
Abstract
Otosclerosis is a bone remodeling disorder of complex etiology. Persistent measles virus infection of the otic capsule could increase the expression level of measles virus receptors (CD46) on the osteoclasts and endothelial cells of the otosclerotic foci. Presence of measles virus RNA was demonstrated in the footplates of histologically diagnosed otosclerotic patients by RT–PCR; however, no reports were available about the CD46 expression pattern and level in otosclerosis. Nucleic acid was extracted from stapes footplates of clinically otosclerotic patients (N = 116). Genomic RNA of measles virus was amplified by RT–PCR. Amplification results were correlated with postoperative histologic and CD46 specific immunhistologic findings. Among 116 stapes fixation cases, 87 otosclerotic stapes contained measles virus RNA. Histology for virus negative stapes (N = 29) represented degenerative disorders with heterogeneous histopathology. Active otosclerosis was featured by increased numbers of osteoclasts showing strong CD46 expression. In virus negative, non-otosclerotic stapes fixation and in normal stapes footplates weak CD46 immunoreaction was demonstrated on the osteocytes and fibroblasts. In otosclerosis, it is reasonable to assume that measles virus increases the expression level of its own cellular receptor. Furthermore, intensive CD46 reaction could relate to active virus replication and continuous receptor internalisation. Otosclerosis is a disease of disturbed osteoid turnover due to persistent measles virus infection and special CD46 receptor pattern of the otic capsule.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Otosclerosis (otospongiosis) is a special bone remodeling disorder with complex etiology causing progressive conductive and sensorineural hearing loss [1, 2]. In the Caucasian population the prevalence of clinical otosclerosis (symptomatic hearing loss of conductive type) is 0.3–0.4% of the general population and 9–21% of those with conductive hearing loss [1]. Histological otosclerosis is about ten times as common as clinical otosclerosis (3–4%) [1, 3].
The characteristic histologic findings in active otosclerosis occur only in the otic capsule [1–3] and are featured by focal, resorptive bone lesions with high cellularity and vascularisation in the pericochlear region, near the oval window and in the stapes footplate [1, 4]. The wide pseudovascular spaces are filled with numerous plump and misshapen osteoclasts, multinucleated giant cells, fibroblasts and proliferating endothelial cells [3, 4]. A most important feature of otosclerosis is the character of the ground and pattern of extracellular matrix. In otosclerosis, the amount of woven and basophilic osteoid substance is increased [1]. The histologic changes of active otosclerosis are quite similar to those of Paget’s disease [1, 3, 5]. The precocious active stage may be followed by intermediate and inactive stages, in which the histological appearances show very little or no recognisable evidence of the lesion [1, 3].
The etiologic role of measles virus arose in the pathogenesis of the otosclerosis in the past 20 years [2, 6]. Measles virus is a wide-spread Paramyxovirus with RNA genome [7]. The presence of measles virus in otosclerotic stapes footplates was shown by RT–PCR [8, 9]. Virus-like pleomorphic structures have been recognised in the osteoclasts of otosclerotic foci by electronmicroscopy [10]. Measles virus derived proteins have been detected on the surface of osteoclasts, chondrocytes and the proliferating endothelial cells of the otosclerotic foci [11, 12]. Measles virus specific immunoglobulin G has been detected in the otosclerotic perilymph [6, 12].
One of the human cellular receptors of measles virus is the CD46 molecule (MCP—membrane cofactor protein), which has cofactor activity for inactivation of complement components C3b and C4b by serum factor I, which protects the host cell from damage by complement [13, 14]. All nucleated human cells coexpress multiple CD46 isoforms; however, no functions have been attributed to isoform coexpression [14]. CD46 is strongly expressed on epithelial cells, fibroblasts and chondrocytes; moderately on lymphocytes and endothelium and weakly on osteoclasts and osteocytes [14, 15]. The effect of CD46 on reduction of inflammatory IL-12 production may be especially important in the immunosuppressive sequel of measles virus infections [16, 17].
