
Abstract
Leprosy is a complex, chronic disease of low infectivity caused by Mycobacterium leprae (M. leprae). The clinical presentation of leprosy is varied and polymorphous; clinical features range from a small single hypopigmented or erythematous skin patch to diffuse infiltration of skin involvement of the peripheral nerve trunk and other organs like the eyes, spleen, liver, testis, bones, and joints. The disease course in leprosy is interspersed with lepra reactions, which are hypersensitivity reactions and are the main cause of morbidity in leprosy. Leprosy is also considered one of the leading causes of infectious peripheral neuropathy. It is associated with both sensory and motor impairment leading to deformities and disabilities, often causing significant social stigma.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Leprosy is a complex, chronic disease of low infectivity caused by Mycobacterium leprae (M. leprae). The clinical presentation of leprosy is varied and polymorphous; clinical features range from a small single hypopigmented or erythematous skin patch to diffuse infiltration of skin involvement of the peripheral nerve trunk and other organs like the eyes, spleen, liver, testis, bones, and joints. The disease course in leprosy is interspersed with lepra reactions, which are hypersensitivity reactions and are the main cause of morbidity in leprosy. Leprosy is also considered one of the leading causes of infectious peripheral neuropathy. It is associated with both sensory and motor impairment leading to deformities and disabilities, often causing significant social stigma.
Leprosy has been known to man since time immemorial. DNA taken from the shrouded remains of a man from the Old City of Jerusalem shows him to be the earliest human proven to have suffered from leprosy. The remains were dated by radiocarbon methods to 1–50 AD. The origin of leprosy has always been a matter of uncertainty, and an Indian or African origin for the disease has often been assumed based on historical sources that support an initial spread of the disease from Asia to Europe. Dr. Robbins and colleagues reported a case of leprosy in a skeleton showing changes associated with leprosy buried around 2000 BC in Rajasthan, India, at the site of Balathal [1].
Leprosy was considered incurable, and this was one of the other causes of stigma associated with the disease. The discovery of dapsone in 1940 and then the introduction of multidrug therapy in 1984 were responsible for reducing the case burden of leprosy. Early detection and initiating prompt treatment with multidrug therapy (MDT) remains the key strategy to reduce global burden of leprosy and to prevent associated disabilities and deformities.
Leprosy is one of the least infectious diseases because majority of the population have natural immunity against it. The only natural reservoir of M. leprae is man, and the most important source of infection is an untreated case of multibacillary leprosy, although all untreated cases should be considered as potential sources of infection. Leprosy is also found in animals like wild armadillos, chimpanzees, sooty mangabey monkeys, and cynomolgus macaque. Leprosy is considered a zoonosis in the southern United States, and epidemiological studies from the United States and Brazil have implicated contact with armadillos as a risk factor for leprosy infection [2, 3].
2 Epidemiology
Leprosy is no longer an ancestral plague that it has been, and globally leprosy has been almost eliminated or it is no longer a public health problem as the number of registered cases has decreased from 5.4 million in the year 1985 to 171,948 in 2016, and the prevalence rate per 10,000 fell from 21.1 to 0.23 over the last three decades [4] (Table 1).
As per “Global leprosy update, 2015: time for action, accountability and inclusion,” published by WHO in September 2017, the leprosy statistics revealed the following [4]:
-
214,783 newly diagnosed patients were reported in 2016 (detection rate of 2.9 per 100,000 population).
-
94–96% of leprosy patients reported in 2016 were from 22 countries; India reported 135,485 new cases, accounting for 63% of the global new leprosy cases; Brazil reported 25,218 new cases, representing 13% of the global new cases; and Indonesia reported 16,826 new cases, 8% of the global case load.
-
39.2% of patients were females and 8.5% of patients were children.
-
59.18% of patients reported were of multibacillary (MB) type.
-
3039 cases of relapse were reported from 46 countries.
-
With 12,437 new G2D cases, the proportion of new G2D cases was 12% lower than 2015, and it corresponds to a detection rate of 1.7 per million population.
The global burden of leprosy necessitated a massive and combined effort of various organizations like the World Health Organization (WHO), various NGOs, governmental bodies, and healthcare professionals to tackle it together. Multidrug therapy (MDT), first conceived in 1982, has been the main weapon against leprosy. However, as seen in the past few years, new cases continue to occur in most endemic countries, and high-burden pockets exist against a low-burden background.
The WHO launched Global Leprosy Strategy 2016–2020 with the following aims [5]:
-
Zero grade 2 disability (G2D) among pediatric leprosy patients
-
Reduction of new leprosy cases with G2D to less than one case per million population
-
Zero countries with legislation allowing discrimination on basis of leprosy
Leprosy continues to be an important infectious disease as is evident by (a) a relatively stable new case detection over the last decade, (b) a growing number of treated leprosy patients with recurrent reactions, and (c) a long-term neurologic dysfunction and disability as a result of irreversible peripheral nerve injury. We may have eliminated leprosy as a public health problem at a global level, but there are some issues that remain unanswered, and if we don’t find a solution or answer to these, we may be faced with the problem of leprosy resurgence. The challenges or unsolved issues are lack of clarity about (a) the precise mode and route of transmission; (b) environmental, socioeconomic, and behavioral factors that promote its transmission; and (c) strategies for early diagnosis and prevention of neurologic impairment to reduce the disability burden among newly identified cases and among treated cases who continue to endure long-term disability [6].
3 Situation of Leprosy in India [7, 8]
-
A total of 135,485 new cases were detected during the year 2016–2017, which gives an annual new case detection rate (ANCDR) of 10.2 per 100,000 population, as against 127,326 cases in 2015–2016. This showed increased in ANCDR in 2016–2017 (Table 2).
-
A total of 88,166 cases were on record as of 1 April 2017, giving a prevalence rate (PR) of 0.66 per 10,000 population, as against 86,147 cases in 1 April 2016. This showed increase in PR in 2016–2017. This increase is due to active case finding under Leprosy Case Detection Campaigns (LCDC) organized all over the country.
-
Among new leprosy cases detected, the proportion was as follows: MB (49.57%), female (39.17%), child (8.65%), grade 2 deformity (3.87%).
-
A total of 5245 cases with grade 2 disability were detected among the new leprosy cases during 2016–2017, indicating the grade 2 disability rate of 3.87 per million.
-
A total of 11,792 child cases were recorded, indicating a child case rate of 0.86/100,000 population. This was less than the figure of 2015–2016.
4 Targets Under Program Implementation Plan (PIP) of NLEP to Be Achieved by 2016–2017 [8]
The 12th Five Year Plan for National Leprosy Eradication Programme (NLEP) for the period 2012–2013 to 2016–2017 was approved by the Government of India.
The objectives under PIP or 12th Plan were:
-
(a)
Elimination of leprosy, i.e., prevalence of less than 1 case per 10,000 population in all districts of the country
-
(b)
Strengthening of Disability Prevention and Medical Rehabilitation of persons affected by leprosy
-
(c)
Reduction in the level of stigma associated with leprosy
To achieve the objectives of the plan, the main strategies to be followed include:
-
Integrated leprosy services through general healthcare system
-
Early detection and complete treatment of new leprosy cases
-
Carrying out of household contact survey for early detection of cases
-
Involvement of Accredited Social Health Activist (ASHA) in the detection and completion of treatment of leprosy cases on time
-
Strengthening of Disability Prevention and Medical Rehabilitation (DPMR) services and Information, Education and Communication (IEC) activities in the community to improve self-reporting to Primary Health Centre (PHC) and reduction of stigma
-
Intensive monitoring and supervision at block Primary Health Centre/Community Health Centre
The targets under PIP include decrease prevalence rate < 1/10,000 in 100% of districts, new ANCDR of less than 10 per 100,000 population in 100% districts, and decrease of grade 2 disability rate by 35%. The targets are summarized in Table 3.
5 Etiology
M. leprae is a non-motile, non-spore-forming, acid-fast, gram-positive, microaerophilic obligate intracellular bacillus that shows tropism for cells of the reticuloendothelial system and peripheral nervous system (notably Schwann cells). It is a slow-growing bacillus and takes 12–14 days to divide into two. It is present in large numbers in lesions of lepromatous leprosy, often grouped together and arranged like bundles of cigars. Under the electron microscope, the bacillus appears to be polymorphous with the commonest form being a slightly curved filament 0.3–1 μm in width and 1–8 μm in length. Studies in animal models indicate that M. leprae grows best at 27 °C to 30 °C, correlating with its predilection to affect cooler areas of the body (the skin, nerve segments close to the skin, and the mucous membranes of the upper respiratory tract) [10, 11].
The inability of M. leprae to grow and survive at elevated temperatures is probably due to its inability to mount a protective heat stress response. M. leprae grows extensively in the nine-banded armadillo (Dasypus novemcinctus), which has a core body temperature of 34 °C [12].
The genome of M. leprae has been fully sequenced, and it was observed that M. leprae has less than half of the functional genes of M. tuberculosis. It contains an extraordinary number of pseudogenes, and genes for key enzymes of many essential metabolic pathways are missing [13, 14]. The M. leprae genome is highly conserved, but, using a combination of single-nucleotide polymorphisms and variable number tandem repeats, the major strain types can be reasonably discriminated [15].
6 M. lepromatosis
Han and Quintanilla reported this organism which is very similar to M. leprae but with some distinct differences in the DNA sequence for 16S RNA [16]. A total of 64 cases of leprosy caused singly by M. lepromatosis have been reported so far from Mexico or in patients of Mexican origin. Cases reported from other parts of the world are five cases from Singaporean Chinese, one case of a native Canadian, and two cases in native Costa Ricans. There are reports of coinfection with M. leprae and M. lepromatosis in patients from Mexico. Initially the bacterium was isolated form cases of diffuse lepromatous leprosy or Lucio leprosy, and subsequent reports show a more variable clinical presentation similar to M. leprae [16]. Limited data is available regarding M. lepromatosis; it has not yet been cultured, and its ability to infect nerves and other basic aspects of its biology is still unknown. Limited clinical experience with this isolate indicates that it presents with the same clinical features, responds well to same anti-mycobacterial drugs, and has same prognosis as M. leprae infection [17,18,19]. The identification of M. lepromatosis may be of epidemiological importance in the current scenario.
7 Pathogenesis of Leprosy
The clinical manifestations of leprosy are related to M. leprae survival and depend upon the interplay of innate and acquired immune responses involving interactions of the bacterial proteins with immune components of the host. These interactions may either prevent the invasion and infection or promote their growth and development of pathology. The immune system has evolved primarily to combat infection, but in leprosy, the immune response is responsible for the broad clinical spectrum of the disease and, similar to an autoimmune disease, seems to trigger further complications such as nerve damage [20].
8 Genetic Determinants of Host Response
Even after sustained exposure to M. leprae, only a subset of individuals develop clinical leprosy as majority of the population is immune to leprosy. Based on early studies on familial aggregation of leprosy cases to the most recent genome-wide association studies on leprosy-associated genetic polymorphisms, there is a strong evidence that human genetic factors influence the acquisition of leprosy and its further clinical course [21]. The polarization concept in leprosy has been studied by both DNA-independent analyses (familial correlations, twin and segregation studies) and DNA-based analyses (linkage and association studies). The first genome-wide linkage study of leprosy was performed in India in 2001. The sample included 224 families comprising 245 sibling pairs affected by leprosy [22]. A significant linkage hit (p < 2 × 10−5) for leprosy was observed with genetic markers located on chromosomal region 10p13. However, the study population had 98% PB cases; hence, it was not possible to decide whether the mapped locus influenced leprosy per se or was specific for the PB form. Overall, the results of the linkage studies in Indian and Vietnamese leprosy patients suggest that the 10p13 and 20p12 regions are differentially implicated according to the subtype considered [23, 24].
The various genes and genetic polymorphisms that have been studied for association with leprosy subtypes are (Box 1):
Box 1. Genetic Polymorphisms Associated with Leprosy [21]
Validated studies from different parts of the world | Genes that have been studied once from a particular region |
|---|---|
Toll-like receptor 2 (TLR2) from Ethiopia and Malawi | IFN-γ and HLA-G in Brazil |
TNF-α gene from India and Thailand | TLR4 and leukotriene A4 hydrolase (LTA4H) in Ethiopia |
Mannose-binding lectin 2 (MBL2) in Brazil and Nepal | Vitamin D receptor (VDR), killer cell immunoglobulin-like receptor, two Ig domains and short cytoplasmic tail 3 (KIR2DS3), heat shock protein 1A (HSPA1A), and IL-23R from India |
Mannose receptor C type 1 (MRC1) from Brazil and Vietnam | |
Interleukin-10 (IL-10) from Brazil | |
MHC class I chain-related gene A (MICA) from China and Brazil |
9 Transmission
The skin and the nasal mucosa are the major exit routes of M. leprae from the human body. Lepromatous cases harbor large numbers of organisms deep in the dermis, and sometimes they may also be found in the stratum corneum. These organisms from the superficial keratin layer could exit through the skin by exfoliation. However, transmission through this route has still not been definitely proven [25].
