
Abstract
Otosclerosis is a unique osseous remodeling disorder of the human temporal bone, which is also considered as a disease of measles virus-associated inflammatory-autoimmune reaction against the middle layer of the otic capsule: globuli interossei. Its preoperative diagnosis is rather difficult, and there is no consensus-based diagnostic protocol with enough high sensitivity and specificity for the clinical confirmation of the disease. On the other hand, the preoperative diagnosis or clinical diagnosis of otosclerosis was potentially important considering several differential diagnostic-, prognostic-, and legal-ethical factors and problems. At this time, combination of various well-defined and new preoperative diagnostic methods might serve a strong clinical suspicion for otosclerosis. This fact might provide the basis of diagnosis and helps to avoid unnecessary stapes surgeries, serious intraoperative complications, and “blinded surgeries”: explorative tympanostomies that are unacceptable for most of the patients with conductive hearing loss. In this chapter, an overview is provided about the potential preoperative diagnostic tools and their specificity and sensitivity levels in case of otosclerosis or non-otosclerotic stapes fixations. Finally, authors recommend a considerable preoperative diagnostic protocol for the confirmation or exclusion of otosclerosis.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
3.1 Introduction
Otosclerosis is a special inflammatory bone dyscrasia of the human otic capsule, which is quite difficult to diagnose preoperatively [1, 2]. However, it is a very important question from the clinical point of view, since there are several differential diagnostic problems. Furthermore, about one-third of stapes fixations can be considered as non-otosclerotic stapes ankylosis [3]. This point time, preoperative diagnosis of otosclerosis is not resolved completely. Preoperative consensus-based diagnostic protocols are also not available. It is reasonable to say that preoperative diagnostic methods and tools only focus on stapes fixation or other middle ear pathologies [4, 5]. Therefore, in the clinical nomenclature, it is recommended to use the terms of stapes fixation or stapes ankylosis for the cases with air-bone gap (ABG) and intact tympanic membranes [3]. Nevertheless, stapes surgery and precise intraoperative findings might not really modify this recommendation, because exact diagnosis of otosclerosis is still based on the histopathologic examination of the removed stapes footplates [1–3].
Furthermore, there are several other middle or inner ear disorders that must be distinguished from stapes fixations to avoid unnecessary stapes surgery or serious intraoperative complications, such as large vestibular aqueduct, enlarged cochlear canaliculi, superior semicircular canal dehiscence syndrome (SSCCD), embryonic disorders of the hearing ossicles, stapes malformations, persisting stapedial artery, or prolapsing facial nerve into the oval window niche [6–8]. These are both differential diagnostic problems and ethical-legal issues. It can be envisioned that in the future and also today, more and more rigorous legal restrictions will apply [9, 10]. This situation requires a quick reaction from ear surgeons and a rather distinct and consensus-based preoperative diagnostic protocol or recommendation from the otologic societies [9, 10]. Precise preoperative examinations may help to avoid “blind surgery,” i.e., explorative tympanotomy [10]. We should accept and understand that most of the patients want to know the background of their hearing loss before signing an informed consent for stapes surgery [9].
Finally, a question arises: why is it so important to diagnose otosclerosis itself? The answer is hiding in the characteristics and consequences of the disease. Otosclerosis is a progressive disease of young patients with female dominancy. It can lead to serious sensorineural hearing loss in contrast to the successful stapes surgery [1, 2]. Usually, the inflammatory bone remodeling disorder affects both ears. Female patients have serious contraindications for the usage of oral anticoncipients and also for sexual hormone substitution [11, 12]. The pregnancy and family planning is another and a rather difficult question. In conclusion, the diagnosis of otosclerosis has a great prognostic value, which can modify patient’s future and quality of life in several points [11, 12].
3.2 Preoperative Diagnostic Tools
It should be established that there are no otosclerosis-specific preoperative diagnostic evaluations, which might reach enough high levels of specificity or sensitivity for the disease. However, combination of various examinations may be helpful in the differential diagnosis and can provide a rather strong clinical suspicion for otosclerosis.
Clinical diagnosis of stapes fixation is based on case history (progressive hearing loss, tinnitus, dizziness, paracusis, familial aggregation, etc.), normal otoscopic findings, negative Rinne’s test, conductive and/or mixed hearing loss, type-As tympanograms, and increased resonance frequency (>1100 Hz) confirmed by multifrequency tympanometry [13, 14]. The most exact diagnosis of otosclerosis is still based on the postoperative histopathologic analysis of the removed ankylotic stapes footplates [3, 15, 16]. However, there are several limitations: most ear surgeons prefer stapedotomy or partial stapedectomy by piston technique, which are not suitable methods to obtain whole stapes footplate specimens [17]. Furthermore, in some cases of early otosclerosis, the stapes footplate is not affected by spongiotic lesions (e.g., ligament fixation), which can lead to misdiagnosis [1, 3, 12].
3.2.1 Otomicroscopy
During the physical examination, otomicroscopy has the most important role in the first medical visit. In case of otosclerosis, we can find a normal and intact tympanic membrane. Calcification of the annulus fibrocartilaginous or small calcified patches on the tympanic membrane are not those findings which would exclude the diagnosis of otosclerosis. In some cases, active otosclerosis might be associated with Schwartze’s sign (flamingo symptom) as a consequence of hypervascularization of the promontorial mucosal lining (Fig. 3.1). It can be rarely observed, because it presumes a thin and transparent tympanic membrane [18]. This finding, however, is not specific, and its absence does not exclude existing otosclerosis.

