
Abstract
Significant or not, polymerization shrinkage stress deserves a special chapter when resin composites are discussed. Subject of numerous publications based on in vitro tests and of intensive debates, the real significance of this phenomenon has been challenged by recently published clinical findings. The aim of this chapter is to present the main outcomes of research papers in the field of polymerization shrinkage stress followed by critical analysis of this complex phenomenon, consequences, clinical significance and education.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

1 Introduction
Resin composite has been widely used and is the first choice as restorative material in dentistry due to the possibility to perform minimally invasive, or noninvasive, treatments associated with favorable properties and reliable clinical performance.
Despite many advantages, some drawbacks have been described in the scientific literature, and “shrinkage stress” has been widely cited as one of the most problematic ones [1, 2]. Basically, the shrinkage-derived stress is a resultant phenomenon from the polymerization process, which involves mass densification resultant from the molecular approximation of monomers when carbon double bonds are converted into single ones. Due to the clinical situations and restriction for material’s flow by vitrification—such as the boundary conditions imposed by the surrounding cavity walls that were previously treated with an adhesive layer—the deformation of the growing polymer is restricted, and consequently, stress arises in the whole system [3, 4]. Therefore, a list of clinical consequences has been cited through the years in publications derived from numerous in vitro and few in vivo data. A recent study called into question how deleterious this phenomenon might be for long-term success of restorative procedures in a realistic clinical setting [5]. This doubt comes from the fact that it has not been possible to confirm a direct relationship between in vivo and in vitro data. Furthermore, recent publications have demonstrated that other factors related to personal and clinical conditions might overcome the importance of the polymerization shrinkage stress [6,7,8,9,10,11]. Nevertheless it is necessary to consider the importance of polymerization shrinkage stress and clarify its real effects on the resin composite restoration during function and, more importantly, to intensify knowledge transfer in education at all levels.
Over the last 10–15 years, extensive research in this field has been summarized in several literature reviews containing valuable data considering origins, ways of evaluation, and management of stress and is a mandatory source for those who seek a deeper insight [1,2,3,4, 12]. Polymerization stress is not a myth nor is its clinical significance even though state-of-the-art resin composites may exert fewer problems and consequences than did previous composite materials. The aim of this chapter is to provide a critical overview and, somehow, raise in readers’ minds the question “what are we looking for when considering stress?”
2 Origins of Stress
The shrinkage stress phenomenon may be associated with two main origins: the polymerization process and clinical situations. Resin composites are typically formulated with ceramic-derived filler particles, treated with a coupling agent, dispersed into a resinous matrix usually formulated with methacrylate monomers. These monomers typically appear in the fluid state and need to be rapidly converted into rigid polymers through a polymerization process during the material’s clinical application [13]. By using an initiator—photoinitiators are regularly used to facilitate materials handling and clinical applications—reactive radicals react with monomer molecules. Active centers are then created and propagate the polymerization process. The propagation reaction involves polymer chain growth by rapid sequential addition of monomer to the active centers via covalent bonds until the maximum degree of conversion of C=C double bond into C–C bond is achieved. During the polymerization process, van der Waals forces are substituted by covalent bonds, and the distances is reduced from 4 to approximately 1.5 Å, and, consequently, volumetric shrinkage occurs [14].
Besides shrinkage, the polymerization process also involves elastic modulus development, meaning that materials’ flowability becomes restricted due to polymer chains’ growth and vitrification and, thus, stress release becomes also reduced [3, 4]. It has also been considered that thermal variations may play an important role in material deformation during the polymerization reaction. It is of fundamental importance to consider that the polymerization process is dynamic and that the effect of speed of reaction, the rate of polymerization, has also been evaluated but with conflicting results [15,16,17,18].
In clinical situations, resin composites usually have to be placed inside cavities and are bonded to the surrounding walls. Therefore, the material deformation is restricted in these constrained conditions, thereby developing stresses. In 1987, Feilzer, de Gee, and Davidson [19] developed the well-known theory of the “configuration factor,” or “C-factor”, an approach considering that the ratio between bonded and unbonded surfaces might predict the relationship between confinement and stress development. Afterward, authors have demonstrated that the C-factor should not be solely considered, since the materials’ used volume (the “V-factor”), or mass, and the condition—the compliance—of the surrounded areas of the remaining tooth need to be considered [20,21,22,23]. Han et al. [23] suggest the C-factor is a valid parameter in comparisons of restorations of identical shapes and volumes.
Some other issues regarding origins of stress must be addressed when considering the multiple situations that clinicians have to deal in the daily practice. It was demonstrated that increasing the local temperature and humidity might increase post-gel shrinkage and cusp deformation with higher shrinkage stresses at the tooth structure and tooth/restoration interface [24]. Also important are those factors that might occur just after the materials’ final placement or as the patients leave the dental office. For example, Bicalho et al. [25] demonstrated that the contact on the tooth/composite restoration margin increases the stresses around the margins of the restoration. Another research has shown that relaxation of the shrinkage-derived stress might occur due to material expansion caused by liquid uptake (water, saliva, etc.) that might compensate the negative effects of stress [26].
3 Consequences
It has been suggested that polymerization-derived stresses might cause deleterious effects on the bonding area (with consequent formation of gaps, lack of adaptation, infiltration, “leakage,” “secondary/recurrent caries”), cusp deflection (with tooth fracture as an extreme possible consequence), postoperative sensitivity, and reduction of clinical lifespan of composite restorations. However, questions have arisen over the true clinical significance of such possible shortcomings. Numerous papers have reported on in vitro evaluations, but very rarely have the data been derived from clinically-based systematic observations.
3.1 Consequences Related to the Bonding Area
It is believed that polymerization shrinkage leads to a competition between the internal composite stresses and the bonded interface, potentially leading to gap formation and consequent “microleakage” and “secondary,” or “recurrent,” caries lesions and/or marginal staining.
With the current data available in the literature, it is not possible to clearly state that the presence of “micro-gaps” would result in the formation of new caries lesions [27,28,29,30,31]. Besides, educators and researchers who deal with dental materials should keep in mind that caries is a behavioral disease and, undoubtedly, a question of patient’s behavior and way of life, and then efforts must be driven to habit modifications. If not, we will continuously observe dental companies and researchers aiming to develop better materials to compensate the lack of proper education at all levels in dentistry. And, to date, no material is able to replace enamel and dentin as nature created these tissues. In addition, the clinical effectiveness of antibacterial adhesives and composites has not been confirmed.
