ 2014 review (Weitlauf et al., 2014) concerns the extent to which comprehensive, parent-mediated interventions improve patterns of parent-child interaction, specifically the use of development-enhancing parental strategies. Recent years have witnessed an emerging consensus around evidence-based, development-enhancing intervention strategies. This consensus has been articulated under the moniker of Naturalistic Developmental Behavioral Interventions (NDBI; Schreibman et al., 2015) and includes strategies such as child choice, environmental arrangement, natural reinforcement, balanced turn taking, contingent imitation, and broadening the child’s attentional focus. Although there are currently no universal fidelity measures to capture these development-enhancing intervention strategies, most of the nine comprehensive, parent-mediated intervention studies identified in the current literature update (Table 1.4) measured changes in parental behaviors and strategies. For example, Hardan et al. (2015) used prespecified fidelity criteria derived from Pivotal Response Treatment, demonstrating that parents were able to learn and implement the intervention strategies with high accuracy. Similarly, three studies used observational fidelity scales capturing a range of intervention strategies (Casenhiser et al., 2013, 2015; Solomon et al., 2014; Stadnick et al., 2015), demonstrating significant increases in parental use of these strategies over the course of the intervention. Finally, two studies used measures of parental responsiveness (Carter et al., 2011; Green et al., 2010), demonstrating treatment effects on this measure.
Conclusions:
-
Comprehensive, parent-mediated interventions are effective for increasing a range of development-enhancing parental behaviors and intervention strategies. Although different intervention approaches target and measure different parental behaviors, an emerging consensus has been articulated under the moniker of NDBI.
-
To date, only one comprehensive, parent-mediated intervention study has investigated whether the parents’ use of NDBI strategies mediates the relation between treatment and child outcome. That is, a clinical trial of the PACT intervention reported that the parents’ synchronous responses to the child partially mediated gains in social communication (Pickles et al., 2015).
-
Future research would benefit greatly from a universal fidelity measure that evaluates the extent to which parents implement key, evidence-based intervention strategies, as summarized under the NDBI moniker (Schreibman et al., 2015).
Newer Evidence About Focused, Play-/Interaction-Based, Parent-Mediated Intervention Approaches
Improvements in language/communication
The 2014 AHRQ report identified three Play-/Interaction-Based Interventions that reported significant treatment effects on communication outcomes (Kasari et al., 2008; Schertz, Odom, Baggett, & Sideris, 2013; Venker, McDuffie, Weismer, & Abbeduto, 2012). Kasari et al. (2008) evaluated the efficacy of a clinician-implemented JASPER intervention and found significant treatment-related gains in children’s expressive, but not receptive, language outcomes. Evaluating a joint attention parent-mediated intervention, Schertz et al. (2013) reported significant treatment effects on a standardized measure of receptive language, as well as parent-reported communication skills (i.e., Vineland Adaptive Behavior Scales, VABS; Sparrow, Cicchetti, & Balla, 2005). Finally, evaluating a parent-mediated intervention targeting the parents’ verbal responsiveness, Venker et al. (2012) reported a significant treatment effect on an observational measure of children’s communication , demonstrating increases in prompted, but not spontaneous, communicative acts. Based on this limited evidence, the 2014 AHRQ review concluded that there was low evidence supporting a positive effect of Play-/Interaction-Based Interventions on children’s language/communication outcomes.
Of the eleven focused, parent-mediated intervention studies identified in the current literature update (Table 1.5), six evaluated treatment-related gains in spoken communication/language (Ginn, Clionsky, Eyberg, Warner-Metzger, & Abner, 2015; Kasari, Siller et al., 2014; Kasari, Gulsrud, Paparella, Hellemann, & Berry, 2015; Siller et al., 2013; Siller, Swanson, Gerber, Hutman, & Sigman, 2014; Thompson, McFerran, & Gold, 2014; Woo, Donnelly, Steinberg-Epstein, & Leon, 2015). Of these six studies, only one study reported a significant treatment effect on children’s receptive, but not expressive, language skills evaluated using a standardized, examiner-administered measure (Woo et al., 2015). In addition, Siller et al. (2013) found that children’s expressive language abilities at baseline moderated subsequent treatment-related gains in expressive language. For preschoolers who entered the program with delayed expressive language skills (i.e., skills associated with children below 12 months of age, n = 24), results showed a significant, medium-to-large treatment effect that accounted for approximately 25% of the variance in children’s subsequent language gains. A comparable treatment effect was not found for children who entered the study with more advanced language skills.
Conclusions:
-
The only focused, parent-mediated intervention study that identified a significant treatment effect on children’s language abilities (i.e., receptive language) evaluated an intervention designed to enrich children’s sensorimotor experience (Woo et al., 2015). The intervention was delivered by email, and parents were instructed to implement two daily sessions (15–30 min) for 6 months. Given the intervention’s low intensity (at least in terms of clinician time), a significant treatment effect on children’s receptive language abilities is surprising and may be attributed to several methodological weaknesses of the research design. Most importantly, less than half of the families randomized to the experimental group completed the intervention protocol and were included in the data analyses. Thus, a certain amount of intensity in terms of clinician time, as well as a focus on intervention strategies that parents can implement across multiple natural routines (Wetherby et al., 2014), may be necessary to affect generalized language gains.
-
Consistent with developmental theory and research evaluating comprehensive, parent-mediated interventions (Carter et al., 2011), findings presented by Siller et al. (2013) suggest that responsiveness-based parent-mediated interventions may be most effective at facilitating children’s earliest language milestones.
Improvements in autism symptoms
In evaluating the effect of Play-/Interaction-Based Interventions on autism symptoms, the AHRQ 2014 report addressed three specific symptom domains: joint attention, play/imitation skills, and social skills.
Improvements in joint attention
The AHRQ 2014 review identified nine intervention studies that incorporated play- or interaction-based strategies to target joint attention outcomes (Weitlauf et al., 2014). Based on this body of literature , the authors noted consistent evidence to suggest that Play-/Interaction-Based Interventions increase joint attention outcomes. Despite this consistent evidence, the authors rated the Strength of Evidence as moderate because (1) the duration of effects is unclear and (2) participants in most studies were also receiving other early intervention and disentangling effects is difficult. In light of the current focus, it is also noteworthy that only two of these studies evaluated parent-mediated interventions (Kasari, Gulsrud, Wong, Kwon, & Locke, 2010; Schertz et al., 2013). Both studies reported significant treatment effect on children’s responsiveness to other’s bids for joint attention that were maintained over a 2–12-month follow-up period. Treatment effects on children’s initiations of joint attention were not statistically significant.
