
Abstract
It is believed that the development of metastatic cancer requires the presence of circulating tumor cells (CTCs) , which are found in a patient’s circulation as rare abnormal cells comingled with billions of the normal red and white blood cells. The systems developed for detection of CTCs have brought progress to cancer treatment. The molecular characterization of CTCs can aid in the development of new drugs, and their presence during treatment can help clinicians determine the prognosis of the patient. Studies have been carried out in patients early in the disease course, with only primary tumors, and the role of CTCs in prognosis seems to be as important as it is in patients with metastatic disease. The published studies on CTCs have focused on their prognostic significance, their utility in real-time monitoring of therapies, the identification of therapeutic and resistance targets, and understanding the process of metastasis . The analysis of CTCs during the early stages, as a “liquid biopsy,” helps to monitor patients at different points in the disease course, including minimal residual disease, providing valuable information about the very early assessment of treatment effectiveness. Finally, CTCs can be used to screen patients with family histories of cancer or with diseases that can lead to the development of cancer. With standard protocols, this easily obtained and practical tool can be used to prevent the growth and spread of cancer. In this chapter, we review some important aspects of CTCs , surveying the disease aspects where these cells have been investigated.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1.1 Circulating Tumor Cells (CTCs) as Prognostic Factors in the Metastatic Setting
It is believed that the dissemination of cancer requires the presence of CTCs, which are defined as isolated single or clusters of cancerous cells in the blood or lymphatic fluids co-mingled with billions of normal hematopoietic cells (Mego et al. 2010). The presence of CTCs in the peripheral blood was first reported by Thomas Ashworth (1869) , an Australian doctor at Melbourne Hospital. He studied material obtained from the autopsy of a patient with metastatic subcutaneous tumors located in the anterior wall of the chest and abdomen. He noted circulating cells (obtained from the saphenous vein of the right leg) identical to those from tumors and postulated that these cells were derived from an existing tumor structure, they must have traversed a large part of the circulatory system to reach the inside of the saphenous vein the right leg.
The development of enrichment systems and immunohistochemical detection of CTCs represents significant progress for the scientific community. The best known is the CellSearch® System, which separates the cells with magnetic beads coated with anti-epithelial cell adhesion molecule (EpCAM) antibody followed by flow cytometry of cells captured with anti-cytokeratin fluorescence. Reading is done in semi-automated microscope (revised by Riethdorf and Pantel 2008). In 2007, the U.S. Food and Drug Administration (FDA) approved the system for monitoring patients with metastatic breast, prostate, and colorectal tumors (www.accessdata.fda.gov/cdrh_docs/reviews/K071729).
The overall majority of metastases are localized in internal organs, such as lung, bone, or liver. Because of this, conventional biopsies of metastatic lesions are invasive, painful and expensive. Accordingly, both the isolation and characterization of CTCs might serve as a real time “liquid biopsy ” (Hayes and Paoletti 2013).
Using the CellSearch® System, Cristofanilli et al. (2004) reported a study of 177 patients with metastatic breast cancer , performing the CTC counts before and after the start of treatment for metastatic disease. Patients with ≥5 CTCs/7.5 ml of blood when compared to those with less <5 CTCs/7.5 ml, had lower progression-free survival (2.7 versus 7 months, p < 0.001) and reduced overall survival (10.1 versus 18 months, p < 0.001). After the first segment following the beginning of treatment, this difference between the groups persisted (in relation to the survival and the number of CTCs). Multivariate analysis of CTCs levels before and after the start of treatment proved the significance of these predictors of overall survival (OS) and progression-free survival (PFS). Furthermore, it was observed that about 70% of patients with metastatic disease had CTC counts above 1/7.5 ml of peripheral blood. This study provided key evidence for the use of CTCs and was used to clear CellSearch® by the FDA.
Using the same CTC detection system, Nolé et al. (2008) studied 80 patients with metastatic breast cancer and evaluated them at the beginning of treatment, at 4 and 8 weeks after the first clinical assessment, and then every 2 months thereafter. Before the start of the treatment, 49 patients had ≥5 CTCs. In multivariate analysis, the CTC levels before treatment were significantly associated with PFS (relative risk [RR] 2.5, 95% CI). Patients with persistent levels of CTCs ≥5 had increased risk of progression compared to those with CTCs <5 (RR 6.4, 95% CI). These studies indicate the likely utility of CTCs in assessing the responses of patients with metastatic breast tumors.
For colorectal cancers (CRC) , the primary strategy for treatment is complete resection of the primary lesion (Katsumata et al. 2006). However, despite this, some patients experience recurrences that are believed to reflect residual micrometastases. Conventional diagnostic methods are not capable of detecting CTCs present in these sites that are eventually released into the circulation. Katsumata et al. (2006) used the reverse transcription polymerase chain reaction (RT-PCR) to detect CTCs, through the identification of cytokeratin genes and carcinoembryonic antigen (CEA). They analyzed 57 patients with CRC who underwent surgery. The presence of cytokeratin 20 (CK20) in peripheral blood was evaluated. The CK20 mRNA was found in 42.1% of patients and was correlated with lymph node metastasis (p = 0.037). The 5-year overall survival (5y–OS) for CK20 positive patients was 62.5% whereas for CK20 negative it was 87.5% (p = 0.048). Therefore, the authors advocate the idea of looking at CTCs as being one of the best predictors of disease recurrence. However, it is known that hematopoietic cells may express “not legitimate” antigens associated with tumor or epithelial cells, and pseudogenes can lead to PCR products identical to imprinted genes, which can lead to false positive results by RT-PCR (Gunn et al. 1996).
Sastre et al. (2008) observed a positive correlation between the number of CTCs and clinical stage in 97 patients with the following characteristics: non-metastatic CRC newly diagnosed or rectal cancer without neoadjuvant chemo-radiotherapy; metastatic CRC newly diagnosed; and CRC recurrence. They used a control group of 30 healthy patients. A cut-off of 2 CTCs/7.5 ml was chosen for this study. There was an observed relationship between CTCs and location of the primary tumor, increased levels of CEA, lactate dehydrogenase and degree of differentiation.
De Giorgi et al. (2010) evaluated the relation between the detection and prognostic significance of CTCs and sites of metastases detected by 2 [fluorine-18]-fluoro-2-deoxy-D-glucose-positron emission tomography/computed tomography (FDG-PET/CT) in patients with metastatic breast cancer . The study included 195 patients. Higher numbers of CTCs were observed in patients with bone metastases (detected by PET/CT) than in patients without these metastases (mean 65.7 versus 3.3; p = 0.012) as well as in patients with multiple metastases in relation to one or two bone lesions (mean 77.7 versus 2.6; p < 0.001). CTCs were OS predictors in 108 patients with multiple metastases, including bone (p ≤ 0.0001) but not in 58 without bone metastasis (p = 0.411) and in 29 involving bone alone (p = 0.3552). In multivariate analysis, the CTCs, but not bone metastasis, remained as significant predictors of SG.
A meta-analysis of 36 CTC studies with 3094 CRC patients was published by Rahbari et al. (2010). The authors concluded that CTC detection in peripheral blood was an indicator of poor prognosis in patients with primary CRC (Rahbari et al. 2010).
Hofman et al. (2011) evaluated CTC detection, by CellSearch®, in lung cancer patients after surgical resection and correlated it with pathologic findings and clinical outcomes. They analyzed the blood of 208 patients with non-small cell lung cancer (NSCLC) with diverse histology before surgery and also blood of 39 healthy volunteers. Of these, 44% were in stage I, 25% in stage II, 28% in stage III, and 6% in stage IV. CTCs were detected in 37% of the NSCLC patients but there were no CTCs detected in the healthy individuals. There was no correlation between the presence of CTCs and the different stages, but equal counts or those above 50 CTCs were related to worse OS (p = 0.002) and PFS (p = 0.001) compared to counts less than 50 CTCs.
Krebs et al. (2011) studied 101 patients with NSCLC in stages III and IV without prior treatment, to determine the ability of CTCs to indicate the response to therapy to a standard cycle of chemotherapy. CTCs were evaluated by CellSearch® and their numbers were higher in patients with stage IV (n = 60) than in patients with stage IIIB (n = 27) and IIIA (n = 14), where no CTC was detected (n = 14). PFS was 6.8 vs. 2.4 months (p < 0.001) and OS was 8.1 vs. 4.3 months (p < 0.001) in patients with less than 5 CTCs compared with patients with 5 or more CTCs before chemotherapy. In multivariate analysis, the number of CTCs was the strongest predictor of OS (hazard ratio [HR] = 7.92; 95% CI: 2.85 to 22.01; p < 0.001) and the estimated HR increased with the second sample of CTC harvested after the first cycle of chemotherapy (HR = 15.65; 95% CI: 3.63 to 67.53; p < 0.001).
In concordance with this study, Punnoose et al. (2012) performed CTC collections before treatment of NSCLC and on days 14, 28 and 56 after the start of this study. The response ratings were evaluated by PET-CT on days 14, 28, and 56 after start of treatment. Patients who had partial or complete response by PET-CT showed greater reduction of CTCs from baseline (p = 0.014) as did patients with partial response in CT at day 56 (p = 0.019). Recently, Muinelo-Romay et al. (2014), used CellSearch® and found a statistically significant difference in PFS (8.5 versus 4.2 months; p = 0.016) before the second cycle of chemotherapy among patients who had CTCs drop to less than 2 CTCs/mL compared to those who maintained levels above that. Patients whose CTCs counts remained at or above the top after the first chemotherapy cycle showed greater radiographic progression rates compared to patients whose scores decreased after the first cycle.
Our group (Chinen et al. 2013) reported the case of a patient with NSCLC where two methods were used to detect CTCs: one method was antibody-based and similar to CellSearch®, while the other method was size based (ISET®, or the Isolation by Size of Tumor cells method, Rarecells, France). The levels of CTCs detected by ISET® had correlation with image exams and showed circulating tumor microemboli (CTM), which is known as a poor prognostic factor. In fact, the patient had disease progression just 1 month after the detection of CTM.
Some studies indicated that CTCs have the ability to form clusters of CTCs, named CTM, in the circulation . CTM were demonstrated in a variety of tumor types, providing pro-metastatic capabilities compared to solitary CTCs in circulation (Brandt et al. 1996; Hou et al. 2012). Hou et al. (2012) hypothesized that because CTM appear to lack apoptotic features, they may be more resistant to anoikis and hence have a survival advantage in circulation as compared to singular CTCs. Some authors believe that CTM, at least in some cases, result in clinically detectable metastases (Brandt et al. 1996; Hou et al. 2012; Caixeiro et al. 2014).
