
Abstract
Saliva plays an important role in maintaining healthy oral mucosa and teeth as well as oral function by continually covering and lubricating the oral tissues. Salivary gland dysfunction designates decreased saliva flow rate (salivary gland hypofunction), increased saliva flow rate (sialorrhea or hypersalivation), and changed saliva composition. Xerostomia (the subjective feeling of oral dryness) is often associated with salivary gland hypofunction and may severely affect nutritional intake, social interaction and quality of life. Local or systemic disorders and diseases are common causes of compromised saliva secretion. Some of these are related to gland pathology or to the pathophysiological conditions of the host, whereas others affect the gland innervation or are an iatrogenic result of treatment of a disease (e.g., radiation therapy for head and neck cancer, side effects of medications). In general, many patients suffering from diseases that influence salivary gland function also undergo treatments that may impair saliva secretion and/or induce xerostomia as an adverse effect. Consequently, it can be difficult to distinguish what can be attributed to the disease per se or what can be induced by treatment (e.g., medication intake). Thus, a thorough diagnostic workup and early diagnosis of salivary gland dysfunction are crucial to provide appropriate evidence-based treatment of salivary gland dysfunction to prevent oral sequelae and to initiate individualized alleviating management strategies of xerostomia.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Salivary gland
- Disorders
- Diseases
- Medications
- Dysfunction
- Hyposalivation
- Xerostomia
- Hypersalivation
- Histopathology
- Sialometry
- Subjective/objective/semiquantitative assessment
Introduction
Saliva plays an essential role in maintaining oral mucosal and tooth integrity by continually covering and lubricating the oral tissues. Salivary gland dysfunction includes a decreased saliva flow rate (salivary gland hypofunction), an increased saliva flow rate (sialorrhea or hypersalivation), or changed saliva composition. Salivary gland hypofunction designates a decreased saliva flow rate, while a diagnosis of hyposalivation implies a pathological low saliva flow rate, i.e., unstimulated whole saliva flow rate ≤ 0.1 ml/min and/or chewing-stimulated whole saliva flow rate ≤ 0.5–0.7 ml/min. Xerostomia (the subjective feeling of oral dryness) is often associated with salivary gland hypofunction and usually occurs when the unstimulated whole saliva flow rate has decreased to approximately 50% or less of its normal level in any given individual, indicating that more than one major salivary gland must be affected (Dawes 1987; Fox et al. 1987). Individuals can, however, also complain about xerostomia while the salivary flow rate is not reduced .
The composition of saliva is dependent on the type of glands from which the saliva is secreted and on the salivary flow rate and thus also on the type and duration of the stimuli that activates the secretory reflex (Pedersen et al. 2002). Consequently, the saliva composition varies in different sites of the oral cavity.
Saliva contains a large variety of proteins and peptides with lubricating and antimicrobial properties, including mucins, lysozyme, lactoferrin, histatins, and antibodies, the latter predominantly secretory immunoglobulin A (s-IgA). Thus, saliva reduces the risk of oral infection by preventing adhesion and proliferation of bacteria and fungi and reduces the risk of oral mucosal trauma from mechanical irritation and noxious substances. Furthermore, saliva provides protection against dental caries by diluting food detritus and bacteria, neutralizing acids from food and bacteria by salivary buffer systems, and contributing to formation of the pellicle and by clearance of the oral cavity. Moreover, tooth demineralization is prevented by salivary proteins such as statherin and proline-rich proteins, which ensure that saliva is supersaturated with respect to calcium phosphate salts (Lagerlof and Oliveby 1994; Lenander-Lumikari and Loimaranta 2000; Dawes et al. 2015). Regardless of the etiology of salivary gland hypofunction, a shift toward a more aciduric and acidophilic oral microbiota occurs when the unstimulated whole saliva flow rate is reduced below 0.20 ml/min with an increased risk of dental caries and oral candidosis as a consequence (Navazesh et al. 1995; Bardow et al. 2001).
The most common causes of salivary gland hypofunction and xerostomia include medication intake and polypharmacy, systemic diseases such as Sjögren’s syndrome (SS), and cancer treatment such as radiotherapy in the head and neck region and treatment with radioactive iodine. Furthermore, since salivary flow rate and composition are dynamic parameters that are strictly controlled by the physiological conditions of the host, numerous other systemic diseases and conditions influence salivary gland function. Some of these are related to gland pathology (immune-mediated or endocrine disorders) or interfere with salivary gland innervation (neurological disorders), whereas others are related to metabolic disturbances of the host (e.g., uncontrolled diabetes mellitus). In general, many of the patients who suffer from diseases or conditions that affect salivary gland function are also prescribed treatments with medications that, as an adverse effect, decrease saliva flow rate and/or induce compositional changes as well as xerostomia. In relation to the diagnostic workup of salivary gland hypofunction and xerostomia, it may therefore be difficult to distinguish between what can be attributed to the disease per se and what effects are induced by the treatment.
This chapter addresses normal salivary gland anatomy, histology, and physiology; describes a number of diseases, conditions, and other causes that may induce salivary gland dysfunction and/or xerostomia; summarizes the clinical manifestations and diagnostic workup of salivary gland pathology and dysfunction; and provides evidence-based management strategies for salivary gland dysfunction and xerostomia.
Salivary Gland Anatomy, Histology, and Physiology
Salivary Gland Anatomy
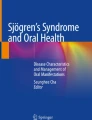
Saliva is produced by three paired major salivary glands, i.e., the parotid, the submandibular, and the sublingual glands, as well as 600–1000 minor salivary glands. The largest of these, the parotid glands, are located subcutaneously anterior to the external ear and posterior to the ramus of the mandible (Fig. 1). The parotid duct (Stensen’s duct) extends anteriorly across the masseter muscle to the front border where it turns sharply inward and opens into the oral cavity in the buccal mucosa located in the region of the second maxillary molar. The submandibular glands are located in the floor of the mouth where they fold around the posterior border of the mylohyoid muscle in close proximity to the inner surface of the mandibular body (Fig. 1). The excretory duct (Wharton’s duct) extends forward in the floor of the mouth and opens into the oral cavity on a small mucosal eminence, the sublingual caruncle. The sublingual glands are the smallest of the major salivary glands and are located in the floor of the mouth, anterior to the submandibular glands, in close proximity to the inner surface of the mandibular body (Fig. 1). In addition to the 8–20 small excretory ducts exiting directly into the oral cavity along the plica sublingualis, the sublingual gland also has a major sublingual duct (Bartholin’s duct) which opens into the submandibular duct (Wharton’s duct) terminating in the sublingual caruncle. The minor salivary glands are located within the submucosa of the buccal, lingual, palatal, and labial mucosa and floor of the mouth. Each minor gland has a single excretory duct, which exits directly into the oral cavity.

Anatomic location of the major salivary glands (Original drawing by Dr Hala Al-Janaby, Perth WA, Australia)
Salivary Gland Histology
The parotid gland is composed of serous acini made up of pyramidal-shaped cells with a basophilic appearance due to the presence of zymogen granules in the acinar cells. The submandibular and sublingual glands are composed of a mixture of mucous and serous acini (Fig. 2). The lobules of acini and associated ductal structures are separated by fibrous connective tissue septa, and variable amounts of adipose tissue may be present. The minor glands of the palate consist of mucous acini located in the submucosa with a lobular arrangement and clear to pale basophilic finely granular-appearing cytoplasm. The minor glands of the lip are a mixture of mucous and serous acini, and the lobules of acini are closely associated with surrounding structures including the skeletal muscle and nerves. The von Ebner’s glands in the tongue are purely serous.

Salivary gland histology, hematoxylin, and eosin staining. (a) Parotid gland. Parotid gland acini are exclusively serous made up of pyramidal-shaped cells with a basophilic appearance due to the presence of zymogen granules in the acinar cells. (b) Submandibular glands. Submandibular gland acini are mixed seromucous with a predominance of serous acini. (c) Sublingual glands. Sublingual glands and minor gland acini are mixed mucoserous with a predominance of mucous acini (Images courtesy of Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
The associated ductal system consists of intercalated, striated, and interlobular excretory ducts. Intercalated ducts are closest to the acinus and are continuous with striated ducts, which are larger. Both of these ducts are intralobular and known as secretory ducts. The striated ducts connect with interlobular ducts located in the septal connective tissue and are referred to as excretory ducts. Acini and intercalated ducts have surrounding myoepithelial cells, while the striated and excretory ducts are associated with basal cells. Myoepithelial cells are flat with cytoplasmic processes .
Salivary Gland Physiology
Saliva is of great importance for preserving oral health, as it is essential for oral functioning and preservation of the integrity of oral hard and soft tissues. Daily, in health, salivary glands secrete approximately 0.6 liter of a complex fluid from the major salivary glands, which accounts for about 90% of the saliva production, while approximately 10% is derived from minor salivary glands. The salivary flow rate has a circadian variation with a peak in the late afternoon. Unstimulated whole saliva flow rate averages 0.2–0.5 ml/min, while chewing-stimulated whole saliva flow rate is approximately 1.0–2.0 ml/min. Most of the unstimulated saliva during the daytime is produced by the submandibular glands (60%), followed by the parotid glands (25%), the sublingual glands (7–8%), and the minor salivary glands (7–8%) (Pedersen et al. 2002; Dawes et al. 2015).
Saliva is produced by the acinar cells that can be classified as serous or mucous. Parotid gland acini are exclusively serous, submandibular gland acini are mixed seromucous with a predominance of serous acini, and sublingual glands and minor glands acini are mixed mucoserous with a predominance of mucous acini (Fig. 2) with the exception of the von Ebner’s glands in the tongue, which are purely serous. Serous acini predominantly secrete non-glycosylated proteins, while the mucous acini predominantly secrete mucins.
The primary saliva is produced by the acinar cells and is isotonic to plasma due to the relatively high water permeability of the epithelium (Fig. 3). The ion composition of primary saliva is modified during its transport through the striated ducts. In these ducts, among others, sodium and chloride are reabsorbed, and bicarbonate and potassium are secreted (Fig. 3). As a result, the saliva secreted into the oral cavity is hypotonic to plasma. The hypotonicity and the final electrolyte composition are dependent on the saliva flow rate. In this respect, it is important to mention that potassium and bicarbonate are secreted from the ductal cells into the lumen of the salivary duct at a lower rate compared with that of the reabsorption of sodium and chloride. Since the ductal epithelium is impermeable to water and thus water does not accompany the reabsorption of sodium and chloride, this results in hypotonic saliva (Ekstrom et al. 2012; Villa et al. 2016). Myoepithelial cells surrounding the acini and ducts help to move saliva through the ducts (Bardow and Vissink 2015; Villa et al. 2016).

Salivary gland physiology (Reproduced with permission from Bardow and Vissink (2015))
Salivary secretion is evoked by reflex, nerve-mediated stimulation (Fig. 3). It is controlled by autonomic parasympathetic and sympathetic nerves. The parasympathetic nerves originate from the salivary nuclei in the pons and medulla oblongata, whereas the sympathetic center resides in the thoracic segments of the spinal cord. The salivary nuclei are modulated by neural inputs from the higher brain centers resulting in altered secretory signaling to salivary glands. Parasympathetic stimulation elicits water, electrolyte, and protein secretion, while sympathetic stimulation results in secretion of proteins and, to a lesser extent, secretion of water and electrolytes (Proctor and Carpenter 2007; Ekstrom et al. 2012; Villa et al. 2016).
The salivary acinar cells carry muscarinic M1 and M3 receptors, which bind acetylcholine released from parasympathetic nerves. Both types of receptors mediate fluid secretion as well as protein secretion via the inositol 1,4,5-trisphosphate/calcium (IP3/Ca2+) signaling pathway. Norepinephrine released from the sympathetic nerves and circulating epinephrine from the adrenal medulla act on α1- and β1-adrenergic receptors of the acinar cells to cause protein secretion and, to lesser extent, fluid secretion (Ekstrom et al. 2012; Proctor and Carpenter 2007; Bardow and Vissink 2015; Villa et al. 2016). Acinar cells provide most of the proteins and peptides, while the contribution of the ductal cells is minor .
Epidemiology of Xerostomia and Salivary Gland Hypofunction
Xerostomia is a common health issue worldwide. It is estimated that on average 20% of the adult population has xerostomia on a daily basis. However, it is surprising that around 10–20% in the age group of 20–30 years report xerostomia (Sreebny 2010). A study among 950 men and women aged 32 years showed that 10% had xerostomia (Murray et al. 2006). Xerostomia was associated with medication intake and medical conditions such as anemia, arthritis, and cardiovascular disease (Murray et al. 2006). In the age group over 65 years, the prevalence of xerostomia increases to 30–40%, but these studies also include populations of institutionalized and hospitalized elderly persons. The majority of studies have shown a correlation between xerostomia and hyposalivation, systemic diseases, and medication intake (Sreebny 2010; Villa et al. 2015). It is therefore not surprising that the prevalence of xerostomia increases with age. A large number of studies have also shown that xerostomia is more common in women than in men. This cannot only be explained by menopause and postmenopause but may be attributed to the fact that women generally have a higher medication intake than men (Smidt et al. 2010). There is a significant variation in the prevalence of xerostomia between studies, which is most likely due to the wide variety of questionnaires used to evaluate prevalence and severity of xerostomia.
In a Danish study of 668 elderly people (age 65–95 years), 12% had xerostomia and 36% of these also had significantly decreased unstimulated whole saliva flow rates, i.e., ≤0.1 ml/min, and 6% had low stimulated whole saliva flow rates, i.e., ≤0.7 ml/min (Smidt et al. 2010). About 5% had both low unstimulated and chewing-stimulated whole saliva secretion. Low minor salivary gland secretion was also found to be associated with a high prevalence of systemic diseases and medication intake, in particular in relation to cardiovascular disease and the pharmacological treatment hereof, including aspirin and statins (Smidt et al. 2010). Overall, there is consensus that xerostomia and decreased saliva secretion in the elderly mainly are associated with the increasing number of systemic diseases and medication intake with age, and not with age and gender per se. In the years to come, the incidence of xerostomia and hyposalivation is expected to increase in line with the higher average life expectancy and thus an associated increase in systemic diseases and concomitant medication intake. However, it should also be emphasized that minor salivary gland secretion plays a major role in the lubrication of the oral mucosa. Thus, age-related degeneration of the minor salivary glands may lead to decreased secretion of mucins, consequently contributing to xerostomia in the elderly, in spite of normal whole saliva flow rates (Eliasson and Carlen 2010).
Diagnostic Workup of Salivary Gland Disorders and Diseases
Salivary gland dysfunction and xerostomia can be a result of local or systemic diseases or disorders, medication intake, or other iatrogenic factors, e.g., an adverse effect of cancer treatment. A diagnostic workup includes examination of subjective symptoms, past and present oral and general medical history, a physical examination of the oral region, head and neck, and assessment of salivary gland function, as well as relevant additional clinical and laboratory tests (e.g., diagnostic imaging such as ultrasound and magnetic resonance imaging (MRI), pathology, serology, ophthalmology).
Subjective Symptoms
Xerostomia is rarely an isolated symptom. Usually, it is elicited by chronic salivary gland hypofunction and accompanied by other oral and systemic complaints. The general complaint and severity of xerostomia are not always related to a decrease in the saliva flow rate. In about a quarter of the patients complaining of moderate to severe xerostomia, the mouth might even appear moist on clinical inspection (Fox et al. 1987). Patients may complain of xerostomia that is present throughout their oral cavity or localized xerostomia, e.g., the lips, cheeks, tongue, palate, floor of the mouth, or throat. Patients may also complain of difficulty with chewing, swallowing, and speaking. Most patients carry bottles of water or other fluids with them at all times to aid speaking and swallowing and for their overall oral comfort. The patients also often have a bottle or glass of water beside their bed. Mild to modest oral pain is common. The mucosa may be sensitive to spicy or coarse foods. This limits the patient’s enjoyment of meals and may compromise their nutritional status (Dormenval et al. 1998; Walls and Steele 2004).
Assessment of Xerostomia
Assessment of xerostomia by patient-reported outcome measures is an important component of the diagnostic workup. A systematic and validated assessment approach will determine the severity of the patient’s subjective feeling of oral dryness and to what extent xerostomia interferes with oral function (chewing, swallowing, and speech) and impacts on quality of life. A systematic assessment will also enable monitoring of disease progression and effect of treatment/efforts to alleviate xerostomia.
Xerostomia can be assessed by a visual analogue scale (100 mm horizontal line ranging from 0 [no xerostomia] to 100 [worst imaginable xerostomia]) addressing oral dryness-related difficulties with speech, chewing, and swallowing; amount of saliva; feeling of dryness of the mouth, throat, tongue, and lips; as well as level of thirst. In addition, standardized, validated questionnaires have been developed for assessment of xerostomia and underlying salivary gland hypofunction. For getting some insight into whether and to what extent xerostomia is present, the following questions can be asked (Fox et al. 1987):
-
1.
Does the amount of saliva in your mouth seem to be too little, too much, or do you not notice it?
-
2.
Do you have any difficulty in swallowing?
-
3.
Does your mouth feel dry when eating a meal?
-
4.
Do you sip liquids to aid in swallowing dry food?
Clinical Manifestations
Most patients with chronic salivary gland hypofunction have obvious signs of mucosal dryness. The buccal mucosa may be atrophic, pale, and corrugated in appearance, and the tongue may be reddish, smooth, and depapillated (Fig. 4). The lips are often atrophic, cracked, and peel off (Fig. 5). There is often a marked increase in erosion of the teeth and dental caries, particularly carious lesions in relation to fillings and decay on root surfaces and even cusp tip involvement (Fig. 6). The decay may progress, even in the presence of thorough oral hygiene. With decreased saliva secretion, there is an increased tendency for accumulations of food debris in the interproximal regions, especially where recession has occurred (Sreebny and Vissink 2010).

Hyposalivation and dry, reddish, depapillated dorsum of the tongue

Hyposalivation and dry, peeling lips with angular cheilitis (Reproduced with permission from Pedersen et al. (2011))

Hyposalivation and dental caries
Due to the reduced saliva flow rate and changed saliva composition, colonization defense is reduced and is accompanied by a higher level of colonization with Candida spp. As a result, patients with salivary gland hypofunction are predisposed to oral fungal infection. Oral candidosis most often presents as erythematous oral candidosis characterized by erythematous patches on the oral mucosa, e.g., dorsum of the tongue, cheeks, palate, or beneath dentures (Fig. 7), or it may appear as white, curd-like mucosal lesions (thrush), i.e., pseudomembranous oral candidosis (Fig. 8). Fungal infection of the corners of the mouth (angular cheilitis) (Fig. 5) is more likely to occur in patients with salivary gland hypofunction who wear dentures and have a posterior bite collapse (Sreebny and Vissink 2010).

Erythematous oral candidosis

Pseudomembranous oral candidosis (Reproduced with permission from Stegenga et al. (2013))
It is important to assess if saliva can be expressed from the main excretory ducts, either by visual inspection of saliva expressed from individual major salivary glands following gland massage from back to front or by bimanual palpation. The expressed saliva should be clear, watery, and copious. Viscous or scant secretions suggest chronically reduced function.
In addition, the secretory capacity of the salivary glands should be assessed. This can easily be done by applying a gustatory or tactile stimulant such as drops of citric acid or chewing gum. If an increase of salivary flow rate is observed, it indicates that it may be worthwhile to prescribe a pharmacologic sialagogue or to use gustatory or tactile stimulants. If no increase in salivary flow rate is observed, frequent moistening of the mouth with water or saliva substitutes is the only option for alleviation (Sreebny and Vissink 2010).
Assessment of Salivary Gland Dysfunction
Saliva flow rate and composition vary widely interindividually and have a diurnal variation. It also varies dependent on type of secretion, i.e., whole saliva or selective gland saliva, and stimulatory state. These variables should be standardized when collecting saliva. For routine collection of saliva, the time of the day for collection is critical, and collection is recommended in the morning hours between 8 am and 11 am. The patient should refrain from eating, drinking, smoking, and oral hygiene measures for at least 60 min before saliva collection to ensure an unstimulated baseline measurement .
Unstimulated Whole Saliva
Unstimulated whole saliva flow rate can be measured by the draining method, the spitting method, the suction method, or the swab technique. They provide virtually similar results; however, the suction and the swab techniques are the least reliable due to slight tactile stimulation of saliva secretion during collection. The draining method (Fig. 9) is the most inert method where whole saliva is allowed to drain passively from the mouth into a collecting device (Navazesh and Christensen 1982). The spitting method is similar, but the accumulated saliva is expectorated periodically into a collecting device. The suction method involves the use of a standard, disposable, plastic dental saliva ejector suction tip. The swab technique is performed by placing pre-weighed cotton rolls or gauze sponges in the mouth and leaving them for a standardized collection time and then reweighing the cotton rolls after the collection period .

Sialometry, unstimulated and stimulated whole saliva (draining method) (Navazesh and Christensen 1982). (a) Sialometry requires a balance with two digits precision, a clock or timer and a plastic cup. (b) The patient sits relaxed in a chair and is instructed to lean the head forward, to keep the mouth slightly open and the eyes open, and to minimize orofacial movements and to avoid swallowing of saliva during the collection process. The procedure should take place in a quiet room, where the patient can sit alone. The unstimulated whole saliva flow rate is measured over a 15 min period. The stimulated whole saliva flow rate is measured over at least a 5 min period, where the patient is stimulated by application of 1–2% citric acid on the lateral margins of the tongue, chewing a piece of sugar-free chewing gum (exerts both gustatory and masticatory stimulation) or 1–2 g of paraffin wax (neutral taste). The patient is chewing with his/her own normal chewing frequency and spitting the saliva into a pre-weighed plastic cup. (c) After the saliva collection, the plastic cup is weighed including the collected saliva, and the weight of the plastic cup is subtracted and divided with the collection time, i.e., 15 min for the unstimulated and 5 min for the stimulated sialometry, respectively. Since 1 g is considered equivalent to 1 ml saliva, the saliva flow rate is given in ml/min (Reproduced with permission from Pedersen et al. (2011))
Stimulated Whole Saliva
Standardized stimulation of salivary glands is either gustatory, with the use of 1–2% citric acid, and/or masticatory, induced by chewing on 1–2 g paraffin wax with melting point 42–44 °C, a piece of gum base, or a piece of crumbled Parafilm (Parafilm M®, Bemis Company Inc., Neenah, Wisconsin, USA). The citric acid can be applied to the lateral margins of the tongue with a cotton swab every 30 s for 5 min. Saliva flow rates using acidic stimulation are generally higher than other stimuli. The stimulated whole saliva accumulated in the mouth is actively spit into the collection device every minute during the collection period (Fig. 9) .
Parotid Saliva
Parotid saliva can be collected selectively from the orifice by a Lashley cup or Carlsson-Crittenden cup. The collection is easily performed by applying the bichambered cup over the orifice of the Stensen duct. The inner chamber covers the duct orifice to collect the saliva and is connected to a graduated test tube or syringe via a plastic tube, while the outer chamber is connected to a suction device to ensure adherence of the cup to the surrounding oral mucosa by vacuum (Fig. 10). Parotid saliva flow rate is low or even absent in the resting state; thus generally parotid saliva is collected under stimulated conditions. Parotid saliva flow rate is usually measured over a 10 min period, where the patient is stimulated by application of 1–2% citric acid on the lateral margins of the tongue with a cotton swab at 30 or 60 s intervals .

Collection of parotid saliva. (a) Lashley cup prepared in metal, (b) Lashley cup prepared in transparent polymethylmethacrylate, ruler unit (centimeter), and (c) the Lashley cup in place over the orifice of the parotid (Stensen’s) duct in the cheek. The cup consists of an inner and outer chamber. The inner chamber serves as the collection chamber and the parotid saliva is clearly visible. The outer chamber is for suction to hold the cup in place on the mucosa
Submandibular/Sublingual Saliva
Mixed submandibular and sublingual gland saliva is usually collected from the floor of the mouth by the suction method, e.g., aspiration of the accumulated saliva with a syringe, pipette, or gentle suction (Fig. 11), while the parotid gland secretion from the Stensen ducts is blocked with either Lashley cups or cotton rolls. The submandibular/sublingual salivary glands contribute about 2/3 of the unstimulated whole saliva. Stimulated submandibular/sublingual saliva is usually measured over a 5 min period, where the patient is stimulated by application of 1–2% citric acid on the lateral margins of the tongue with a cotton swab at 30 or 60 s intervals. Mixing the acid stimulant with the collected saliva should be avoided .