Of the eleven focused, parent-mediated intervention studies identified in the current literature update (Table 1.5), five studies investigated treatment effects on joint attention outcomes (Carr et al., 2016; Chiang, Chu, & Lee, 2016; Kasari et al., 2015; Kasari, Lawton, et al., 2014; Kasari, Siller, et al., 2014; Poslawsky et al., 2015). Out of these five studies, two reported significant treatment effects on joint attention outcomes evaluated using the Early Social Communication Scale (Mundy, Sigman, Ungerer, & Sherman, 1986), a structured, examiner-administered observational measure of nonverbal communication. Kasari, Lawton, et al. (2014) evaluated a parent-mediated intervention based on JASPER, reporting a significant treatment effect on children’s initiations of joint attention between baseline and exit. This treatment effect was not maintained during a 3-month follow-up. Similarly, Poslawsky et al. (2015) reported a conditional treatment effect of a video-feedback intervention to promote positive parenting adapted to autism (VIPP-AUTI) on child initiations of joint attention, moderated by school attendance. That is, the intervention effectively increased joint attention outcomes, but only for children who were not attending school.
Improvements in play skills and imitation
The 2014 AHRQ report identified several Play-/Interaction-Based Interventions that reported significant treatment effects on children’s functional and symbolic play (Kasari et al., 2006; Kasari et al., 2010; Murdock & Hobbs, 2011; Wong, 2013) and imitation skills (Ingersoll, 2010, 2012). Based on this small and somewhat inconsistent body of literature, the 2014 AHRQ report concluded that there is low confidence in a positive effect of Play-/Interaction-Based Interventions on play/imitation outcomes . Again, only one of the above-mentioned studies tested the efficacy of a parent-mediated intervention on this symptom domain (Kasari et al., 2010).
Of the eleven focused, parent-mediated intervention studies identified in the current literature update (Table 1.5), four studies reported outcome measures of functional/symbolic play (Carr et al., 2016; Kasari et al., 2015; Kasari, Lawton, et al., 2014; Poslawsky et al., 2015) or imitation skills (Sanefuji & Ohgami, 2013). Kasari et al. (2015) reported a significant treatment effect on the frequency of functional play acts as well as the overall play level between baseline and exit, but treatment effects were not maintained at follow-up. Similarly, Kasari, Lawton, et al. (2014) and Carr et al. (2016) reported significant treatment effect on the diversity of symbolic play acts, but only for children who showed at least one symbolic play act at study entry. Finally, Sanefuji and Ohgami (2013) reported that parent-mediated contingent imitation intervention significantly improved children’s imitative abilities.
Improvements in social abilities
The 2014 AHRQ report identified five studies that effectively increased children’s social engagement (i.e., joint engagement, shared positive affect) with teachers (Lawton & Kasari, 2012; Wong, 2013) or parents (Kaale, Smith, & Sponheim, 2012; Kasari et al., 2010). Based on this evidence, the 2014 AHRQ review concluded that there was low evidence supporting a positive effect of Play-/Interaction-Based Interventions on social skills.
Of the eleven focused, parent-mediated intervention studies identified in the current literature update (Table 51.), three studies found that parent-mediated JASPER increased children’s observed joint engagement during parent-child interaction (Carr et al., 2016; Chiang et al., 2016; Kasari et al., 2015; Kasari, Lawton, et al., 2014). In addition, Siller et al. (2014) reported a significant treatment effect on children’s attachment-related behaviors (both, observed during a brief separation-reunion episode and evaluated using a parent-report questionnaire). This is the first clinical trial to demonstrate that responsiveness-based interventions can enhance the attachment-related behaviors of children with autism, a finding that has previously been shown for other high-risk populations (Heinicke et al., 1999; Heinicke, Fineman, Ponce, & Guthrie, 2001; Juffer, Bakermans-Kranenburg, & van IJzendoorn, 2008; Powell, Cooper, Hoffman, & Marvin, 2007; van der Boom, 1994, 1995). In addition, two studies reported significant treatment effects on parent-reported measures of social/emotional awareness and functioning (Ginn et al., 2015; Thompson et al., 2014).
Conclusions:
-
Focused, parent-mediated interventions can improve core autism symptoms, including joint attention, functional/symbolic play, and imitation. Given differences in intervention and measurement approach, findings are somewhat inconsistent and the duration of effects is unclear.
-
Several clinician-administered, semi-structured observational measures have been used to evaluate gains in joint attention, play skills, and imitation (e.g., Early Social Communication Scale, Mundy et al., 1986; Communication and Symbolic Behavior Scales, Wetherby & Prizant, 2002; Structured Play Assessment, Ungerer & Sigman, 1981; Motor Imitation Scale, Motor Imitation Scale, Stone, Ousley, & Littleford, 1997). In the context of clinical trials, clinician-administered measures allow the concealment of children’s group assignment. However, age norms are typically not available for these measures (e.g., the CSBS is normed for children up to 24 months), making the longer-term impact on core deficits difficult to evaluate.
-
Focused, parent-mediated interventions can improve children’s social engagement during interactions with the caregiver, including markers of the relationship quality (i.e., attachment-related child behaviors). Since play-based interactions between parent and child often provide the context for both, intervention and measurement, the degree of generalization implicit in these measures is limited.
Improvements in pattern of parent-child interaction
Consistent with the literature on comprehensive, parent-mediated interventions (i.e., Behavioral and Developmental Early Intervention-Parent Training), focused interventions also provide support that parents can effectively learn and implement a broad range of intervention strategies, aiming to promote their children’s social communication skills . Of the eleven focused, parent-mediated intervention studies identified in the current literature update (Table 1.5), two used prespecified criteria for parent fidelity of implementation, demonstrating that 50% of parents demonstrated skill mastery of implementing intervention strategies derived from parent-child interaction therapy (Ginn et al., 2015) and 75% of parents demonstrated complete fidelity in implementing Qigong massage therapy (Silva & Schalock, 2013). In addition, four studies reported significant treatment effects on a range of development-enhancing intervention strategies, including non-intrusiveness, positive following, and responsive communication (Ginn et al., 2015; Kasari, Siller, et al., 2014; Poslawsky et al., 2015; Siller et al., 2013; Siller et al., 2014).
Conclusions:
-
Consistent with results from research evaluating comprehensive, parent-mediated interventions, focused interventions have also been shown to increase a range of development-enhancing parental behaviors and intervention strategies. Although heterogeneous measures are used, underlying concepts relate to child choice, environmental arrangement, natural reinforcement, balanced turn taking, contingent imitation, and broadening the child’s attentional focus (i.e., NDBI).
