
Abstract
In 1896, Vaughan Pendred, MD, wrote a case report about two siblings that presented with hearing loss and goiter. This initial report was followed over the next 100 years with additional cases, and the condition became known as Pendred syndrome. The underlying gene, SLC26A4, which codes for the protein pendrin, was discovered in 1997, and mutations of SLC26A4 have since been recognized to underlie not only Pendred syndrome but also nonsyndromic hearing loss associated with an enlargement of the vestibular aqueduct (EVA) and variable deficits in vestibular function. In 2001, Dr. Lorraine Everett, in a team led by Dr. Eric Green, reported the first mouse model that recapitulates EVA, deafness, and vestibular dysfunction. This and other mouse models have proven to be tremendously valuable in the quest to understand the role of pendrin in hearing and vestibular function. This chapter summarizes work on these mouse models that are revealing the role of pendrin in the inner ear.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
With permission of S. Karger AG this chapter represents an update of an article published in 2013 (Wangemann 2013).
The gene SLC26A4 (MIM #605646) codes for the protein pendrin, which is an electroneutral exchanger for anions such as HCO3 −, Cl−, and I− (Scott et al. 1999; Scott and Karniski 2000; Soleimani et al. 2001). Pendrin is expressed in the apical membrane of epithelial cells in the inner ear, the thyroid, and the kidney (Royaux et al. 2000, 2001; Wangemann et al. 2004). Additional expression has been found in airways, mammary glands, uterus, placenta, liver, platelets, and adrenal glands (Bidart et al. 2000; Suzuki et al. 2002; Rillema and Hill 2003; Nakao et al. 2008; Alesutan et al. 2011; Pelzl et al. 2013; Lazo-Fernandez et al. 2015). The expression of SLC26A4 in the inner ear and the thyroid is consistent with the observations that mutations of SLC26A4 cause hearing loss associated with an enlarged vestibular aqueduct (EVA; MIM #600791), Mondini-like dysplasia of the cochlea, vestibular dysfunction, and enlargement of the thyroid (Pendred syndrome; MIM #274600). The prevalence and spectra of SLC26A4 mutations vary among different populations (Park et al. 2003; Tsukada et al. 2015). The highest prevalence of SLC26A4 mutations has been reported in East Asian populations in China, Taiwan, Japan, and Korea. Notably, in some Chinese populations, 13.7, 16.8, or 18.6 % of children attending schools for the deaf carry mutations of SLC26A4 (Yuan et al. 2009; Zhu et al. 2015; Jiang et al. 2015). Between 82 and 98 % of East Asian patients with EVA carry mutations of SLC26A4 (Choi et al. 2009; Tsukada et al. 2015). The prevalence of SLC26A4 mutations in European and North American Caucasians is much lower. About 50 % of North American and European Caucasian patients with EVA carry mutations of SLC26A4 (Campbell et al. 2001). Of these patients, about one-half carry one detectable mutation in the coding regions and splice sites of SLC26A4, whereas the other one-half of patients carry mutations on both alleles. Hearing loss is sometimes congenital, but typically fluctuating and progressive with an onset before or around the time of oral-auditory speech and language acquisition (Pryor et al. 2005; Choi et al. 2009; Miyagawa et al. 2014). Vestibular dysfunction is less overt and less common (Abe et al. 1999; Sugiura et al. 2005; Suzuki et al. 2007; Zhou and Gopen 2011; Zalewski et al. 2015; Jung et al. 2016), and the onset of goiter occurs typically after puberty (Fraser et al. 1960; Fraser 1965; Ajij et al. 2016). In contrast to mutations of other genes that cause hearing loss, there is no close correlation between mutation type and phenotype for SLC26A4 (Choi et al. 2009; Tsukada et al. 2015). However, in north American and European Caucasian EVA patients, the number of mutant alleles of SLC26A4 is correlated with both the thyroid and auditory phenotypes. Bilateral EVA and a biochemical defect in thyroid iodine organification are penetrant features of two mutant alleles of SLC26A4, whereas unilateral EVA and a normal thyroid iodination phenotype are observed in association with one mutant allele of SLC26A4. The incomplete penetrance of EVA and variability in the severity of hearing loss suggest that additional genetic or environmental factors play a critical role, which merits further investigations into the physiology and pathobiology of pendrin-related deafness with the goal to ameliorate or prevent hearing loss in individuals carrying mutations of SLC26A4.
Most research into the physiology and pathobiology of pendrin-associated hearing loss has been carried out in mice. The goal of this review is to provide a brief summary of studies in mouse models that have been developed to delineate the role of pendrin in the physiology of hearing and balance with the ultimate goal to develop strategies to preserve hearing in individuals that carry mutations of SLC26A4. Clinical phenotypes and the genetics of hearing loss associated with EVA are reviewed elsewhere (Griffith and Wangemann 2011; Ito et al. 2011, 2013).
2 Synopsis of the Development of the Murine Inner Ear
The development of the inner ear begins in mice at embryonic day 9.5 (E9.5) with the formation of an otocyst (reviewed in: (Mansour and Schoenwolf 2005)). The otocyst encloses amniotic fluid, which is a plasma-like fluid containing ~140 mM Na+ and ~10 mM K+ (Cheung and Brace 2005). Between E10 and E10.5, two protrusions begin to extend from the otocyst: one forms the cochlea and the other forms the endolymphatic sac. While the protrusions elongate, the center of the otocyst reorganizes into the vestibular labyrinth. The lumen of the endolymphatic sac opens at E10.5, and the lumen of the cochlea opens at E14.5 (Kim and Wangemann 2010). Lumen formation during the growth phase of the inner ear is controlled by a balance of fluid secretion and absorption. Fluid secretion appears to occur in the vestibular labyrinth and fluid absorption in the endolymphatic sac (Kim and Wangemann 2010). The hypothesis that NaCl secretion and NaCl absorption control luminal volume during the growth phase of the inner ear is consistent with the finding that the luminal fluid in the cochlea is filled until E17.5 with a solution that contains ~140 mM Na+, ~126 mM Cl−, ~10 mM K+, and ~25 mM HCO3 − (Kim and Wangemann 2011, Li et al. 2013b).