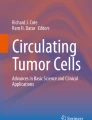
Recently, we observed the presence of CTM by ISET® in 43 patients with locally advanced head and neck squamous cell carcinoma (LAHNSCC), who had been treated with curative intention and evaluated as to their drug resistance and to their protein expression (excision repair cross-complementation 1 [ERCC1] and multidrug resistance protein 7 [MRP-7] related to cisplatin and taxane resistance, respectively) with PFS (De Oliveira et al. 2016). The median number of CTCs at baseline (before any treatment) was 2.0 CTCs/ml (0–8), and 27 of 43 patients had CTCs analyzed after treatment, with a median count of 3.0 CTCs/ml (0–12). Patients with CTC counts under the median had better PFS after treatment (11.66 versus 9.5 months; p = 0.132). The presence of CTM was strongly correlated with worse PFS after treatment; about 2 months after the beginning of treatment (first follow-up; p = 0,012), especially if ERCC1 (7.2 versus 17.9 months; p < 0.001) or MRP-7 staining (10.4 versus 17.4 months; p = 0.025) were positive in these CTM (Fig. 1.1). These results show that not only the presence of CTM but also their molecular features can help physicians to understand the biology of these diseases and their evolution, and to provide better treatment for their patients.

Immunostaining of CTMs (a) CTM from rectum cancer patient visualized with haematoxilin-eosin (HE) (×40) (b) CTM from LAHNSCC stained for ERCC1, visualized with DAB (3,3′-diaminobenzidine) and counterstained with HE (×20) (c) CTM from LAHNSCC stained for MRP-7, visualized with DAB (diaminobenzidine) and counterstained with HE (×40). Photomicrograps were taken using a light microscope (Research System Microscope BX61—Olympus, Tokyo, Japan) coupled to a digital camera (SC100—Olympus, Tokyo, Japan)
There a few studies about the role of CTCs in epithelial ovarian carcinoma (EOC), probably because the primary route of metastasis in this type of cancer is peritoneal spread in the abdominal cavity, with distant metastases occur in only about one-third of the patients (reviewed by Van Berckelaer et al. 2016). The few studies that exist, made with diverse methods, have shown the role of hematogenous spread in EOC and that CTC levels ≥2 CTC/7.5 mL (CellSearch®) or ≥1 tumor-associated transcript above threshold (Adnatest) is associated with poor PFS and OS (Poveda et al. 2011; Aktas et al. 2011; Kuhlmann et al. 2014). However, as for all solid tumors, the prognostic role of CTCs in EOC is dependent on the isolation and detection methods. Recently, we (Corassa et al. 2016, submitted) reported a case of a 19-year-old woman with advanced low-grade serous papillary adenocarcinoma that relapsed disease with no corresponding cancer antigen 125 (CA 125). CTCs were evaluated by ISET® method and compared with CA 125 levels and image exams. Although relapses were not correspondent to elevations of CA 125, they were related to CTC counts, which were proportional to disease relapse. After exposure to two different chemotherapy regimens, CA 125 could not detect uncontrolled disease, remaining low despite the ongoing symptoms and novel imaging findings. CTCs, on the other hand, if used in clinical practice, would be helpful in determining the quality of treatment decision-making, as their levels were related to clinical outcome. In a disease where the unique biomarkers have had controversial roles CTC monitoring seems promising (Fig. 1.2).

(a) CTC from a patient with epithelial ovarian cancer. CTC was visualized with haematoxilin-eosin (HE) (×40) (b) Leucocyte stained for CD45, visualized with DAB (3,3′-diaminobenzidine) and counterstained with HE (x40). Photomicrographs were taken using a light microscope (Research System Microscope BX61—Olympus, Tokyo, Japan) coupled to a digital camera (SC100—Olympus, Tokyo)
As for EOC, there are few studies with pancreatic cancer (PC), with a large variety of CTC platforms, limiting the balance among the studies. Kurihara et al. (2008) analyzed the CTC count in 26 patients with metastatic pancreatic cancer by CellSearch® System and correlated it with various clinical findings. They could not observe statistically significant differences in tumor size; blood invasion ; or splenic vein, portal vein, superior mesenteric artery, or vascular invasion. However, patients with CTC ≥1/7.5 ml serum showed higher CA 19.9 levels compared to the negative CTC (15,496 ± 22,572 U/ml versus 1452 ± 3800 U/ml; p < 0.05), demonstrating positive correlation between the number of CTCs and serum CA 19.9. They also found a correlation between CTC levels and OS (p < 0.001). Bidard et al. (2013) found the same results with another cohort. A meta-analysis recently published by Han et al. (2014) showed that patients who had any CTC in their blood had a lower PFS (p = 0.001) and OS (p < 0.001) compared to patients who did not present these cells. The results held for PFS, whether dividing the sample by the detection method of CTC by CellSearch® (p < .001) or by RT-PCR (p = 0.032). According to the author, these results indicate that the prognosis of patients with PC is associated with the presence of CTCs. Despite these results, limitations such as the small number of studies and patients, different methods of detection, and various treatments can lead to controversial results.
Although CTCs have been exhaustively explored in solid tumors, these cells can be recognized in the blood of patients with mesenchymal tumors. Our group was successful in demonstrating the possibility of ISET® in isolating CTCs from blood of patients with metastatic sarcoma. Before our study, others had detected CTCs in the blood of patients with different types of sarcoma (rhabdomyosarcoma, Ewing’s sarcoma, alveolar rhabdomyosarcoma, and neuroblastoma) by RT-PCR, which has its sensitivity questionable, as the presence leucocytes can mask the result. In our study, we performed spiking analyses with HT 1080 cell line derived from a human fibrosarcoma to assess the ability and sensitivity of the ISET® in isolating sarcoma cells from blood and observed that the ISET® practically does not lose tumor cells from sarcomas (Chinen et al. 2014).
The results of the first clinical trial with CTCs was reported in 2013. The clinical trial Southwest Oncology Group (SWOG) S0500 assessed the benefit of an early change in chemotherapy for patients with breast cancer with persistent increase of CTCs levels in the first follow-up after the start of first-line chemotherapy. A total of 595 patients were included: 123 of them had levels of CTCs persistently elevated on day 21 of treatment and were therefore randomized to continue the same treatment or switched to an alternative drug therapy, by their treating physician’s choice. What can be seen is that an early change to an alternative chemotherapy did not increase overall survival. Although CTCs were a potent prognostic factor, the lack of a survival benefit after switching from treatment based on high scores suggests that the early detection of relapse can be important when a more effective treatment is available. Changing an ineffective therapy to another that also is ineffective does not change the outcome. Instead, a change of the treatment based on the molecular characterization of CTC could be a promising approach (Smerage et al. 2014).
The molecular characterization of CTCs could potentially play a role in the development of new drugs, and changes their counts during treatment may help oncologists to evaluate the patient’s status. The COU-AA-301 (A Phase 3, Randomized, Double-Blind, Placebo-Controlled Study of Abiraterone Acetate (CB7630) Plus Prednisone in Patients with Metastatic Castration-Resistant Prostate Cancer Who Have Failed Docetaxel-Based Chemotherapy) study was the first phase III trial aimed to evaluate CTC counts as an outcome measure for new therapies for castration-resistant, metastatic prostate cancer in patients previously treated with docetaxel. This study demonstrated that abiraterone inhibition of the cytochrome P450 17 (CYP17) enzyme required for androgen synthesis significantly prolonged the OS of the patients. The conversion of CTC from unfavorable to favorable (using the cut-off ≥5 CTCs/7.5 mL) demonstrated a significant effect on OS, suggesting a key role of access to serially CTCs as a predictor of survival (Scher et al. 2015).
Bidard et al. (2014) published the first pooled analysis on clinical validity of CTC in 1944 patients with metastatic breast cancer diagnosed between 2003 and 2012 in 17 centers in Europe. This was the largest pooled analysis of the clinical utility of CTC count by CellSearch® system. As Cristofanilli et al. (2004), these authors showed that more than 5 CTCs/7.5 ml at baseline were associated with shorter PFS and OS. They also showed that the analysis of patients was improved by adding CTC counts at baseline to the clinicopathologic features, whereas CEA and cancer antigen 15–3 (CA15–3) levels at this point and during therapy did not add significant benefit.
Although he acknowledged methodology limitations, Cristofanilli (2014) states that a critical review of the data suggests that enumeration of CTCs provides a baseline therapeutic benefit ratio, independent of the treatment selected. Patients with indolent disease (≤5 CTCs) might derive benefit, such as better OS, from sequential standard treatments. Bidard et al. (2014) showed that longitudinal monitoring enabled early identification of patients with a refractory disease (no decrease <5 CTCs/7.5 mL or unchanged ≥5 CTCs/7.5 mL).
In prostate cancer, CTC levels have been measured in about 2000 patients. The collective data show that CTC measurements have potential to identify patients with primary resistance 4–8 weeks after treatment initiation, making it possible to monitor treatment efficacy, study drug target interactions, and identify mechanisms of resistance at an individual level (Mehra et al. 2015).
After conducting this review of the history of research on CTCs, we observed that the discovery of their existence mainly involved metastatic cancer. In recent years research addressing non-metastatic tumors suggests that CTCs may have promise for early diagnosis of primary lesions.
1.2 CTCs as Prognostic Factors in Advanced Stages of Disease
Studies have been done with non-metastatic cancer and the role of CTCs in prognosis also seems to be as important as it is in metastatic disease. In the study of Magni et al. (2014), 16 of 90 patients (19%) had CTCs ≥1 at the outset (t0) and a reduction in CTC number in cases of objective remissions. The proportion of patients with CTCs ≥1 decreased over time as the therapeutic course proceeded. Increasing CTC detection rate by enhancing the available laboratory tests and achieving better patient characterization would be productive (Magni et al. 2014).