The main portal of entry of M. leprae is through the nasal mucosa. Whether this exposure results in infection or not depends largely on genetic susceptibility, immunological response of the individual, and the bacillary load. Hematological dissemination of the bacilli is considered to be the route of spread and widespread clinical pattern of the disease. A successful immune response or innate immunity aborts the further invasion, and M. leprae is eliminated in majority of the individuals. However, in a minority, M. leprae evades immunological defenses and continues to multiply in macrophages and the Schwann cells surrounding peripheral nerves and subsequently in the skin and other tissues. Studies of household contacts who do not manifest leprosy have detected disseminated subclinical autonomic neuropathy in them, as evident by abnormal vasomotor reflexes—that might be like the Ghon’s focus in the lung seen after exposure to Mycobacterium tuberculosis [26].
Environmental factors such as soil and water exposure, insect vectors, and the free-living amoebae (e.g., Acanthamoeba spp.) may also play an important role in the transmission of leprosy [6, 27, 28]. These environmental factors may also participate in the environmental viability of leprosy in some biotopes [27]. However some of the experts believe that most of these reports are on PCR-based studies, and although leprosy bacilli may remain viable in certain cell-free environments for a variable period, it does not mean that they remain infectious or they can replicate; moreover, with an abbreviated genome, it is most unlikely that M. leprae can replicate in any extracellular environment [29].
Zoonotic transmission of leprosy from natural infection of armadillos in the Southeast United States has been confirmed as responsible for the majority of autochthonous (indigenous or not from other regions/migrants) transmission in this area. It is likely that animals like armadillos may also play an important role in the transmission of leprosy in some areas of Latin America such as in Colombia, Venezuela, Mexico, and Brazil. Understanding how environmental factors influence host-pathogen interactions in complex natural systems, where multiple feedbacks between biotic and abiotic factors take place, is especially important in the context of environmentally persistent pathogens such as M. leprae [6, 30, 31].
10 Immunopathogenesis
In leprosy the clinical phenotype that the patient develops depends on the immunological response of the host. When M. leprae is first encountered, the monocytes may phagocytose all bacilli; however, in tuberculoid leprosy, the organisms may be totally destroyed, while in lepromatous leprosy, microvacuolated monocytes (phagocytes) with bacillary debris and live bacilli may persist [20, 32]. Although the precise mechanisms are unclear, the level of cell-mediated immunity or Th1 vs Th2 response to infection with M. leprae in the host determines the progression of disease toward tuberculoid or the lepromatous spectrum. Toll-like receptors on innate immune cells may recognize mycobacterial lipoproteins, generating cytokines that mediate specific responses in a Th1 or Th2 direction. A robust CMI or Th1 response either aborts the infection in the initial stages or contains it as is seen in the tuberculoid leprosy. Nonresponsiveness toward M. leprae seems to correlate with a Th2 cytokine profile and development of lepromatous leprosy [25]. In addition to Th1 and Th2, the concept of T cell plasticity is also seen, and various subsets like Th17, Th22, and T-Reg cells have also been described in the pathogenesis of leprosy, and sometimes the distribution of these subsets depends on the level of antigenic stimulation or infection [32].
11 Pathogenesis of Nerve Involvement in Leprosy
All patients with leprosy have some degree of nerve involvement. Perineural inflammation is the histopathologic hallmark of leprosy, and this localization may reflect a vascular route of entry of M. leprae into nerves. Axonal atrophy may occur early in this process; ultimately, affected nerves undergo segmental demyelination [33]. The invasion of Schwann cells by M. leprae is the first step in the induction of nerve damage. The neurotropism of M. leprae is due to its affinity for the G-domain of laminin-alpha 2, an extracellular matrix protein that is present in the basal lamina of Schwann cells. M. leprae/laminin-alpha 2 complexes bind to alpha/beta dystroglycan complexes expressed on the Schwann cell surface. The bacterial components involved in the interaction are ML-LBP21, PDIM, and PGL-1. Recent in vitro work has suggested that early M. leprae-induced nerve damage is mediated via ErbB2 receptor tyrosine kinase signaling, which results in early nerve demyelination [25]. Another in vitro study suggested that early molecular pathways of nerve damage originate from M. leprae-induced excessive Schwann cell survival, which triggers glial cell proliferation and the inflammatory response [25, 33, 34]. Nerve damage may also be mediated by inflammatory and immune-mediated processes, as well as due to edema and mechanical processes.
Nerve damage due to leprosy can be divided into two phases:
-
1.
Initial phase: This phase is common to both tuberculoid and lepromatous ends. The hallmark of this phase is the absence of inflammatory cells. It is due to early biochemical changes in the axonal compartment and axonal atrophy and occurs before structural changes in myelinated fibers; these changes are seen more in small, poorly myelinated or unmyelinated nerve fibers [33].
-
2.
Later phase: It is characterized by the presence of inflammatory response which ranges from well-organized granulomatous response in tuberculoid disease that aggressively affects the nerve to a disorderly chronic inflammation in lepromatous patients which eventually destroys the nerve and the surrounding tissue.
12 Stages of Nerve Involvement [25]
Five stages of nerve involvement can be recognized, the first two being identifiable only by histological scrutiny while the later three are clinical:
-
1.
Stage of parasitization: M. leprae found within nerves.
-
2.
Stage of tissue response: inflammatory response to the presence of bacilli.
-
3.
Stage of clinical infection: nerve thickening with no apparent nerve function impairment.
-
4.
Stage of nerve damage: apparent nerve function impairment. This stage is reversible.
-
5.
Stage of nerve destruction: nerve fibers are totally destroyed and collagenized.
13 Risk Factors for Leprosy
Poor socioeconomic status and unhygienic living conditions like contaminated water, inadequate housing, malnutrition, and diseases compromising the immune function are usually the risk factors for leprosy. HIV infection has not been reported to increase the susceptibility to leprosy, although initiation of antiretroviral therapy can either activate subclinical leprosy or exacerbate pre-existing lesions due to immune reconstitution inflammatory syndrome [25].
Results of various studies suggest that susceptibility to leprosy is multigenic, with a high degree of heterogeneity among different populations studied. HLA-DR2 and the Taq1 polymorphism of the vitamin D receptor gene, alleles in the PARK2 and PACRG, and NOD2 have been found to be associated with susceptibility to infection with M. leprae [35, 36].
14 Incubation Period of Leprosy
Leprosy has a relatively long incubation period with the average incubation period varying between 3 and 10 years. However it is difficult to measure the accurate period because of the paucity of adequate immunological tools and slow onset of disease [25].
15 Clinical Features of Leprosy
Leprosy patients have skin lesions varying from ill- to well-defined macules, patches, nodules, and plaques to diffuse involvement which is often difficult to distinguish from the normal skin. However, in most leprosy cases, the lesions are in the form of a hypoesthetic, hypopigmented, or erythematous patches, but papular, annular, nodular, and plaque types of lesions occur in variable numbers and are distributed on various parts of the body. Most of these lesions have diminished or absent sensations, impairment of sweating, and reduced hair density.
Leprosy is diagnosed when at least one of the cardinal signs is manifested [37]:
-
A definite loss of sensation in a pale (hypopigmented) or reddish skin patch
-
A thickened or enlarged peripheral nerve, with loss of sensation and/or weakness of the muscle supplied by that nerve
-
The presence of acid-fast bacilli in a slit skin smear [37]
16 Classification of Leprosy
The classification of a disease is used to identify and understand the different aspects of disease presentation and linking them to the underlying immunopathogenesis which is helpful for the treatment decisions, prognosis, and research. Classification of leprosy allows the risk of complications to be predicted; for example, leprosy patients with borderline leprosy are at a much higher risk of developing reactions than patients with tuberculoid disease. The first system for classification of leprosy was proposed at an international meeting in Manila in 1931. This was followed by systems proposed in Cairo in 1938, Rio de Janeiro in 1946, Havana in 1948, and Madrid in 1953, followed by an Indian classification in 1955 [38] (Box 2). The initial classifications were predominantly based on clinical features with some support from histological and lepromin testing. They classified leprosy into tuberculoid and lepromatous poles and borderline, dimorphous, or intermediate categories.
Box 2. The Indian Classification System
-
1.
Tuberculoid (T)
-
2.
Lepromatous (L)
-
3.
Maculoanesthetic (MA)
-
4.
Polyneuritic (P)
-
5.
Borderline (B)
-
6.
Indeterminate (I)
Ridley-Jopling classification is the most widely used classification system in leprosy. They classified leprosy into five types: lepromatous leprosy (LL), borderline lepromatous leprosy (BL), borderline leprosy (BB), borderline tuberculoid leprosy (BT), tuberculoid leprosy (TT), and indeterminate. This classification of leprosy is recognized to be an expression of the patient’s resistance to infection or the immunity and the spectrum ranges from a form with a robust immune response and very few organisms (tuberculoid or paucibacillary) to a form with a weaker immune response and a higher burden of organisms (lepromatous or multibacillary). The classification is based on the cutaneous, neurologic, and biopsy findings, all of which correlate with immunological capability of the individual. The categories also correlate with the number of acid-fast bacilli present in the dermis [39, 40].
-
1.
Tuberculoid form (TT): Characterized by a single lesion (maximum up to three lesions). The lesions are usually large in size, well-defined, and in the form of erythematous plaques with raised clear-cut edges (Fig. 1). The surface of lesion(s) looks dry, scaly, and turgid. Sensations as well as hair are usually absent on the lesion. Lepromin test is strongly positive (++++). On histopathological examination, large epithelioid cells are found to be arranged in compact granulomas along neurovascular bundles, with dense peripheral lymphocytic infiltrate. Langhans giant cells are usually absent. Dermal nerves may be obliterated and destroyed by dense lymphocyte cuffs. Acid-fast bacilli are rarely found even in nerves. The granuloma usually reaches and may even erode the epidermis [41].
-
2.
Borderline tuberculoid (BT): The lesions are few (maximum of ten). The lesions are well defined and variable in size. Many lesions may slope outward or fade into surrounding skin. Few satellite lesions may sometimes be seen (Fig. 2). The surface of lesions is dry, scaly, and infiltrated. Sensations and hair over the lesion are usually absent, just like in TT. AFBs when seen are scanty. Lepromin reactivity is positive (++ or +). Histology shows Langhans giant cells, which are variable in number and not large in size. Granulomas along the superficial vascular plexus are frequent, but they do not infiltrate up into the epidermis (grenz zone). Nerve invasion and obliteration are typical. BI ranges from 0 to 2+.
-
3.
Borderline borderline (BB): Several lesions (10–30) may have an inverted saucer appearance, where the outer margin is sloping and the inner margin is punched out (Fig. 3). They may be dull or shiny. Sensations and hair over the lesions are moderately diminished. Lepromin test is negative or weakly positive (+ or −). Histology shows a grenz zone; macrophages are activated into epithelioid cells, but there are only few distinct granulomas. Lymphocytes are scanty. There are no giant cells. BI ranges from 3 to 4+.
-
4.
Borderline lepromatous (BL): The lesions are numerous and tend to be symmetrical. Size may vary from small to large (Fig. 4). Most lesions are ill-defined, although few may show a better defined edge. The surface of lesions is shiny and sensations and hair are only mildly affected. Numerous AFBs are found in the lesion and lepromin test is negative. Histopathology shows a grenz zone and prominent lymphocytic infiltrate, with activation of macrophages to form poorly to moderately defined granulomas. There is perineural fibroblast proliferation, forming an “onion peel” in cross section. Foamy cells are present but not prominent, and BI ranges from 4 to 5+.
-
5.
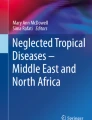
Lepromatous leprosy (LL): The lesions are innumerable and skin may even be diffusely infiltrated (Fig. 5a). The lesions are ill-defined, small, shiny plaques that are distributed symmetrically. In the early stage of the disease, sensations are not affected and overlying hairs are normally present. AFBs are plentiful, some forming “globi.” Lepromin test is negative. Histopathological examination shows extensive cellular infiltrate separated from the flattened epidermis by a narrow grenz zone, causing destruction of the cutaneous appendages and may extend even into the subcutaneous fat. Macrophages have abundant eosinophilic cytoplasm and contain a mixed population of solid and fragmented bacilli. Foamy cells, granulomas, and globi are seen (Fig. 5b).
-
6.
