
Abstract
Parastomal hernias are a common and challenging occurrence after stoma creation. There is no universally agreed upon classification system. Many risk factors for parastomal hernia are not modifiable. Imaging can serve as an adjunct to a history and physical exam in diagnosing parastomal hernia. Complications can vary in severity and may warrant operative intervention. Operative approach can be open or laparoscopic, but mesh repairs are preferred to non-mesh repairs. It is our preference to perform a laparoscopic modified Sugarbaker technique for both initial and recurrent parastomal hernias. Prophylactic mesh placement at the time of stoma creation has been shown to decrease rates of parastomal hernia development without increasing the rate of infectious complications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Parastomal hernia
- Incidence
- Risk factors
- Complications
- Prevention
- Sugarbaker technique
- Keyhole technique
- Laparoscopic
- Prosthetic mesh
- Outcomes
Overview
Stoma creation is necessary for a number of elective and emergent gastrointestinal and urological procedures. Unfortunately, parastomal hernia (PH) can be a ubiquitous complication which poses a great challenge for general, colorectal, and urological surgeons.
Definition and Classificatio n
PH is often defined as a protrusion in proximity to a stoma or the abnormal protrusion of abdominal cavity contents through the abdominal wall defect resulting from colostomy, ileostomy, or ileal conduit creation [1, 2]. There are a number of PH classification systems based on clinical, radiographic, or intraoperative criteria; however, no classification system is universally agreed upon [3–6].
Risk Factors
A number of risk factors for PH development relating to patient, disease, and surgical factors have been proposed. Female gender is associated with a greater risk of PH [7, 8]. Increasing patient age, defined in some studies as age >60 years, is also a risk factor [7–12]. Body mass index (BMI) is a controversial risk factor as studies have shown a higher rate of PH in patients with a waist circumference >100 cm and a doubling in the rate of PH when comparing patients with a BMI ≥30 versus <30, while another study showed no significant risk when comparing PH development with waist circumference or BMI [8, 13, 14]. Other comorbidities including chronic obstructive pulmonary disease, hypertension, and ascites have been shown to be independent risk factors for PH development [7, 15]. Risk factors for surgical site infection or wound dehiscence in general, specifically smoking, diabetes mellitus, cardiovascular or pulmonary comorbidities, amount of blood loss, and type of surgery performed, should also be kept in mind [16]. Patients with inflammatory bowel disease commonly undergo stoma creation procedures, and those patients with Crohn’s disease have a higher rate of PH formation compared to those patients with ulcerative colitis [17]. The type of stoma created also has an impact on the rate of PH development with the highest rates occurring after colostomy creation and the lowest rates occurring after loop ileostomy creation [18, 19].
Incidence
The incidence of PH can vary greatly (0–80%) based on the definition used, diagnostic technique, and surgical approach at the time of stoma creation [20–22]. The incidence of PH for end and loop colostomies is as high as 48% and 38%, respectively, while the rates of PH are notably lower for end and loop ileostomies at 1.8–28.3% and 0–6.2%, respectively [18].
Diagnosis
PH diagnosis is often made by a history and physical exam with various imaging modalities serving as an adjunct to clinical diagnosis. The median time between formation of the stoma and detection of PH was 44 months in one study while others believe that most PHs develop within the first 2 years of stoma creation [5, 23]. A review of the French federation of ostomy patients determined 76% of patients with PH were symptomatic citing pain, difficulty with appliance fit, and leakage [12]. In another series, 85% of patients with a clinically detectable PH were also symptomatic [5]. Physical examination may uncover a fascial defect or reveal parastomal bulging with a Valsalva maneuver [24]. Imaging can increase the rate of PH detection, however, some PH may not be detectable by CT scan [5, 8, 24, 25]. Intrastomal ultrasonography may also be utilized to evaluate for PH while magnetic resonance imaging is rarely used for this purpose [26, 27].