Nesteruk et al. (2014) analyzed the CTC prevalence in 162 patients with rectal cancer after preoperative short-term radiotherapy. CTCs were evaluated by RT-PCR, based on expression of CEA, CK20, and/or cancer stem cells marker CD133 (CEA/CK20/CD133). CTC detection 7 days after surgery was a prognostic factor for local recurrence (p = 0.006). However, CTC detected preoperatively and after 24 hours of resection was not. There was a significant relationship between the presence of lymph node metastasis (positive node 1–2 [pN1–2]) and CTC prevalence after 24 hours of the surgery. These results indicate that in these patients with advanced rectal disease, preoperative sampling was not significant for prognosis.
In the study of Murray et al. (2015), primary CTC counts are said to have a role in colorectal cancer screening. But analyzing primary CTCs - detected before surgical removal – did not predict clinicopathologic features of the primary tumor. However, the same group described the secondary CTC levels as associated with these features after surgical removal, and suggested that this secondary count may be important in identifying patients at high risk of relapse.
Hinz et al. (2015) analyzed the response after chemoradiation (RCTX) in patients with rectal cancer with locally advanced disease and found that responders had a lower incidence of CTCs compared to non-responders, which might be a reflection of effective systemic and local treatment prior to surgery. They also found no correlation between CTCs and tumor stage, which is in agreement with Tsai et al. (2016).
Using immunofluorescence and immunohistochemistry techniques, Hong et al. (2016) isolated and identified CTCs in 100% of (29) patients with early (non-metastatic) breast cancer , indicating that this procedure allowed detection of these cells with greater accuracy, sensitivity, and specificity. In addition, they demonstrated in situ “naked eye” identification of the captured cancer cells via a simple colorimetric immunoassay.
The use of CTC in non-metastatic colorectal cancer requires very sensitive and specific detection methods. An international consensus on the assessment of detection method and markers needs to be finalized before incorporating CTC detection into risk stratification in the clinical setting (Thorsteinsson and Jess 2011).
1.3 CTCs as a Predictor of Drug Resistance
It is well described that cancer is a heterogeneous disease composed of various differing cell clones in different patients, with each clone having different characteristics, including metabolism, mutations , gene regulation, gene expression, and protein translation as well as signaling pathway alterations (Fearon and Vogelstein 1990; Gerlinger et al. 2012). These different characteristics reflect the natural history of the disease, resulting in different tumor behavior, and therefore, tumor prognosis , depending on how the neoplastic cells respond to treatment. This theory can explain why patients with the same tumor localization, histopathological classification, and stage have different outcomes and treatment responses (Marusyk and Polyak 2010).
Advanced and metastatic solid tumors are commonly treated with chemotherapy, one of the most aggressive types of treatment. Because its lack of specificity ensures that it will affect many different kinds of cancer cells. Although chemotherapy has high potential activity against tumor cells, the toxicity of these drugs on normal growing cells is a significant problem (Phillips et al. 2001; Roden and George 2002). Even with targeted therapies, resistance mechanisms as well as toxic side effects occur frequently (Holohan et al. 2013). The pharmacokinetics and tolerability of the chemotherapy agents can also differ in cancer patients, and many patient characteristics have to be taken into account before a specific chemotherapy treatment is selected.
Resistance to chemotherapy is a very common issue in cancer (Haber et al. 2011). It can be an early or late event, which is attributed to intrinsic and acquired resistance, respectively (Holohan et al. 2013). When chemotherapy agents affect their target cancer cells, the sensitive cells undergo cell cycle arrest and as consequence the tumors eventually show shrinkage. But resistant clones in the tumor can persist and grow again, increasing the tumor mass, with cancer cells with characteristics completely different from the previous ones. The process of mutation and deregulation in gene expression is continuous. Chemotherapy can also lead to such modulations, making it difficult for clinicians to choose the best sequence of treatment to control tumor growth (Holohan et al. 2013; Kuczynski et al. 2013).
There are some genes and proteins that have been described as factors that contribute to resistance or to the responses to chemotherapy treatment, by transporting drugs inside or outside of cells, repairing DNA damage, and/or evading cell death (Holohan et al. 2013).
Acquired chemo-resistance is one of the recurrent issues in almost all tumors after the exposition to chemotherapy. Many types of cancer cells have plasma membrane proteins that transport chemicals and toxins out of the cytoplasm. These proteins are mainly from the multi-drug resistance (MDR) family and have been widely studied (Flens et al. 1996; Cui et al. 1999; Doyle and Ross 2003). Their functions are ATP dependent, and they act as efflux pumps, with different membrane proteins functioning to transport specific classes of drugs.
CTCs shed by the both primary and metastatic cancers during tumor formation and progression are now considered to be a real-time “liquid biopsy ” reflecting the disease complexity (Salvianti et al. 2016). Thus far, studies on CTCs have been focused on their prognostic significance, their utility for real-time monitoring of therapies, the identification of therapeutic and resistance targets, and understanding the process of metastasis (Salvianti et al. 2016).
CTCs can be considered pharmacological markers, and their analysis may allow researchers to (a) provide proof of the mechanisms of action of a drug; (b) select optimal doses and scheduling of antineoplastic drug administration; (c) gain an understanding of both the therapeutic and resistance mechanisms of anti-cancer drugs; (d) design rational combination therapies; and (e) predict treatment outcomes, as postulated for pharmacodynamic biomarkers by Sarker and Workman (2007) (reviewed by Devriese et al. 2011). Recently, it has been postulated that molecular characterization of CTCs is key for increasing the diagnostic specificity of CTC assays and investigate therapeutic targets and their downstream pathways (Gasch et al. 2013).
CTCs have been demonstrated to be efficient markers for providing tumor information, presenting predictive markers, optimizing choices of therapeutic strategies, and thus opening new perspectives to achieve personalized medicine (Gazzaniga et al. 2010; Gradilone et al. 2011a, b; Abdallah et al. 2015, 2016). Some MDR-related markers were successfully derived from CTCs, correlating with drug resistance (MRP1, MRP2, MRP4, MRP5, and MRP7). Gazzaniga and colleagues (2010) performed a drug-resistance profile of CTCs from 105 patients with epithelial tumors (bladder, colorectal, breast, gastric, urothelial, ovarian, esophageal, head and neck cancers, and NSCLC), who received adjuvant or palliative chemotherapy by analyzing messenger RNA expression. They analyzed mRNA from CTCs looking for drug transporters (MRP1, MRP2, MRP4, MRP5, MRP7, human equilibrative nucleoside transporter [hENT] and deoxycytidine kinase [dCK]) as markers of resistance. They found presence of CTCs by the CELLection™ Dynabead® method in 51% of samples and the drug resistance profiles were correlated with DFS (p = 0.001) and time to progression (TTP; p = 0.001) (for adjuvant and metastatic settings, respectively), and predicted the treatment resistance in 98% of the cases. The same group (Gradilone et al. 2011a), using the same principle, was able to evaluate MRP1 and MRP2 messenger RNA expression in CTCs from metastatic breast cancer (mBC) patients treated with conventional anthracyclines or nonpegylated liposomal doxorubicin. They observed that patients treated with conventional anthracyclines showing CTCs expressing MRP1 and MRP2 had a significant shorter progression-free survival (PFS; p < 0.005).
In our study (Abdallah et al. 2016), the same results were observed working with MRP1 in metastatic colorectal cancer (mCRC). MRP1 expression was linked to short PFS in mCRC patients when it was found expressed in CTCs in relation to negative ones (p = 0.003). This relation of MRP-1 to poor PFS was not observed in primary or metastatic tissues.
Another interesting result from Gradilone et al. (2011b) involved MRPs, human epidermal growth factor receptor 2 (HER-2/neu), estrogen receptor α (ERα), and aldehyde dehydrogenase 1 (ALDH1) expression in CTCs from mBC patients. Patients who had CTCs expressing two or more MRPs had shorter PFS. Moreover, the expression of ALDH1 (a stemness marker) was statistically correlated with the number of MRPs. This suggests potential retention of stem cell properties within the MRPs-expressing CTCs group, therefore resisting chemotherapeutic treatment, and becoming more invasive and with high migratory capabilities.
The expression of stemness and epithelial-mesenchymal transition (EMT)-related genes detected in CTCs seem to have a crucial role in chemo-resistance in several tumors, such as castration-resistant prostatic cancers compared to castration-sensitive ones (Chen et al. 2013), and breast cancer (Mego et al. 2012; Nadal et al. 2013). These two cellular conditions are correlated. Studies have shown that stem cell properties can be acquired during the EMT process (Mani et al. 2008; Morel et al. 2008).
Continuing with well-known markers of drug resistance, our group (Abdallah et al. 2015) compared the expression of thymidylate synthase (TYMS), an enzyme involved in the process of metabolism of 5-fluorouracil (5-FU) in primary tumors (mCRC), CTCs, and metastatic tissue. TYMS is constitutively expressed in leucocytes and is found with augmented expression in some tumors, and confers resistance to the effects of 5-FU (Popat et al. 2004). Surprisingly, the expression of TYMS in CTCs (analyzed by immunocytochemistry ) but not in primary tumors or in metastatic tissue, was associated with rapid disease progression. We observed that the expression of TYMS was statistically associated with high CTC’s levels in the blood of mCRC patients.
Studies performing analysis of molecular profiles and molecular markers like CEA, epidermal growth factor receptor (EGFR) , Kirsten rat sarcoma viral oncogene homolog (KRAS), v-rapidly accelerated fibrosarcoma (RAF) murine sarcoma viral oncogene homolog B (BRAF) , vascular endothelial growth factor (VEGF), adenomatous polyposis coli (APC), and tumor protein p53 (TP-53) in the CTCs have raised hope that personalized treatments can be more effective and less aggressive (Fina et al. 2015; Buim et al. 2015; Sawada et al. 2016; Bredemeier et al. 2016; Huang et al. 2016).
Increasing attention has been given in recent years to CTCs from castration-resistant prostate cancer (CRPC) patients. CTC counts were reported to predict poor overall survival (OS) in patients with progressive CRPC starting a new line of therapy (de Bono et al. 2008). Both CTC count and CTC characterization were reported in patients with androgen-receptor splice variant 7 messenger RNA (AR-V7) in CTCs, mainly because it was correlated with resistance to enzalutamide or abiraterone. Mutations in androgen receptor genes were reported in CTCs (Jiang et al. 2010). Antonarakis and colleagues (2014) were able to detect AR-V7 positivity in CTCs from metastatic CRPC patients and to significantly associate these results with low prostate-specific antigen (PSA) response rates, PSA PFS, clinical or radiographic PFS, and OS in both arms, whose received enzalutamide and abiraterone.