Polar and subpolar forms: LL may be polar LL (LLp) or subpolar LL (LLs). LLp is immunologically stable and starts and stays as lepromatous throughout. LLs is unstable, and it evolves from downgrading of the borderline group and may have some lesions of borderline leprosy as evidence of having downgraded. Similarly, TT may also be polar TT (TTp) or subpolar TT (TTs). TTp originates as tuberculoid and hardly ever downgrades, while TTs is the unstable form, usually downgrades to borderline leprosy, and may rarely upgrade from borderline spectrum [41].

Well defined erythematous plaque of tuberculoid leprosy (TT)

Erythematous plaque with pseudopodia and few satellite lesions in borderline tuberculoid (BT) leprosy

Inverted saucer appearance of lesions in mid borderline (BB) leprosy

Multiple hypopigmented plaques in borderline lepromatous (BL) leprosy

(a) Diffuse infiltration with papules and nodules in lepromatous leprosy (LL). (b) Fite-Faraco Stain: numerous foamy macrophages and lymphocytes, containing many acid fast bacilli
17 Other Forms of Leprosy
-
1.
Indeterminate: Characterized by ill-defined hypopigmented scaly macules or patches (Fig. 6). The lesions are few in number, and slight impairment of sensation may be present. There is mild lymphocytic and macrophage accumulation around neurovascular bundles, sweat glands, and erector pili muscle. Diagnosis should only be made on finding one or more acid-fast bacilli at the sites of predilection: in the nerve, in the erector pili muscle, just under the epidermis, or in a macrophage around a vessel [41].
-
2.
Lucio Leprosy: Lucio leprosy (lepra bonita), first described by Lucio and Alvarado in 1852, is characterized by a diffuse shiny infiltration of all body skin with widespread sensory loss. As the disease progresses, the eyelids become thickened, giving the patients a sleepy and sad appearance. Madarosis is often the first sign. Patients may complain of numbness of the hands and feet, nasal congestion and epistaxis, hoarseness of the voice, and edema of the feet. Bacteriological smears are highly positive (BI 6+) and lepromin reaction is negative. Lucio leprosy is considered to be the most anergic of all the immunological spectrum of leprosy [41]. Endothelial cell injury appears to be the main event in the pathogenesis of diffuse leprosy of Lucio and Latapí. Once M. leprae has entered the endothelial cell, the microorganism damages the blood vessels, leading to the specific changes seen in this variety of lepromatous leprosy [42].
-
3.
Histoid Leprosy: Histoid leprosy is a special manifestation of lepromatous leprosy and was first described by Wade in 1963 [43]. It is characterized by papules and sharply demarcated, firm nodules. Histoid leprosy has been generally reported to manifest in patients after long-term dapsone monotherapy and irregular or inadequate therapy. However, there are also reports of disease developing as relapse after successful treatment or even appearing de novo without a prior history of any antileprosy treatment. Clinically the histoid lesions appear as smooth, shiny, hemispherical, dome-shaped, nontender soft to firm nodules which may be superficial, subcutaneous, or deep dermal nodules and plaques or pads appearing on otherwise normal-looking skin (Fig. 7). The lesions are usually located on the face, back, buttocks, and extremities and over bony prominences, especially around the elbows and knees. On histological examination, spindle-shaped cells containing M. leprae are found. Bacteriological smears are highly positive (BI 6+) and the lepromin reaction is negative [44].
-
4.
Pure Neuritic Leprosy: There is thickening of the peripheral nerve trunk with sensory loss in the area of its distribution, with or without associated motor paralysis, primarily in the absence of any skin patch regardless of clinical evidence of reaction involving the nerve. It accounts for around 4–6% of leprosy cases in the Indian subcontinent. Commonly affected nerves are ulnar, median, radial, lateral popliteal, posterior tibial, sural, facial, and sometimes trigeminal. Mononeuritis or mononeuritis multiplex is the most common presentation [45].
Slit skin smear or a skin biopsy usually does not reveal changes of leprosy. Nerve conduction studies, FNAC, nerve biopsy, PCR, etc. may be used for diagnosis. All other causes of peripheral neuropathy should be excluded, and the clinician should have a high index of suspicion [46].

Ill defined hypopigmented patch of indeterminate leprosy

Papules and sharply demarcated firm nodules on apparently normal appearing skin in histoid leprosy
WHO Classification
The World Health Organization (WHO) classification system was designed for use in situations in which there is little or no clinical expertise or laboratory support; it is based upon the number of skin lesions present [47]:
-
Paucibacillary (PB) leprosy is defined as five or fewer skin lesions without detectable bacilli on skin smears.
-
Multibacillary (MB) leprosy is defined as six or more lesions and may be skin smear positive. Counting skin lesions alone may lead to misclassification of many patients with PB leprosy rather than MB leprosy, leading to undertreatment in some cases [37].
18 Neuropathy in Leprosy
Classical Leprosy Neuropathy
This involves nerves of the extremities (both upper and lower), which may present as:
-
1.
Thickening of nerve trunks
-
2.
Mononeuritis
-
3.
Mononeuritis multiplex
-
4.
Polyneuropathy with a “glove and stocking”-type distribution
-
5.
Cranial neuropathies
-
6.
Peripheral autonomic dysfunctions (anhidrotic dry skin, compromised sudomotor and vasomotor responses, and trophic ulcers) [47]
Acute Neuritis
This is one of the most common and dramatic presentations in leprosy and generally occurs during the leprosy reactions. It often starts with spontaneous nerve pain, paresthesias, and nerve tenderness. These symptoms are followed by nerve function impairment with objective sensory-motor loss. Recognition of the symptoms at onset is crucial, as initiation of steroids reduces long-term damage [26].
Silent Neuropathy
The patient has only neurological deficit which is mostly progressive in the absence of nerve pain and tenderness with no evidence of reaction. The lack of spontaneous subjective nerve impairment makes this condition detectable only when specifically assessed with standardized monofilament testing for sensory impairment and voluntary muscle strength for motor impairment [48].
Subclinical Neuropathy
Subclinical neuropathy appears to be more prevalent in leprosy than was previously believed [47]. Testing using monofilaments and other sensitive methods has demonstrated that functional nerve impairment occurs earlier in the course of lepromatous disease than in tuberculoid disease, even though patients with tuberculoid disease may be aware of numbness or weakness earlier in the course of their illness than patients with lepromatous disease [49]. In a prospective study of early neuropathy diagnosis in leprosy, sensory nerve conduction and warmth perception were the most frequently and earliest affected tests; in a large proportion of patients, these became abnormal ≥3 months or more before other abnormalities were identified using monofilaments [50].
Chronic Neuropathic Pain
It is diagnosed when the patient presents with pain and new nerve function impairment in the absence of leprosy reaction after completion of MDT. The pain is described as continuous burning type with glove and stocking distribution. It can also manifest as paresthesias, dysesthesias, hyperesthesia, and allodynia along the nerve and in its area of distribution. Different pathophysiological mechanisms possibly leading to leprosy-related neuropathic pain are small fiber neuropathy and persistent intraneural inflammation due to residual bacterial antigens or persisters in the Schwann cells. We should rule out pain due to extraneural pathology such as osteitis, periosteitis, and osteomyelitis in all these cases. Management is difficult and tricyclic antidepressants, anticonvulsants, and opioids have been tried [51].
Childhood Leprosy
Childhood leprosy is a significant indicator of control programs in the society as the detection of new cases in children under 15 years of age reveals an active circulation of bacilli, continued transmission, and lack of disease control by the health system. According to the NLEP report of 2017, children constituted 8.65% of the newly detected leprosy cases in India [7]. Among patients under 15 years of age, the most affected age group is children between 10 and 14 years of age, although there are case reports of patients younger than 1 year as well. Household contacts are the primary source of infection. Various studies have reported rates varying from 8.7% to 38.8% [52, 53]. Paucibacillary forms of the disease are more common, especially borderline tuberculoid leprosy, with a single lesion in exposed areas of the body representing the main clinical manifestation. Lepra reactions are rare, although some authors have reported high frequencies of type 1 lepra reaction. Peripheral nerve involvement has been described at very high rates in some studies, which increases the chance of deformities, a serious problem, especially if one considers the age of these patients. High disability rates have been reported in studies from India ranging from 0.5% to 24%, which could be due to delay in diagnosis or detection of leprosy in these cases. If we have to bring this figure to zero by 2020, then we will have to initiate the school health surveys and household contact surveys again [54].
Physical Examination
The diagnosis of leprosy should be considered in patients with skin lesions and/or enlarged nerve(s) accompanied by sensory loss or motor weakness. Leprosy should be suspected in the setting of the following symptoms:
-
Hypopigmented or reddish patch(es) on the skin
-
Diminished sensation or loss of sensation within skin patch(es)
-
Paresthesias (tingling or numbness in the hands or feet)
-
Painless wounds or burns on the hands or feet
-
Lumps or swelling on the earlobes or face
-
Tender, enlarged peripheral nerves [55]
Late findings include weakness of the hands with claw fingers, foot drop, facial paralysis or lagophthalmos, lack of eyebrows and eyelashes, collapsed nose, or perforated nasal septum. Clinical findings correlate with the extent of nerve involvement, classification of disease, and presence of the immunologic complications known as reactions.
The examination should include evaluation of skin lesions and palpation of peripheral nerves for enlargement and/or tenderness, including the ulnar nerve at the elbow, median and superficial radial cutaneous nerve at the wrist, great auricular nerve in the neck, and common peroneal nerve at the popliteal fossa (Fig. 8). A sensory examination of skin lesions, distal extremities, and motor evaluation should also be performed. Eyes should be examined by simple inspection of the conjunctiva and cornea, as well as assessment of corneal sensation.

The peripheral nerves that should be examined in a case of leprosy
Ocular involvement is also commonly seen in leprosy and is estimated to be present in about 70–75% of all cases of leprosy. About 10–50% of leprosy patients suffer from severe ocular symptoms (potential sight-threatening complications/involvement), and blindness occurs in about 5% of patients [56]. Complications like lagophthalmos, corneal hypoanesthesia, neurotrophic or infectious keratitis, iridocyclitis, and cataract formation are considered potentially sight-threatening complications and should be managed urgently. Completion of multidrug treatment does not guarantee the prevention from ocular complications which may continue to occur years after completion of MDT [57].
Rheumatologic Manifestations of Leprosy
Musculoskeletal involvement is the third most common manifestation in leprosy following the cutaneous and neural manifestations but is less frequently reported.
Different patterns of musculoskeletal presentation can occur in leprosy patients. Joint involvement can be monoarticular, oligoarticular, or polyarticular. It can present as acute symmetrical polyarthritis or chronic symmetrical polyarthritis mimicking rheumatoid arthritis. Enthesitis and tenosynovitis are also common presentations in leprosy.
Chauhan et al. classified the arthritis in leprosy into the following groups: (1) Charcot arthropathy secondary to peripheral sensory neuropathy, (2) swollen hands and feet syndrome, (3) acute polyarthritis of lepra reaction, and (4) chronic arthritis from direct infiltration of the synovium by lepra bacilli [58, 59]. Hence it is important to include leprosy in the list of possible differential diagnosis of arthritis, mainly in those countries where leprosy is prevalent or those patients who have traveled from endemic areas.
Differential Diagnosis
The clinical presentation of leprosy is highly variable and it can mimic a variety of other dermatological and neurological disorders.
Dermatological Disorders [60]
Macular hypopigmented lesions | Annular lesions | Infiltrated plaques |
|---|---|---|
Vitiligo, pityriasis versicolor, nevus anemicus, nevus depigmentosus, and pityriasis alba | Granuloma annulare, tinea corporis, lichen planus, syphilis, and granuloma multiforme | Lupus vulgaris, sarcoidosis, discoid lupus erythematosus, cutaneous leishmaniasis |
Neurological Disorders
Neurological disorders that need to be differentiated from leprosy include hereditary neuropathy, mono- or polyneuritis, nutritional and alcoholic neuropathy, lead poisoning, nerve damage after trauma, entrapment neuropathy, poliomyelitis, syringomyelia, Guillain-Barré syndrome, and neurogenic muscular atrophy [61]. Leprosy has to be differentiated from other causes presenting as thickened peripheral nerves (Box 3). Because leprosy does not affect the central nervous system, the presence of signs such as loss of tendon reflexes, pathological reflexes, and nystagmus will exclude leprosy. Hence a detailed neurological examination is mandatory when the diagnosis of leprosy is in doubt.
Box 3. Differential diagnosis of enlarged peripheral nerves
-
1.
Hereditary motor and sensory neuropathy
-
2.
Neurofibromatosis
-
3.
Refsum’s disease
-
4.
Perineuroma/localized hypertrophic neuropathy
-
5.
