
Abstract
Otosclerosis is a complex and progressive disease of bone remodeling that affects the otic capsule of the human temporal bone, resulting primarily in a conductive hearing loss with a normal tympanic membrane.
Family history, clinical assessment, and audiological evaluation are usually sufficient to establish the diagnosis. Imaging contributes greatly not only to determine important clinicoradilogic correlations but also to elucidate associated anatomic abnormalities and disease extensions, along with the differential diagnosis. Evolution, prognosis of otosclerosis along with its surgical strategy, related approaches, and complications are explained.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Otosclerosis is a progressive temporal bone dysplasia that affects the human otic capsule selectively. It causes stapes fixation and is the most common cause of conductive hearing loss in adults with an intact tympanic membrane.
2 Epidemiology
It can be divided into clinical and histological [1]. Histological osteosclerosis is a situation when patients have the disease without causing symptoms. Clinical otosclerosis is more common in females (2/1). Family history is found in half of the patients [2, 3]. It is more common in white races and Indian [2, 3] and has a lower rate in Africans. Moreover, it has a tendency to progress during pregnancy [4].
3 Pathogenesis
The otic capsule bone normally has two main features that distinguish it from other bones: a very low remodeling rate [5] and the presence of immature cartilage called Globuli Interossei [6, 7].
Several factors are involved in the pathogenesis of otosclerosis, which can affect the physiological inhibition of bone turnover in the otic capsule leading to otic dysplasia known as otosclerosis:
-
1.
Genetic inheritance: Mode of inheritance is autosomal dominant with incomplete penetrance [8].
-
2.
Viral infection: It is believed that the persistence of measles infection in the otic capsule is one of the etiological factors of otosclerosis [9].
-
3.
Hormonal effect: Pregnancy may lead to the progression of otosclerosis [4].
-
4.
Autoimmunity: An elevated level of collagen II autoantibody was found in patients with otosclerosis [10].
4 Histology
Classically, otosclerosis has two histological phases: the active phase (spongiosis) manifested by bone resorption and a stabilized phase (sclerosis) manifested by bone deposition [11, 12] (see Fig. 8.1). Otosclerosis can form in four stages:
-
1.
Stage 1: The resorptive or active stage: bone osteoclasts resorb the endochondral bone.
-
2.
Stage 2: The production of dysplastic immature basophilic bone.
-
3.
Stage 3: The remodeling phase in which the basophilic bone becomes less vascular and replaced by more mature acidophilic bone with the laminated matrix.
-
4.
Stage 4: The mature or otosclerotic stage; a new dense, compact bone with the formation of a woven pattern [11, 12].

Axial cut of right temporal bone at the level of fissula ante-fenestram showing the two phases of otosclerosis at the same time, active phase (1) and stabilized phase (2) [7]
The most common site of involvement is the oval window, followed by the round window and the pericochlear area [13].
5 Sites of Predilection
Two types of otosclerosis are described based on the location as follows (see Fig. 8.2):
-
1.
Fenestral involvement of the oval window and round window niche. Oval window involvement is more commonly found in the fissula ante-fenestram in front of the vestibule. Round window otosclerosis is observed in 13% of patients with conductive hearing loss (CHL) and stapedial otosclerosis [7].
-
2.
Retrofenestral is the involvement of the pericochlear otic capsule. Usually, it is associated with fenestral otosclerosis. Pure cochlear otosclerosis can cause sensorineural hearing loss (SNHL) without CHL. The earlier the involvement occurs, the more severe the symptoms will be [13, 14].