Unlike “secondary caries,” the resultant gap formation is clearly associated with higher marginal staining incidence [32]. Unfortunately, marginal staining is frequently associated with secondary/recurrent caries by many clinicians and subsequent repair or—much worse—premature substitution of the restoration [33]. Therefore, clinicians should be aware of stress management when dealing with composites, and it is of paramount importance that educators include teaching appropriate methods to determine the need for restorations’ substitutions based on systematic criteria, considering not only the restoration per se but also patients’ and clinicians’ behavior and preferences. Another important aspect of marginal staining relies on the proper bonding procedures, as the adhesive layer is, unfortunately, semipermeable to oral fluids and, consequently, to infiltration of pigments during the years of service.
3.2 Cusp Deflection, Tooth Cracking, and Postoperative Sensitivity
Cusp deflection, tooth cracking, and postoperative sensitivity have been cited as the main consequences of volumetric shrinkage when the bond strength is superior to the developed stress [34]. Cusp deflection and tooth fracture are directly associated with the quality of the remaining surrounding area; thus, clinicians should be aware about the quality of the remaining tissues and cavity designs. It is obvious that within the perspective of minimally invasive dentistry, all efforts should be aimed at healthy tooth tissue preservation. However, both clinicians and patients must consider that premature failure might occur due to the unfavorable cavity design.
A recent publication demonstrates that the third most common reason for failure of posterior composite restorations during the 2006–2016 decade was tooth fracture, which changed from 3.45% in 1995–2005 to 23.76% in 2006–2016 [35]. The authors also state that fracture of restoration and of the tooth, together, represents 62.83% of failures in the 2006–2016 period compared with 32.29% in the 1995–2005 period. It could be hypothesized that such differences could be due to the use of more powerful light sources, but an increase in materials’ fracture ratio has also been reported. The authors attribute this change to the increased and wider use of composite materials in complex and multi-surface cavities, which are known to be more prone to tooth and restoration fracture [35].
Postoperative sensitivity has been traditionally described in publications as a potential problem associated with stress. However, this aspect has to be critically analyzed, and nowadays postoperative sensitivity seems more related to difficulties in obtaining a proper hybrid layer in dentin [5, 27]. Postoperative sensitivity is not described as a common cause of premature failure in recent systematic reviews [10, 36]. Considering the approach by Alvanforoush et al. [35] who compared the clinical success of direct composite restorations in vital posterior teeth in two different time periods, it is possible to verify that the incidence of postoperative sensitivity decreased from 11.60% in studies published between 1995 and 2005 to 0.96% in studies published between 2006 and 2016. It is necessary to consider the fact that when resin composites were introduced for posterior restorations, general knowledge about bonding procedures, especially wet bonding associated with the total etch technique, and stress management was not sufficient and consequent pain was probably more frequent. Additionally, Alvanforoush’s study [35] shows that different materials were used in the two decades, so we can speculate that the reduction in postoperative sensitivity over the last decade might also be associated with materials’ improvements in terms of lower volumetric shrinkage.
3.3 What Is the Effect of Stress over the Restoration Longevity?
With the current data available in the literature, it is not possible to clearly state the real effect of stress on the final restoration longevity. However, recent findings on the long-term success of composite restorations show that some factors commonly associated with material properties might not be crucial for real clinical lifespan or could be suppressed by other factors that are out of clinician’s control, such as patients’ general behavior and socioeconomic status [7, 8].
Publications considering more than 20 or even 30 years of follow-up demonstrate that when the patients’ conditions are favorable—i.e., low caries risk and no parafunctional habits—the annual failure rate is low, usually between 1% and 4% [7, 9, 36,37,38]. On the other hand, the annual failure rate varied between 2.3 and 7.9% in a recent study about longevity of direct restorations performed by Dutch dental practitioners [39]. Instead of claiming that material associated properties affect clinical lifespan, or that the amount of stress development may directly affect the clinical lifespan of a composite restoration, one should consider that education in dentistry has to be improved instead of solely relying on materials’ development. There is also the possibility that such differences among clinicians might be related to differences in stress management.
4 Methods for Shrinkage and Stress Evaluation
Since polymerization stress is considered one of the main drawbacks of resin composites, a series of methods have been used throughout the years to determine strain and stress, and numerous publications with detailed explanations may be found in the literature.
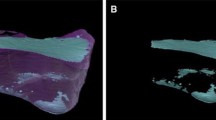
A general list of methodologies used to determine shrinkage/strain must include the mercury dilatometer [40] (Fig. 14.1), the bonded-disc method developed by Watts and Cash [41] (Fig. 14.2), the strain gauges [42, 43], and the linometer [44]. More recently, some complex methods have been based on video and digital images [45,46,47]: laser speckle contrast analysis [48], the mathematical and computational models [49, 50], the X-ray microtomography [51,52,53], and optics [54, 55].

(a) Mercury dilatometer. The figure shows a mercury column and the clasp that holds the resin composite sample and (b) the place where the LCU is positioned. These pictures were kindly donated by Dr. Carmen Silvia C. Pfeifer. Equipment is from the Division of Biomaterials and Biomechanics, School of Dentistry, Oregon Health & Sciences University (Portland, USA). The original picture was published in “Shrinkage Stresses Generated during Resin-Composite Applications: A Review. Schneider LF, Cavalcante LM, Silikas N. 2010; doi:10.4061/2010/131630”

The “Bonded-disc” apparatus. (b) A close view of the LVDT probe in contact with the glass slide during the resin composite photoactivation. Equipment is from the Biomaterials Research Group, School of Dentistry, University of Manchester (Manchester, UK). The original picture was published in “Shrinkage Stresses Generated during Resin-Composite Applications: A Review. Schneider LF, Cavalcante LM, Silikas N. 2010; doi:10.4061/2010/131630”
Stress development is not a material property but a consequence of multiple factors, and specific research methods have been used including the ring-slitting method [56, 57], photoelastic analysis [58, 59], finite element analysis [60, 61], mathematical models [45], force transducers [4, 19, 62,63,64,65,66], and, more recently, crack propagation in ceramics [67,68,69].