At E17.5, closure of the utricular-saccular duct separates the interconnected fluid compartments of the inner ear into two fluid systems (Cantos et al. 2000). One system consists of the cochlea, the saccule, and the endolymphatic sac, and the other consists of the utricle, the three ampullae, and the three semicircular canals (Fig. 2.1). The separation of the vestibular labyrinth from the cochlea coincides with the acquisition of mechanosensitivity of vestibular hair cells at E17 (Geleoc and Holt 2003; Lelli et al. 2009). The onset of vestibular function occurs ~8 days later, at postnatal day 4 (P4), concurrent with the general maturation of the organ and the maturation of the innervation (Nordemar 1983; Desmadryl and Sans 1990). With the conclusion of the growth phase of the inner ear, the luminal fluid, endolymph, in the cochlea and the vestibular labyrinth changes from a NaCl-rich to a KCl-rich solution. The onset of K+ secretion in the utricle is currently under investigation. The onset of K+ secretion in the cochlea, however, has been found to occur at ~ E19.5. Two days later, at P0, when cochlear sensory cells acquire mature mechanosensitivity, cochlear endolymph contains ~70 mM K+ (Lelli et al. 2009, Li et al. 2013b). Five days later, at P3, endolymph contains ~100 mM K+, which is close to the mature concentration of 150 mM K+ (Li et al. 2013b). Concurrent with the rise of the K+ concentration occurs a decline of the Na+ concentration (Li et al. 2013b). The onset of hearing at ~P12 coincides with the maturation of the endocochlear potential, which rises between P5 and P15 from ~10 mV to the mature voltage of ~90 mV (Steel and Barkway 1989; Yamasaki et al. 2000; Wangemann et al. 2007). In the mature inner ear, the Na+ concentration is ~1 mM and the Ca2+ concentration is 22 μM, both concentrations being unusually low for an extracellular fluid since most extracellular fluids contain ~150 mM Na+ and 1.5 mM Ca2+(reviewed in: Wangemann 2006).

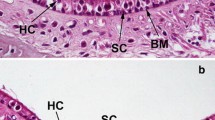
Pendrin expression in the inner ear. (a) Schematic overview. The inner ear consists of the cochlea, saccule, and utricle and three ampullae with semicircular canals and the endolymphatic sac and duct. All compartments are lined with epithelial cells and filled with endolymph. (b) Cross section of one turn of the mature cochlea. Pendrin is expressed in epithelial cells of the spiral prominence (long arrows) and in spindle cells of stria vascularis (short arrows). (c–d) Cross sections of the saccule or utricle and an ampulla. Pendrin is expressed in transitional cells, which are epithelial cells surrounding the maculae in the saccule and utricle and the cupulae in the ampullae. (e) Cross sections of the endolymphatic duct and sac. The endolymphatic duct runs through a bony canal, which is called the vestibular aqueduct. Pendrin is expressed in mitochondria-rich cells in the endolymphatic sac (arrows). Similar diagrams were contributed to other papers (Li et al. 2013a, Wangemann 2013)
3 Pendrin Expression in the Inner Ear
Pendrin in the inner ear functions as an exchanger of Cl− and HCO3 − and thereby may contribute to an elevated endolymphatic HCO3 − concentration and an elevated endolymphatic pH (Nakaya et al. 2007; Wangemann et al. 2007; Kim and Wangemann 2011). In the mature inner ear, pendrin is expressed in the apical membrane of nonsensory epithelial cells in the cochlea, the vestibular labyrinth, and the endolymphatic sac (Royaux et al. 2003; Wangemann et al. 2004). During development, the earliest expression of pendrin in the inner ear occurs at E11.5 in the endolymphatic sac (Kim and Wangemann 2011). Between E13.5 and E14.5, expression in the endolymphatic sac increases dramatically. At E14.5, virtually all pendrin expression in the inner ear is located in the endolymphatic sac. In the cochlea, the earliest expression of pendrin is found in the hook region at E14.5. The hook region is the most basal part of the cochlea. Between E14.5 and E17.5, pendrin expression expands from the hook region to the lower and then to the upper turn of the cochlea. The onset of pendrin expression in the vestibular labyrinth occurs at E14.5 in the utricle and at E16.5 in the ampullae.
4 Mouse Models That Lack Pendrin Expression
The first mouse model, Slc26a4 Δ/Δ (formerly called Slc26a4 −/− or Pds −/−), is a knock-out mouse maintained in the 129S6 strain, in which exon 8 of Slc26a4 is replaced with a neomycin cassette (Everett et al. 2001). The replacement introduces a frame shift, which prevents the generation of a functional protein. Slc26a4 Δ/Δ mice develop an enlarged vestibular aqueduct and a Mondini-like dysplasia of the cochlea, fail to develop hearing and display vestibular deficits. The hearing and balance phenotype of Slc26a4 Δ/Δ mice is more severe than the phenotype in most patients with DFNB4 or Pendred syndrome, who, in many cases, are born with residual hearing that often deteriorates within the first 3 years (Kim et al. 2015).
Consistent with the recessive inheritance pattern, Slc26a4 Δ/+ mice develop normal sensory systems and normal hearing and balance. Slc26a4 Δ/Δ and Slc26a4 Δ/+ mice have been used extensively to investigate the consequence of a complete lack of pendrin for the development of the inner ear. Further, Slc26a4 Δ/Δ and Slc26a4 Δ/+ mice have been used as background for transgenic mouse models that feature temporally or spatially limited pendrin expression from a transgene (Choi et al. 2011, Li et al. 2013a).
Several of the phenotypic features of Slc26a4 Δ/Δ mice have been observed in the pendrin-mutation knock-in mouse, Slc26a4 Tm1Dontuh/Tm1Dontuh. Slc26a4 Tm1Dontuh/Tm1Dontuh mice, which are maintained in the C57BL/6 strain, contain a splice-site mutation at exon 8 of Slc26a4. This mutation introduces a frame shift and a new stop-codon designed to recapitulate the human mutation c.919-2A > G, which is the most prevalent mutation in China, Taiwan, and Mongolia (Lu et al. 2011; Tsukada et al. 2015). Similar to Slc26a4 Δ/Δ mice, Slc26a4 Tm1Dontuh/Tm1Dontuh mice lack exon 8 of Slc26a4, which leads to a similar phenotype.
