
Abstract
Leprosy is one of the most primitive diseases with which human beings have been confronted for thousands of years. It primarily affects skin and peripheral nervous system. The cause of disease, Mycobacterium leprae, was discovered by Armauer Hansen in 1873. After the introduction of Multi Drug Therapy (MDT ) by WHO in 1982 as the first effective treatment for leprosy, the prevalence of the disease has decreased significantly in most parts of the world.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Definition
Leprosy is a chronic infectious disease caused by Mycobacterium leprae. It prominently affects the skin and peripheral nerves of the extremities; however, during the advanced stage of multibacillary leprosy, the M. leprae will be found in most of the body tissues and organs with the exception of central nervous system, gastrointestinal tract, and lungs (James et al. 2011).
Historical Overview
One of the most primitive diseases with which human beings have been confronted for their survival is Hansen’s disease or leprosy. As a brief allusion to the provenance of this disease in the history of medicine, one can exemplify the epistle that has been found in India , which is also known to be the oldest of its kind.
In addition, it should be noted that the first-proven documented case of this disease has been discovered in mummies of ancient Egypt . Based on the previously mentioned historical references, it seems that the origin of the disease could be traced back to the Far East and India . Later it expanded to the Middle East and Europe through the ancient Macedonian army during fourth century BC (Browne 1985). After its inception throughout the European countries, the prevalence of leprosy reached to its highest level during the medieval era. Although no treatment for leprosy was available until the twentieth century, it has been widely believed that the occurrence of the disease had been reduced markedly because of noticeable improvements in socioeconomic and healthcare conditions as well as a reduction in population density of families. Leprosy was transmitted to Africa and Canada via European immigrants and later on to the USA through African migrants (Monot et al. 2009).
Epidemiology
Before 1981, when there was no definite treatment for leprosy, patients had to use Dapsone throughout the remainder of their lifetime. The prevalence of this disease was estimated to embrace 11 million of the world population (Daumerie 2003). However, in 1982 after the introduction of Multidrug Therapy (MDT ) by World Health Organization (WHO), its occurrence was decreased significantly and in the beginning of 2012 reached 181,941 (0.34 cases/10,000 population). The tropical regions of South-East Asia (India , Bangladesh , Indonesia , Nepal , and Myanmar ), South America (Brazil ), and Africa (Congo , Ethiopia , Madagascar , Tanzania ) have the highest prevalence of leprosy due to their poverty and overcrowded populations. The majority of cases (117,147) are from South-East Asia and 7,368 cases are reported from Eastern Mediterranean (WHO 2013). Due to the long latency period, the exact incidence of the disease is not clear.
Subclinical infection is prevalent in endemic regions and there is a possibility of spontaneous cure especially in children with paucibacillary disease. New detected cases of leprosy are registered and reported annually. The annual case detection rate has decreased from 600,000 to 800,000 during pre- MDT to 219,075 (4.06 cases/100,000 population) in 2011. The number of cases reported from Eastern Mediterranean region in this year (January to December, 2011) is 4,346 (0.71/100,000).
In 1991 WHO introduced the goal of elimination (but not eradication) of leprosy in the world. WHO defined this goal as a decrease in leprosy prevalence to less than one case per 10,000 population. This target was globally met in 2000, but due to the latest WHO data, in eight countries, Marshall Islands , Micronesia , Kiribati , Kumori, South Sudan , Burundi , Brazil , and Liberia, the prevalence of leprosy is still more than 1/10,000. Among these countries, Marshall Islands have the highest prevalence of leprosy with the prevalence of 25/10,000 population. In the Eastern Mediterranean region, the highest numbers are reported from South Sudan and Sudan (WHO 2013).
In the years1992 and 1997, Iran reached the goal of leprosy elimination across the whole country and its associated townships, respectively. In 2011, prevalence of leprosy was limited to 78 cases (0.017/10,000) and the new registered cases were 36 (0.04/100,000). Most of the patients were male aged 50–70 years with multibacillary type of leprosy (WHO 2013). Provinces where the most cases of leprosy occurred were the following: Qazvin, Hormozgan, Gilan, Ardebil, West Azerbaijan, Golestan, Sistan and Balouchestan, and Khorasan Razavi (Dowlati et al. 2012).
The leprosy latency period is long and the mean duration of incubation period for the paucibacillary leprosy and the multibacillary leprosy are 4 and 8 years, respectively. In most parts of the world, leprosy is more prevalent in male than female patients and the paucibacillary type is more common. Although leprosy can occur at any age, most patients in endemic areas are younger than 35 years, and the mean age of paucibacillary patients is lower than multibacillary, due to the shorter incubation period.
Etiology
In 1873, a Norwegian scientist, Armauer Hansen, identified Mycobacterium leprae as the definitive cause of leprosy. This weakly acid-fast bacillus has the following unique characteristics:
-
1.
Human is its only known reservoir. However, in some recent studies the possibility that armadillo might be the reservoir of M. leprae and transmit it to humans is proposed (Truman et al. 2011).
-
2.
This bacillus is considered an obligate intracellular microorganism (mainly within macrophages and Schwann cells) with which the body confronts through cell-mediated immunity (CMI).