ERCC1 is a protein involved in nucleotide excision repair pathway, mainly repairing helix-distorting DNA damage induced by ultraviolet light or electrophilic compounds, such as cisplatin (Houtsmuller et al. 1999). ERCC1 was already evaluated in CTCs from breast (Somlo et al. 2011), NSCLC (Das et al. 2012) and ovarian cancer (Kuhlmann et al. 2014). Somlo and colleagues (2011) found weak correlation of expression of ERCC1 among CTCs, primary tumors and metastases. Das et al. (2012) correlated lack of ERCC1 expression in CTCs with better PFS (p < 0.02, HR: 4.2). Ovarian cancer patients whose CTCs had ERCC1 expression had worse PFS and OS (p = 0.02 and p = 0.009, respectively) (Kuhlmann et al. 2014).
Hoshimoto and colleagues (2012a) performed CTC (blood) analysis by multimarker RT-quantitative PCR assay (melanoma-specific proteins: melanoma antigen recognized by T cells 1 [MART-1], melanoma-associated antigen 3 [MAGE-A3], and GalNac-T) in 331 patients with melanoma with sentinel lymph node (SLN) metastases after complete metastasis resection. They found that patients with two or more positive biomarkers had worse distant metastasis DFS (HR = 2.13, p = 0.009) and reduced recurrence-free survival (HR = 1.70, p = 0.046) and melanoma-specific survival (HR = 1.88, p = 0.043) by multivariable analysis, suggesting they are good biomarkers to stratify patients with respect to additional aggressive adjuvant therapy.
Regarding prognosis , CTC measurements have demonstrated to be useful in paired analysis to primary tumors. Ilie and colleagues (2012) were able to detect in CTCs isolated from 87 lung cancer patients by ISET® technology, anaplastic lymphoma kinase (ALK)-rearrangement by fluorescence in situ hybridization (FISH), and immunocytochemistry , demonstrating consistent results when compared with matched primary tumors. Similarly, Pailler and colleagues (2013) found 18 of 18 NSCLC ALK-positive patients also positive in CTCs. However, among the 14 NSCLC ALK-negative patients, they found 10 patients with at least 1 ALK-positive CTC. This is an important result, because lung biopsies are difficult and obtaining enough cellular content to provide for a definitive tissue diagnosis coveys significant risk.
BRAF mutations (V600E) in circulating melanoma cells (CMCs) can be identified by immunocytochemistry using anti-VE1 antibodies. This can reach a high specificity and sensitivity compared with mutation status for corresponding primary tumors (by pyrosequencing and immunohistochemistry), making it possible to monitor patients focusing on a targeted therapy (Hofman et al. 2013). We (Buim et al. 2015) also observed an interesting level of correlation between the primary tumor and CTCs from mCRC patients in relation to levels of KRAS mutations (71%), similar to results found in other studies (Mostert et al. 2013; Fabbri et al. 2013; Gasch et al. 2013; Raimondi et al. 2014). Kalikaki et al. (2014) evaluated CTCs from 31 mCRC patients (14 primary tumors with mutant KRAS and 17 primary tumors wild-type KRAS). CTCs were isolated, counted, and captured for further DNA analysis for KRAS status evaluation. The blood collections ranged from one to four, and CTC ranged from 0 to 865/7.5 mL of blood. It was observed that: (a) some patients had the same variations of mutations between CTC and tumor: (b) some patients with mutations in the primary tumor lost the mutation in CTCs over the course of treatment as well as returning to the prior mutation status, and (c) patients with wild-type tumors and mutations in CTC. They were able to find similar tumor mutation variants in only 3 CTCs from patients and by contrast, they did not find mutations in 865 CTCs from patients with mutations in the primary tumor. This shows the importance of follow-up of such patients by CTC analysis as well as for genotypic changes, in order to change treatments as needed in a timely fashion.
HER-2 overexpression and amplification in breast cancer is an important prognostic and predictive marker. It predicts a good response to HER-2 inhibitors (trastuzumab and lapatinib) in both adjuvant and metastatic lesions (Paik et al. 2008). HER-2 was observed in CTCs from breast cancer patients by laser microdissection (Pinzani et al. 2006). They could compare the DNA of matched CTCs and primary tumors from 7 CTC+ cases and found a good correlation of HER-2 amplification in these two sites (R = 0.918; p < 0.01). This result could represent an advance in the follow-up of these patients in order to evaluate the status of HER-2 by CTC counts, reflecting the primary tumor as well as the response to trastuzumab over time. Interestingly, Gasch and colleagues (2016) demonstrated the feasibility in detecting CTCs with strong HER-2 positivity from mBC HER-2-negative patients. Furthermore, they found mutations in phosphatidylinositol 4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA) in 12 of 33 patients by micromanipulation, whole genome amplification , and Sanger sequencing of their CTCs. These results move us toward use of personalized mBC treatment, giving a better understanding of some mechanisms to HER-2 blockade resistance by single cell analysis .
Recently, much effort has been expended to assess proteins with potential predictive and therapeutic interest in CTCs. Some examples follow: B-cell lymphoma 2 (Bcl-2) (Smerage et al. 2013): Kiel-67 (Ki-67) (Paoletti et al. 2015): γ-H2A histone family, member X (γ-H2AX) (Garcia-Villa et al. 2012): programmed death-ligand 1 (PDL1) (Mazel et al. 2015; Satelli et al. 2016): and folate receptors, mainly in NSCLC (Yu et al. 2013; Lou et al. 2013; Chen et al. 2015).
Finally, CTCs can be also expanded and cultivated in vitro, allowing molecular characterization , and may even provide drug sensitivity data, to select patients who will benefit from specific drug combinations (Yu et al. 2014; Cayrefourcq et al. 2015).
In this brief summary, we have addressed role and feasibility of CTCs as a mirror of tumor signatures and identified them as a potentially valuable tool to monitor the response to treatment. Further study should yield increased benefits over time. The contents of Table 1.1 show an overview of studies with drug resistance gene detection in CTCs and their relation with clinical outcome. Beyond the quantification of CTCs, their molecular analysis can provide clinicians insights into the pattern of a patient’s disease and provide tools for better management and treatment.
With the advance of techniques for detection and purification of CTCs, it should be possible to develop better individualized patient care, at different time-points, thus continually re-evaluating a cancer throughout the course of treatment. Furthermore, studies with larger numbers of patients should be performed in order to evaluate the accuracy and the substantial clinical gains that molecular analysis of CTCs can provide for clinical cancer therapy.
1.4 CTCs as Prognostic Factors in Early Stages of Cancer
It has been demonstrated in several clinical studies that the presence of malignant cells in the blood is associated with a poor prognosis , even in the context of early-stage disease. Lucci et al. (2012) carried out a prospective study involving 302 women with early-stage breast cancer . They observed, using the CellSearch® system to isolate CTCs, that 73 of 302 (24%) patients had ≥1 CTCs/7.5 mL of blood before surgery. These patients had poor PFS (log-rank p = 0.005; HR = 4.62, 95% CI 1.79–11.9) and OS (log-rank p = 0.01; HR = 4.04, CI 1.28–12.8). Although this study showed the prognostic value of initial CTCs in malignant disease, the CTCs were not monitored during the follow-up period nor was minimal residual disease analyzed. Prospective studies with standard procedures to detect CTCs, with well-established inclusion criteria, are currently needed (Hayes and Paoletti 2013).
CTC detection in non-metastatic breast cancer is more difficult because the cells occur at a lower frequency. Pierga et al. (2008) found CTC ≥1/7.5 ml in 23% of 97 patients before administering neoadjuvant chemotherapy and in 17% of 86 patients after neoadjuvant chemotherapy. The detection of CTC ≥1/7.5 ml prior to neoadjuvant chemotherapy, after neoadjuvant chemotherapy, or at both time points in the above study was associated with worse distant metastasis-free and OS at a median follow-up period of 36 months (Bidard et al. 2010). Moreover, it was associated to poor clinical outcome, especially in patients with estrogen receptor (ER)-negative, triple negative, and HER2-positive cancer (Ignatiadis et al. 2007). When the CTC detection occurs before and after neoadjuvant chemotherapy, it appears that the detection of ≥1 CTCs/7.5 ml of blood can accurately predict the poor overall survival of patients (Pierga et al. 2008).
Studies demonstrating CTC detection in non-metastatic CRC require specific and sensitive methods, because of the low incidence of these cells in the initial stage of the tumor, as in breast cancer . The presence of CTCs in the peripheral blood of CRC patients is a potential marker of poor DFS (Thorsteinsson and Jess 2011).
Wong et al. (2009) examined 101 patients with tumor, node, metastasis (TNM) stage I e III CRC, detecting CTC with a gastrointestinal-specific CK20. Sixty-two of 101 patients were followed for a period of 24 months and the association between preoperative elevated CK20 and recurrence was found to be highly significant (p < 0.001). The CTCs were an independent prognostic factor of survival (p < 0.005) in a multivariate regression analysis including TNM-stage, lymph node status, age, sex, tumor stage and degree of differentiation. In accordance, Iinuma et al. (2006) was also able to demonstrate poor DFS for CRC patients with preoperatively elevated CTC using a RT-PCR based method.
Allen-Mersh et al. (2007) demonstrated that poor DFS was associated with the occurrence of CEA or CK20 24 hours postoperatively (p < 0.001). Uen et al. (2008) used a multi-marker membrane array method to detect CTC in 438 patients with TNM stage I e III colorectal cancer. Presence of all four markers (human telomerase reverse transcriptase [hTERT], CK19, CK20, and CEA) was considered as a positive result for CTC. The authors demonstrated that patients with persistent presence of CTC after surgery had a significantly poorer relapse-free survival compared with patients without CTC (p < 0.001).
The CTCs analysis may also be useful for patients with melanoma. The detection of CTCs in these patients may help for determining prognosis . Hoshimoto et al. (2012a) reviewed the clinical usefulness of an RT-qPCR MultiMarker (MART-1, MAGE-A3, and GalNAc-T) for detection of CTCs in 331 melanoma patients who were clinically free of disease after lymphadenectomy. The individual detection of CTCs ranged from 13.4 to 17.5% and there was no stated association of CTC with known clinical or pathological prognostic variables. However, the presence of two or more positive biomarkers was significantly associated with distant metastasis and recurrence-free survival.