The phenotypes of Slc26a4 Δ/Δ and Slc26a4 Tm1Dontuh/Tm1Dontuh mice bear a clear resemblance to the human phenotype. In contrast, Slc26a4 Tm2Dontuh/Tm2Dontuh mice, also maintained in the C57BL/6 strain, contain a single-nucleotide mutation designed to recapitulate the human mutation p. H723R, which is the most prevalent mutation in Japan and Korea (Lu et al. 2013; Tsukada et al. 2015). Slc26a4 Tm2Dontuh/Tm2Dontuh mice, however, have normal hearing and balance (Lu et al. 2013). The basis for this latter observation is unknown, but illustrates the challenges in developing mouse models that closely approximate the human EVA phenotype.
4.1 Development of the Cochlea Without Pendrin
The first pathobiological alteration of the inner ear in Slc26a4 Δ/Δ mice is the abnormal enlargement of the luminal volume that begins at E14.5. The enlargement coincides with cochlear lumen formation and persists throughout adulthood (Everett et al. 2001; Kim and Wangemann 2011). Formation of the enlargement during the growth phase of the inner ear appears to be the consequence of an imbalance between NaCl secretion and pendrin-dependent NaCl absorption. At E18.5, when the growth phase of the inner ear comes to an end, the enlargement amounts to a ~10-fold larger volume of scala media in the cochlea of Slc26a4 Δ/Δ mice compared to that of Slc26a4 Δ/+ mice.
The second pathobiological alteration in the inner ear in Slc26a4 Δ/Δ mice is the acidification of cochlear endolymph that begins at E15.5 and coincides with the enlargement and the failed rise in pendrin expression at E14.5 (Kim and Wangemann 2011). Acidification of the luminal fluid also occurs in the endolymphatic sac and has been documented in the mature inner ear in the cochlea and the utricle of the vestibular labyrinth (Nakaya et al. 2007; Wangemann et al. 2007).
Luminal enlargement and acidification are the primary pathobiological alterations, which distribute the effect of pendrin deficiency from pendrin-expressing cells to the entire inner ear (Kim and Wangemann 2010). Luminal acidification alters pH-sensitive mechanisms, and luminal enlargement limits cell-to-cell communication mechanisms that rely on contact or diffusible factors transmitted via the luminal or abluminal compartment. A remarkable number of secondary consequences of the lack of pendrin expression have been observed. Impaired cell-to-cell communication may be responsible for the premature onset of connexin 26 expression in basal cells of stria vascularis at E18.5, for the retarded development of the layered structure of stria vascularis observed at P3, the retarded development of the organ of Corti between age P5 and P10 that includes a delayed opening of the tunnel, failure to express BK K+ channels in inner hair cells, and a delayed innervation of the organ of Corti (Wangemann et al. 2009; Kim and Wangemann 2011).
One of the diffusible factors affected by the impaired cell-to-cell communication appears to be thyroid hormone (T3) that is generated from the pro-hormone thyroxine (T4) produced in the thyroid gland and delivered to the inner ear via the vasculature. In the cochlea, T3 is generated from T4 in fibrocytes located in the modiolus, the spiral limbus, and the spiral ligament. Receptors for T3, however, are located in the organ of Corti and the cochlear capsule. Enlargement and consequently delays in thyroid hormone signaling lead to signs of a local cochlear hypothyroidism that is evident between P5 and P10 from a delayed opening of the tunnel of Corti, delayed innervation, thickening of the tectorial membrane, failure to express BK K+ channels in inner hair cells, and a delayed ossification of the cochlear capsule (Wangemann et al. 2009; Kim and Wangemann 2011; Dror et al. 2014).
Additional consequences of the enlargement include an increase in the rate of K+ secretion by strial marginal cells (Li et al. 2013b), an increase in the rate of Na+ absorption by Reissner’s membrane epithelial cells (Kim et al. 2014), oxidative and nitrative stress in stria vascularis (Singh and Wangemann 2008), loss of the K+ channel KCNJ10 in intermediate cells of stria vascularis and loss of the endocochlear potential (Wangemann et al. 2004), a rise in the endolymphatic Ca2+ concentration (Wangemann et al. 2007), and finally degeneration of sensory cells and stria vascularis (Jabba et al. 2006). The increase in the rate of K+ secretion is evident from the finding that differences in endolymph K+ concentrations between Slc26a4 Δ/Δ and Slc26a4 Δ/+ mice never exceed a factor of 2, while the volume of endolymph differs by a factor of 10 (Kim and Wangemann 2010, Li et al. 2013b). Whether the increase in the rate of K+ secretion is a function of the enlarged luminal volume or a function of the lower pH is not known. Marginal cells sense K+ concentrations at the apical membrane by an unknown mechanism, and low apical K+ concentrations lead to an increase in the rate of K+ secretion (Wangemann et al. 1995; Wangemann et al. 1996). A pH effect on K+ secretion is also conceivable since the K+ channel KCNQ1/KCNE1 (formerly known as KvLQT1/minK or IsK) in the apical membrane of marginal cells is activated by extracellular acidification (Unsold et al. 2000). In spite of the elevated rate of K+ secretion, the K+ concentration in endolymph remains slightly lower in Slc26a4 Δ/Δ compared to Slc26a4 Δ/+ or Slc26a4 +/+ mice (Royaux et al. 2003, Li et al. 2013b). The lower K+ concentration may be balanced by a higher endolymphatic Na+ concentration, which, in turn, may be responsible for the observed upregulation of Na+ reabsorption and ENaC in Reissner’s membrane epithelial cells (Kim et al. 2014).
A plausible consequence of higher metabolic rates necessary to maintain higher rates of K+ secretion is oxidative and nitrative stress that results in elevated amounts of nitrated and oxidized proteins in stria vascularis of Slc26a4 Δ/Δ mice (Singh and Wangemann 2008). Incompletely developed defense mechanisms may contribute to the free radical load. Expression levels of the K+ channel KCNJ10 are reduced in the combined presence of oxidative and nitrative stress (Singh and Wangemann 2008), and loss of KCNJ10 is sufficient to abolish the endocochlear potential (Marcus et al. 2002). The endocochlear potential, however, depends not only on the expression of KCNJ10 but also on the integrity of epithelial and endothelial barriers that separate the intrastrial fluid space from endolymph, perilymph, and blood. Studies which used fluorescent beads (~20 nm diameter) as tracer have failed to demonstrate a compromise of the barrier between the intrastrial fluid space and blood; however, studies that used the smaller tracer biotin have demonstrated a compromise in the barrier between the intrastrial fluid space and perilymph in Slc26a4 Δ/Δ mice (Ito et al. 2014). This compromise in the barrier integrity in conjunction with the loss of KCNJ10 appears to cause the observed loss of the endocochlear potential.