Collection of submandibular/sublingual saliva by gentle suction from the floor of the mouth while the orifices of the parotid glands are blocked by Lashley cups (Reproduced with permission from Stegenga et al. (2013))
Salivary Gland Biopsy
Minor Salivary Glands
Biopsy of minor salivary gland tissue involves removal of glands from the mucosal aspect of the lower lip (Fig. 12). Enough lobules need to be removed to provide adequate tissue for pathological examination. This may be difficult if significant fibrosis has occurred. The technique involves a horizontal or vertical linear incision in the midportion of the mucosal aspect of the lip, through which the lobules will protrude with external digital pressure for removal. A vertical incision may result in only one or two lobules being removed. Similarly a punch biopsy may not provide enough lobules for examination and includes the risk of damaging nerve fibers as the neurons cannot be located and avoided through the incision.

Minor salivary gland biopsy exposing the salivary lobules through a vertical incision on the labial aspect of the lower lip (Image courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)
Major Salivary Glands
Biopsies can be taken from all major salivary glands but are mostly limited to biopsies from the parotid gland to diagnose Sjögren’s syndrome (SS) or lymphomas associated with SS. Parotid gland biopsies have few complications, which include saliva extravasation phenomenon (mucocele) development (which can be prevented by meticulous suturing of the parotid gland capsula) and a temporary change in sensation in the preauricular area, generally recovering within 6 months. The efficacy of parotid biopsy for diagnosis of SS compared with minor salivary gland biopsy is comparable (Pijpe et al. 2007). Open biopsy is not a recommended first-line investigation for parotid gland tumors because of a high risk of facial nerve injury and potential risk for tumor seeding. Consequently, fine needle aspiration cytology (FNAC) and core needle biopsy (CNB) are the diagnostic methods of choice for parotid gland tumors. FNAC is technically simple, safe, fast, and cost-effective but demonstrates relatively low sensitivity in comparison with its high specificity for diagnosing salivary gland tumors. The low sensitivity of FNAC is due to several factors but is primarily due to the difficulty of diagnosing low-grade carcinomas by cellular morphology alone. CNB is a newer technique for diagnosing major salivary gland lesions. Since intact tissue cores can be retrieved using ultrasound-guided CNB, improved specimen adequacy is expected with high sensitivity and specificity as a result .
Diagnostic Salivary Imaging Techniques
Imaging of salivary gland disease is covered in extensive detail in the chapter on “Diagnostic Imaging Principles and Applications in Head and Neck Pathology.”
Sialography
Sialography is the radiographic imaging of the salivary duct system following the retrograde ductal infusion of oil- or water-based iodine contrast fluid (Fig. 13). Sialography has a low morbidity and is well accepted by patients. The main sialographic characteristic of a normal gland is a ductal system without dilations or strictures and without diffuse collections of contrast fluid at the terminal acini. By contrast, the main sialographic characteristic of SS and other inflammatory diseases (the appearance is not specific for SS) is a diffuse collection of contrast fluid at the terminal acini of the ductal tree, so-called sialectasia or sialectasis. Sialographs of metabolic disorders often show enlarged glands with normal (resembling the sialograph of a healthy salivary gland) or rather thin ducts. Sialography is no longer used for detection of salivary gland tumors. Currently, multislice compute tomography (CT), MRI, and salivary gland ultrasonography (US) are used for detecting salivary gland tumors. Moreover, sialography is still in use in Japan to detect SS (it is part of the Japanese criteria (Fujibayashi et al. 2004)), while it is replaced by other functional tests in most other countries (Kalk et al. 2001; Sreebny and Vissink 2010). Moreover, salivary gland US is an emerging technique to diagnose SS, relegating sialography further to the background (Mossel et al. 2017).

Normal right parotid sialogram. Four images from a normal right parotid sialogram, demonstrating a smooth regular main (Stensen’s) duct (arrows) and a fine branching duct pattern within the gland (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)
Salivary Scintigraphy
Salivary scintigraphy is based on the ability of the parotid and submandibular glands to trap the radionuclide isotope technetium-sodium (Tc99m) pertechnetate. This ability is due to the fact that Tc99m replaces the chloride ion in the active sodium/potassium/chloride cotransport pump that is located in the striated ducts of the salivary glands (Hakansson et al. 1994; Klein Hesselink and Links 2015). Scintigraphy employs a gamma scintillation camera. The radioactive isotope is injected intravenously, and its uptake, accumulation, and excretion are photographically recorded. Salivary scintigraphy is used in the diagnostic workup of SS but is not commonly applied for this purpose anymore and, like sialography, probably will be replaced by salivary gland US for this purpose .
Ultrasonography
US may reveal parenchymal inhomogeneity of salivary glands. A characteristic alteration, metaphorically named pepper-and-salt appearance, is used to describe sonographic images of patients with SS (Fig. 14). The hypoechoic areas in the salivary parenchyma are either considered to represent local lymphocytic infiltrates (Takashima et al. 1992) or dilated ducts surrounded by dense lymphocytic infiltrates (Salaffi et al. 2000), but it is still not agreed what these areas represent. US seems to be a valuable tool for detecting salivary gland abnormalities in SS, but the quality of current studies in SS is low and does not yet allow assessment of the likelihood of salivary gland US as a reliable and practical tool in diagnosing SS (Delli et al. 2015; Jousse-Joulin et al. 2016). However, very recent studies indicate that salivary gland US is indeed a valid tool in characterizing patients with SS; specifically, when the ultrasonographic image of the major salivary gland is indicative of SS and the patient also has autoantibodies directed toward SS-A, the patient is very likely to suffer from SS (Mossel et al. 2017).

Ultrasonography of the parotid glands. (a) Normal parotid gland. (b) “Pepper-and-salt appearance,” a characteristic alteration in ultrasonographic images of patients with Sjögren’s syndrome (Images courtesy of Dr Konstantina Delli, University Medical Center Groningen, The Netherlands)
US is also used to facilitate needle aspiration biopsies of masses within the salivary glands as well as to inject botulinum toxin into the major salivary glands of children and elderly with drooling problems (Jongerius et al. 2003) .
Computed Tomography and Magnetic Resonance Imaging
Although CT and MRI can be used to detect salivary gland disorders such as SS, they are mainly used to detect salivary gland tumors. For this purpose, MRI is better suited than CT as it provides better imaging of soft tissues. For more detail on these imaging approaches, refer to the chapter on “Diagnostic Imaging Principles and Applications in Head and Neck Pathology.”
Sialendoscopy
Sialendoscopy allows for endoscopic intraluminal visualization of the ductal system of the major salivary glands and offers mechanisms to diagnose and treat inflammatory and obstructive pathology related to the ductal system (Gallo et al. 2015) .
Serology
Just as saliva can be used as an indicator of systemic disease, tests conducted on serum can be used to confirm or deny the presence of oral disease (Vissink 2010). For example, amylase tests performed on serum can distinguish levels of the enzyme that arise from the pancreas from those which stem from the salivary glands. Elevated salivary gland amylase, amylasemia, may be associated with sialadenitis, from initial gland damage due to radiotherapy and/or SS. Follow-up tests can measure the rate of progress of the disease(s). Tests for serum autoantibodies, especially anti SS-A (anti-Ro) and anti-SS-B (anti-La), might reveal the presence of SS; antibodies against dsDNA suggest the presence of systemic lupus erythematosus (SLE). Analysis of the serum for HbA1c may uncover long-standing undiagnosed, or poorly controlled diabetes mellitus. Testing for thyroid hormones might help explain a case of persisting salivary gland enlargement and xerostomia. For more detail on these tests, refer to the chapters on “Clinical Immunology in Diagnoses of Maxillofacial Disease” and “Laboratory Medicine and Diagnostic Pathology.”
Ophthalmology
Ophthalmologic tests within the dental field are mainly used to assess ocular symptoms related to SS (Meiners et al. 2010). The subjective ocular symptoms are obtained by history taking. With regard to SS, patients need to have a positive response to at least one of the following questions: (1) Have you had daily, persistent, troublesome dry eyes for more than 3 months? (2) Do you have a recurrent sensation of sand or gravel in the eyes? (3) Do you use tear substitutes more than three times a day? (Vitali et al. 2002; Shiboski et al. 2017). To objectively rate the ocular function in patients complaining of xerostomia, the following tests are commonly used. In the Schirmer test, a piece of filter paper is placed laterally on the lower eyelid, which results in wetting due to tear production (Fig. 15). If less than 5 mm of paper is wetted after 5 min, the test result is positive. This test can also be done in the dental office. The other tests are in need of an ophthalmologist as special equipment is needed. In the Rose Bengal test, dye stains devitalized areas of the cornea and conjunctiva, which can be scored using a slit lamp. A Rose Bengal score ≥ 4 according to the van Bijsterveld scoring system is considered abnormal. Lissamine green is currently used instead of Rose Bengal stain, which shows comparable results but is less painful. In 2010, the ocular staining score was introduced (Whitcher et al. 2010). This ocular staining score is a composite score of staining of the surface of the eye with fluorescein and lissamine green. An ocular staining score ≥ 5 equals a Rose Bengal score ≥ 4.

Schirmer test
Salivary Gland Disorders and Diseases
Medication-Induced Salivary Gland Dysfunction and Xerostomia
Across the spectrum of symptomatology related to medication-induced salivary gland dysfunction (MISGD), xerostomia is the best documented (Aliko et al. 2015; Villa et al. 2015, 2016; Wolff et al. 2017). A reduced saliva flow rate is considered the major cause of xerostomia related to MISGD, but xerostomia cannot consistently be attributed to salivary gland dysfunction as most studies on MISGD do not include measurements of actual saliva flow rate (sialometry) or saliva composition (sialochemistry). Thus, the degree of xerostomia and salivary gland hypofunction does not always correlate.
While generally speaking xerostomia is accompanied by a reduced saliva flow rate, an absence of xerostomia does not necessarily indicate that there is adequate saliva secretion. Likewise, hyposalivation does not necessarily mean that the patients feel that their mouth is dry (Sreebny and Vissink 2010). This discrepancy occurs in a quarter to one-third of patients (Vissink et al. 1983). Changes in saliva composition and medications that interfere with the local sensory system or the cognitive functions that lead to xerostomia (e.g., lithium is related to a sensation of thirst which is commonly misinterpreted by patients as xerostomia) may also underlie the sensation of oral dryness. In other words, the association between xerostomia and xerogenic medications is probably a multidimensional phenomenon (see Fig. 16).

Algorithm for diagnosis of systemic diseases/conditions as causes of dry mouth (Reproduced with permission from Sreebny and Vissink (2010))
Xerostomia can be a clinically serious health problem, which may contribute to impaired tolerability and patients’ compliance with the intake of some medications (Aliko et al. 2015). In fact, xerostomia has been found to be the most frequent among oral adverse effects of medications in most studies. A recent systematic review documented that xerostomia was associated with medication use in a dose-dependent manner in just a few studies, while the majority of studies did not correlate actual saliva flow rates with xerostomia. So, dose-escalation studies are needed to clarify the true relation of xerostomia to medication dosage. Finally, the driest mouths are seen in patients using several different medications, e.g., polypharmacy (Fig. 17) (Narhi et al. 1992). Therefore, a careful check whether a patient indeed needs all medications he or she uses might be a favorable approach.

Association between medication intake and whole saliva flow rate (Adapted from Narhi et al. 1992)
Although commonly MISGD goes into remission when the administration of a medication is ceased, this does not always occur spontaneously. Occasionally, if the secretory mechanisms of the gland tissue have been inhibited by medications for a longer period of time, the gland has to be “reactivated” by a systematic gustatory stimulation therapy approach. Moreover, one medication of a particular category can cause xerostomia in one patient and another medication from the same category in another patient. See Table 1 for medications reported to induce xerostomia, salivary gland hypofunction, or sialorrhea (Wolff et al. 2017). So, when the administration of a presumed causative medication cannot be discontinued, substitution of a medication with another with a comparable action is worthwhile (Sreebny and Vissink 2010; Wolff et al. 2017). In case the administration of a medication cannot be changed or ceased at all, prescribing a gustatory (e.g., sugar-free sweets) or mechanical (e.g., chewing gum) stimulation therapy can help the patient. A saliva substitute does not always provide alleviation of the feeling of oral dryness, particularly if the patient still has salivary function left as the saliva substitute may cause a rather sticky feeling and potentially worsen xerostomia (Regelink et al. 1998). The exception is a gel for night use as the patient cannot continue a stimulatory action at night. Finally, medications like pilocarpine and cevimeline can be prescribed, but it is not advised to counteract the adverse effect of a medication with another medication that has adverse effects of its own (Sreebny and Vissink 2010) .
Hypersalivation
Hypersalivation, often also called drooling, is a phenomenon that often causes distress, irrespective of whether it is absolute (too much saliva secretion) or relative (the salivary secretion itself is not increased, but handling of the saliva in the mouth is impeded). Common phenomena are irritation of the corners of the mouth, nausea, a wet pillow on awaking, and wet, dirty clothing. Particularly, the latter is often a distress to individuals themselves as well as their relatives.
Hypersalivation is a normal phenomenon in early childhood (increased basal secretion from the parotid glands) (Blasco and Allaire 1992), particularly when teeth are emerging. In elderly, hypersalivation is often related to orofacial dysfunction, such as incompetence of the lips, but also neurological disorders may be the underlying factor (disturbed sensibility of the oral mucosa or lips, swallowing difficulties). Finally, drooling is a common phenomenon in the multiple disabled.
When measuring the actual saliva flow rate, often saliva secretion is not increased but even decreased. It is often more a saliva handling disturbance than an objectively increased saliva flow rate .
Local Obstructive, Inflammatory, or Reactive Disorders
Sialolithiasis
Sialoliths (salivary calculus/salivary stones) most commonly present in Wharton’s (submandibular) duct in the floor of the mouth causing pain due to pressure in the region of the obstructed gland around meal time. When sufficiently calcified, they may be seen on an intraoral occlusal radiograph, orthopantomogram, or cone-beam computed tomogram (Fig. 18). Uncalcified mucous plugs have the same presentation and if not removed, act as a nidus for sialolith development.

Sialolith. Clinical (a), radiographic (b), gross presentation (c), and histopathology (d) (Image (c) courtesy of Dr Omar Kujan, and image (d) courtesy Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia (Images (a) and (b) reproduced with permission from Stegenga et al. (2013))
Sialoliths vary considerably in size. Radiographs of submitted salivary gland tissue may help determine what to section for histopathological review and examination in order to demonstrate the presence of a sialolith, remembering that sialoliths can occur in glands affected by an unrelated pathological process. When sialoliths are cut in cross-section, they frequently exhibit concentric laminations. Histologically, the ductal epithelium is often compressed and frequently shows squamous, oncocytic, or mucous cell metaplasia.
Lesions associated with the minor salivary glands can be excised with the associated gland. When a sialolith can be palpated in the oral cavity (bimanual palpation), the sialolith often can be removed by an intraoral or sialoendoscopic approach and the affected gland can be left in situ. Otherwise, the associated gland is often removed .
Mucoceles and Ranulas
Mucoceles are common lesions usually presenting as a lump on the mucosa or vermilion of the lower lip but can present at other intraoral sites (Fig. 19). Young persons are more frequently affected, and there is often a history of lip trauma (Bezerra et al. 2016). Duration is variable and often dependent on how much inconvenience the lesion causes. Two histological types of mucoceles occur. The most common is the mucous extravasation cyst on the lower lip and the other is the ranula or mucous retention cyst occurring in the floor of mouth (Ha et al. 2014; Kelloway et al. 2014).

Mucocele involving lower lip appearing as a dome shaped raised fluctuant soft tissue lump (Reproduced with permission from Stegenga et al. (2013))
Self-treatment by puncturing the lesion or incision results in rapid deflation but can be followed by recurrence of the swelling. Removal of the lesion by complete excision without rupture including removal of the associated minor salivary glands is curative (Fig. 20). Damage to the duct of an adjacent gland during removal may result in a new lesion developing. It is prudent to warn the patient of sensory nerve damage (typically paresthesia) or the possible recurrence of the mucocele if another excretory duct is damaged during the excisional biopsy. Macroscopically, a pool of mucin may be visible within the excised mucous extravasation cyst (mucocele) submitted specimen on sectioning. The mucin may exude out during the sectioning process. Frequently, lobules of salivary gland are also submitted separately with the main specimen. Microscopically, a space is frequently encountered partially or completely surrounded by a rim of granulation tissue without an epithelial lining (Fig. 21). If present, part of the duct epithelium may be seen and has often undergone squamous metaplasia. A mixed acute and chronic inflammatory cell infiltrate containing often numerous foamy macrophages is present in the granulation tissue, and if mucin is still present, numerous foamy macrophages can be seen within it. The associated minor salivary glands usually contain a moderately intense chronic inflammatory cell infiltrate but generally maintain their normal architecture .

Surgical removal of mucous extravasation cyst. Mucocele on the lower left lip (a), exposed before excision (b) and removed intact without rupture (c) (Images courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)

Histopathology of mucous extravasation cyst (mucocele) shown in Fig. 20 (Image courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)
An alternative curative approach for treating mucoceles is cryotherapy where deliberate destruction of the mucocele and underlying associated salivary gland tissue results in resolution of the condition (Farah and Savage 2006). Both open and closed cryotherapy approaches have been used for this purpose depending on availability (Figs. 22 and 23). Care should be taken with use of cryotherapy as unjudicial use can cause damage to the underlying structures particularly nerves causing paresthesia. The disadvantage of this approach is that no specimen is available for histopathologic review, so an accurate clinical diagnosis is paramount.

Mucous extravasation cyst (mucocele) on the lower lip (a) treated with cryotherapy (b) (Images courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)

Mucous retention cyst (a) treated with cryotherapy (b) (Images courtesy of Professor Camile Farah, Queensland Oral Medicine & Pathology, Brisbane QLD, Australia)
Mucous retention cysts are treated by removal of the lesion by complete excision without rupture including removal of the associated minor salivary glands. Mucous retention cysts are caused by obstruction of a duct rather than trauma and therefore histopathologically present with an epithelial lined dilated duct. The epithelium is frequently flattened columnar or metaplastic squamous in type. On occasions, it may be columnar with oncocytic change. The surrounding salivary gland tissue often shows acinar atrophy and may demonstrate ductal dilation .
Necrotizing Sialometaplasia
Necrotizing sialometaplasia is a benign, inflammatory disorder of the salivary glands. The etiology is unknown; however, ischemic necrosis of minor salivary gland tissue may be the causative factor, associated with smoking, local trauma, pressure from a denture, local anesthetic injection, local surgical procedures, or an immune response to an unknown allergen. The lesion is usually located in the posterior region of the hard palate. The clinical and histopathologic manifestations of necrotizing sialometaplasia may resemble malignancies (Fig. 24).

(a) Necrotizing sialometaplasia appearing as chronic ulcer in palate (Image courtesy of Dr Omar Kujan, UWA Dental School, Perth WA, Australia). (b) Necrotizing sialometaplasia demonstrating infarcted, necrotic salivary gland acini present at the base of the biopsy. Pseudoepitheliomatous hyperplasia and ducts with squamous metaplasia can be seen at one end of the specimen, and a large excretory duct with squamous metaplasia is in continuity with the overlying epithelium. Necrotic debris is present in several of these ducts. A sparse to moderately intense chronic inflammatory cell infiltrate is present in the connective tissue, but does not extend into the necrotic acini
The characteristic histopathologic features of necrotizing sialometaplasia are a lobular arrangement of salivary tissue with squamous cell metaplasia of the ductal system centrally. Islands of squamous cells can be close to salivary ducts with features of hyperplasia. These features may be useful in distinguishing necrotizing sialometaplasia from squamous cell carcinoma and mucoepidermoid carcinoma. Necrotic acini and inflammatory cells are present at the periphery. The inflammatory infiltrate is diffuse and mixed with lymphocytes, plasma cells, neutrophils, occasional eosinophils, and macrophages. Necrotizing sialometaplasia is self-limiting and typically resolves within 3–10 weeks. Symptomatic treatment is usually adequate, e.g., analgesics combined with 0.12% chlorhexidine gluconate mouthwash. Surgical intervention is usually not required .
Salivary Gland Tumors
Salivary gland tumors are a heterogeneous group of neoplasms, knowledge of which has been evolving over many years. This is reflected in the number of changes to the classification of these lesions. It is beyond the scope of this chapter to discuss all salivary gland tumors in detail (see Table 2), but several common neoplasms are discussed. More detailed information about classification of salivary gland tumors can be obtained from other excellent resources (WHO Classification of Head and Neck Tumours 2017) . Staging applies to carcinomas of the major salivary glands (Table 3). Tumors arising in minor salivary glands are not included in the staging classification, but instead at their anatomic site of origin, e.g. the lip. There should be histological confirmation of the disease.
Benign Tumors
Pleomorphic Adenoma
Pleomorphic adenoma is the most common benign neoplasm (including both benign and malignant) in both the major and minor salivary glands (Fig. 25). Pleomorphic adenomas usually present as a slow-growing painless mass, occuring over a wide age range, and have a female predominance (Fig. 26). (Buchner et al. 2007). There is often a delay of some years before medical attention is sought. Thus, while most parotid tumors are 2–6 cm in diameter, giant lesions have been reported in the literature (Perumal et al. 2012; Tarsitano et al. 2015).

Pleomorphic adenoma: ultrasound (a) and ultrasound-guided FNA (b) of a well-circumscribed rounded mass in the right submandibular salivary gland. This lesion is rounded and slightly distorts the contour of the gland, consistent with a true neoplasm, which proved to be a pleomorphic adenoma (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)

Pleomorphic adenoma. Soft tissue lump involving the posterior left soft palate in a 46-year-old female (a). The lesion was raised and covered with normal surface mucosa. The patient reported that the lesion had been present for up to 1 year. The lesion was excised completely under local anesthesia (b). Histopathological sections show a salivary gland tumor composed predominantly of epithelial and myoepithelial cells with numerous duct-like structures in a number of regions at low magnification (c). The stroma consists predominantly of hyalinized connective tissue and myxoid areas on higher magnification (d) (Images courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)
Pleomorphic adenoma is extremely variable in the range of histopathological appearances seen (Fig. 26). The essential elements are both epithelial and myoepithelial cells, ductal structures, and mesenchymal stroma. The proportion of epithelial/myoepithelial cell component compared with the stroma leads to the terminology cell-rich or stroma-rich, with the latter being more prone to recurrence and more common in the parotid gland rather than the minor salivary glands. Encapsulation is highly variable but when present is useful in determining that the lesion is benign. Diagnosis is straightforward when a completely excised lesion with a range of epithelial and stromal features is examined but can be difficult when small incisional biopsies or fine needle aspirates are submitted for examination as they may not be representative of the entire lesion.
Excision of intraoral lesions with a clear margin is curative. The recurrence rate is very low even if margins are not definitively clear. Parotid lesions are however associated with a significant recurrence rate related to enucleation with rupture and incomplete tumor excision at operation. Extracapsular extension may also be associated with recurrence. Malignant transformation may occur in long-standing lesions, often associated with accelerated growth after a lengthy period of slow growth. Pain, facial nerve palsy and skin fixation may also occur (Quer et al. 2017; Machado et al. 2017) .
Warthin Tumor
Warthin tumor is the second most common salivary gland neoplasm. It almost exclusively involves the parotid glands presenting as a painless slow-growing lump. It is frequently located in the inferior pole of the parotid gland and presents with a mass in the upper part of the neck near the angle of the mandible (Patel and Morton 2016). It may be clinically indistinguishable from an enlarged lymph node of the upper neck. The mass is generally non-tender, mobile, and well circumscribed. Ultrasound will often show a partially cystic mass, and fine needle aspiration cytology (FNAC) is usually diagnostic (Fig. 27).

Warthin tumors: coronal PET image (a) performed for surveillance of treated lymphoma in a 71-year-old man showing two incidental right parotid FDG-avid tumors (arrows); US-guided FNA (b) confirmed Warthin tumor in both lesions. This tumor is frequently multifocal and/or bilateral. FDG uptake is not specific for malignancy and can be seen in benign tumors and inflammatory lesions (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)
Warthin tumor is characterized histopathologically by the presence of papillary epithelial projections into cyst-like spaces containing eosinophilic secretions and a lymphoid stroma (Fig. 28). A more solid growth pattern with smaller cystic spaces and less stroma or a multifocal growth pattern may be encountered. Superficial parotidectomy and enucleation are the primary treatment modalities. Malignant transformation of either epithelial (e.g., squamous, adenocarcinoma, mucoepidermoid, oncocytic) or lymphoid components (nodal or MALT-type neoplasms) has been reported (Bunker and Locker 1989; Skalova et al. 1994; Nagao et al. 1998; Williamson et al. 2000; Foschini et al. 2005; Arcega et al. 2015).