Lowes et al. (2012) were able to detect CTCs in patients with early stage prostate cancer and suggested the possibility that the reduction after treatment of CTC levels may be indicative of response to radiotherapy.
The main advantage of CTC analysis in early stages is based on the ease of obtaining a “liquid biopsy ” and thus being able to monitor patients over the course of the disease, providing valuable information about the very early assessment of treatment effectiveness and helping towards establishing individualized therapies that will improve the efficiency with less cost and fewer side effects for cancer patients.
More studies on the molecular characterization of CTCs in early stage may provide important information for the identification of therapeutic targets and understand resistance to therapies (Lianidou et al. 2013). According to Lianidou et al. (2014) CTCs characterization is promising in combination with sequencing technologies that will allow the elucidation of molecular pathways in these cells, generating new molecular therapies. The real-time monitoring of therapy in early stages will have a major impact on personalized medicine in many types of cancers, allowing the choice of more effective and less toxic therapies.
1.5 Role of CTCs in Minimal Residual Disease
Minimal residual disease (MRD) has usually been studied after surgery and treatment with targeted therapies (Maheswaran et al. 2008). Defined as micrometastatic cells undetectable by laboratory tests and conventional imaging, some MRD “substitutes” are detected in the peripheral blood (CTCs) and bone marrow (disseminated tumor cells [DTCs]). The detection of CTCs and DTCs leads to new strategies for personalized treatment and therapeutic agents for breast cancer , and brings new knowledge of tumor biology (Riethdorf and Pantel 2010).
DTC and CTC detection is a challenge, and different enrichment techniques are applied for each. The techniques are based on physical properties or immunological characteristics of these cells. Braun et al. (2005) detected micrometastases in 30.6% of the patients with stage I, II, or III breast cancer . The presence of micrometastases was a significant prognostic factor with respect to poor OS, breast-cancer-specific survival, poor DFS, and distant-DFS during a 10-year observation period. Micrometastasis was an independent predictor of a poor outcome. In the univariate subgroup analysis, breast-cancer-specific survival among patients with micrometastasis was significantly shortened (p < 0.001 for all comparisons) among those receiving adjuvant endocrine treatment (mortality ratio, 3.22) or cytotoxic therapy (mortality ratio, 2.32) and among patients who had tumors no larger than 2 cm in diameter without lymph-node metastasis and did not receive systemic adjuvant therapy (mortality ratio, 3.65).
Several authors performed studies comparing CTCs and DTCs and demonstrated correlation between them (Bidard et al. 2014; Goldkorn et al. 2014). Furthermore, given that blood is more easily obtained than bone marrow, CTCs are now being widely used as surrogate markers for DTCs.
Kasimir-Bauer et al. (2012), detected CTCs in 97 of 502 (19%) patients and DTCs in 107 of 502 (21%) patients, showing the value of CTCs and DTCs, despite the detection method for CTCs not being as efficient for identifying circulating tumor cells undergoing EMT .
At the time of initial diagnosis, patients often have DTCs (at bone marrow) or even undetected micrometastasis. The long dormancy period of MRD offers an opportunity to develop agents that can eradicate clinically relevant metastatic sites (Wan et al. 2013). In vivo experiments suggest that DTCs from bone marrow (BM) can be turned into CTCs and return to the primary tumor, a process called “tumor self-seeding,” leading to aggressive metastatic variants (Kim et al. 2009).
Gao et al. (2016) adopted an integrated cellular and molecular approach of subtraction enrichment and immunostaining-fluorescence in situ hybridization (SE-iFISH (SE-iFISH, to investigate the chromosome 8 polyploidy, found in many solid tumors) to detect CTCs in the peripheral blood of patients with glioma, a disease considered restricted to brain, as very few cases with extracranial metastases has been observed (Fonkem et al. 2011; Kalokhe et al. 2012). However, the idea that brain glioma cells never enter the bloodstream has been put in doubt recently. Müller et al. (2014) were the first to find CTCs in the peripheral blood of patients with glioblastoma multiform (GBM) and declared that CTC is the “intrinsic property” of GBM biology. However, it is important to consider the methodological deficiencies in previous studies, the low incidence of CTCs and the fact that results were exclusively limited to high-grade gliomas (Gao et al. 2016). So, these authors investigated 31 patients with 7 different pathologic features (grade II-IV) of primary gliomas. They identified CTCs in 24 of 31 (77%) patients with no statistical difference of CTC incidence/count in different pathological subtypes or World Health Organization (WHO) grades of glioma. Clinical data demonstrate that CTCs , to some extent, was superior to magnetic resonance imaging (MRI) in monitoring the treatment response and differentiating radionecrosis from recurrence of glioma. The authors propose the use of CTCs to monitor the microenvironment of gliomas dynamically, as a complement to radiographic imaging.
The role of CTCs in micrometastatic disease is not completely understood, as CTCs compose a very heterogeneous population of cells, Meng et al. (2004) showed that the presence of documented micrometastases by CTCs detection does not imply absolute risk of subsequent recurrence. These authors reported that 13 of 36 (36%) women who had no evidence of clinical disease 7–22 years after mastectomy had detectable aneusomic CTCs. In other study (Wiedswang et al. 2004) it was reported that 53 of 356 (15%) patients who were disease-free after 3 years of follow-up had bone marrow micrometastases. After a follow-up of about 3 years, only 21% of these patients with documented persistent bone marrow metastases relapsed.
Studies suggest that simply finding cells using high sensitivity assays may not have clinical implications and that future studies using next-generation capture devices need to be planned carefully, taking into consideration clinical outcomes and not just diagnostic comparisons with the current gold standard. Molecular characterization of captured CTCs might provide insight into the future clinical behavior of the cancer, especially in relation to targeted therapy. However, it is not clear that CTCs actually reflect the biology of the tissue-based cancer. It is possible that the detected cells identified by currently available techniques are merely those that were shed and are only the “tip of the iceberg”, as stained by Hayes and Paoletti (2013). Or, these are terminally differentiated cells that reflect the presence of more malignant cancer stem cells that are not captured by CellSearch®, (Hayes and Paoletti 2013), which can be captured by other antibody independent methods.
1.6 Role of CTCs in Screening and Diagnosis
Kohn and Liotta (1995) published a study showing that in situ breast cancer is a clonal precursor of breast carcinoma and that tumor invasion starts 5–10 years before cancer diagnosis. According to Paterlini-Bréchot (2014) , this raises the hypothesis that it should be possible to detect cancer at a pre-diagnostic stage through the very sensitive detection techniques for “sentinel” cancer cells in blood.
More recently, Ilie et al. (2014) collected blood samples from 168 individuals with chronic obstructive pulmonary disease (COPD), a disease that typically results from long-term cigarette smoking, causing breakdown of lung tissues, and an increased risk of lung cancer. They also studied 77 control subjects. They looked for CTCs by ISET® in the blood of all 245 subjects, to investigate CTCs as a possible new marker for early lung cancer. They also obtained annual CT-scans in the COPD (68.6%) and control subjects (31.4%), none of whom were known to have lung cancer. CTCs were identified by cytomorphological analysis and characterized by expression of epithelial and mesenchymal markers. CTCs were detected during the study in 5 of the COPD patients (3%). The annual evaluation of the CTC-positive COPD patients by CT-scan screening then detected lung nodules 1–4 years later and led to surgical resection of early-stage lung cancers. Follow-up of these 5 cancer patients (by CT-scan and ISET®) 12 months after surgery showed no tumor recurrence. CTCs detected in COPD patients had a heterogeneous expression of epithelial and mesenchymal markers. No CTCs were detected in the 77 control subjects.
So, maybe, the utility of CTCs will not be only for follow-up of patients with well-known disease but also prove to be useful for screening of patients with family history of cancer, or with underlying diseases that can predispose to the development of cancers. With standardized protocols, we may be able to develop a practical tool for the early detection and prevention of untoward outcomes in this difficult, harmful, and deadly disease.
1.7 Conclusions
Raimondi et al. (2014) started his paper with a statement: “If one could translate the “Divina Commedia” into a scientific language and try to imagine where Dante Alighieri would have placed circulating tumor cells (CTCs), the answer would be, without a doubt, “in limbo”. These authors affirm that despite the increasing scientific evidence collected in the last decade, “which is enough to avert the danger of Hell,” the use of CTC in clinical practice is still “far from the light that suits to Heaven.” They support their idea based on disappointing results obtained in the Phase III SWOG S0500 trial, concluding that CTCs are not a good marker to help to decide when to choose chemotherapy in women with metastatic breast cancer . They wrote a very interesting paper arguing that CTCs are “not in heaven yet.”
These authors also discuss the CellSearch® system, which is the most used method to isolate CTCs in clinical trials. It was cleared by the FDA in 2004, but its clinical utility is still to be fully demonstrated. To date, no large prospective studies using CellSearch® have shown any predictive value for CTCs, and their clinical utility is therefore limited . The effect of the type of treatment on the prognostic and predictive value of CTCs has not been directly evaluated, and the ability of targeted therapies to modify the predictive value of CTC count has not yet been demonstrated. CellSearch® is based on the capture of cells expressing an epithelial antigen, without morphological verification of the neoplastic nature of the captured cells. This is a weakness of the test, because it therefore can misidentify nonmalignant circulating epithelial cells as CTCs. In addition, CellSearch® is unable to detect cells that have undergone epithelial mesenchymal transition, which explains the absence of CTCs in the subset of patients with metastatic cancer with documented progression of the disease in many clinical trials (Paterlini-Bréchot and Benali 2007; Pantel et al. 2012; Hofman et al. 2014, 2016).
Alternatively, there are investigators, who argue that the prognostic significance of CTC counts should not be ignored, even when the system used to evaluate CTCs—the CellSearch® System-has well known limitations (Kang and Pantel 2013; Paterlini-Bréchot 2014; Hofman and Popper 2016). Thus, CTC evaluations are included as a biomarker in more than 400 clinical trials using various assays (see Table 1.2).
We believe that CTCs studies have potential to help physicians use a more rational approach for management of both metastatic and non-metastatic tumors, reflecting solid tissue or mesenchymal cancers. However, we will need to develop a standard system and protocol in order to be able to use CTCs in routine clinical settings. There are systems that provide for CTC isolation in a marker independent manner, by cytopathological analysis, which seems promising in capturing all malignant cells.