Schwartze’s sign (otomicroscopic photograph, left ear). The white arrow indicates the promontorial hyperemia as a consequence of hypervascularization due to the reactivated bone remodeling. It is a.k.a flamingo symptom
3.2.2 Audiological Examinations
Spongiotic new bone formation in otosclerosis can result in conductive – (CHL) – and sensorineural hearing loss (SNHL) due to stapes ankylosis and pericochlear bone lesions [1, 2]. Fenestral otosclerosis is characterized by aberrant bone apposition at the fissula ante fenestram, which tends to grow toward the annular ligament (e.g., ligament fixation) and also the stapes footplate (stapes ankylosis) [1]. Retrofenestral otosclerosis can cause pure SNHL due to fine architectural changes in the modiolar and in the pericochlear bone (both apical and basal) resulting in decreased elasticity of the spiral ligament [1, 2, 19].
Complex audiologic evaluation serves as the basis of the diagnosis of CHL, mixed hearing loss (MHL), or SNHL. Subjective or objective audiological examinations, however, are not specific for otosclerosis. In contrast, they can confirm the diagnosis of stapes ankylosis or ossicular chain fixation. Nevertheless, these examinations are not suitable for the exclusion of large vestibular aqueduct or SSCCD syndrome [6]. Negative Rinne’s test (C3, 1024 Hz tuning fork) on the affected ear might confirm the diagnosis of ossicular chain fixation. It is so sensitive method that a well-experienced stapes surgeon can make a decision for surgical intervention observing this phenomenon [20, 21]. However, indication for stapes surgery is based on 30 dB ABG at 1000 Hz on pure tone audiometry (PTA) [2]. The presence of ABG is very important; however, in some cases, we can find moderate or severe sensorineural component in the hearing impairment [2]. Stapes fixation is usually associated with the presence of Carhart’s notch at 2000 Hz, which is a characteristic bone conduction threshold shift (Fig. 3.2). Its origin is not exactly known; however, it usually disappears after a successful stapes surgery [22]. Characteristics of ABG are also very important: toward the higher frequencies, it shows a decreasing level indicating the elastic rigidity of ossicular chain, which is sine qua non for stapes ankylosis (Fig. 3.2). PTA is seemingly a simple examination; however, it always requires adequate masking with white noise, which can be performed only by well-experienced audiologist [23]. Speech audiometry may be helpful and can provide valuable information about speech understanding, but it is not an obligatory audiologic examination in the preoperative diagnosis of otosclerosis. However, it is recommended in case of bone conduction threshold shift (MHL, SNHL) in order to exclude or confirm roll-over recruitment phenomenon [24]. On the other hand, speech audiometry is a mandatory examination, if hearing deteriorates after stapes surgery and we have to choose and fit hearing aid [24]. Preoperative tympanometry usually reveals type-As tympanograms in the affected ears. Its positivity varies between 44.18 % and 93.02 % [5, 14, 25, 26]. Stapedial reflexes show quite similar upper values, since stimulus-evoked stapedial reflex responses usually missing in the affected ears due to the immobilized stapes footplate. Multifrequency tympanometry (MFT) is much more sensitive for stapes fixation. It usually reveals 1100 Hz or higher resonance frequency in 95.34 % of the affected ears [5, 14, 25, 26]. Transient-evoked otoacoustic emission (TEOAE) or distortion product otoacoustic emission (DPOAE) measurements do not help the diagnosis [5]. Stapes fixations are characterized by the absent of vestibular-evoked myogenic potential (VEMP) responses triggered by air-conduction stimuli [27]. Zhou et al. have reported that abnormally low VEMP thresholds were found in 71 of 73 ears with inner ear anomalies, such as SSCCD syndrome and enlarged vestibular aqueduct [28]. According to their results, VEMP test failed to provide accurate diagnosis in only three cases [28]. These authors have stated that VEMP test is useful during clinical evaluation of various middle and inner ear pathologies, which is characterized by higher sensitivity than tympanometry or acoustic reflexes [28]. As a final conclusion, authors have recommended the routine application of VEMP test in the differential diagnosis of these disorders to avoid unnecessary middle ear surgery for ABGs with unknown causes [28].

Characteristic audiograms of clinically active and inactive (far advanced) otosclerosis. (a) Pure CHL, with Carhart’s notch. (b) MHL with severe sensorineural hearing impairment
3.2.3 Anti-measles IgG Serology (ELISA, Enzyme-Linked Immunosorbent Assay)
Otosclerosis can be considered as a persisting measles virus infection-associated inflammatory bone remodeling disorder [29–34]. The exact role of measles virus is still not clarified in the pathogenesis of otosclerosis [1, 2, 12]. Measles virus can be an inflammatory trigger (“hit and run” hypothesis) and also can be a chronic antigen-presenting factor (autoimmune hypothesis), which lead to several immunologic or autoimmune responses in the otic capsule and also in the stapes footplate [1, 2, 12].