This study investigated the distribution pattern and expression level of CD46—measles virus binding receptor—in otosclerotic, non-otosclerotic and in normal stapes footplate specimens in conjunction with measles virus nucleoprotein RNA specific RT–PCR results.
Materials and methods
Patients
A total of 116 ankylotic stapes footplate samples (N = 116, male = 38, female = 78) removed during stapedectomies was analysed. Patients included in this study gave their informed consent to all molecular, histological and serological examinations of their stapes and serum specimens. The mean age of clinically stapes fixation patients was 37.33 years (range: 19–67 years). The diagnosis of stapes fixation was based on clinical, audiometric and tympanometric findings. Air-bone gap at 1,000 Hz was at least 30 dB. None of the patients remembered measles virus infection in childhood; however, 31 patients (born after 1969) had documented anti-measles vaccination. These patients were absolutely different from those reported in previous studies. Twenty-five cadaver stapes specimens with negative otopathologic history were employed as negative controls of otosclerotic patients (N = 25, male = 12, female = 13). The mean age of negative controls was 51.85 years (range: 42–69 years). Present study has been approved by local (University of Debrecen) and national ethical committees (Hungarian Scientific and Research Ethical Committee).
Histology and CD46 (measles virus receptor) specific immunohistochemistry
A total of 116 ankylotic stapes specimens (N = 116, 93 complete stapes and 23 complete stapes footplates) and 25 normal stapes (N = 25) were fixed in 10% buffered formalin and decalcified in 0.5 M Na-EDTA (sodium ethylene-diamino-tetraacetate, 72 h, 4°C). Specimens were embedded in 15% purified gelatine (24 h, 56°C) and refixed in 4% paraformaldehyde (24 h, 20°C). Blocks were cryoprotected in 20% sacharose-solution (2 h, 4°C) and sectioned by a cryomicrotome into 10 μm slides (−25°C). Slides were stored in 0.1 M PBS (phosphate-buffered saline) containing sodium-azide at 4°C. One stapes was grouped of three consecutive, 10 μm frozen cut sections that were examined as follows. First sections were processed for nucleic acid extraction and RT–PCR amplification, second ones were stained by haematoxylin–eosin and the last third ones were processed for CD46 specific immunohistochemistry.
The third ones of sections were washed in 0.2 M PBS containing goat normal serum as blocking component. Blocked sections were incubated with 0.2 mg/ml goat anti-human CD46 (MCP) primary antibody solution (20°C, 48 h, continuous shaking) (R&D Systems, UK). Primary antibody was washed with 0.2 M PBS and sections were incubated with 0.008 mg/ml mouse (15H6 clone) anti-goat FITC (fluorescein isothiocyanate isomer 1) labelled IgG1κ solution (20°C, 12 h, continuous shaking) (Southern Biotech, Birmingham, AL, USA). Slides were covered by UV transparent mounting medium (Vectashield, Vector Laboratories, CA, USA). Imaging was performed under UV-light with a 96–123 ms exposure time and the photographs were archived in jpeg file format (Axioskop2 MOT, Axiovision 3.0, Zeiss, Jena, Germany). Intensity of immunoreactions was featured by relative luminosity, which was calculated by a post processing PC software (Quantity One 1-D Analysis, Bio-Rad, USA). Histologic specimens were independently analysed by T.K. and M.P.
Nucleic acid extraction from histologic slides and RT–PCR detection of measles virus RNA
Histologic slides were frozen in liquid nitrogen and pulverised in a sterile, dry rubber cup. The pulverised tissue was suspended in DEPC (diethyl-pirocarbonate) treated thermo-sterilised distilled water. Human and viral nucleic acids (mRNA, vRNA, DNA) were extracted by a nucleic acid isolation kit according to the manufacturer’s instructions (High Pure Viral Nucleic Acid Kit, Roche, Basel, Switzerland). The nucleic acid extraction method used in this study consists of pulverisation of the stapes footplates, enzymatic release of nucleic acids from the protein matrix, spinning the gross insoluble material and affinity purification of the nucleic acids. The latter step is performed with a filter device that removes any insoluble material left after spinning and ensures the elution of purified nucleic acids [9].