Nerve tumors
-
6.
Amyloidosis
19 Laboratory Diagnosis
Although leprosy is considered a clinical diagnosis, laboratory diagnostic tests such as slit skin smear (SSS) and histopathology of involved tissues provide the necessary information to make the diagnosis in almost all cases. Serology, polymerase chain reaction, and bacteriologic, histopathologic, and immunologic studies provide evidence to support the clinical diagnosis and are more important for research.
19.1 Slit Skin Smear (SSS)
Slit skin smear examination is helpful in classification and management of disease, as well as in following up of patients for response to treatment and detecting relapse. The diagnostic specificity of skin smears is almost 100%; however, its sensitivity is rarely more than 50% because smear-positive patients represent only 10–50% of all cases. SSS is prepared by scraping the sides of slit(s) made in the skin over lesion(s) and other sites like earlobes, forehead, knees, elbows, and fingers. Bacterial index (BI) and morphological index (MI) are calculated for follow-up. The density of bacilli in smears is known as the bacteriological index (BI) and includes both living and dead bacilli. It is reported in a scale from 1 to 6 depending upon the number of bacilli in a smear. The morphological index (MI) is the percentage of solid-stained bacilli, calculated after examining 200 red staining elements, lying singly. It is a useful indicator of progress in patients under treatment and changes more rapidly than the BI. Ideally the MI should become zero in about 6 weeks after starting MDT as more than 99% of bacilli are killed with the first dose. A rise in the MI while a patient is receiving treatment indicates lack of compliance by the patient, incomplete absorption of the drug, or that the bacilli have become resistant to the drug. SSS is no longer recommended by WHO in screening or diagnosis of leprosy because it has the potential risk of transmitting HIV and HBV infections and wide interobserver variations [62].
Skin/Nerve Biopsies
The histopathology of the skin or nerves is an important modality for confirmation of diagnosis and classification of disease and evolution of the disease which may not be evident clinically (downgrading/upgrading). Hematoxylin-eosin staining should always be complemented with Fite-Faraco staining or one of its variations to detect the bacillary load. Sometimes the inflammatory infiltrate of the nerves may be distinct from the ones in the cutaneous lesions, with lower histological grading (toward the lepromatous pole) in the nerves as compared to the cutaneous lesions. Histopathology is also important in differentiating relapse from reversal reactions [63].
Skin Tests
Efforts to develop a diagnostic skin test using proteins and peptides from antigens purified from M. leprae are underway since a long time, but we still do not have an ideal skin test to diagnose patients with paucibacillary spectrum where the CMI predominantly plays a role in the disease pathogenesis [64]. The lepromin test is not a useful diagnostic tool; it consists of injecting a calibrated number of autoclaved M. leprae into the skin; the results are assessed after 3–4 weeks. The test does not measure exposure or infection. A positive test reflects the ability to develop a granuloma following exposure to M. leprae antigens; a positive test does not indicate exposure to leprosy [64]. Tuberculin skin tests (TSTs) do not significantly cross-react with M. leprae infection; in one study of a population in which tuberculosis was highly endemic, 70% of controls had positive TST, but only 15–50% of leprosy patients had positive TST [65, 66].
Immunohistochemistry
Immunohistochemistry using monoclonal or polyclonal antibodies to detect M. leprae antigens may provide higher sensitivity and specificity than conventional methods, especially in the initial stage of illness or in PB cases. The antibodies against PGL-1, S-100, 35 kDa, 65 kDa, and BCG are used to demonstrate M. leprae in the tissues [63].
19.2 Serology and PCR
PCR is helpful in detecting slow-growing or uncultivable microorganisms and, based on the available genetic data, has been used to detect M. leprae, since 1989. PCR made it possible to detect, quantify, and determine M. leprae viability, showing significantly better results compared to common microscopic examinations. PCR may allow confirming cases of initial, PB, and pure neural leprosy, demonstrating subclinical infection in contacts, monitoring treatment, determining patients’ cure or their resistance to MDT drugs, and helping to understand the mechanisms of M. leprae transmission [67, 68].
Serologic tests—Serologic tests for M. leprae phenolic glycolipid-1 (PGL-1) are described but are not freely available because they are not sufficiently sensitive to provide a reliable measure of infection without other clinical or histologic evidence [69, 70]. Patients with lepromatous disease develop a strong polyclonal antibody response to M. leprae and have positive serologic responses to PGL-1. Patients with tuberculoid disease seldom produce antibody to PGL-1, and therefore the test is not helpful for diagnosis in these patients. Many contacts have been found to have antibodies to PGL-1 also, but only a small percentage of them go on to develop the infection. Thus, PGL-1 is not a reliable diagnostic test nor is it satisfactorily predictive of the development of infection. Further development of serologic tests is an area of active investigation [70].
Detection of anti-PGL-1 by immunochromatographic flow test (ML-Flow test) which is a simple dipstick assay using whole blood samples has been shown to be comparable to the ELISA in its sensitivity, being able to detect >90% of MB patients and 40% of PB patients, with background seropositivity in endemic controls at around 10%. It can prove to be a useful tool in high endemic areas for the control of transmission, and it may even obviate the need for SSS [71, 72].
Another protein termed LID-1 (leprosy IDRI diagnostic 1) constructed from two proteins named ML0405 and ML2331 has also shown promising results as diagnostic tool for leprosy. Positive titers of antibodies against LID-1 protein were found in 87–92% MB and 7–48% PB patients in different populations [71, 73]. Some individuals had high titers of anti-LID-1 antibodies 1 year before the appearance of clinical symptoms of leprosy suggesting a role of this protein in the monitoring of contacts. Interestingly, LID-1 can also be used in a cell-based IGRA assay to determine the cell-mediated immune status as in case of the “QuantiFERON” assay for TB. There has been a lot of research on the immunology and biomarkers of leprosy and its reactions in the past few decades; however, it has not translated into clinical practice, and at present there are no good biomarkers for leprosy diagnosis, susceptibility, detection of reactions, or neuritis [71].
19.3 Evaluation of Nerve Damage
Electrophysiology (EPG) of the peripheral nerves especially the nerve conduction studies with or without sympathetic skin response (which measures autonomic dysfunction) is a sensitive tool for the detection of the earliest alterations of sensory fibers or autonomic functions, thereby detecting the neuropathy much before the clinical symptoms appear. However, EPG is an invasive procedure, and it requires expensive equipment and a neurologist for its interpretation, which limits its applications in leprosy. Moreover it is overly sensitive and at times may detect changes which are not of clinical significance and is not preferred by some researchers [36].
Another emerging investigational modality is high-resolution ultrasonography (HRUS) which is a useful noninvasive tool in the evaluation of the nerve involvement of leprosy. HRUS provides useful information about the nerves involved and degree of nerve enlargement, alterations in nerve morphology, echotexture, vascularity, and fascicular pattern that may be helpful in the diagnosis and treatment of peripheral nerve disorders. The increased blood flow and vascularity observed on ultrasound (US) have been associated with the inflammatory process, and therefore, it could be a useful modality for determining the need to initiate corticosteroid therapy to prevent/treat the nerve damage associated with reactions [74].
19.4 Reactions in Leprosy
Leprosy reactions are responsible for the morbidity associated with the disease. Reactions are seen in up to 50% of patients and are the consequence of the dynamic nature of the immune response to M. leprae . Reactions are responsible for much of the permanent nerve damage, leading to disability and deformities. The term reaction is used to describe the appearance of symptoms and signs of acute inflammation in the lesions of leprosy. Clinically redness, swelling, and tenderness of skin lesions are present with associated swelling, pain, and tenderness of nerves often accompanied by nerve function impairment. New skin lesions may appear and new nerve involvement may become apparent. Three types of reactions are seen in leprosy: type 1 (reversal reaction), type 2 (erythema nodosum leprosum), and type 3 (Lucio phenomenon). These reactions can occur before, during, and after treatment. Some patients have recurrent or persistent reactions which are difficult to manage and cause significant morbidity; it is essential to identify the triggering factors for reaction in these patients.
One of these triggering factors is oral infections (periodontitis, gingivitis, poor dental hygiene and caries teeth, etc.) which favor the expression of intracellular cytokines and probably the inflammatory reaction, acting as a stimulatory signal triggering the reactional episodes, and sometimes treatment of these coinfections may prevent recurrent reactional episodes [36, 75, 76].
19.5 Type 1 Reaction (Reversal Reaction)
It is the delayed type of hypersensitivity due to killing of M. leprae and can occur in any spectrum of the disease but mostly seen in the unstable borderline (BT, BB, BL) leprosy. Type 1 reactions in leprosy can be both upgrading and downgrading reactions; however, it is difficult to clinically differentiate the two, so the term reversal reaction is used for both. It is associated with rapid increase in the specific CMI which presents as inflammatory reaction in the existing skin and nerve lesions. It is characterized by increase in redness, swelling, tenderness/discomfort, and even ulceration in the existing lesions (Fig. 9). There may be a rapidly progressive neuritis which can lead to muscle paralysis and subsequent deformities. Constitutional symptoms are usually absent in these cases [75, 76].

Intense erythema and edema of a lesion in type 1 reaction
19.6 Pathogenesis of Type 1 Reaction
It is related to upregulation in CMI and subsequent interaction of the breakdown product of lepra bacilli with T lymphocytes. Some studies have observed that it is not only the killed bacilli or bacillary products but also the metabolically active M. leprae in the skin or nerve lesion(s) can also trigger type 1 reaction especially in BT-BL spectrum. Incomplete killing or refractoriness to treatment or persistence of M. leprae increases the risk of reaction [77]. There is activation of CD4+ T lymphocytes and macrophages with production of Th1-type cytokines—IFN-γ, IL-2, and IL-12. TNF-α plays a crucial role in induction of type 1 reaction which is evident from the rise of TNF-α levels 4–8 weeks before type 1 reaction and reaction-related nerve impairment episodes [75, 77]. However so far there are no routine laboratory tests or biomarkers to assist in the diagnosis. Elevated serum levels of chemokine CXCL10 have been strongly associated with the occurrence of T1R, although CXCL10 levels are not elevated prior to occurrence of reaction and therefore are not predictive [78, 79].
19.7 Type 2 Reaction
It occurs in patients with multibacillary disease and is seen in the LL and BL spectrum. Attacks are often acute in onset but may become chronic or recur over several years. The cutaneous lesions in type 2 reaction or erythema nodosum leprosum (ENL) typically manifest as painful, red evanescent nodules on the face and extensor surfaces of the limbs (Fig. 10). Rarely the lesions may be bullous, pustular, necrotic, or ulcerative (Fig. 11). Systemic symptoms like fever and malaise are often present, and in severe form, uveitis, dactylitis, arthritis, neuritis, lymphadenitis, myositis, and orchitis are also observed. Sometimes type 2 reaction may present without ENL or cutaneous lesions, and the patient may present with fever and arthritis or severe neuritis. Nerve involvement in the form of acute or subacute neuritis with or without nerve function impairment (NFI) is one of the major criteria for distinguishing mild and severe ENL [75, 76].

Nodular lesions of LL and red evanescent nodules on the back in type 2 reaction

Ulcero-necrotic lesions in severe type 2 reaction
19.8 Pathogenesis of Type 2 Reaction
Type 2 reaction is due to Th2-mediated type 3 hypersensitivity. Lepromatous leprosy is mainly characterized by the predominance of CD8+ cells. With onset of type 2 reaction, macrophages present the M. leprae antigens to the T cells, and there is infiltration of CD4+ cells in the dermis. Increase in IL-4, IL-5, and IL-10 cytokines is indicative of Th2-type response. They stimulate antibody release. Following antibody release, immune complex deposition takes place followed by complement stimulation. There is neutrophilic chemotaxis and levels of TNF-α are increased. This is followed by fever and tissue damage including the nerves [75, 76, 78]. Some studies have also implicated interleukin-6 as a susceptibility gene for leprosy type 2 reaction [80].
20 Systemic Involvement
Leprosy manifestations can resemble many dermatologic and neurological diseases and affect multiple organs, making its recognition challenging. In particular, the neurological and endocrine manifestations caused by leprosy have been long recognized but underestimated, even by specialists. Systemic involvement is usually seen in long-standing disease and predominantly in patients near lepromatous pole due to bacillary dissemination and associated granulomatous infiltration affecting various organs especially the nasal mucosa, eyes, bones, testes, kidneys, lymph nodes, liver, and spleen [81]. Besides the disease, systemic manifestations in the form of constitutional symptoms like fever, malaise, joint pains, and acute inflammation of eyes, joints, and related to reticuloendothelial system, etc. occur mostly as a part of type 2 lepra reaction. Systemic involvement is of significance because it may serve as a sanctuary of M. leprae, which may be responsible for relapse even after adequate therapy [81].