Complications
PH complications can range from mild abdominal discomfort to intestinal perforation requiring emergent laparotomy [24]. Repeat surgical intervention is required in approximately 30% of patients with PH often due to bleeding, poor appliance fit, obstruction, and/or strangulation [28, 29]. Less severe symptoms may be managed nonoperatively. Expert consultation with a stoma nurse, if available, can often be helpful. It is recommended that the aperture size should be tailored to leave no more than a 2–3 mm rim around the stoma [30]. Flexible appliances can mold to uneven contours of the skin, and protective skin sealants may optimize appliance adherence [30–32]. Stoma belts may also improve appliance security and abdominal binders may help to relieve abdominal discomfort [32].
Operative Management
Laparoscopic Approac h
One of the main benefits of laparoscopy is limiting the potential sites for new hernia formation. Similar to the open intraperitoneal repairs, the modified Sugarbaker and keyhole techniques are utilized in addition to the sandwich technique which is a combination of the two approaches. For the sandwich technique, one piece of mesh is placed in a keyhole configuration while a second piece of mesh covers the first piece and the remaining abdominal wall [33]. A 2012 review of laparoscopic PH repairs demonstrated a 2.7% mesh infection rate, 3.6% rate of conversion to open, 4.1% iatrogenic bowel injury, and an overall morbidity of 17.2% [34]. The recurrence rate was significantly lower in the Sugarbaker technique at 11.6% versus 34.6% for the keyhole technique (Odds Ratio 2.3, 5% CI 1.2–4.6, p = 0.016) [34]. The recurrence rate for the sandwich technique was 2.1% but this was based solely on one series of 47 patients [34]. Table 23.1 details the outcomes of laparoscopic parastomal hernia repairs for studies with greater than 15 patients.
Our Approach
Operative Technique
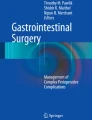
It is our preference to perform the laparoscopic modified Sugarbaker technique for PH and recurrent PH repairs. A first generation cephalosporin is given within 1 hour of the incision. Laparoscopic monitors and surgeon position are shown in Fig. 23.1. After induction of general anesthesia, the patient is placed in the supine position with both arms tucked. A Foley catheter is placed into the bladder, if the operation is expected to take longer than 1 hour. An additional Foley catheter (16 French) is placed directly into the ostomy and 10 mL of sterile water is placed in the Foley balloon (Fig. 23.2a). This allows for easy identification of the loop of intestine terminating in the stoma which can be helpful in the case of dense adhesions. The abdomen, stoma, and additional Foley catheter are prepped and then covered by an Ioban drape (3M Company, St. Paul, MN) (Fig. 23.2b). The peritoneal cavity is accessed with a Veress needle placed subcostally in the left upper quadrant in the midclavicular line. Once adequate pneumoperitoneum is obtained (15 mmHg of carbon dioxide), a 5 mm Optiview port is used to enter the peritoneal cavity laterally, on the side opposite to the stoma. Two additional 5 mm trocars are placed in the lateral position near the Optiview port (Fig. 23.3). External manipulation of the Foley catheter in the ostomy can help to identify the correct loop of bowel ending in the ostomy and can guide lysis of adhesions accordingly (Fig. 23.4). Once adhesiolysis is complete, the hernia contents, with the exception of the stoma, are reduced. The entire abdominal wall and the hernia defect, including any coexisting ventral or incisional hernia defects, can then be visualized and measured. Four spinal needles are used to mark the extent of the defect at the superior, inferior, and lateral-most aspects. A laparoscopic ruler is then inserted to measure the extent of the defect from the superior to inferior spinal needles for length and between lateral spinal needles for width (Fig. 23.5a). The defect is also measured and marked on the patient’s abdominal skin to assist with centering the prosthesis later in the procedure (Fig. 23.5b). The size of mesh is selected based on the defect measurements and allowing for a 5 cm overlap beyond all fascial edges. The mesh is then trimmed to the appropriate size. It is our preference to utilize ePTFE (Gore DUAL-MESH; W.L. Gore, Flagstaff, AZ). The textured surface of the mesh is marked to identify the superior and inferior portions of the mesh. A single Gore-Tex transfascial suture (CV-0) is placed at the edge of the mesh on three of the four sides that are not associated with the stoma. Two Gore-Tex transfascial sutures are placed on the fourth side on either side of where the stoma will lay creating a mesh flap valve. Two knots are tied at the time of each suture placement to secure each suture to the mesh. A 5 mm trocar is then placed in the lateral abdomen on the ipsilateral side of the stoma. A 12 