-
3.
It has a relatively prolonged period of cell division, approximately 12–14 days that in turn results in a lengthy latency period.
-
4.
An ideal ambient temperature for its growth is 30 °C that allows the bacteria to proliferate in cutaneous and peripheral nerves—zones with relatively lower temperatures compared to other tissues.
-
5.
Despite various efforts that have taken place to discover a synthetic culture medium, no such environment has been found thus far. Furthermore, it is not possible to culture M. leprae in vitro. Instead, armadillo or mouse footpad is used for proliferation, which can introduce difficulties in laboratory diagnosis, study of susceptibility and resistance to antibiotics, and discovery of new drugs.
-
6.
Mutation rate of this bacillus, in contrast to Mycobacterium tuberculosis bacillus, is relatively low and genetic sequences of bacilli that have been isolated from patients all over the world (including Iran) are quite similar (Monot et al. 2009). Recently some cases of diffuse lepromatous leprosy (LL) have been reported which is caused by a related but genetically different mycobacterium. This new mycobacterium is called M. lepromatosis (Han et al. 2008).
-
7.
The cell wall of M. leprae consists of several antigenic molecules which are used as substrates for serological tests. The most important antigens include Phenolic Glycolipid 1 (PGL -1) and Lipoarabinomannan (LAM ).
Pathogenesis
The main reservoir of the M. leprae is the upper respiratory tract of the untreated patient with multibacillary leprosy. The disease is transmitted through the nasal secretion of patients to those with a long close contact with them (Job et al. 2008).
Normal skin is resistant to the bacillus penetration but there are rare cases of leprosy caused by inoculation (vaccination, penetrating trauma, tattooing, surgery) (Ghorpade 2009). There is no case of congenital leprosy since M. leprae cannot be transmitted through the placenta.
There are rare cases of leprosy reported in the USA that have no history of close contact with leprosy patients or of travelling to endemic areas. However, these individuals have had exposure to armadillos, despite the fact that the role of armadillo in the transmission of the disease is not yet defined (Truman et al. 2011).
Nearly 90 % of people are genetically resistant to leprosy and their cell-mediated immune system will kill the bacillus after infection. Susceptible individuals will contract the disease after a long household contact with patients having multibacillary leprosy. If the cell-mediated immune function fails to eradicate the microorganism, the bacilliproliferate slowly in the upper respiratory tract and after a relatively lengthy incubation period, the bacilli are disseminated throughout the body and initially inhabit the skin and peripheral nerves, due to their lower temperature.
Genetics
The susceptibility of developing leprosy is under the control of genetic factors. The coincidence of leprosy among monozygotic twins and dizygotic twins are 60–80 % and 15–25 %, respectively, emphasizing the role of genetic factors (Mohammed and Ramanujam 1966). However, a single gene effect has yet to be defined. Different genes have been identified from different parts of the world, suggesting that multiple genes might be involved in susceptibility to leprosy. The type of the disease depends on the CMI response that is controlled by the major histocompatibility complex (MHC) genes. Multiple studies revealed that the HLA -DR2 and HLA -DR3 are more prevalent in tuberculoid leprosy, whereas the HLA -DQ1 prevalence is higher in lepromatous and borderline leprosy (BB) (Worobec 2009).
Immunology
Granuloma formation around the bacillus, which occurs by having a good CMI response with production of Th1 cytokines (IL-2 , IL-12 , IFN-γ ) and the CD4/CD8 ratio of two, restricts bacillus proliferation. The resulting disease is called tuberculoid leprosy (TT ). During TT , there are few and asymmetric skin and nervous lesions and the bacillus is rarely found in these lesions. The lepromin skin test (see below) is positive in these patients but the serologic test is positive in only 40–50 % of these individuals.
If the CMI response is not adequate with a CD8/CD4 ratio of two, the Th2 cytokines (IL-4 , IL-10 ) will be secreted. These processes do not form granulomas and prevent the bacillus proliferation. The resulting disease is called lepromatous leprosy (LL ). In this type of leprosy, multiple symmetrical cutaneous and nervous lesions do exist, containing numerous Hansen (M. leprae) bacilli. Although the clinical signs are usually restricted to the skin and nerves, the bacillus disseminates to other organs. The lepromin skin test is negative for these patients but the serologic test is positive in more than 90 % of them. Lepromatous patients have polyclonal hypergammaglobulinemia and high antibody titers to M. leprae unique antigens and may have false-positive syphilis serology, rheumatoid factor, and antinuclear antibodies.
In the case of an intermediate CMI response, the patient will have the borderline leprosy (BB ) with intermediate clinical symptoms and a negative lepromin test. In this group, there are borderline tuberculoid (BT ) patients, who are more similar to the tuberculoid leprosy with a positive lepromin test, and borderline lepromatous (BL ) patients who are more similar to LL with a negative lepromin test.
LL and TT patients are immunologically stable and will not convert to other disease forms. Borderline leprosy, on the other hand, may convert to other forms if the patient’s CMI responses change (e.g., by treatment, pregnancy, immunosuppression, drug consumption, vaccination, HIV infection, etc.). This response can be associated with severe inflammation of skin and peripheral nerves which contain M. leprae antigens. This reaction is called a type-1 reaction and is a delayed-type hypersensitivity reaction.