20.1 Treatment
Multidrug therapy (MDT) recommended by WHO in 1982 has proved to be the most effective tool in the treatment of leprosy. It has cured approximately 16 million patients over the last 15 to 20 years. The three main objectives in management of leprosy are to interrupt transmission, cure patients, and prevent development of deformities due to reactions [82].
The concept of giving multiple drugs for treatment of leprosy was based on estimation that an advanced, untreated lepromatous leprosy patient harbors about 11 logs of live bacilli. Out of these, the proportion of naturally occurring drug-resistant mutants is estimated to be 1 in 7 logs for rifampicin and 1 in 6 logs each for dapsone and clofazimine. The organisms resistant to one drug will be susceptible to the other drugs in MDT, because their mechanisms of action are different. With combination therapy, the probability of emergence of mutant resistance to any two drugs reduces to 1 in 13 logs, which is negligible [83].
MDT comprises three drugs: dapsone, rifampicin, and clofazimine.
PB patients are treated with MDT-PB (rifampicin + dapsone) regimen for 6 months, and MB patients are treated with MDT-MB (rifampicin + dapsone + clofazimine) regimen for 12 months [82].
MDT is safe and effective and can be easily administered under field conditions. It is available in convenient monthly calendar blister packs.
MDT-PB | ||
|---|---|---|
Age (in years) | Dapsone: daily unsupervised (mg) | Rifampicin: monthly supervised (mg) |
<10 | 2 mg/kg | 10 mg/kg |
10–14 | 50 | 450 |
15 and above | 100 | 600 |
Duration, 6 months | ||
MDT-MB | ||||
|---|---|---|---|---|
Age group (in years) | Dapsone: daily unsupervised (mg) | Rifampicin: monthly supervised(mg) | Clofazimine | |
Unsupervised: (mg) | Monthly supervised (mg) | |||
<10 | 2 mg/kg | 10 mg/kg | 1 mg/kg | 6 mg/kg |
10–14 | 50 | 450 | 50 on alternate days | 150 |
15 and above | 100 | 600 | 50 daily | 300 |
Duration, 12 months | ||||

Children must receive the same multidrug therapy regimen, and the doses should, ideally, be calculated based on the weight of the child.
21 Other Regimens for Special Situations
Uniform MDT (U-MDT)
Uniform MDT implies same treatment for all patients irrespective of the classification; all leprosy patients (PB and MB) receive 6 months of treatment with rifampicin, clofazimine, and dapsone. WHO in collaboration with the Global Leprosy Programme (GLP) launched a clinical trial for comparative evaluation of U-MDT with conventional WHO-MDT regimens for MB and PB leprosy. In a study from Bangladesh, 1612 patients were enrolled and followed up for over 7 years after diagnosis. During 11,425 person years at risk (PYAR) of follow-up, no relapses were detected, by bacteriological or clinical criteria, in the 918 patients in the 6-month MB-MDT group nor in the 694 patients in the control group. Rate of decline of BI in those who were smear positive was not significantly different between groups. The authors were of the opinion that shortening the duration of treatment from 12 months to 6 months MDT for MB leprosy patients does not lead to increased rates of relapse [84]. However the other view is that although U-MDT for 6 months is well tolerated and may have a marginal beneficial effect in PB leprosy, it is too short a regimen to adequately treat MB leprosy [83].
Accompanied MDT (A-MDT)
It was recommended by WHO for people living in hard-to-reach border areas, urban slums, areas of civil strife, and those working as migrant laborers. The patient is provided with a full course of treatment on their first visit to the leprosy clinics after diagnosis. It is no longer a favorite with leprosy specialists because of issues of nonadherence [83].
Special treatment regimens are required for individual patients who cannot take rifampicin or clofazimine due to side effects or intercurrent diseases or are infected with drug-resistant M. leprae.
The WHO Expert Committee on Leprosy has recommended alternative regimen for adult patients, comprising of ofloxacin, minocycline, and clarithromycin, given in different dosage schedules and different durations for PB and MB leprosy [37, 83].
Drug Resistance
MDT has been the backbone of leprosy elimination so far; hence, drug resistance in leprosy is a matter of concern. The WHO convened a working group of collaborating laboratories to use molecular methods for monitoring of drug resistance globally [85]. There are sporadic reports of drug resistance for dapsone, rifampicin, and ofloxacin, from India and various parts of the world [86]. However, as per the drug resistance surveillance report of 2014:
drug resistance in leprosy is not a big problem at present but it is a potential future challenge [87]. Longitudinal observation however, should be continued, alongside primary and other secondary leprosy case surveillance. The situation in leprosy control is not the same as in TB, and vigilance needs to be continued to prevent the occurrence and spread of drug resistance and thus maintain the effectiveness of MDT [87].
Although mouse foot pad assay is considered to be the gold standard for diagnosing drug resistance, it is a very cumbersome and tedious method and has been replaced by mutation detection by sequencing or DNA microarray for the identification of several mutations associated with resistance to individual agents [86]. The drug resistance-determining region (DRDR) of the genome is amplified for mutations in the rpoB, folP, and gyrA genes to look for resistance for rifampicin, dapsone, and ofloxacin, respectively [86].
Response to Treatment and Follow-up
The erythema and induration of skin lesions may decrease within a few months of starting MDT. Most lesions heal without scarring; however, it may take a few years for cutaneous lesions to resolve fully, and some lesions may persist, depending on the initial number of lesions and severity of infection [82].
After treatment completion, the dead M. leprae are removed from the tissues very slowly; some may persist in the tissues for several years. There is no definitive bacteriological endpoint for treatment since M. leprae cannot be grown in culture and its viability cannot be assessed in biopsies. The presence of bacilli in smears or biopsies after treatment does not indicate treatment failure or drug resistance, and there is no evidence that prolonged antimicrobial treatment enhances the removal of dead M. leprae from tissues although immunotherapy may be helpful in some of these cases.
Given the lack of a definitive therapeutic endpoint (clinical, bacteriological, or immunological), assessing treatment adherence is extremely important in assessing treatment completion. Laboratory evidence has shown that M. leprae are killed rapidly after exposure to rifampicin and the other drugs used in the treatment of leprosy. Experience with WHO-MDT protocols with 1–2 years of treatment has provided good evidence of cure with very few relapses. Therefore, if adherence to these WHO-MDT protocols is good, killing of the bacilli and resolution of the lesions can be expected in majority of patients [88].
During the treatment, the first follow-up visit should be done in 2–4 weeks to evaluate for side effects of medications. After that, routine follow-up visits can be scheduled every 1–3 months. Follow-up visits should include clinical examination, including assessment of the skin, nerves, limbs, and eyes, and laboratory studies to assess drug toxicity wherever facilities are available. Patients should be instructed to report appearance of new skin lesions, nerve function impairment in the form of sensory or motor loss, eye symptoms, reactions, or other complaints. Routine laboratory studies to assess drug toxicity while on treatment include a complete blood count, urinalyses, and renal and liver function tests. Drug toxicity is relatively uncommon after the first year of treatment, and serious toxicity may manifest clinically before it is detected in the laboratory. Asymptomatic liver enzyme elevation of up to three times normal is acceptable.
It is believed that disease progression or worsening during therapy is almost always due to poor adherence to treatment regimes. Therefore, patient education is an important part of each visit; compliance with a prolonged drug regimen is unlikely unless the patient fully understands its necessity. Family cooperation is also very important in ensuring good adherence and treatment completion [89].
The patients should be taught to evaluate the anesthetic or hypoesthetic areas of their hands and feet regularly for evidence of injury and should seek treatment if they find any evidence of injury. Special protective shoes are also required to avoid injury or ulceration in cases of sensory impairment of feet. Motor loss resulting in deformities and disabilities may require physiotherapy and eventually corrective surgery.
Ocular examination should include assessment of lid closure, cornea, and conjunctiva which should be done at the first visit and repeated on follow-up. Complex problems such as iridocyclitis should be managed by an ophthalmologist. Potentially sight-threatening ocular involvements like corneal anesthesia and lagophthalmos require protective measures and corrective surgery.
After completion of treatment, annual follow-up for 3 more years is warranted for tuberculoid (PB) cases and for at least 9 more years for lepromatous (MB) patients. Patients should be advised to return for evaluation if new lesions or other problems develop. The follow-up visits can be planned every 3–6 months where, besides the clinical, neurological, and ocular examination, SSS and biopsy can be repeated in (MB) cases. Skin biopsies should be done preferably from the same lesion at 1- to 2-year intervals to assess the response to treatment by evaluating the reduction of granulomatous inflammation and the decline of bacilli in the tissues.
The proportion of MB cases has been gradually increasing in the post-elimination era. There are unpublished reports about clinical nonresponsiveness to fixed duration MDT in some patients with high bacillary index, and some leprosy workers/physicians feel that something other than the standard MDT may be required for this subset of patients. Some experts feel that since the standard MDT has only one bactericidal drug, rifampicin, newer bactericidal agents like rifapentine, moxifloxacin, sparfloxacin, ofloxacin, minocycline, clarithromycin, etc. may be used in alternative antileprosy regimes for these patients and may prove to be helpful in patients who have drug resistance or are not responsive to WHO-MDT MBR. However there are no guidelines or recommendations for these alternative drug regimes [89].
21.1 Vaccines in Leprosy
Vaccination in leprosy can be immunoprophylactic or immunotherapeutic. Several studies have found immunotherapy with MIP (Mycobacterium indicus pranii) or BCG to be useful particularly in multibacillary patients with high bacterial load as it enhances bacterial clearance by upregulating the specific immune response [90, 91]. Vaccines are better than drugs for a sustained protection because vaccines provide memory but drugs do not. There is an emerging need in leprosy research to further evaluate the vaccines BCG, BCG with heat-killed M. leprae, MIP, ICRC (Indian Cancer Research Centre) strain, M. vaccae, M. vaccae with BCG, and M. habana for leprosy prevention and immunomodulation. Newer vaccines like a subunit vaccine developed by IDRI (Infectious Disease Research Institute) have been tested in armadillo, wherein it was able to prevent nerve damage and may prove useful in humans [89].
MIP has been found to be effective as an immunotherapeutic modality in few studies from India. It was seen that the MIP vaccine led to a faster reduction in bacillary load along with decrease in the frequency and severity of type 2 reactions without exacerbating type 1 reactions and neuritis. It can be used as an adjunct to MDT in leprosy patients with a high bacillary load [90, 91].
21.2 Management of Lepra Reactions
Lepra reactions should be treated promptly to control and prevent complications and deformities. The principles of treatment of reactions are to control the acute inflammation in skin and nerves, alleviate the pain, stop progression of eye damage, and prevent disease progression or worsening. Standard antileprosy treatment (WHO-MDT) should be started or continued along with treatment of reactions. Clinical evidence of ongoing neuritis or new nerve function impairment (NFI) (nerve tenderness, new anesthesia, and/or motor loss) should be carefully sought, and, if present, corticosteroid treatment should be started immediately. Patients need to be reassured and explained about the need to continue MDT [92].
Mild reversal reactions can be treated with aspirin and nonsteroidal anti-inflammatory drugs (NSAIDS). In severe reversal reactions, the presence of neuritis, or involvement of facial lesions, corticosteroids are the drug of choice. The 7th WHO Expert Committee on Leprosy recommended (WHO, 1998) [37] that most reactions and neuritis can be treated successfully under field conditions by a standard 12-week course of prednisolone (starting dose 40–60 mg daily); however, some clinicians believe that this duration might be short and could lead to recurrences. The dose should be maintained until the inflammatory changes in skin lesions and the neuritic pain have subsided. Then tapering of the drug can begin slowly until a maintenance dose of 10–15 mg (0.3 mg/kg) prednisolone daily is reached, which must be continued for 3–4 months. Resting of the affected limb in case of neuritis to prevent further deterioration and splinting in the functional position with gentle joint movements to prevent contractures are important components of care. Once the acute inflammation has subsided, physiotherapy should be initiated. For the patients who cannot tolerate or become steroid dependent, alternate drugs most commonly used are azathioprine, methotrexate, cyclosporine, mycophenolate mofetil, etc. In cases of persistent severe nerve pain or nerve abscess, surgery (decompression) is necessary.