Genomic nucleoprotein (NP) RNA of measles virus was detected by RT–PCR amplification using NP RNA specific primers (MV2 5′–3′: GTTCTTCCGAGATTCCTGCCA and MV3 5′–3′: GCATCTGAACTCGGTATCAC) [9]. rTth reverse-transcriptase and DNA-polymerase enzyme (Applied Biosystems, Lincoln, Foster City, USA) was used by RT–PCR (reverse transcriptase) and cDNA-PCR [9]. First round cDNA was amplified in the second round, semi-nested polymerase chain reaction. Red Taq DNA-polymerase (Sigma-Aldrich, Missouri, St. Louis, USA) was used in this reaction [9]. In the semi-nested PCR, two measles virus NP RNA specific primer combinations were employed (MV3 and MV4 5′–3′: AGCTCTCGCATCACTTGCTCT; MV2 and NP14 5′–3′: GCAAGGAAGATAGGAGGGTC) [9]. The suitability of extracted RNA samples for RT–PCR detection of measles virus RNA was tested by using h36B4+ (5′–3′: AGATGCAGCAGATCCGCAT) and h36B4− (5′–3′: ATATGAGGCAGGAGTTTCTCCAG) primer set targeting human ribosomal RNA [9]. Enhanced Avian reverse-transcriptase (Sigma-Aldrich) and Genomic Red Taq DNA-polymerase (Sigma-Aldrich) were used in the cellular control RT–PCR [9]. Live, attenuated, Edmonston-type measles virus was employed as a positive control of otosclerotic stapes footplate specimens. Cortical bone fragments (N = 51) removed during stapedectomies (external auditory meatus) and non-otosclerotic cadaver stapes samples (N = 31) were used as negative controls.
Results
Consecutive sections were subjected to histologic examination and nucleic acid extraction, respectively. Histologic diagnosis of otosclerosis was established in 87 ankylotic stapes footplates [3, 4] (Figs. 1, 2, 3). Among these patients, the otosclerotic foci were seen to be active in 59 stapes footplates and inactive in 28 cases [3, 4] (Fig. 3). The localisation of otosclerotic foci was different among the 87 patients with manifest involvement of the stapedial footplate by otosclerosis at the anterior pole (N = 43), posterior pole (N = 21), bipolar (N = 9) or obliteration (N = 14) (Table 1). We did not analyse partial stapes or stapes footplates because the anterior or posterior poles containing the fixative bone lesions were retained in the oval window niche. In the 29 non-otosclerotic stapes footplates, histologic examinations revealed annular, stapediovestibular calcification (N = 21) and polar, stapediovestibular fibrosis with thickened stapedial mucosal layer (N = 8) (Fig. 4).

CD46 specific immunohistologic findings in a small otosclerotic focus at the anterior pole of the stapes footplate. a Hypervascularised, hypercellular otosclerotic focus showing strong CD46 positivity (RL: relative luminosity, 3.59) compared to the surrounding normal bone (white arrow heads). Focus of otosclerosis invades to the annular ligament (AL) and destroys the vestibular hyalin cartilage (white arrow). The white star indicates the stapediovestibular space. b Phase contrast view of the previous section showing the sharp osteolytic boundary of the lesion. c Merged view of the previous sections showing CD46 positive cells and borders of the otosclerotic focus. d High power magnification view of the injured hyaline cartilage layer (rectangular area of the previous section). Chondrocytes disappeared from the frontline of otosclerotic lesion; only empty cellular spaces can be seen (white arrows)

Immunohistologic demonstration of CD46 expression in a large obliterative otosclerotic lesion. a Focus of active otosclerosis has sharply defined osteolytic boundary. The lesion forming cells and vascular endothelium represent intensive CD46 positivity (RL: relative luminosity, 3.45). White arrows indicate a CD46 positive cell migrating from the lesion into the anterior crus (AC). White arrow head indicates normal osteocytes with annular CD46 expression. AP anterior pole. b Phase contrast microscopic view of the previous section. The cement lines show irregular, gland-like pattern. White arrows show the migrating cell. c Incipient otosclerotic lesion (white stars) at the posterior pole (PP) of the stapes footplate. The hyalin cartilage layer is bulky trabeculated structure with undefined margins. Chondrocytes show strong CD46 positivity (RL: relative luminosity, 4.58). AL: annular ligament. d Phase contrast microscopic view of the previous section. The pathologic bone is represented by vortical structure surrounded by concentric, woven osteoid lamellas (white arrows)