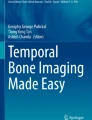
In 2006, Karosi et al. have performed a prospective case-controlled study including audiologic and histopathologic examinations and measles virus-specific RT-PCR (surgically removed whole stapes footplates) and anti-measles IgG serology in four patient groups [35]. Patient groups consisted of (1) histologically confirmed otosclerosis cases, (2) histologically confirmed non-otosclerosis cases, (3) patients with non-operated CHL, and (4) patients without otological disorders [35]. The serum levels of anti-measles IgG showed a statistically significant difference between the patients with virus-positive otosclerotic stapes footplates, virus-negative non-otosclerotic stapes footplates, and the control group (negative controls and patients with non-operated conductive hearing loss) [35]. It has been reported that anti-measles IgG levels were significantly lower in the sera of patients with measles virus-positive stapes footplate (median = 4 IU/ml) compared to the control groups [35]. In contrast, anti-measles IgG serum levels were normal in the controls (patients with virus-negative stapes footplates, median = 70 IU/ml; patients without hearing disorder, median = 40 IU/ml; and patients with non-operated CHL, median = 87 IU/ml) [35]. Analysis of anti-measles IgG serum levels in virus-positive stapes fixations and in virus-negative stapes fixations resulted an ROC curve (receiver operating characteristics) demonstrating diagnostic quality of anti-measles ELISA (area under curve = 0.979, p < 0.001, standard error = 0.01) (Fig. 3.3). Authors have found that specificity and sensitivity of anti-measles serology were 90 % and 96.2 % with 96.5 % positive and 91.1 % negative predictive values, when anti-measles IgG serum concentration was established at 12 IU/ml as a diagnostic threshold [35]. Interestingly, low levels of anti-measles IgG in case of CHL might confirm the preoperative diagnosis of otosclerosis [35, 36].

ROC curve (receiver operating characteristics) analysis of anti-measles IgG levels of patients having measles virus-positive and virus-negative stapes footplates. Specificity and sensitivity of anti-measles ELISA were 90 % and 95.5 % by establishment of 12 IU/ml anti-measles IgG concentration in the serum as diagnostic level (area under curve = 0.968; p < 0.001; standard error = 0.013; asymptotic 95 % confidence interval, 0.943–0.993; positive predictive value, 96.5 %; and negative predictive value, 91.1 %) [35]
3.2.4 High-Resolution Computed Tomography (HRCT) and Cone-Beam Computed Tomography (CBCT)
Modern imaging techniques introduced new insights into the preoperative evaluation of various osseous disorders of the human temporal bone, which have been described by several studies in otosclerosis [37–39]. High-resolution computed tomography (HRCT) scans having 0.3–0.5 mm power of resolution could detect very fine architectural changes in the otic capsule and surrounding bone structures [40] (Fig. 3.4). HRCT has also been reported as an important tool in the differential diagnosis of various middle and inner ear diseases causing conductive hearing loss, i.e., malleus head fixation, otosclerosis, and SSCCD syndrome [6, 38, 41]. Furthermore, HRCT is the main imaging method of choice in the evaluation of structural disorders in the petrous bone in cases of conductive and mixed hearing loss with normal tympanic membranes [42, 43]. HRCT is characterized by 70.5 % up to 84.2 % sensitivity levels in the detection of otosclerosis-like hypodense lesions in the otic capsule [43–45]. The specificity values of HRCT for otosclerosis, however, are not confirmed, since there are few systematic studies correlating HRCT scans to the postoperative histopathologic findings of ankylotic stapes footplates [46–48]. The diagnostic capability of HRCT is continuously developing due to the advent of more precise and higher resolution CT techniques. Preoperative detection of otosclerosis-specific hypodense lesions has great clinical significance, since it might correspond to the type, severity, and progression of hearing loss [42–45]. Furthermore, it might be a real prognostic factor in the assessment of surgical success rates according to the extension and location of otosclerotic foci [45].

Regions of interest (ROI) at HRCT scans. (a) Facial nerve and vestibular aqueduct. (b) Oval window niche. (c) Semicircular canals. (d) Round window
Cone-beam computed tomography (CBCT) is a relatively new imaging method that is widely used in the fields of endodontics and orthodontics, respectively [49, 50]. The diagnostic capability of CBCT is continuously developing due to the advent of more precise and higher resolution CT techniques and new analyzer software [49, 50]. During a CBCT scan, the single scanner and the detector rotate around the patient’s head working by a cone-shaped X-ray source that results in up to 1200–2400 distinct images [49]. The specialized scanning software collects data and produces a digital volume that can be reconstructed as three-dimensional voxels containing axial-, coronal-, and sagittal dimensions [49]. The emitted X-ray dose of CBCT is about 1 % of the conventional temporal bone HRCT scans [38, 39, 50]. The scanning procedure (20–40 s) and the reconstruction time (2 min) are significantly shorter than those in HRCT [38, 50]. There are only three papers in the literature that assessed the use of CBCT in the diagnosis of otosclerosis [47, 48, 51]. In their prospective study, Redfors et al. have compared the diagnostic values of CBCT and HRCT in patients with otosclerosis, who underwent stapedectomy 30 years ago [51]. The authors have reported that CBCT is a valuable and robust imaging method for the detection of otosclerosis-like hypodense lesions in the otic capsule, which is equivalent to HRCT in many ways [51].
There is no widely accepted HRCT grading system in the assessment of severity and extension of otosclerosis in the otic capsule [41, 52–55]. Valvassori proposed a grading system for cochlear otosclerosis based on the size and location of hypodense lesions [41]. Later, Shin et al. reported a location-based classification for the otosclerotic foci into fenestral and pericochlear groups [43]. Pericochlear lesions were divided into two subgroups (groups 1 and 2) depending on the endosteal involvement of the cochlea [43]. Kiyomizu et al. classified the lesions into five groups as follows: Group A, no pathological CT findings; Group B1, demineralization localized in the region of the fissula ante fenestram; Group B2, demineralization extending toward the cochleariform process from the anterior region of the oval window; Group B3, extensive demineralization surrounding the cochlea; and Group C, thick anterior and posterior calcified plaques [52]. Rotteveel et al. introduced the terms of “double ring effect,” “narrowed cochlear turns,” and “aberrant channels” [53]. Marshall et al. and Lee et al. proposed a clinically valuable grading system for cochlear implantation in otosclerosis, which rates fenestral and cochlear lesions together (Fig. 3.5) [54, 55]. They found significant correlation between the extent of the disease and facial nerve stimulation after activation of the cochlear implant [54].