mm trocar is placed through the hernia defect where it will later be covered by the mesh repair to minimize the risk of trocar site hernia. The Gore-Tex suture tails are arranged in the middle of the mesh, and the two marked edges of the mesh (superior and inferior) are rolled tightly toward one another. A grasper is placed through the ipsilateral trocar and is brought out through the 12 mm trocar to grasp the rolled mesh helping to guide it into the abdomen (Fig. 23.6a). The 12 mm trocar may need to be removed if the mesh size prohibits its passage through the trocar (Fig. 23.6b). The mesh is unrolled utilizing two graspers and oriented according to the earlier markings. The open jaws of an atraumatic bowel grasper are used to measure a 5 cm overlap from the edge of each of the fascial defects and these areas are marked with new spinal needles. Following the direction of the spinal needle, a suture passer is used to pass the transfascial sutures through the sites marked by the spinal needles while being careful to avoid the stoma as it traverses the edge of the mesh (Fig. 23.7). The mesh flap valve is crafted such that the stoma crosses the lateral or inferior edge. The transfascial sutures are secured with hemostats rather than tied until the most ideal mesh coverage and placement has been achieved. A laparoscopic tacker is used to secure the mesh in place circumferentially with the exception of the area around the stoma (Fig. 23.8a). Additional Gore-Tex transfascial sutures are placed with a suture passer every 4 to 5 cm around the mesh (Fig. 23.8b). The transfascial sutures are tied with ten knots in the subcutaneous tissues and the skin is freed from the knot with a hemostat so as to prevent dimpling (Fig. 23.9a). The trocar sites are closed with 4-0 monocryl suture and the stab incisions from the suture passer are closed with skin adhesive (Fig. 23.9b).

Laparoscopic monitors are positioned on either side of the patient. The surgeon (S) and the first assistant (FA) stand on the side opposite the stoma and the second assistant (SA) stands on the side of the stoma. The camera is placed in the most cephalad lateral port and is driven by the FA

A 16 French foley is placed into the stoma so as to help with lysis of adhesions (a). The abdomen is prepped with an Ioban drape (b)

Trocar placement consists of three 5 mm trocars placed laterally on the side opposite of the stoma. Later, a fourth 5 mm port will be placed on the ipsilateral side of the stoma

External manipulation of the intrastomal foley catheter helps to identify the loop of bowel terminating in the stoma and facilitates lysis of adhesions (white arrow marks the intrastomal foley balloon)

Spinal needles are used to demarcate the superior, inferior, and lateral borders of the hernia defect. A laparoscopic ruler is used to measure the defect (a). Mesh size is selected based on the internal measurement allowing for an overlap of 5 cm in all directions. The defect is also measured externally with the center of the defect marked (black circle) so as to allow for centering of the mesh by placing sutures on the dashed lines for the superior, inferior, and contralateral side to the stoma (b)

A locking grasper is inserted through a 12 mm port placed through the fascial defect to grasp the rolled mesh and guide it into the abdomen (a). The 12 mm port may need to be removed to allow for mesh entry pending size of the mesh (b)

A transfascial suture device is inserted into the abdomen (through the dotted line shown in Fig. 23.5b) following the angle of the spinal needle to retrieve the tails of the Gore-Tex suture (a). A grasper is used to identify and hand the correct tail to the suture passer, one at a time (b)

Once all sutures are tied after achieving ideal mesh placement, a laparoscopic tacker is used to circumferentially secure the mesh, with the exception of around the stoma (a). The secured mesh creates a flap valve allowing the stoma to pass through the lateral edge (b)

A total of ten knots are tied with the knots located in the subcutaneous tissues (a). A hemostat clamp is used to release the skin from the knots to prevent undesirable skin puckering at the incision sites (b). The skin is closed with suture and adhesive bandage. This patient also had an open left inguinal hernia repair (c)
Recurrent Parastomal Hernia
Data on recurrent PH is limited, and repair of recurrent PH presents the same challenges as initial PH repair. Failure of primary fascial repair is reported as high as 100% [3]. Stoma relocations fair only slightly better with a failure rate of 71% [3]. Prosthetic mesh repair failure has a lower recurrence rate of 33%, however, in Sugarbaker’s original description, six of his seven patients had recurrent PHs and he reported 100% success rate [3, 35]. It is our preference to approach recurrent PH the same as for initial PH with a laparoscopic modified Sugarbaker technique as described above.