Types of otosclerosis
6 Clinical Manifestations
-
1.
Hearing loss: progressive CHL in a patient with a normal otoscopy without a history of head trauma or ear infection may indicate otosclerosis. In 10% of the cases, patients complain of mixed hearing loss due to the involvement of the cochlea. Seventy to 80% of cases show bilateral involvement. Paracusis of Willis is a phenomenon reported by patients with otosclerosis in which they hear better in a noisy environment [15].
-
2.
Tinnitus: Roaring or hissing, but it can be of pulsatile quality due to the hypervascularity in otosclerotic areas [16].
-
3.
Dizziness: It is seen in 25–30% of the cases. It can be due to otolithic dysfunction. Vertigo can also be due to endolymphatic hydrops or Meniere’s disease, revealed by vestibular evoked myogenic potential (VEMP), and that becomes an important issue to be kept in mind while considering a surgical treatment for such patients [17, 18].
7 Clinical Evaluation
-
1.
Otoscopy: shows normal TM. Rarely Schwartze’s sign can be seen.
-
2.
Tuning fork: in the early stages, Rinne is negative at 256 Hz only. As the disease progresses, 512 and 1024 Hz forks, Rinne will be negative.
-
3.
Audiological testing:
-
(a)
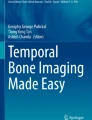
Pure tone audiogram: At the start of clinical otosclerosis, a progressive low-frequency conductive hearing loss is shown and then high-frequency CHL will occur, changing the audiogram to a flat pattern. If there is no cochlear involvement, then the hearing loss will be conductive with a maximum air-bone gap up to 40 or 50 dB. In the cochlear type, there will be mixed hearing loss in the mid frequencies giving cookie bite appearance [19]. Stapes fixation can give Carhart’s notch with an elevation of bone conduction threshold 5 dB at 500 Hz, 10 dB at 1000 Hz, 15 dB at 2000 Hz, and 5 dB at 4000 Hz. Word recognition and speech discrimination scores usually are normal unless there is significant SNHL (see Fig. 8.3).
-
(b)
Tympanogram shows type A or type As.
-
(c)
Stapedial reflex: if the stapes is not yet firmly fixed, it will show an on/off phenomenon. If stapes is fixed, then the stapedial reflex will be absent [20].
-
(a)

Pure tone audiogram of a patient with bilateral otosclerosis, showing bilateral conductive hearing loss with bilateral Carhart’s notch
8 Imaging: High-Resolution CT Scan
CT is considered the gold standard for imaging of otosclerosis [21]: high sensitivity of 91% and 99% specificity. Evaluation of the following is as follows:
-
1.
Oval window: A hypodense area in the fissula ante-fenestram is diagnostic of otosclerosis, footplate thickness being normal, moderately thickened, or even obliterative (above 0.8–0.9 mm) (Fig. 8.4).
-
2.
Round window otosclerosis: A classification system of CT findings of round window otosclerosis (RW1–RW5) correlates with the extent of the pathology in relation to a preoperative and postoperative hearing results [7, 21]: RW1–RW2 do not have an impact on postoperative air-bone gap closure, and RW4–RW5 contraindicate stapedectomy (Fig. 8.5).
-
3.
Retrofenestral otosclerosis: CT scan can show retro-fenestral disease invasion which is relevant to the prognosis (Fig. 8.6).
-
4.
Associated abnormalities: like narrow oval window niche (Fig. 8.7), an overhanging facial nerve, or persistent stapedial artery could be found and are of high diagnostic interest for the surgical strategy [7].

Axial CT images of right ears with otosclerosis: (a) typical otosclerotic hypodense focus at the fissula ante-fenestram (empty arrow), dense footplate moderately thickened, (b) obliterative thickening of the footplate (arrow), with only small otosclerosis focus at the fissula ante-fenestram (empty arrow)

Axial CT image of a left ear, showing otosclerosis of the round window (empty arrow) occupying the entire round window recess and adjacent calcification of the very proximal part of the retrofenestral scala tympani (arrow)

Axial CT image with a complete pericochlear otosclerotic rim (black arrows), coming into close contact with the cochlear endosteum (thick black arrow). In addition, intracochlear calcifications concerning the scala tympani of the basal turn (white arrow)