The loss of the endocochlear potential and the acidification of endolymph are likely the main factors that contribute to the elevation of the endolymphatic Ca2+ concentration in Slc26a4 Δ/Δ mice. The concentration of Ca2+ in endolymph of normal mice, such as Slc26a4 Δ/+ mice, is 22 μM, whereas the Ca2+ concentration in Slc26a4 Δ/Δ mice is higher by a factor of ~100 (Wangemann et al. 2007). The reduction of the endocochlear potential could contribute to the observed elevation of the endolymphatic Ca2+ concentration since suppression of the endocochlear potential has been shown to coincide with a rise in the endolymphatic Ca2+ concentration (Ninoyu and Meyer zum Gottesberge 1986; Ikeda et al. 1987). The elevated luminal Ca2+ concentration in Slc26a4 Δ/Δ mice is likely to contribute to the degeneration of sensory hair cells that becomes overt at P15 (Everett et al. 2001). Contributing factors may be the luminal acidification, local cochlear hypothyroidism, and the lack of the endocochlear potential. Similarly, marginal cells of stria vascularis degenerate after P15, and macrophages appear in stria vascularis of Slc26a4 Δ/Δ mice at P30 (Jabba et al. 2006). Macrophages that accumulate in stria vascularis are strongly pigmented and give stria vascularis a dark appearance (Wangemann et al. 2004). It is unclear whether pigmentation is inherent to macrophages or whether pigmentation is acquired by phagocytosis of melanin-containing intermediate cells of stria vascularis.
4.2 Development of the Vestibular Labyrinth Without Pendrin
Secondary consequences of the lack of pendrin expression in the vestibular labyrinth include an increase in the endolymphatic Ca2+ concentration and the formation of giant otoconia which leads to vestibular dysfunction (Everett et al. 2001; Wangemann et al. 2004; Nakaya et al. 2007). Otoconia are protein-containing CaCO3 crystals that enable the detection of linear acceleration in the utricle and saccule of the vestibular labyrinth. Normal otoconia vary in size but do not exceed ~20 μm, whereas giant otoconia reach sizes of ~200 μm. Giant otoconia have been reported in Slc26a4 Δ/Δ mice as well as in Slc26a4 loop/loop and Slc26a4 Tm1Dontuh/Tm1Dontuh mice (Everett et al. 2001; Wangemann et al. 2004; Dror et al. 2010; Lu et al. 2011). The concentration of Ca2+ in vestibular endolymph of normal mice, such as Slc26a4 Δ/+ mice, is 250 μM, whereas the Ca2+ concentration in Slc26a4 Δ/Δ mice is higher by a factor of ~10 (Nakaya et al. 2007). The higher endolymphatic Ca2+ concentration may be a function of the larger transepithelial potential (−4 mV in Slc26a4 Δ/Δ mice vs. −1.5 mV in Slc26a4 Δ/+ mice), the more acidic pH (pH 7.1 in Slc26a4 Δ/Δ mice vs. pH 7.4 in Slc26a4 Δ/+ mice), and a failure to absorb Ca2+ (Nakaya et al. 2007; Yamauchi et al. 2010).
5 Mouse Models That Express Hypomorphic Pendrin
Slc26a4 loop/loop mice were identified in a mutagenesis screen for neurosensory disorders and found to contain a point mutation, S408F, that reduces the anion exchange activity of pendrin without affecting protein expression (Dror et al. 2010). Interestingly, this hypomorphic mutant results in a phenotype that is similar to the phenotype of Slc26a4 Δ/Δ mice, which features a complete loss of pendrin expression. Similar to Slc26a4 Δ/Δ mice, Slc26a4 loop/loop mice do not acquire hearing or vestibular function, develop an enlargement of the cochlea, and form giant otoconia in the vestibular labyrinth. Further, Slc26a4 loop/loop mice, similar to Slc26a4 Δ/Δ mice, develop signs of cochlear hypothyroidism including a thickened tectorial membrane with reduced beta-tectorin expression, a lack of BK K+ channels in inner hair cells, and a delayed ossification of the temporal bone (Dror et al. 2014). These findings underscore the importance of sufficient pendrin function during development of the inner ear.
6 Mouse Models with Spatially Limited Pendrin Expression
Slc26a4 transcription is controlled by various regulatory elements in the promoter region of Slc26a4 that allow the expression to be cell-specific and responsive to specific situations (Yang et al. 2007; Adler et al. 2008; Rozenfeld et al. 2012; Vanoni et al. 2013). Notably, expression in mitochondria-rich cells of the endolymphatic sac of the inner ear is driven by the transcription factor FOXI1, whereas expression in the cochlea and the vestibular labyrinth is driven by other regulators (Yang et al. 2007). FOXI1 in mitochondria-rich cells of the endolymphatic sac drives not only the expression of pendrin but also the expression of ATP6V1B1, a subunit of the H+ ATPase that is expressed in the inner ear only in these cells (Vidarsson et al. 2009). FOXI1 and ATP6V1B1 have therefore been used to generate mouse models that exclude the expression of pendrin from the endolymphatic sac or that limit the expression of pendrin in the inner ear to the endolymphatic sac.
6.1 Inner Ears Without Pendrin Expression in the Endolymphatic Sac
The mouse model Foxi1 −/−, which lacks expression of the transcription factor FOXI1, expresses pendrin in the cochlea and in the vestibular labyrinth but lacks pendrin expression in the endolymphatic sac (Hulander et al. 2003). The observations that Foxi1 −/− mice are deaf, have vestibular dysfunction, and develop an enlargement of the inner ear point to the importance of the endolymphatic sac for the development of the cochlea and the vestibular labyrinth.