Warthin tumor characterized histopathologically by the presence of papillary epithelial projections into cyst-like spaces containing eosinophilic secretions and a lymphoid stroma. This parotid tumor appears thinly encapsulated, and the capsule appears intact (a). The tumor is composed of cystic spaces containing eosinophilic proteinaceous material lined by dual layered oncocytic epithelium interspersed with large lymphoid follicles with prominent germinal centers (b and c) (Images courtesy of Drs David Paton, Benjamin Wood and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Basal Cell Adenoma
Basal cell adenoma can have four different growth patterns: solid, trabecular, tubular, and membranous. Basal cell adenomas make up 1–3.7% of all salivary gland tumors (Ethunandan et al. 2002), and more than 80% occur in the parotid gland, followed by the submandibular gland and only rarely in the minor glands (Wilson and Robinson 2015). The lesion is typically a well defined and moveable solitary mass. The tumor is usually a well-circumscribed encapsulated mass measuring 0.2–5.5 cm (Wilson and Robinson 2015). The solid type may resemble cutaneous basal cell carcinoma with solid nests of basaloid cells with a peripheral palisading layer of cuboidal/columnar cells (Fig. 29). The trabecular type consists of basaloid cells arranged as strands and cords, varying in thickness, but frequently thin and narrow. The tubular type has strands of basaloid cells but has numerous duct lumina lined by cuboidal cells and frequently both trabecular and tubular types. The membraneous type consists of multiple islands and nests of basaloid cells with palisading of the peripheral cells .


Basal cell adenoma. The tumor is composed predominantly of basaloid cells with rounded or oval nuclei, eosinophilic cytoplasm, and indistinct cell borders (a). Toward the periphery the stroma is somewhat less dense and more myxoid. A lymphoplasmacytic infiltrate is noted, particularly at the edge of the tumor. The basaloid cells are mostly arranged in a glandular and trabecular pattern with cells showing predominantly ovoid to spindled nuclei and pale cytoplasm arranged in anastomosing cords and nests, separated by loose or more densely hyalinized connective tissue (b). The gland lumina contain thick densely eosinophilic secretions. In some areas neoplastic cells are more closely packed and spindled in outline but show no marked pleomorphism, and mitotic activity is not observed. Neoplastic cells show positivity by immunohistochemistry for CK7 (c), P63 (d), and bcl2 (e) (Images courtesy of Drs Kate Francis, Anitha Thomas, Jennet Harvey and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Myoepithelioma
Myoepitheliomas are an uncommon salivary gland tumor representing 1–1.5% of all salivary gland tumors. Of benign neoplasms they account for 2.2% of major gland lesions and 5.7% of minor salivary gland lesions (Sciubba and Brannon 1982; Dardick et al. 1989; Alos et al. 1996). Lesions usually present as a slow-growing painless mass (Simpson et al. 1995; Alos et al. 1996). Myoepitheliomas are usually encapsulated and have a combination of morphological types, although one cell type usually predominates. Spindle, plasmacytoid, hyaline, epithelioid, or clear cells therefore may predominate (Fig. 30). The growth pattern may be solid, myxoid, or reticular in a uniform pattern. The reticular pattern consists of a netlike arrangement of cell cords (Dardick et al. 1992). Recurrences are infrequent and are generally associated with incomplete removal (Sciubba and Brannon 1982).


Myoepithelioma. The macroscopically detected nodules show similar lesional cells with variable cellularity and variable amount of cytoplasm and intra-lesional collagen (a). The lesional cells are arranged in swirls and fascicles (b). They have oval to spindled nuclei with eosinophilic cytoplasm and inconspicuous cytoplasmic borders. Occasional cells with clear cytoplasm are also present. Mitotic figures, necrosis, and pleomorphism are not seen. Focally toward the edge, an area of myxoid change with ducts lined by flattened epithelium containing eosinophilic material is also seen. The tumor cells stain positively with S100 (c) and smooth muscle actin (d) (Images courtesy of Drs Sooraj Pillai, Ramela Rajakaruna and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Oncocytoma
Oncocytomas account for 2% of all salivary gland tumors occurring predominantly in the sixth to eighth decade with equal sex distribution, although clear cell oncocytoma is much more prevalent in women. The lesion is most commonly found in the parotid (Fig. 31). Submandibular and minor gland tumors also occur (Thompson et al. 1996). Presentation is usually a unilateral painless swelling. Oncocytomas are well-circumscribed tumors composed of oncocytes with eosinophilic granular cytoplasm and centrally located vesicular nuclei and a single prominent nucleolus. The arrangement of the oncocytes is in sheets, nests, trabeculae, and duct-like patterns with an intervening fibrovascular stroma. Cyst-like structures may be seen. The clear cell oncocytoma consists of cells with clear cytoplasm and must be distinguished from other clear cell salivary gland tumors which are malignant. Immunohistochemistry may be helpful in diagnosis with expression of p63 and CK5/CK6 (McHugh et al. 2007). Recurrence is rare following surgical excision .

Oncocytoma composed of oncocytes with eosinophilic granular cytoplasm and centrally located vesicular nuclei and a single prominent nucleolus (Image courtesy of Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Lymphadenoma
Lymphadenoma is a rare benign salivary gland tumor occurring over a wide age range between 11 and 79 years (Seethala et al. 2012) with equal sex predilection. Eighty percent of cases occur in the parotid and two forms exist, sebaceous and non-sebaceous with the latter accounting for a third of cases and occurring at a younger age (Seethala et al. 2012; Liu et al. 2014). Lesions are encapsulated and may be solid or multicystic and are composed of anastomosing cords and nests of basaloid cells and tubuloglandular structures. Reactive lymphoid follicles with germinal centers are present throughout. Sebaceous differentiation is seen in the sebaceous type, and rupture with release of sebum leads to a foreign body giant cell reaction (Seethala et al. 2012). Complete resection is curative, although malignant transformation of the sebaceous cells (sebaceous lymphadenocarcinoma) or basal cells (basal cell adenocarcinoma) has been reported with remnants of benign lymphadenoma seen in lymphadenocarcinoma (Croitoru et al. 2003) .
Cystadenoma
Cystadenomas account for 4% of salivary gland tumors, occur in the fifth to seventh decades, and are more common in females (Tjioe 2015). Forty-five to fifty percent occur in the parotid, and the minor glands are next most frequently involved (lips, buccal mucosa) (Tijoe 2015). Presentation is a slow-growing mass, which may contain mucin and therefore clinically thought to be a mucocele. They are usually multicystic with papillary projections lined by columnar and/or cuboidal epithelial cells often with oncocytic differentiation, which may predominate. Mucous and squamous epithelial cells may be seen, and eosinophic material may be present in lumina with foamy macrophages evident. Cellular atypia, mitoses, or an aggressive growth pattern is not seen. Recurrence following complete conservative local excision is rare .
Sialadenoma Papilliferum
Sialadenoma papilliferum is a benign tumor most commonly affecting males over 50 years of age but has been reported in younger individuals (Mahajan et al. 2007). Intraoral sites including the hard palate and buccal mucosa are the most common sites of occurrence (Fantasia et al. 1986; Kubota et al. 2012; Ubaidat et al. 2001). The lesion presents with an exophytic papillary configuration frequently thought clinically to be squamous papilloma. Papillary projections are lined by squamous epithelium with parakeratosis and acanthosis. Ductal structures are lined by cuboidal luminal cells and abluminal flattened myoepithelial cells. Immunohistochemistry shows positive expression for high molecular weight cytokeratins CK 13 and 14 and myoepithelial markers SMA, S100, and GFAP (Maiorano 1996). This benign lesion is managed by surgical excision, and recurrences are rare (Pimentel et al. 1995) .
Ductal Papillomas
Both intraductal and inverted ductal papillomas occur and are rare occurring mainly in adults with sexes affected evenly (Fig. 32). Lesions have been reported in children (Noseri et al. 2007). Lesions occur in both the minor and major salivary glands presenting as a painless submucosal nodule. Intraductal papillomas are typically well circumscribed with epithelial cells and mucous cells forming broad luminal papillary projections. Inverted ductal papillomas present with an endophytic squamous cell proliferation composed of sheets of epithelial cells, and a crypt may communicate with the surface epithelium (Brannon and Sciubba 2001). Complete excision is curative.

Soft tissue lump presenting on the labial surface of the lower lip (a). Histopathology confirms the presence of an inverted papilloma (b) (Images courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)
Sebaceous Adenoma
Sebaceous adenomas are very rare, comprising less than 0.1% of all salivary gland neoplasms with about half in the parotid, followed by the minor glands and submandibular gland (Apple 2009; Gnepp 2012; Zare-Mahmoodabadi et al. 2009). Lesions are typically well circumscribed and composed of sheets and nests of sebaceous cells interspersed with fibrous connective tissue stroma. Duct-like spaces may be present. Both squamous differentiation and oncocytic metaplasia may be seen. Complete excision is curative.
Canalicular Adenoma and Other Ductal Adenomas
These benign neoplasms are composed of epithelial ductal cells arranged in anastomosing cords within a fibrous connective tissue stroma. Lesions rarely occur before the age of 50 years and men are more frequently affected (Buchner et al. 2007; Thompson et al. 2015). It accounts for up to 12% of salivary gland neoplasms (Buchner et al. 2007; Pires 2007; Waldron et al. 1988; Yih et al. 2005). In a large series of neoplasms from China, no canalicular adenomas were found in the minor glands (Wang et al. 2007; Wang et al. 2015). Canalicular adenoma most commonly involves the upper lip (Thompson et al. 2015). Lesions typically present as a painless mass. Lesions are well circumscribed and may contain multiple nodules. The tumor cells are columnar or cuboidal epithelial cells arranged as anastomosing, branching, or budding parallel cords. Cellular atypia is absent and mitotic figures rare. Complete excision is curative.
Malignant Tumors
Polymorphous Adenocarcinoma
Formerly known as polymorphous low-grade adenocarcinoma, the name has changed in the 2017 World Health Organization (WHO) classification of salivary gland tumors. The most common site of polymorphous adenocarcinoma is the palate, and this occurs in the hard palate more frequently than soft palate (Fig. 33), followed by lips, buccal mucosa, alveolar mucosa, and other intraoral sites (Aberle et al. 1985; Frierson et al. 1985; Kimple et al. 2014; Castle et al. 1999). Polymorphous adenocarcinoma is characterized by an infiltrative growth pattern, cellular organizational diversity, relative histologic blandness, and cytologic uniformity. The tumor cells are generally small and uniform, with slightly hyperchromatic nuclei, inconspicuous to slightly enlarged nucleoli, and scant to moderately abundant, clear to eosinophilic cytoplasm. Mitoses are generally infrequent. The lesion is usually nonencapsulated but may be circumscribed; however foci of infiltrative growth (which may take multiple sections to find) occur in almost all cases. Tumors that commonly invade adjacent soft tissue including salivary gland lobules may infiltrate the adjacent bone, and perineural involvement is a common finding as it is for adenoid cystic carcinoma. Diagnostic difficulty may arise in small biopsy samples where a cellular pleomorphic adenoma or adenoid cystic carcinoma may be considered. Excision with clear margins is considered the treatment of choice. Radiotherapy may play a role in local control in selected cases (Uemaetomari et al. 2007; Patel et al. 2015).

(a) Polymorphous adenocarcinoma (formerly known as polymorphous low-grade adenocarcinoma) presenting as a hard raised multilobulated lump on the hard palate in a 65-year-old female patient (Image courtesy of Professor Camile Farah, Queensland Oral Medicine & Pathology, Brisbane QLD, Australia). (b) Polymorphous adenocarcinoma is characterized by an infiltrative growth pattern, cellular organizational diversity, relative histologic blandness, and cytologic uniformity. (c) Polymorphous adenocarcinoma. The tumor cells are generally small and uniform, with slightly hyperchromatic nuclei, inconspicuous to slightly enlarged nucleoli, and scant to moderately abundant, clear to eosinophilic cytoplasm
Mucoepidermoid Carcinoma
Mucoepidermoid carcinoma, a malignant salivary gland tumor, occurs over a wide age range and is the most frequently encountered malignant salivary gland tumor in the young. It generally presents as a slow-growing mass but if cystic may resemble a mucocele, with mucin released if rupture occurs. The lesion is usually nonencapsulated and composed of a mixture of mucous, intermediate, and epidermoid cells (essential for diagnosis) and varying numbers of clear cells, columnar cells, and oncocytes. The cells invade the surrounding stroma producing solid areas and duct or cyst-like areas in varying proportions. Inflammation and fibrosis are common and perineural invasion may be present (Fig. 34). The presence of mucin can best be demonstrated by mucicarmine or Alcian blue staining. The clear cells are diastase-sensitive periodic acid-Schiff (PAS) positive indicating the presence of glycogen. Excision with clear margins is considered the treatment of choice. Radiotherapy may play a role in local control in selected cases (Chen et al. 2013) .

Mucoepidermoid carcinoma. Sections show parotid parenchyma with a mucoepidermoid carcinoma, occupying predominantly the inferior half of the gland (a). The tumor is composed of numerous mucin-filled cysts of varying shape and size and cribriform structures set within dense desmoplastic stroma (b). The cystic spaces are lined by a combination of mucocytes, intermediate cells, and epidermoid cells (c). The mucous cells contain pale cytoplasm and peripherally displaced nuclei. The epidermoid cells are polygonal with central, mildly pleomorphic nuclei and abundant cytoplasm, but no definite keratinization (d). In the surrounding stroma, there is extensive sclerosis and a prominent peritumoral inflammatory infiltrate composed of lymphocytes and plasma cells, with small lymphoid aggregates containing reactive germinal centers (e) (Images courtesy of Drs Nithya Menon and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Adenoid Cystic Carcinoma
Adenoid cystic carcinoma is a slow-growing but relentless malignant salivary gland neoplasm (Fig. 35). Females are affected more commonly and the median age is 57 years with no ethnic predilection (Boukheris et al. 2009). Presentation is a mass and neurological signs or symptoms may be evident. The major glands are involved more frequently than minor glands or other sites including the sinonasal tract (Figs. 36 and 37) (Boukheris et al. 2009; Ellington et al. 2012). The WHO classification separates adenoid cystic carcinoma into three microscopic patterns: cribriform (glandular), tubular, and solid with the cribriform being the most frequent and the solid the least frequent pattern observed (Figs. 38 and 39). Adenoid cystic carcinoma is composed of cells of two types: ductal cells and abluminal myoepithelial cells. Cytologically, adenoid cystic carcinoma is composed of a uniform, bland population of cells with oval basophilic nuclei with homogeneous chromatin distribution usually with little cytoplasm, similar to basal cell carcinoma of the skin. The nuclei are frequently angulated (WHO Classification of Head and Neck Tumours 2017). Wide excision with clear margins is considered the treatment of choice. Treatment of recurrent or metastatic disease by radiotherapy with or without chemotherapy has shown limited success. Radiotherapy, however, has been shown to improve local control in cases with microscopic residual disease .

Adenoid cystic carcinoma presenting as a discrete palatal lump in a female patient with no surface changes (Image courtesy of Professor Camile Farah, Queensland Oral Medicine & Pathology, Brisbane QLD, Australia)

Adenoid cystic carcinoma submandibular gland. Ultrasound (a) and axial post-contrast CT (b) in a 68-year-old woman presenting with a left submandibular mass (arrows). Although well circumscribed, with no aggressive features on imaging, this proved to be an adenoid cystic carcinoma on histopathology (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)

Adenoid cystic carcinoma arising as a lump involving the right hard palate in a 38-year-old female (a). CT shows permeation of the alveolar bone of the right maxilla surrounding the roots 16 and partial resorption of the cortex of the floor of the right maxillary antrum with mild mucosal thickening of the right antral floor (b). MR shows marked palatal soft tissue thickening which extends into submucosa of the right side of the hard palate just across the midline (c) and diffuse infiltration of marrow of the right hemi-maxilla extending from the maxillary tuberosity to the midline (d) (Images courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)

Histopathology of adenoid cystic carcinoma shown in Fig. 37. Adenoid cystic carcinoma showing tubular and focally cribriform growth patterns (a) composed of uniform bland cells with oval basophilic nuclei (b). By immunohistochemistry, the abluminal cells are positive for p63 (c), and both abluminal and luminal components are positive for SOX10 (d). MYB FISH analysis with Zytovision Zytolight SPEC MYB Dual color break-apart probe (e). Only one cell is in the right focal plane with complete break-apart signal (1 yellow, 1 red, 1 green; arrow) (Images courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia, and IGENZ Ltd., Auckland, New Zealand (image e))

Adenoid cystic carcinoma. This section shows a grade 3 adenoid cystic carcinoma composed of mainly cribriform glands but with at least 40% solid component and a minor tubular component. The stroma ranges from myxohyaline to dense hyalinized fibrosis. Small foci of tumor necrosis are observed within the solid tumor islands (a and b). By immunohistochemistry, the tumor is diffusely positive for MNF116 (c) and CK7 (d) (Images courtesy of Drs Jia Chu, Benhur Amanuel and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Acinic Cell Carcinoma
Acinic cell carcinoma occurs over a wide age range with most cases occurring in patients over 60 years and is more frequent in females. The parotid gland is mostly commonly involved (Fig. 40). Presentation is usually a slow-growing mass, usually not fixed to the overlying skin. Pain occurs in some patients and facial nerve involvement may result in facial paralysis. Acinic cell carcinoma presents a number of diagnostic difficulties. There are five cell types (Ellis and Corio 1983): acinar cells are similar to normal serous acinar cells containing PAS-positive diastase-resistant (PAS-D) zymogen granules, vacuolated cells with clear cytoplasmic vacuoles, clear cells with clear PAS-negative cytoplasm, nonspecific glandular cells and intercalated duct type cells, which are smaller with less, usually eosinophilic cytoplasm and central nuclei. These cells surround luminal spaces of varying sizes (Fig. 41).

Acinic cell carcinoma: malignant parotid neoplasm without aggressive imaging appearance. A 29-year-old woman presented with a right parotid mass. Ultrasound (a) shows a well-circumscribed mass with which it is predominantly solid but hypoechoic with posterior acoustic enhancement. An axial T2-weighted fat-saturated MRI image shows the mass in the superficial lobe in the right parotid gland (arrow in (b)), appearing hyperintense and well circumscribed. Although there are no aggressive features and the imaging could be consistent with pleomorphic adenoma, this proved to be acinic cell carcinoma on histopathology (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)

Acinic cell carcinoma. Sections show parotid salivary gland with an acinar cell carcinoma (a). The lesional cells are large and polygonal, arranged in acinar formations (b). The nuclei are round and eccentric and surrounded by abundant granular cytoplasm. The acinic cell granules are highlighted with PAS-D (c) (Images courtesy of Drs Celia Green, Nathan Harvey and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
There is wide variation in the histomorphologic configurations seen including solid, microcystic, papillary-cystic, and follicular (Ellis and Corio 1983). The microcystic pattern, which is the most common, contains small spaces in the tumor giving it a lattice-like appearance. Acinic cells and vacuolated and intercalated type cells are common. In the solid type, the cells are closely aggregated in sheets or nodules. Acinic cells are common, but nonspecific glandular and clear cells may also be seen. In the papillary-cystic variant, the cysts are usually prominent and show intraluminal papillary projections. The follicular variant consists of multiple, variably sized cystic spaces lined mostly by intercalated duct-type cells and contains homogeneous, eosinophilic, proteinaceous fluid resembling follicular thyroid carcinoma. Surgical excision is considered the treatment of choice. Radiotherapy may play a role in selected cases (Andreoli et al. 2012).
Clear Cell Carcinoma
Clear cell carcinoma occurs most frequently intraorally presenting as a mass. They are poorly circumscribed and infiltrative and consist of sheets, nests, cords, trabeculae, or single-cell growth patterns of polygonal cells with lightly eosinophilic to clear cytoplasm (Milchgrub et al. 1994). Intracytoplasmic glycogen is PAS positive and diastase sensitive and may also demonstrate mucicarmine-positive staining. The tumor cells are positive for cytokeratins and p63 but negative for other myoepithelial markers (Lai et al. 2008).
Basal Cell Adenocarcinoma
Basal cell adenocarcinoma is a rare malignancy usually involving the parotid gland with no sex predilection and occurs most frequently in the sixth or seventh decades (Ellis and Wiscovitch 1990). The tumors are unencapsulated with solid, tubular, trabecular, and membranous growth patterns. Typically the cells show peripheral palisading of the basal cells and variable deposition of basement membrane-like material. Perineural or perivascular invasion may be found .
Intraductal Carcinoma
These are very rare with little epidemiological data. The parotid is most commonly affected (Delgado et al. 1996; Brandwein-Gensler et al. 2004; Kuo et al. 2013). Lesions are unencapsulated and show cystic spaces macroscopically (Delgado et al. 1996; Brandwein-Gensler et al. 2004). Lesions can be graded on the basis of cytological features as low, intermediate or high grade. Low-grade tumors are predominantly cystic with cribriform and papillary patterns (Delgado et al. 1996; Brandwein-Gensler et al. 2004). The tumor cells may show apocrine differentiation with nuclear pleomorphism, hyperchromatism, and frequent mitoses particularly in the intermediate- and high-grade lesions where necrosis may also be found .
Adenocarcinoma, Not Otherwise Specified (NOS)
Approximately 10–15% of salivary gland carcinomas are adenocarcinoma NOS (Spiro et al. 1982; Waldron et al. 1988; Bjorndal et al. 2011). There is a wide age range, but they are rare in children. Over 50% arise in the parotid, but the majority of the rest involve the palate, buccal mucosa, and lips (Waldron et al. 1988; Foss et al. 1996; Wang et al. 2007). The usual clinical presentation is an asymptomatic mass although occasionally they are painful at presentation. The tumor may be partially circumscribed with an infiltrative appearance. The lesion shows ductal or glandular differentiation and may have cyst formation. The cells in the tumor may be cuboidal, columnar, polygonal, clear, mucinous, oncocytoid, or plasmacytoid with a range of growth patterns including nest cords or large islands. Grading (low, intermediate, or high) is based on cellular atypia. Ductal and glandular structures are more prevalent in the low- and intermediate-grade lesions. In order to make the diagnosis, the more common subtypes of malignant salivary gland carcinomas must first be excluded and immunohistochemistry may be useful (Nikitakis et al. 2004) .
Secretory Carcinoma (Mammary Analogue Secretory Carcinoma)
Secretory carcinoma is morphologically similar to mammary analogue secretory carcinoma and is generally a low-grade malignancy of salivary glands, predominantly parotid (70%), but also of the oral cavity (20%) (lip, soft palate, buccal mucosa) (Bishop 2013). The entity was first described in 2010 (Skalova et al. 2010). The tumor, which generally presents as a painless slow-growing mass, generally occurs in adults (mean age 47 years) and more frequently in males (Chiosea, Griffith et al. 2012; Bishop 2013). Macroscopically lesions are generally poorly defined and microscopically may be circumscribed but are frequently infiltrative. Perineural invasion may be seen, but lymphovascular invasion is not. Growth patterns include microcystic, follicular, papillary, and solid. The cells have apocrine features with eosinophilic granular cytoplasm, a large nucleus with prominent nucleoli. Eosinophilic secretions can be seen within the glandular spaces. The secretory material stains positively for PAS with and without diastase digestion and for Alcian blue (Fig. 42). The cells of secretory carcinoma lack PAS-positive secretory zymogen granules. These features are useful in excluding other salivary gland tumors including acinic cell carcinoma, low-grade cribriform cystadenocarcinoma, cystadenocarcinoma NOS, and low-grade mucoepidermoid carcinoma (Skalova 2013). Treatment is generally wide surgical excision with good success rates. Need for post-operative radiotherapy is equivocal. Fluorescence in situ hybridization (FISH) for ETV6 rearrangement is required for definitive diagnosis (Majewska et al. 2015).

Secretory carcinoma (mammary analogue secretory carcinoma). Sections show secretory carcinoma of the parotid salivary gland (a). The cells have apocrine features with eosinophilic granular cytoplasm, large nuclei with prominent nucleoli. Eosinophilc secretions can be seen within the glandular spaces (b). The secretory material stains positively for PAS-D (Images courtesy of Drs Greg Sterrett and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Epithelial-Myoepithelial Carcinoma
Epithelial-myoepithelial carcinoma is uncommon, representing less than 5% of salivary gland malignancies (Vazquez, Patel et al. 2015) predominantly presenting as a slow-growing lump in the parotid and submandibular glands. It occurs predominantly in the sixth and seventh decades and has a slight female predilection. It often has a multinodular appearance and is characterized by a biphasic appearance consisting of small inner luminal ductal cells and abluminal polygonal myoepithelial cells with clear cytoplasm in contrast to the dense eosinophilic cytoplasm of the luminal cells (Fig. 43) (Fonseca and Soares 1993; Seethala et al. 2007). Necrosis may be seen and perineural invasion is common and vascular invasion less so (Fonseca and Soares 1993; Seethala et al. 2007). The abluminal cells stain with myoepithelial markers, e.g., SMA, HHF35, p63, and calponin (Seethala et al. 2007) .