Current Trends
Parastomal Hernia Prevention
Although not a new concept, the prevention of PH with prophylactic mesh has been the focus of recent and ongoing research. The idea was first introduced by Bayer et al. in 1986 who reported no PH over a four-year follow-up period in 43 patients who had Marlex mesh (Phillips Petroleum Company, Bartlesville, OK) placed at the time of colostomy creation [36]. Following Bayer’s initial success, there have since been many observational studies evaluating the efficacy and safety of prophylactic mesh placement. Figel et al. demonstrated no mesh complications or PH recurrences in 16 patients who underwent placement of a bioprosthetic mesh with a median 38-month follow-up [37]. Gogenur et al. demonstrated no infectious complications, an 8% rate of minor complications, and an 8% rate of PH recurrence in 25 patients who had an onlay of polypropylene mesh with a median follow-up of 12 months [38]. A small series of intraperitoneal onlay of polyvinylidene mesh during laparoscopic abdomino-perineal resection (APR) showed no mesh-related complications, infections, or PH recurrence at a mean follow-up of 6 months [39]. A study by Nagy et al. evaluated the polypropylene hernia system large device in 14 cases after APR with sigmoid colostomy and noted no PH recurrence in the first postoperative year [40]. Marimuthu et al. studied a polypropylene monofilament mesh with a circle cut in it for the stoma placed in the preperitoneal space without stitches in 18 patients and found no PH at a mean follow-up of 16 months. One patient did require revision for stoma necrosis on postoperative day 1 and subsequently developed a wound infection, but no other complications were noted [41]. A prospective study of preperitoneal polypropylene mesh placed in 42 patients with a mean follow-up of 31 months demonstrated an incidence of 10% for PH [42]. Cost-effectiveness of mesh prophylaxis has also been studied by Lee et al. They looked at mesh prophylaxis in 60 year olds who underwent APR with end colostomy for rectal cancer and found mesh prophylaxis to be less costly and more effective compared to no mesh for those patients with stage I-III rectal cancers [43]. Another RCT found significantly decreased presence of radiological PH in patients who had a lightweight intraperitoneal/onlay mesh placed for laparoscopic APR compared to those without mesh (50% versus 94%, p = 0.008) [44].