6.2 Inner Ear Without Pendrin Expression in the Cochlea and Vestibular Labyrinth
Slc26a4 Δ/Δ and Slc26a4 Δ/+ mice have been used as genetic background for a model that features a spatially limited pendrin expression (Li et al. 2013a). Tg(B1-hPDS)Slc26a4 Δ/Δ mice contain a transgene, which consists of the promoter for human ATP6V1B1 that drives the expression of human SLC26A4, formerly called hPDS. ATP6V1B1 codes for the B1-subunit of the H+ ATPase, which is expressed in mitochondria-rich cells of the endolymphatic sac but not in the cochlea or in the vestibular labyrinth. Thus, Tg(B1-hPDS)Slc26a4 Δ/Δ mice express human pendrin in mitochondria-rich cells of the endolymphatic sac but lack pendrin expression in the cochlea and the vestibular labyrinth of the inner ear (Li et al. 2013a). Tg(B1-hPDS)Slc26a4 Δ/Δ mice do not develop the enlargement typically observed in Slc26a4 Δ/Δ mice. This finding demonstrates that restoration of pendrin expression in the endolymphatic sac is sufficient to restore fluid absorption in the endolymphatic sac and to restore normal fluid homeostasis throughout the inner ear. Most interestingly, hearing and balance are restored in Tg(B1-hPDS)Slc26a4 Δ/Δ mice. These findings raise the possibility that a spatially limited therapy focused on the endolymphatic sac (a structure that is relatively remote from the cochlea) might restore normal hearing and balance. Although this finding suggests that the expression of pendrin in the cochlea and the vestibular labyrinth is dispensable for hearing and balance, it remains to be determined whether a cochlea without pendrin has a robust hearing phenotype or whether pendrin expression has a protective or homeostatic role in response to common stressors such as noise and aging.
7 Mouse Models with Temporally Limited Pendrin Expression
Slc26a4 Δ/Δ and Slc26a4 Δ/+ mice have also been used in combination with a binary transgenic line that permits temporally limited pendrin expression. Tg[E],Tg[R]Slc26a4 Δ/Δ mice contain two transgenes, an effector transgene, Tg[E], which consists of the murine promoter of Slc26a4 in series with the coding sequence of the tet-on transactivator rtTA, and a responder transgene, Tg[R], which consists of a response-element for the doxycycline-bound rtTA-regulating expression of a murine Slc26a4 cDNA (Choi et al. 2011). Since rtTA expression is driven by an Slc26a4 promoter and regulatory elements, the temporal and spatial domains of expression of pendrin are limited to those in which pendrin is expressed in wild-type mice. Both transgenes, which were randomly inserted at unlinked locations in the genome, were crossed with the Slc26a4 Δ/Δ line so that pendrin is expressed in the inner ear when doxycycline is present. Omission of doxycycline prohibits expression, and withdrawal of doxycycline leads to a rapid cessation of pendrin expression. Thus, pendrin expression can be controlled through the administration of doxycycline. When doxycycline was present from conception onward, mice developed a normal anatomy of the inner ear with no evidence of enlargement and normal hearing thresholds similar to Slc26a4 Δ/+ mice, and when doxycycline was absent, mice developed an enlargement of the inner ear and failed to acquire hearing similar to Slc26a4 Δ/Δ mice. Interestingly, cessation of pendrin expression in a fully functional inner ear did not affect hearing (Choi et al. 2011). These findings demonstrate that pendrin is required for the development but not for the maintenance of hearing in a normally developed ear.
7.1 Pendrin Expression Is Required During a Critical Time Period During Development
The mouse model Tg[E],Tg[R]Slc26a4 Δ/Δ was used to determine the time period during which pendrin expression is required for normal cochlear development (Choi et al. 2011). Mice developed normal hearing, when doxycycline was administered from conception onward. Normal hearing thresholds developed even when the normal onset of pendrin expression at E11.5 was delayed by 5 days to E16.5 in the conditional mutant mice. Further, mice developed normal hearing thresholds, when pendrin expression was terminated by withdrawal of doxycycline as early as P2. These data define E16.5 to P2 as the most critical time period during which pendrin is needed for the development of normal hearing thresholds (Choi et al. 2011). The time period needed for the development of an uncompromised endocochlear potential and a normal endolymphatic pH begin earlier and last longer, which may imply that the hearing phenotype may be less robust in spite of normal thresholds when pendrin expression is restricted to the most critical time period (Choi et al. 2011). Taken together, the observations open the prospect that a temporally limited therapy focused on the prenatal phase of development may restore hearing in individuals bearing mutations of SLC26A4.
7.2 Pendrin Deficiency During Development Leads to Degeneration of Stria Vascularis and Causes Fluctuating and Progressive Hearing Loss
The mouse model Tg[E],Tg[R]Slc26a4 Δ/Δ was used to determine the effect of pendrin deficiency on hearing thresholds and on the stability of the hearing phenotype (Ito et al. 2014). Doxycycline was administered from conception until E17.5 and thus, pendrin expression was terminated within the critical time period. Mice developed a normal anatomy of the inner ear with no evidence of an enlargement; however, the hearing phenotype was not stable. Mice developed fluctuating and progressive hearing loss, which recapitulates a hearing phenotype often observed in patients with mutations of SLC26A4 (Griffith and Wangemann 2011; Ito et al. 2014, 2015).
Several observations point to stria vascularis as the major player in the development of fluctuating hearing loss (Ito et al. 2014; Ito et al. 2015). Hearing thresholds correlated with the magnitude of the endocochlear potential in pendrin-deficient mice. The expression level of KCNJ10 was reduced, and the normal complex morphological interdigitations between marginal and intermediate cells were diminished (Ito et al. 2014). Progressive hearing loss correlated with degeneration of stria vascularis including loss of KCNQ1 expression and enlargement of apical cell surfaces of marginal cells, hyperpigmentation, and expression of macrophage markers such as CD68 (Ito et al. 2015). Degeneration of stria vascularis in pendrin-deficient mice resembles, to some extent, the degeneration observed, at a faster time scale, in Slc26a4 Δ/Δ mice that are devoid of pendrin expression (Jabba et al. 2006). The link between pendrin deficiency and degeneration of stria vascularis may involve the pendrin-expressing spindle-shaped cells of stria vascularis (Wangemann et al. 2004; Nishio et al. 2016). Spindle-shaped cells provide the upper and lower limits of stria vascularis, face endolymph on their apical membrane, and connect marginal cells to basal cells (Katagiri et al. 1968; Luciano et al. 1995). Unlike marginal cells, spindle-shaped cells do not express KCNQ1 in their apical membrane but do express pendrin and ATP-gated cation channels P2RX2 (Wangemann et al. 2004; Housley et al. 2013).