Immunohistologic representation of CD46 expression in different stages of otosclerosis. a Inactive otosclerosis with destroyed perifocal hyalin cartilage layer (white arrow heads). The rests of chondrocytes show rather intensive, granular CD46 reaction. White arrow indicates the vestibular surface of the stapes footplate. b Deformed hyalin cartilage layer of a trabeculated structure in the stapes footplate, which takes place near an otosclerotic focus (white arrow heads). Pathologic chondrocytes show much more intensive CD46 expression compared to the surrounding normal cells (RL: relative luminosity, 3.97). White star indicates the middle layer of the stapes footplate, while white arrows show the periosteal and enchondral layers. c Otosclerotic focus with moderate activity. Wide pseudovascular spaces (white stars) are present. Heterogeneous cell groups showing weak annular [(osteocytes) RL1: relative luminosity1, 1.21] and intensive granular [(osteoclasts) RL2: relative luminosity2, 3.63] CD46 expression can be seen. d Active, hypervascularised and hypercellular otosclerotic lesion with confluent CD46 positive reaction (RL: relative luminosity, 4.19). Pseudovascular spaces are filled with CD46 positive osteoclasts

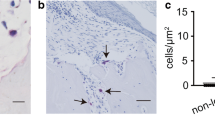
CD46 specific immunohistologic findings in non-otosclerotic stapes ankylosis and in a normal stapes. a Annular calcification with weak CD46 reaction (RL: 1.23) at the anterior pole (AP) of the thickened stapes footplate (FP). The anterior crus (AC) is normal in appearance. White arrow shows the stapediovestibular surface. White arrow head indicates a dilated blood vessel with CD46 positive endothelium. b Stapediovestibular fibrosis with deformed and bulky anterior pole (AP), thickened stapes footplate (FP) and anterior crus (AC). Annular ligament (AL) is a CD46 positive robust structure. White arrow shows the distorted stapediovestibular joint. White arrow head shows the middle ear surface of the stapes with a lacuna filled with fibrous tissue. c Annular calcification at the posterior pole of the stapes footplate, which has angled edges. There are few osteocytes with weak CD46 reaction in the dark osteoid background (RL: 1.11). Hyaline cartilage layer is shown by white arrow heads. White arrow indicates the thickened middle ear mucosa. d The normal stapes is usually hypocellular and hypovascularised tissue and featured by homogeneous osteoid structure. There are few monomorph osteocytes with marked CD46 receptor expression in the anterior pole (AP) and anterior crus (AC) of the stapes. White arrows show the CD46 positive hyalin cartilage layer of the vestibular and annular surface of the stapes footplate (FP). White arrow head indicates the middle ear mucosal layer with strong CD46 expression
It was shown that the histologic lesions of stapes footplates correlate well with measles virus RNA specific RT–PCR results (Table 1). Measles virus nucleoprotein (NP) RNA sequences were detected in all otosclerotic lesions (N = 87) (Table 1). None of the 29 non-otosclerotic, ankylotic stapes contained measles virus RNA (Table 1). Human cellular RNA was successfully detected by cellular control RT–PCR in each of the 141 stapes footplates and control bone specimens, therefore all samples were eligible for testing the presence of measles virus RNA. Cortical bone fragments (N = 51) and non-otosclerotic cadaver stapes specimens (N = 31) employed as negative controls did not contain measles virus RNA.