Force transducers have been widely used as the main method of stress development analyses. Although the basic principle is the same for all force transducers, there are different measurement approaches for each system, the instrument compliance being the most significant one [2]. Universal testing machines modified with extensometers connected to a computer unit are very precise and can identify movement of extension caused by the polymerization shrinkage and by feedback response compensate deformations, while the sample’s length remains constant (Fig. 14.3). This system does not allow material deformation, and consequently, the registered values of stress tend to be higher than by more compliant methods [70]. Some variations exist within this method, and a significant one is the kind of substrate to which the resin composite sample is attached [71].

Extensometer apparatus connected to a universal testing machine. As a feedback response, the system compensates deformations, and the sample remains constant. Consequently, this kind of method is known as a “low-compliant method.” Pictures kindly donated by Dr. Carmen Silvia C. Pfeifer. Equipment is from the School of Dentistry, University of São Paulo (São Paulo, Brazil). The original picture was published in “Shrinkage Stresses Generated during Resin-Composite Applications: A Review. Schneider LF, Cavalcante LM, Silikas N. 2010; doi:10.4061/2010/131630”
There are also force transducers adapted to systems with unknown or calculated compliance [18, 21, 22, 49, 64, 72, 73] (Figs. 14.4 and 14.5). Unfortunately, besides variations in the final stress values, the comparisons among different materials can also be affected [2], and different interpretations about a given aspect may also vary when all these methods are used. Therefore, it must be clear that care should be taken when analyzing stress data, since the system compliance should also be considered. As the final objective of the in vitro research is to provide valid data that simulate the clinical situations, instrument compliance should be similar to that of the prepared tooth [20]. Wang and Chiang recently demonstrated that the correlation between polymerization shrinkage stress and the C-factor [21] and also the effect of composite filler content on stress development depend on the compliance of the testing instrument [22]. Unfortunately, to date, there are no studies on the validation of polymerization stress analysis based on clinical conditions.

Controlled compliance apparatus for contraction stress test. (a) The entire apparatus with a view of the steel frame and the upper load cell holder; (b) slot for light guide; (c) glass plate positioned; (d) steel piston in position and the space where the resin composite specimen is positioned; (e) equipment ready for use and (f) light-curing procedure during an experiment. These pictures were kindly donated by Dr. Carmen Silvia C. Pfeifer. Equipment is from Division of Biomaterials and Biomechanics, the School of Dentistry, Oregon Health & Sciences University (Portland, USA). The original picture was published in “Shrinkage Stresses Generated during Resin-Composite Applications: A Review. Schneider LF, Cavalcante LM, Silikas N. 2010; doi:10.4061/2010/131630”

(a) The Bioman stress measurement device. (b) A close view of the resin composite specimen. Equipment is from the Biomaterials Research Group, School of Dentistry, University of Manchester (Manchester, UK). The original picture was published in “Shrinkage Stresses Generated during Resin-Composite Applications: A Review. Schneider LF, Cavalcante LM, Silikas N. 2010; doi:10.4061/2010/131630”
5 Stress Control by Clinical Management
Several attempts have been suggested to control or reduce stress development during placement of resin composites. The placement, or filling, technique—incremental vs. bulk—and the photoactivation protocols are under clinicians’ control and have been widely advocated. The use of stress-absorbing layers and thermally modified composites theoretically could reduce stress development, but these two approaches have not become the standard of care. Model and experimental materials have been extensively used to understand the stress phenomenon and to find ways of reduction. Nevertheless only a few new formulations have become commercially available but without guarantees of stress reduction, such as “ormocers,” dimer acid, and “silorane”-based materials [74, 75].
5.1 Placement Techniques
The incremental layering techniques have been advocated due to the inherent confinement of cavities. The rationale is that shrinkage may be less detrimental when there are fewer bonded cavity walls involved at each stage of the restoration procedures. Furthermore, such techniques also enhance the degree of conversion as thin sections undergo higher degree of cure due to lower light attenuation, yielding better mechanical properties [76].
For a long time, the filling technique has been a matter of discussion [34, 60, 77] and came to focus again with the launch of bulk-fill resin composites, which will be addressed further below. The literature is not conclusive concerning the advantages promoted by the incremental layering technique over the effects of resin composite polymerization shrinkage. Versluis et al. [60] assessed the developing stress fields for different incremental filling techniques by finite element analysis (FEA) and concluded that the incremental filling technique increased the deformation of the restored tooth and could actually produce higher polymerization stresses at the restoration interface compared with bulk filling, particularly when many small increments and consecutive light activations are used [78, 79]. Additionally, multiple increments showed to induce greater cuspal movement than a bulk increment in cuspal deflection measurements of premolars [80]. Loguercio et al. [81] reported that some evaluated effects of polymerization shrinkage such as gap width, adhesive bond strength, and the cohesive strength of the resin composite were not reduced by the filling technique under the different C-factor cavities. Lee et al. [82] observed that cusp deflection increased with increasing cavity dimension and C-factor; thus, the use of an incremental filling technique or an indirect composite inlay restoration could reduce the cuspal strain. Conversely, Park et al. [76] found that the bulk-filling technique yielded significantly more cuspal deflection than the incremental filling techniques, concluding that cuspal deflection resulting from polymerization shrinkage can be reduced by incremental filling techniques to obtain optimal outcomes in clinical situations.
Despite the controversy over the advantages of incremental buildup of resin composites, this technique has been broadly recommended for direct resin composite restorations to assure sufficient polymerization in deep cavities with the traditional materials [83].
5.2 Photoactivation Protocols
Photoactivation protocols that were theoretically able to control or reduce stress were strongly suggested in the past. The explanation is that stress release is possible by viscous flow before the vitrification stage, popularly called as the pre-gel state, without compromising the final polymer properties and became very popular with clinicians [84,85,86]. It has been accepted that initial light exposure at lower irradiance values would lead to the formation of a reduced number of polymer growth centers, slowing down the reaction and decreasing the rate and the final stress development due to increased time for polymer relaxation. Some outcomes suggest that a possible stress reduction is derived from lower degree of conversion [87].
Despite large breadth of in vitro studies about curing protocols such as soft-start and pulse-delay, scientific literature lacks data from clinical trials. A few studies have suggested that those alternative protocols do not have a measurable effect on the longevity of composite restorations [88,89,90,91]. In another publication, the significance of the C-factor has been questioned in a scenario with low failure after 12 years in cavities with a high C-factor [6]. However, Ferracane and Hilton [5] suggest that the excellent outcomes found by van Dijken [6] also “resulted from the efforts to reduce or minimize stress by the curing methods used.”