Even considering their weak points, CTCs are one of the most promising and versatile biomarkers in translational oncology (Mehra et al. 2015). As highlighted by Kang and Pantel (2013), viewing CTCs as a “liquid biopsy ” opens new opportunities for genotyping and phenotyping micrometastatic cells derived from various distant sites, which, if adequately developed, may provide clinical oncology with more complete pictures of the evolution of cancers compared to those provided by biopsies of single metastatic sites.
References
Abdallah EA, Fanelli MF, Buim ME et al (2015) Thymidylate synthase expression in circulating tumor cells: a new tool to predict 5-fluorouracil resistance in metastatic colorectal cancer patients. Int J Cancer 137(6):1397–1405
Abdallah EA, Fanelli MF, Souza E, Silva V et al (2016) MRP1 expression in CTCs confers resistance to irinotecan-based chemotherapy in metastatic colorectal cancer. Int J Cancer 139(4):890–898
Aktas B, Kasimir-Bauer S, Heubner M et al (2011) Molecular profiling and prognostic relevance of circulating tumor cells in the blood of ovarian cancer patients at primary diagnosis and after platinum-based chemotherapy. Int J Gynecol Cancer 21(5):822–830
Allen-Mersh TG, McCullough TK, Patel H et al (2007) Role of circulating tumour cells in predicting recurrence after excision of primary colorectal carcinoma. Br J Surg 94(1):96–105
Antonarakis ES, Lu C, Wang H, Luber B et al (2014) AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med 371(11):1028–1038
Ashworth TR (1869) A case of cancer in which cells similar to those in the tumours were seen in the blood after death. Med J Aust 14:146–147
Azim HA Jr, Rothé F, Aura CM et al (2013) Circulating tumor cells and response to neoadjuvant paclitaxel and HER2-targeted therapy: a sub-study from the NeoALTTO phase III trial. Breast 22(6):1060–1065
Behbakht K, Sill MW, Darcy KM et al (2011) Phase II trial of the mTOR inhibitor, temsirolimus and evaluation of circulating tumor cells and tumor biomarkers in persistent and recurrent epithelial ovarian and primary peritoneal malignancies: a Gynecologic Oncology Group study. Gynecol Oncol 123(1):19–26
Bertucci F, Fekih M, Autret A et al (2016) Bevacizumab plus neoadjuvant chemotherapy in patients with HER2-negative inflammatory breast cancer (BEVERLY-1): a multicentre, single-arm, phase 2 study. Lancet Oncol 17(5):600–611
Bidard FC, Mathiot C, Delaloge S et al (2010) Single circulating tumor cell detection and overall survival in nonmetastatic breast cancer. Ann Oncol 21(4):729–733
Bidard FC, Huguet F, Louvet C et al (2013) Circulating tumor cells in locally advanced pancreatic adenocarcinoma: the ancillary CirCe 07 study to the LAP 07 trial. Ann Oncol 24(8):2057–2061
Bidard FC, Peeters DJ, Fehm T et al (2014) Clinical validity of circulating tumour cells in patients with metastatic breast cancer: a pooled analysis of individual patient data. Lancet Oncol 15(4):406–414
Brandt B, Junker R, Griwatz C et al (1996) Isolation of prostate-derived single cells and cell clusters from human peripheral blood. Cancer Res 56(20):4556–4561
Braun S, Vogl FD, Naume B et al (2005) A pooled analysis of bone marrow micrometastasis in breast cancer. N Engl J Med 353:793–802
Bredemeier M, Edimiris P, Tewes M et al (2016) Establishmernt of a multimarker qPCR panel for the molecular characterization of circulating tumor cells in blood samples of metastatic breast cancer patients during the course of palliative treatment. Oncotarget 7:41677–41690
Buim ME, Fanelli MF, Souza VS et al (2015) Detection of KRAS mutations in circulating tumor cells from patients with metastatic colorectal cancer. Cancer Biol Ther 16(9):1289–1295
Caixeiro NJ, Kienzle N, Lim SH et al (2014) Circulating tumour cells—a bona fide cause of metastatic cancer. Cancer Metastasis Rev 33(2–3):747–756
Cayrefourcq L, Mazard T, Joosse S et al (2015) Establishment and characterization of a cell line from human circulating colon cancer cells. Cancer Res 75(5):892–901
Chen CL, Mahalingam D, Osmulski P et al (2013) Single-cell analysis of circulating tumor cells identifies cumulative expression patterns of EMT-related genes in metastatic prostate cancer. Prostate 73(8):813–826
Chen X, Zhou F, Li X et al (2015) Folate receptor-positive circulating tumor cell detected by LT-PCR-based method as a diagnostic biomarker for non-small-cell lung cancer. J Thorac Oncol 10(8):1163–1171
Chinen LT, de Carvalho FM, Rocha BM et al (2013) Cytokeratin-based CTC counting unrelated to clinical follow-up. J Thorac Dis 5(5):593–599
Chinen LT, Mello CA, Abdallah EA et al (2014) Isolation, detection, and immunomorphological characterization of circulating tumor cells (CTCs) from patients with different types of sarcoma using isolation by size of tumor cells: a window on sarcoma-cell invasion. Onco Targets Ther 7:1609–1617
Corassa M, Fanelli M, Guimarães APG et al (2016) Circulating Tumor Cells (CTCs) as a new and additional approach to follow-up patients with serous papillary low-grade ovarian adenocarcinoma – a case report and review of the literature (submitted)
Cristofanilli M (2014) Circulating tumour cells: telling the truth about metastasis. Lancet Oncol 15(4):365–366
Cristofanilli M, Budd GT, Mathew JE et al (2004) Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med 351(8):781–791
Cui Y, König J, Buchholz JK et al (1999) Drug resistance and ATP-dependent conjugate transport mediated by the apical multidrug resistance protein, MRP2, permanently expressed in human and canine cells. Mol Pharmacol 55(5):929–937
Das M, Riess JW, Frankel P et al (2012) ERCC1 expression in circulating tumor cells (CTCs) using a novel detection platform correlates with progression-free survival (PFS) in patients with metastatic non-small-cell lung cancer (NSCLC) receiving platinum chemotherapy. Lung Cancer 77(2):421–426
de Bono JS, Scher HI, Montgomery RB et al (2008) Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res 14(19):6302–6309
de Bono JS, Logothetis CJ, Molina A et al (2011) Abiraterone and Increased Survival in Metastatic Prostate Cancer. N Engl J Med 364(21):1995–2005
De Giorgi U, Valeo V, Rohren E et al (2010) Circulating tumor cells and bone metastases as detected by FDG-PET/CT in patients with metastatic breast cancer. Ann Oncol 21(1):33–39
De Oliveira TB, Nicolau UR, Braun AC et al (2016) Detection of drug resistance proteins in CTC from patients with locally advanced head and neck squamous cell carcinoma and their relation with survival. 7th ECHNO (European Congress on Head and Neck Oncol) abstract OP011
Devriese LA, Voest EE, Beijnen JH et al (2011) Circulating tumor cells as pharmacodynamic biomarker in early clinical oncological trials. Cancer Treat Rev 37(8):579–589
Doyle L, Ross DD (2003) Multidrug resistance mediated by the breast cancer resistance protein BCRP (ABCG2). Oncogene 22(47):7340–7358
Fabbri F, Carloni S, Zoli W et al (2013) Detection and recovery of circulating colon cancer cells using a dielectrophoresis-based device: KRAS mutation status in pure CTCs. Cancer Lett 335(1):225–231
Fearon ER, Vogelstein B (1990) A genetic model for colorectal tumorigenesis. Cell 61(5):759–767
Fina E, Reduzzi C, Motta R et al (2015) Did circulating tumor cells tell us all they could? The missed circulating tumor cell message in breast cancer. Int J Biol Markers 30(4):e429–e433
Flens MJ, Zaman GJ, van der Valk P et al (1996) Tissue distribution of the multidrug resistance protein. Am J Pathol 148(4):1237–1247
Fonkem E, Lun M, Wong ET (2011) Rare phenomenon of extracranial metastasis of glioblastoma. J Clin Oncol 29(34):4594–4595
Franken B, de Groot MR, Mastboom WJ et al (2012) Circulating tumor cells, disease recurrence and survival in newly diagnosed breast cancer. Breast Cancer Res 14(5):R133
Gao F, Cui Y, Jiang H et al (2016) Circulating tumor cell is a common property of brain glioma and promotes the monitoring system. Oncotarget 7:71330–71340
Garcia-Villa A, Balasubramanian P, Miller BL et al (2012) Assessment of γ-H2AX levels in circulating tumor cells from patients receiving chemotherapy. Front Oncol 2:128
Gasch C, Bauernhofer T, Pichler M et al (2013) Heterogeneity of epidermal growth factor receptor status and mutations of KRAS/PIK3CA in circulating tumor cells of patients with colorectal cancer. Clin Chem 59(1):252–260
Gasch C, Oldopp T, Mauermann O et al (2016) Frequent detection of PIK3CA mutations in single circulating tumor cells of patients suffering from HER2-negative metastatic breast cancer. Mol Oncol pii: S1574-7891(16)30065-5
Gazzaniga P, Naso G, Gradilone A et al (2010) Chemosensitivity profile assay of circulating cancer cells: prognostic and predictive value in epithelial tumors. Int J Cancer 126(10):2437–2447
Gerlinger M, Rowan AJ, Horswell S et al (2012) Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med 366(10):883–892
Goldkorn A, Ely B, Quinn DI et al (2014) Circulating tumor cell counts are prognostic of overall survival in SWOG S0421: a phase III trial of docetaxel with or without atrasentan for metastatic castration-resistant prostate cancer. J Clin Oncol 32(11):1136–1142
Gradilone A, Naso G, Raimondi C et al (2010) Circulating tumor cells (CTCs) in metastatic breast cancer (MBC): prognosis, drug resistance and phenotypic characterization. Ann Oncol 22(1):86–92
Gradilone A, Raimondi C, Naso G et al (2011a) How circulating tumor cells escape from multidrug resistance: translating molecular mechanisms in metastatic breast cancer treatment. Am J Clin Oncol 34(6):625–627
Gradilone A, Naso G, Raimondi C et al (2011b) Circulating tumor cells (CTCs) in metastatic breast cancer (MBC): prognosis, drug resistance and phenotypic characterization. Ann Oncol 22(1):86–92