Marshall’s HRCT grading system. (a) Grade 0 otosclerosis without manifest signs of hypodense lesions in the otic capsule (right ear). (b) Grade 1 otosclerosis with solely fenestral lesion at the anterior pole of the stapes footplate (white arrow). Focus of otosclerosis has a well-defined border at the fissula ante fenestram (right ear). (c) Grade 2a otosclerosis is featured by both fenestral (white arrow) and basal cochlear turn lesions (black arrow), (left ear). (d) Grade 2b otosclerosis is presented by both fenestral (white arrow) and apical cochlear turn foci (white empty arrow), (right ear). (e) Grade 2c otosclerosis with characteristic hypodense lesions located into the anterior pole of the stapes footplate (white arrow), and both apical (white empty arrow) and basal (black arrow) cochlear turn of the otic capsule (left ear). (f) Grade 3 otosclerosis is characterized by severe cochlear disintegration with multiple hypodense fenestral and pericochlear foci (white arrows). Disruption of the cochlear architecture is represented by black arrows (left ear) [46]
Révész et al. performed a prospective case-controlled study on 43 patients with histologically confirmed stapedial otosclerosis, who underwent unilateral stapedectomies [48]. Preoperative temporal bone CBCT and HRCT scans were performed in all cases. Both CBCT and HRCT imaging were characterized by a slice thickness of 0.4–0.625 mm and multiplanar image reconstruction. Histopathologic examination of the removed stapes footplates was performed in all cases. Findings of CBCT and HRCT were categorized according to the modified Marshall’s grading system (fenestral or retrofenestral lesions). Histopathologic results were correlated to multiplanar reconstructed CBCT and HRCT scans, respectively [48]. Negative control groups for CBCT and HRCT examinations consisted of patients, who underwent CBCT imaging due to various dental disorders or HRCT analysis due to idiopathic sudden sensorineural hearing loss. Histologically active foci of otosclerosis (n = 31, 72 %) were identified by both CBCT and HRCT in all cases with a sensitivity of 100 %. However, CBCT could not detect histologically inactive otosclerosis (n = 12, 23 %; sensitivity = 0 %) [48]. In contrast, HRCT showed inactive otosclerosis with a sensitivity of 59.3 % [48]. According to CBCT results, no retrofenestral lesions were found, and the overall sensitivity for hypodense lesions was 61.37 % [48]. They concluded that CBCT could be used only in the detection of histologically active fenestral hypodense foci of otosclerosis with high sensitivity and radiologic specificity (Figs. 3.6 and 3.7) [48].

HRCT scans of histologically confirmed otosclerosis patients. (a) Several hypodense lesions indicated by white arrows (right ear). (b) White arrow shows the thickened stapes footplate and calcified, bulky anterior pole (right ear) [46]


CBCT scans of histologically confirmed otosclerosis patients. (a) Axial, coronal, and sagittal reconstructions of CBCT images. White arrow indicates a hypodense lesion at the anterior part of the oval window niche. Yellow rectangles show the region of interest (ROI). The upper right insert represents a three-dimensional reconstruction of volume rendering (left ear). (b) CBCT scans in histologically inactive otosclerosis (right ear). Axial, coronal, and sagittal reconstructions of CBCT images. Grade 0 otosclerosis with no signs for hypodense lesions at the oval window niche (axial reconstruction, white arrow) [48]
3.3 Discussion
Otomicroscopic examination is the first and most important step in the preoperative diagnosis of stapes fixation. It is obligatory in all cases [18]. The main purpose is the exclusion of other types of middle ear disorders, which can cause CHL (chronic mesotympanic otitis, cholesteatoma, or otitis media with effusion) [18]. As we have mentioned previously, complex audiologic evaluation serves as the basis of the diagnosis of CHL, MHL, and SNHL [26]. Subjective or objective audiologic examinations, however, are not specific for otosclerosis [26]. In contrast, they can confirm the diagnosis of stapes fixation or ossicular chain fixation. Nevertheless, these examinations are not suitable for the exclusion of special disorders of the inner ear that might lead to CHL [5, 14, 24, 26].
Middle ear pathologies, such as stapes fixations and otosclerosis, are characterized by the absent of VEMP responses triggered by air-conduction stimuli. VEMP seems to be a useful test during clinical evaluation of various middle and inner ear pathologies that has been reported to have higher sensitivity than tympanometry or acoustic reflexes [27, 28]. Routine application of VEMP test is recommended in the differential diagnosis of large vestibular aqueduct or SSCCD syndrome in order to avoid unnecessary middle ear surgery for ABGs with unknown causes [28]. The exact diagnostic role of VEMP test requires further systemic examinations in the future.