In LL and BL patients numerous bacilli and high levels of serum antibody are found. Immune complexes precipitate in tissues that, in turn, activate the complement system, causing leukocytoclastic vasculitis in different body organs. This occurrence, which is called a type-2 leprosy reaction, is considered a type-III hypersensitivity reaction. The course of these immunologic reactions is not correlated to the course of the disease and can occur before, after, or during treatment.
The immune insufficiency in patients with leprosy is completely specific to the M. leprae antigens and all their other immune responses, even to other mycobacterium, are normal. Coinfection with HIV does not change the incidence or severity of leprosy and the treatment response is not be decreased as well; however, the risk of type-1 reaction might be increased after the antiretroviral treatment, which is called “immune reconstitution syndrome” (Lockwood and Lambert 2011).
Classification
Most commonly, patients with leprosy are classified by the use of two classifications: WHO classification, which is more simple and practical, and the Ridley-Jopling that is more specialized but less practical (Prasad 2005).
WHO Classification
In this classification, patients are classified in two groups based on their positive or negative skin smear test.
-
1.
Paucibacillary patients with negative skin smear
-
2.
Multibacillary patients with positive skin smear
Due to some reasons such as difficulty in preparation and interpretation of the skin smear and a false-negative result in some patients, WHO, recently, classified the patients based on the number of skin lesions.
Patients with five lesions or less are classified as paucibacillary group and those with more than five skin lesions are in the multibacillary leprosy group. Certainly, this type of classification has some drawbacks; for instance, some multibacillary patients will be classified in the paucibacillary group and will not receive the adequate treatment. In case of uncertainty regarding the exact classification, patients should be treated as a multibacillary leprosy case.
Ridely–Jopling Classification
During the 1960’s Ridely and Jopling introduced their classification based on clinical signs and histopathological findings. It is now clear that the basis of this classification is CMI reaction against M. leprae.
-
1.
Indeterminate (I)
-
2.
Tuberculoid (TT )
-
3.
Borderline tuberculoid (BT )
-
4.
Mid-borderline (BB )
-
5.
Borderline lepromatous (BL )
-
6.
Lepromatous (LL )
The first three groups are almost similar to the paucibacillary group and the last three are roughly consistent with the multibacillary group of WHO. The first three groups have negative cutaneous smear and a limited number of skin and nerve lesions both with an asymmetrical distribution.
By moving toward the multibacillary pole, the number of lesions increases gradually and their distribution becomes more symmetrical. Furthermore, they are morphologically more diverse and the number of Hansen bacilli increases as well. However, the paucibacillary group has more pronounced neurological symptoms than the multibacillary group, while the latter shows these symptoms in later stages of their disease.
Clinical Features
There is a diverse range of clinical features in patients with leprosy. About 90 % of population are resistant to leprosy and their CMI system kill the bacilli after entering the body without developing any clinical symptoms. Susceptible individuals have a range of clinical findings that depends on their CMI response (Moschella 2004).
Indeterminate leprosy (I)
The most common outcome after exposure to M. leprae is spontaneous healing. If the disease occurs, the initial presentation is indeterminate leprosy. In the indeterminate type, usually there is a single hypopigmented macule or patch with an ill-defined border. Occasionally, there is a faded erythema that accompanies the hypopigmented macule. The common sites of involvement are face, upper arms, buttocks, and upper thighs. The scalp, axilla, and inguinal region are usually spared due to their higher temperature. Patient may complain from tingling, despite no sensory dysfunction during physical examination. This clinical manifestation is called indeterminate because the course of disease cannot be predicted. Although most of the patients recover spontaneously, some of them progress to the other forms of the disease.
Tuberculoid Leprosy (TT )
In TT leprosy, the skin and peripheral nerves are the only sites of involvement. There are one or a few skin lesions (less than five lesions). Lesions are well demarcated with elevated borders. The central part of the lesion may be hypopigmented or erythematous in darkly pigmented patients and in lightly pigmented skin, respectively. The lesion may be a macule/patch or an annular plaque (Fig. 1).

Tuberculoid leprosy
TT lesions are anesthetic. Loss of temperature sensation occurs early followed by loss of sensation of light touch, pain, and deep touch. Due to the extensive nervous supply on the face, the loss of sensation of facial lesions may not be evident during the examination. Usually a peripheral nerve near the skin lesion is involved and becomes large and palpable and occasionally tender. Reduced hair growth and anhidrosis might be observed in a skin lesion due to autonomic nerve involvement. In addition, there may be atrophy of the muscle groups served by the involved nerve. Wasting of the thenar and hypothenar eminences, contracture of the fingers, paralysis of the facial muscles, and foot drop may also occur. Facial nerve damage dramatically increases the risk for ocular involvement and vision loss.
The TT course of the disease is prolonged. It may heal spontaneously in a few years (especially in children) or faster with treatment. Even without treatment, this manifestation never progresses to other forms of leprosy.