Mild cases of type 2 lepra reaction can be managed symptomatically with analgesics and rest and taking care of the precipitating factors like intercurrent infections like malaria, filariasis, tuberculosis, and helminthic infections and psychological and physical stress. In cases of severe reaction, thalidomide is the drug of choice, if available and not contraindicated in the given patient. Thalidomide is given in an initial dosage of 300–400 mg/day (6 mg/kg/day), which will control the reaction within 48 h. The dose is then reduced gradually (100 mg/week). Patients should be stabilized on the lowest possible dose of thalidomide to control symptoms (50–100 mg daily) and be maintained on this till the control of the disease. A good alternative if thalidomide is unavailable or contraindicated in the patient is corticosteroids; 60 mg of prednisolone (1–2 mg/kg/day) daily will control most reactions, and tapering can usually be done more quickly compared with type 1 lepra reaction.
In a significant proportion of patients, ENL becomes chronic and the patient will need continuous steroid treatment. In these cases, high-dose clofazimine is useful, given in a dose of 300 mg daily until the steroids are discontinued. The dose of clofazimine can be then tapered gradually to 50 mg daily. Other drugs tried in refractory cases of ENL are azathioprine, cyclosporine, methotrexate, pentoxifylline, colchicine, mycophenolate mofetil, zinc, and infliximab. Newer drugs like leukotriene receptor antagonist (zafirlukast and montelukast), thalidomide derivative (Revlimid and Actimid), and anti-TNF-α antibody like infliximab have also been tried successfully in few cases, but the evidence is lacking [75, 76]. Immunotherapy (MIP/BCG) and minocycline can also be tried in some patients with high bacillary load as these agents also help to reduce the bacillary load, and minocycline has additional anti-inflammatory properties [93].
21.3 Treatment and Prophylaxis for Nerve Damage
The multidrug therapy used in the treatment in leprosy is mostly targeted at killing the organism but not preventing the nerve damage. Hence interventions to prevent or treat the nerve damage are required. Steroids are the most commonly used drug for this purpose although the recovery may be limited and prevention is not guaranteed. Few studies have been undertaken to see the response to treatment in prevention and recovery of the nerve damage in leprosy.
TRIPOD study is a triad of randomized, controlled trial on prevention of neuropathy which leads to impairment and disability in leprosy.
TRIPOD I
In the study done in Nepal and Bangladesh, 20 mg of prednisolone was given to multibacillary patients requiring 12 months of MDT. Prednisolone was started with MDT; full dose was given for the first 3 months and tapered and stopped in the 4th month. There was significant reduction of the events of neuritis/reaction by 75% in the first 4 months, but the effect was not sustained. At the end of 12 months, only 31% reduction in the events occurred as compared to control group which was not significant [94].
TRIPOD II
It was designed to investigate whether the leprosy patients with mild sensory impairment have a better prognosis when treated with steroids than similarly impaired patients treated with placebo. The patients were treated with prednisolone starting at 40 mg daily and tapered over 16 weeks. The study showed no significant difference in the outcome at the end of study [95].
TRIPOD III
In this study, patients with untreated nerve function impairment for less than 6 months and those with NFI of more than 6 months and less than 24 months were included. The patients with nerve function impairment of more than 6 months are usually not offered any treatment. The patients were started on prednisolone 40 mg OD, and it was tapered by 5 mg every 2 weeks until 16 weeks when the steroids were tapered and stopped. The study showed there was no significant difference between the patients administered with steroids and in the placebo group both with recent or long-standing NFI [96].
Although steroids are effective in acute neuritis and recent onset NFI, evidence from these three randomized controlled trials is insufficient to draw robust conclusions about the long-term effect of corticosteroids for treating nerve damage in leprosy. Two trials, of which one treated long-standing nerve function impairment and the other mild sensory impairment, did not show significantly better outcomes with corticosteroids than placebo for treating nerve damage in leprosy in the long term [97]. However, another study with 5-month duration of steroid therapy reported better results compared to the group which was given steroids for 3 months. May be the dose or duration of therapy was not adequate—in the TRIPOD series [98]. However, it was observed that standard corticosteroid regimens are not significantly more harmful than placebo treatment. Despite known adverse effects of corticosteroids [98], in a recent update on use of corticosteroids in management of leprous neuropathy, it was concluded that more RCTs are required to establish optimal corticosteroid regimens (dose and duration) and to examine the efficacy and safety of adjuvant or new therapies for treating nerve damage in leprosy. Nerve decompression is another alternative in case of acute neuritis or nerve abscess in leprosy which is generally reserved for cases not responding to medical treatment, although some researchers believe that it can be considered in early management of acute neuritis as well. Besides the efficacy and safety, we should also address nonclinical aspects, such as costs and impact on quality of life, which are highly relevant indicators for both policymakers and participants [98].
22 Other Treatment Issues
22.1 Relapse
WHO recommends 1 year of MB-MDT for MB patients (12 pulses in 18 months) and 6 months of PB-MDT (6 pulses in 9 months) for PB patients. At any point of time during therapy, the patient should have ingested two-thirds of the pulses till that time. For operational purposes, once a patient receives adequate chemotherapy, he is considered “cured” [99]. Histopathological resolution of the lesions and clinical subsidence of the disease may take months to years after MDT is stopped. So it is difficult to define relapse when there are no defined criteria of clinical or bacteriological cure. However for operational purposes, the WHO in 1988 proposed that “A patient who successfully completes an adequate course of MDT, but who subsequently develops new signs and symptoms of the disease, either during the surveillance period (2 years for PB and 5 years for MB leprosy) or thereafter” as relapse [37]. However some of the leprosy researchers are of the opinion that a period of 2 and 5 years is very short when we are defining follow-up for detecting relapse rate and should be extended to 3 and 9 years. The other definitions and criteria like clinical, bacteriological, histopathological, or immunological criteria are used for research. Relapse of leprosy is relatively rare and must be distinguished from immunologic reaction (which is more common). The World Health Organization has reported that among 103 countries reporting relapses, 57 reported zero relapses and 46 reported relapse after treatment, with a total of 3039 cases reported in 2015 [4].
Most relapses occur 5–10 years after completion of treatment. Relapse is more likely to occur in the setting of incomplete treatment or a very high bacterial load at the onset of treatment [100]. Patients who have had recurrent or persistent reactions and have been treated with steroids are also more likely to relapse than patients with lesser reactions during true relapse; the tissue bacterial load generally rises steadily. Relapse can be distinguished from immunologic reaction in that the latter should improve after a short course of prednisone [99].
There is little evidence to guide the approach to retreatment after relapse. In general, treatment consists of reinitiating the same regimen used for initial therapy [99]. Patients who presented initially with tuberculoid (paucibacillary, PB) disease but relapse with lepromatous (multibacillary, MB) leprosy should be retreated with an MB regimen. Drug resistance is extremely unlikely to have developed as long as the original M. leprae strain was fully sensitive to the drugs used, although there is no role for baseline testing of drug resistance. When indicated, testing for mutations can be done from paraffin-embedded tissues taken at the time of diagnosis (i.e., before treatment) and at the time of suspected relapse or resistance.
Leprosy and HIV
There has been no increase in leprosy in regions where HIV is prevalent. In patients coinfected with M. leprae and HIV, initiation of antiretroviral therapy may trigger a type 1 reaction; this is a manifestation of the immune reconstitution inflammatory syndrome [101]. Although worsening of disease and increased incidence of reactions in patients with HIV coinfection have been observed by some, this has not been confirmed in all the studies.
The response to leprosy treatment in HIV-infected individuals appears to be comparable with the response in HIV-uninfected individuals.
Leprosy and Pregnancy
Management of leprosy and immunologic reactions in pregnancy is the same as described above for other patients. Leprosy can be exacerbated during pregnancy, and without treatment it can permanently damage the skin, nerves, limbs, and eyes; therefore WHO-MDT should be taken regularly in all the stages of pregnancy and during lactation as it also protects the child from getting infected. Immunologic reactions appear to occur more frequently in pregnancy and postpartum period. In two small series, such reactions were observed in up to 38 percent of patients [102]. Type 2 reactions were observed more frequently during pregnancy; type 1 reactions were observed more frequently in the postpartum period.
22.2 Prevention
Control measures for leprosy include clinical management of active cases as well as contact management. Household contacts should be evaluated annually for evidence of disease for at least 5 years and should be educated to seek immediate attention if skin or neurologic changes suggestive of leprosy develop.
There are no universally accepted recommendations for prophylaxis in contacts; however, a randomized controlled trial with chemoprophylaxis for contacts of leprosy patients using a single dose of rifampicin (SDR) has shown an overall protective effect of approximately 60%, effective in the first 2 years after the intervention. This protective effect increased to 80% in contacts who had previously received BCG vaccination. It was observed that SDR for contacts of patients with newly diagnosed leprosy was effective for preventing development of clinical disease within 2 years, and the authors observed no difference between the placebo and rifampicin groups after 2 years.
BCG alone or in combination with Mycobacterium leprae or related mycobacterial vaccines has been used in vaccine trials for immunoprophylaxis in contacts of leprosy patients, with BCG giving the best results. Meta-analysis shows that the protective effect of BCG is better in observational studies (60%) than in clinical trials, 41%, and it is higher among contacts of leprosy patients than among the general population, 68% versus 53% [103].
BCG is administered at birth in most countries with high rates of leprosy, and vaccination with BCG is partially protective for leprosy; a single dose appears to be 50% protective, and two doses further increase this protection. However vaccination for prevention of leprosy is economically feasible only in areas with an extremely high incidence of the disease and may not be feasible in other areas with low endemicity. There has been a renewed interest in development of an improved BCG vaccine, BCG booster, or alternate vaccine strain that could benefit control of both tuberculosis and leprosy. Skin test antigen studies and the identification of the appropriate protective M. leprae genomic DNA sequence could also help in the development of an improved vaccine for leprosy. The future leprosy control strategy should include contact management, consisting of a contact survey, and chemoprophylaxis or immunoprophylaxis. Modeling studies have shown that both interventions will lower the incidence of leprosy in the population by interrupting the transmission of M. leprae. Implementation studies of such contact-based strategy are the need of the hour.
In an attempt to check the transmission of leprosy and further reduce the leprosy burden, the Indian government has started a pilot project in five districts of Bihar and Gujarat where the MIP vaccine will be administered as a preventive measure to people living in close contact with those infected.
22.3 Rehabilitation in Leprosy: Prevention of Impairment and Disabilities and Deformities
Although leprosy is responsive to MDT, disabilities of the eyes, hands, and feet due to neuropathy are often not reversible and may require lifelong care and rehabilitation. Therefore, early diagnosis and complete treatment are necessary to minimize the likelihood of these disabilities. The central goal of rehabilitation is to restore the health and dignity of someone affected by an illness that may have caused physical, mental, or emotional hurt and that may have led to social problems, such as the loss of a job or the disruption of close relationships [82].
Transient or permanent nerve damage is responsible for most of the impairments and disabilities in leprosy. A baseline nerve function assessment should be done at the time of diagnosis, and it should be repeated at regular intervals; after diagnosis the frequency of assessment can be more if patients have neuritis at the time of diagnosis or are undergoing treatment for neuropathy [104]. Motor function can be assessed and monitored by the manual muscle strength tests, and sensory function can be assessed by tests for touch or temperature perception.
Footwear with a hard under sole and soft, cushioned insoles are required for people with sensory impairment of feet to prevent further injuries and deformities. In cases with severe structural deformity of feet due to previous ulcers, fitted shoes may be necessary. Regular physiotherapy or specific exercises should be taught to prevent (or overcome) contractures of paralyzed hands. The leprosy-affected person with paralyzed eyelid muscles needs to develop the habit of attempting regular eye closure (think and blink). They should take safety precautions when cooking, insulating all the cooking utensils and keeping a distance from open fires. They also need to rehydrate dry skin due to loss of autonomic nerve function via soaking and oiling [104].
22.4 Role of Surgery
The residual disability or deformity due to leprosy is a serious long-term condition, which requires ongoing care and attention and eventually surgery. Surgical management is required for deformities and disabilities, like claw hand and lagophthalmos, by reconstructive and tendon transfer surgeries. Decompression of nerves (neurolysis) was undertaken as a management of acute neuritis, and, although it does provide pain relief in chronic painful nerves and can be used to evacuate nerve abscesses, the evidence to recommend it for all cases of neuritis is lacking [104].
22.5 Stigma and Socioeconomic Rehabilitation with Empowerment of Leprosy Patients
Leprosy stigma is still a global phenomenon in both endemic and non-endemic countries. In the past, the stigma was due to the fact that leprosy was considered incurable, but now when we have a robust MDT which can cure leprosy, the stigma continues in the mind of community due to deformities associated with leprosy. The social and emotional consequences of leprosy are often far more deep-seated and disruptive and last a lifetime. Rehabilitation in the field of leprosy is an immense and wide-ranging challenge due to all these factors. Community education and changes in legislation are still needed in leprosy-endemic countries to eradicate the stigma associated with leprosy and ensure equal rights and opportunities for people affected by leprosy.