According to our previous results, ELISA-based anti-measles serology is highly recommended in the preoperative evaluation of patients with suspected otosclerosis [35, 36]. The humoral immune response of patients with otosclerosis should be permissive to persisting viral replication, because anti-measles IgG level is significantly decreased in these cases [35, 36]. This permissive feature of humoral immune reaction may be characteristic for otosclerosis that can be determined genetically [56, 57]. However, it is not likely that persistently infecting measles virus could directly impair the humoral immune response [56, 57]. Vaccination against measles could decrease the incidence of otosclerosis in the future; however, in spite of worldwide vaccination, measles virus circulates in the population and can induce subclinical infections in the upper respiratory tract with primary viremia [58]. Note the new measles cases in the United States [59]. Combination of decreased anti-measles IgG serum level (<12 IU/ml) and CHL with ABG at lower frequencies has a great specificity (90 %) and sensitivity (96.2 %) as a diagnostic method in the preoperative evaluation of otosclerosis [35]. This serologic method might provide the preoperative diagnosis of otosclerosis and serves as a differential diagnostic tool distinguishing non-otosclerotic stapes fixations [35]. Genetic background of the organotropism of measles virus to the otic capsule without eliciting systemic immune response remains to be elucidated [56, 57].
The most interesting question is the role and reliability of different imaging methods in the preoperative diagnosis of otosclerosis. Since, in some cases, otosclerosis might appear as the clinical picture of idiopathic sudden sensorineural hearing loss (ISSNHL), imaging is absolutely indicated in order to exclude retrocochlear lesions [60]. If we follow this train of thought, preoperative imaging is recommended in all cases of CHL with unknown origin [47, 48, 51]. Révész et al. have demonstrated various statistical associations between CBCT and HRCT scans and audiometric findings in patients with histologically confirmed otosclerosis [48]. In contrast to the relatively low number of subjects, the paper represented a comprehensive imaging and histologic study that could assess the sensitivity and specificity levels of CBCT and HRCT scans in histologically confirmed otosclerosis [48].
Sensitivity levels of HRCT scans have been reported as 70.5–84.5 % in patients with stapes fixation [44, 46]. In histologically confirmed cases, specificity levels were estimated as 100 % [46]. Redfors et al. have reported 85 % sensitivity of CBCT scans in patients with clinical otosclerosis [51]. According to our previous observations, in the group of histologically confirmed otosclerosis, CBCT showed 61.37–65.62 % overall sensitivity, which was lower, than that of previous reports [46–48]. In case of otosclerosis, HRCT showed 76.29 % overall sensitivity, which is more robust, compared to the sensitivity levels of CBCT [48]. Révész et al. have reported that CBCT was less sensitive for non-symptomatic otosclerotic foci revealing bilateral otosclerosis as 48.83 %, in contrast to the 58.14 % prevalence revealed by PTA [48]. In contrast, HRCT showed a good correspondence (55.81 %) with audiologic findings in the clinical assessment of bilateral cases [48].
As a replication of previously published data, a statistically significant association was found between the ABG averages and CBCT grades including the location of hypodense lesions in patients with histologically confirmed otosclerosis [47, 48]. This association followed an inverse function: histologically active otosclerosis with less ABG averages was characterized by positive CBCT findings; however, histologically inactive cases with larger ABG averages displayed negative CBCT scans [47, 48]. CBCT grades did not present statistically significant association with BC averages that was independent from the histologic activity of otosclerosis. On the contrary, HRCT grades (fenestral or retrofenestral) showed a statistically significant association with ABG and BC averages in the contralateral ears and also in the histologically confirmed group of stapes footplates depending on the histologic activity of otosclerosis. Regarding to HRCT findings, in case of inactive otosclerosis, the sensorineural component of hearing impairment shows a strong correlation with the severity and extension of otosclerosis. However, it cannot be confirmed by CBCT [48].
Previous studies have reported significant association between HRCT grades and the severity of preoperative ABG [42, 44, 45]. Other reports have confirmed that extension of cochlear otosclerosis estimated by HRCT correlates with the severity of SNHL [43, 46]. Similar observations, however, are not available in case of CBCT application for the preoperative diagnosis and severity assessment of otosclerosis [47, 51]. Preoperative evaluation of the extension of otosclerosis by combined application of HRCT and audiometry has a great clinical significance, since patients with far advanced cochlear otosclerosis may have benefit from cochlear implantation rather than from stapedectomy [54]. The risk of facial nerve stimulation or mispositioning of the electrode increases in this group of patients [54, 55].
The main predictors of SNHL are the endosteal involvement and cochlear wall disruption that can be well evaluated by the simple application of HRCT [46, 54, 55]. The term of histologic otosclerosis without hearing impairment can be explained by this phenomenon: the numbers and the location of retrofenestral otosclerotic foci are not independent predictors for the severity of SNHL [3, 15, 16]. Regarding to our previous reports, CBCT grades did not present statistically significant association with BC averages in the group of ears with different histopathologic activity of otosclerosis [48]. Therefore, CBCT seems to be an ineffective imaging method in the assessment of exact disease extension and in the evaluation of progression of SNHL [48].
In histologically inactive cases of otosclerosis, CBCT displayed 0 % sensitivity, which significantly differs from that of active otosclerosis and from that of HRCT showing 59.3 % sensitivity levels [46, 47, 51]. Inactive otosclerosis is characterized by dense and calcified osteoid substance [1, 16, 61]. Since HRCT has significantly higher sensitivity for spongiotic osseous lesions, the prevalence of sclerotic foci may be underestimated [47, 49–51]. This underestimation employing HRCT does not seriously affect the diagnosis of otosclerosis itself due to the multifocal characteristics of disease with coexisting of active and inactive foci [1, 37, 38]. CBCT is much more different: it is almost blind for retrofenestral lesions and for inactive otosclerosis [48]. In case of a solely histologically inactive fenestral otosclerotic lesion, this feature of CBCT might cause a serious diagnostic problem [6, 46, 47, 50, 51]. In the lack of histologic diagnosis, inactive fenestral otosclerosis, retrofenestral otosclerosis, and non-otosclerotic stapes fixations may occur as differential diagnostic difficulties during CBCT imaging [3, 16, 46–48]. Audiometry may be helpful in differentiation, since non-otosclerotic stapes fixations usually do not associate with SNHL [26, 37, 46, 47].