Epithelial-myoepithelial carcinoma. Sections show salivary gland tissue with a central fairly encapsulated, cystic, and solid neoplasm (a). The solid areas show bi-layered duct-like structures composed of an inner layer of single row of cuboidal cells with eosinophilic cytoplasm and central or basal round nuclei (b). The outer or abluminal layer shows single or multiple layers of polygonal cells. The clear abluminal cells have central to eccentric larger irregular nuclei showing some variation in size and shape and small nucleoli. The cystic areas are lined by single layer of columnar cells and some contain luminal blood. Immunohistochemical staining shows the epithelial cells to be strongly positive for the broad-spectrum cytokeratin MNF-116 (c). The abluminal myoepithelial cells are strongly positive for S100 (d) and CK5/CK6 (e) (Images courtesy of Drs Jason Dyke, Anitha Thomas and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Carcinoma ex Pleomorphic Adenoma
By definition carcinoma ex pleomorphic adenoma is an epithelial and/or myoepithelial malignancy arising in a primary or recurrent pleomorphic adenoma (McNamara et al. 2009). It is more common in females, and peak incidence is approximately 10 years later than the peak incidence of pleomorphic adenoma and most commonly presenting as a rapidly growing parotid mass (Fig. 44). Usually part of the benign preexisting lesion can be seen macroscopically. A variety of appearances can be seen microscopically due to the variety of appearances seen in pleomorphic adenoma and the type of malignancy which has developed (Fonseca and Soares 1993; Griffith et al. 2014). The malignant component is most frequently high-grade adenocarcinoma of salivary duct carcinoma phenotype, but in a number of cases, a low-grade myoepithelial phenotype is encountered (Fig. 44). Intracapsular carcinomas, which is a high-grade ductal lesion, may be seen (Altemani et al. 2005). Assessing extracapsular involvement may be difficult due to incomplete removal with positive margins or within multinodular or recurrent pleomorphic adenoma (Griffith et al. 2014) .

Recurrent carcinoma ex pleomorphic adenoma. Axial T1-weighted MRI (a) and coronal post-gadolinium T1 fat-saturated MRI (b) showing an aggressive mass (arrows) arising in the left parotid bed, 13 years after previous resection of a carcinoma ex pleomorphic adenoma. The coronal image shows that the tumor extends intracranially, focally invading the left sigmoid venous sinus (dotted arrow in b) (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia). (c) Carcinoma ex pleomorphic adenoma. Sections show a multinodular myoepithelial proliferation associated with varying amounts of stroma. Much of the tumor is surrounded by fibrous pseudocapsule though some nodules lie outside the capsule within fat and infiltrate with a pushing margin (c). The tumor displays a variety of growth patterns including solid sheets and large islands with a peripheral festooning and trabecular growth patterns and abundant central myxohyaline stroma (d). The cells are also arranged in narrow anastomosing cords and reticular patterns, and there are large pools of myxoid stromal material. The cytomorphology varies from predominantly small epithelioid cells with pale eosinophilic or clear cytoplasm to minor foci of plasmacytoid hyaline cells and spindle cells (Images courtesy of Dr Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Sebaceous Adenocarcinoma
Sebaceous adenocarcinoma is a rare malignant salivary gland tumor occurring over a wide age range (6–93 years) with peak incidences in the third decade and in the sixth and seventh decades and equal male/female ratio (Altemani et al. 2008; Takada et al. 2015). About fifty cases have been reported (Altemani, Vargas et al. 2008; Gnepp 2012; Manteghi et al. 2014; Takada et al. 2015; Wang et al. 2015). The tumors are often well circumscribed and are composed of nests and sheets of tumor cells with hyperchromatic nuclei, clear vacuolated to eosinophilic cytoplasm, and variable cellular pleomorphism. Tumor necrosis is common, perineural invasion infrequent (20%), and vascular invasion rare. There is positive staining with EMA, CA15–3, androgen receptor, and anti-adipophilin and negative with BerEP4 (Ansai et al. 2011) .
Carcinosarcoma
Carcinosarcoma is a biphasic malignant neoplasm with both carcinomatous and sarcomatoid components. It is a very rare malignancy most commonly affecting the parotid, followed by the submandibular gland. Of the minor salivary glands, the palate is most commonly affected. A reasonably high proportion of lesions arises as carcinoma ex pleomorphic adenoma. A rapidly growing mass is often the presenting complaint, and macroscopically a large fleshy mass with hemorrhage and necrosis may be seen. The microscopic features show a lesion composed often of poorly differentiated carcinoma or adenocarcinoma and a high-grade sarcomatoid component with chondrosarcoma or osteosarcoma being the most common. This is a highly aggressive neoplasm, and while surgery combined with radiotherapy may aid local control, mean survival remains less than 2.5 years (Stephen et al. 1986; Alvarez-Canas and Rodilla 1996) .
Cancer Therapy-Associated Salivary Gland Dysfunction and Xerostomia
Radiation-Induced Salivary Gland Dysfunction and Xerostomia, Early and Late Effects
Radiation therapy may induce salivary gland hypofunction and xerostomia, including treatment regimens of head and neck radiation therapy in which the salivary glands are within the treatment portal, total body irradiation in hematopoietic stem cell transplantation, and radioactive iodine in thyroid cancer. Irradiation of salivary glands in head and neck cancer patients results in a substantial decline in saliva secretion within the first week of radiation therapy with a subsequent continuous reduction where whole saliva secretion may reach practically nil by the sixth week of treatment. Xerostomia induced by radiation therapy has a major deteriorating impact on patients’ quality of life during and long-term after treatment (Tribius et al. 2015). When salivary gland-sparing radiation regimens are applied, such as intensity-modulated radiation therapy, and if it has been feasible to keep the cumulative radiation dose to the gland tissue below thresholds of ~39 Gy for both the parotid gland and submandibular gland, the reduction of saliva secretion will be less and some recovery can be expected (Jensen et al. 2010; Vissink et al. 2015).
Salivary gland function is also affected after high-activity radioiodine ablation therapy in patients with differentiated thyroid cancer (Klein Hesselink et al. 2016). Radioactive iodine is actively accumulated in salivary gland tissue, and sialadenitis is a common sequela along with decreased saliva secretion and xerostomia. Radiation-induced salivary gland hypofunction results in xerostomia and implies a high risk of rapidly progressing dental caries, attrition, abrasion, and erosion of the teeth, oral candidosis, increased mucosal sensitivity, and risk for mucosal trauma .
Cancer Chemotherapy
Cancer chemotherapy may induce temporary salivary gland hypofunction, although there is some controversy whether it is caused by the chemotherapy per se or by other factors, such as the concomitant intake of xerogenic medications like antiemetics (Jensen et al. 2010). Salivary secretion may even be lower in individuals with cancer prior to the initiation of treatment (Harrison et al. 1998; Napenas et al. 2013). Chemotherapy can induce compositional changes in saliva. Decreased whole saliva flow rates combined with the finding of slightly increased salivary sodium and chloride concentrations as well as decreased inorganic phosphate concentration suggest that salivary gland acinar secretion and duct modification mechanisms are impaired by chemotherapy (Jensen et al. 2008). The saliva concentration and output of secretory IgA have also been shown to decrease during and following chemotherapy (Meurman et al. 1997; Harrison et al. 1998; Jensen et al. 2008). Thus, chemotherapy-induced salivary gland hypofunction may potentially impair the oral host defense against oral infecti ons.
Allogeneic Hematopoietic Stem Cell Transplantation/Chronic Oral Graft-Versus-Host Disease
Graft-versus-host disease (GVHD) is an autoimmune-like complication and is a collective name for the systemic consequences induced by the production of antibodies against the host of an allograft bone marrow transplant or peripheral blood stem cell transplant, where various tissues and organs are damaged by the infiltrating donor graft T-lymphocytes. GVHD can present in either an acute or chronic form. Salivary glands are a major target of GVHD and manifest as hyposalivation and xerostomia (Bassim et al. 2015). Changes of saliva composition have also been reported with decreased salivary concentrations of secretory IgA, as well as increased concentrations of sodium, epidermal growth factor, IgG, and albumin (Izutsu et al. 1983; Nagler and Nagler 2003). Some of these possibly reflect the leakage of serum into saliva. Salivary gland biopsies show lymphocytic infiltration, parenchymal destruction, and fibrosis .
Advanced Cancer/Terminally Ill Patients
Advanced cancer patients and terminally ill patients commonly suffer from salivary gland hypofunction and xerostomia. Xerostomia causes significant morbidity in these patient populations, and aggravating factors are extensive, such as a high risk of dehydration and xerogenic medications that are impossible to discontinue or can be difficult to substitute, e.g., opioid analgesics, corticosteroids, antiemetics, and antidepressants. Hyposalivation has been reported at a prevalence of 82% and xerostomia at a prevalence of up to 88% in patients with advanced malignancies (Davies et al. 2001). Since patients with advanced cancer are likely to underreport xerostomia, special care and attention need to be drawn to these vulnerable patient groups in order to relieve xerostomia and to prevent the oral sequelae related to salivary gland hypofunction .
Immune-Mediated Diseases
Sjögren’s Syndrome (SS)
SS is an autoimmune systemic rheumatic disease characterized by progressive focal lymphocytic cell infiltration and destruction of exocrine glands. In particular, salivary and lacrimal glands are affected by SS, leading to dry eyes (keratoconjunctivitis sicca) and subjective dry mouth (xerostomia). SS is in many cases a primary, idiopathic condition of unknown etiology (primary SS). The syndrome may, however, also be secondary to other connective tissue diseases such as RA, SLE, scleroderma, and mixed connective tissue disease. In these cases, the condition is designated as secondary SS (Fox 2005; Moerman et al. 2013) (see Fig. 16).
Dry mouth and dry eyes are common presenting symptoms, and many patients complain of malaise and fatigue. In addition, extraglandular manifestations, like purpura, polyneuropathy, arthritis, and others, can also be present (see Table 4). SS is also associated with organ-specific autoimmune diseases, in particular, autoimmune thyroid disease, primary biliary cirrhosis, and autoimmune gastritis. SS patients are prone to develop malignant lymphomas, mostly of the mucosa-associated lymphoid tissue (MALT) type. Five to 10% of SS patients develop such lymphomas during their life, often in the parotid glands (Figs. 45, 46 and 47) (Fox 2005; Sreebny and Vissink 2010; Pollard et al. 2011).

Bilateral parotid lymphoma in a background of Sjögren’s syndrome. Coronal T1-weighted MRI (a) and axial T2-weighted MRI with fat saturation (b) show marked enlargement of both parotid glands by confluent homogeneous masses of relatively low T2 signal in a middle-aged woman with a long history of Sjögren’s syndrome (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)

Lymphoma in patient with Sjögren’s syndrome: Ultrasound in a 43-year-old woman with a long history of Sjögren’s syndrome shows a hypervascular mass in the right submandibular salivary gland on color Doppler imaging (a). The right parotid gland is also shown (b) and is atrophic and heterogeneous consistent with the long-standing Sjögren’s syndrome (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)

MALT lymphoma. The parotid harbors an extranodal marginal zone lymphoma, arising in a background of chronic lymphoepithelial sialadenitis. The nodule shows replacement of the normal parotid architecture by a lymphoid infiltrate including the formation of numerous lymphoepithelial islands (a). Peppered throughout are residual, often hyperplastic lymphoid follicles with widened and distorted follicular dendritic networks. Atypical small- to medium-sized centrocytoid lymphocytes, often with abundant pale cytoplasm imparting a monocytoid appearance, grow as broad concentric collars and anastomosing swathes around the lymphoepithelial islands and follicles (b). They variably infiltrate into residual follicles. Scattered large lymphocytes are present but nowhere do these cluster or form sheets. Plasmacytoid lymphocytes are also present in small numbers though mature plasma cells are relatively few. Immunohistochemically the tumor is positive for CD43 (c), IgM (d), Kappa light chain (e), and CD20 (f) (Images courtesy of Drs Celia Green, Dominic Spagnolo, Chris Van De Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
SS affects mainly females with a female/male ratio of 9:1. The syndrome can occur at all ages, but the median age of presentation is around 50 years. In the elderly, clinical presentation of SS can be atypical, and in some cases, it is difficult to distinguish SS from SLE (Moerman et al. 2013). Although SS can occur at any age, it seems to be diagnosed nowadays at an earlier age than previously and is also seen in children. The prevalence of diagnosed primary SS is estimated at 0.05% of the general population (Qin et al. 2015).
The lymphocytic infiltrates in the exocrine glands result in malfunctioning glands with sicca complaints of the eyes (keratoconjunctivitis sicca) and mouth (xerostomia) as a result (Fig. 48). With respect to the eyes, symptoms of burning, sandy sensations with pain, and photophobia/photosensitivity prevail. The decreased saliva secretion results in difficulties with swallowing and speech, burning sensations in the mouth, and an increased risk of progressive dental caries and oral infections (Fox 2005; Sreebny and Vissink 2010; Moerman et al. 2013).

Sjögren’s syndrome. Keratoconjunctivitis sicca (punctate stained with lissamine green) (a) and salivary gland hypofunction and xerostomia (b)
Besides redness and dryness of the eyes, enlargement of the salivary glands (Fig. 49) is a common phenomenon, in particular of the parotid and submandibular glands. Enlargement is, generally, due to the presence of an autoimmune inflammatory process in these glands. The glandular enlargement may also be due to lymphoma development within, as mentioned before, in most cases the parotid gland. Primary SS patients have a 10–44-fold greater risk of lymphoma than healthy individuals (odds ratio 18.8; 95% confidence interval, 9.5–37.3) (Zintzaras et al. 2005). It is usually a MALT lymphoma. Risk factors for the development of lymphoma are the presence of cryoglobulins, low complement C4 levels, and palpable purpura (Voulgarelis and Skopouli 2007; Sreebny and Vissink 2010; Pollard et al. 2011). Primary SS is also associated with the development of non-hematological cancers of the thyroid, oral cavity, and stomach in particular (Brito-Zeron et al. 2017).

Enlargement of the parotid gland in a patient with primary Sjögren’s syndrome
Intraoral examination shows dry oral and tongue mucosa, often erythematous and coated by adherent, sticky mucus (Fig. 50). Dental caries, particularly of the smooth surfaces and cervical regions of the teeth, is not uncommon, as well as secondary infection of the mucosa with Candida albicans. It is also not uncommon to observe a viscous, occasionally purulent, discharge from the parotid and submandibular main excretory duct (Fig. 51).

Intraoral examination shows dry oral and tongue mucosa, often erythematous and coated by adherent, sticky mucus

Purulent discharge from the orifice of the parotid (Stensen’s) duct in a patient with primary Sjögren’s syndrome (Reproduced with permission from Stegenga (2013))
Dryness is not restricted to the eyes and mouth. Dryness also occurs at mucosal surfaces in the upper and lower airways frequently leading to coughing and dryness of the vagina associated with dyspareunia and at other locations, the skin in particular (xerosis).
A labial salivary gland biopsy in which 3–6 glands are harvested from the lower lip is the most common biopsy site to histologically evaluate SS. The microscopic feature essential for a possible diagnosis of SS is the presence of focal inflammatory infiltrates in the glandular tissue. This differs from the more common diffuse inflammatory cell infiltrate seen in chronic sialadenitis. The accepted definition of a focus is the presence of at least 50 mononuclear cells (lymphocytes with no more than a small proportion of plasma cells) per 4 mm2 (Fig. 52). Usually many more (several hundred) lymphocytes in periductal or perivascular distribution adjacent to normal acini in glands with no duct dilation or fibrosis are observed. A focal score is ascribed per 4 mm2, so if no foci are present, a score of 0 is made and if ten foci are present (in all likelihood they would be confluent through the lobules examined), the score is 10. The Greenspan scoring system in which >1 focus per 4 mm2 is an acceptable threshold for diagnosis is the most frequently used (Vitali et al. 2002).

Focal inflammatory infiltrates in the glandular tissue in Sjögren’s syndrome (arrow) (Image courtesy of Professor Jesper Reibel, University of Copenhagen, Denmark)
The aims of treatment of SS are to control glandular and extraglandular manifestations, to prevent damage to organ systems and loss of function, and to decrease morbidity and mortality (Moerman et al. 2013). Preventive management of oral complications includes regular dental visits (usually every 3–4 months), guidance from a team of oral health professionals, and 0.1% fluoride oral rinse (weekly to daily in case of severe hyposalivation) or up to daily application of a neutral 1% sodium fluoride gel with a custom-made carrier. Remineralizing pastes containing casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) and casein phosphopeptide-amorphous calcium fluoride phosphate (CPP-ACFP) may also play a role in prevention of caries in patients with SS (Peric et al. 2015). Secondary infection with Candida albicans is common in patients with SS and may require prolonged treatment. Oral candidosis has been reported to occur in 30–70% of SS patients, especially after use of corticosteroids or antibiotics. Infection should be treated with topical (sugar-free) or systemic antifungal drugs. Patients should not wear dentures overnight, and the dentures should be soaked in chlorhexidine solution or diluted sodium hypochlorite (1:10) to prevent reinfections. Among others, antifungals, e.g., nystatin or clotrimazole cream, can be used to treat angular cheilitis, or if candidal infection is excluded, topical steroid, e.g., triamcinolone ointment, can be used (Sreebny and Vissink 2010).
Avoidance of medications that may worsen sicca symptoms is recommended. If the glands respond to stimulation, sugar-free gums or mints are recommended for patients with xerostomia. Combined gustatory and masticatory stimulatory techniques, such as the use of candies, assuming they are sugar-free (and acid-free in dentate patients), are easy to implement and generally harmless. Alternatively, muscarinic medications can be tried. Pilocarpine (2.5–5 mg q.i.d.) and cevimeline (30 mg t.i.d.) are effective in the treatment of dry eyes and xerostomia (Brito-Zeron et al. 2013). Both drugs are muscarinic agonists and can be used in patients who have residual functional gland tissue. Common adverse effects include sweating, flushing, urinary urgency, and gastrointestinal discomfort but are rarely severe. Patients with primary SS patients are, however, more likely to continue cevimeline than pilocarpine long-term due to fewer reported adverse effects with cevimeline (Noaiseh et al. 2014). When stimulation is insufficient, many patients use frequent sips of water during the day and with meals, but the alleviation is of short duration. There are numerous oral rinses, mouthwashes, gels, and saliva substitutes available (Sreebny and Vissink 2010; Dost and Farah 2013; Epstein and Jensen 2015). Whether saliva substitutes will be accepted by a patient is heavily dependent on proper instruction given to the patient (Regelink et al. 1998).
Relief of ocular and oral symptoms has been reported with the use of biologicals. Well-defined SS patients treated with anti-CD20, anti-BAFF, or abatacept showed improvement of subjective and/or objective measures (Meijer et al. 2010; Meiners et al. 2014; De et al. 2015). In a larger phase 3 trial with less well-defined patients, these results could not be repeated for anti-CD20 (Devauchelle-Pensec et al. 2014; Bowman et al. 2017). However, the inclusion of patients in the phase 3 trials was not sufficiently targeted toward the patients who might benefit from rituximab. Thus, there may be a place for rituximab and other biologicals in precision medicine for SS (Bootsma et al. 2017). With regard to the treatment of MALT lymphoma, the algorithm suggested by Pollard et al. (2011) can be used (Fig. 53) (Pollard et al. 2011). There is a treatment need in patients with a high disease activity, while a regimen of watchful waiting can be applied in patients with a low disease activity .

Treatment algorithm for mucosa-associated lymphoid tissue (MALT) lymphoma (Adapted from Pollard et al. 2011). SS Sjögren’s syndrome, FNA fine needle aspiration, R-CP, rituximab with cyclophosphamide and prednisone, NSAID nonsteroidal anti-inflammatory drugs; *Extraglandular disease: polyarthritis/myositis and glomerulonephritis; nervous system involvement; cryoglobulinemic vasculitis; other severe organ involvement; and serological abnormalities, cryoglobulinemia, C4 < 0.10 g/l. ** Six intravenous infusions of 375 mg/m2 of rituximab and 6–8 cycles of cyclophosphamide, given every 3 weeks
Rheumatoid Arthritis
Rheumatoid arthritis (RA) is a chronic auto-inflammatory polyarthritis with a prevalence of 0.5–1.0% in the adult population. RA is more frequent among women than men (3:1), and its prevalence rises with age. RA is known to develop in genetically susceptible individuals under certain environmental conditions. Years before start of the synovial inflammation in RA, autoantibodies such as rheumatoid factor (RF) and anticitrullinated protein antibodies (ACPA; also known as CCP) are found to be present in conjunction with elevated cytokines in non-symptomatic so-called arthritis risk patients (Nielen et al. 2004; Trouw et al. 2009; van de Stadt et al. 2011; Hunt et al. 2016; Rantapaa-Dahlqvist 2009; Willemze et al. 2012). After the first stage (activation of the innate response) and the second stage (activation of the adaptive response), the third stage of the disease is known as the destructive phase. Long-standing destructive RA is characterized by synovitis, fibrous deposition and damage of the cartilage, erosions of the subchondral bone, and periosteal soft tissue inflammation (Janssen et al. 2013). Patients with RA are more likely to present with periodontal disease, poorer oral hygiene manifesting as an increased accumulation of bacterial plaque, and decreased salivary flow rates. The prevalence of secondary SS in RA patients is about 30%, but there is also evidence that salivary flow rate is reduced in RA patients without SS (Silvestre-Rangil et al. 2016) .
Systemic Lupus Erythematosus
SLE is an autoimmune disease in which the body’s immune system mistakenly attacks healthy tissue in many parts of the body. Symptoms vary between people and may be mild to severe. Common symptoms include painful and swollen joints, fever, chest pain, hair loss, mouth ulcers, swollen lymph nodes, feeling tired, and a red rash, which is most commonly on the face. The cause of SLE is not entirely clear. It is believed to involve hormonal, environmental, and genetic factors.
Salivary gland involvement, at least salivary gland dysfunction, is common in SLE. The prevalence of secondary SS in SLE patients is about 20%. A recent study showed that the caries frequency was 85% for SLE subjects (73.3% for inactive SLE and 100% for active SLE). Active SLE patients had a lower stimulated salivary flow rate than inactive SLE patients, 0.65 ml/min versus 0.97 ml/min, respectively. The salivary pH also was in the critical region in active SLE patients (pH 3.9 versus pH 6.1). Moreover, the numbers of S. mutans and S. sobrinus were high in SLE patients (Loyola Rodriguez et al. 2016) .
Sarcoidosis
Sarcoidosis is a systemic disease of unknown cause characterized by the formation of immune granulomas in involved organs. Sarcoidosis most often involves the lung and lymphatic system, but virtually any organs can be affected. Sarcoidosis may encompass numerous different clinical presentations. It may be symptomatic or not, acute or not, and involve variable organs with a diverse clinical impact from benign to very severe.
Oral sarcoidosis is rare, but salivary gland involvement is rather common. Although being an exclusion criterion for SS, sarcoidosis can coexist with SS. Sarcoidosis and primary SS share pathogenic, immunogenetic, and clinical features. Both diseases are characterized by an intense cellular immune response at disease sites, predominantly composed of T-lymphocytes. The prevalence of sarcoidosis in large series of patients with primary SS ranges from 1 to 2%. Although differentiating between sarcoidosis and primary SS may be easy, usually difficulties emerge when the initial symptoms of sarcoidosis are sicca symptoms or parotid gland enlargement. Sarcoidosis affects the lacrimal and salivary glands in 3% and 6% of cases, respectively, and parotidomegaly is detected in 6% (Ramos-Casals et al. 2004).
Sarcoidosis involving the salivary glands is characterized by the presence of numerous granulomas, generally noncaseating, distributed through the glandular tissue (Fig. 54). The granulomas are composed of a central focus of packed macrophages surrounded by lymphocytes and fibroblasts at the periphery. An epithelioid appearance of the packed macrophages may be conspicuous and the formation of multinucleate giant cells (often Langhans-type) may be seen (Fig. 54) .