Gunn J, McCall JL, Yun K et al (1996) Detection of micrometastases in colorectal cancer patients by K19 and K20 reverse-transcription polymerase chain reaction. Lab Investig 75(4):611–616
Haber DA, Gray NS, Baselga J (2011) The evolving war on cancer. Cell 145(1):19–24
Han L, Chen W, Zhao Q (2014) Prognostic value of circulating tumor cells in patients with pancreatic cancer: a meta-analysis. Tumour Biol 35(3):2473–2480
Hayes DF, Paoletti C (2013) Circulating tumour cells: insights into tumour heterogeneity. J Intern Med 274(2):137–143
Hinz S, Röder C, Tepel J et al (2015) Cytokeratin 20 positive circulating tumor cells are a marker for response after neoadjuvant chemoradiation but not for prognosis in patients with rectal cancer. BMC Cancer 15:953
Hofman P, Popper HH (2016) Pathologists and liquid biopsies: to be or not to be? Virchows Arch 469:601–609
Hofman V, Ilie MI, Long E et al (2011) Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: comparison of the efficacy of the CellSearch Assay™ and the isolation by size of epithelial tumor cell method. Int J Cancer 129(7):1651–1660
Hofman V, Ilie M, Long-Mira E et al (2013) Usefulness of immunocytochemistry for the detection of the BRAF(V600E) mutation in circulating tumor cells from metastatic melanoma patients. J Invest Dermatol 133(5):1378–1381
Hofman V, Ilie M, Long E et al (2014) Detection of circulating tumor cells from lung cancer patients in the era of targeted therapy: promises, drawbacks and pitfalls. Curr Mol Med 14(4):440–456
Hofman VJ, Ilie M, Hofman PM (2016) Detection and characterization of circulating tumor cells in lung cancer: why and how? Cancer Cytopathol 124(6):380–387
Holohan C, Van Schaeybroeck S, Longley DB et al (2013) Cancer drug resistance: an evolving paradigm. Nat Rev Cancer 13(10):714–726
Hong W, Lee S, Chang HJ et al (2016) Multifunctional magnetic nanowires: a novel breakthrough for ultrasensitive detection and isolation of rare cancer cells from non-metastatic early breast cancer patients using small volumes of blood. Biomaterials 106:78–86
Hoshimoto S, Shingai T, Morton DL et al (2012a) Association between circulating tumor cells and prognosis in patients with stage III melanoma with sentinel lymph node metastasis in a phase III international multicenter trial. J Clin Oncol 30(31):3819–3826
Hoshimoto S, Faries MB, Morton DL et al (2012b) Assessment of prognostic circulating tumor cells in a phase III trial of adjuvant immunotherapy after complete resection of stage IV melanoma. Ann Surg 255(2):357–362
Hou JM, Krebs MG, Lancashire L et al (2012) Clinical significance and molecular characteristics of circulating tumor cells and circulating tumor microemboli in patients with small-cell lung cancer. J Clin Oncol 30(5):525–532
Houtsmuller AB, Rademakers S, Nigg AL et al (1999) Action of DNA repair endonuclease ERCC1/XPF in living cells. Science 284(5416):958–961
Huang MY, Tsai HL, Huang JJ et al (2016) Clinical implications and future perspectives of circulating tumor cells and biomarkers in clinical outcomes of colorectal cancer. Transl Oncol 9(4):340–347
Ignatiadis M, Perraki M, Apostolaki S et al (2007) Molecular detection and prognostic value of circulating cytokeratin-19 messenger RNA-positive and HER2 messenger RNA-positive cells in the peripheral blood of women with early-stage breast cancer. Clin Breast Cancer 7(11):883–889
Iinuma H, Okinaga K, Egami H et al (2006) Usefulness and clinical significance of quantitative real-time RTPCR to detect isolated tumor cells in the peripheral blood and tumor drainage blood of patients with colorectal cancer. Int J Oncol 28(2):297–306
Ilie M, Long E, Butori C et al (2012) ALK-gene rearrangement: a comparative analysis on circulating tumour cells and tumour tissue from patients with lung adenocarcinoma. Ann Oncol 23(11):2907–2913
Ilie M, Hofman V, Long-Mira E et al (2014) “Sentinel” circulating tumor cells allow early diagnosis of lung cancer in patients with chronic obstructive pulmonary disease. PLoS One 9(10):e111597
Jiang Y, Palma JF, Agus DB et al (2010) Detection of androgen receptor mutations in circulating tumor cells in castration-resistant prostate cancer. Clin Chem 56(9):1492–1495
Kalikaki A, Politaki H, Souglakos J et al (2014) KRAS genotypic changes of circulating tumor cells during treatment of patients with metastatic colorectal cancer. PLoS One 9(8):e104902
Kalokhe G, Grimm SA, Chandler JP et al (2012) Metastatic glioblastoma: case presentations and a review of the literature. J Neuro-Oncol 107(1):21–27
Kang Y, Pantel K (2013) Tumor cell dissemination: emerging biological insights from animal models and cancer patients. Cancer Cell 23(5):573–581
Kasimir-Bauer S, Hoffmann O, Wallwiener D et al (2012) Expression of stem cell and epithelial-mesenchymal transition markers in primary breast cancer patients with circulating tumor cells. Breast Cancer Res 14(1):R15
Katsumata K, Sumi T, Mori Y et al (2006) Detection and evaluation of epithelial cells in the blood of colon cancer patients using RT-PCR. Int J Clin Oncol 11(5):385–389
Kim MY, Oskarsson T, Acharyya S et al (2009) Tumor self-seeding by circulating cancer cells. Cell 139(7):1315–1326
Kohn EC, Liotta LA (1995) Molecular insights into cancer invasion: strategies for prevention and intervention. Cancer Res 55(9):1856–1862
Krebs MG, Sloane R, Priest L et al (2011) Evaluation and prognostic significance of circulating tumor cells in patients with non–small-cell lung cancer. J Clin Oncol 29(12):1556–1563
Kuczynski EA, Sargent DJ, Grothey A et al (2013) Drug rechallenge and treatment beyond progression—implications for drug resistance. Nat Rev Clin Oncol 10(10):571–587
Kuhlmann JD, Wimberger P, Bankfalvi A et al (2014) ERCC1-positive circulating tumor cells in the blood of ovarian cancer patients as a predictive biomarker for platinum resistance. Clin Chem 60(10):1282–1289
Kurihara T, Itoi T, Sofuni A et al (2008) Detection of circulating tumor cells in patients with pancreatic cancer: a preliminary result. J Hepato-Biliary-Pancreat Surg 15(2):189–195
Lianidou ES, Mavroudis D, Georgoulias V (2013) Clinical challenges in the molecular characterization of circulating tumour cells in breast cancer. Br J Cancer 108(12):2426–2432
Lianidou ES, Strati A, Markou A (2014) Circulating tumor cells as promising novel biomarkers in solid cancers. Crit Rev Clin Lab Sci 51(3):160–171
Lou J, Ben S, Yang G et al (2013) Quantification of rare circulating tumor cells in non-small cell lung cancer by ligand-targeted PCR. PLoS One 8(12):e80458
Lowes LE, Lock M, Rodrigues G et al (2012) Circulating tumour cells in prostate cancer patients receiving salvage radiotherapy. Clin Transl Oncol 14(2):150–156
Lucci A, Hall CS, Lodhi AK et al (2012) Circulating tumour cells in non-metastatic breast cancer: a prospective study. Lancet Oncol 13(7):688–695
Magni E, Botteri E, Ravenda PS et al (2014) Detection of circulating tumor cells in patients with locally advanced rectal cancer undergoing neoadjuvant therapy followed by curative surgery. Int J Color Dis 29(9):1053–1059
Maheswaran S, Sequist LV, Nagrath S et al (2008) Detection of mutations in EGFR in circulating lung-cancer cells. N Engl J Med 359(4):366–377
Mani SA, Guo W, Liao MJ et al (2008) The epithelial mesenchymal transition generates cells with properties of stem cells. Cell 133(4):704–715
Marusyk A, Polyak K (2010) Tumor heterogeneity: causes and consequences. Biochim Biophys Acta 1805(1):105–117
Mazel M, Jacot W, Pantel K (2015) Frequent expression of PD-L1 on circulating breast cancer cells. Mol Oncol 9(9):1773–1782
Mego M, Mani SA, Cristofanilli M (2010) Molecular mechanisms of metastasis in breast cancer-clinical applications. Nat Rev Clin Oncol 7(12):693–701
Mego M, Mani SA, Lee B et al (2012) Expression of epithelial-mesenchymal transition-inducing transcription factors in primary breast cancer: the effect of neoadjuvant therapy. Int J Cancer 130(4):808–816
Mehra N, Zafeiriou Z, Lorente D et al (2015) CCR 20th anniversary commentary: circulating tumor cells in prostate cancer. Clin Cancer Res 21(22):4992–4995
Meng S, Tripathy D, Frenkel EP et al (2004) Circulating tumor cells in patients with breast cancer dormancy. Clin Cancer Res 10(24):8152–8162
Miyamoto DT, Lee RJ, Stott SL et al (2012) Androgen receptor signaling in circulating tumor cells as a marker of hormonally responsive prostate cancer. Cancer Discov 2(11):995–1003
Miyamoto DT, Zheng Y, Wittner BS et al (2015) RNA-Seq of single prostate CTCs implicates noncanonical Wnt signaling in antiandrogen resistance. Science 349(6254):1351–1356
Morel AP, Lievre M, Thomas C et al (2008) Generation of breast cancer stem cells through epithelial mesenchymal transition. PLoS One 3(8):e2888
Mostert B, Jiang Y, Sieuwerts AM et al (2013) KRAS and BRAF mutation status in circulating colorectal tumor cells and their correlation with primary and metastatic tumor tissue. Int J Cancer 133(1):130–141
Muinelo-Romay L, Vieito M, Abalo A et al (2014) Evaluation of circulating tumor cells and related events as prognostic factors and surrogate biomarkers in advanced NSCLC patients receiving first-line systemic treatment. Cancers (Basel) 6(1):153–165
Müller C, Holtschmidt J, Auer M et al (2014) Hematogenous dissemination of glioblastoma multiforme. Sci Transl Med 6(247):247ra101
Murray NP, Albarran V, Perez G et al (2015) Secondary Circulating Tumor Cells (CTCs) but not primary CTCs are associated with the clinico-pathological parameters in Chilean patients with Colo-rectal cancer. Asian Pac J Cancer Prev 16(11):4745–4749