The three RCTs by Hammond, Janes, and Serra-Aracil are the most cited papers on the topic of PH prevention. In 2008, Hammond et al. published a RCT of 20 patients undergoing defunctioning stomas with a porcine-derived collagen implant placed in the sublay position in 10 patients. With a median follow up of 6.5 months, there were no complications and there were no PHs in the mesh group compared to 30% in the non-mesh group [45]. Janes et al. evaluated 54 patients undergoing permanent colostomy creation (27 patients with a conventional stoma and 27 with placement of a sublay large-pore lightweight polypropylene and polyglactin mesh). They found a lower rate of PH in the mesh group compared to the non-mesh group at 12-month follow-up (4.8% vs 50%). There were no infectious complications [46]. A five-year follow-up study again revealed a lower rate of PH in the mesh group 13.3% versus 81%): (p < 0.001) [22]. The RCT by Serra-Aracil evaluated 54 patients undergoing end colostomy for distal rectal cancer and utilized a sublay lightweight mesh in 27 patients. At a median 29-month follow-up, there were fewer PHs in the mesh group 14.8% (4/27) compared to 40.7% (11/27) in the non-mesh group (p = 0.03). Importantly, the morbidity between the two groups was similar [47]. In 2012, Sajid et al. and Shabbir et al. performed systematic reviews of the RCT literature. Sajid et al. analyzed the three RCTs by Janes, Hammond, and Serra-Aracil encompassing 128 patients who underwent colorectal resections with stoma creation (64 patients in the mesh group versus 64 patients in the non-mesh group), and found significantly decreased odds for developing a PH with the use of mesh without added morbidity [48]. Shabbir et al. reviewed 27 RCTs and excluded all but the same three RCTs as the Sajid paper. This review demonstrated an incidence of PH in 13% in the mesh group compared to 53% in the control group (p < 0.0001). There were no differences in mesh-related complications between the two groups [49]. A similar systematic review that included the same three RCTs, but also three prospective observational studies and one retrospective study, found a lower rate of PH in the mesh group [50]. All three systematic reviews concluded the use of prophylactic mesh at the time of stoma creation can reduce the incidence of PH. In contrast, a recently published prospective multicenter randomized controlled trial examined the utility of porcine-derived acellular dermal matrix reinforcement at the time of end-stoma creation in 55 patients compared to 58 control patients without mesh reinforcement. They found a similar incidence of PH for both groups at 12.2% for the mesh group and 13.2% for the control group [51]. The ideal technique including mesh selection and operative approach for PH prevention remains to be determined.
Conclusion
Parastomal hernias commonly develop after stoma creation, and the sequelae can range from mild to severe necessitating repeat operative intervention. Open and laparoscopic repairs with mesh are preferable to non-mesh repairs. For the open approach, a sublay or intraperitoneal placement of mesh is favored, and for the laparoscopic approach, the Sugarbaker technique has been shown to have a lower recurrence rate. It is our preference to perform a laparoscopic modified Sugarbaker technique. The use of prophylactic prosthetic mesh decreases the rate of PH development and is not associated with increased infectious complications.
References
Janes A, Cengiz Y, Israelsson LA. Randomized clinical trial of the use of a prosthetic mesh to prevent parastomal hernia. Br J Surg. 2004;91(3):280–2.
Smietanski M, Szczepkowski M, Alexandre JA, Berger D, Bury K, Conze J, et al. European Hernia Society classification of parastomal hernias. Hernia. 2013;18(1):1–6.
Rubin MS, Schoetz Jr DJ, Matthews JB. Parastomal hernia. Is stoma relocation superior to fascial repair? Arch Surg. 1994;129(4):413–8. discussion 8–9.
Devlin HB, Kingsnorth AN. Management of abdominal hernias. London: Hodder Arnold; 1998.
Moreno-Matias J, Serra-Aracil X, Darnell-Martin A, Bombardo-Junca J, Mora-Lopez L, Alcantara-Moral M, et al. The prevalence of parastomal hernia after formation of an end colostomy. A new clinico-radiological classification. Colorectal Dis. 2009;11(2):173–7.
Gil G, Owski MS. A new classification of parastomal hernias—from the experience at Bielanski Hospital in Warsaw. Pol Przegl Chir. 2011;83(8):430–7.
Sohn YJ, Moon SM, Shin US, Jee SH. Incidence and risk factors of parastomal hernia. J Kor Soc Coloproctol. 2012;28(5):241–6.
Hong SY, Oh SY, Lee JH, Kim do Y, Suh KW. Risk factors for parastomal hernia: based on radiological definition. J Korean Surg Soc. 2013;84(1):43–7.
Leong AP, Londono-Schimmer EE, Phillips RK. Life-table analysis of stomal complications following ileostomy. Br J Surg. 1994;81(5):727–9.