Borderline Tuberculoid Leprosy
BT lesions are well defined with a hypopigmented center; in lightly pigmented individuals, it may be erythematous. BT is defined by more lesions than TT leprosy and satellite lesions usually exist. The skin lesions are usually asymmetric and the borders are less infiltrative, however, sensation loss of the lesion is still an important feature.BT lesions have no scale or are slightly scaly. Peripheral nerve involvement is more prominent than TT leprosy and usually the large nerve trunks are involved asymmetrically. These nerves are large and tender or exhibit sensory, motor, and autonomic nerve fiber dysfunction (in the late stage) during neurologic examination.
Borderline Leprosy
BB leprosy usually has a short duration and will upgrade or downgrade to other forms. In this group, there are generalized and numerous lesions but not as many as in lepromatous leprosy. Lesion distribution is more symmetrical than BT lesions. The lesions may be macular, papular, or plaque type. In the typical form of the disease, lesions have a well-demarcated inner margin and an ill-defined outer margin, although these lesions are rare. Peripheral nerve involvement is variable and their manifestations depend on the involved nerve.
Borderline Lepromatous Leprosy
Skin lesions are almost symmetrical, multiple, and disseminated with no well-defined margin in BL leprosy. Initially, fade macules are present and gradually symmetric disseminated papules, plaques, and nodules will develop. In this type of leprosy, involvement of large nerve trunks without clinical symptoms is observed that is usually symmetrical. Although loss of sensation in a stocking and glove pattern may occur, sensation and sweating on individual skin lesions is normal.
The possibility of leprosy reactions is high in this type of leprosy. The signs and symptoms of oral and nasal involvement such as epistaxis, nasal septum perforation and saddle nose, and eyebrow loss usually are not observed in the early stages of this type of leprosy.
Lepromatous Leprosy
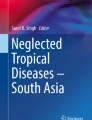
In this leprosy type, there is a huge proliferation of the bacteria and the bacilli are disseminated through skin, nerves, and other sites of the body. The skin lesions are diffuse and symmetric macules (with ill-defined borders in contrast to well-defined tuberculoid macules), papules, nodules (lepromas), and plaques are seen. The scalp and intertriginous areas are not involved. Diffuse infiltration of the bacillus in facial skin causes the typical feature of the leonine face (Fig. 2). Neuropathy might be observed as anesthesia in a bilateral symmetrical stocking and glove distribution during the late stage of the disease. But similar to BL , sensation and sweating on individual skin lesions are normal. Symptoms in the advanced stage include, saddle nose deformity, and nasal bridge damage due to bacillus infiltration, madarosis (decreased eyebrow hair), epistaxis, and ichthyosiform skin. Infiltration of the earlobe causes enlargement and swelling. Fusiform swelling of digits might be another sign of LL .

Leonine facies in lepromatous leprosy
Histoid Leprosy
This uncommon form of multibacillary leprosy may occur de novo or more commonly in LL patients who become resistant to Dapsone . There are numerous yellow-red dermal or subcutaneous shiny papules and nodules appearing on a background of normal skin.
Nerve Involvement
Nerve involvement is characteristic of leprosy and due to neurotropism of M. leprae. Different types of peripheral nerves involvement might be observed in leprosy:
-
1.
Peripheral nerves enlargement. This symptom is diagnosed through palpation of the peripheral nerves, which are asymmetric in the tuberculoid spectrum and symmetric in lepromatous pole of disease. The most important nerves that are involved in leprosy are the greater auricular, ulnar, and cutaneous branch of the radial nerve, lateral popliteal, sural, common peroneal, and posterior tibial nerves. The nerve trunks that are more superficial and are close to the skin such as the ulnar and greater auricular are more obvious in physical examination.
-
2.
Loss of skin sensation. Temperature sensation is the first sense that is lost, followed by loss of sensation of light touch, pain, and deep touch. This impaired sensation is in the skin lesion in the paucibacillary form. However, in the multibacillary type the anesthesia is in acral parts in a pattern of stocking and glove during the advanced stage of the disease with no loss of sensation in the skin lesions.
-
3.
Motor nerve paralysis. This paralysis may have inflammatory symptoms (tenderness and swelling) or without symptoms (silent neuropathy). Gradually atrophy and wasting of small muscles of hands and feet and occasionally face served by involved nerves develops. Contracture and deformity of the extremities might be seen gradually. Ulnar and median nerve involvement can cause claw hand and thumb deformity, respectively. Wrist drop is the result of radial nerve involvement. Foot drop deformity and claw toe are due to common peroneal nerve and posterior tibial nerve involvement, respectively. Facial nerve involvement causes lagophthalmus (eye will not close during the sleep) and finally may lead to blindness due to trauma and secondary infection.
-
4.
Anhidrosis. Loss of sweating is the result of autonomic nerve dysfunction. In the paucibacillary type, this symptom is limited to skin lesions but in the multibacillary form, it involves the acral areas and in late stage, the trunk becomes anhidrotic.
-
5.