Sarcoidosis. There are granulomas, generally noncaseating, distributed through the glandular tissue (Image courtesy of Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Scleroderma
Scleroderma is a chronic disease characterized by excessive deposits of collagen in many organs, especially the skin. It is a diffuse disease, which can be lethal due to heart, kidney, lung, or intestinal damage. It is four times more common in women than in men. Symptoms usually appear about the age of 40. The most common clinical manifestations include changes of the skin of the fingers, hands, arms, and face (with edema, sclerosis, and atrophy), sclerodactyly (localized thickening and tightness of the skin of the fingers or toes), and telangiectasia. Also, commonly seen are calcinosis, Raynaud’s phenomenon (discolorations of the fingers and toes with changes in temperature and emotions), esophageal changes, microstomia, musculoskeletal pain, lung fibrosis, nephropathy, and hypertension. Seventy percent of the patients suffer from xerostomia, and, in about 50% of the patients, the whole saliva flow rate is reduced. The labial salivary glands display a large variety of inflammatory changes including glandular fibrosis. About 20% of the scleroderma patients qualify the criteria for secondary SS (Sreebny and Vissink 2010) .
Mixed Connective Tissue Disease
Mixed connective tissue disease (MCTD) is a systemic disorder characterized by Raynaud’s phenomenon, nonerosive polyarthritis, and swollen fingers. MCTD exhibits overlapping features of SLE, scleroderma, and dermatomyositis/polymyositis. MCTD primarily affects women (90%), and the onset is approximately at the age of 30. Xerostomia and reduced salivary secretion are quite common (Helenius et al. 2005). The parenchyma of the salivary glands often demonstrates focal lymphocytic infiltrates. It is not uncommon that MCTD patients suffer from secondary SS .
IgG4-Related Disease
IgG4-related disease is a protean condition that mimics many malignant, infectious, and inflammatory disorders. This multi-organ immune-mediated condition links many disorders previously regarded as isolated, single-organ diseases without any known underlying systemic condition. The disease has many similarities to sarcoidosis and some forms of systemic vasculitis (Figs. 55 and 56) (Kamisawa et al. 2015). IgG4-related disease is a rare, clinical, and pathologic disease entity of unknown etiology. Its main features are increased serum concentrations of IgG4 > 1.35 g/l, lymphocyte, and IgG4+ plasma cell infiltration within tissues, fibrosis, or sclerosis. The classical presentation of IgG4-related disease is pancreatitis, which is combined with the involvement of biliary ducts in 74% of patients. Extrapancreatic manifestations include abdominal or mediastinal lymphadenopathy and the involvement of salivary glands and lacrimal glands, kidneys, lungs, and retroperitoneum (Szanto et al. 2014; Tuttolomondo et al. 2016) .

Kuttner’s pseudotumor. Ultrasound of the left submandibular salivary gland in a patient presenting with a painless palpable submandibular. Ultrasound (a) shows the lesion clearly as a circumscribed geographic hypoechoic lesion, not deforming the contour of the gland, with increased vascularity on color Doppler imaging (b). Ultrasound also guides fine needle aspiration (c) which is always performed to exclude a true neoplastic mass. The entity, also known as focal chronic sialadenitis, is now known to be part of the spectrum of IgG4-related disease. It is a common cause of a submandibular mass (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)

Kuttner’s pseudotumor. Sections show a chronic sclerosing sialadenitis with relative sparing of only a few lobules within the salivary gland where there is retention of acinar cells although chronic inflammation encroaches on these lobules (a). The lobular architecture is maintained and increased amounts of fibrosis separate lobules from one another. Most of the lobules have lost acini, and only ducts remain with no ductal proliferation seen. The inflammation consists of a lymphoplasmacytic infiltrate with many lymphoid follicles and large geographic germinal centers. There are many plasma cells in the inflammatory infiltrate (b). There are many cells staining positively with IgG (c) and some are plasma cells, whereas others appear lymphoid. There are also many plasma cells expressing IgG4. CD20 is concentrated in lymphoid follicles and germinal centers (d), but there are also many CD3-positive T-cells (e) and CD43 positivity (f) throughout the gland (Images courtesy of Drs Felicity Frost and Chris Van Vliet, PathWest, and Professor Camile Farah, UWA Dental School, University of Western Australia, Perth WA, Australia)
Chronic Inflammatory Bowel Diseases
Crohn’s Disease
Crohn’s disease is a chronic inflammatory, granulomatous disorder that primarily affects the lowest portion of the terminal ileum; however it can affect any part of the gastrointestinal tract. The inflammation often leads to erosions, ulcers, intestinal obstruction, and the formation of fistulas and abscesses. Symptoms include chronic diarrhea, abdominal pain, fever, loss of appetite, weight loss, arthritis, and ocular infections. The exact cause of Crohn’s disease remains unknown, but various genetic and environmental factors have been proposed. The onset of Crohn’s disease most commonly occurs between the ages of 15 and 30. More than one-third of all children with Crohn’s disease exhibit oral manifestations including mucogingivitis, mucosal tags, lip swelling, aphthous ulcerations, and pyostomatitis vegetans. Also, the salivary glands may display noncaseating granulomatous inflammation. Although about one-third of the patients suffer from xerostomia, salivary flow rates seem unaffected (Katz et al. 2003). Levels of salivary IgA, IgM, and IgG and interleukin-6 are elevated in patients with Crohn’s disease (see Fig. 16) .
Ulcerative Colitis
Ulcerative colitis is a chronic inflammation of the large intestine (colon). The inflammation affects the mucosa and submucosa and leads to ulcers that bleed and produce pus and mucous. Its symptoms include abdominal pain, diarrhea, rectal bleeding, painful rectal and/or vesical spasms, loss of appetite, fever, fatigue, arthritis, and inflammation of the eyes. The cause of ulcerative colitis is still unknown, but genetic and environmental factors may be involved in the pathogenesis. Symptoms usually develop between the ages of 15 and 30. The levels of IgA and IgG are elevated in whole saliva (Crama-Bohbouth et al. 1989) .
Autoimmune Liver Diseases
Autoimmune liver diseases are chronic inflammatory disorders of unknown etiology in which an immune-mediated attack is directed toward the hepatocytes, small bile ducts, or the entire biliary system (see Fig. 16). The most predominant diseases are autoimmune hepatitis, primary biliary cirrhosis, and primary sclerosing cholangitis. The clinical symptoms include fatigue, fever, jaundice, polymyalgia, arthralgia, and symptoms of progressive hepatic dysfunction. These liver diseases are often present in association with other autoimmune diseases, predominantly diabetes mellitus type 1, thyroid disease, RA, and ulcerative colitis. Both xerostomia and decreased salivary flow rates have been reported in autoimmune liver diseases (Mang et al. 1997) .
Musculoskeletal Disorders
Fibromyalgia
The term fibromyalgia covers a syndrome of chronic, widespread musculoskeletal pain, tenderness to light touch, moderate to severe fatigue, and disturbed sleep. In addition, patients often suffer from migraine, headache, temporomandibular disorders, depression, and irritable bowel syndrome. The syndrome more commonly affects women than men. Xerostomia, glossodynia, and dysgeusia are common oral symptoms (Rhodus et al. 2003). Salivary gland hypofunction has also been shown in fibromyalgia. However, labial salivary gland biopsies have not revealed any specific histopathological changes. Fibromyalgia patients commonly share many symptoms with SS patients, but there are great dissimilarities in the pathophysiology underlying both diseases as most objective criteria used in the diagnostic workup of SS are negative in fibromyalgia patients (see Fig. 16) .
Chronic Fatigue Syndrome
Chronic fatigue syndrome is a condition characterized by severe, chronic mental and physical exhaustion, arising in previously healthy and active persons. Other symptoms include malaise, dysphagia, widespread musculoskeletal pain, headache, depression, irritability, and sleep disturbances. Chronic fatigue syndrome usually appears after a period of stress or after a flu-like illness. Chronic fatigue syndrome resembles SS in many aspects, but, like fibromyalgia, most patients do not qualify for the criteria of SS. The majority of patients with chronic fatigue syndrome is affected by xerostomia and dry eyes (Ruiz et al. 2011). Xerostomia occurs in approximately 50% of the patients, and salivary flow rate may be decreased. Labial salivary gland biopsies have shown varying degrees of ductal and acinar dilation, periductal fibrosis, lymphoplasmacytic infiltrates, and lymphocytic foci but lack the characteristics typical for SS patients (Woo et al. 2000; Sirois and Natelson 2001) .
Amyloidosis
Amyloidosis refers to a variety of conditions in which an abnormal protein polysaccharide substance with starch-like characteristics, called amyloid, is deposited in tissues and organs, thereby impairing their function. Primary amyloidosis occurs independently of other diseases and usually affects the skin, tongue, thyroid gland, intestines, liver, kidneys, spleen, lung, and heart. Secondary amyloidosis, the most common type, often appears with other chronic diseases like multiple myeloma, RA, tuberculosis, osteomyelitis, or Crohn’s disease, and it typically affects the kidneys, liver, spleen, lymph nodes, and vascular system. Other types include hemodialysis-associated, inherited, and senile amyloidosis. Amyloidosis is usually diagnosed after the age of 40, and most patients are men. Xerostomia and decreased saliva flow rate, as well as enlargement of the submandibular glands, have been reported (Prokaeva et al. 2007; Juusela et al. 2013). Amyloid deposits may appear in the oral mucosa. Labial salivary gland biopsy is a highly sensitive method for the diagnosis of primary and secondary amyloidosis with features distinct from SS. However, the presence of SS should be considered in patients with cutaneous amyloidosis. The combination of cutaneous amyloidosis and SS has been shown to be a distinct disease entity reflecting a particular and benign part of the polymorphic spectrum of lymphoproliferative diseases related to SS (Meijer et al. 2008).
Endocrine Diseases
Diabetes Mellitus
Diabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia due to insufficient insulin secretion and/or reduced insulin sensitivity. Type 1 DM is characterized by a gradual cellular-mediated autoimmune destruction of the insulin-producing β-cells in the pancreas. An exogenous supply of insulin is critical to affected individuals. Type 1 DM mainly affects children and adolescents, but it may occur at any age. The initial classical symptoms include polydipsia, polyphagia, polyuria, fatigue, weakness, irritability, weight loss, and pruritus. Type 2 DM is caused by a combination of insufficient insulin secretion in the pancreatic β-cells and insulin resistance in tissues, primarily in skeletal muscles and hepatic cells. Type 2 DM is predominantly a disease of middle-aged and older people, but in recent years, the age of onset has decreased, even to children and adolescents (see Fig. 16).
Both type 1 and type 2 DM are associated with an increased risk of developing oral diseases including periodontal disease, oral candidosis, dental caries, salivary gland hypofunction, sialadenosis, and impairment of taste. Xerostomia is a relatively common complaint, especially among patients with poorly controlled DM. Xerostomia is related to decreased unstimulated and stimulated whole saliva flow rates (Lopez-Pintor et al. 2016; Malicka et al. 2014). An enlargement of the parotid glands may also occur in patients with poorly controlled DM .
Hyperthyroidism
Hyperthyroidism includes any disease which results in excessive secretion of thyroid hormones, such as Graves’ disease, diffuse toxic goiter, Basedow’s disease, Parry’s disease, and thyrotoxicosis. Hyperthyroidism mainly affects women. Although it occurs at all ages, hyperthyroidism is most likely to occur after the age of 15 years. Regardless of the cause, hyperthyroidism produces the same symptoms, including heart palpitations, weight loss with increased appetite, diarrhea, fatigue, intolerance to heat, weak muscles, tremors, anxiety, eye symptoms, difficulty sleeping, decreased menstrual flow, and irregular menstrual cycles.
Hyperthyroidism has been found associated with an increased salivary flow rate or normal flow rates (Muralidharan et al. 2013). However, complaints of xerostomia are not uncommon after treatment with radioactive iodine and are most probably related to some extent of radiation injury to salivary gland tissue due to the uptake of radioactive iodine also by the salivary glands (Jensen et al. 2010) .
Hypothyroidism
Hypothyroidism represents a decreased activity of the thyroid gland that may affect all body functions. The most common cause of hypothyroidism is Hashimoto’s thyroiditis, in which the immune system of genetically predisposed individuals destroys the thyroid gland. Other causes of hypothyroidism are surgical removal of the thyroid gland and irradiation of the gland (e.g., status after radioactive iodine administration to treat hyperthyroidism). Symptoms include fatigue, weakness, weight gain, coarse, dry hair and dry, pale skin, hair loss, cold intolerance, muscle pain, constipation, depression, irritability, memory loss, abnormal menstrual cycles, and decreased libido.
It has been shown that both unstimulated and stimulated salivary flow rate is decreased in patients with hypothyroidism and autoimmune thyroiditis (Muralidharan et al. 2013; Agha-Hosseini et al. 2016). Salivary gland enlargement (sialadenosis) has been described in hypothyroidism .
Cushing’s Syndrome and Addison’s Disease
In general, endocrine disorders involving the adrenal cortex will affect the salivary composition. Cushing’s syndrome is a relatively rare hormonal disorder caused by prolonged exposure to excessive levels of cortisol or other glucocorticoids. It can result from excessive adrenocorticotropic hormone (ACTH) production by a pituitary adenoma or by ectopic tumors secreting ACTH or corticotropin-releasing hormone. ACTH-independent Cushing’s syndrome is caused by adrenocortical tumors or hyperplasias. It primarily affects adults aged 20–50 years. Symptoms vary, but most patients have upper body obesity, a rounded face (moon face), increased fat around the neck, and thinning arms and legs, fragile and thin skin that bruises easily, purple striae on the abdomen, hirsutism, hypertension, fatigue, elevated blood sugar, irritability, anxiety and depression, irregular or absent menstrual periods in women, and erectile dysfunction in men.
Addison’s disease, also called primary adrenal insufficiency, is an endocrine disorder caused by insufficient production of glycocorticoids and mineralocorticoids by the adrenal glands. Reduced secretion of cortisol can lead to reduced sodium and increased potassium concentrations in the blood and acidosis, mainly due to lack of aldosterone. The disease occurs in all age groups and afflicts men and women equally. The symptoms and disease manifestations include weight loss, muscle weakness, joint and back pain, fatigue, hypotension, and darkening of the skin especially in sun-exposed areas and hyperpigmentation of the palmar creases, frictional surfaces, vermilion border, and oral mucosa. Since the concentration of cortisol in the saliva is in equilibrium with the free, active cortisol in the plasma, measurement of nighttime salivary cortisol or cortisone may be a relevant adjunct or alternative to serum screening tests for Cushing’s syndrome (Antonelli et al. 2015; Restituto et al. 2008) and morning salivary cortisol as a screening test for Addison’s disease (Restituto et al. 2008) .
Neurological Disorders
Central Nervous System Trauma
Craniocerebral injuries can lead to salivary gland dysfunction and xerostomia (see Table 5). These include craniofacial fractures; neural disruption by surgical trauma; cerebrovascular accidents including stroke, cerebral ischemia, or hemorrhage; brain edema; and brain stem injury.
Stroke patients often suffer from reduced whole saliva flow rate as well as impaired masticatory function, which adds to the complexity of dysphagia (Kerr et al. 2009). Patients with CNS trauma may also experience drooling. This is not necessarily due to an increased saliva secretion, but either a disturbed swallowing ability (disturbed motor control of the muscles involved in swallowing) or a disturbed sensibility of the oral mucosa (the patients do not feel that there is too much saliva in the mouth), thereby not eliciting the swallowing reflex (see Fig. 16).
Cerebral Palsy
Cerebral palsy syndromes occur in 0.1–0.2% of children and the prevalence is higher in babies born prematurely. The term is an umbrella for a group of disorders affecting body movement, balance, and posture caused by abnormal development or damage of the part(s) of the brain that control muscle tone and motor activity. The syndrome is characterized by lack of muscle coordination when performing voluntary movements (ataxia); stiff muscles and exaggerated reflexes (spasticity) are also common. Children with cerebral palsy may have a low whole saliva flow rate (see Table 5) (Santos et al. 2010). Drooling is a major morbidity associated with cerebral palsy related to swallowing difficulties and is often causing social handicaps and stigmatization for the child.
Bell’s Palsy
Bell’s palsy is an idiopathic unilateral disruption of the facial nerve. It may occur suddenly and it can be total or partial. Around 70% of the patients recover spontaneously within weeks to a few months, although it can be permanent. Pregnancy, diabetes mellitus, and SS are predisposing factors. Other factors that could induce facial paralysis include trauma, stroke, tumor, influenza or a bad cold, middle ear disease, and herpes simplex virus infection.
Since parasympathetic nerve fibers to the salivary glands travel with the facial nerve, damage to these nerves, as seen in Bell’s palsy, may result in a decreased saliva flow rate (see Table 5). A follow-up time of 12 months is recommended to assess the ultimate outcome of Bell’s palsy. The ability of a patient to respond to strong salivary stimulants seems to be a reliable prognostic factor for the course of the disease (Ekstrand 1979) .
Parkinson’s Disease
Parkinson’s disease (PD) is a progressive neurodegenerative cerebral disorder with an unknown etiology. It is mostly seen in people aged over 50 years. PD causes degeneration of dopamine-producing neurons. This induces motor dysfunction, wherein all voluntary movements, particularly those carried out by the small muscles, are notably slowed (bradykinesia), and spontaneous movement is diminished (akinesia).
Patients with PD have been shown to have decreased unstimulated and stimulated whole saliva flow rates (Fedorova et al. 2015). Furthermore, xerostomia is a common problem in PD (Barbe et al. 2017; Zlotnik et al. 2015). It has been suggested that the decreased saliva flow rate is an indicator of the autonomic dysfunction seen in early PD (see Table 5). With advanced PD symptoms, the saliva flow rates become even lower. This may in some cases be caused by antiparkinson xerogenic medications. On the other hand, administration of levodopa has been demonstrated to elicit an increase in saliva secretion without affecting saliva composition. Decreased frequency and efficacy of swallowing and dysphagia are likely to be the causes of drooling in PD .
Alzheimer’s Disease
This neurodegenerative disorder is progressive and is seen mostly in people aged above 60 years. Patients are characterized by loss of intellectual functions like memory, undergo personality change, and lose the ability to take care of themselves. It is common for patients with Alzheimer’s disease to be treated with antipsychotics and antidepressants to ameliorate behavioral symptoms and stabilize mood; thus medication-induced hyposalivation is a common finding. It has been shown that in unmedicated patients with Alzheimer’s disease, impaired saliva flow rate is limited to the submandibular glands (see Table 5) (Ship et al. 1990).
Oral Dysesthesia
Oral dysesthesia also known as burning mouth syndrome (BMS) is characterized by a painful burning sensation of the oral mucosa of long-term duration without any detectable local or systemic causes. The etiology remains unknown, but recent research suggests that BMS is a neuropathy (Puhakka et al. 2016). It typically affects women over the age of 50 years. Xerostomia is a frequent symptom in patients with BMS (30–70%), but both whole saliva and parotid saliva flow rates are normal, so is the concentration of salivary high molecular weight proteins. However, recently it has been found that patients with BMS have a lower expression of salivary low molecular weight proteins (de Moura et al. 2007). For more details on this topic, refer to the chapter on “Oral Dysesthesia.”
Infectious Diseases
Epidemic Parotitis
Epidemic parotitis is an acute febrile sialadenitis caused by a paramyxovirus. It is spread via saliva droplet infection, the incubation period being 2–3 weeks. Epidemic parotitis commonly affects children and young adults, but in parts of the world where the measles, mumps, and rubella (MMR) vaccine is routinely used, the prevalence of the disease is declining. Clinically, epidemic parotitis causes fever, malaise, nausea, and a tender uni- or bilateral enlargement of the major salivary glands, primarily the parotids (Iro and Zenk 2014). Eating or talking provokes pain. In addition, the enlargement of the parotid glands may induce an obstruction of the parotid duct that will further aggravate the pain when saliva secretion is stimulated. Salivary gland symptoms usually peak within 2–3 days after the first clinical symptoms and resolve within 1–2 weeks. According to clinical experience, the affected glands hardly secrete any saliva, and if saliva is secreted, it is usually a clear, watery solution (see Fig. 16).
Juvenile Parotitis/Recurrent Parotitis
Juvenile recurrent parotitis is a common condition of the salivary glands in children, which is characterized by intermittent swelling of the parotid glands on one or both sides, with or without pain, and generally associated with nonobstructive sialectasis of the parotid gland, as well as salivary gland hypofunction (Leerdam et al. 2005). It is diagnosed from the medical history and confirmed by sialography or ultrasonography. Recurrent juvenile parotitis might be linked to SS, which occurs in some patients (Nieto-Gonzalez et al. 2014), but in many patients, juvenile parotitis resolves during adulthood .
Bacterial Sialadenitis
Bacterial sialadenitis can be either acute or chronic. Decreased saliva flow rate is the primary predisposing factor, and this allows retrograde microbial colonization of the duct, which may result in the development of acute or chronic suppurative infection. Acute sialadenitis is characterized by a painful swelling of a single salivary gland, commonly affecting the parotid gland (Figs. 57 and 58). A purulent discharge may be expressed from the salivary duct orifice, and the patient may present with redness of the overlying skin or even abscess formation within the inflamed gland tissue, malaise, fever, and cervical lymphadenopathy. Bacterial sialadenitis often occurs in elderly patients who suffer from salivary gland hypofunction due to systemic diseases, medication intake, or dehydration, or it may be associated with obstruction of the salivary ducts by deposition of calculi, mucus plugs, and tumor growth or by trauma. In medically compromised or immunosuppressed patients, the infection may even become life-threatening due to sepsis. Chronic sialadenitis may develop following acute sialadenitis if the predisposing factors cannot be eliminated. Staphylococcus aureus is the most common pathogen isolated from purulent sialadenitis; sometimes, it may be caused by streptococci, anaerobic bacteria and, more rarely, by gram-negative facultative bacteria (Brook 2009). For more details on this topic, refer to the chapter on “Non-odontogenic Bacterial Infections.”