Coronal CT image showing a reduced height of the oval window niche due to a large bony apposition in the superior part of the niche (white arrow), inferior border of the oval niche (black arrow), VII facial nerve
Cone Beam-CT is positive to detect active otosclerotic focus that is characteristically hypodense to the surrounding hyperdense otic capsule bone; however, its sensitivity is low for the sclerotic phase of the disease process (hyperdense foci) and for pericochlear foci. When available, cone-beam is highly valuable for follow-up and postoperative prosthesis conditions [22, 23].
9 Stapes Surgery
9.1 Indications
-
1.
CHL with at least 25 dB and negative Rinne at 512 Hz is the minimum requirement to propose surgery.
-
2.
Speech discrimination more than 60% in order to obtain a favorable hearing outcome.
9.2 Contraindications
-
1.
Stapes surgery of the only hearing ear.
-
2.
Chronic otitis media or externa.
-
3.
Labyrinthine hydrops.
-
4.
Unfavorable systemic disease.
-
5.
Patients above 70 years old as they have more chance of worsening of speech discrimination and perilymphatic fistula complication.
-
6.
Pregnancy.
Informed Consent is mandatory and must be clear.
9.3 Surgical Steps (Video 8.1)
-
1.
Elevation of the tympanomeatal flap after assessment of the Malleus head mobility.
-
2.
Curetting the scutum for appropriate exposure of the facial nerve, round window, and pyramidal process.
-
3.
Assessment of the mobility of the ossicles.
-
4.
Separation of the incudostapedial joint.
-
5.
Stapedial tendon sectioning.
-
6.
Removal of the posterior crura by microdrill, micro scissor, or laser.
-
7.
Down fracturing the remaining stapes suprastructure.
-
8.
Measuring the distance between footplate and incus.
-
9.
Fenestration by perforator, microdrill, or laser. The best location is the posterior half of the footplate.
-
10.
Insertion and crimping of the piston. The prosthesis should extend at least 0.25 mm into the vestibule. It is usually 4.25–4.5 mm in length.
9.3.1 Stapedectomy vs. Stapedotomy
See Table 8.1 for a comparison between stapedectomy and stapedotomy [24,25,26,27,28,29,30].
9.3.2 Laser in Stapes Surgery
Using laser in stapes surgery may cause less postoperative SNHL incidence and give better control of hemostasis. However, there is no difference in the result regarding postoperative vertigo and air-bone gap closure [31].
Advantages of stapes laser surgery:
-
1.
Good hemostasis.
-
2.
Increased precision.
-
3.
Less risk of the floating footplate.
-
4.
Decreased risk of perilymph leakage.
See Table 8.2 and Fig. 8.8 for comparison between Argon/KTP laser and CO2 laser.

Argon or KTP laser can penetrate till the utricle and saccule. The CO2 laser is absorbed by perilymph causing heating side effects [7]
Microdrill can be used to perform the fenestration of the footplate during stapes surgery. It gives a hole with regular margins similar to a piston shaft, without causing acoustic trauma to the ear [32]. It is appreciated in obliterative otosclerosis.
9.3.3 Prosthesis Selection
-
Material: Titanium and Teflon are the most commonly used material for the piston.
-
Length: should be 0.5 mm longer than the distance between the footplate and medial edge of the incus. Another 0.25 mm should be added if the piston required bending during insertion.
-
Diameter: the larger the diameter, the better the hearing will be, but it can cause more damage to the inner ear. The best diameter is 0.6 mm, with 0.4 mm reserved for narrow OW [33].
-
Adequate crimping of the prosthesis to the long process of the incus is essential for energy transmission. It can be crimped by heat, by forceps, or it comes as clipping piston [34].
-
Oval window sealing with fat or vein for patient at risk for barotrauma (divers and pilots).
9.3.4 Intraoperative Challenges in Stapes Surgery [7]
-
1.
Malleus ankylosis: it may be congenital or acquired. Palpation of malleus should be done before addressing the stapes. Unrecognized malleus fixation can be the cause of failure of air-bone gap closure postoperatively.
-
2.
High jugular bulb: jugular bulb can be laterally located even near the annulus rendering it vulnerable to injury during the elevation of the tympanomeatal flap (Fig. 8.9).
-
3.
Overhanging facial nerve (Fig. 8.10) covering a large part of the footplate, then the surgery should not be done. The laser should be avoided in these cases (see Video 8.2).
-
4.
Obliterative otosclerosis: in which a thick otosclerotic deposit invades and covers the footplate. A large stapedotomy is the procedure of choice in these cases (Fig. 8.11) [35].
-
5.
Incidental disarticulation of the incus: In this case, the incus should be relocated into its anatomical place. However, if the incus can not be relocated, then malleus attachment for the prosthesis is the best solution.
-
6.
Narrow oval window niche (Video 8.3).
-
7.
Round window otosclerosis: A preoperative CT scan is required for diagnosis purposes (see Fig. 8.5).
-
8.
Perilymph oozer and gusher: oozer is usually due to a large vestibular aqueduct and treated by perichondrium or vein seal. Gusher is rare and usually due to a defect of cribrosa of internal auditory meatus. A preoperative CT scan can suspect a Gusher, but not in all cases (Fig. 8.12).
-
9.
Persistent stapedial artery (Fig. 8.13): a rare incident, CT finding of the absence of foramen spinosum should alert the surgeon of this pathology. The procedure should be aborted.