7.3 Reinstatement of Pendrin Expression Alleviates Fluctuating Hearing Loss
The mouse model Tg[E],Tg[R]Slc26a4 Δ/Δ was further used to determine whether restoration of pendrin expression has a beneficial effect on hearing (Nishio et al. 2016). Doxycycline was administered from conception until E17.5, which resulted in the development of fluctuating and progressive hearing loss. Doxycycline was then reinstated either at P6 or at P30, which is before or after the establishment of the endocochlear potential and the onset of hearing. Reinstatement of pendrin expression at P6 alleviated hearing fluctuations, but reinstatement at P30 had no beneficial effect. An inverse correlation was noted between hearing thresholds and the amount of pendrin expression in the apical membrane of spindle-shaped cells. These observations underscore the importance of spindle-shaped cells for the homeostasis of stria vascularis, link deficient spindle-shaped cells to fluctuating hearing loss, and indicate that restoration of pendrin expression may be beneficial to ameliorate progression and fluctuations of hearing in individuals bearing mutations of SLC26A4.
Conclusions
Studies in mouse models have provided tremendous insights into the role of pendrin in inner ear development and the etiology of an enlargement of the vestibular aqueduct. Studies of pendrin-related mouse models have revealed pathobiological mechanisms that may have broad implications beyond hearing loss associated with loss-of-function or hypo-functional mutations of SLC26A4. The concept that a temporally and spatially limited therapy may be sufficient to restore normal hearing or to ameliorate fluctuations and progression of hearing loss provides an imperative to develop interventions that secure a lifetime of normal hearing for individuals bearing mutations of SLC26A4.
References
Abe S, Usami S, Hoover DM et al (1999) Fluctuating sensorineural hearing loss associated with enlarged vestibular aqueduct maps to 7q31, the region containing the Pendred gene. Am J Med Genet 82:322–328
Adler L, Efrati E, Zelikovic I (2008) Molecular mechanisms of epithelial cell-specific expression and regulation of the human anion exchanger (pendrin) gene. Am J Physiol Cell Physiol 294:C1261–C1276
Ajij M, Shambhavi, Patra B et al (2016) Pendred syndrome in a newborn with neck swelling: a case report. J Trop Pediatr pii: fmw002
Alesutan I, Daryadel A, Mohebbi N et al (2011) Impact of bicarbonate, ammonium chloride, and acetazolamide on hepatic and renal SLC26A4 expression. Cell Physiol Biochem 28:553–558
Bidart JM, Lacroix L, Evain-Brion D et al (2000) Expression of Na+/I− symporter and Pendred syndrome genes in trophoblast cells. J Clin Endocrinol Metab 85:4367–4372
Campbell C, Cucci RA, Prasad S et al (2001) Pendred syndrome, DFNB4, and PDS/SLC26A4 identification of eight novel mutations and possible genotype-phenotype correlations. Hum Mutat 17:403–411
Cantos R, Cole LK, Acampora D et al (2000) Patterning of the mammalian cochlea. Proc Natl Acad Sci U S A 97:11707–11713
Cheung CY, Brace RA (2005) Amniotic fluid volume and composition in mouse pregnancy. J Soc Gynecol Investig 12:558–562
Choi BY, Stewart AK, Madeo AC et al (2009) Hypo-Functional SLC26A4 variants associated with nonsyndromic hearing loss and enlargement of the vestibular aqueduct: Genotype-phenotype correlation or coincidental polymorphisms? Hum Mutat 30:599–608
Choi BY, Kim HM, Ito T et al (2011) Mouse model of enlarged vestibular aqueducts defines temporal requirement of Slc26a4 expression for hearing acquisition. J Clin Invest 121:4516–4525
Desmadryl G, Sans A (1990) Afferent innervation patterns in crista ampullaris of the mouse during ontogenesis. Brain Res Dev Brain Res 52:183–189
Dror AA, Politi Y, Shahin H et al (2010) Calcium oxalate stone formation in the inner ear as a result of an Slc26a4 mutation. J Biol Chem 285:21724–21735
Dror AA, Lenz DR, Shivatzki S et al (2014) Atrophic thyroid follicles and inner ear defects reminiscent of cochlear hypothyroidism in Slc26a4-related deafness. Mamm Genome 25:304–316
Everett LA, Belyantseva IA, Noben-Trauth K et al (2001) Targeted disruption of mouse Pds provides insight about the inner-ear defects encountered in Pendred syndrome. Hum Mol Genet 10:153–161
Fraser GR (1965) Association of congenital deafness with goitre (Pendred’s syndrome) a study of 207 families. Ann Hum Genet 28:201–249
Fraser GR, Morgans ME, Trotter WR (1960) The syndrome of sporadic goiter and congenital deafness. Quart J Med 29:279–295
Geleoc GS, Holt JR (2003) Developmental acquisition of sensory transduction in hair cells of the mouse inner ear. Nat Neurosci 6:1019–1020
Griffith AJ, Wangemann P (2011) Hearing loss associated with enlargement of the vestibular aqueduct: mechanistic insights from clinical phenotypes, genotypes, and mouse models. Hear Res 281:11–17
Housley GD, Morton-Jones R, Vlajkovic SM et al (2013) ATP-gated ion channels mediate adaptation to elevated sound levels. Proc Natl Acad Sci U S A 110:7494–7499
Hulander M, Kiernan AE, Blomqvist SR et al (2003) Lack of pendrin expression leads to deafness and expansion of the endolymphatic compartment in inner ears of Foxi1 null mutant mice. Development 130:2013–2025
Ikeda K, Kusakari J, Takasaka T et al (1987) The Ca2+ activity of cochlear endolymph of the guinea pig and the effect of inhibitors. Hear Res 26:117–125
Ito T, Choi BY, King KA et al (2011) SLC26A4 genotypes and phenotypes associated with enlargement of the vestibular aqueduct. Cell Physiol Biochem 28:545–552
Ito T, Muskett J, Chattaraj P et al (2013) SLC26A4 mutation testing for hearing loss associated with enlargement of the vestibular aqueduct. World J Otorhinolaryngol 3:26–34