Pure neural leprosy. Although leprosy frequently involves both skin and peripheral nerves, in some patients the peripheral nerves are involved in the absence of cutaneous lesions. This type of leprosy is called pure neural leprosy. Some patients have undergone unnecessary orthopedic surgery and neurosurgical procedures due to the misdiagnosis. This type of leprosy is more commonly seen in paucibacillary patients and may represent up to 5 % of new cases of leprosy in some countries such as India and Nepal . Histological changes compatible with leprosy have been observed in normal appearing skin of some of these patients. (Menicucci et al. 2005)
Leprosy Reactions
In some leprosy patients, acute signs and symptoms of inflammation may occur. Physical examination may reveal erythema, tenderness, and swelling in skin lesions or nerves. New skin lesions with inflammation and erythema may occur abruptly. This phenomenon is called a leprosy reaction. Leprosy reactions are destructive inflammatory reactions due to immune system hyperactivity. Its occurrence is reported in 50 % of patients after starting therapy. In some instances, it is the first sign of leprosy and the cause of patient referral. In addition, this reaction can occur long after therapy cessation.
Leprosy reaction is an emergency with a high degree of importance that should be diagnosed and treated promptly. Otherwise, permanent sequelae and disability occur due to the fibrosis of the nerve fibers. Occasionally, the reaction may be subacute with the presence of progressive destructive non-inflammatory neuropathy. In case of reaction occurrence during therapy, both patient and physician should be aware that these new symptoms are not the result of incompetency or side effects and that treatment should be continued.
There are two types of leprosy reactions. A type-1 reaction is due to a shift in delayed-type hypersensitivity (type IV reaction), which occurs in borderline leprosy (BT , BB , or BL ). In these patients, the immune system is unstable and when it attenuates (for example during pregnancy, lactation, vaccination, immune suppressive drug consumption, and other infections), BT can shift to BB and even LL (reversal reaction or down grading). On the other hand, BL patients might shift to BT after reinforcement of the immune system especially after treatment (upgrading). In this reaction, the previous skin lesion becomes inflamed and erythematous, even new lesions might occur. In addition, the involved nerves might be swollen and inflamed. A type-1 reaction has no systemic symptoms and the manifestations are restricted to skin and peripheral nerves.
A type-2 reaction is a type-III hypersensitivity reaction and the result of antigen-antibody complex deposition in various tissues. It occurs in half of the LL and BL patients and is a multisystem disease due to leukocytoclastic vasculitis of various organs. The immune complex deposition in different organs causes inflammation: neuritis, arthritis, hepatitis, conjunctivitis, keratitis, uveitis, orchitis, and lymphadenopathy may develop. The systemic symptoms such as fever, chills, arthralgia, etc., are present.
The skin lesion is called erythema nodosum leprosum (ENL ). Lesions are subcutaneous erythematous and painful nodules with shorter duration than the usual erythema nodosum. In addition to lower extremities, nodules might occur in upper extremities, face, and trunk (Fig. 3). This reaction may be mild to severe and may last from a few days to even years.

Erythema nodosum leprosum
Systemic Involvement
Except for skin and peripheral nerves, other systemic manifestations are rare in leprosy (Klioze and Ramos-Karo 2000). However, in multibacillary leprosy, M. leprae might exist in most organs usually without any symptoms. The exceptions are the involvement of eyes (which is frequent in all types of leprosy due to the infiltration of bacilli, neuropathy, or reaction), upper respiratory tract, and testis (in multibacillary type) and the type-2 reaction which induces systemic leukocytoclastic vasculitis in several organs.
Diagnosis
Diagnosis of leprosy is based on clinical suspicion and accurate physical examination. The co-occurrence of peripheral neuropathy and skin lesions should lead to suspicion of leprosy, especially in patients with positive family history or background of living in endemic areas. Laboratory tests are not very sensitive and are not necessary if there are not adequate facilities.
Presence of two of the following clinical signs may confirm the diagnosis: (Prasad 2005)
-
1.
Skin lesion
-
2.
Sensory dysfunction in vicinity of skin lesions or in extremities
-
3.
Enlargement of peripheral nerves
If there is any suspicion of leprosy, skin should be examined precisely and completely under proper lighting conditions. Any skin lesion might be due to leprosy because of the diversity of leprosy manifestations. But congenital, pruritic, hyperpigmented, or depigmented skin lesions and severe scaling are less suggestive of leprosy.
Leprosy is a chronic, long lasting disease that is progressive; repetitive courses of relapse and spontaneous remission are uncommon and are only observed in leprosy reactions.
After thorough skin examination, peripheral nerves should be palpated for thickness and tenderness, and then their function should be examined. Senses of temperature, superficial touch, pain, and deep touch should be examined by cold and hot water tubes, cotton ball or feather, needle tip, and pinching, respectively. This examination should be performed on skin lesion surfaces in case of paucibacillary leprosy and on skin of hands and feet in patients with multibacillary leprosy. The motor nerves should be evaluated by examination of the force of hand and foot muscles and presence of muscle atrophy or contracture. Hypohidrosis and hypotrichosis might be the signs of autonomic nerve dysfunction. In all patients, ophthalmologic examination is mandatory.
Although the diagnosis of leprosy is clinical and based on physical examination and WHO excludes the laboratory studies from the diagnostic criteria of leprosy, the following tests could be helpful.