Large jugular bulb (IVJ) coming in close contact with the tympanic membrane (arrow)

A Left ear stapes surgery challenged by the overhanging facial nerve (VII) that is lying on the crura of the stapes (asterisk in a) and narrowing the oval window niche significantly. (b) Coronal CT showing a procident facial nerve (empty arrow) in front of the oval window, in proximity to the stapes suprastructure (arrow)

Left middle ear with obliterative otosclerosis

Axial CT of a left ear, showing enlargement of the angle between the first and second portion of the facial nerve, highly suspicious of Gusher syndrome

Right ear otosclerosis with the persistent stapedial artery (PSA). The posterior half of the footplate is visible (asterisk) and could be exceptionally accessible for fenestration
9.4 Outcome of Stapes Surgery
-
1.
Closure of air-bone gap to less than 10 dB in 95% of the cases [36].
-
2.
Improvement in tinnitus in 89% of cases [37].
9.5 Complications of Stapes Surgery
-
1.
Taste disturbance: due to chorda tympani injury. Usually, the symptoms are transient, and recovery can happen within 3–6 months [38]. Relevant information for contralateral Stapes surgery.
-
2.
Dizziness or vertigo: it can be due to labyrinthitis, which is self-limited and resolves within 3–6 days [39]. Other factors can cause dizziness like the heating effect of laser, long prosthesis, and depressed footplate fragment [40]. Long-lasting dizziness requires exploration to rule out a perilymph fistula.
-
3.
Sensorineural hearing loss: less than 1% in experienced hands [41]. It can be caused by perilymph fistula, granuloma formation, or very long prosthesis that penetrates deep into the vestibule (Fig. 8.14).
-
4.
Perilymph fistula: primary perilymph fistula occurs just after the fenestration and persists long after, while secondary perilymph fistula appears after a period of time of successful sealing. The latter is usually due to the dislocation of the prosthesis. Perilymph fistula indicates explorative tympanotomy.
-
5.
Reparative granuloma: it is a reactive granulation tissue that occurs after the surgery. It can invade the vestibule leading to hearing loss, tinnitus, and dizziness that appear after 7–12 days after the surgery. Most of the cases end in a profound permanent sensorineural hearing loss (Fig. 8.15).
-
6.
Facial palsy: an immediate post stapedectomy facial palsy is usually due to excessive local anesthesia infiltration. Delayed palsy is usually due to reactivation of the VZ virus or Bell’s palsy.
-
7.
Otitis media: Rare, but can cause sensorineural hearing loss. The patient should be admitted to the hospital to receive antibiotics and steroid. Ear packs, if still in the canal, should be removed.

Reformatted CT-Image along the prosthesis axis: stapes prosthesis laterally in contact with the long process of incus and the tympanic membrane (empty arrow), medially the long piston of the stapes prosthesis penetrates deep into the vestibule (white arrow). Thickened footplate between the black arrows