Nadal R, Ortega FG, Salido M et al (2013) CD133 expression in circulating tumor cells from breast cancer patients: potential role in resistance to chemotherapy. Int J Cancer 133(10):2398–2407
Nesteruk D, Rutkowski A, Fabisiewicz S et al (2014) Evaluation of prognostic significance of circulating tumor cells detection in rectal cancer patients treated with preoperative radiotherapy: prospectively collected material data. Biomed Res Int 2014:712827
Nolé F, Munzone E, Zorzino L et al (2008) Variation of circulating tumor cell levels during treatment of metastatic breast cancer: prognostic and therapeutic implications. Ann Oncol 19(5):891–897
Paik S, Kim C, Wolmark N (2008) HER2 status and benefit from adjuvant trastuzumab in breast cancer. N Engl J Med 358(13):1409–1411
Pailler E, Adam J, Barthélémy A et al (2013) Detection of circulating tumor cells harboring a unique ALK rearrangement in ALK-positive non-small-cell lung cancer. J Clin Oncol 31(18):2273–2281
Pailler E, Auger N, Lindsay CR et al (2015) High level of chromosomal instability in circulating tumor cells of ROS1-rearranged non-small-cell lung cancer. Ann Oncol 26(7):1408–1415
Pantel K, Denève E, Nocca D et al (2012) Circulating epithelial cells in patients with benign colon diseases. Clin Chem 58(5):936–940
Paoletti C, Muñiz MC, Thomas DG et al (2015) Development of circulating tumor cell-endocrine therapy index in patients with hormone receptor-positive breast cancer. Clin Cancer Res 21(11):2487–2498
Paterlini-Bréchot P (2014) Circulating tumor cells: who is the killer? Cancer Microenviron 7(3):161–176
Paterlini-Brechot P, Benali NL (2007) Circulating tumor cells (CTC) detection: clinical impact and future directions. Cancer Lett 253(2):180–204
Phillips KA, Veenstra DL, Oren E (2001) Potential role of pharmacogenomics in reducing adverse drug reactions: a systematic review. JAMA 286(18):2270–2279
Pierga JY, Bidard FC, Mathiot C et al (2008) Circulating tumor cell detection predicts early metastatic relapse after neoadjuvant chemotherapy in large operable and locally advanced breast cancer in a phase II randomized trial. Clin Cancer Res 14(21):7004–7010
Pierga JY, Petit T, Delozier T et al (2012) Neoadjuvant bevacizumab, trastuzumab, and chemotherapy for primary inflammatory HER2-positive breast cancer (BEVERLY-2): an open-label, single-arm phase 2 study. Lancet Oncol 13(4):375–384
Pinzani P, Salvadori B, Simi L et al (2006) Isolation by size of epithelial tumor cells in peripheral blood of patients with breast cancer: correlation with real-time reverse transcriptase-polymerase chain reaction results and feasibility of molecular analysis by laser microdissection. Hum Pathol 37(6):711–718
Popat S, Matakidou A, Houlston RS (2004) Thymidylate synthase expression and prognosis in colorectal cancer: a systematic review and meta-analysis. J Clin Oncol 22(3):529–536
Poveda A, Kaye SB, McCormack R et al (2011) Circulating tumor cells predict PFS and overall survival in patients with relapsed/recurrent advanced ovarian cancer. Gynecol Oncol 122(3):567–572
Punnoose EA, Atwal S, Liu W et al (2012) Evaluation of circulating tumor cells and circulating tumor DNA in non-small cell lung cancer: association with clinical endpoints in a phase II clinical trial of pertuzumab and erlotinib. Clin Cancer Res 18(8):2391–2401
Punnoose EA, Ferraldeschi R, Szafer-Glusman E et al (2015) PTEN loss in circulating tumour cells correlates with PTEN loss in fresh tumour tissue from castration-resistant prostate cancer patients. Br J Cancer 113(8):1225–1233
Rack B, Schindlbeck C, Jückstock J et al (2014) Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J Natl Cancer Inst 106(5):dju066
Rahbari NN, Aigner M, Thorlund K et al (2010) Meta-analysis shows that detection of circulating tumor cells indicates poor prognosis in patients with colorectal cancer. Gastroenterol 138(5):1714–1726
Raimondi C, Nicolazzo C, Gradilone A et al (2014) Circulating tumor cells: exploring intratumor heterogeneity of colorectal cancer. Cancer Biol Ther 15(5):496–503
Riethdorf S, Pantel K (2008) Disseminated tumor cells in bone marrow and circulating tumor cells in blood of breast cancer patients: current state of detection and characterization. Pathobiology 75(2):140–148
Riethdorf S, Pantel K (2010) Advancing personalized cancer therapy by detection and characterization of circulating carcinoma cells. Ann N Y Acad Sci 1210:66–77
Riethdorf S, Müller V, Zhang L et al (2010a) Detection and HER2 expression of circulating tumor cells: prospective monitoring in breast cancer patients treated in the neoadjuvant GeparQuattro trial. Clin Cancer Res 16(9):2634–2645
Riethdorf S, Mueller V, Mauermann O et al (2010b) Abstract PD04-06: changes in circulating tumor and endothelial cells in peripheral blood of patients treated in the neoadjuvant chemotherapy plus targeted treatment breast cancer study “GeparQuinto”. Cancer Res 70(24 Suppl):PD04-6-PD-6
Roden DM, George AL Jr (2002) The genetic basis of variability in drug responses. Nat Rev Drug Discov 1(1):37–44
Salvianti F, Pazzagli M, Pinzani P (2016) Single circulating tumor cell sequencing as an advanced tool in cancer management. Expert Rev Mol Diagn 16(1):51–63
Sarker D, Workman P (2007) Pharmacodynamic biomarkers for molecular cancer therapeutics. Adv Cancer Res 96:213–268
Sastre J, Maestro ML, Puente J et al (2008) Circulating tumor cells in colorectal cancer: correlation with clinical and pathological variables. Ann Oncol 19(5):935–938
Sastre J, Vidaurreta M, Gómez A et al (2013) Prognostic value of the combination of circulating tumor cells plus KRAS in patients with metastatic colorectal cancer treated with chemotherapy plus bevacizumab. Clin Colorectal Cancer 12(4):280–286
Satelli A, Batth IS, Brownlee Z et al (2016) Potential role of nuclear PD-L1 expression in cell-surface vimentin positive circulating tumor cells as a prognostic marker in cancer patients. Sci Rep 6:28910
Sawada T, Watanabe M, Fujimura Y et al (2016) Sensitive cytometry based system for enumeration, capture and analysis of gene mutations of circulating tumor cells. Cancer Sci 107(3):307–314
Scher HI, Fizazi K, Saad F et al (2012) Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med 367(13):1187–1197
Scher HI, Heller G, Molina A et al (2015) Circulating tumor cell biomarker panel as an individual-level surrogate for survival in metastatic castration-resistant prostate cancer. J Clin Oncol 33(12):1348–1355
Scher HI, Lu D, Schreiber NA et al (2016) Association of AR-V7 on circulating tumor cells as a treatment-specific biomarker with outcomes and survival in castration-resistant prostate cancer. JAMA Oncol 2:1441–1449
Smerage JB, Budd GT, Doyle GV et al (2013) Monitoring apoptosis and Bcl-2 on circulating tumor cells in patients with metastatic breast cancer. Mol Oncol 7(3):680–692
Smerage JB, Barlow WE, Hortobagyi GN et al (2014) Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J Clin Oncol 32(31):3483–3489
Somlo G, Lau SK, Frankel P et al (2011) Multiple biomarker expression on circulating tumor cells in comparison to tumor tissues from primary and metastatic sites in patients with locally advanced/inflammatory, and stage IV breast cancer, using a novel detection technology. Breast Cancer Res Treat 128(1):155–163
Steinestel J, Luedeke M, Arndt A et al (2015) Detecting predictive androgen receptor modifications in circulating prostate cancer cells. Oncotarget. doi:10.18632/oncotarget.3925
Thorsteinsson M, Jess P (2011) The clinical significance of circulating tumor cells in non-metastatic colorectal cancer—a review. Eur J Surg Oncol 37(6):459–465
Tsai WS, Chen JS, Shao HJ et al (2016) Circulating tumor cell count correlates with colorectal neoplasm progression and is a prognostic marker for distant metastasis in non-metastatic patients. Sci Rep 6:24517
Uen YH, Lu CY, Tsai HL et al (2008) Persistent presence of postoperative circulating tumor cells is a poor prognostic factor for patients with stage I-III colorectal cancer after curative resection. Ann Surg Oncol 15(8):2120–2128
Van Berckelaer C, Brouwers AJ, Peeters DJ et al (2016) Current and future role of circulating tumor cells in patients with epithelial ovarian cancer. Eur J Surg Oncol 42:1772–1779
Wan L, Pantel K, Kang Y (2013) Tumor metastasis: moving new biological insights into the clinic. Nat Med 19(11):1450–1464
Wiedswang G, Borgen E, Karesen R et al (2004) Isolated tumor cells in bone marrow three years after diagnosis in disease-free breast cancer patients predict unfavorable clinical outcome. Clin Cancer Res 10(16):5342–5348
Wong SC, Chan CM, Ma BB et al (2009) Clinical significance of cytokeratin 20-positive circulating tumor cells detected by a refined immunomagnetic enrichment assay in colorectal cancer patients. Clin Cancer Res 15(3):1005–1012
Yu Y, Chen Z, Dong J et al (2013) Folate receptor-positive circulating tumor cells as a novel diagnostic biomarker in non-small cell lung cancer. Transl Oncol 6(6):697–702
Yu M, Bardia A, Aceto N et al (2014) Cancer therapy. Ex vivo culture of circulating breast tumor cells for individualized testing of drug susceptibility. Science 345(6193):216–220
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Chinen, L.T.D. et al. (2017). Circulating Tumor Cells as Cancer Biomarkers in the Clinic. In: Magbanua, M., Park, J. (eds) Isolation and Molecular Characterization of Circulating Tumor Cells. Advances in Experimental Medicine and Biology, vol 994. Springer, Cham. https://doi.org/10.1007/978-3-319-55947-6_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-55947-6_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-55946-9
Online ISBN: 978-3-319-55947-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)