Skin Smear
Skin slit smear samples can be obtained from the periphery of active skin lesions or cold body areas such as ear lobe, forehead, chin, and extensor surface of forearm, dorsal surface of fingers, buttocks, and trunk. Sometimes smears can be prepared from the nasal mucosa discharges. Nevertheless, the skin smear is more valuable.
Fite stain, which is the modified form of Ziehl–Neelson, is used for staining after the slide is dried, where the bacilli are seen as red rods against a blue background. Smear is positive in 100 % of multibacillary patients but is negative in all TT patients and most of BT patients. Bacteriological index (BI) indicates the density of bacilli in the smear on a 0–6 scale.
Although the bacilli are killed after a short duration after the onset of therapy, they may remain in skin tissue for many years and smears could remain positive. Therefore, the smear test is not a suitable way to monitor the disease treatment response. Live bacilli are solid, whereas killed bacilli are granular and crushed. The proportion of live solid bacilli in a smear is called morphological index (MI) which is a useful index for monitoring patients after treatment.
WHO has discontinued recommendation of taking skin smears in endemic areas for diagnosis or classification or in order to monitor progress with treatment (WHO 2003), because:
-
Leprosy can be easily diagnosed and classified on the basis of clinical findings.
-
MDT treatment regimens are standardized and usually do not require mid-course changes based on results of smear examinations.
-
Cure of leprosy is based on completion of a full course of standard MDT regimen and skin smears from most leprosy patients will yield negative results.
-
Unnecessary skin-piercing procedures are unethical, painful and carry the risk of serious infection (particularly HIV and hepatitis).
-
Use of skin smears should be limited to referral centres, particularly for special investigations (suspicion of resistance, complex relapse cases) and research purposes.
Histopathology
Skin biopsy samples should contain the full thickness of the skin. Nerve biopsy is rarely used and might be performed from only sensory nerves such as great auricular, sural, and superficial peroneal nerves. Different types of leprosy have distinctive histologic patterns:
-
At the lepromatous pole, histological examination reveals diffuse dermal infiltration composed of lymphocytes and plasma cells. In addition, several bacilli are observed in the dermis, forming aggregates known as globi. The Grenz zone, a band of normal appearing dermis, separates the epidermis from the dermal infiltration. If treatment is successful, granular and fragmented bacilli will be seen.
-
At the tuberculoid pole, granulomatous infiltration in the dermis is observed that might have a linear pattern that follows the nerve course. Epithelioid cells and Langhans giant cells are surrounded by lymphocytes but there is no bacteria present in the tissue. The cutaneous nerves are edematous, a symptom that differs from other granulomatous reactions such as sarcoidosis.
The borderline spectrum of leprosy contains the histological features of both mentioned forms.
Serology
Serologic assays to detect antibodies against M. leprae specific antigens (anti-PGL ) are only sensitive and specific in multibacillary disease because it is positive in nearly all of the patients. Serologic tests are only positive in half of the paucibacillary patients. Due to the presence of positive serology in 5–10 % of healthy people in endemic areas for leprosy (likely due to subclinical infection), this method is of no value in the diagnosis of leprosy and should only be utilized in epidemiologic surveys or to identify persons at risk of developing leprosy in endemic areas (Oskam et al. 2003).
Lepromin Skin Test
Lepromin test is an intradermal test in which a 0.1 ml suspension of heat-killed M. leprae (from lepromatous nodule or infected armadillo liver) is injected intradermally. Forty-eight hours later, the injection site is examined as in the tuberculin test. This reaction, called Fernandez reaction, has cross-reaction with other mycobacteria species. A reaction with induration of more than 7 mm developing 3–4 weeks following injection is more specific than the former reaction and is called Mitsuda reaction. This test is an indication of cell-mediated immune response against M. leprae antigen. It does not require the existence of bacilli in the body or the history of contact with it, so it is positive in healthy people that are resistant to leprosy and also in paucibacillary patients. However, it is negative in multibacillary patients. Thus this test cannot be used as a diagnostic method, but may be useful for the classification of leprosy.
Polymerase Chain Reaction
Polymerase chain reaction (PCR) can detect even very small numbers of organism in infected tissues and is universally positive in multibacillary disease, in which the diagnosis is not difficult. But it is negative in as many as half of the paucibacillary patients and cannot improve the diagnosis in these patients.
Differential Diagnosis
Hypopigmented lesions in leprosy may mimic pityriasis alba, pityriasis versicolor, the early stage of vitiligo, post inflammatory hypopigmentation, and achromic or anemic nevus. Erythematous lesions with well-demarcated borders in paucibacillary leprosy may be misdiagnosed as dermatophytosis, granuloma annulare, cutaneous TB, and allergic contact dermatitis. The differential diagnosis of diffuse erythematous lesions in multibacillary leprosy includes xanthomas, guttate psoriasis, pityriasis rosea, and sarcoidosis. Although leonine facies is a characteristic for lepromatous leprosy, it is not pathognomonic and it might be observed in other infiltrative diseases such as leishmaniasis, lymphoma, and pseudolymphoma.