Reformatted CT along the prosthesis axis: hazy condensations around the piston (white arrows) due to the proliferative inflammatory tissue of the granuloma. Intravestibular tip of the prosthesis: black arrow
9.5.1 Failure in Stapes Surgery
Causes of persistent conductive hearing loss | Causes of recurrent conductive hearing loss |
|---|---|
1. Malleus ankylosis 2. Round window otosclerosis 3. Third window 4. Short prosthesis or small diameter prosthesis 5. Prosthesis abutting fenestration margin | 1. Resorptive osteitis of the incus 2. Displacement of the prosthesis 3. New bone formation in the oval window 4. Obliteration of the round window by otosclerosis |
The most common cause to perform revision stapes surgery is prosthesis displacement followed by incus erosion.
10 Conservative Treatment of Hearing Loss in Otosclerosis
-
1.
Hearing aid.
-
2.
BAHA or middle ear implant.
-
3.
Medical treatment: Given in cases of active otosclerosis. Signs and symptoms like the presence of Schwartz sign and onset or worsening of tinnitus, vertigo, or hearing loss can indicate active disease. The options for medical therapy include:
-
(a)
Sodium Fluoride: change the active lesion to an inactive lesion.
-
(b)
Bisphosphonates: it induces apoptosis in osteoclasts, reducing toxic enzymes’ production secondary to abnormal bone metabolism.
-
(a)
Take-Home Messages
-
Otosclerosis typically presents with slowly progressive unilateral or bilateral deafness, tinnitus, and vertigo may also occur.
-
The hearing loss encountered in these patients can be conductive, sensorineural, or mixed.
-
In patients with typical clinical features and uncomplicated conductive hearing loss, audiometry tests are mandatory to establish the diagnosis.
-
Imaging study is helpful to determine the disease stages and differential diagnosis, assess associated anatomic abnormalities, and evaluate postoperative prosthesis status.
References
Schuknecht HF, Barber W. Histologic variants in otosclerosis. Laryngoscope. 1985;95:1307–17.
Altmann F, Glasgold A, Macduff JP. The incidence of otosclerosis as related to race and sex. Ann Otol Rhinol Laryngol. 1967;76:377–92.
Cawthorne T. Otosclerosis. J Laryngol Otol. 1955;9:437–56.
Precechtel A. Determination of the effect of pregnancy on the activation of otosclerosis. Acta Otolaryngol. 1967;63:121–7.
Zehnder AF, Kristiansen AG, Adams JC, Kujawa SG, Merchant SN, McKenna MJ. Osteoprotegrin knockout mouse demonstrate abnormal remodeling of the otic capsule and progressive hearing loss. Laryngoscope. 2006;116:201.
Sørensen MS, Jørgensen MB, Bretlau P. Drift barriers in the postcartilaginous development of the mammalian otic capsule. Eur Arch Otorhinolaryngol. 1992;249:56–61.
Mansour S, Nicolas K, Ahmad HH. Round window otosclerosis: radiologic classification and clinical correlations. Otol Neurotol. 2011;32:384–92.
Moumoulidis I, Axon P, Baguley D, Reid E. A review on the genetics of otosclerosis. Clin Otolaryngol. 2007;32(4):239–47. Review.
Niedermeyer HP, Gantumur T, Neubert WJ, Arnold W. Measles virus and otosclerosis. Adv Otorhinolaryngol. 2007;65:86–92.
Yoo TJ. Etiopathogenesis of otosclerosis: a hypothesis. Ann Otol Rhinol Laryngol. 1984;93:28–33.
Cureoglu S, Schachern PA, Ferlito A, Rinaldo A, Tsuprun V, Paparella MM. Otosclerosis: etiopathogenesis and histopathology. Am J Otolaryngol. 2006;27(5):334–40.
Valvassori GE. Imaging of otosclerosis. Otolaryngol Clin N Am. 1993;26:359–71.
Hueb MM, Goycoolea MV, Paparella MM, Oliveira JA. Otosclerosis: the University of Minnesota temporal bone collection. Otolaryngol Head Neck Surg. 1991;105:396–405.
Schuknecht HF, Kirchner JC. Cochlear otosclerosis: fact or fantasy? Laryngoscope. 1974;84:766–82.
van Loon MC, Merkus P, Smit CF, Smits C, Witte BI, Hensen EF. Stapedotomy in cochlear implant candidates with far advanced otosclerosis: a systematic review of the literature and meta-analysis. Otol Neurotol. 2014;35(10):1707–14.
Gristwood RE, Venables WN. Otosclerosis and chronic tinnitus. Ann Otol Rhinol Laryngol. 2003;112:398–403.
Sando I, Hemenway WG, Miller DR, Black FO. Vestibular pathology in otosclerosis temporal bone histopathological report. Laryngoscope. 1974;84:593–605.
Paparella MM, Chasin WD. Otosclerosis and vertigo. J Laryngol Otol. 1966;80:511–9.