Bacterial sialadenitis. The right parotid gland is swollen, although less than the left gland (Image courtesy of Professor Camile Farah, Perth Oral Medicine & Dental Sleep Centre, Perth WA, Australia)

Acute suppurative parotitis (nonobstructive). Axial post-contrast CT images in a 77-year-old man presenting with acute pain and swelling in the right cheek. The right parotid gland appears enlarged and edematous, with a rim-enhancing fluid collection (arrow in a) consistent with an abscess. Inferior to the parotid tail, there is peri-parotid edema deep to the platysma (arrow in b). No calculus or other precipitating lesion was shown (Images courtesy of Dr Rudolf Boeddinghaus, Perth Radiological Clinic, Perth WA, Australia)
HIV/AIDS
Human immunodeficiency virus (HIV), a retrovirus transmitted via blood and infection, induces a chronic progressive decrease in the number of CD4+ T-cells and seriously weakens the immune system. It may be clinically asymptomatic in its early stages, but an effect on salivary gland function has been reported in early-stage HIV disease (Lin et al. 2003). If untreated, the mean period of asymptomatic HIV infection is 10 years before the onset of severe symptoms or illnesses leading to a diagnosis of acquired immunodeficiency syndrome (AIDS). Later, symptoms of HIV infection can include HIV-associated salivary gland disease expressed as a uni- or bilateral enlargement of the major salivary glands, particularly the parotid glands. This may be due to lymphocytic infiltration of the salivary glands or to an increase in the amount of lymphoid tissue within them. HIV patients demonstrate salivary gland hypofunction and xerostomia (Navazesh et al. 2003). Low whole saliva flow rates have been associated with low CD4+ cell counts and with highly active antiretroviral therapy (HAART), reflecting disease progression and adverse effects of the treatment. The HIV virus is present at low concentrations in saliva of infected persons, but there is no evidence that the virus is spread by contact with saliva. Clinical and histological manifestations of HIV-associated salivary gland disease may resemble SS.
Hepatitis C Virus
Hepatitis C virus is primarily spread by parenteral transmission. A chronic hepatitis C virus infection is established in about 80% of infected individuals. It is commonly associated with an increased risk of liver cirrhosis and liver cancer. Chronic hepatitis C virus infection may present with extrahepatic manifestations, including salivary gland hypofunction (Grossmann et al. 2010). Xerostomia has also been associated with hepatitis C infection. Active infection with hepatitis C is an exclusion criterion for the classification of SS .
Epstein-Barr Virus
The Epstein-Barr virus (EBV) is a member of the herpes virus family. Primary infection by EBV generally occurs during childhood and is asymptomatic. Primary infection in adolescents or in adults is the etiological cause of infectious mononucleosis, glandular fever that clinically presents with a sore throat, fever, malaise, cervical lymphadenopathy, and in some cases, hepatosplenomegaly. EBV is primarily transmitted from asymptomatic individuals through saliva, and it establishes lifelong latent infections of B-cells. EBV can infect salivary gland tissue, and, in rare cases, this may present as parotitis (Lee et al. 1997). EBV-associated oral tumors can involve the parotid gland .
Tuberculosis
Tuberculosis is a bacterial infection primarily caused by Mycobacterium tuberculosis; it is spread via droplet infection. Primary infection of the lungs induces the development of a granulomatous inflammatory reaction that attempts to limit or stop the infectious process. This leads to the development of a latent infection of the tubercle bacilli in dystrophic calcified foci. Secondary infections may involve other organs. Oral involvement is not common, but in rare cases, salivary glands may be affected, primarily the parotid gland (Catano and Robledo 2016). The infection may involve the gland parenchyma or the intraparotid lymph nodes. More detail on this topic is provided in the chapter on “Non-odontogenic Bacterial Infections.”
Genetic Disorders
Salivary Gland Aplasia
Salivary gland aplasia is the congenital absence of salivary glands. Aplasia is rare and may comprise absence of some or all of the major salivary glands. It may be related to genetic syndromes of the ectodermal tissues, e.g., ectodermal dysplasia .
Ectodermal Dysplasia
Ectodermal dysplasia (ED) is a group of more than 150 heritable disorders that affect the ectoderm, the outer germ layer in the embryo. The most common and best characterized type of ED is the X-linked recessive hypohidrotic ED. The ectoderm contributes to the formation of most of the body’s surface tissues: skin, hair, nails, teeth, and sweat glands. The prominent developmental defects of ED can be manifested clinically as hypotrichosis (reduced hair growth), hypodontia or anodontia (congenital missing number of teeth or absence of all teeth), and hypohidrosis (reduced or absent sweat secretion) causing dry skin and heat intolerance. Salivary glands are derived from the ectoderm and may be affected by ED so whole saliva flow rates may be decreased (Lexner et al. 2007). In a subset of ED patients, hypoplasia and aplasia of the major salivary glands may be present. Reduced unstimulated and stimulated whole saliva flow rates and reduced submandibular gland secretion have been shown, but no alteration of the parotid gland secretion .
Cystic Fibrosis
Cystic fibrosis (CF) is an autosomal recessive inheritable disorder that primarily affects the lungs and the digestive system. CF is caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene on chromosome 7 (Harrington et al. 2016). More than 950 different CFTR mutations have been classified, with deltaF508 the most frequent. The mutations of the CFTR gene influence epithelial ion transport in exocrine glands. This affects the transport of sodium and chloride, as well as protein, and results in the production of highly mucous secretions. Clinically, CF is characterized by recurrent and chronic pulmonary infections leading to chronic obstructive pulmonary disease, which is the major cause of morbidity and mortality. Furthermore, glandular dysfunctional manifestations of CF include elevated salt concentrations (sodium and chloride) in sweat and pancreatic and lacrimal fluids.
Salivary gland dysfunction is associated with CF. Decreased whole saliva flow rates may be manifest in CF patients, but CF seems to affect serous and mucous salivary gland types differently. In seromucous submandibular secretions, low salivary flow rates and high viscosity as well as significantly higher concentrations of total calcium and total protein have been found (Davies et al. 1990). Findings in serous parotid gland function are more inconsistent and parotid flow rate seems to be little affected (Davis 1987). Salivary gland hypofunction in CF patients may become further aggravated due to a daily intake of xerogenic medications .
Prader-Willi Syndrome
Prader-Willi syndrome (PWS) is associated with genetic abnormalities of chromosome 15. Manifestations of PWS are abnormal growth (short stature, small hands and feet, prominent forehead), hypogonadism (decreased function of the testes or ovaries), infantile hypotonia (abnormally low muscle tone), strabismus (ocular misalignment), mild to moderate mental retardation, and hyperphagia (abnormally increased appetite) with consequent obesity. Oral findings of delayed tooth eruption and hypoplastic teeth have been reported. Whole saliva flow rate is significantly decreased and saliva consistency is highly viscous (Saeves et al. 2012). The thick, viscous saliva is part of the minor diagnostic criteria for PWS .
Metabolic Disturbances
Dehydration
Saliva flow rate and composition are dynamic parameters controlled by the physiological and pathophysiological conditions of the host. The salivary glands, in particular the acinar end pieces, have a high capability of transporting water from the interstitial fluid to form primary saliva. Impairment of the body’s regulation of water might have a significant impact on the salivary gland fluid output (see Fig. 16). It has been shown that body dehydration is associated with decreased parotid flow rates and that these changes are age-independent in healthy adults (Ship and Fischer 1997). Furthermore, dehydration is an occasional cause of decreased saliva secretion and complaints of xerostomia, especially in elderly patients who consume less water and take many medications that interfere with the body’s salt and water balance. Also, alcoholics may suffer from dehydration and consequently salivary gland hypofunction and xerostomia (Inenaga et al. 2017).
Malnutrition
Patients living on a considerably unbalanced diet or patients who suffer from malabsorption and vitamin and mineral deficiencies may develop salivary gland hypofunction and xerostomia (Sheetal et al. 2013). Besides giving rise to hormonal disturbances including increased concentrations of blood and saliva cortisol and impaired oral mucosal integrity, malnutrition, in particular insufficient intake of protein, can result in decreased whole saliva flow rate and compositional changes. Included among the salivary compositional changes are significantly decreased concentrations of secretory IgA. Hunger-induced salivary changes are rare in Western populations, but among patients with poor nutritional status such as some elderly, food eccentrics, alcoholics, and persons with eating disorders, it is rather common to experience salivary changes. Thus, significant associations have been found between malnutrition, decreased salivary secretion, and reduced serum albumin concentration, and it has been suggested that salivary gland hypofunction and xerostomia have a negative effect on alimentation, appetite, and oral comfort .
Sodium Retention Syndrome
Besides the rather typical sialometrical/sialochemical profile of patients with hypothyroidism (sialadenosis), there are also patients who are characterized by a low sodium concentration in spite of a high flow rate, especially of stimulated parotid saliva (van den Berg et al. 2007). Clinically, this condition is characterized by short lasting (about one hour), often unilateral, swellings of the parotid glands. When occurring bilaterally, the patients may complain about painful tension. In the latter cases, the swelling regresses within days. This concept is named sodium retention syndrome. The mechanism underlying sodium retention syndrome is still not well understood, but this condition has been related to hyper- and hypotension, cardiac failure, local and systemic edema from other causes, and dehydration .
Eating Disorders
Bulimia Nervosa
Bulimia nervosa is a serious eating disorder primarily affecting young women. In countries with a westernized lifestyle, it has a prevalence of 1–2% in 16–35-year-old females but may be even higher, as persons with bulimia nervosa tend to hide their disease and avoid professional help. Persons with bulimia nervosa have an irrational, morbid fear of weight gain and obesity with immense efforts to control food intake and eliminate it when food is consumed. Typically, their lifestyle is characterized by recurrent episodes of binge eating, recurrent self-induced vomiting, and misuse of medicines like laxatives and diuretics. Also, they commonly fast and engage in excessive exercise. Persons with bulimia nervosa often present with a normal body appearance.
Dental and salivary gland changes have been reported in up to two-thirds of the study populations (Dynesen et al. 2008). Frequently observed are dental erosion, especially the lower anterior teeth (Fig. 59) due to vomiting, and intermittent painless bilateral enlargement of the major salivary glands, especially the parotids. The enlargements of the parotids usually develop within a few days after a bulimic episode (see Fig. 16).

Dental erosion in a patient with bulimia nervosa. Maxillary teeth (a) and mandibular teeth (b) (Images courtesy of Dr Anja Weirsøe Dynesen, University College Absalon, Denmark)
Anorexia Nervosa
Anorexia nervosa is a serious eating disorder primarily affecting young women. Its early diagnosis is often difficult as persons with anorexia nervosa often hide their disease and avoid professional help. The prevalence is around 1% with an incidence that has been stable since the 1970s. It is characterized by the person’s refusal to maintain their normal body weight and struggle to attain a weight that is less than 85% of normal weight expected for their age and height. Despite their loss of weight, they still possess an intense fear of gaining weight and suffer from the self-perception and firm belief that they are too fat. Furthermore, young post-menarche females often suffer from amenorrhea. Self-induced vomiting and misuse of laxatives, diuretics, and enemas are seen in anorexia nervosa of the purging type, whereas the restricted type presents without any significant history of vomiting. Xerostomia is a rather common complaint among persons with anorexia nervosa who show different grades of dehydration caused by starvation, laxatives, diuretics, and/or vomiting (Montecchi et al. 2003). Decreased unstimulated whole saliva flow rate and xerostomia have been reported in anorexia nervosa. The impaired salivary secretion could play a role in the development of dental erosion often seen in persons with anorexia nervosa, even in the restricted type who may have an excessive intake of acidic foods like fruit .
Management Protocols
The treatment of xerostomia and salivary gland hypofunction should be based on answers to the following determinations (Sreebny and Vissink 2010):
-
1.
Determine the cause of the xerostomia. If the cause can be determined, attempt to eliminate it. This may reduce the problem and alleviate the symptoms that are consequentially associated with it.
-
2.
If the cause cannot be assessed or if treating the cause only partially relieves the xerostomia, determine if it is possible to stimulate the saliva secretion. This, per se, may readily diminish oral desiccation.
-
3.
If saliva cannot be adequately stimulated, determine whether the xerostomia can be alleviated by lubricating the surfaces of the oral mucosa with saliva substitution.
-
4.
Determine what else can be done to preserve and protect the teeth and oral mucosa and provide relief to the patient.
Masticatory, Gustatory, and Mild Acid Stimulation Techniques
Dryness of oral mucosal surfaces, difficulty wearing dentures, interproximal plaque accumulation, and difficulty with speaking, tasting, and swallowing may all improve from saliva stimulatory methods. The stimulation will only function if residual salivary gland capacity remains. In patients with long-term SS and other autoimmune diseases, the acinar fluid-producing cells may have undergone atrophy and been replaced by connective tissue. Similarly, irradiated head and neck cancer patients with the salivary glands included in the radiation field are likely to have lost all functional acinar cells and will not benefit from salivary stimulatory methods.
Masticatory and gustatory stimulation are easy to implement, are acceptable to most patients, and have few adverse effects. The combination of chewing and taste, as provided by gums, lozenges, or mints, can be very effective in relieving symptoms for patients who have remaining salivary function. Table 6 lists products that stimulate saliva secretion. Due to the increased risk for dental caries and erosion in dentate patients with salivary gland hypofunction, only sugar-free stimulatory products and acidic products that are specially prepared, e.g., nonerosive, should be used. Nonerosive acidic tablets contain a weak acid, often malic acid, to stimulate saliva secretion; however, this may be erosive to the teeth in patients suffering from salivary gland hypofunction, in particular if used numerous times daily. Therefore, phosphate and fluoride may be added to the tablet to compensate for the erosive potential (examples of commercially available tablets, lozenges, and wine gums are Xerodent™, Stisal®, Ekulf) (Lajer et al. 2009). Electrostimulation (Fig. 60) may also be beneficial in the treatment of xerostomia as a non-pharmacological approach with no reported adverse effects. Electrostimulation of salivary secretion may be of particular benefit for potential use in medicated/polypharmacy patients; however, there is limited evidence to determine the effects of electrostimulation devices (Furness et al. 2013; Alajbeg et al. 2012) .

Device for electrostimulation of salivary secretion and alleviation of xerostomia. SaliPen (Saliwell Ltd.) electrostimulating device (a), recommended use 1–5 min, four times daily or as needed. Placement of SaliPen in the mouth (b). Placement of SaliPen between the lips (c) (Images courtesy of Dr Andy Wolff, Saliwell Ltd.)
Pharmacologic Stimulation
Pilocarpine and cevimeline are used to treat xerostomia in patients with some residual function of the salivary glands. Both of these drugs are muscarinic agonists that induce a transient increase in salivary secretion and improve xerostomia. Common adverse effects of both medications include sweating, flushing, urinary urgency, and gastrointestinal discomfort. These adverse effects are frequent but are rarely severe. Parasympathomimetics are contraindicated in patients with uncontrolled asthma, narrow-angle glaucoma, or acute iritis and should be used with caution in patients with significant cardiovascular disease, Parkinson’s disease, asthma, or chronic obstructive pulmonary disease.
The best tolerated doses for pilocarpine are 2.5–5 mg, given three or four times daily. The duration of action is approximately 2–3 h. Cevimeline is currently recommended at a dosage of 30 mg 8 hourly, and the duration of secretagogue activity is longer than pilocarpine (3–4 h), but the onset is somewhat slower. Patients, however, are more likely to continue cevimeline than pilocarpine long-term due to fewer reported adverse effects with cevimeline (Noaiseh et al. 2014).
The maximum therapeutic effect of pilocarpine on xerostomia is normally obtained after 4–8 weeks; however the time to response can be up to 12 weeks in some patients. Pilocarpine and cevimeline tablets are not available worldwide, so an empiric alternative to pilocarpine tablets is the oral use of pilocarpine eye drops (off license). Pilocarpine eye drops are generally available as 2% or 4% solutions. One drop of the 2% pilocarpine eye drops approximately equals 1 mg pilocarpine, and one drop of the 4% pilocarpine eye drops approximately equals 2 mg pilocarpine. Thus, a recommended dose of 2.5–5 mg pilocarpine tablets three or four times daily would be approximately equivalent to 2–5 drops of 2% pilocarpine eye drops (2–5 mg) or 1–3 drops of 4% pilocarpine eye drops (2–6 mg) taken orally three or four times daily. The eye drops may be diluted in water before taking. There is limited literature available to support the use of pilocarpine eye drops as an alternative to pilocarpine tablets for the treatment of xerostomia. Thus, the use of pilocarpine eye drops to manage xerostomia is unlicensed, and the indication and prescription dose should always be advised by a healthcare professional, with the same contraindications as for pilocarpine tablets taken into consideration .
Oral Moisturization
For most patients, frequent sips of water during daytime are the most efficacious method to alleviate xerostomia. However, patients should be advised that aqueous solutions only provide short-term alleviation from xerostomia (Vissink et al. 1986).
There are numerous oral rinses, mouthwashes, and gels available for alleviation of xerostomia (Dost and Farah 2013; Epstein and Jensen 2015). Patients should be warned to avoid products containing alcohol, sugar, or strong flavorings that may irritate the sensitive, dry oral mucosa. Moisturizing creams can also be very helpful. The frequent use of products containing aloe vera or vitamin E should be encouraged. Persistent cracking and erythema at the corners of the mouth (angular cheilitis) should be investigated for a fungal or bacterial cause .
A variety of commercially available salivary substitutes has demonstrated some efficacy in patients with xerostomia (Fig. 61). Table 6 lists saliva substitutes/oral moisturizers. However, saliva replacements (saliva substitutes or “artificial saliva”) are not well accepted long-term by many patients; thus careful instructions on how to use saliva substitutes are needed for them to be effective. As a guide to choosing the best substitute for a patient, the following recommendations for the treatment of hyposalivation and xerostomia can be used (Regelink et al. 1998):
-
Severe hyposalivation: A saliva substitute with gel-like properties should be used during the night and when daily activities are at a low level. During the day, a saliva substitute with properties resembling the viscoelasticity of natural saliva, such as substitutes that have xanthan gum and mucin (particularly bovine submandibular mucin) as a base, is indicated .
-
Moderate hyposalivation: If gustatory or pharmacological stimulation of residual saliva secretion does not ameliorate xerostomia, saliva substitutes with a rather low viscoelasticity, such as substitutes, which have carboxymethylcellulose, hydroxypropylmethylcellulose, mucin (porcine gastric mucin), or low concentrations of xanthan gum as a base, are indicated. During the night or other periods of severe oral dryness, the application of a gel is helpful .
-
Mild hyposalivation: The salivary glands of these patients usually contain viable, responsive acinar cells. Gustatory or pharmacological stimulation of residual secretion is the treatment of choice. Little amelioration is to be expected from the use of saliva substitutes .