According to our previous findings, CBCT scans have very low sensitivity for retrofenestral otosclerosis [46–48]. Our previous study has concluded the following as a potential explanation for this blind phenomenon: “we do think that these are distorted findings, since our patients were not characterized by significant SNHL. These audiologic findings might reveal that our patients were not affected by cochlear otosclerosis” [47]. This conclusion must be withdrawn, since in the newest study, there were several patients suffering from significant SNHL [48]. Furthermore, HRCT scans of the individual patients revealed 13 retrofenestral and 2 round window lesions caused by otosclerosis [48].
In the light of these results, preoperative HRCT scan may serve as a valuable imaging method in the planning of stapes surgery [46]. It helps to avoid serious complications and unnecessary stapes surgeries by the detection of several abnormalities in the middle or inner ear [6, 38, 46, 47]. In contrast, Redfors et al. have reported that selected anatomic structures (n = 16) were clearly reconstructed by CBCT and no discrepancies were found compared to HRCT findings [51]. These results indicate that CBCT may also serve as a choice of temporal bone imaging in case of CHL with normal tympanic membranes [51]. Nevertheless, CBCT is a cheap, easy, and a rapid imaging method that is characterized by considerably lower radiation dose than HRCT [47, 49–51].
In conclusion, temporal bone HRCT is a useful imaging method in the preoperative evaluation of different types of stapes fixations and may serve as a reliable tool in the assessment of disease extension. Its sensitivity is much higher for retrofenestral lesions and for inactive otosclerosis than that of CBCT. Therefore, it can be stated that HRCT must be the first choice of temporal bone imaging. Temporal bone CBCT is a reliable imaging method in the preoperative evaluation of histologically active fenestral otosclerosis. Its overall sensitivity falls away from that of HRCT and histologic analysis, however; it continuously improves due to the introduction of more powerful analyzer software. CBCT has a doubtful correlation with hearing thresholds that depends on the histopathologic activity, the grading system, and the size of subject group. Finally, further studies are necessary to assess the precise diagnostic values of these imaging techniques.
3.4 Recommended Preoperative Diagnostic Protocol
This is a subjective, however, experience-based recommendation of the authors, which requires consensus by the national otologic societies. This recommendation considers the clinical, surgical, and also legal conditions and questions [9, 10] (Fig. 3.8).

Schematic representation of recommended diagnostic protocol for preoperative evaluation of otosclerosis
-
1.
Obtain a correct and precise patient’s history (note the familial aggregation).
-
2.
Perform otomicroscopy.
-
3.
Perform subjective and objective audiologic examinations (tuning fork tests, PTA, speech audiometry, tympanometry, MFT, and VEMP).
-
4.
Analyze the anti-measles IgG serum level of the patient suspected for otosclerosis (whole blood sample without anticoagulant – ELISA).
-
5.
Perform preoperative imaging (HRCT or CBCT) and analyze precisely the regions of interest.
-
6.
Communicate with the radiologist/neuro-radiologist.
References
Chole RA, McKenna M. Pathophysiology of otosclerosis. Otol Neurotol. 2001;22:249–57.
Sziklai I, Batta TJ, Karosi T. Otosclerosis: an organ-specific inflammatory disease with sensorineural hearing loss. Eur Arch Otorhinolaryngol. 2009;266:1711–8.
Karosi T, Csomor P, Petkó M, Liktor B, Szabó LZ, Pytel J, Jóri J, Sziklai I. Histopathology of nonotosclerotic stapes fixations. Otol Neurotol. 2009;30:1058–66.
Redfors YD, Möller C. Otosclerosis: thirty-year follow-up after surgery. Ann Otol Rhinol Laryngol. 2011;9:608–14.
Mantzari E, Maragoudakis P, Kandiloros D, Ferekidis E, Korres SG. The profile of otoacoustic emissions and multifrequency tympanometry in otosclerotic patients undergoing two types of stapes surgery: small fenestra and microtraumatic stapedotomy. Med Sci Monit. 2014;20:1613–20.
Merchant SN, Rosowski JJ, McKenna MJ. Superior semicircular canal dehiscence mimicking otosclerotic hearing loss. Adv Otorhinolaryngol. 2007;65:137–45.
Moskowitz HS. Book review: review of otosclerosis diagnosis, evaluation, pathology, surgical techniques, and outcomes. Ann Otol Rhinol Laryngol. 2015;3:250–1.
Sugimoto H, Ito M, Hatano M, Yoshizaki T. Persistent stapedial artery with stapes ankylosis. Auris Nasus Larynx. 2014;6:582–5.
Ruhl DS, Hong SS, Littlefield PD. Lessons learned in otologic surgery: 30 years of malpractice cases in the United States. Otol Neurotol. 2013;7:1173–9.
Blake DM, Svider PF, Carniol ET, Mauro AC, Eloy JA, Jyung RW. Malpractice in otology. Otolaryngol Head Neck Surg. 2013;4:554–61.
Liktor B, Szekanecz Z, Batta TJ, Sziklai I, Karosi T. Perspectives of pharmacological treatment in otosclerosis. Eur Arch Otorhinolaryngol. 2013;3:793–804.
Karosi T, Sziklai I. Etiopathogenesis of otosclerosis. Eur Arch Otorhinolaryngol. 2010;9:1337–49.