Hannley MT. Audiologic characteristics of the patient with otosclerosis. Otolaryngol Clin N Am. 1993;26(3):373–87.
Bel J, Causse J, Michaux P, Cézard R, Canut Y, Tapon J. Mechanical explanation of the on-off effect (diphasic impedance change) in otospongiosis. Audiology. 1976;15(2):128–40.
Lagleyre S, Sorrentino T, Calmels MN, Shin YJ, Escudé B, Deguine O, Fraysse B. Reliability of high-resolution CT scan in diagnosis of otosclerosis. Otol Neurotol. 2009;30(8):1152–9.
Révész P, Liktor B, Liktor B, Sziklai I, Gerlinger I, Karosi T. Comparative analysis of preoperative diagnostic values of HRCT and CBCT in patients with histologically diagnosed otosclerotic stapes footplates. Eur Arch Otorhinolaryngol. 2016;273(1):63–72.
Ariadna M, Cozma S, Murariu O, Radulescu L, Haba MSC, Vreme RM, Haba D, Iasi/ RO. ECR 2017 diagnostic value of CBCT in otosclerosis. Poster No 2283; 2017.
Fisch U. Stapedotomy versus stapedectomy. Otol Neurotol. 2009;30(8):1166–7.
Cremers CW, Beusen JM, Huygen PL. Hearing gain after stapedotomy, partial platinectomy, or total stapedectomy for otosclerosis. Ann Otol Rhinol Laryngol. 1991;100:959–61.
Spandow O, Soderberg O, Bohlin L. Long-term results in otosclerotic patients operated by stapedectomy and stapedotomy. Scand Audiol. 2000;29:186–90.
Persson P, Harder H, Magnuson B. Hearing results in otosclerosis surgery after partial stapedectomy, total stapedectomy and stapedotomy. Acta Otolaryngol. 1997;117:94–9.
Fisch U. Stapedectomy versus stapedectomy. Am J Otol. 1982;4:112–7.
Esquivel CR, Mamikoglu B, Wiet RJ. Long-term results of small fenestra stapedectomy compared with large fenestra technique. Laryngoscope. 2002;112:1338–41.
House HP, Hansen MR, Al Dakhail AAA, House JW. Stapedectomy versus stapedotomy: comparison of results with long-term follow-up. Laryngoscope. 2002;112:2046–50.
Wegner I, Kamalski DM, Tange RA, Vincent R, Stegeman I, van der Heijden GJ, Grolman W. Laser versus conventional fenestration in stapedotomy for otosclerosis: a systematic review. Laryngoscope. 2014;124(7):1687–93.
Yavuz H, Caylakli F, Ozer F, Ozluoglu LN. Reliability of microdrill stapedotomy: comparison with pick stapedotomy. Otol Neurotol. 2007;28(8):998–1001.
Rosowski JJ, Merchant SN. Mechanical and acoustic analysis of middle ear reconstruction. Am J Otol. 1995;16:486–97.
Huber AM, Ma F, Felix H, Linder T. Stapes prosthesis attachment: the effect of crimping on sound transfer in otosclerosis surgery. Laryngoscope. 2003;113:853–8.
Gierek T, Witkowska M, Zbrowska-Bielska D, Klimczak-Gołab L. Analysis of results of stapedotomy in patients with obliterative otosclerosis. Otolaryngol Pol. 2006;60(3):377–83.
Vincent R, Sperling NM, Oates J, Jindal M. Surgical findings and long-term hearing results in 3050 Stapedotomies for primary otosclerosis: a prospective study with the otology-neurotology database. Otol Neurotol. 2006;27:S25–47.
Gersdorff M, Nouwen J, Gilain C, Decat M, Betsch C. Tinnitus and otsclerosis. Eur Arch Otorhinolaryngol. 2000;257:314–6.
Berling Holm K, Knutsson J, Strömbäck K, Danckwardt Lillieström N, Papatziamos G, Rosenblad A, Von Unge M. Taste disturbance after stapes surgery: an evaluation of frequency, severity, duration, and quality-of-life. Acta Otolaryngol. 2017;137(1):39–43.
Birch L, Elbrond O. Stapedectomy and vertigo. Clin Otolaryngol. 1985;10:217–23.
Mansour S, Magnan J, Haidar H, et al. Comprehensive and clinical anatomy of the middle ear. Berlin: Springer; 2013. p. 49–81.
Glasscock ME III, Storper IS, Haynes DS, Bohrer PS. Twenty-five years of experience with stapedectomy. Laryngoscope. 1995;105:899–904.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
1 Electronic Supplementary Material
(MP4 33620 kb)
(MP4 24252 kb)
(MP4 77160 kb)
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Mansour, S., Al Shawabkeh, M.A., Nicolas, K., Haidar, H. (2021). Otosclerosis. In: Al-Qahtani, A., Haidar, H., Larem, A. (eds) Textbook of Clinical Otolaryngology. Springer, Cham. https://doi.org/10.1007/978-3-030-54088-3_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-54088-3_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-54087-6
Online ISBN: 978-3-030-54088-3
eBook Packages: MedicineMedicine (R0)