By careful analyses of articles derived from clinical trials, it is possible to relate scientific evidence of certain material properties with clinical outcomes. In a 30-year follow-up of three dental composites, it was found that the chemically-cured resin composites showed better performance than the light-cured composite [38] contrary to expectations. However, the rate of polymerization for chemically-cured materials is known to be lower than that of photoactivated, and, therefore, stress release would be possible. It is also necessary to consider the chance of poor conversion of the photoactivated material, especially considering the light sources available 30 years ago and the lack of familiarity in clinical use of light-curable composites for posterior restorations by clinicians at that time.
5.3 Stress-Absorbing Layers
The suggested use of flowable composites as “stress-absorbing layers” is based on the “elastic cavity wall concept.” Although controversial, this concept suggests that the shrinkage stress generated by a subsequent layer of higher modulus resin composite can be absorbed by an elastic intermediary layer, thereby reducing the stress at the tooth-restoration interface manifested clinically as a reduction in cuspal deflection [92,93,94,95]. However, van Dijken and Pallesen [96] found that flowable resin composite as an intermediate layer did not result in improved effectiveness in Class II restorations during a 7-year evaluation period.
A different approach is the use of glass ionomer cements to replace part of the tooth and reduce the amount of the shrinkable composite. However, the systematic review by Opdam et al. [10] clearly demonstrated no benefits of using this technique. In fact, a possibility of higher prevalence of fractures was suggested due to differences of elastic moduli and consequent fatigue over time.
5.4 Pre-warming Composites
The idea behind pre-warming composites is that increased temperature decreases system viscosity and enhances radical mobility, resulting in additional polymerization and higher conversion [97, 98]. At raised temperatures, in theory, it would be possible to obtain higher degree of conversion before the vitrification point, decreasing the magnitude of stress [99]. In a recent study by Tauböck et al. [98], the authors demonstrated that composite pre-warming reduced the shrinkage stress formation of high-viscosity bulk-fill and conventional resin composites while maintaining or increasing degree of conversion. Apart from in vitro data, there are no published clinical data. It should be pointed out that such pre-warming composites could increase technique sensitivity/variability or only be useful for marketing new gadgets.
6 Stress Development Understanding and Control Related to Material Composition
Undoubtedly serious academic research in the field of dental materials science has provided theories and knowledge that have become widely accepted in both the academic and clinical community, improving education of dentists and clinical practice as well as development of new materials. At this point, a few questions should be pointed out: how many “experimental materials” do indeed find their way to the market? And do those marketed materials indeed affect the final clinical outcome? Is this a cost-effective model?
Since Bowen’s pioneering work resulting in BisGMA-based formulations, the basic principles of dental composites have changed very little. But it was from the industry that we saw the evolution from paste-to-paste mixed formulations to nowadays materials that facilitate clinicians’ work and improved restoration general qualities. Nevertheless, stress development reduction is still a matter of concern, and dental industry has launched the so-called low-shrinkage materials over the years. However, there is no evidence that such “improvements” do have a positive effect on the performance of composite restorations. In a fierce competition on the dental market, the manufacturers are sometimes urged by marketing rather than scientific needs to launch new materials. Yet it is the duty of the scientific community to critically ascertain new materials and their effects on clinical practice.
6.1 Model and Experimental Composites
Model composites are valuable means to systematically understand the effect of materials’ components on their final properties and behavior [100,101,102,103,104]. One very interesting study, for example, was published by Gonçalves et al. [103]. By using different concentrations of BisGMA and TEGDMA and/or BisEMA as comonomers, the authors analyzed the contraction stress determinants in dimethacrylate composites and demonstrated that the association between polymerization stress and conversion (R2 = 0.905) was higher than stress and shrinkage (R2 = 0.825) and stress and elastic modulus (R2 = 0.623).
Recent studies have shown that ester-free thiol-ene derivatives exhibit lower shrinkage stress and moisture absorption than conventional BisGMA/TEGDMA resin and that low viscosity allows high filler content [105, 106]. Thio-urethane oligomers improved conversion and mechanical properties with reduced shrinkage and stress of model resin cements in a study by Bacchi et al. [107]. As stated by the authors, the success was accomplished by the use of photoinitiators commonly applied in commercial materials, which facilitates the benchtop to chairside implementation of such additives without changing common operatory procedures. Improved conversion and mechanical properties allied with lower stress values were also found for restorative composite by the same group [108]. Although promising, there is a long way until such innovations become potentially useful for the market.
6.2 Commercially Available Materials
Methacrylate-based materials represent the vast majority of commercially available materials and have been used to systematically understand shrinkage stress phenomenon through in vitro tests [74, 75]. Considering clinical data within systematic reviews, methacrylate-based hybrid composites have demonstrated the best performance over the years [7, 33, 109]. At this point, a question may be asked: if such materials are still the gold standard and several developments were claimed over the last years, why do we not see major clinical success? A possible explanation may be the fact that clinical trials are often performed in very well-controlled conditions, such as experienced operators with proper time for careful execution of all procedures, highly motivated patients with low caries risk, etc. The question is whether or not the new materials would impact the clinical performance in not so well-controlled conditions. Anyway, it may be assumed that clinical success is possible with materials available on the market in the last 10 years.
Silorane-based materials and bulk-fill composites represent two interesting groups of commercially available materials that caught attention of the scientific community. Silorane-based materials were launched promising less than 1% volumetric shrinkage and quickly became largely investigated materials [75, 110, 111]. It is possible to find more than 300 articles published over the past 10 years on PubMed by simple typing “silorane AND dental.” Unfortunately, silorane-based materials failed to produce significant improvements in both in vitro and in vivo studies and are off the market today. In addition, a recent systematic review of clinical studies showed no gain in clinical performance of silorane compared with methacrylate-based resin composites [112].
Currently “bulk-fill” composites are in focus of a number of studies [113,114,115,116,117]. Although dental companies might claim certain innovative components—like specific photoinitiators and polymerization modulators—these materials are, in fact, derived from a combination of well-known possibilities. The use of UDMA-based molecules, the better matching of refractive indexes from monomers and filler particles, and the affordable high-intensity light sources are some of them. It should be highlighted that the use of bulk-fill composites is encouraged on the notion that stress development would not be a detrimental adverse effect. Only few studies have been conducted with such materials and have provided good results in the studies with no more than 5-6 years [118, 119]. More clinical data is necessary to answer those questions arising from in vitro studies [113,114,115,116].