The rehabilitation interventions and the organizations associated with it have changed dramatically over years. In the past, the focus was on the professional, biomedical remedies organized by hospitals and similar institutions; however, this approach was costly and underutilized resources were available in the community. Initiatives by individuals and groups in the community gradually led to community-based rehabilitation (CBR) [3]. CBR has grown in scope over the years and now has strong links with community development and poverty alleviation as poverty and disability generally go hand in hand [105].
In order to be truly restored to their lives of dignity, those affected need to feel that they have more control over key areas of their lives. A certain level of empowerment is needed to provide the motivation for change, leading to normalization. This has led to self-care and self-help movements in the leprosy-endemic areas The leprosy patients need to be actively involved in leprosy control and rehabilitation programs [105].
22.6 Multimorbidity in Leprosy
Leprosy patients are also at risk of incurring numerous other comorbidities or chronic conditions (like hypertension tuberculosis, diabetes, etc.) which can further adversely affect their quality of life. Integration of leprosy into basic healthcare services (with leprosy-related treatment being offered by the same staff at the same place and time as treatment for other medical conditions) is one solution to tackle this problem and is being done in most endemic countries, although such full integration is not yet achieved everywhere [106].
Another potential approach is the concept of “reverse integration,” which means bringing other healthcare services into existing leprosy services, which is difficult but is being done in some endemic countries. Advantages include accessibility to specialized services under one place, affordability, and better integration of patients into rehabilitation programs [107].
22.7 Leprosy Control
The overall declining trend in the prevalence or new case detection rates should not lead to complacency and stopping further active surveillance or contact tracing. There are millions of cases that are not detected by the current practice of self-reporting as about half of the undiagnosed cases are symptomatic, which clearly indicates the failure of practice to identify all cases. According to a mathematical model to predict the number of cases at a given time, a study estimated that more than 4 million cases will be missed worldwide between 2000 and 2020 [108]. This clearly indicates the necessity of additional strategies such as chemoprophylaxis to household contacts and preferably a wider range of contacts, as well as active case finding in high-risk populations [109].
22.8 Prognosis
Long-term prognosis in leprosy patients treated with the recommended dose and duration of therapy is good, as evidenced by the low relapse rates. Mortality in leprosy is very low; however, it causes significant physical and psychological comorbidity due to its sequelae-like deformities and disfigurement. Despite high cure rates after introduction of MDT, nerve involvement, neuritis, and nerve function impairment frequently lead to deformities which are common in all types of leprosy especially where diagnosis is delayed and in those with manual occupations. This leads to social stigmatization which remains one of the most unfortunate aspects of the disease.
22.9 Research Priorities in Post-elimination Era
Leprosy has been eliminated (as a public health problem) but it has not been eradicated. Leprosy transmission continues unabated in the endemic countries as the new case detection rate has not reduced significantly. MDT alone may not be sufficient to eradicate leprosy. There is the need for continued efforts that promote educational programs for health professionals, sustain control activities in the developing world, and promote investment in primary care systems. We will have to alleviate poverty, illiteracy, and ignorance if we want to eradicate leprosy. Leprosy research should continue on all fronts and the priorities in the next few years will be:
-
To develop better and sensitive laboratory tools for early diagnosis of leprosy
-
To work on identification of predictors for reactions and their treatment
-
To develop tools for predicting neuritis and its prevention and development of neuroprotective agents for treatment of neuritis
-
To develop vaccine for prophylaxis
-
To improve the understanding of transmission dynamics
-
To monitor and evaluate treatment failures and delayed and altered clinical responses
-
To train and reorient workers with latest technologies and developments
-
To monitor drug resistance
-
To eradicate the stigma by creating awareness about leprosy in the community and empower people affected by leprosy
References
Robbins G, Tripathy VM, Misra VN, Mohanty RK, Shinde VS, Gray KM, Schug MD. Ancient skeletal evidence for leprosy in India (2000 B.C.). PLoS One. 2009;4(5):e5669.
Eichelmann K, González González SE, Salas-Alanis JC, Ocampo-Candiani J. Leprosy. An update: definition, pathogenesis, classification, diagnosis, and treatment. Actas Dermosifiliogr. 2013;104:554–63.
Suzuki K, Akama T, Kawashima A, Yoshihara A, Yotsu RR, Ishii N. Current status of leprosy: epidemiology, basic science and clinical perspectives. J Dermatol. 2012;39:121–9.
Global Leprosy Update, 2016: Accelerating Reduction Of Disease Burden. Wkly Epidemiol Rec. 2017;92:501–20.
WHO. Global leprosy strategy 2016–2010. Accelerating towards a leprosy-free world World Health Organization (2015).
Franco-Paredes C, Rodriguez-Morales AJ. Unsolved matters in leprosy: a descriptive review and call for further research. Ann Clin Microbiol Antimicrob. 2016;15(1):33.
NLEP – Annual Report for the year 2016–17. Central Leprosy Division, DGHS, Govt of India. 2017.
NLEP. Programme Implementation Plan (PIP) for 12th Plan Period (2012–13 to 2016–17). Available from nlep.nic.in/pdf/Final%20PIP,on%203%20May%202013.pdf.
NLEP – Progress Report for the year 2015–16 Central Leprosy Division, DGHS, Govt of India. 2016.
Scollard D, Stryjewska B. Epidemiology, microbiology, clinical manifestations, and diagnosis of leprosy. http://www.uptodate.com/patients/content/topic.do. Accessed 13 Oct 2016.
Sekar B. Bacteriological aspects. In: Kumar B, Kar HK, editors. IAL textbook of leprosy. New Delhi: Jaypee; 2016. p. 90–104.
Gupta UD, Katoch VM. Animal models in leprosy. Indian J Med Microbiol. 1995;13:57–64.
Cole ST, Eiglmeier K, Parkhill J, James KD, Thomson NR, Wheeler PR, et al. Massive gene decay in the leprosy bacillus. Nature. 2001;409:1007.
Eiglmeier K, Parkhill J, Honoré N, Garnier T, Tekaia F, Telenti A, Klatser P, James KD, Thomson NR, Wheeler PR, Churcher C, Harris D, Mungall K, Barrell BG, Cole ST. The decaying genome of Mycobacterium leprae. Lepr Rev. 2001;72(4):387.
Monot M, Honoré N, Garnier T, Zidane N, Sherafi D, Paniz-Mondolfi A. Comparative genomic and phylogeographic analysis of Mycobacterium leprae. Nat Genet. 2009;41:1282.
Han XY, Quintanilla M. Diffuse lepromatous leprosy caused by mycobacterium Lepromatosis in Quintana Roo, Mexico. J Clin Microbiol. 2015;53:3695–8.
Singh P, Benjak A, Schuenemann VJ. Insight into the evolution and origin of leprosy bacilli from the genome sequence of Mycobacterium lepromatosis. Proc Natl Acad Sci USA. 2015;112:4459–64.
Han XY, Seo Y-H, Sizer KC, et al. A new Mycobacterium species causing diffuse lepromatous leprosy. Am J Clin Pathol. 2008;130:856–64.
Han XY, Sizer KC, Thompson EJ, et al. Comparative sequence analysis of Mycobacterium leprae and the new leprosy-causing Mycobacterium lepromatosis. J Bacteriol. 2009;191:6067–74.
Goulart LR, Goulart IM. Leprosy pathogenetic background: a review and lessons from other mycobacterial diseases. Arch Dermatol Res. 2009;301(2):123–37.
Gaschignard J, Grant AV, Thuc NV, Orlova M, Cobat A, Huong NT, Ba NN, Thai VH, Abel L, Schurr E, Alcaïs A. Pauci- and multibacillary leprosy: two distinct, genetically neglected diseases. PLoS Negl Trop Dis. 2016;10(5):e0004345.
Siddiqui MR, Meisner S, Tosh K, Balakrishnan K, Ghei S, Fisher SE, et al. A major susceptibility locus for leprosy in India maps to chromosome 10p13. Nat Genet. 2001;27:439–41.
Mira MT, Alcaïs A, Van Thuc N, Thai VH, Huong NT, Ba NN, et al. Chromosome 6q25 is linked to susceptibility to leprosy in a Vietnamese population. Nat Genet. 2003;33:412–415. doi:10.1038/ng1096. PMID:12577057.
Tosh K, Meisner S, Siddiqui MR, Balakrishnan K, Ghei S, Golding M, et al. A region of chromosome 20 is linked to leprosy susceptibility in a South Indian population. J Infect Dis. 2002;186:1190–3.
Bhat RM, Prakash C. Leprosy: an overview of pathophysiology. Interdiscip Perspect Infect Dis. 2012;2012:181089.
Wilder-Smith EP, Van Brakel WH. Nerve damage in leprosy and its management. Nat Clin Pract Neurol. 2008;4:656–63.
Turankar RP, Lavania M, Singh M, Siva Sai KSR, Jadhav RS. Dynamics of Mycobacterium leprae transmission in environmental context: deciphering the role of environment as potential reservoir. Infect Genet Evol. 2012;12:121–6.
Wheat WH, Casali AL, Thomas V, Spencer JS, Lahiri R, Williams DL, McDonnell GE, Gonzalez Juarrero M, Brennan PJ, Jackson M. Long-term survival and virulence of Mycobacterium leprae amoebal cysts. PLoS Neglec Trop Dis. 2014;8(12):e3405.
Truman R, Fine PE. ‘Environmental’ sources of Mycobacterium issues and evidence. Lepr Rev. 2010;81:89–95.
Sharma R, Singh P, Loughry WJ, Lockhart JM, Inman WB, Duthie MS, Pena MT, Marcos LA, Scollard DM, Cole ST, Truman RW. Zoonotic leprosy in the Southeastern United States. Emerg Infect Dis. 2015;21:2127–34.
Bratschi MW, Steinmann P, Wickenden A, Gillis TP. Current knowledge on Mycobacterium leprae transmission: a systematic literature review. Lepr Rev. 2015;86:142–55.
Polycarpou A, Walker SL, Lockwood DN. New findings in the pathogenesis of leprosy and implications for the management of leprosy. Curr Opin Infect Dis. 2013;26:413–9.
Scollard DM, Truman RW, Ebenezer GJ. Mechanisms of nerve injury in leprosy. Clin Dermatol. 2015;33:46–54.
Shetty VP. Pathomechanisms of nerve damage. In: Kumar B, Kar HK, editors. IAL textbook of leprosy. New Delhi: Jaypee; 2016. p. 170–81.
Pinheiro RO, De Souza Salles J, Sarno EN, Sampaio EP. Mycobacterium leprae host-cell interactions and genetic determinants in leprosy: an overview. Future Microbiol. 2011;6:217–30.
Foss NT, Motta AC. Leprosy, a neglected disease that causes a wide variety of clinical conditions in tropical countries. Mem Inst Oswaldo Cruz. 2012;107(Suppl 1):28–33.
WHO Expert Committee on Leprosy. WHO Expert Committee on Leprosy: Eighth report Report. WHO Tech Rep Ser. 968; Geneva, Switzerland 2012.
Lockwood DNJ, Sarno E, Smith WC. Classifying leprosy patients – searching for the perfect solution? Lepr Rev. 2007;78:317–20.
Moschella SL. An update on the diagnosis and treatment of leprosy. J Am Acad Dermatol. 2004;51(3):417–26.
Ridley DS, Jopling WH. Classification of leprosy according to immunity. A five-group system. Int J Lepr Other Mycobact Dis. 1966;34:255–73.
Kumar B, Dogra S. Case definition and clinical types of Leprosy. In: Kumar B, Kar HK, editors. IAL textbook of leprosy. New Delhi: Jaypee; 2016. p. 236–53.
Vargas-Ocampo F. Diffuse leprosy of Lucio and Latapí: a histologic study. Lepr Rev. 2007;78(3):248–60.
Wade HW. The histoid variety of lepromatous leprosy. Int J Lepr. 1963;31:129–42.
Kaur I, Dogra S, De D, et al. Histoid leprosy: a retrospective study of 40 cases from India. Br J Dermatol. 2009;160:305–10.
Kumar B, Kaur I, Dogra S, Kumaran MS. Pure neuritic leprosy in India: an appraisal. Int J Lepr Other Mycobact Dis. 2004;72:284–90.
Rao PN, Suneetha S. Pure neuritic leprosy: Current status and relevance. Indian J Dermatol Venereol Leprol. 2016;82(3):252–61.
Nascimento OJ. Leprosy neuropathy: clinical presentations. Arq Neuropsiquiatr. 2013;71:661–6.