Treatment
Despite thousands of years of history and recognition of causative agent of leprosy for many years, Dapsone as the first effective treatment was introduced in 1941. Dapsone is a bacteriostatic agent and it should be consumed throughout the patient’s lifetime. Gradually, some of leprosy patients became resistant to Dapsone (secondary resistance). Transmission of Dapsone-resistant M. leprae to new patients caused primary resistance to Dapsone. The first bactericidal drug that had been discovered against M. leprae was Rifampin , which is still the drug of choice, and is the base of all the leprosy treatment regimens. Finally, the definite treatment for leprosy was introduced by WHO in 1982 as Multidrug Therapy (MDT ): (WHO 1982).
-
Paucibacillary leprosy: Rifampin 600 mg once a month + Dapsone 100 mg daily for 6 months.
-
Multibacillary leprosy: Rifampin 600 mg once a month + Dapsone 100 mg daily + Clofazimine 300 mg once a month and 50 mg daily for 12 months.
Prior to 1998, the duration of the therapy was 24 months and then it was decreased to 12 months (Firooz 2006).
The most important bactericidal drug in leprosy and the base of all of regimens is Rifampin . Due to the bacillus proliferation period, increasing patient compliance, and decreasing the risk of resistance, Rifampin is used in a single monthly dose and under supervision.
If Rifampin is contraindicated or cannot be used for any other reasons, two drugs, mostly Minocycline and Ofloxacin can be substituted. Although there have not been any clinical trials comparing a placebo control to MDT , this treatment is very effective and the risk of recurrence is less than one per 1,000 cases per year. (Lockwood 2007; WHO 2003) The cases of recurrence are not due to drug resistance and patients should be retreated with the same MDT . Treatment in pregnancy and lactation is MDT and, in children, the dose should be adjusted concerning their age or weight (WHO 2003).
Side effects of MDT are rare. The most common side effects of Rifampin are gastrointestinal side effects and urinary discoloration. Hepatic toxicity is rare due to monthly consumption. Hemolytic anemia is not common during Dapsone consumption and it is not necessary to evaluate G6PD in all patients before starting treatment. The rare but important side effect of Dapsone is a hypersensitivity reaction with fever, generalized rash, pruritus, and lymphadenopathy. The most common side effect of Clofazimine is skin hyperpigmentation, which usually occurs a few months after starting the drug and will resolve spontaneously after drug discontinuation.
The new treatment regimen is ROM which consists of Rifampin 600 mg + Minocycline 100 mg + Ofloxacin 400 mg once a month for 6 months and 24 months in paucibacillary leprosy and multibacillary leprosy, respectively. Although this treatment appears to be as effective as MDT in randomized clinical trials, it is not useful in most of the endemic countries due to its high cost, and it is not recommended by WHO (Setia et al. 2011).
Treatment of leprosy reactions is an emergency and more important than the leprosy itself, because they will damage the nerves very quickly. In the case of a reaction, which may happen during MDT therapy, MDT should not be discontinued; rather it should be continued without any change.
For the mild reactions without nerve involvement, bed rest and NSAIDs are enough.
Nerve involvement requires prompt prednisolone therapy with the dose of 40–60 mg daily in an adult patient. It will be gradually tapered and then discontinued when the symptoms are controlled.
In type-2 reaction (ENL ), thalidomide 100–200 mg daily with or without prednisolone is useful. Occasionally, differentiation between relapse and reaction is difficult. Usually reactions occur shortly after the therapy cessation while relapse happens after some years. Reaction is always acute but relapse has an insidious course. Reaction responds to oral corticosteroids rapidly, while relapse does not respond to corticosteroid therapy. If there is any doubt in the differentiation between reaction and relapse, it is recommended to start corticosteroid therapy. Therefore any possible nerve damage can be prevented.
Prevention
Long before discovering the cause of leprosy and its treatment, the only way for its prevention was to isolate patients and to reject them from society due to their deformed appearances. As most of the population are resistant to leprosy naturally, the paucibacillary leprosy is not contiguous, the possibility of transmission of the multibacillary form will disappear shortly after the treatment is started, and the only way for leprosy transmission is prolonged close contact, therefore, patient isolation is not required.
Those with household contact are more susceptible to catch the disease, and they should undergo precise examination: once for contact of paucibacillary leprosy patients and once a year for 5 years for contact of multibacillary leprosy patients. Contacts should be educated for leprosy symptoms and necessity of seeking medical care promptly in case of any suspicious lesion.
Extensive studies evaluating possible anti-leprosy vaccines were carried out before the advent of (Gupte et al 2003) different vaccines, such as BCG alone or with M. leprae or other mycobacterium antigens have been studied, but their efficacy was variable. There is some recommendation that leprosy patients’ household contacts should be vaccinated with a booster dose of BCG for prevention (Merle et al. 2010).
Prevention of leprosy-induced disabilities is very important. Patients should moisturize skin daily. If there is any scratch or ulcer, lesions should be irrigated and antiseptics applied to prevent secondary infection and if there are any signs of infection, treatment with appropriate antibiotics is prescribed.
Also wearing fitted shoes, physiotherapy, and exercise for prevention of muscular atrophy and contracture, frequent use of artificial eye drops, and eye dressing by ointment during night for the prevention of xerosis and abrasion of cornea have significant importance.