Sanford CA, Schooling T, Frymark T. Determining the presence or absence of middle ear disorders: an evidence-based systematic review on the diagnostic accuracy of selected assessment instruments. Am J Audiol. 2012;2:251–68.
Shahnaz N, Bork K, Polka L, Longridge N, Bell D, Westerberg BD. Energy reflectance and tympanometry in normal and otosclerotic ears. Ear Hear. 2009;2:219–33.
Declau F, van Spaendonck M, Timmermans JP, Michaels L, Liang J, Qiu JP, van de Heyning P. Prevalence of histologic otosclerosis: an unbiased temporal bone study in Caucasians. Adv Otorhinolaryngol. 2007;65:6–16.
Iyer PV, Gristwood RE. Histopathology of the stapes in otosclerosis. Pathology. 1984;16:30–8.
Kamalski DM, Wegner I, Tange RA, Vincent R, Stegeman I, van der Heijden GJ, Grolman W. Outcomes of different laser types in laser-assisted stapedotomy: a systematic review. Otol Neurotol. 2014;6:1046–51.
Nakashima T, Sone M, Fujii H, Teranishi M, Yamamoto H, Otake H, Sugiura M, Naganawa S. Blood flow to the promontory in cochlear otosclerosis. Clin Otolaryngol. 2006;2:110–5.
Sellari-Franceschini S, Ravecca F, De Vito A, Berrettini S. Progressive sensorineural hearing loss in cochlear otosclerosis. Acta Otorhinolaryngol Ital. 1998;18:59–65.
MacKechnie CA, Greenberg JJ, Gerkin RC, McCall AA, Hirsch BE, Durrant JD, Raz Y. Rinne revisited: steel versus aluminum tuning forks. Otolaryngol Head Neck Surg. 2013;6:907–13.
Gordon MA, Silverstein H, Willcox TO, Rosenberg SI. A reevaluation of the 512-Hz Rinne tuning fork test as a patient selection criterion for laser stapedotomy. Am J Otol. 1998;6:712–7.
Kashio A, Ito K, Kakigi A, Karino S, Iwasaki S, Sakamoto T, Yasui T, Suzuki M, Yamasoba T. Carhart notch 2-kHz bone conduction threshold dip: a nondefinitive predictor of stapes fixation in conductive hearing loss with normal tympanic membrane. Arch Otolaryngol Head Neck Surg. 2011;3:236–40.
Miller MH. How to eliminate air-bone gaps audiometrically: use too much masking. Ear Nose Throat J. 2008;5:273–6.
Abdelghaffar H, Fakhry S, Fawzy T. Aided air conduction threshold as a predictor of cochlear reserve in otosclerosis patients. ORL J Otorhinolaryngol Relat Spec. 2010;1:12–5.
Miani C, Bergamin AM, Barotti A, Isola M. Multifrequency multicomponent tympanometry in normal and otosclerotic ears. Scand Audiol. 2000;4:225–37.
Probst R. Audiological evaluation of patients with otosclerosis. Adv Otorhinolaryngol. 2007;65:119–26.
Tramontani O, Gkoritsa E, Ferekidis E, Korres SG. Contribution of Vestibular-Evoked Myogenic Potential (VEMP) testing in the assessment and the differential diagnosis of otosclerosis. Med Sci Monit. 2014;20:205–13.
Zhou G, Poe D, Gopen Q. Clinical use of vestibular evoked myogenic potentials in the evaluation of patients with air-bone gaps. Otol Neurotol. 2012;8:1368–74.
Arnold W, Niedermeyer HP, Lehn N, Neubert W, Höfler H. Measles virus in otosclerosis and the specific immune response of the inner ear. Acta Otolaryngol. 1996;116:705–9.
Niedermeyer HP, Arnold W. Otosclerosis: a measles virus associated inflammatory disease. Acta Otolaryngol. 1995;115:300–3.
Karosi T, Kónya J, Petkó M, Sziklai I. Histologic otosclerosis is associated with the presence of measles virus in the stapes footplate. Otol Neurotol. 2005;26:1128–33.
Arnold W, Friedmann I. Otosclerosis – an inflammatory disease of the otic capsule of viral aetiology? J Laryngol Otol. 1988;102:865–71.
McKenna MJ, Mills BG. Ultrastructural and immunohistochemical evidence of measles virus in active otosclerosis. Acta Otolaryngol Suppl. 1990;470:130–40.
Niedermeyer HP, Arnold W, Schuster M, Baumann C, Kramer J, Neubert WJ, Sedlmeier R. Persistent measles virus infection and otosclerosis. Ann Otol Rhinol Laryngol. 2001;110:897–903.
Karosi T, Kónya J, Petkó M, Szabó LZ, Pytel J, Jóri J, Sziklai I. Antimeasles IgG for serologic diagnosis of otosclerotic hearing loss. Laryngoscope. 2006;116:488–93.
Lolov SR, Encheva VI, Kyurkchiev SD, Edrev GE, Kehayov IR. Antimeasles immunoglobulin G in sera of patients with otosclerosis is lower than that in healthy people. Otol Neurotol. 2001;22:766–70.
Mafee MF, Henrikson GC, Deitch RL, Norouzi P, Kumar A, Kriz R, Valvassori GE. Use of CT in stapedial otosclerosis. Radiology. 1985;156:709–14.
Shaffer KA, Haughton VM, Wilson CR. High resolution computed tomography of the temporal bone. Radiology. 1980;134:409–14.