Van Brakel WH, Khawas IB. Silent neuropathy in leprosy: an epidemiological description. Lepr Rev. 1994;65:350–60.
van Brakel WH, Nicholls PG, Wilder-Smith EP, Das L, Barkataki P, Lockwood DN, INFIR Study Group. Early diagnosis of neuropathy in leprosy – comparing diagnostic tests in a large prospective study (the INFIR cohort study). PLoS Negl Trop Dis. 2008;2(4):e212.
Garbino JA, Heise CO, Marques W Jr. Assessing nerves in leprosy. Clin Dermatol. 2016;34:51–8.
Raicher I, Stump PR, Baccarelli R, Marciano LH, Ura S, Virmond MC, Teixeira MJ, Ciampi de Andrade D. Neuropathic pain in leprosy. Clin Dermatol. 2016;34:59–65.
Gitte SV, Sabat RN, Kamble KM. Childhood leprosy in an endemic area of Central India. Indian Pediatr. 2016;53:221–4.
Dogra S, Narang T, Khullar G, Kumar R, Saikia UN. Childhood leprosy through the post-leprosy-elimination era: a retrospective analysis of epidemiological and clinical characteristics of disease over eleven years from a tertiary care hospital in North India. Lepr Rev. 2014;85:296–310.
Oliviera MB, Diniz LM. Leprosy among children under 15 years of age: literature review. An Bras Dermatol. 2016;91:196–203.
WHO Global Leprosy Strategy agreed for 2011–2015. www.searo.who.int/EN/Section980/Section2572/Section2578_14961.htm
Grzybowski A, Nita M, Virmond M. Ocular leprosy. Clin Dermatol. 2015;33:79–89.
Malik AN, Morris RW, Ffytche TJ. The prevalence of ocular complications in leprosy patients seen in the United Kingdom over a period of 21 years. Eye (Lond). 2011;25:740–5.
Chauhan S, Wakhlu A, Agarwal V. Arthritis in leprosy. Rheumatology (Oxford). 2010;49:2237–42.
Prasad S, Misra R, Aggarwal A, Lawrence A, Haroon N, Wakhlu A, Krishnani N, Agrawal V, Paliwal VK, Jha S, Agarwal V. Leprosy revealed in a rheumatology clinic: a case series. Int J Rheum Dis. 2013;16:129–33.
Mahajan V, Sharma NL. Differential diagnosis of dermatological conditions. In: Kumar B, Kar HK, editors. IAL textbook of leprosy. New Delhi: Jaypee; 2016. p. 298–315.
Shah BJ. Differential diagnosis of neurological and other disorders in relation to leprosy. In: Kumar B, Kar HK, editors. IAL textbook of leprosy. New Delhi: Jaypee; 2016. p. 316–30.
Mahajan VK. Slit-skin smear in leprosy: lest we forget it! Indian J Lepr. 2013;85:177–83.
Lastória JC, de Abreu MA. Leprosy: a review of laboratory and therapeutic aspects – part 2. An Bras Dermatol. 2014;89:389–401.
Brennan PJ. Skin test development in leprosy: progress with first-generation skin test antigens, and an approach to the second generation. Lepr Rev. 2000;71 Suppl:S50.
Mitra DK, Joshi B, Dinda AK, Rai AK, Girdhar BK, Katoch K, Bindra MS, Sengupta U. Induction of lepromin reactivity in cured lepromatous leprosy patients: impaired chemokine response dissociates protective immunity from delayed type hypersensitivity. Microbes Infect. 2009;11(14–15):1122.
Kaplan G, Laal S, Sheftel G, Nusrat A, Nath I, Mathur NK, Mishra RS, Cohn ZA. The nature and kinetics of a delayed immune response to purified protein derivative of tuberculin in the skin of lepromatous leprosy patients. J Exp Med. 1988;168:1811.
Job CK, Jayakumar J, Williams DL, Gillis TP. Role of polymerase chain reaction in the diagnosis of early leprosy. Int J Lepr Other Mycobact Dis. 1997;65:461–4.
Banerjee S, Biswas N, Kanti Das N, Sil A, Ghosh P, Hasanoor Raja AH, Dasgupta S, et al. Diagnosing leprosy: revisiting the role of the slit-skin smear with critical analysis of the applicability of polymerase chain reaction in diagnosis. Int J Dermatol. 2011;50:1522–7.
Butlin CR, Soares D, Neupane KD, Failbus SS, Roche PW. IgM anti-phenolic glycolipid-I antibody measurements from skin-smear sites: correlation with venous antibody levels and the bacterial index. Int J Lepr Other Mycobact Dis. 1997;65:465.
Oskam L, Slim E, Bührer-Sékula S. Serology: recent developments, strengths, limitations and prospects: a state of the art overview. Lepr Rev. 2003;74:196.
De Souza VN, Iyer AM, Lammas DA, Naafs B, Das PK. Advances in leprosy immunology and the field application: a gap to bridge. Clin Dermatol. 2016;34(1):82–95.
Aseffa A, Brennan P, Dockrell H, Gillis T, Hussain R, Oskam L, Richardus JH, Ideal Consortium. Report on the first meeting of the IDEAL (Initiative for Diagnostic and Epidemiological Assays for Leprosy) consortium held at Armauer Hansen Research Institute, ALERT, Addis Ababa, Ethiopia on 24–27 October 2004. Lepr Rev. 2005;76:147.
Fabri Ada C, Carvalho AP, Vieira NF, Bueno Ide C, Rodrigues RN, Monteiro TB, Correa-Oliveira R, Duthie MS, Lana FC. Integrative literature review of the reported uses of serological tests in leprosy management. Rev Soc Bras Med Trop. 2016;49:158–64.
Jain S, Visser LH, Suneetha S. Imaging techniques in leprosy clinics. Clin Dermatol. 2016;34:70–8.
Kar HK, Chauhan A. Leprosy reactions: pathogenesis and clinical features. In: Kumar B, Kar HK, editors. IAL textbook of leprosy. New Delhi: Jaypee; 2016. p. 416–40.
Kamath S, Vaccaro SA, Rea TH, Ochoa MT. Recognizing and managing the immunologic reactions in leprosy. J Am Acad Dermatol. 2014:1268–7.
Save MP, Dighe AR, Natrajan M, Shetty VP. Association of viable Mycobacterium leprae with Type 1 reaction in leprosy. Lepr Rev. 2016;87:78–92.
Stefani MM, Guerra JG, Sousa AL, Costa MB, Oliveira ML, Martelli CT, Scollard DM. Potential plasma markers of Type 1 and Type 2 leprosy reactions: a preliminary report. BMC Infect Dis. 2009;9:75.
Scollard DM, Chaduvula MV, Martinez A, Fowlkes N, Nath I, Stryjewska BM, Kearney MT, Williams DL. Increased CXC ligand 10 levels and gene expression in type 1 leprosy reactions. Clin Vaccine Immunol. 2011;18:947.
Sousa AL, Fava VM, Sampaio LH, Martelli CM, Costa MB, Mira MT, Stefani MM. Genetic and immunological evidence implicates interleukin 6 as a susceptibility gene for leprosy type 2 reaction. J Infect Dis. 2012;205:1417–24.
Ramesh V, Kataria JK. Systemic involvement in leprosy. In: Kumar B, Kar HK, editors. IAL textbook of leprosy. New Delhi: Jaypee; 2016. p. 331–43.
Scollard D, Stryjewska B. Treatment and prevention of leprosy. https://www.uptodate.com/contents/treatment-and-prevention-of-leprosy? Accessed 30 Sep 2016.
Kar HK, Gupta R. Treatment of leprosy. Clin Dermatol. 2015;33:55–65.
Butlin RC, Pahan D, Maug AKJ, Withington S, Nicholls P, Alam K, Salim AH. Outcome of 6 months MBMDT in MB patients in Bangladesh-preliminary results. Lepr Rev. 2016;87:171–82.
Sentinel surveillance for drug resistance in leprosy. Report of the WHO Global Leprosy Programme Meeting Cotonou, Benin, 12–13 November 2012.
Moraes MO. Drug-resistance in leprosy: moving toward understanding the scope of the problem and how to tackle it. Clin Infect Dis. 2016 Aug 23. pii: ciw574. No abstract available.
World Health Organisation. Drug resistance surveillance in leprosy: report of the WHO-ILEP joint meeting 4–6 February 2014, Cebu City, Philippines. 1–31. SEA−GLP−2014.1.
Kaur I, Dogra S, Kumar B, Radotra BD. Combined 12-month WHO/MDT MB regimen and Mycobacterium w. vaccine in multibacillary leprosy: a follow-up of 136 patients. Int J Lepr Other Mycobact Dis. 2002;70:174–81.
Singh I, Lavania M, Nigam A, Turankar RP, Ahuja M, John AS, Sengupta U. Symposium on emerging needs in leprosy research in the post elimination era: The Leprosy Mission Trust India. Lepr Rev. 2016;87:132–43.
Katoch K, Katoch VM, Natrajan M, et al. Treatment of bacilliferous BL/LL cases with combined chemotherapy and immunotherapy. Int J Lepr. 1995;63:202–12.
Narang T, Kaur I, Kumar B, et al. Comparative evaluation of immunotherapeutic efficacy of BCG and Mw vaccines in patients of borderline lepromatous and lepromatous leprosy. Int J Lepr. 2005;73:105–14.
Sehgal VN, Sardana K, Dogra S. Management of complications following leprosy: an evolving scenario. J Dermatolog Treat. 2007;18:366–74.
Narang T, Sawatkar GU, Kumaran MS, Dogra S. Minocycline for recurrent and/or chronic erythema nodosum leprosum. JAMA Dermatol. 2015;151:1026–8.
Smith WC, Anderson AM, Withington SG, van Brakel WH, Croft RP, Nicholls PG, Richardus JH. Steroid prophylaxis for prevention of nerve function impairment in leprosy: randomised placebo controlled trial (TRIPOD 1). BMJ. 2004;328:1459.
Van Brakel WH, Anderson AM, Withington SG, Croft RP, Nicholls PG, Richardus JH, Smith WC. The prognostic importance of detecting mild sensory impairment in leprosy: a randomized controlled trial (TRIPOD 2). Lepr Rev. 2003;74:300–10.
Richardus JH, Withington SG, Anderson AM, Croft RP, Nicholls PG, Van Brakel WH, Smith WC. Treatment with corticosteroids of long-standing nerve function impairment in leprosy: a randomized controlled trial (TRIPOD 3). Lepr Rev. 2003;74:311–8.
Van Veen NH, Nicholls PG, Smith WC, Richardus JH. Corticosteroids for treating nerve damage in leprosy. A Cochrane review. Lepr Rev. 2008;79:361–7.
Van Veen NH, Nicholls PG, Smith WC, Richardus JH. Corticosteroids for treating nerve damage in leprosy. Cochrane Database Syst Rev. 2016;23(5):CD005491. https://doi.org/10.1002/14651858.CD005491.pub3.
Kaimal S, Thappa DM. Relapse in leprosy. Indian J Dermatol Venereol Leprol. 2009;75:126–35.
WHO Expert Committee on Leprosy. WHO Expert Committee on Leprosy: Seventh Report. WHO Tech Rep Ser. 874; Geneva, 1998.
Lockwood DN, Lambert SM. Human immunodeficiency virus and leprosy: an update. Dermatol Clin. 2011;29:125.
Lockwood DN, Sinha HH. Pregnancy and leprosy: a comprehensive literature review. Int J Lepr Other Mycobact Dis. 1999;67:6.
Richardus JH, Oskam L. Protecting people against leprosy: chemoprophylaxis and immunoprophylaxis. Clin Dermatol. 2015;33:19–25.
Brandsma JW. Rehabilitation of Leprosy-affected people: an overview. Clin Dermatol. 2016;34:66–9.
Saunderson P. Rehabilitation & social aspects: introductory overview. International textbook of leprosy. www.internationaltextbookofleprosy.org. Last Accessed 05 Oct 2016.
Butlin CR. The challenge of multi-morbidity in the context of leprosy. Lepr Rev. 2016;87:151–7.
Iyer FT. Reverse integration in leprosy: lessons from Mker, Nigeria. Asia Pacific Disabil Rehab J. 2006;17:35–41.
Smith WC, van Brakel W, Gillis T, Saunderson P, Richardus JH. The missing millions: a threat to the elimination of leprosy. PLoS Negl Trop Dis. 2015;9:e0003658.
de Matos HJ, Blok DJ, de Vlas SJ, Richardus JH. Leprosy new case detection trends and the future effect of preventive interventions in Para State, Brazil: a modelling study. PLoS Negl Trop Dis. 2016;10:e0004507.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Kumar, B., Narang, T. (2017). Leprosy. In: Singh, S. (eds) Neglected Tropical Diseases - South Asia. Neglected Tropical Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-68493-2_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-68493-2_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-68492-5
Online ISBN: 978-3-319-68493-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)