7 Final Thoughts: What Do We Need to Look For?
Longevity of direct restorations is related to many factors including patient’s general and health conditions and the clinical condition of the tooth to be restored—such as the volume of remaining walls, previous endodontic treatment, and others—but also the clinician who executes the procedure. The understanding of materials handling characteristics is crucial for the success of any clinical procedure pointing to the need for better teaching strategies.
The present discussion has not the intention to underestimate the importance of polymerization shrinkage stress in direct restorations since this phenomenon was part of a series of industrial developments and academic research over the last years leading to the current state of dental composites. However, the lack of clear clinical evidence about the effect of shrinkage stress on the restoration longevity suggests that shrinkage stress alone may not be of such a great interest. Clinical trials comparing a wide range of materials have hardly shown differences that might be related to shrinkage stress. A slow decline in the volume of published data on the phenomenon, even in vitro studies, also suggests that this topic may not be the main problem of resin composites as it was believed in recent past. It is, however, important to keep an open mind with regard to those aspects that clearly influence the treatment immediate success and restoration longevity. Although this entire chapter aimed to address direct restorations, researchers and clinicians should be aware of potential negative effects of polymerization stress when resin composites are applied as luting materials (as resin cements, flowable composites or thermally-modified resin composites) for indirect restorations - specially those fabricated with ceramics - due to the very high constriction and low compliant situation.
References
Ferracane JL. Developing a more complete understanding of stresses produced in dental composites during polymerization. Dent Mater. 2005;21(1):36–42.
Ferracane JL. Buonocore Lecture. Placing dental composites – a stressful experience. Oper Dent. 2008;33(3):247–57.
Braga RR, Ferracane JL. Alternatives in polymerization contraction stress management. Crit Rev Oral Biol Med. 2004;15(3):176–84.
Braga RR, Ballester RY, Ferracane JL. Factors involved in the development of polymerization shrinkage stress in resin-composites: a systematic review. Dent Mater. 2005;21(10):962–70.
Ferracane JL, Hilton TJ. Polymerization stress – is it clinically meaningful? Dent Mater. 2016;32(1):1–10.
van Dijken JW. Durability of resin composite restorations in high C-factor cavities: a 12-year follow-up. J Dent. 2010;38(6):469–74.
Demarco FF, Corrêa MB, Cenci MS, Moraes RR, Opdam NJ. Longevity of posterior composite restorations: not only a matter of materials. Dent Mater. 2012;28(1):87–101.
Correa MB, Peres MA, Peres KG, Horta BL, Barros AJ, Demarco FF. Do socioeconomic determinants affect the quality of posterior dental restorations? A multilevel approach. J Dent. 2013;41(11):960–7.
van de Sande FH, Opdam NJ, Rodolpho PA, Correa MB, Demarco FF, Cenci MS. Patient risk factors’ influence on survival of posterior composites. J Dent Res. 2013;92(7 Supplement):78S–83S.
Opdam NJM, van de Sande FH, Bronkhorst E, Cenci MS, Bottenberg P, Pallesen U, Gaengler P, Lindberg A, Huysmans MCDNJM, van Dijken JWV. Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res. 2014;93(10):943–9.
van Dijken JW, Lindberg A. A 15-year randomized controlled study of a reduced shrinkage stress resin composite. Dent Mater. 2015;31(9):1150–8.
Cramer NB, Stansbury JW, Bowman CN. Recent advances and developments in composite dental restorative materials. J Dent Res. 2011;90(4):402–16.
Schneider LF, Cavalcante LM, Silikas N. Shrinkage stresses generated during resin-composite applications: a review. J Dent Biomech. 2010:1–14. doi:10.4061/2010/131630.
Loshaek S, Fox TG. Cross-linked polymers. I. Factors influencing the efficiency of cross-linking in copolymers of methyl methacrylate and glycol dimethacrylate. J Am Chem Soc. 1953;75(14):3544–50.
Cunha LG, Alonso RC, Pfeifer CS, Correr-Sobrinho L, Ferracane JL, Sinhoreti MA. Modulated photoactivation methods: influence on contraction stress, degree of conversion and push-out bond strength of composite restoratives. J Dent. 2007;35(4):318–24.
Pfeifer CS, Ferracane JL, Sakaguchi RL, Braga RR. Factors affecting photopolymerization stress in dental composites. J Dent Res. 2008;87(11):1043–7.
Palin WM, Hadis MA, Leprince JG, Leloup G, Boland L, Fleming GJ, Krastl G, Watts DC. Reduced polymerization stress of MAPO-containing resin composites with increased curing speed, degree of conversion and mechanical properties. Dent Mater. 2014;30(5):507–16.
Wang Z, Landis FA, Giuseppetti AA, Lin-Gibson S, Chiang MY. Simultaneous measurement of polymerization stress and curing kinetics for photo-polymerized composites with high filler contents. Dent Mater. 2014;30(12):1316–24.
Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in relation to configuration of the restoration. J Dent Res. 1987;66(11):1636–9.
Watts DC, Satterthwaite JD. Axial shrinkage-stress depends upon both C-factor and composite mass. Dent Mater. 2008;24(1):1–8.
Wang Z, Chiang MY. Correlation between polymerization shrinkage stress and C-factor depends upon cavity compliance. Dent Mater. 2016;32(3):343–52.
Wang Z, Chiang MY. System compliance dictates the effect of composite filler content on polymerization shrinkage stress. Dent Mater. 2016;32(4):551–60.
Han SH, Sadr A, Tagami J, Park SH. Internal adaptation of resin composites at two configurations: influence of polymerization shrinkage and stress. Dent Mater. 2016;32(9):1085–94.
Bicalho AA, de Souza SJ, de Rosatto CM, Tantbirojn D, Versluis A, Soares CJ. Effect of temperature and humidity on post-gel shrinkage, cusp deformation, bond strength and shrinkage stress – construction of a chamber to simulate the oral environment. Dent Mater. 2015;31(12):1523–32.
Bicalho AA, Tantbirojn D, Versluis A, Soares CJ. Effect of occlusal loading and mechanical properties of resin composite on stress generated in posterior restorations. Am J Dent. 2014;27(3):129–33.