-
Above, we cited a comprehensive, parent-mediated intervention study that showed that parents’ synchronous responses to the child partially mediated gains in social communication (Pickles et al., 2015). Similarly, results from a clinical trial of parent-mediated JASPER (a focused, parent-mediated intervention) found that parents’ use of mirrored pacing mediated subsequent treatment gains in joint engagement (Gulsrud, Hellemann, Shire, & Kasari, 2016). Both measures of synchronous responsiveness and mirrored pacing emphasize the parents’ ability to respond to and elaborate on the child’s focus of attention, interest, and play actions.
General Conclusions About the Efficacy of Parent-Mediated Interventions
The 2013 Cochrane review and meta-analysis of clinical trials “did not find statistical evidence of gains from parent-mediated approaches in most of the primary outcomes assessed” (p. 2, Oono et al., 2013). That is, evidence of treatment effects on most aspects of language and communication , including child initiations observed during parent-child interaction, was “largely inconclusive and inconsistent across studies” (p. 2). In contrast, the Cochrane report revealed strong and consistent treatment effects on patterns of parent-child interaction (i.e., shared attention, parent synchrony) and some suggestive evidence of improvements in language comprehension and reductions in autism symptoms. These overall conclusions about intervention efficacy are consistent with those of a similar literature review of parent-mediated interventions for children under 3 years of age (Beaudoin et al., 2014), as well as the AHRQ reviews discussed in detail above (Warren et al., 2011; Weitlauf et al., 2014).
The conclusions drawn in the 2013 Cochrane report were based on 17 clinical trials of parent-mediated interventions published before August 2012. The current literature review discussed an additional 20 studies published between 2012 and October 2015. Despite some differences in study selection methods, 17 of the 20 studiesFootnote 1 identified for the current literature review update were randomized clinical trials, effectively doubling the amount of evidence available in 2013. Despite this exponential increase in the number rigorous studies evaluating the efficacy of parent-mediated interventions in autism, the dominant characteristic of this body of literature continues to be its heterogeneity – heterogeneity of outcome measures, participant characteristics, and intervention strategies (i.e., structure, content, approach). In the following section, we will briefly discuss three general conclusions from this literature review update and refer the reader to corresponding chapters of the Handbook where related issues are discussed in greater detail.
Generalization of intervention outcomes
The primary question addressed in the 2013 Cochrane review (Oono et al., 2013) was whether the available evidence (defined broadly in terms of quality, quantity, and consistency) is sufficient to confidently determine that a given intervention approach produces favorable outcomes. In contrast, the 2014 AHRQ review aimed to answer more specific questions about the interventions’ impact on specific outcome domains. For example: Is the given intervention approach effective for increasing children’s language/communication outcomes? Results from the current literature review update highlight the importance of organizing outcome measures not only by outcome domain, but also the degree of similarity between the intervention and assessment context. That is, meaningful learning implies that a skill that is acquired in one setting (i.e., the intervention setting) can be applied in another setting (i.e., the assessment setting). Similarly, meaningful learning implies that a skill that is acquired in a certain way (e.g., with a certain material or interactive partner) can be applied in a different way (e.g., with different materials or interactive partners). When presenting the primary results of a clinical trial evaluating the PACT intervention, Green et al. (2010) concluded very eloquently that the generalization of the intervention effect was attenuated across interaction and context. That is, results revealed significant treatment effects on outcome measures that were more proximal to the intervention, including measures of parent and child communication observed during parent-child interaction. In contrast, treatment effects on outcome measures that were more distal to the intervention including measures of social communication skills assessed during interactions with an assessor or observed in children’s natural school environment were smaller and nonsignificant.
At this point, we do not have a quantitative way to represent the degree of generalization that is necessary in order to apply a skill that is acquired in one way (i.e., in accordance with the intervention procedures) and assessed in another (i.e., as part of the outcome assessment). In the absence of such a quantitative representation, the conclusions we can draw from a systematic review of the literature are limited in several ways. First, the interpretation of each outcome measure changes depending on the nature of the evaluated intervention. This complicates the comparison between different kinds of interventions. For example, consider an intervention that is implemented by a clinician and uses a structured teaching approach where skills are broken down into separate components and taught one at a time using behavioral learning principles (e.g., Discrete Trial Training; Lovaas, 1987). In the context of such an intervention, a clinician-administered, standardized test of cognitive abilities evidences many similarities with the intervention procedures and should be interpreted as a relatively proximal outcome measure. That is, intervention and assessment activities are typically administered at a table, target discrete, de-contextualized skills; focus on basic cognitive functions such as matching, imitation, and responding to prompts; and involve a clinician that implements behavioral principals to elicit specific child behaviors. In contrast, the same assessment should be interpreted as a relatively distal outcome measure when used to evaluate a parent-mediated intervention that is implemented in the context of natural family routines and focuses on social communication outcomes.
Second, the attenuation of intervention effects across interaction and context described by Green et al. (2010) for the PACT intervention reveals a pattern that is consistent across the literature on parent-mediated interventions more broadly. Arguably, interventions that are more successful at achieving more generalized outcomes are those that are implemented over longer durations, involve more hours of clinician time, and are implemented across multiple natural family routines (Wetherby et al., 2014). The likely association between the intensity of a parent-mediated intervention and the degree of generalization in children’s learning outcomes raises questions about the cost-effectiveness relationship, including “how much generalization” you can reasonably expect from a short-term, parent-mediated intervention. Eighteen of the 20 parent-mediated intervention studies included in the current literature review update involved fewer than 25 intervention sessions and were implemented over a period less than 12 months.
Finally, a quantitative way to represent the degree of generalization between intervention and assessment would facilitate the integration of evidence from studies using a controlled group design and studies using single-subject research. That is, single-subject research is generally more suitable for evaluating more proximal as compared to more distal intervention outcomes.
Supporting diverse parents
During the last decade, intervention research in autism has started to recognize that not all children benefit from interventions in the same way. For example, results from the current literature review update suggest that responsiveness-based parent-mediated interventions may be most effective for children with autism who have limited language skills (Siller et al., 2013) or limited object interest (Carter et al., 2011). Along the same lines, Part I of this volume (Chaps. 2, 3, and 4) explores the role of child age on the implementation and efficacy of parent-mediated interventions. Specifically, the authors describe current research on interventions for infants at high risk for autism and discuss how their needs, and those of their families, can be met in the context of parent-mediated interventions.