Examples of some commercially available saliva substitutes (spray and gel), saliva stimulating tablets, and water in a spray bottle for alleviating xerostomia
Prevention and Treatment of Infection
Caries
The use of topical fluorides in a patient with salivary gland hypofunction is absolutely critical to the control of dental caries. There are many different fluoride therapies available, from low concentration, over-the-counter fluoride toothpaste, gel, or mouthwash to more potent highly concentrated prescription fluorides: fluoride paste (e.g., 5000 ppm toothpaste), gel (e.g., 1.0% neutral sodium fluoride gel applied by brush or in a custom carrier), or varnish to be delivered by oral healthcare practitioners. The dosage chosen and the frequency of application (from daily to once a week) should be based on the severity of the salivary gland hypofunction and the rate of caries development (Sreebny and Vissink 2010). In patients with severe salivary gland hypofunction, nonacidic fluoride gels and/or solutions should be used. Other potential anticariogenic formulations are casein phosphopeptides (CPPs) which have the ability to stabilize calcium and phosphate ions, thus creating the casein phosphopeptides with amorphous calcium phosphate (CPP-ACP) complex promoting the remineralization process, and phosphoryl oligosaccharides of calcium and commercially available fluoride-containing preparations of these (e.g., Tooth Mousse®).
Oral Candidosis
Patients with salivary gland hypofunction also have an increased risk of oral infections, particularly oral candidosis. This condition often assumes an erythematous form (without the easily recognized removable pseudomembranous plaques). The mucosa is red and the patients complain of a burning sensation of the oral mucosa, particularly the tongue, or a metallic taste or intensified feeling of xerostomia .
Conclusions and Future Directions
Xerostomia is defined as the subjective sensation of oral dryness and is usually associated with decreased saliva secretion, but may occur without objective salivary gland hypofunction. The principal causes of xerostomia and salivary gland hypofunction are various systemic diseases, the intake of a wide variety of medications, as well as adverse effects of cancer therapies, e.g., head and neck radiotherapy and cancer chemotherapy.
Hence, xerostomia is a common complaint, particularly in the elderly population. However, xerostomia does not appear to be related to age per se but rather to the fact that elderly people suffer from a higher number of systemic diseases and thus have a higher medication intake.
For adequate and timely diagnosis and management of xerostomia and salivary gland hypofunction, a thorough workup including patient history, clinical examination, and measurement of unstimulated and stimulated whole saliva flow rate is essential. Further diagnosis may include various imaging techniques, salivary gland biopsies, and blood tests. The diagnostic approach often requires an interdisciplinary collaboration.
However, in some cases, it is not possible to identify the potential underlying causes due to coexisting systemic diseases that may affect salivary gland function and the intake of potentially xerogenic medication or polypharmacy, and often it is limited to what can be done to alter the underlying cause. Still, in most cases, the symptoms and potential oral sequelae of salivary gland dysfunction can be alleviated to some extent. Current management strategies and symptomatic treatment should focus on ensuring that the patient is informed of salivary gland dysfunction, advice is given on methods to stimulate any secretory capacity of the salivary glands, and advice on adequate use of oral lubricants/saliva substitutes as well as prevention and treatment of dental caries and oral infections, in particular oral candidosis. A variety of newer management strategies under development include use of biologics, gene transfer, stem cell therapy, and different salivary gland-sparing approaches in radiation therapy for head and neck cancer.
Biologicals
Biologicals are currently used or tested in many autoimmune diseases including SS (Brito-Zeron et al. 2016). Of all clinical trials that have been conducted in primary SS, only few have evaluated the effect of treatment on extraglandular symptoms. This lack of data can be partially explained by (i) heterogeneity of extraglandular symptoms, (ii) inclusion of patients with low systemic disease activity in clinical trials, (iii) inclusion of a heterogeneous group of SS patients, and (iv) the former lack of validated outcome measures to evaluate systemic disease activity. These methodological issues should be addressed in future clinical trials. The ultimate goal in the management of primary SS is evidence-based and precision treatment of the broad range of symptoms experienced by patients suffering from this disease, including extraglandular symptoms (Verstappen et al. 2015; van Nimwegen et al. 2016; Bootsma et al. 2017) .
Gene Transfer
Depending on the total radiation dose to the salivary glands, few acinar cells survive radiation therapy leaving the salivary gland tissue with little residual capacity for primary fluid secretion; however, salivary duct cells are much less affected after irradiation. The therapeutic rationale of gene therapy for functional recovery of radiation-damaged salivary gland tissue is based on a possible insertion of a pathway for water transport in the remaining duct cell membranes to elicit water secretion. Phase 1 trials have been performed (ClinicalTrials.gov Identifier: NCT00372320 and Principal Investigator I.G.Alevizos 2014; ClinicalTrials.gov Identifier: NCT02446249 and Principal Investigator J.A.Chiorini 2015) .
Stem Cell Therapy
Another potential method to salvage salivary glands that are damaged by radiation is stem cell therapy (Vissink et al. 2015). Preclinical studies have shown that stem/progenitor cell transplantation not only rescues salivary gland secretion but also restores tissue homeostasis of the irradiated gland, necessary for long-term maintenance of adult tissue. Stem/progenitor cells might be harvested from salivary glands before start of radiotherapy and be returned to the salivary complex after radiotherapy has been completed. The salivary stem/progenitor cells might then repopulate the damaged salivary glands. Phase 1–2 trials are commencing testing stem cells harvested from different tissues, e.g., salivary gland stem cells and adipose-derived mesenchymal stem cells (Pringle et al. 2016; Gronhoj et al. 2017) .
Other Management Approaches Under Development
Each year 500,000 patients are treated with radiotherapy for head and neck cancer, resulting in relatively high survival rates. However, in 40% of patients, quality of life is severely compromised because of radiation-induced salivary gland hypofunction and consequent xerostomia (van Luijk et al. 2015). New radiation treatment technologies enable sparing of parts of the salivary glands. In mice, rats, and humans, it has been shown that stem and progenitor cells reside in the region of the parotid gland containing the major ducts. Minimizing the cumulative radiation dose on the region of the salivary gland containing the stem/progenitor cells is accompanied by better salivary gland function after radiation therapy (van Luijk et al. 2015).
Current methods to prevent damage are radiation techniques to reduce radiation injury to salivary gland tissue, as described above, surgical techniques to relocate salivary glands to a region receiving a lower cumulative radiation dose, and techniques to make salivary gland cells more resistant to radiation injury. These preventive techniques cannot be applied in all cases, may reduce tumor sensitivity, or do not result in a sufficient amelioration of dryness-related complaints. Stem cell therapy might help recover salivary gland function in those patients in whom other techniques have been unsuccessful (Vissink et al. 2015).
Cross-References
-
Diagnostic Imaging Principles and Applications in Head and Neck Pathology
-
Normal Variation in the Anatomy, Biology, and Histology of the Maxillofacial Region
-
Oral Manifestations of Systemic Diseases and Their Treatments
-
Soft and Hard Tissue Operative Investigations in the Diagnosis and Treatment of Oral Disease
References
Aberle AM, Abrams AM, Bowe R, Melrose RJ, Handlers JP. Lobular (polymorphous low-grade) carcinoma of minor salivary glands. A clinicopathologic study of twenty cases. Oral Surg Oral Med Oral Pathol. 1985;60:387–95.
Agha-Hosseini F, Shirzad N, Moosavi MS. Evaluation of Xerostomia and salivary flow rate in Hashimoto's thyroiditis. Med Oral Patol Oral Cir Bucal. 2016;21:e1–5.
Alajbeg I, Falcao DP, Tran SD, Martin-Granizo R, Lafaurie GI, Matranga D, Pejda S, Vuletic L, Mantilla R, Leal SC, Bezerra AC, Menard HA, Kimoto S, Pan S, Maniegas L, Krushinski CA, Melilli D, Campisi G, Paderni C, Mendoza GR, Yepes JF, Lindh L, Koray M, Mumcu G, Elad S, Zeevi I, Barrios BC, Lopez Sanchez RM, Lassauzay C, Fromentin O, Beiski BZ, Strietzel FP, Konttinen YT, Wolff A, Zunt SL. Intraoral electrostimulator for xerostomia relief: a long-term, multicenter, open-label, uncontrolled, clinical trial. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113:773–81.
Aliko A, Wolff A, Dawes C, Aframian D, Proctor G, Ekstrom J, Narayana N, Villa A, Sia YW, Joshi RK, McGowan R, Beier JS, Kerr AR, Lynge Pedersen AM, Vissink A. World workshop on oral medicine VI: clinical implications of medication-induced salivary gland dysfunction. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120:185–206.
Altemani AMT, Martins L, Freitas F, Soares NS, Araujo and VC Araujo. Carcinoma ex pleomorphic adenoma (CXPA): immunoprofile of the cells involved in carcinomatous progression. Histopathology. 2005;46:635–41.
Alvarez-Canas C, Rodilla IG. True malignant mixed tumor (carcinosarcoma) of the parotid gland. Report of a case with immunohistochemical study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 81:454–58.
Andreoli MT, Andreoli SM, Shrime MG, Devaiah AK. Radiotherapy in parotid acinic cell carcinoma: does it have an impact on survival? Arch Otolaryngol Head Neck Surg. 2012;138:463–6.
Ansai SH, Takeichi S, Arase S, Kawana and T Kimura. Sebaceous carcinoma: an immunohistochemical reappraisal. Am J Dermatopathol. 2011;33:579–87.
Antonelli G, Ceccato F, Artusi C, Marinova M, Plebani M. Salivary cortisol and cortisone by LC-MS/MS: validation, reference intervals and diagnostic accuracy in Cushing's syndrome. Clin Chim Acta. 2015;451:247–51.
Apple SK, Moatamed NA, Lai CK, Bhuta S. Sebaceous adenoma of the parotid gland: a case report with fine needle aspiration findings and histologic correlation. Acta Cytol. 2009;53:419–22.
Arcega RS, Feinstein AJ, Bhuta S, Blackwell KE, Rao NP, Pullarkat ST. An unusual initial presentation of mantle cell lymphoma arising from the lymphoid stroma of warthin tumor. Diagn Pathol. 2015;10:209.
Barbe AG, Bock N, Derman SH, Felsch M, Timmermann L, Noack MJ. Self-assessment of oral health, dental health care and oral health-related quality of life among Parkinson's disease patients. Gerodontology. 2017;34:135–43.
Bardow A, Vissink A. Saliva and caries development. In: Fejerskov O, Nyvad B, Kidd E, editors. Dental caries. The disease and its clinical management. Oxford: Wiley Blackwell; 2015. p. 83–106.
Bardow A, Nyvad B, Nauntofte B. Relationships between medication intake, complaints of dry mouth, salivary flow rate and composition, and the rate of tooth demineralization in situ. Arch Oral Biol. 2001;46:413–23.
Bassim CW, Fassil H, Mays JW, Edwards D, Baird K, Steinberg SM, Cowen EW, Naik H, Datiles M, Stratton P, Gress RE, Pavletic SZ. Oral disease profiles in chronic graft versus host disease. J Dent Res. 2015;94:547–54.
Bezerra TM, Monteiro BV, Henriques AC, de Vasconcelos CM, Nonaka CF, da Costa Miguel MC. Epidemiological survey of mucus extravasation phenomenon at an oral pathology referral center during a 43 year period. Braz J Otorhinolaryngol. 2016;82:536–42.
Bishop JA. Unmasking MASC: bringing to light the unique morphologic, immunohistochemical and genetic features of the newly recognized mammary analogue secretory carcinoma of salivary glands. Head Neck Pathol. 2013;7:35–9.
Blasco PA, Allaire JH. Drooling in the developmentally disabled: management practices and recommendations. Consortium on drooling. Dev Med Child Neurol. 1992;34:849–62.
Bootsma H, Kroese FGM, Vissink A. Rituximab in the treatment of Sjögren's syndrome: is it the wrong drug? Arthritis Rheumatol. 2017;69(7):1346–49.
Bowman SJ, Everett CC, O'Dweyer JL, Emery P, Pitzalis C, Ng WF. Randomized controlled trial and cost-effectiveness analysis in treating fatigue and oral dryness in primary Sjögren's syndrome. Arthritis Rheumatol. 2017; 69(7):1440–50.
Brandwein-Gensler MJ, Hille BY, Wang M, Urken R, Gordon LJ, Wang JR Simpson RH, Gnepp DR. Low-grade salivary duct carcinoma: description of 16 cases. Am J Surg Pathol. 2004;28:1040–44.
Brannon RB, Sciubba JJ, Giulani M. Ductal papillomas of salivary gland origin: a report of 19 cases and a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:68–77.
Brierley JD, Gospodarowicz MK,Wittekind C. TNM classification of malignant tumours. Union for International Cancer Control; 2017, London.
Brito-Zeron P, Siso-Almirall A, Bove A, Kostov BA, Ramos-Casals M. Primary Sjogren syndrome: an update on current pharmacotherapy options and future directions. Expert Opin Pharmacother. 2013;14:279–89.
Brito-Zeron P, Retamozo S, Gheitasi H, Ramos-Casals M. Treating the underlying pathophysiology of primary Sjogren syndrome: recent advances and future prospects. Drugs. 2016;76:1601–23.
Brito-Zeron P, Kostov B, Fraile G, Caravia-Duran D, Maure B, Rascon FJ, Zamora M, Casanovas A, Lopez-Dupla M, Ripoll M, Pinilla B, Fonseca E, Akasbi M, de la Red G, Duarte-Millan MA, Fanlo P, Guisado-Vasco P, Perez-Alvarez R, Chamorro AJ, Morcillo C, Jimenez-Heredia I, Sanchez-Berna I, Lopez-Guillermo A, Ramos-Casals M. Characterization and risk estimate of cancer in patients with primary Sjogren syndrome. J Hematol Oncol. 2017;10:90.
Brook I. The bacteriology of salivary gland infections. Oral Maxillofac Surg Clin North Am. 2009;21:269–74.
Buchner A, Merrell PW, Carpenter WM. Relative frequency of intra-oral minor salivary gland tumors: a study of 380 cases from northern California and comparison to reports from other parts of the world. J Oral Pathol Med. 2007;36:207–14.
Bunker ML, Locker J. Warthin's tumor with malignant lymphoma. DNA analysis of paraffin-embedded tissue. Am J Clin Pathol. 1989;91:341–4.
Castle JT, Thompson LD, Frommelt RA, Wenig BM, Kessler HP. Polymorphous low grade adenocarcinoma: a clinicopathologic study of 164 cases. Cancer. 1999;86:207–19.
Catano JC, Robledo J. Tuberculous lymphadenitis and parotitis. Microbiol Spectr. 2016;4(6): https://doi.org/10.1128/microbiolspec.TNMI7-0008-2016.
Chen AM, Lau VH, Farwell DG, Luu Q, Donald PJ. Mucoepidermoid carcinoma of the parotid gland treated by surgery and postoperative radiation therapy: clinicopathologic correlates of outcome. Laryngoscope. 2013;123:3049–55.
ClinicalTrials.gov Identifier: NCT00372320 and Principal Investigator I.G.Alevizos. Effect of AdhAQP1 on salivary flow in patients treated with radiation for head and neck cancer. [The study has been completed]. 19–3-2014. Bethesda, National Institute of Dental and Craniofacial Research (NIDCR).
ClinicalTrials.gov Identifier: NCT02446249 and Principal Investigator J.A.Chiorini. Safety of a single administration of AAV2hAQP1, an Adeno-Associated Viral Vector Encoding Human Aquaporin-1 to One Parotid Salivary Gland in People With Irradiation-Induced Parotid Salivary Hypofunction. [The study is currently recruiting participants, Study Start Date: 30 Apr 2015, Estimated Study Completion Date: 1 Nov 2022]. 30–4-2015. Bethesda, National Institute of Dental and Craniofacial Research (NIDCR).
Crama-Bohbouth G, Pena AS, Verspaget HW, vd ZA, Biemond I, Weterman IT, Lamers CB. Immunological findings in whole and parotid saliva of patients with ulcerative colitis and healthy controls. Hepato-Gastroenterology. 1989;36:185–7.
Croitoru CM, Mooney JE, Luna MA. Sebaceous lymphadenocarcinoma of salivary glands. Ann Diagn Pathol. 2003;7:236–9.
Dardick I, Thomas MJ, van Nostrand AW. Myoepithelioma – new concepts of histology and classification: a light and electron microscopic study. Ultrastruct Pathol. 1989;13:187–224.
Dardick I, Ostrynski VL, Ekem JK, Leung R, Burford-Mason AP. Immunohistochemical and ultrastructural correlates of muscle-actin expression in pleomorphic adenomas and myoepitheliomas based on comparison of formalin and methanol fixation. Virchows Arch A Pathol Anat Histopathol. 1992;421:95–104.
Davies H, Bagg J, Goodchild MC, McPherson MA. Examination of submandibular fluid in cystic fibrosis. Acta Univ Carol [Med ] (Praha). 1990;36:84–5.
Davies AN, Broadley K, Beighton D. Xerostomia in patients with advanced cancer. J Pain Symptom Manag. 2001;22:820–5.
Davis PB. Pathophysiology of cystic fibrosis with emphasis on salivary gland involvement. J Dent Res. 1987;66:667–71.
Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66:648–53.
Dawes C, Pedersen AM, Villa A, Ekstrom J, Proctor GB, Vissink A, Aframian D, McGowan R, Aliko A, Narayana N, Sia YW, Joshi RK, Jensen SB, Kerr AR, Wolff A. The functions of human saliva: a review sponsored by the world workshop on oral medicine VI. Arch Oral Biol. 2015;60:863–74.
de Moura SA, de Sousa JM, Lima DF, Negreiros AN, Silva FV, da Costa LJ. Burning mouth syndrome (BMS): sialometric and sialochemical analysis and salivary protein profile. Gerodontology. 2007;24:173–6.
De VS, Quartuccio L, Seror R, Salvin S, Ravaud P, Fabris M, Nocturne G, Gandolfo S, Isola M, Mariette X. Efficacy and safety of belimumab given for 12 months in primary Sjogren's syndrome: the BELISS open-label phase II study. Rheumatology (Oxford). 2015;54:2249–56.
Delgado R, Klimstra D, Albores-Saavedra J. Low grade salivary duct carcinoma. A distinctive variant with a low grade histology and a predominant intraductal growth pattern. Cancer. 1996;78:958–67.
Delli K, Dijkstra PU, Stel AJ, Bootsma H, Vissink A, Spijkervet FK. Diagnostic properties of ultrasound of major salivary glands in Sjogren's syndrome: a meta-analysis. Oral Dis. 2015;21:792–800.
Devauchelle-Pensec V, Mariette X, Jousse-Joulin S, Berthelot JM, Perdriger A, Puechal X, Le GV, Sibilia J, Gottenberg JE, Chiche L, Hachulla E, Hatron PY, Goeb V, Hayem G, Morel J, Zarnitsky C, Dubost JJ, Pers JO, Nowak E, Saraux A. Treatment of primary Sjogren syndrome with rituximab: a randomized trial. Ann Intern Med. 2014;160:233–42.
Dormenval V, Budtz-Jorgensen E, Mojon P, Bruyere A, Rapin CH. Associations between malnutrition, poor general health and oral dryness in hospitalized elderly patients. Age Ageing. 1998;27:123–8.
Dost F, Farah CS. Stimulating the discussion on saliva substitutes: a clinical perspective. Aust Dent J. 2013;58:11–7.
Dynesen AW, Bardow A, Petersson B, Nielsen LR, Nauntofte B. Salivary changes and dental erosion in bulimia nervosa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:696–707.
Ekstrand T. Bell's palsy; prognostic accuracy of case history, sialometry and taste impairment. Clin Otolaryngol Allied Sci. 1979;4:183–96.
Ekstrom J, Khosravani N, Castagnola M, Messana I. Saliva and the control of its secretion. In: Ekberg O, editor. Dysphagia: diagnosis and treatment. Berlin/Heidelberg: Springer; 2012. p. 19–47.
Eliasson L, Carlen A. An update on minor salivary gland secretions. Eur J Oral Sci. 2010;118:435–42.
Ellis GL, Corio RL. Acinic cell adenocarcinoma. A clinicopathologic analysis of 294 cases. Cancer. 1983;52:542–9.
Ellis GL, Wiscovitch JG. Basal cell adenocarcinomas of the major salivary glands. Oral Surg Oral Med Oral Pathol.1990;69:461–9.
Epstein JB, Jensen SB. Management of Hyposalivation and Xerostomia: criteria for treatment strategies. Compend Contin Educ Dent. 2015;36:600–3.
Ethunandan M, Pratt CA, Macpherson DW. Changing frequency of parotid gland neoplasms—analysis of 560 tumours treated in a district general hospital. Ann R Coll Surg Engl. 2002;84:1–6.
Fantasia JE, Nocco CE, Lally ET. Ultrastructure of sialadenoma papilliferum. Arch Pathol Lab Med. 1986;110:523–527.
Farah CS, Savage NW. Cryotherapy for treatment of oral lesions. Aust Dent J. 2006;51:2–5.
Fedorova T, Knudsen CS, Mouridsen K, Nexo E, Borghammer P. Salivary acetylcholinesterase activity is increased in Parkinson's disease: a potential marker of parasympathetic dysfunction. Parkinsons Dis. 2015;2015:156479.
Fonseca I, Soares J. Epithelial-myoepithelial carcinoma of the salivary glands. A study of 22 cases. Virchows Arch A Pathol Anat Histopathol. 1993;422:389–96.
Foschini MP, Malvi D, Betts CM. Oncocytic carcinoma arising in Warthin tumour. Virchows Arch. 2005;446:88–90.
Foss RD, Ellis GL, Auclair PL. Salivary gland cystadenocarcinomas. A clinicopathologic study of 57 cases. Am J Surg Pathol. 1996;20:1440–7.
Fox RI. Sjogren's syndrome. Lancet. 2005;366:321–31.
Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 1987;115:581–4.
Frierson HF Jr, Mills SE, Garland TA. Terminal duct carcinoma of minor salivary glands. A nonpapillary subtype of polymorphous low-grade adenocarcinoma. Am J Clin Pathol. 1985;84:8–14.
Fujibayashi T, Sugai S, Miyasaka N, Hayashi Y, Tsubota K. Revised Japanese criteria for Sjogren's syndrome (1999): availability and validity. Mod Rheumatol. 2004;14:425–34.
Furness S, Bryan G, McMillan R, Worthington HV. Interventions for the management of dry mouth: non-pharmacological interventions. Cochrane Database Syst Rev. 2013;8. https://doi.org/10.1002/14651858.CD009603.pub3.
Gallo A, Benazzo M, Capaccio P, De CL, De VM, Fusconi M, Martellucci S, Paludetti G, Pasquini E, Puxeddu R, Speciale R. Sialoendoscopy: state of the art, challenges and further perspectives. Round table, 101(st) SIO National Congress, Catania 2014. Acta Otorhinolaryngol Ital. 2015;35:217–33.
Gnepp DR. My journey into the world of salivary gland sebaceous neoplasms. Head Neck Pathol. 2012;6:101–10.
Griffith CC, Thompson LD, Assaad A, Purgina BM, Lai C, Bauman JE, Weinreb I, Seethala RR, Chiosea SI. Salivary duct carcinoma and the concept of early carcinoma ex pleomorphic adenoma. Histopathology. 2014;65:854–60.
Gronhoj C, Jensen DH, Glovinski PV, Jensen SB, Bardow A, Oliveri RS, Specht L, Thomsen C, Darkner S, Kiss K, Fischer-Nielsen A, First-in-man v BC. Mesenchymal stem cells for radiation-induced xerostomia (MESRIX): study protocol for a randomized controlled trial. Trials. 2017;18:108.
Grossmann SM, Teixeira R, Oliveira GC, Gleber-Netto FO, Araujo FM, Araujo FM, Carmo MA. Xerostomia, hyposalivation and sialadenitis in patients with chronic hepatitis C are not associated with the detection of HCV RNA in saliva or salivary glands. J Clin Pathol. 2010;63:1002–7.
Ha WN, Kelloway E, Dost F, Farah CSA. Retrospective analysis of oral and maxillofacial pathology in an Australian paediatric population. Aust Dent J. 2014;59:221–5.
Hakansson U, Jacobsson L, Lilja B, Manthorpe R, Henriksson V. Salivary gland scintigraphy in subjects with and without symptoms of dry mouth and/or eyes, and in patients with primary Sjogren's syndrome. Scand J Rheumatol. 1994;23:326–33.
Harrington N, Barry PJ, Barry SM. Dental treatment for people with cystic fibrosis. Eur Arch Paediatr Dent. 2016;17:195–203.
Harrison T, Bigler L, Tucci M, Pratt L, Malamud F, Thigpen JT, Streckfus C, Younger H. Salivary sIgA concentrations and stimulated whole saliva flow rates among women undergoing chemotherapy for breast cancer: an exploratory study. Spec Care Dentist. 1998;18:109–12.
Helenius LM, Meurman JH, Helenius I, Kari K, Hietanen J, Suuronen R, Hallikainen D, Kautiainen H, Leirisalo-Repo M, Lindqvist C. Oral and salivary parameters in patients with rheumatic diseases. Acta Odontol Scand. 2005;63:284–93.
Hunt L, Hensor EM, Nam J, Burska AN, Parmar R, Emery P, Ponchel FT. Cell subsets: an immunological biomarker to predict progression to clinical arthritis in ACPA-positive individuals. Ann Rheum Dis. 2016;75:1884–9.
Inenaga K, Ono K, Hitomi S, Kuroki A, Ujihara I. Thirst sensation and oral dryness following alcohol intake. Jpn Dent Sci Rev. 2017;53:78–85.
Iro H, Zenk J. Salivary gland diseases in children. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2014;13:Doc06.
Izutsu KT, Sullivan KM, Schubert MM, Truelove EL, Shulman HM, Sale GE, Morton TH, Rice JC, Witherspoon RP, Storb R, Thomas ED. Disordered salivary immunoglobulin secretion and sodium transport in human chronic graft-versus-host disease. Transplantation. 1983;35:441–6.
Janssen KM, Vissink A, de Smit MJ, Westra J, Brouwer E. Lessons to be learned from periodontitis. Curr Opin Rheumatol. 2013;25:241–7.
Jensen SB, Mouridsen HT, Reibel J, Brünner N, Nauntofte B. Adjuvant chemotherapy in breast cancer patients induces temporary salivary gland hypofunction. Oral Oncol. 2008;44:162–73.
Jensen SB, Pedersen AML, Vissink A, Andersen E, Brown CG, Davies AN, Dutilh J, Fulton JS, Jankovic L, Lopes NNF, Mello ALS, Muniz LV, Murdoch-Kinch CA, Nair RG, Napeñas JJ, Nogueira-Rodrigues A, Saunders D, Stirling B, von Bültzingslöwen I, Weikel DS, Elting LS, Spijkervet FKL, Brennan MTA. Systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support Care Cancer. 2010;18:1039–60.
Jongerius PH, Joosten F, Hoogen FJ, Gabreels FJ, Rotteveel JJ. The treatment of drooling by ultrasound-guided intraglandular injections of botulinum toxin type a into the salivary glands. Laryngoscope. 2003;113:107–11.
Jousse-Joulin S, Milic V, Jonsson MV, Plagou A, Theander E, Luciano N, Rachele P, Baldini C, Bootsma H, Vissink A, Hocevar A, De VS, Tzioufas AG, Alavi Z, Bowman SJ, Devauchelle-Pensec VI. Salivary gland ultrasonography a useful tool in Sjogren's syndrome? A systematic review. Rheumatology (Oxford). 2016;55:789–800.
Juusela P, Tanskanen M, Nieminen A, Kari K, Suominen L, Uitto VJ, Kiuru-Enari S. Xerostomia in hereditary gelsolin amyloidosis. Amyloid. 2013;20:39–44.
Kalk WW, Vissink A, Spijkervet FK, Bootsma H, Kallenberg CG, Nieuw Amerongen AV. Sialometry and sialochemistry: diagnostic tools for Sjogren's syndrome. Ann Rheum Dis. 2001;60:1110–6.
Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2015;385:1460–71.
Katz J, Shenkman A, Stavropoulos F, Melzer E. Oral signs and symptoms in relation to disease activity and site of involvement in patients with inflammatory bowel disease. Oral Dis. 2003;9:34–40.