Suiter EA, Watson LE, Tantbirojn D, Lou JS, Versluis A. Effective expansion: balance between shrinkage and hygroscopic expansion. J Dent Res. 2016;95(5):543–9.
Sarrett DC. Clinical challenges and the relevance of materials testing for posterior composite restorations. Dent Mater. 2005;21(1):9–20.
Cenci MS, Tenuta LM, Pereira-Cenci T, Del Bel Cury AA, ten Cate JM, Cury JA. Effect of microleakage and fluoride on enamel-dentine demineralization around restorations. Caries Res. 2008;42(5):369–79.
Cenci MS, Pereira-Cenci T, Cury JA, Ten Cate JM. Relationship between gap size and dentine secondary caries formation assessed in a microcosm biofilm model. Caries Res. 2009;43(2):97–102.
Nedeljkovic I, Teughels W, De Munck J, Van Meerbeek B, Van Landuyt KL. Is secondary caries with composites a material-based problem? Dent Mater. 2015;31:e247–77.
Jokstad A. Secondary caries and microleakage. Dent Mater. 2016;32:11–25.
Ferracane JL, Mitchem JC. Relationship between composite contraction stress and leakage in Class V cavities. Am J Dent. 2003;16(4):239–43.
Heintze SD, Rousson V, Hickel R. Clinical effectiveness of direct anterior restorations – a meta-analysis. Dent Mater. 2015;31(5):481–95.
Rosatto CM, Bicalho AA, Veríssimo C, Bragança GF, Rodrigues MP, Tantbirojn D, Versluis A, Soares CJ. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J Dent. 2015;43(12):1519–28.
Alvanforoush N, Palamara J, Wong R, Burrow MF. A Comparison between published clinical success of direct resin composite restorations in vital posterior teeth in 1995–2005 and 2006–2016 periods. Aust Dent J. 2017;62(2):132–45. doi:10.1111/adj.12487.
Demarco FF, Collares K, Coelho-de-Souza FH, Correa MB, Cenci MS, Moraes RR, Opdam NJ. Anterior composite restorations: a systematic review on long-term survival and reasons for failure. Dent Mater. 2015;31(10):1214–24.
Da Rosa Rodolpho PA, Donassollo TA, Cenci MS, Loguércio AD, Moraes RR, Bronkhorst EM, Opdam NJ, Demarco FF. 22-year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater. 2011;27(10):955–63.
Pallesen U, van Dijken JW. A randomized controlled 30 years follow up of three conventional resin composites in Class II restorations. Dent Mater. 2015;31(10):1232–44.
Laske M, Opdam NJ, Bronkhorst EM, Braspenning JC, Huysmans MC. Longevity of direct restorations in Dutch dental practices. Descriptive study out of a practice based research network. J Dent. 2016;46:12–7.
de Gee AJ, Davidson CL, Smith A. A modified dilatometer for continuous recording of volumetric polymerization shrinkage of composite restorative materials. J Dent. 1981;9(1):36–42.
Watts DC, Cash AJ. Determination of polymerization shrinkage kinetics in visible-light-cured materials: methods development. Dent Mater. 1991;7(4):281–7.
Sakaguchi RL, Sasik CT, Bunczak MA, Douglas WH. Strain gauge method for measuring polymerization contraction of composite restoratives. J Dent. 1991;19(5):312–6.
Sakaguchi RL, Peters MC, Nelson SR, Douglas WH, Poort HW. Effects of polymerization contraction in composite restorations. J Dent. 1992;20(3):178–82.
de Gee AF, Feilzer AJ, Davidson CL. True linear polymerization shrinkage of unfilled resins and composites determined with a linometer. Dent Mater. 1993;9(1):11–4.
Li J, Li H, Fok SL. A mathematical analysis of shrinkage stress development in dental composite restorations during resin polymerization. Dent Mater. 2008;24(7):923–31.
Miletic V, Manojlovic D, Milosevic M, Mitrovic N, Stankovic TS, Maneski T. Analysis of local shrinkage patterns of self-adhering and flowable composites using 3D digital image correlation. Quintessence Int. 2011;42(9):797–804.
Fok AS. Shrinkage stress development in dental composites – an analytical treatment. Dent Mater. 2013;29(11):1108–15.
Sato T, Miyazaki M, Rikuta A. Real-time dimensional change in light-cured composites at various depths using laser speckle contrast analysis. Eur J Oral Sci. 2004;112(6):538–44.
Sakaguchi RL, Wiltbank BD, Murchison CF. Prediction of composite elastic modulus and polymerization shrinkage by computational micromechanics. Dent Mater. 2004;20(4):397–401.
Atai M, Watts DC. A new kinetic model for the photopolymerization shrinkage-strain of dental composites and resin-monomers. Dent Mater. 2006;22(8):785–91.
Kakaboura A, Rahiotis C, Watts DC, Silikas N, Eliades G. 3D-marginal adaptation versus setting shrinkage in light-cured microhybrid resin composites. Dent Mater. 2007;23(3):272–8.
Sun J, Eidelman N, Lin-Gibson S. 3D mapping of polymerization shrinkage using X-ray micro-computed tomography to predict microleakage. Dent Mater. 2009;25(3):314–20.
Van Ende A, Van de Casteele E, Depypere M, De Munck J, Li X, Maes F, Wevers M, Van Meerbeek B. 3D volumetric displacement and strain analysis of composite polymerization. Dent Mater. 2015;31(4):453–61.
Kweon HJ, Ferracane J, Kang K, Dhont J, Lee IB. Spatio-temporal analysis of shrinkage vectors during photo-polymerization of composite. Dent Mater. 2013;29(12):1236–43.
Tantbirojn D, Pfeifer CS, Amini AN, Versluis A. Simple optical method for measuring free shrinkage. Dent Mater. 2015;31(11):1271–8.
Park JW, Ferracane JL. Measuring the residual stress in dental composites using a ring slitting method. Dent Mater. 2005;21(9):882–9.
Park JW, Ferracane JL. Residual stress in composites with the thin-ring-slitting approach. J Dent Res. 2006;85(10):945–9.
Ernst CP, Meyer GR, Klöcker K, Willershausen B. Determination of polymerization shrinkage stress by means of a photoelastic investigation. Dent Mater. 2004;20(4):313–21.