Arguably the most robust finding from the current literature review update is that, on average, parents can be effectively taught to implement a broad range of intervention strategies. However, the emerging evidence also suggests that not all parents acquire the same level of proficiency in using the targeted strategies, maintain the use of these strategies over time, and implement the acquired strategies with sufficient intensity to affect children’s longer-term outcomes. Research on parent-mediated interventions in autism is only beginning to systematically identify parent or family characteristics that predict parent buy-in or treatment efficacy. Results from several studies suggest that higher baseline levels of self-reported parenting stress are related to smaller gains from parent-mediated interventions (see Chaps. 2 and 10; Osborne, McHugh, Saunders, & Reed, 2008; Robbins, Dunlap, & Plienis, 1991; Stadnick et al., 2015). However, other research suggests that a certain level of parenting stress increases (rather than reduces) parent implementation of intervention strategies during everyday interactions and routines. That is, Alquraini and Mahoney (2015) found that high levels of parenting stress enhance the extent to which treatment-related gains in maternal responsiveness lead to improvements in child development. In addition to this emerging literature on the role of parenting stress, Siller et al. (2013) reported that parents who were better able to describe their child’s experience and behaviors in a complex, open, and accepting way are more likely to benefit from an intervention based on parent coaching, compared to parents who find it more difficult to engage in such conversations about their child. As discussed in detail in Chap. 12, current parent coaching approaches are based on the recognition that (1) parents have an intimate knowledge of the child’s abilities, challenges, and typical performance; (2) parents understand the child’s and the family’s daily routines, environments, and culture; and (3) parents have ideas about the goals they would like to accomplish for their child, themselves, and as a family. Not all parents may be equally prepared to engage in such conversations about their child. Interestingly, results presented by Siller et al. (2018) suggest that the parents’ capacity for reflection and self-evaluation can be effectively increased in the context of parent coaching. Part II of this volume focuses on a broad range of individual differences between parents of children with autism, discussing strategies to support parents who experience financial hardship and poverty (Chap. 5 and 7), cultural differences and stigma (Chap. 6), and cognitions/emotions that may make it difficult to fully engage in parent coaching (Chap. 8).
Differences and similarities between parent-mediated intervention approaches
Parent-mediated intervention approaches in autism have been developed, and are implemented, by professionals with training across many disciplines, including early childhood education, clinical or developmental psychology, speech-language pathology, and behavior analysis, holding a range of professional licenses, degrees, or certifications. Further, available interventions differ from each other in their approach (e.g., theoretical framework, terminology), content (e.g., targeted family routines, learning outcomes, adult-learning strategies), and structure (e.g., number of weekly, clinician-implemented sessions, duration of the intervention period, training, and experience of the interventionists). Given the existing heterogeneity of intervention approaches, broad statements about the efficacy/effectiveness of parent-mediated interventions are not intellectually satisfying or useful in practice. What would be more helpful is a greater understanding of the active ingredients that are shared across different approaches and responsible for increases in child development and parent learning. Further, it would be useful to have access to tools to effectively monitor the implementation of these active ingredients (i.e., fidelity measures) and to measure proximal outcomes to ensure that child and parent learning is impacted as predicted. Part VI and Part VII of this handbook discuss the implementation science perspective on parent-mediated interventions in greater detail. This includes strategies for supporting families across the globe (Chaps. 22, 23, and 24), as well as successful initiatives to support the community implementation of parent-mediated intervention strategies in the USA (Chaps. 25, 26, 27, and 28).
One distinction that was operationalized by Rogers and Vismara (2008), and applied in the 2014 AHRQ review concerns the distinction between comprehensive (i.e., interventions that are implemented during many hours per week, targeting multiple outcome domains) and focused intervention approaches (i.e., interventions that are implemented with relatively low intensity, focusing on a smaller number of outcomes). As discussed above, the current literature review supports the notion that parent-mediated interventions that are implemented over longer durations involve more hours of clinician time and are implemented across multiple natural family routines (Wetherby et al., 2014) and are more likely to produce generalized learning outcomes, compared to interventions that are more focused and short-term. However, in the context of parent-mediated interventions, a clear distinction between focused and comprehensive approaches proves to be difficult. First, many parent-mediated interventions emphasize the integration of learning outcomes across multiple developmental domains (e.g., social, play, language). Second, the intensity of a parent-mediated intervention is not only defined in terms of clinician hours but also the intensity with which parents implement the intervention during daily routines, as well as how many daily routines are directly targeted by the intervention.
Our ability to draw empirical conclusions about active ingredients from this heterogeneous body of literature is limited by the fact that (1) few studies directly compare different parent-mediated intervention approaches to each other and (2) most studies have relatively small sample sizes, providing limited statistical power to test hypotheses about mediators and moderators of intervention efficacy. This being said, the last decade has witnessed an emerging consensus about active ingredients of effective interventions (Schreibman et al., 2015). The current Handbook aims to capture this emerging consensus.
References
Adamson, L. B., Bakeman, R., Deckner, D. F., & Romski, M. A. (2009). Joint engagement and the emergence of language in children with autism and down syndrome. Journal of Autism and Developmental Disorders, 39, 84–96.
Aldred, C., Green, J., Emsley, R., & McConachie, H. (2012). Mediation of treatment effect in a communication intervention for pre-school children with autism. Journal of Autism and Developmental Disorders, 42, 447–454.
Alquraini, T., & Mahoney, G. (2015). An exploratory investigation of the role of parenting stress in relationship focused intervention. Journal of Applied Research in Intellectual Disabilities, 28, 536–547.
Baker, J. K., Messinger, D. S., Lyons, K. K., & Gantz, C. J. (2010). A pilot study of maternal sensitivity in the context of emergent autism. Journal of Autism and Developmental Disorders, 40, 988–999.