Kelloway E, Ha WN, Dost F, Farah CSA. Retrospective analysis of oral and maxillofacial pathology in an Australian adult population. Aust Dent J. 2014;59:215–20.
Kerr GD, Sellars C, Bowie L, Bagg J, Sweeney MP, Langhorne P, Stott DJ. Xerostomia after acute stroke. Cerebrovasc Dis. 2009;28:624–6.
Kimple AJ, Austin GK, Shah RN, Welch CM, Funkhouser WK, Zanation AM, Shockley WW. Polymorphous low-grade adenocarcinoma: a case series and determination of recurrence. Laryngoscope. 2014;124:2714–9.
Klein Hesselink EN, Links TP. Radioiodine treatment and thyroid hormone suppression therapy for differentiated thyroid carcinoma: adverse effects support the trend toward less aggressive treatment for low-risk patients. Eur Thyroid J. 2015;4:82–92.
Klein Hesselink EN, Brouwers AH, de Jong JR, van der Horst-Schrivers AN, Coppes RP, Lefrandt JD, Jager PL, Vissink A, Links TP. Effects of radioiodine treatment on salivary gland function in patients with differentiated thyroid carcinoma: a prospective study. J Nucl Med. 2016;57:1685–91.
Kubota Y, Kubo C Mori Y. Sialadenoma papilliferum of the hard palate: a case report. J Oral Maxillofac Surg. 2012;70:1609–12.
Kuo YJ, Weinreb I, Perez-Ordonez B. Low-grade salivary duct carcinoma or low-grade intraductal carcinoma? Review of the literature. Head Neck Pathol. 2013;7 Suppl 1: S59-67.
Lagerlof F, Oliveby A. Caries-protective factors in saliva. Adv Dent Res. 1994;8:229–38.
Lai G, Nemolato S, Lecca S, Parodo G, Medda C, Faa G. The role of immunohistochemistry in the diagnosis of hyalinizing clear cell carcinoma of the minor salivary gland: a case report. Eur J Histochem. 2008;52:251–4.
Lajer C, Buchwald C, Nauntofte B, Specht L, Bardow A, Jensdottir T. Erosive potential of saliva stimulating tablets with and without fluoride in irradiated head and neck cancer patients. Radiother Oncol. 2009;93:534–8.
Lee AC, Lim WL, So KT. Epstein-Barr virus associated parotitis. J Paediatr Child Health. 1997;33:177–8.
Leerdam CM, Martin HC, Isaacs D. Recurrent parotitis of childhood. J Paediatr Child Health. 2005;41:631–4.
Lenander-Lumikari M, Loimaranta V. Saliva and dental caries. Adv Dent Res. 2000;14:40–7.
Lexner MO, Bardow A, Hertz JM, Almer L, Nauntofte B, Kreiborg S. Whole saliva in X-linked hypohidrotic ectodermal dysplasia. Int J Paediatr Dent. 2007;17:155–62.
Li LJ. Clinical analysis of salivary gland tumor cases in West China in past 50 years. Oral Oncol. 2014;44:187–92.
Lin AL, Johnson DA, Stephan KT, Yeh CK. Alteration in salivary function in early HIV infection. J Dent Res. 2003;82:719–24.
Liu G, He J, Zhang C, Fu S, He Y. Lymphadenoma of the salivary gland: report of 10 cases. Oncol Lett. 2014;7:1097–101.
Lopez-Pintor RM, Casanas E, Gonzalez-Serrano J, Serrano J, Ramirez L, de Arriba L, Hernandez G. Xerostomia, Hyposalivation, and salivary flow in diabetes patients. J Diabetes Res. 2016;2016:4372852.
Loyola Rodriguez JP, Galvan Torres LJ, Martinez Martinez RE, Abud MC, Medina Solis CE, Ramos CS, Garcia Cortes JO, Dominguez Perez RA. Frequency of dental caries in active and inactive systemic lupus erythematous patients: salivary and bacterial factors. Lupus. 2016;25:1349–56.
Machado RA, Moubayed SP, Khorsandi A, Hernandez-Prera JC, Urken ML. Intermittent facial spasms as the presenting sign of a recurrent pleomorphic adenoma. World J Clin Oncol. 2017;8:86–90.
Mahajan D, Khurana N, Setia N. Sialadenoma papilliferum in a young patient: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:e51-54.
Maiorano E, et al. Sialadenoma papilliferum: an immunohistochemical study of five cases. J Oral Pathol Med. 1996;25(6):336–42.
Majewska H, Skálová A, Stodulski D, Klimková A, Steiner P, Stankiewicz C, Biernat W. Mammary analogue secretory carcinoma of salivary glands: a new entity associated with ETV6 gene rearrangement. Virchows Arch. 2015;466(3):245–54. https://doi.org/10.1007/s00428-014-1701-8.
Malicka B, Kaczmarek U, Skoskiewicz-Malinowska K. Prevalence of xerostomia and the salivary flow rate in diabetic patients. Adv Clin Exp Med. 2014;23:225–33.
Mang FW, Michieletti P, O'Rourke K, Cauch-Dudek K, Diamant N, Bookman A, Heathcote J. Primary biliary cirrhosis, sicca complex, and dysphagia. Dysphagia. 1997;12:167–70.
Manteghi A, Zwillenberg S, Arguello-Guerra V. Sebaceous carcinoma of the parotid gland: a case report and review of the literature. Ear Nose Throat J. 2014;93:E29–32.
McHugh JB, Hoschar AP, Dvorakova M, Parwani AV, Barnes EL, Seethala RR. p63 immunohistochemistry differentiates salivary gland oncocytoma and oncocytic carcinoma from metastatic renal cell carcinoma. Head Neck Pathol. 2007;1:123–31.
McNamara ZJ, Batstone M, Farah CS. Carcinoma ex pleomorphic adenoma in a minor salivary gland of the upper lip. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e51–3.
Meijer JM, Schonland SO, Palladini G, Merlini G, Hegenbart U, Ciocca O, Perfetti V, Leijsma MK, Bootsma H, Hazenberg BP. Sjogren's syndrome and localized nodular cutaneous amyloidosis: coincidence or a distinct clinical entity? Arthritis Rheum. 2008;58:1992–9.
Meijer JM, Meiners PM, Vissink A, Spijkervet FK, Abdulahad W, Kamminga N, Brouwer E, Kallenberg CG, Bootsma H. Effectiveness of rituximab treatment in primary Sjogren's syndrome: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2010;62:960–8.
Meiners PM, Meijer JM, Vissink A, Bootsma H. Management of Sjögren's syndrome. In: Weisman MH, Weinblatt ME, Louie JS, van Vollenhoven R, editors. Targeted treatment of the rheumatic diseases. Philadelphia: Saunders; 2010. p. 133–55.
Meiners PM, Vissink A, Kroese FG, Spijkervet FK, Smitt-Kamminga NS, Abdulahad WH, Bulthuis-Kuiper J, Brouwer E, Arends S, Bootsma H. Abatacept treatment reduces disease activity in early primary Sjogren's syndrome (open-label proof of concept ASAP study). Ann Rheum Dis. 2014;73:1393–6.
Meurman JH, Laine P, Keinanen S, Pyrhonen S, Teerenhovi L, Lindqvist C. Five-year follow-up of saliva in patients treated for lymphomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:447–52.
Milchgrub S, Gnepp DR, Vuitch F, Delgado R, Albores-Saavedra J. Hyalinizing clear cell carcinoma of salivary gland. Am J Surg Pathol. 1994;18:74–82.
Moerman RV, Bootsma H, Kroese FG, Vissink A. Sjogren's syndrome in older patients: aetiology, diagnosis and management. Drugs Aging. 2013;30:137–53.
Montecchi PP, Custureri V, Polimeni A, Cordaro M, Costa L, Marinucci S, Montecchi F. Oral manifestations in a group of young patients with anorexia nervosa. Eat Weight Disord. 2003;8:164–7.
Mossel E, Delli K, van Nimwegen JF, Stel AJ, Kroese FGM, Spijkervet FKL, Vissink A, Arends S, Bootsma H. Ultrasonography of major salivary glands compared with parotid and labial gland biopsy and classification criteria in patients with clinically suspected primary Sjogren's syndrome. Ann Rheum Dis 2017; https://doi.org/10.1136/annrheumdis-2017-211250.
Muralidharan D, Fareed N, Pradeep PV, Margabandhu S, Ramalingam K, Ajith Kumar BV. Qualitative and quantitative changes in saliva among patients with thyroid dysfunction prior to and following the treatment of the dysfunction. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:617–23.
Murray TW, Poulton R, Mark BJ, Al-Kubaisy S. Xerostomia and medications among 32-year-olds. Acta Odontol Scand. 2006;64:249–54.
Nagao T, Sugano I, Ishida Y, Tajima Y, Furuya N, Kondo Y, Nagao K. Mucoepidermoid carcinoma arising in Warthin's tumour of the parotid gland: report of two cases with histopathological, ultrastructural and immunohistochemical studies. Histopathology. 1998;33:379–86.
Nagler RM, Nagler A. Sialometrical and sialochemical analysis of patients with chronic graft-versus-host disease—a prolonged study. Cancer Investig. 2003;21:34–40.
Napenas JJ, Miles L, Guajardo-Streckfus C, Streckfus CF. Salivary flow rates among women diagnosed with benign and malignant tumors. Spec Care Dentist. 2013;33:102–10.
Narhi TO, Meurman JH, Ainamo A, Nevalainen JM, Schmidt-Kaunisaho KG, Siukosaari P, Valvanne J, Erkinjuntti T, Tilvis R, Makila E. Association between salivary flow rate and the use of systemic medication among 76-, 81-, and 86-year-old inhabitants in Helsinki, Finland. J Dent Res. 1992;71:1875–80.
Navazesh M, Christensen CMA. Comparison of whole mouth resting and stimulated salivary measurement procedures. J Dent Res. 1982;61:1158–62.
Navazesh M, Wood GJ, Brightman VJ. Relationship between salivary flow rates and Candida Albicans counts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:284–8.
Navazesh M, Mulligan R, Barron Y, Redford M, Greenspan D, Alves M, Phelan J. A 4-year longitudinal evaluation of xerostomia and salivary gland hypofunction in the Women's interagency HIV study participants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:693–8.
Nielen MM, van Schaardenburg D, Reesink HW, van de Stadt RJ, van der Horst-Bruinsma IE, de Koning MH, Habibuw MR, Vandenbroucke JP, Dijkmans BA. Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum. 2004;50:380–6.
Nieto-Gonzalez JC, Monteagudo I, Bello N, Martinez-Estupinan L, Naredo E, Carreno L. Salivary gland ultrasound in children: a useful tool in the diagnosis of juvenile Sjogren's syndrome. Clin Exp Rheumatol. 2014;32:578–80.
Nikitakis NG, Tosios KI, Papanikolaou VS, Rivera H, Papanicolaou SI, Ioffe OB. Immunohistochemical expression of cytokeratins 7 and 20 in malignant salivary gland tumors. Mod Pathol. 2004;17:407–15.
Noaiseh G, Baker JF, Vivino FB. Comparison of the discontinuation rates and side-effect profiles of pilocarpine and cevimeline for xerostomia in primary Sjogren's syndrome. Clin Exp Rheumatol. 2014;32:575–7.
Noseri H, Erden T, Toros S, Habesoglu M, Egeli E, Aker F, Cetin S. Intraductal papilloma of the parotid gland in a child. Eur Arch Otorhinolaryngol. 2007;264:1385–6.
Patel DK, Morton RP. Demographics of benign parotid tumours: Warthin's tumour versus other benign salivary tumours. Acta Otolaryngol. 2016;136:83–6.
Patel TD, Vazquez A, Marchiano E, Park RC, Baredes S, Eloy JA. Polymorphous low-grade adenocarcinoma of the head and neck: a population-based study of 460 cases. Laryngoscope. 2015;125:1644–9.
Pedersen AM, Bardow A, Jensen SB, Nauntofte B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis. 2002;8:117–29.
Pedersen AML, Dynesen AW, Jensen SB. Udredning af xerostomi og hyposalivation. Tandlægebladet [in Danish] 2011;115:374–382.
Peric T, Markovic D, Petrovic B, Radojevic V, Todorovic T, Radicevic BA, Heinemann RJ, Susic G, Popadic AP, Spiric VT. Efficacy of pastes containing CPP-ACP and CPP-ACFP in patients with Sjogren's syndrome. Clin Oral Investig. 2015;19:2153–65.
Perumal CJ, Meyer M, Mohamed AA. Giant pleomorphic adenoma of the submandibular salivary gland: a case report. Craniomaxillofac Trauma Reconstr. 2012;5:185–8.
Pijpe J, Kalk WW, van der Wal JE, Vissink A, Kluin PM, Roodenburg JL, Bootsma H, Kallenberg CG, Spijkervet FK. Parotid gland biopsy compared with labial biopsy in the diagnosis of patients with primary Sjogren's syndrome. Rheumatology (Oxford). 2007;46:335–41.
Pimentel MT, López Amado M, García Sarandeses A. Recurrent sialadenoma papilliferum of the buccal mucosa. J Laryngol Otol. 1995;109:787–90.
Pires FR, Pringle GA, de Almeida OP, Chen SY. Intra-oral minor salivary gland tumors: a clinicopathological study of 546 cases. Oral Oncol. 43(5):463–70.
Pollard RP, Pijpe J, Bootsma H, Spijkervet FK, Kluin PM, Roodenburg JL, Kallenberg CG, Vissink A, van Imhoff GW. Treatment of mucosa-associated lymphoid tissue lymphoma in Sjogren's syndrome: a retrospective clinical study. J Rheumatol. 2011;38:2198–208.
Pringle S, Maimets M, van der Zwaag M, Stokman MA, van Gosliga D, Zwart E, Witjes MJ, de Haan G, van Os R, Coppes RP. Human salivary gland stem cells functionally restore radiation damaged salivary glands. Stem Cells. 2016;34:640–52.
Proctor GB, Carpenter GH. Regulation of salivary gland function by autonomic nerves. Auton Neurosci. 2007;133:3–18.
Prokaeva T, Spencer B, Kaut M, Ozonoff A, Doros G, Connors LH, Skinner M, Seldin DC. Soft tissue, joint, and bone manifestations of AL amyloidosis: clinical presentation, molecular features, and survival. Arthritis Rheum. 2007;56:3858–68.
Puhakka A, Forssell H, Soinila S, Virtanen A, Roytta M, Laine M, Tenovuo O, Teerijoki-Oksa T, Jaaskelainen SK. Peripheral nervous system involvement in primary burning mouth syndrome—results of a pilot study. Oral Dis. 2016;22:338–44.
Qin B, Wang J, Yang Z, Yang M, Ma N, Huang F, Zhong R. Epidemiology of primary Sjogren's syndrome: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74:1983–9.
Quer M, Vander PV, Takes RP, Silver CE, Boedeker CC, de Bree R, Rinaldo A, Sanabria A, Shaha AR, Pujol A, Zbaren P, Ferlito A. Surgical options in benign parotid tumors: a proposal for classification. Eur Arch Otorhinolaryngol 2017;274:3825.
Ramos-Casals M, Brito-Zeron P, Garcia-Carrasco M, Font J. Sarcoidosis or Sjogren syndrome? Clues to defining mimicry or coexistence in 59 cases. Medicine (Baltimore). 2004;83:85–95.
Rantapaa-Dahlqvist S. What happens before the onset of rheumatoid arthritis? Curr Opin Rheumatol. 2009;21:272–8.
Regelink G, Vissink A, Reintsema H, Nauta JM. Efficacy of a synthetic polymer saliva substitute in reducing oral complaints of patients suffering from irradiation-induced xerostomia. Quintessence Int. 1998;29:383–8.
Restituto P, Galofre JC, Gil MJ, Mugueta C, Santos S, Monreal JI, Varo N. Advantage of salivary cortisol measurements in the diagnosis of glucocorticoid related disorders. Clin Biochem. 2008;41:688–92.
Rhodus NL, Fricton J, Carlson P, Messner R. Oral symptoms associated with fibromyalgia syndrome. J Rheumatol. 2003;30:1841–5.
Ruiz E, Alegre J, Garcia Quintana AM, Aliste L, Blazquez A, de Sevilla TF. Chronic fatigue syndrome: study of a consecutive series of 824 cases assessed in two specialized units. Rev Clin Esp. 2011;211:385–90.
Saeves R, Nordgarden H, Storhaug K, Sandvik L, Espelid I. Salivary flow rate and oral findings in Prader-Willi syndrome: a case-control study. Int J Paediatr Dent. 2012;22:27–36.
Salaffi F, Argalia G, Carotti M, Giannini FB, Palombi C. Salivary gland ultrasonography in the evaluation of primary Sjogren's syndrome. Comparison with minor salivary gland biopsy. J Rheumatol. 2000;27:1229–36.
Santos MT, Guare R, Leite M, Ferreira MC, Nicolau J. Does the neuromotor abnormality type affect the salivary parameters in individuals with cerebral palsy? J Oral Pathol Med. 2010;39:770–4.
Sciubba JJ, Brannon RB. Myoepithelioma of salivary glands: Report of 23 cases. Cancer. 1982;49:562–72.
Seethala RR, Thompson LD, Gnepp DR, Barnes EL, Skalova A, Montone K, Kane S, Lewis JS Jr, Solomon LW, Simpson RH, Khan A, Prasad ML. Lymphadenoma of the salivary gland: clinicopathological and immunohistochemical analysis of 33 tumors. Mod Pathol. 2012;25:26–35.
Sheetal A, Hiremath VK, Patil AG, Sajjansetty S, Kumar SR. Malnutrition and its oral outcome - a review. J Clin Diagn Res. 2013;7:178–80.
Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, Rasmussen A, Scofield H, Vitali C, Bowman SJ, Mariette X. 2016 American College of Rheumatology/European league against rheumatism classification criteria for primary Sjogren's syndrome: a consensus and data-driven methodology involving three international patient cohorts. Ann Rheum Dis. 2017;76:9–16.
Ship JA, Fischer DJ. The relationship between dehydration and parotid salivary gland function in young and older healthy adults. J Gerontol A Biol Sci Med Sci. 1997;52:M310–9.
Ship JA, DeCarli C, Friedland RP, Baum BJ. Diminished submandibular salivary flow in dementia of the Alzheimer type. J Gerontol. 1990;45:M61–6.
Silvestre-Rangil J, Bagan L, Silvestre FJ, Bagan JV. Oral manifestations of rheumatoid arthritis. A cross-sectional study of 73 patients. Clin Oral Investig. 2016;20:2575–80.
Sirois DA, Natelson B. Clinicopathological findings consistent with primary Sjogren's syndrome in a subset of patients diagnosed with chronic fatigue syndrome: preliminary observations. J Rheumatol. 2001;28:126–31.
Skalova A. Mammary analogue secretory carcinoma of salivary gland origin: an update and expanded morphologic and immunohistochemical spectrum of recently described entity. Head Neck Pathol. 2013;7 Suppl 1:S30-36.
Skalova A, Michal M, Nathansky Z. Epidermoid carcinoma arising in Warthin's tumour: a case study. J Oral Pathol Med. 1994;23:330–3.
Skalova A, Vanecek T, Sima R, Laco J, Weinreb I, Perez-Ordonez B, Starek I, Geierova M, Simpson RH, Passador-Santos F, Ryska A, Leivo I, Kinkor Z, Michal M. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010;34:599–608.
Smidt D, Torpet L A, Nauntofte B, Heegaard K M, Pedersen A M. Associations between oral and ocular dryness, labial and whole salivary flow rates, systemic diseases and medications in a sample of older people. Community Dent Oral Epidemiol 2010;39(3):276–88.
Spiro RH, Huvos AG, Strong EW. Adenocarcinoma of salivary origin. Clinicopathologic study of 204 patients. Am J Surg. 1982;144:423–31.
Sreebny LM. The enigma of dry mouth. Dry mouth: a common worldwide tormentor. In: Sreebny LM, Vissink A, editors. Dry mouth – the malevolent symptom: a clinical guide. Iowa: Wiley-Blackwell; 2010. p. 3–9.
Sreebny LM, Vissink A, editors. Dry mouth – the malevolent symptom: a clinical guide. Iowa: Wiley-Blackwell; 2010.
Stegenga B, Vissink A, de Bont LGM, Spijkervet FKL (Eds). MKA chirurgie. Handboek voor Mondziekten, Kaak‐ en Aangezichtschirurgie. Assen: van Gorcum. Chapter 7: Spijkervet FKL, Vissink A. Afwijkingen van speeksel en speekselklieren; 2013, p 244.
Szanto A, Nagy G, Molnar CS, Griger Z, Tarr T, Zeher M. Description of patients with IgG4-related disease from a Hungarian centre. Scand J Rheumatol. 2014;43:334–7.
Takashima S, Morimoto S, Tomiyama N, Takeuchi N, Ikezoe J, Kozuka T. Sjogren syndrome: comparison of sialography and ultrasonography. J Clin Ultrasound. 1992;20:99–109.
Takada Y, Kawamoto K, Baba S, Takada T, Inoue T, Tomoda K. Sebaceous carcinoma of the parotid gland: a case report. Case Rep Oncol. 2015;8:106–12.
Tarsitano A, Pizzigallo A, Giorgini F, Marchetti C. Giant pleomorphic adenoma of the parotid gland: an unusual case presentation and literature review. Acta Otorhinolaryngol Ital. 2015;35:293–6.
Thompson LD, Bauer JL, Chiosea S, McHugh JB, Seethala RR, Miettinen M, Müller S. Canalicular adenoma: a clinicopathologic and immunohistochemical analysis of 67 cases with a review of the literature. Head Neck Pathol. 2015;9:181–95.
Thompson LD, Wenig BM, Ellis GL. Oncocytomas of the submandibular gland. A series of 22 cases and a review of the literature. Cancer. 1996;78:2281–7.
Tjioe KC, de Lima HG, Thompson LD, Lara VS, Damante JH, de Oliveira-Santos C. Papillary cystadenoma of minor salivary glands: report of 11 cases and review of the english literature. Head Neck Pathol. 2015;9:354–9.
Tribius S, Raguse M, Voigt C, Munscher A, Grobe A, Petersen C, Krull A, Bergelt C, Singer S. Residual deficits in quality of life one year after intensity-modulated radiotherapy for patients with locally advanced head and neck cancer: results of a prospective study. Strahlenther Onkol. 2015;191:501–10.
Trouw LA, Haisma EM, Levarht EW, van der Woude D, Ioan-Facsinay A, Daha MR, Huizinga TW, Toes RE. Anti-cyclic citrullinated peptide antibodies from rheumatoid arthritis patients activate complement via both the classical and alternative pathways. Arthritis Rheum. 2009;60:1923–31.
Tuttolomondo A, Simonetta I, Di R D, Conigliaro R, Corpora F, Vassallo V, Pinto A. A Case report of IgG4-related syndrome and literature review. Curr Pharm Des 2016 [Epub ahead of print].
Ubaidat MA, Robinson RA, Belding PJ, Merryman DJ. Sialadenoma papilliferum of the hard palate: report of 2 cases and immunohistochemical evaluation. Arch Pathol Lab Med. 2001;125:1595–7.
Uemaetomari I, Tabuchi K, Tobita T, Tsuji S, Wada T, Kamma H, Hara A. The importance of postoperative radiotherapy against polymorphous low-grade adenocarcinoma of the parotid gland: case report and review of the literature. Tohoku J Exp Med. 2007;211:297–302.
van de Stadt LA, van der Horst AR, de Koning MH, Bos WH, Wolbink GJ, van de Stadt RJ, Pruijn GJ, Dijkmans BA, van Schaardenburg D, Hamann D. The extent of the anti-citrullinated protein antibody repertoire is associated with arthritis development in patients with seropositive arthralgia. Ann Rheum Dis. 2011;70:128–33.
van den Berg I, Pijpe J, Vissink A. Salivary gland parameters and clinical data related to the underlying disorder in patients with persisting xerostomia. Eur J Oral Sci. 2007;115:97–102.
van Luijk P, Pringle S, Deasy JO, Moiseenko VV, Faber H, Hovan A, Baanstra M, van der Laan HP, Kierkels RG, van der Schaaf A, Witjes MJ, Schippers JM, Brandenburg S, Langendijk JA, Wu J, Coppes RP. Sparing the region of the salivary gland containing stem cells preserves saliva production after radiotherapy for head and neck cancer. Sci Transl Med. 2015;7:305ra147.
van Nimwegen JF, Moerman RV, Sillevis SN, Brouwer E, Bootsma H, Vissink A. Safety of treatments for primary Sjogren's syndrome. Expert Opin Drug Saf. 2016;15:513–24.
Verstappen GM, Kroese FG, Vissink A, Bootsma H. Pharmacotherapy for managing extraglandular symptoms of primary Sjögren's syndrome. Expert Opin Orphan Drugs. 2015;3:125–39.
Villa A, Wolff A, Aframian D, Vissink A, Ekstrom J, Proctor G, McGowan R, Narayana N, Aliko A, Sia YW, Joshi RK, Jensen SB, Kerr AR, Dawes C, Pedersen AM. World workshop on oral medicine VI: a systematic review of medication-induced salivary gland dysfunction: prevalence, diagnosis, and treatment. Clin Oral Investig. 2015;19:1563–80.
Villa A, Wolff A, Narayana N, Dawes C, Aframian DJ, Lynge Pedersen AM, Vissink A, Aliko A, Sia YW, Joshi RK, McGowan R, Jensen SB, Kerr AR, Ekstrom J, Proctor G. World workshop on oral medicine VI: a systematic review of medication-induced salivary gland dysfunction. Oral Dis. 2016;22:365–82.
Vissink A. Other ways to assess salivary gland disease. In: Sreebny LM, Vissink A, editors. Dry mouth – the malevolent symptom: a clinical guide. Iowa: Wiley-Blackwell; 2010. p. 77–88.
Vissink A, Gravenmade EJ, Panders AK, Vermey A, Petersen JK, Visch LL, Schaub RMA. Clinical comparison between commercially available mucin- and CMC-containing saliva substitutes. Int J Oral Surg. 1983;12:232–8.
Vissink A, De Jong HP, Busscher HJ, Arends J, Gravenmade EJ. Wetting properties of human saliva and saliva substitutes. J Dent Res. 1986;65:1121–4.
Vissink A, van Luijk P, Langendijk JA, Coppes RP. Current ideas to reduce or salvage radiation damage to salivary glands. Oral Dis. 2015;21:e1–10.
Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alexander EL, Carsons SE, Daniels TE, Fox PC, Fox RI, Kassan SS, Pillemer SR, Talal N, Weisman MH. Classification criteria for Sjogren's syndrome: a revised version of the European criteria proposed by the American-European consensus group. Ann Rheum Dis. 2002;61:554–8.
Voulgarelis M, Skopouli FN. Clinical, immunologic, and molecular factors predicting lymphoma development in Sjogren's syndrome patients. Clin Rev Allergy Immunol. 2007;32:265–74.
Walls AW, Steele JG. The relationship between oral health and nutrition in older people. Mech Ageing Dev. 2004;125:853–7.
Waldron CA, el-Mofty SK, Gnepp DR. Tumors of the intraoral minor salivary glands: a demographic and histologic study of 426 cases. Oral Surg Oral Med Oral Pathol. 1988;66:323–33.
Wang D, Li Y, He H, Liu L, Wu L, He Z. Intraoral minor salivary gland tumors in a Chinese population: a retrospective study on 737 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:94–100.
Wang XD, Meng LJ, Hou TT, Zheng C, Huang SH. Frequency and distribution pattern of minor salivary gland tumors in a northeastern Chinese population: a retrospective study of 485 patients. J Oral Maxillofac Surg. 2015;73:81–91.
Whitcher JP, Shiboski CH, Shiboski SC, Heidenreich AM, Kitagawa K, Zhang S, Hamann S, Larkin G, McNamara NA, Greenspan JS, Daniels TEA. Simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjogren’s syndrome international registry. Am J Ophthalmol. 2010;149:405–15.
WHO. Classification of Head and Neck Tumours. In: El-Naggar AK, Chan J, Grandis J, Takata T, Slootweg PJ, editors. Lyon: IARC Press; 2017.
Willemze A, Trouw LA, Toes RE, Huizinga TW. The influence of ACPA status and characteristics on the course of RA. Nat Rev Rheumatol. 2012;8:144–52.
Williamson JD, Simmons BH, el-Naggar A, Medeiros LJ. Mucoepidermoid carcinoma involving Warthin tumor. A report of five cases and review of the literature. Am J Clin Pathol. 2000;114:564–70.
Wilson TC, Robinson RA. Basal cell adenocarcinoma and Basal cell adenoma of the salivary glands: a clinicopathological review of seventy tumors with comparison of morphologic features and growth control indices. Head Neck Pathol. 2015;9:205–13.
Wolff A, Joshi RK, Ekstrom J, Aframian D, Pedersen AM, Proctor G, Narayana N, Villa A, Sia YW, Aliko A, McGowan R, Kerr AR, Jensen SB, Vissink A, Dawes CA. Guide to medications inducing salivary gland dysfunction, Xerostomia, and subjective Sialorrhea: a systematic review sponsored by the world workshop on oral medicine VI. Drugs R D. 2017;17:1–28.
Woo SB, Schacterle RS, Komaroff AL, Gallagher GT. Salivary gland changes in chronic fatigue syndrome: a case-controlled preliminary histologic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:82–7.
Yih WY, Kratochvil FJ, Stewart JC. Intraoral minor salivary gland neoplasms: review of 213 cases. J Oral Maxillofac Surg. 2005;63:805–10.
Zare-Mahmoodabadi R, Salehinejad J, Saghafi S, Ghazi N, Mahmoudi P, Harraji A. Sebaceous adenoma of the submandibular gland: a case report. J Oral Sci. 2009;51:641–4.
Zintzaras E, Voulgarelis M, Moutsopoulos HM. The risk of lymphoma development in autoimmune diseases: a meta-analysis. Arch Intern Med. 2005;165:2337–44.
Zlotnik Y, Balash Y, Korczyn AD, Giladi N, Gurevich T. Disorders of the oral cavity in Parkinson's disease and parkinsonian syndromes. Parkinsons Dis. 2015;2015:379482.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this entry

Cite this entry
Jensen, S.B., Vissink, A., Firth, N. (2019). Salivary Gland Disorders and Diseases. In: Farah, C., Balasubramaniam, R., McCullough, M. (eds) Contemporary Oral Medicine. Springer, Cham. https://doi.org/10.1007/978-3-319-72303-7_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-72303-7_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-72301-3
Online ISBN: 978-3-319-72303-7
eBook Packages: MedicineReference Module Medicine