Grayeli AB, Yrieix CS, Imauchi Y, Cyna-Gorse F, Ferrary E, Sterkers O. Temporal bone density measurements using CT in otosclerosis. Acta Otolaryngol. 2004;124:1136–40.
Lagleyre S, Sorrentino T, Calmels MN, Shin YJ, Escudé B, Deguine O, Fraysse B. Reliability of high-resolution CT scan in diagnosis of otosclerosis. Otol Neurotol. 2009;30:1152–9.
Valvassori GE. Imaging of otosclerosis. Otolaryngol Clin N Am. 1993;26:359–71.
Naumann IC, Porcellini B, Fisch U. Otosclerosis: incidence of positive findings on high-resolution computed tomography and their correlation to audiological test data. Ann Otol Rhinol Laryngol. 2005;114:709–16.
Shin YJ, Fraysse B, Deguine O, Cognard C, Charlet JP, Sévely A. Sensorineural hearing loss and otosclerosis: a clinical and radiologic survey of 437 cases. Acta Otolaryngol. 2001;121:200–4.
Marx M, Lagleyre S, Escudé B, Demeslay J, Elhadi T, Deguine O, Fraysse B. Correlations between CT scan findings and hearing thresholds in otosclerosis. Acta Otolaryngol. 2011;131:351–7.
Wycherly BJ, Berkowitz F, Noone AM, Kim HJ. Computed tomography and otosclerosis: a practical method to correlate the sites affected to hearing loss. Ann Otol Rhinol Laryngol. 2010;119:789–94.
Karosi T, Csomor P, Sziklai I. The value of HRCT in stapes fixations corresponding to hearing thresholds and histologic findings. Otol Neurotol. 2012;8:1300–7.
Liktor B, Révész P, Csomor P, Gerlinger I, Sziklai I, Karosi T. Diagnostic value of cone-beam CT in histologically confirmed otosclerosis. Eur Arch Otorhinolaryngol. 2014;8:2131–8.
Révész P, Liktor B, Liktor B, Sziklai I, Gerlinger I, Karosi T. Comparative analysis of preoperative diagnostic values of HRCT and CBCT in patients with histologically diagnosed otosclerotic stapes footplates. Eur Arch Otorhinolaryngol. 2016 Jan;273(1):63–72. http://www.ncbi.nlm.nih.gov/pubmed/25559466 doi: 10.1007/s00405-015-3490-3. Epub 2015 Jan 6. PMID: 25559466.
Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40:818–30.
Small BW. Cone beam computed tomography. Gen Dent. 2007;55:179–81.
Redfors YD, Gröndahl HG, Hellgren J, Lindfors N, Nilsson I, Möller C. Otosclerosis: anatomy and pathology in the temporal bone assessed by multi-slice and cone-beam CT. Otol Neurotol. 2012;33:922–7.
Kiyomizu K, Tono T, Yang D, Haruta A, Kodama T, Komune S. Correlation of CT analysis and audiometry in Japanese otosclerosis. Auris Nasus Larynx. 2004;31:125–9.
Rotteveel LJ, Proops DW, Ramsden RT, Saeed SR, van Olphen AF, Mylanus EA. Cochlear implantation in 53 patients with otosclerosis: demographics, computed tomographic scanning, surgery, and complications. Otol Neurotol. 2004;25:943–52.
Marshall AH, Fanning N, Symons S, Shipp D, Chen JM, Nedzelski JM. Cochlear implantation in cochlear otosclerosis. Laryngoscope. 2005;115:1728–33.
Lee TC, Aviv RI, Chen JM, Nedzelski JM, Fox AJ, Symons SP. CT grading of otosclerosis. Am J Neuroradiol. 2009;30:1435–9.
Karosi T, Jokay I, Konya J, Petko M, Szabo LZ, Sziklai I. Expression of measles virus receptors in otosclerotic, non-otosclerotic and in normal stapes footplates. Eur Arch Otorhinolaryngol. 2007;264:607–13.
Karosi T, Szalmas A, Csomor P, Konya J, Petko M, Sziklai I. Disease-associated novel CD46 splicing variants and pathologic bone remodeling in otosclerosis. Laryngoscope. 2008;118:1669–76.
Arnold W, Busch R, Arnold A, Ritscher B, Neiss A, Niedermeyer HP. The influence of measles vaccination on the incidence of otosclerosis in Germany. Eur Arch Otorhinolaryngol. 2007;264:741–8.
Liu F, Enanoria WT, Zipprich J, Blumberg S, Harriman K, Ackley SF, Wheaton WD, Allpress JL, Porco TC. The role of vaccination coverage, individual behaviors, and the public health response in the control of measles epidemics: an agent-based simulation for California. BMC Public Health. 2015;1:447.
Schuknecht HF. Myths in neurotology. Am J Otol. 1992;2:124–6.
Parahy C, Linthicum Jr FH. Otosclerosis and otospongiosis: clinical and histological comparisons. Laryngoscope. 1984;94:508–12.
Acknowledgments
Some parts of this chapter are based on previous publications of the authors. According to scientific ethical restrictions, authors have obtained the permission for reusage of these data from Springer Scientific Publishing Group under the license numbers of 3620630353370 and 3620711246137, respectively.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Karosi, T., Sziklai, I. (2016). Preoperative Diagnosis of Otosclerosis. In: Sziklai, I. (eds) Surgery of Stapes Fixations. Springer, Cham. https://doi.org/10.1007/978-3-319-28576-4_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-28576-4_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-28574-0
Online ISBN: 978-3-319-28576-4
eBook Packages: MedicineMedicine (R0)