Baranek, G. T., Watson, L. R., Turner-Brown, L., Field, S. H., Crais, E. R., Wakeford, L., … Reznick, J. S. (2015). Preliminary efficacy of adapted responsive teaching for infants at risk of autism spectrum disorder in a community sample. Autism Research and Treatment, 386951. https://doi.org/10.1155/2015/386951
Bearss, K., Johnson, C., Smith, T., Lecavalier, L., Swiezy, N., Aman, M., … Scahill, L. (2015). Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: A randomized clinical trial. Journal of the American Medical Association, 313, 1524–1533. https://doi.org/10.1001/jama.2015.3150
Beaudoin, A. J., Sébire, G., & Couture, M. (2014). Parent training interventions for toddlers with autism Spectrum disorder. Autism Research and Treatment, 839890. https://doi.org/10.1155/2014/839890
Boyd, B. A., Hume, K., McBee, M. T., Alessandri, M., Gutierrez, A., Johnson, L., … Odom, S. L. (2014). Comparative efficacy of LEAP, TEACCH and non-model-specific special education programs for preschoolers with autism Spectrum disorders. Journal of Autism and Developmental Disorders, 44, 366–380. https://doi.org/10.1007/s10803-013-1877-9
Carr, T., Shih, W., Lawton, K., Lord, C., King, B., & Kasari, C. (2016). The relationship between treatment attendance, adherence, and outcome in a caregiver-mediated intervention for low-resourced families of young children with autism spectrum disorder. Autism, 20, 643–652. https://doi.org/10.1177/1362361315598634
Carter, A. S., Messinger, D. S., Stone, W. L., Celimli, S., Nahmias, A. S., & Yoder, P. (2011). A randomized controlled trial of Hanen's ‘More than Words’ in toddlers with early autism symptoms. Journal of Child Psychology & Psychiatry, 52, 741–752. https://doi.org/10.1111/j.1469-7610.2011.02395.x
Casenhiser, D. M., Binns, A., McGill, F., Morderer, O., & Shanker, S. G. (2015). Measuring and supporting language function for children with autism: Evidence from a randomized control trial of a social-interaction-based therapy. Journal of Autism Developmental Disorders, 45, 846–857. https://doi.org/10.1007/s10803-014-2242-3
Casenhiser, D. M., Shanker, S. G., & Stieben, J. (2013). Learning through interaction in children with autism: Preliminary data from a social-communication-based intervention. Autism, 17, 220–241. https://doi.org/10.1177/1362361311422052
Chiang, C. H., Chu, C. L., & Lee, T. C. (2016). Efficacy of caregiver-mediated joint engagement intervention for young children with autism spectrum disorders. Autism, 20, 172–182. https://doi.org/10.1177/1362361315575725
Dawson, G., Jones, E. J., Merkle, K., Venema, K., Lowy, R., Faja, S., … Webb, S. J. (2012). Early behavioral intervention is associated with normalized brain activity in young children with autism. Journal of the American Academy of Child & Adolescent Psychiatry, 51, 1150–1159. https://doi.org/10.1016/j.jaac.2012.08.018
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., … Varley, J. (2010). Randomized, controlled trial of an intervention for toddlers with autism: The early start Denver model. Pediatrics, 125, e17–e23. https://doi.org/10.1542/peds.2009-0958
Eikeseth, S., Klintwall, L., Jahr, E., & Karlsson, P. (2012). Outcome for children with autism receiving early and intensive behavioral intervention in mainstream preschool and kindergarten settings. Research in Autism Spectrum Disorders, 6, 829–835. https://doi.org/10.1016/j.rasd.2011.09.002
Feinberg, E., Augustyn, M., Fitzgerald, E., Sandler, J., Ferreira-Cesar Suarez, Z., Chen, N., … Silverstein, M. (2014). Improving maternal mental health after a child's diagnosis of autism spectrum disorder: Results from a randomized clinical trial. Journal of the American Medical Association Pediatrics, 168, 40–46. https://doi.org/10.1001/jamapediatrics.2013.3445
Ginn, N. C., Clionsky, L. N., Eyberg, S. M., Warner-Metzger, C., & Abner, J. P. (2015). Child-directed interaction training for young children with autism spectrum disorders: Parent and child outcomes. Journal of Clinical Child & Adolescent Psychology, 46, 101–109. https://doi.org/10.1080/15374416.2015.1015135
Grahame, V., Brett, D., Dixon, L., McConachie, H., Lowry, J., Rodgers, J., … Le Couteur, A. (2015). Managing repetitive behaviours in young children with autism Spectrum disorder (ASD): Pilot randomised controlled trial of a new parent group intervention. Journal of Autism and Developmental Disorders, 45, 3168–3182. https://doi.org/10.1007/s10803-015-2474-x
Green, J., Charman, T., McConachie, H., Aldred, C., Slonims, V., Howlin, P., … Consortium, P. (2010). Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. Lancet, 375, 2152–2160. https://doi.org/10.1016/S0140-6736(10)60587-9
Green, J., Charman, T., Pickles, A., Wan, M. W., Elsabbagh, M., Slonims, V., … Johnson, M. H. (2015). Parent-mediated intervention versus no intervention for infants at high risk of autism: A parallel, single-blind, randomised trial. Lancet Psychiatry, 2, 133–140. https://doi.org/10.1016/s2215-0366(14)00091-1
Green, J., Wan, M. W., Guiraud, J., Holsgrove, S., McNally, J., Slonims, V., … Johnson, M. (2013). Intervention for infants at risk of developing autism: A case series. Journal of Autism and Developmental Disorders, 43, 2502–2514. https://doi.org/10.1007/s10803-013-1797-8
Gulsrud, A. C., Hellemann, G., Shire, S., & Kasari, C. (2016). Isolating active ingredients in a parent-mediated social communication intervention for toddlers with autism spectrum disorder. Journal of Child Psychology and Psychiatry, 57, 606–613. https://doi.org/10.1111/jcpp.12481
Hardan, A. Y., Gengoux, G. W., Berquist, K. L., Libove, R. A., Ardel, C. M., Phillips, J., … Minjarez, M. B. (2015). A randomized controlled trial of pivotal response treatment group for parents of children with autism. Journal of Child Psychology and Psychiatry, 56, 884–892. https://doi.org/10.1111/jcpp.12354
Heinicke, C. M., Fineman, N. R., Ponce, V. A., & Guthrie, D. (2001). Relation-based intervention with at-risk mothers: Outcome in the second year of life. Infant and Mental Health Journal, 22, 431–462.
Heinicke, C. M., Fineman, N. R., Ruth, G., Recchia, S. L., Guthrie, D., & Rodning, C. (1999). Relationship-based intervention with at-risk mothers: Outcome in the first year of life. Infant Mental Health Journal, 20, 349–374.
Ingersoll, B. (2010). Brief report: Pilot randomized controlled trial of reciprocal imitation training for teaching elicited and spontaneous imitation to children with autism. Journal of Autism and Developmental Disorders, 40, 1154–1160. https://doi.org/10.1007/s10803-010-0966-2
Ingersoll, B. (2012). Brief report: Effect of a focused imitation intervention on social functioning in children with autism. Journal of Autism and Developmental Disorders, 42, 1768–1773. https://doi.org/10.1007/s10803-011-1423-6
Ingersoll, B., & Gergans, S. (2007). The effect of a parent-implemented imitation intervention on spontaneous imitation skills in young children with autism. Research in Developmental Disabilities: A Multidisciplinary Journal, 28, 163–175.