Ito T, Li X, Kurima K et al (2014) Slc26a4-insufficiency causes fluctuating hearing loss and stria vascularis dysfunction. Neurobiol Dis 66:53–65
Ito T, Nishio A, Wangemann P et al (2015) Progressive irreversible hearing loss is caused by stria vascularis degeneration in an Slc26a4-insufficient mouse model of large vestibular aqueduct syndrome. Neuroscience 310:188–197
Jabba SV, Oelke A, Singh R et al (2006) Macrophage invasion contributes to degeneration of stria vascularis in Pendred syndrome mouse model. BMC Med 4:37
Jiang Y, Huang S, Deng T et al (2015) Mutation spectrum of common deafness-causing genes in patients with non-syndromic deafness in the Xiamen area, China. PLoS One 10, e0135088
Jung J, Seo YW, Choi JY et al (2016) Vestibular function is associated with residual low-frequency hearing loss in patients with bi-allelic mutations in the SLC26A4 gene. Hear Res 335:33–39
Katagiri S, Kawamoto K, Watanuki K (1968) Some surface views of the stria vascularis and its adjacent areas. Acta Otolaryngol 66:386–398
Kim HM, Wangemann P (2010) Failure of fluid absorption in the endolymphatic sac initiates cochlear enlargement that leads to deafness in mice lacking pendrin expression. PLoS One 5, e14041
Kim HM, Wangemann P (2011) Epithelial cell stretching and luminal acidification lead to a retarded development of stria vascularis and deafness in mice lacking pendrin. PLoS One 6, e17949
Kim BG, Kim JY, Kim HN et al (2014) Developmental changes of ENaC expression and function in the inner ear of pendrin knock-out mice as a perspective on the development of endolymphatic hydrops. PLoS One 9, e95730
Kim BG, Roh KJ, Park AY et al (2015) Early deterioration of residual hearing in patients with SLC26A4 mutations. Laryngoscope. doi:10.1002/lary.25786
Lazo-Fernandez Y, Aguilera G, Pham TD et al (2015) Pendrin localizes to the adrenal medulla and modulates catecholamine release. Am J Physiol Endocrinol Metab 309:E534–E545
Lelli A, Asai Y, Forge A et al (2009) Tonotopic gradient in the developmental acquisition of sensory transduction in outer hair cells of the mouse cochlea. J Neurophysiol 101:2961–2973
Li X, Sanneman JD, Harbidge DG et al (2013a) SLC26A4 targeted to the endolymphatic sac rescues hearing and balance in Slc26a4 mutant mice. PLoS Genet 9, e1003641
Li X, Zhou F, Marcus DC et al (2013b) Endolymphatic Na+ and K+ concentrations during cochlear growth and enlargement in mice lacking Slc26a4/pendrin. PLoS One 8, e65977
Lu YC, Wu CC, Shen WS et al (2011) Establishment of a knock-in mouse model with the SLC26A4 c.919-2A > G mutation and characterization of its pathology. PLoS One 6, e22150
Lu YC, Wu CC, Yang TH et al (2013) Differences in the pathogenicity of the p.H723R mutation of the common deafness-associated SLC26A4 gene in humans and mice. PLoS One 8:e64906
Luciano L, Reiss G, Reale E (1995) The junctions of the spindle-shaped cells of the stria vascularis: a link that completes the barrier between perilymph and endolymph. Hear Res 85:199–209
Mansour SL, Schoenwolf GC (2005) Morphogenesis of the inner ear. In: Kelley MW, Wu D, Popper AN, Fay RR (eds) Development of the inner ear Springer handbook of auditory research. Springer, New York, pp 43–84
Marcus DC, Wu T, Wangemann P et al (2002) KCNJ10 (Kir4.1) potassium channel knockout abolishes endocochlear potential. Am J Physiol Cell Physiol 282:C403–C407
Miyagawa M, Nishio SY, Usami S (2014) Mutation spectrum and genotype-phenotype correlation of hearing loss patients caused by SLC26A4 mutations in the Japanese: a large cohort study. J Hum Genet 59:262–268
Nakao I, Kanaji S, Ohta S et al (2008) Identification of pendrin as a common mediator for mucus production in bronchial asthma and chronic obstructive pulmonary disease. J Immunol 180:6262–6269
Nakaya K, Harbidge DG, Wangemann P et al (2007) Lack of pendrin HCO3 − transport elevates vestibular endolymphatic [Ca2+] by inhibition of acid-sensitive TRPV5 and TRPV6. Am J Physiol Renal Physiol 292:1314–1321
Ninoyu O, Meyer zum Gottesberge AM (1986) Changes in Ca++ activity and DC potential in experimentally induced endolymphatic hydrops. Arch Otorhinolaryngol 243:106–107
Nishio A, Ito T, Cheng H et al (2016) Slc26a4 expression prevents fluctuation of hearing in a mouse model of large vestibular aqueduct syndrome. Neuroscience 329:74–82
Nordemar H (1983) Postnatal development of the vestibular sensory epithelium in the mouse. Acta Otolaryngol 96:447–456
Park HJ, Shaukat S, Liu XZ et al (2003) Origins and frequencies of SLC26A4 (PDS) mutations in east and south Asians: global implications for the epidemiology of deafness. J Med Genet 40:242–248
Pelzl L, Fakhri H, Umbach AT et al (2013) Sgk1 sensitive pendrin expression in murine platelets. Cell Physiol Biochem 32:210–220
Pryor SP, Madeo AC, Reynolds JC et al (2005) SLC26A4/PDS genotype-phenotype correlation in hearing loss with enlargement of the vestibular aqueduct (EVA): evidence that Pendred syndrome and non-syndromic EVA are distinct clinical and genetic entities. J Med Genet 42:159–165
Rillema JA, Hill MA (2003) Prolactin regulation of the pendrin-iodide transporter in the mammary gland. Am J Physiol Endocrinol Metab 284:E25–E28
Royaux IE, Suzuki K, Mori A et al (2000) Pendrin, the protein encoded by the Pendred syndrome gene (PDS), is an apical porter of iodide in the thyroid and is regulated by thyroglobulin in FRTL-5 cells. Endocrinology 141:839–845
Royaux IE, Wall SM, Karniski LP et al (2001) Pendrin, encoded by the Pendred syndrome gene, resides in the apical region of renal intercalated cells and mediates bicarbonate secretion. Proc Natl Acad Sci U S A 98:4221–4226