Chondrocytes of the vestibular, hyaline cartilage layer of each stapes footplate showed considerable positivity on CD46 antigen complex (Figs. 1, 4). This is not unexpected, since these cells are reported to show strong CD46 expression level [5, 14, 15]. Otosclerosis was represented by increased numbers of cellular elements showing very strong CD46 expression (Figs. 2, 3). Osteoclasts, osteoblasts, fibroblasts and proliferating endothelial cells of the otosclerotic foci showed homogeneous, intensive CD46 reaction, which was dependent from the histologic activity of otosclerosis (Fig. 3). Active otosclerosis was represented by wide pseudovascular spaces filled with increased numbers of large, misshapen and multinucleated osteoclasts with very strong granular CD46 expression (Fig. 3). Advanced, inactive stages of otosclerosis were marked by obliterated vascular spaces and resorption lacunae with decreased numbers of osteoclasts showing quite intensive CD46 reaction similar to those observed in the hyalin cartilage layer of the vestibular surface (Fig. 3). The normal hyalin cartilage layer of the stapes footplate was sharply destroyed by the otosclerotic lesion; vanished chondrocytes in the peripheral zone were represented as empty halos (Figs. 1, 3). There was a considerable increased CD46 expression in chondrocytes of the frontline of otosclerotic foci (Fig. 2). In contrast, in non-otosclerotic stapes fixation (N = 29) and in normal cadaver stapes footplates (N = 25) a weak CD46 reaction was demonstrated on the surface of osteocytes, osteoblasts and vascular endothelial cells (Fig. 4).
Discussion
Present study supplies additional information for the presence of measles virus in the stapes footplate specimens from patients with clinically and histologically diagnosed otosclerosis in conjunction with CD46 receptor expression pattern. The failure to detect measles virus nucleoprotein RNA in stapes footplates was associated with histologically non-otosclerotic stapes fixation. Otosclerosis is an inflammatory disease due to persistent measles virus infection of the otic capsule, while measles virus negative, ankylotic stapes footplates are featured as degenerative disorders with variable histopathology.
CD46 usually shows low expression level in different bony tissues [15]. It is weakly expressed on the surface of osteoclasts, osteoblasts and osteocytes [5]. Present observations provide evidence for the increased expression of measles virus binding CD46 receptors in otosclerotic stapes footplates. Since the osteoclasts and osteocytes of measles virus negative non-otosclerotic and normal stapes footplates are featured by low CD46 immunoreaction, there should be specific correlation between measles virus infection and expression level of virus binding receptors. Measles virus having viral transcription factors is potentially able to increase the expression of its own cellular receptor [16, 17]. Furthermore, intensive CD46 immunoreaction could be related to active virus replication and continuous receptor internalisation in the infected osteoclasts and endothelium [7]. However, in a persistent infection the viral replication is reduced to a very low level. Additionally, in active otosclerosis all signs of a chronic inflammation are present. In this condition overexpression of CD46 should be assumed, too.
Measles virus shows organotropism to the otic capsule that could be explained by the special pattern of paramyxovirus favouring receptor isoforms in this region. Although at this time, no distinct functions have been reported to tissue-specific CD46 isoforms and the variable levels of expression [7, 14, 15]. The absence of animal model also emphasises the role of measles virus in the genesis of otosclerosis, since small mammals do not possess measles binding protein CD46 [7, 14].
The humoral immune system of otosclerotic patients could be permissive to persisting virus replication, because anti-measles IgG level is significantly decreased in sera of these cases [18]. Patients with virus positive, otosclerotic stapes footplate have very low or missing anti-measles IgG level in the serum [18, 19]. It is an independent feature from previous antimeasles vaccination or measles virus infection [19]. On the other hand, patients with pseudo-otosclerosis (virus negative stapes fixation) show seroconversion against measles virus antigens and have normally high IgG serum levels due to antimeasles vaccination or manifest measles virus infection [19]. This permissive feature of humoral immune reaction may be characteristic in otosclerosis that can be determined by expression of different CD46 isoforms [14]. Crosslinking CD46 isoforms downregulate IL-12 production, via unknown mechanisms [16, 17]. Nevertheless, IL-12 is a very important cytokine regulator of immunoglobulin production and memory B-cell reactivation [16, 17].
In summary, otosclerosis is a disease of increased osteoid turnover due to persistent measles virus infection and consecutive CD46 receptor overexpression with an osteoclast favouring pattern in the otic capsule.