Johnson, C. R., Turner, K. S., Foldes, E., Brooks, M. M., Kronk, R., & Wiggs, L. (2013). Behavioral parent training to address sleep disturbances in young children with autism spectrum disorder: A pilot trial. Sleep Medicine, 14, 995–1004. https://doi.org/10.1016/j.sleep.2013.05.013
Juffer, F., Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2008). Promoting positive parenting: An attachment-based intervention. New York, NY: Taylor & Francis.
Kaale, A., Smith, L., & Sponheim, E. (2012). A randomized controlled trial of preschool-based joint attention intervention for children with autism. Journal of Child Psychology and Psychiatry, 53, 97–105. https://doi.org/10.1111/j.1469-7610.2011.02450.x
Kasari, C., Freeman, S., & Paparella, T. (2006). Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. Journal of Child Psychology and Psychiatry, 47, 611–620. https://doi.org/10.1111/j.1469-7610.2005.01567.x
Kasari, C., Gulsrud, A., Freeman, S., Paparella, T., & Hellemann, G. (2012). Longitudinal follow-up of children with autism receiving targeted interventions on joint attention and play. Journal of the American Academy of Child and Adolescent Psychiatry, 51, 487–495. https://doi.org/10.1016/j.jaac.2012.02.019
Kasari, C., Gulsrud, A., Paparella, T., Hellemann, G., & Berry, K. (2015). Randomized comparative efficacy study of parent-mediated interventions for toddlers with autism. Journal of Consulting and Clinical Psychology, 83, 554–563. https://doi.org/10.1037/a0039080
Kasari, C., Gulsrud, A. C., Wong, C., Kwon, S., & Locke, J. (2010). Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders, 40, 1045–1056. https://doi.org/10.1007/s10803-010-0955-5
Kasari, C., Lawton, K., Shih, W., Barker, T. V., Landa, R., Lord, C., … Senturk, D. (2014). Caregiver-mediated intervention for low-resourced preschoolers with autism: An RCT. Pediatrics, 134, e72–e79. https://doi.org/10.1542/peds.2013-3229
Kasari, C., Paparella, T., Freeman, S., & Jahromi, L. B. (2008). Language outcome in autism: Randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology, 76, 125–137. https://doi.org/10.1037/0022-006X.76.1.125
Kasari, C., Siller, M., Huynh, L. N., Shih, W., Swanson, M., Hellemann, G. S., & Sugar, C. A. (2014). Randomized controlled trial of parental responsiveness intervention for toddlers at high risk for autism. Infant Behavior & Development, 37, 711–721. https://doi.org/10.1016/j.infbeh.2014.08.007
Landa, R. J., & Kalb, L. G. (2012). Long-term outcomes of toddlers with autism spectrum disorders exposed to short-term intervention. Pediatrics, 130, S186–S190. https://doi.org/10.1542/peds.2012-0900Q
Lawton, K., & Kasari, C. (2012). Teacher-implemented joint attention intervention: Pilot randomized controlled study for preschoolers with autism. Journal of Consulting and Clinical Psychology, 80, 687–693. https://doi.org/10.1037/a0028506
Lieberman-Betz, R. G., Yoder, P., Stone, W. L., Nahmias, A. S., Carter, A. S., Celimli-Aksoy, S., & Messinger, D. S. (2014). An illustration of using multiple imputation versus listwise deletion analyses: The effect of Hanen's “more than words” on parenting stress. American Journal on Intellectual and Developmental Disabilities, 119, 472–486. https://doi.org/10.1352/1944-7558-119.5.472
Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., & Bishop, S. (2012). Autism diagnostic observation schedule (2nd ed.). Torrance, CA: Western Psychological Services.
Lovaas, O. I. (1987). Behavioral treatment and normal educational and intellectual functioning in young autistic children. Journal of Consulting and Clinical Psychology, 55, 3–9.
McDuffie, A., & Yoder, P. J. (2010). Types of parent verbal responsiveness that predict language in young children with autism spectrum disorders. Journal of Speech, Language, and Hearing Research, 53, 1026–1039.
Mundy, P., Sigman, M. D., Ungerer, J., & Sherman, T. (1986). Defining the social deficits of autism: The contribution of non-verbal communication measures. Journal of Child Psychology and Psychiatry & Allied Disciplines, 27, 657–669.
Murdock, L. C., & Hobbs, J. Q. (2011). Picture me playing: Increasing pretend play dialogue of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 41, 870–878. https://doi.org/10.1007/s10803-010-1108-6
National Autism Center. (2015). Findings and conclusions: National Standards Project, phase 2. Randolph, MA: Author.
Oono, I. P., Honey, E. J., & McConachie, H. (2013). Parent-mediated early intervention for young children with autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews, (4. Art. No.: CD009774). https://doi.org/10.1002/14651858.CD009974.pub2
Osborne, L. A., McHugh, L., Saunders, J., & Reed, P. (2008). Parenting stress reduces the effectiveness of early teaching interventions for autistic spectrum disorders. Journal of Autism and Developmental Disorders, 38, 1092–1103.
Perryman, T. Y., Carter, A., Messinger, D. S., Stone, W. L., Ivanescu, A. E., & Yoder, P. J. (2013). Brief report: Parental child-directed speech as a predictor of receptive language in children with autism symptomatology. Journal of Autism and Developmental Disorders, 43, 1983–1987.
Peters-Scheffer, N., Didden, R., Mulders, M., & Korzilius, H. (2010). Low intensity behavioral treatment supplementing preschool services for young children with autism spectrum disorders and severe to mild intellectual disability. Research in Developmental Disabilities, 31, 1678–1684. https://doi.org/10.1016/j.ridd.2010.04.008
Pickles, A., Harris, V., Green, J., Aldred, C., McConachie, H., Slonims, V., … Charman, T. (2015). Treatment mechanism in the MRC preschool autism communication trial: Implications for study design and parent-focussed therapy for children. Journal of Child Psychology and Psychiatry, 56, 162–170. https://doi.org/10.1111/jcpp.12291
Poslawsky, I. E., Naber, F. B. A., Bakermans-Kranenburg, M. J., van Daalen, E., van Engeland, H., & van Ijzendoorn, M. H. (2015). Video-feedback intervention to promote positive parenting adapted to autism (VIPP-AUTI): A randomized controlled trial. Autism, 19, 588–603. https://doi.org/10.1177/1362361314537124
Powell, B., Cooper, G., Hoffman, K., & Marvin, R. (2007). The circle of security project: A case study – ‘It’s hard to give that which you did not receive. In D. Oppenheim & D. F. Goldsmith (Eds.), Attachment theory in clinical work with children (pp. 172–202). New York, NY: Guilford Press.