Kinomoto Y, Torii M. Photoelastic analysis of polymerization contraction stresses in resin composite restorations. J Dent. 1998;26(2):165–71.
Versluis A, Douglas WH, Cross M, Sakaguchi RL. Does an incremental filling technique reduce polymerization shrinkage stresses? J Dent Res. 1996;75(3):871–8.
Versluis A, Tantbirojn D, Douglas WH. Do dental composites always shrink toward the light? J Dent Res. 1998;77(6):1435–45.
Davidson CL, de Gee AJ. Relaxation of polymerization contraction stresses by flow in dental composites. J Dent Res. 1984;63(2):146–8.
Condon JR, Ferracane JL. Assessing the effect of composite formulation on polymerization stress. J Am Dent Assoc. 2000;131(4):497–503.
Watts DC, Marouf AS, Al-Hindi AM. Photo-polymerization shrinkage-stress kinetics in resin-composites: methods development. Dent Mater. 2003;19(1):1–11.
Braga RR, Ferracane JL. Contraction stress related to degree of conversion and reaction kinetics. J Dent Res. 2002;81(2):114–8.
Braga RR, Boaro LC, Kuroe T, Azevedo CL, Singer JM. Influence of cavity dimensions and their derivatives (volume and ‘C’ factor) on shrinkage stress development and microleakage of composite restorations. Dent Mater. 2006;22(9):818–23.
Yamamoto T, Ferracane JL, Sakaguchi RL, Swain MV. Calculation of contraction stresses in dental composites by analysis of crack propagation in the matrix surrounding a cavity. Dent Mater. 2009;25(4):543–50.
Yamamoto T, Kubota Y, Momoi Y, Ferracane JL. Polymerization stresses in low-shrinkage dental resin composites measured by crack analysis. Dent Mater. 2012;28(9):e143–9.
Yamamoto T, Hanabusa M, Momoi Y, Sakaguchi RL. Polymerization stress of dental resin composite continues to develop 12 hours after irradiation. J Esthet Restor Dent. 2015;27(1):44–54.
Witzel MF, Ballester RY, Meira JB, Lima RG, Braga RR. Composite shrinkage stress as a function of specimen dimensions and compliance of the testing system. Dent Mater. 2007;23(2):204–10.
Gonçalves F, Pfeifer CS, Ferracane JL, Braga RR. Contraction stress determinants in dimethacrylate composites. J Dent Res. 2008;87(4):367–71.
Miguel A, de la Macorra JC. A predictive formula of the contraction stress in restorative and luting materials attending to free and adhered surfaces, volume and deformation. Dent Mater. 2001;17(3):241–6.
Lu H, Stansbury JW, Bowman CN. Towards the elucidation of shrinkage stress development and relaxation in dental composites. Dent Mater. 2004;20(10):979–86.
Boaro LC, Gonçalves F, Guimarães TC, Ferracane JL, Versluis A, Braga RR. Polymerization stress, shrinkage and elastic modulus of current low-shrinkage restorative composites. Dent Mater. 2010;26(12):1144–50.
Bacchi A, Feitosa VP, da Silva Fonseca AS, Cavalcante LM, Silikas N, Schneider LF. Shrinkage, stress, and modulus of dimethacrylate, ormocer, and silorane composites. J Conserv Dent. 2015;18(5):384–8.
Park J, Chang J, Ferracane J, Lee IB. How should composite be layered to reduce shrinkage stress: incremental or bulk filling? Dent Mater. 2008;24(11):1501–5.
Kim YJ, Kim R, Ferracane JL, Lee IB. Influence of the compliance and layering method on the wall deflection of simulated cavities in bulk-fill composite restoration. Oper Dent. 2016;41(6):e183–94.
Bicalho AA, Pereira RD, Zanatta RF, Franco SD, Tantbirojn D, Versluis A, Soares CJ. Incremental filling technique and composite material – part I: cuspal deformation, bond strength, and physical properties. Oper Dent. 2014;39(2):E71–82.
Bicalho AA, Valdívia AD, Barreto BC, Tantbirojn D, Versluis A, Soares CJ. Incremental filling technique and composite material – part II: shrinkage and shrinkage stresses. Oper Dent. 2014;39(2):E83–92.
Abbas G, Fleming GJ, Harrington E, Shortall AC, Burke FJ. Cuspal movement and microleakage in premolar teeth restored with a packable composite cured in bulk or in increments. J Dent. 2003;31(6):437–44.
Loguercio AD, Reis A, Ballester RY. Polymerization shrinkage: effects of constraint and filling technique in composite restorations. Dent Mater. 2004;20(3):236–43.
Lee MR, Cho BH, Son HH, Um CH, Lee IB. Influence of cavity dimension and restoration methods on the cusp deflection of premolars in composite restoration. Dent Mater. 2007;23(3):288–95.
Frauscher KE, Ilie N. Depth of cure and mechanical properties of nano-hybrid resin-based composites with novel and conventional matrix formulation. Clin Oral Investig. 2012;16(5):1425–34.
Sakaguchi RL, Berge HX. Reduced light energy density decreases post-gel contraction while maintaining degree of conversion in composites. J Dent. 1998;26(8):695–700.
Sakaguchi RL, Wiltbank BD, Murchison CF. Contraction force rate of polymer composites is linearly correlated with irradiance. Dent Mater. 2004;20(4):402–7.
Pfeifer CS, Braga RR, Ferracane JL. Pulse-delay curing: influence of initial irradiance and delay time on shrinkage stress and microhardness of restorative composites. Oper Dent. 2006;31(5):610–5.
Lu H, Stansbury JW, Bowman CN. Impact of curing protocol on conversion and shrinkage stress. J Dent Res. 2005;84(9):822–6.
Oberländer H, Friedl KH, Schmalz G, Hiller KA, Kopp A. Clinical performance of polyacid-modified resin restorations using “softstart-polymerization”. Clin Oral Investig. 1999;3(2):55–61.
Brackett WW, Covey DA, St Germain HA Jr. One-year clinical performance of a self-etching adhesive in class V resin composites cured by two methods. Oper Dent. 2002;27(3):218–22.