References
Friedmann I (1974) Pathology of the ear. Blackwell Scientific Publications, Oxford
Chole RA, McKenna M (2001) Pathophysiology of otosclerosis. Otol Neurotol 22(2):249–257
Iyer V, Gristwood H (1984) Histopathology of the stapes in otosclerosis. Pathol 16:30–38
Linthicum FH Jr (1993) Histopathology of otosclerosis. Otolaryngol Clin North Am 26(3):335–352
Reddy SV, Kurihara N, Menaa C, Landucci G, Forthal D, Koop BA, Windle JJ, Roodman GD (2001) Osteoclasts formed by measles virus-infected osteoclast precursors from hCD46 transgenic mice express characteristics of Pagetic osteoclasts. Endocrinology 142(7):2898–2905
Arnold W, Niedermeyer HP, Lehn N, Neubert W, Höfler H (1996) Measles virus in otosclerosis and the specific immune response of the inner ear. Acta Otolaryngol (Stockh) 116:705–709
Norrby E, Oxman MN (1990) Measles virus. In: Fields BN, Knipe DM (eds) Fields virology. Raven Press, New York, pp 1013–1044
McKenna MJ, Kristiansen AG, Haines J (1996) Polymerase chain reaction amplification of measles virus sequence from human temporal bone sections with active otosclerosis. Am J Otol 17(6):827–830
Karosi T, Kónya J, Z Szabó L, Sziklai I (2004) Measles virus prevalence in otosclerotic stapes footplate samples. Otol Neurotol 25(4):451–456
McKenna MJ, Mills BG, Galey FR, Linthicum FH Jr (1986) Filamentous structures morphologically similar to viral nucleocapsids in otosclerotic lesions in two patients. Am J Otol 7(1):25–28
McKenna MJ, Mills BG (1989) Immunohistochemical evidence of measles virus antigens in active otosclerosis. Otolaryngol Head Neck Surg 101(4):415–421
Arnold W, Friedmann I (1990) Immunhistochemistry of otosclerosis. Acta Otolaryngol (Stockh) Suppl 470:124–129
Narkio-Makela M, Jero J, Meri S (1999) Complement activation and expression of membrane regulators in the middle ear mucosa in otitis media with effusion. Clin Exp Immunol 116(3):401–409
Erlenhofer C, Duprex WP, Rima BK, ter Meulen V, Schneider-Schaulies J (2002) Analysis of receptor (CD46, CD150) usage by measles virus. J Gen Virol 83(6):1431–1436
Yanagi Y, Takeda M, Ohno S, Seki F (2006) Measles virus receptors and tropism. Jpn J Infect Dis 59(1):1–5
Kerdiles YM, Sellin CI, Druelle J, Horvat B (2006) Immunosuppression caused by measles virus: role of viral proteins. Rev Med Virol 16(1):49–63
Schneider-Schaulies S, Meulen V (2002) Modulation of immune functions by measles virus. Springer Semin Immunopathol 24(2):127–148
Lolov SR, Encheva VI, Kyurchiev SD, Edrev GE, Kehayov IR (2001) Antimeasles immunglobulin G in sera of patients with otosclerosis is lower than that in healthy people. Otol Neurotol 22(6):766–770
Karosi T, Kónya J, Petkó M, Szabó LZ, Pytel J, Jóri J, Sziklai I (2006) Antimeasles IgG for serologic diagnosis of otosclerotic hearing loss. Laryngoscope 116(3):488–493
Acknowledgment
Thanks are due to Éva Jószay (University Medical School of Debrecen, Department of Anatomy, Histology and Embriology) for assistance in the histological examinations. This work was supported by grants from Hungarian Scientific Research Fund (OTKA K63743, OTKA F035251, ETT 010/2001 and ETT 415/2003).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karosi, T., Jókay, I., Kónya, J. et al. Expression of measles virus receptors in otosclerotic, non-otosclerotic and in normal stapes footplates. Eur Arch Otorhinolaryngol 264, 607–613 (2007). https://doi.org/10.1007/s00405-007-0247-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-007-0247-7