Rice, K., Moriuchi, J. M., Jones, W., & Klin, A. (2012). Parsing heterogeneity in autism spectrum disorders: Visual scanning of dynamic social scenes in school-aged children. Journal of the American Academy of Child and Adolescent Psychiatry, 51, 238–248. https://doi.org/10.1016/j.jaac.2011.12.017
Robbins, F. R., Dunlap, G., & Plienis, A. J. (1991). Family characteristics, family training, and the progress of young children with autism. Journal of Early intervention, 15, 173–184.
Roberts, J., Williams, K., Carter, M., Evans, D., Parmenter, T., Silove, N., … Warren, A. (2011). A randomised controlled trial of two early intervention programs for young children with autism: Centre-based with parent program and home-based. Research in Autism Spectrum Disorders, 5, 1553–1566. https://doi.org/10.1016/j.rasd.2011.03.001
Rogers, J. S., Vismara, L., Wagner, L. A., McCormick, C., Young, G., & Ozonoff, S. (2014). Autism treatment in the first year of life: A pilot study of infant start, a parent-implemented intervention for symptomatic infants. Journal of Autism and Developmental Disorders, 44, 2981–2995. https://doi.org/10.1007/s10803-014-2202-y
Rogers, S. J., Estes, A., Lord, C., Vismara, L., Winter, J., Fitzpatrick, A., … Dawson, G. (2012). Effects of a brief early start Denver model (ESDM)–based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 51, 1052–1065. https://doi.org/10.1016/j.jaac.2012.08.003
Rogers, S. J., & Vismara, L. A. (2008). Evidence-based comprehensive treatments for early autism. Journal of Clinical Child and Adolescent Psychology, 37, 8–38. https://doi.org/10.1080/15374410701817808
Sanefuji, W., & Ohgami, H. (2013). “Being-imitated” strategy at home-based intervention for young children with autism. Infant Mental Health Journal, 34, 72–79. https://doi.org/10.1002/imhj.21375
Schertz, H. H., Odom, S. L., Baggett, K. M., & Sideris, J. H. (2013). Effects of joint attention mediated learning for toddlers with autism spectrum disorders: An initial randomized controlled study. Early Childhood Research Quarterly, 28, 249–258.
Schreibman, L., Dawson, G., Stahmer, A. C., Landa, R., Rogers, S. J., McGee, G. G., … Halladay, A. (2015). Naturalistic developmental behavioral interventions: Empirically validated treatments for autism Spectrum disorder. Journal of Autism and Developmental Disorders, 45, 2411–2428. https://doi.org/10.1007/s10803-015-2407-8
Schreibman, L., & Stahmer, A. C. (2013). A randomized trial comparison of the effects of verbal and pictorial naturalistic communication strategies on spoken language for young children with autism. Journal of Autism and Developmental Disorders, 44, 1244–1251. https://doi.org/10.1007/s10803-013-1972-y
Siller, M., Hotez, E., Swanson, M., Delavenne, A., Hutman, T., & Sigman, M. (2018). Parent coaching increases the parents’ capacity for reflection and self-evaluation: Results from a clinical trial in autism. Attachment and Human Development, DOI:10.1080/14616734.2018.1446737
Siller, M., Hutman, T., & Sigman, M. (2013). A parent-mediated intervention to increase responsive parental behaviors and child communication in children with ASD: A randomized clinical trial. Journal of Autism and Developmental Disorders, 43, 540–555. https://doi.org/10.1007/s10803-012-1584-y
Siller, M., & Sigman, M. (2002). The behaviors of parents of children with autism predict the subsequent development of their children’s communication. Journal of Autism and Developmental Disorders, 32, 77–89.
Siller, M., & Sigman, M. (2008). Modeling longitudinal change in the language abilities of children with autism: Investigating the role of parent behaviors and child characteristics as predictors of change. Developmental Psychology, 44, 1691–1704.
Siller, M., Swanson, M., Gerber, A., Hutman, T., & Sigman, M. (2014). A parent-mediated intervention that targets responsive parental behaviors increases attachment behaviors in children with ASD: Results from a randomized clinical trial. Journal of Autism and Developmental Disorders, 44, 1720–1732. https://doi.org/10.1007/s10803-014-2049-2
Silva, L., & Schalock, M. (2013). Treatment of tactile impairment in young children with autism: Results with qigong massage. International Journal of Therapeutic Massage & Bodywork, 6, 12–20.
Solomon, R., Van Egeren, L. A., Mahoney, G., Huber, M. S. Q., & Zimmerman, P. (2014). PLAY project home consultation intervention program for young children with autism spectrum disorders: A randomized controlled trial. Journal of Developmental and Behavioral Pediatrics, 35, 475–485. https://doi.org/10.1097/DBP.0000000000000096
Sparrow, S. S., Cicchetti, D., & Balla, D. A. (2005). Vineland adaptive behavior scales - 2nd edition manual. Minneapolis, MN: NCS Pearson.
Stadnick, N. A., Stahmer, A., & Bookman-Frazee, L. (2015). Preliminary effectiveness of project ImPACT: A parent-mediated intervention for children with autism Spectrum disorder delivered in a community program. Journal of Autism and Developmental Disorders, 45, 2092–2104. https://doi.org/10.1007/s10803-015-2376-y
Stone, W., Ousley, O., & Littleford, C. (1997). Motor imitation in young children with autism: What’s the object? Journal of Abnormal Child Psychology, 25, 475–485.
Strain, P. S., & Bovey, E. H. (2011). Randomized, controlled trial of the LEAP model of early intervention for young children with autism Spectrum disorders. Topics in Early Childhood Special Education, 31, 133–154.