Royaux IE, Belyantseva IA, Wu T et al (2003) Localization and functional studies of pendrin in the mouse inner ear provide insight about the etiology of deafness in pendred syndrome. J Assoc Res Otolaryngol 4:394–404
Rozenfeld J, Tal O, Kladnitsky O et al (2012) The pendrin anion exchanger gene is transcriptionally regulated by uroguanylin: a novel enterorenal link. Am J Physiol Renal Physiol 302:F614–F624
Scott DA, Karniski LP (2000) Human pendrin expressed in Xenopus laevis oocytes mediates chloride/formate exchange. Am J Physiol Cell Physiol 278:C207–C211
Scott DA, Wang R, Kreman TM et al (1999) The Pendred syndrome gene encodes a chloride-iodide transport protein. Nat Genet 21:440–443
Singh R, Wangemann P (2008) Free radical stress mediated loss of Kcnj10 protein expression in stria vascularis contributes to deafness in Pendred syndrome mouse model. Am J Physiol Renal Physiol 294:F139–F148
Soleimani M, Greeley T, Petrovic S et al (2001) Pendrin: an apical Cl−/OH−/HCO3 − exchanger in the kidney cortex. Am J Physiol Renal Physiol 280:F356–F364
Steel KP, Barkway C (1989) Another role for melanocytes: their importance for normal stria vascularis development in the mammalian inner ear. Development 107:453–463
Sugiura M, Sato E, Nakashima T et al (2005) Long-term follow-up in patients with Pendred syndrome: vestibular, auditory and other phenotypes. Eur Arch Otorhinolaryngol 262:737–743
Suzuki K, Royaux IE, Everett LA et al (2002) Expression of PDS/Pds, the Pendred syndrome gene, in endometrium. J Clin Endocrinol Metab 87:938–941
Suzuki H, Oshima A, Tsukamoto K et al (2007) Clinical characteristics and genotype-phenotype correlation of hearing loss patients with SLC26A4 mutations. Acta Otolaryngol 127:1292–1297
Tsukada K, Nishio SY, Hattori M et al (2015) Ethnic-specific spectrum of GJB2 and SLC26A4 mutations: their origin and a literature review. Ann Otol Rhinol Laryngol 124(Suppl 1):61S–76S
Unsold B, Kerst G, Brousos H et al (2000) KCNE1 reverses the response of the human K+ channel KCNQ1 to cytosolic pH changes and alters its pharmacology and sensitivity to temperature. Pflugers Arch 441:368–378
Vanoni S, Nofziger C, Dossena S et al (2013) The human pendrin promoter contains two N(4) GAS motifs with different functional relevance. Cell Physiol Biochem 32:238–248
Vidarsson H, Westergren R, Heglind M et al (2009) The forkhead transcription factor Foxi1 is a master regulator of vacuolar H-ATPase proton pump subunits in the inner ear, kidney and epididymis. PLoS One 4, e4471
Wangemann P (2006) Supporting sensory transduction: cochlear fluid homeostasis and the endocochlear potential. J Physiol 576:11–21
Wangemann P (2013) Mouse models for pendrin-associated loss of cochlear and vestibular function. Cell Physiol Biochem 32:157–165
Wangemann P, Liu J, Marcus DC (1995) Ion transport mechanisms responsible for K+ secretion and the transepithelial voltage across marginal cells of stria vascularis in vitro. Hear Res 84:19–29
Wangemann P, Shen Z, Liu J (1996) K+-induced stimulation of K+ secretion involves activation of the IsK channel in vestibular dark cells. Hear Res 100:201–210
Wangemann P, Itza EM, Albrecht B et al (2004) Loss of KCNJ10 protein expression abolishes endocochlear potential and causes deafness in Pendred syndrome mouse model. BMC Med 2:30
Wangemann P, Nakaya K, Wu T et al (2007) Loss of cochlear HCO3 − secretion causes deafness via endolymphatic acidification and inhibition of Ca2+ reabsorption in a Pendred syndrome mouse model. Am J Physiol Renal Physiol 292:1345–1353
Wangemann P, Kim HM, Billings S et al (2009) Developmental delays consistent with cochlear hypothyroidism contribute to failure to develop hearing in mice lacking Slc26a4/pendrin expression. Am J Physiol Renal Physiol 297:F1435–F1447
Yamasaki M, Komune S, Shimozono M et al (2000) Development of monovalent ions in the endolymph in mouse cochlea. ORL J Otorhinolaryngol Relat Spec 62:241–246
Yamauchi D, Nakaya K, Raveendran NN et al (2010) Expression of epithelial calcium transport system in rat cochlea and vestibular labyrinth. BMC Physiol 10:1
Yang T, Vidarsson H, Rodrigo-Blomqvist S et al (2007) Transcriptional control of SLC26A4 is involved in Pendred syndrome and nonsyndromic enlargement of vestibular aqueduct (DFNB4). Am J Hum Genet 80:1055–1063
Yuan Y, You Y, Huang D et al (2009) Comprehensive molecular etiology analysis of nonsyndromic hearing impairment from typical areas in China. J Transl Med 7:79
Zalewski CK, Chien WW, King KA et al (2015) Vestibular dysfunction in patients with enlarged vestibular aqueduct. Otolaryngol Head Neck Surg 153:257–262
Zhou G, Gopen Q (2011) Characteristics of vestibular evoked myogenic potentials in children with enlarged vestibular aqueduct. Laryngoscope 121:220–225
Zhu J, Cao Q, Zhang N et al (2015) A study of deafness-related genetic mutations as a basis for strategies to prevent hereditary hearing loss in Hebei, China. Intractable Rare Dis Res 4:131–138
Acknowledgment
The authors thank Dr. Thomas Friedman and Dr. Michael Hoa for critical review of the manuscript. The work was supported by Kansas State University and The National Institute on Deafness and Other Communication Disorders grants NIH-R01-DC012151 to P.W. and NIH-Z01-DC000060 and NIH-Z01-DC000060 to A.J.G.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Wangemann, P., Griffith, A.J. (2017). Mouse Models Reveal the Role of Pendrin in the Inner Ear. In: Dossena, S., Paulmichl, M. (eds) The Role of Pendrin in Health and Disease. Springer, Cham. https://doi.org/10.1007/978-3-319-43287-8_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-43287-8_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43285-4
Online ISBN: 978-3-319-43287-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)