Chan DC, Browning WD, Frazier KB, Brackett MG. Clinical evaluation of the soft-start (pulse-delay) polymerization technique in Class I and II composite restorations. Oper Dent. 2008;33(3):265–71.
van Dijken JW, Pallesen U. A 7-year randomized prospective study of a one-step self-etching adhesive in non-carious cervical lesions. The effect of curing modes and restorative material. J Dent. 2012;40(12):1060–7.
Oliveira LC, Duarte S Jr, Araujo CA, Abrahão A. Effect of low-elastic modulus liner and base as stress-absorbing layer in composite resin restorations. Dent Mater. 2010;26(3):e159–69.
Choi KK, Condon JR, Ferracane JL. The effects of adhesive thickness on polymerization contraction stress of composite. J Dent Res. 2000;79(3):812–7.
Braga RR, Hilton TJ, Ferracane JL. Contraction stress of flowable composite materials and their efficacy as stress-relieving layers. J Am Dent Assoc. 2003;134(6):721–8.
Cara RR, Fleming GJ, Palin WM, Walmsley AD, Burke FJ. Cuspal deflection and microleakage in premolar teeth restored with resin-based composites with and without an intermediary flowable layer. J Dent. 2007;35(6):482–9.
van Dijken JW, Pallesen U. Clinical performance of a hybrid resin composite with and without an intermediate layer of flowable resin composite: a 7-year evaluation. Dent Mater. 2011;27(2):150–6.
Daronch M, Rueggeberg FA, De Goes MF. Monomer conversion of pre-heated composite. J Dent Res. 2005;84(7):663–7.
Tauböck TT, Tarle Z, Marovic D, Attin T. Pre-heating of high-viscosity bulk-fill resin composites: effects on shrinkage force and monomer conversion. J Dent. 2015;43(11):1358–64.
Jongsma LA, Kleverlaan CJ. Influence of temperature on volumetric shrinkage and contraction stress of dental composites. Dent Mater. 2015;31(6):721–5.
Schneider LF, Consani S, Sakaguchi RL, Ferracane JL. Alternative photoinitiator system reduces the rate of stress development without compromising the final properties of the dental composite. Dent Mater. 2009;25(5):566–72.
Gonçalves F, Pfeifer CC, Stansbury JW, Newman SM, Braga RR. Influence of matrix composition on polymerization stress development of experimental composites. Dent Mater. 2010;26(7):697–703.
Gonçalves F, Kawano Y, Braga RR. Contraction stress related to composite inorganic content. Dent Mater. 2010;26(7):704–9.
Gonçalves F, Azevedo CL, Ferracane JL, Braga RR. BisGMA/TEGDMA ratio and filler content effects on shrinkage stress. Dent Mater. 2011;27(6):520–6.
Satterthwaite JD, Maisuria A, Vogel K, Watts DC. Effect of resin-composite filler particle size and shape on shrinkage-stress. Dent Mater. 2012;28(6):609–14.
Podgórski M, Becka E, Claudino M, Flores A, Shah PK, Stansbury JW, Bowman CN. Ester-free thiol-ene dental restoratives – Part A: Resin development. Dental Materials. 2015;31:1255–62.
Podgórski M, Becka E, Claudino M, Flores A, Shah PK, Stansbury JW, Bowman CN. Ester-free thiol-ene dental restoratives – Part B: composite development. Dent Mater. 2015;31(11):1263–70.
Bacchi A, Consani RL, Martim GC, Pfeifer CS. Thio-urethane oligomers improve the properties of light-cured resin cements. Dent Mater. 2015;31(5):565–74.
Bacchi A, Nelson M, Pfeifer CS. Characterization of methacrylate-based composites containing thio-urethane oligomers. Dent Mater. 2016;32(2):233–9.
Heintze SD, Rousson V. Clinical effectiveness of direct class II restorations - a meta-analysis. J Adhes Dent. 2012;14(5):407–31.
Almeida e Silva JS, Rolla JN, Baratieri LN, Monteiro S Jr. The influence of different placement techniques on the microtensile bond strength of low-shrink silorane composite bonded to Class I cavities. Gen Dent. 2011;59(6):e233–7.
Arrais CA, Oliveira MT, Mettenburg D, Rueggeberg FA, Giannini M. Silorane- and high filled-based “low-shrinkage” resin composites: shrinkage, flexural strength and modulus. Braz Oral Res. 2013;27(2):97–102.
Magno MB, Nascimento GC, Rocha YS, Ribeiro BD, Loretto SC, Maia LC. Silorane-based composite resin restorations are not better than conventional composites – a meta-analysis of clinical studies. J Adhes Dent. 2016;18(5):375–86.
Yamasaki LC, De Vito Moraes AG, Barros M, Lewis S, Francci C, Stansbury JW, Pfeifer CS. Polymerization development of “low-shrink” resin composites: reaction kinetics, polymerization stress and quality of network. Dent Mater. 2013;29(9):e169–79.
Kim RJ, Kim YJ, Choi NS, Lee IB. Polymerization shrinkage, modulus, and shrinkage stress related to tooth-restoration interfacial debonding in bulk-fill composites. J Dent. 2015;43(4):430–9.
Guo Y, Landis FA, Wang Z, Bai D, Jiang L, Chiang MY. Polymerization stress evolution of a bulk-fill flowable composite under different compliances. Dent Mater. 2016;32(4):578–86.
Al Sunbul H, Silikas N, Watts DC. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent Mater. 2016;32(8):998–1006.
Kalliecharan D, Germscheid W, Price RB, Stansbury J, Labrie D. Shrinkage stress kinetics of bulk fill resin-based composites at tooth temperature and long time. Dent Mater. 2016;32(11):1322–31.
van Dijken JW, Pallesen U. Posterior bulk-filled resin composite restorations: a 5-year randomized controlled clinical study. J Dent. 2016;51:29–35.
van Dijken JW, Pallesen U. Bulk-filled posterior resin restorations based on stress-decreasing resin technology: a randomized, controlled 6-year evaluation. Eur J Oral Sci. 2017;125 (4):303–309
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Schneider, L.F., Moraes, R.R. (2018). Polymerization Shrinkage Stress. In: Miletic, V. (eds) Dental Composite Materials for Direct Restorations. Springer, Cham. https://doi.org/10.1007/978-3-319-60961-4_14
Download citation
DOI: https://doi.org/10.1007/978-3-319-60961-4_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-60960-7
Online ISBN: 978-3-319-60961-4
eBook Packages: MedicineMedicine (R0)