Strauss, K., Vicari, S., Valeri, G., D-Elia, L., Arima, S., & Fava, L. (2012). Parent inclusion in early intensive behavioral intervention: The influence of parental stress, parent treatment fidelity and parent-mediated generalization of behavior targets on child outcomes. Research in Developmental Disabilities, 33, 688–703. https://doi.org/10.1016/j.ridd.2011.11.008
Suzuki, M., Yamada, A., Watanabe, N., Akechi, T., Katsuki, F., Nishiyama, T., … Furukawa, T. A. (2014). A failure to confirm the effectiveness of a brief group psychoeducational program for mothers of children with high-functioning pervasive developmental disorders: A randomized controlled pilot trial. Neuropsychiatric Disease and Treatment, 10, 1141–1153. https://doi.org/10.2147/ndt.s60058
Swanson, M., & Siller, M. (2013). Patterns of gaze behavior during an eye-tracking measure of joint attention in typically developing children and children with autism Spectrum disorder. Research in Autism Spectrum Disorder, 7, 1087–1096. https://doi.org/10.1016/j.rasd.2013.05.007
Thompson, G. A., McFerran, K. S., & Gold, C. (2014). Family-centred music therapy to promote social engagement in young children with severe autism spectrum disorder: A randomized controlled study. Child: Care, Health, and Development, 40, 840–852. https://doi.org/10.1111/cch.12121
Tonge, B., Brereton, A., Kiomall, M., Mackinnon, A., & Rinehart, N. J. (2014). A randomised group comparison controlled trial of ‘preschoolers with autism’: A parent education and skills training intervention for young children with autistic disorder. Autism, 18, 166–177. https://doi.org/10.1177/1362361312458186
Ungerer, J. A., & Sigman, M. (1981). Symbolic play and language comprehension in autistic children. American Academy of Child Psychiatry, 20, 318–337.
van der Boom, D. C. (1994). The influence of temperament and mothering on attachment and exploration: An experimental manipulation of sensitive responsiveness among lower-class mother with irritable infants. Child Development, 65, 1457–1477.
van der Boom, D. C. (1995). Do first-year intervention effects endure? Follow-up during toddlerhood of a sample of Dutch irritable infants. Child Development, 66, 1798–1816.
Venker, C. E., McDuffie, A., Weismer, S. E., & Abbeduto, L. (2012). Increasing verbal responsiveness in parents of children with autism: A pilot study. Autism: The International Journal of Research and Practice, 16, 568–585.
Warren, S. F., Brady, N. C., Sterling, A. M., Fleming, K., & Marquis, J. (2010). The effects of maternal responsivity on the language development of children with fragile X syndrome. American Journal on Intellectual and Developmental Disability, 115, 54–75.
Warren, Z., Veenstra-VanderWeele, J., Stone, W., Bruzek, J. L., Nahmias, A. S., Foss-Feig, J. H., … McPheeters, M. L. (2011). Therapies for children with autism spectrum disorders. Comparative effectiveness Review No. 26. (Prepared by the Vanderbilt Evidence-based Practice Center under Contract No. 290–2007-10065-I.) AHRQ Publication No. 11-EHC029-EF. Rockville, MD: Agency for Healthcare Research and Quality. Available at: www.effectivehealthcare.ahrq.gov/reports/final.cfm.
Weitlauf, A. S., McPheeters, M. L., Peters, B., Sathe, N., Travis, R., Aiello, R., … Warren Z. (2014). Therapies for Children With Autism Spectrum Disorder: Behavioral Interventions Update. Comparative Effectiveness Review No. 137. (Prepared by the Vanderbilt Evidence-based Practice Center under Contract No. 290–2012-00009-I.) AHRQ Publication No. 14-EHC036-EF. Rockville, MD: Agency for Healthcare Research and Quality. Available at: www.effectivehealthcare.ahrq.gov/reports/final.cfm.
Welterlin, A., Turner-Brown, L. M., Harris, S., Mesibov, G., & Delmolino, L. (2012). The home TEACCHing program for toddlers with autism. Journal of Autism and Developmental Disorders, 42, 1827–1835. https://doi.org/10.1007/s10803-011-1419-2
Wetherby, A., & Prizant, B. (2002). Communication and symbolic behavior scales developmental profile- first Normed Edition. Baltimore, MD: Paul H. Brookes.
Wetherby, A. M., Guthrie, W., Woods, J., Schatschneider, C., Holland, R. D., Morgan, L., & Lord, C. (2014). Parent-implemented social intervention for toddlers with autism: An RCT. Pediatrics, 134, 1084–1093. https://doi.org/10.1542/peds.2014-0757
Wong, C., Odom, S. L., Hume, K., Cox, A. W., Fettig, A., Kucharczyk, S., … Schultz, T. R. (2013). Evidence-based practices for children, youth, and young adults with autism Spectrum disorder. Chapel Hill, NC: The University of North Carolina, Frank Porter Graham Child Development Institute, Autism Evidence-Based Practice Review Group.
Wong, C. S. (2013). A play and joint attention intervention for teachers of young children with autism: A randomized controlled pilot study. Autism, 17, 340–357. https://doi.org/10.1177/1362361312474723
Woo, C. C., Donnelly, J. H., Steinberg-Epstein, R., & Leon, M. (2015). Environmental enrichment as a therapy for autism: A clinical trial replication and extension. Behavioral Neuroscience, 129, 412–422. https://doi.org/10.1037/bne0000068
Yoder, P., & Stone, W. L. (2006a). A randomized comparison of the effect of two prelinguistic communication interventions on the acquisition of spoken communication in preschoolers with ASD. Journal of Speech, Language and Hearing Research, 49, 698–711. https://doi.org/10.1111/j.1365-2214.2007.00757_2.x
Yoder, P., & Stone, W. L. (2006b). Randomized comparison of two communication interventions for preschoolers with autism spectrum disorders. Journal of Consulting and Clinical Psychology, 74, 426–435. https://doi.org/10.1037/0022-006X.74.3.426
Zhang, W., Yan, T. T., Du, Y. S., & Liu, X. H. (2014). Brief report: Effects of solution-focused brief therapy group-work on promoting post-traumatic growth of mothers who have a child with ASD. Journal of Autism and Developmental Disorders, 44, 2052–2056. https://doi.org/10.1007/s10803-014-2051-8
Zwaigenbaum, L., Bauman, M., Choueiri, R., Kasari, C., Carter, A., Granpeesheh, D., … Natowicz, M. (2015). Early intervention for children with autism spectrum disorder under 3 years of age: Recommendations for practice and research. Pediatrics, 136, S60–S81. https://doi.org/10.1542/peds.2014-3667E
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Siller, M., Morgan, L. (2018). Systematic Review of Research Evaluating Parent-Mediated Interventions for Young Children with Autism: Years 2013 to 2015. In: Siller, M., Morgan, L. (eds) Handbook of Parent-Implemented Interventions for Very Young Children with Autism. Autism and Child Psychopathology Series. Springer, Cham. https://doi.org/10.1007/978-3-319-90994-3_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-90994-3_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-90992-9
Online ISBN: 978-3-319-90994-3
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)