Conclusion
The prevalence of leprosy has decreased after the introduction of MDT in 1981 and the goal of elimination (prevalence less than 1/10,000 population) has been achieved in most parts of the world including Middle East. Our most important task at present is early detection of new cases in order to both reduce the rate and severity of disabilities and also reduce the risk of transmission to achieve eradication in near future.
References
Browne SG (1985) The history of leprosy. In: Hastings RC (ed) Leprosy. Churchill Livingstone, Edinburgh, pp 1–14
Daumerie D (2003) Elimination of leprosy as a public health problem—current status and challenges ahead. Scientific Working Group Report on leprosy. WHO, Geneva. pp 57–72
Dowlati Y, Shizarpour M, Tabatabaei H, Firooz A, Nassiri-Kashani M, Mapar M (2012) Mycobacterial diseases. In: Mortazavi H, Firooz A, Shahidi M (eds) Text book of dermatology for medical students and general practitioners, 1st edn. Sepidbarg, Tehran, pp 118–137
Firooz A (2006) Multidrug therapy regimen for leprosy. J Am Acad Dermatol 55:1115
Ghorpade A (2009) Inoculable leprosy. Int J Dermatol 48:1267–1268
Gupte MD, Manickam P, Kishore Kumar B (2003) Vaccines for leprosy and other mycobacterial diseases—What do we know today? Scientific Working Group Report on leprosy. WHO, Geneva, pp 86–89
Han XY, Seo YH, Sizer KC et al (2008) A new Mycobacterium species causing diffuse lepromatous leprosy. Am J Clin Pathol 130:856–864
James WD, Berger TG, Elston DM (2011) Andrews’ diseases of the skin, 11th edn. Saunders Elsevier, China, pp 334–344
Job CK, Jayakumar J, Kearney M, Gillis TP (2008) Transmission of leprosy: a study of skin and nasal secretions of household contacts of leprosypatients using PCR. Am J Trop Med Hyg 78:518–521
Klioze AM, Ramos-Karo FA (2000) Visceral leprosy. Int J Dermatol 39:641–658
Lockwood D (2007) Leprosy. BMJ Clin Evid 915:1–11
Lockwood DNJ, Lambert SM (2011) Human immunodeficiency virus and leprosy: an update. Dermatol Clin 29:125–128
Menicucci LA, Miranda A, Antunes SL et al (2005) Microscopic leprosy skin lesions in primary neuritic leprosy. J Am Acad Dermatol 52:648–652
Merle CS, Cunha SS, Rodrigues LC (2010) BCG vaccination and leprosy protection: review of current evidence and status of BCG in leprosycontrol. Expert Rev Vaccines 9:209–222
Mohammed AP, Ramanujam K (1966) Leprosy in twins. Int J Lepr 34:405–406
Monot M, Honoré N, Garnier T, Zidane N, Sherafi D, Paniz-Mondolfi A et al (2009) Comparative genomic and phylogeographic analysis of Mycobacterium leprae. Nat Genet 41:1282–1289
Moschella SL (2004) An update on the diagnosis and treatment of leprosy. J Am Acad Dermatol 51:417–426
Oskam L, Slim E, Bührer-Sékula S (2003) Serology: recent developments, strengths, limitations and prospects: a state of the art overview. Lepr Rev 74:196–205
Prasad PVS (2005) All about leprosy, 1st edn. Jaypee Brothers Medical Publishers, New Delhi, pp 45–60
Setia MS, Shinde SS, Jerajani H, Boivin JF (2011) Is there a role for rifampicin, ofloxacin and minocycline (ROM) therapy in the treatment of leprosy? Systematic review and meta-analysis. Trop Med Int Health 16:1541–1551
Truman RW, Singh P, Sharma R, Busso P, Rougemont J, Paniz-Mondolfi A et al (2011) Probable zoonotic leprosy in the southern United States. N Engl J Med 364:1626–1633
World Health Organization (1982) Chemotherapy of leprosy for control programmes: technical report series 675. WHO, Geneva
World Health Organization (2003) The final push strategy to eliminate leprosy as a public health problem: Questions and answers. WHO, Geneva, pp 25–27
World Health Organization (2013) Leprosy. Prevalence rates (per 10 000 population). Available at: http://apps.who.int/neglected_diseases/ntddata/leprosy/leprosy.html. Last accessed 10 June 2013
Worobec SM (2009) Treatment of leprosy/Hansen’s disease in the early 21st century. Dermatol Ther 22:518–537
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Wien
About this chapter
Cite this chapter
Firooz, A., Dowlati, Y., Ayatollahi, A. (2014). Leprosy. In: McDowell, M., Rafati, S. (eds) Neglected Tropical Diseases - Middle East and North Africa. Neglected Tropical Diseases. Springer, Vienna. https://doi.org/10.1007/978-3-7091-1613-5_7
Download citation
DOI: https://doi.org/10.1007/978-3-7091-1613-5_7
Published:
Publisher Name: Springer, Vienna
Print ISBN: 978-3-7091-1612-8
Online ISBN: 978-3-7091-1613-5
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)