Londono-Schimmer EE, Leong AP, Phillips RK. Life table analysis of stomal complications following colostomy. Dis Colon Rectum. 1994;37(9):916–20.
Pilgrim CH, McIntyre R, Bailey M. Prospective audit of parastomal hernia: prevalence and associated comorbidities. Dis Colon Rectum. 2010;53(1):71–6.
Ripoche J, Basurko C, Fabbro-Perray P, Prudhomme M. Parastomal hernia. A study of the French federation of ostomy patients. J Visc Surg. 2011;148(6):e435–41.
Schreinemacher MH, Vijgen GH, Dagnelie PC, Bloemen JG, Huizinga BF, Bouvy ND. Incisional hernias in temporary stoma wounds: a cohort study. Arch Surg. 2011;146(1):94–9.
De Raet J, Delvaux G, Haentjens P, Van Nieuwenhove Y. Waist circumference is an independent risk factor for the development of parastomal hernia after permanent colostomy. Dis Colon Rectum. 2008;51(12):1806–9.
Carne PW, Frye JN, Robertson GM, Frizelle FA. Parastomal hernia following minimally invasive stoma formation. ANZ J Surg. 2003;73(10):843–5.
Sorensen LT, Hemmingsen U, Kallehave F, Wille-Jorgensen P, Kjaergaard J, Moller LN, et al. Risk factors for tissue and wound complications in gastrointestinal surgery. Ann Surg. 2005;241(4):654–8.
Carlstedt A, Fasth S, Hulten L, Nordgren S, Palselius I. Long-term ileostomy complications in patients with ulcerative colitis and Crohn’s disease. Int J Colorectal Dis. 1987;2(1):22–5.
Carne PW, Robertson GM, Frizelle FA. Parastomal hernia. Br J Surg. 2003;90(7):784–93.
Rullier E, Le Toux N, Laurent C, Garrelon JL, Parneix M, Saric J. Loop ileostomy versus loop colostomy for defunctioning low anastomoses during rectal cancer surgery. World J Surg. 2001;25(3):274–7. discussion 7–8.
Helgstrand F, Rosenberg J, Kehlet H, Jorgensen LN, Wara P, Bisgaard T. Risk of morbidity, mortality, and recurrence after parastomal hernia repair: a nationwide study. Dis Colon Rectum. 2013;56(11):1265–72.
Israelsson LA. Preventing and treating parastomal hernia. World J Surg. 2005;29(8):1086–9.
Janes A, Cengiz Y, Israelsson LA. Preventing parastomal hernia with a prosthetic mesh: a 5-year follow-up of a randomized study. World J Surg. 2009;33(1):118–21. discussion 22–3.
Rieger N, Moore J, Hewett P, Lee S, Stephens J. Parastomal hernia repair. Colorectal Dis. 2004;6(3):203–5.
Cingi A, Cakir T, Sever A, Aktan AO. Enterostomy site hernias: a clinical and computerized tomographic evaluation. Dis Colon Rectum. 2006;49(10):1559–63.
Gurmu A, Matthiessen P, Nilsson S, Pahlman L, Rutegard J, Gunnarsson U. The inter-observer reliability is very low at clinical examination of parastomal hernia. Int J Colorectal Dis. 2011;26(1):89–95.
Gurmu A, Gunnarsson U, Strigard K. Imaging of parastomal hernia using three-dimensional intrastomal ultrasonography. Br J Surg. 2011;98(7):1026–9.
Smietanski M, Bury K, Matyja A, Dziki A, Wallner G, Studniarek M, et al. Polish guidelines for treatment of patients with parastomal hernia. Pol Przegl Chir. 2013;85(3):152–80.
Burgess P, Matthew V, Devlin H. A review of terminal colostomy complications following abdominoperineal resection for carcinoma. Br J Surg. 1984;71:1004.
Burns F. Complications of colostomy. Dis Colon Rectum. 1970;13:448–50.
Rolstad BS, Boarini J. Principles and techniques in the use of convexity. Ostomy Wound Manage. 1996;42(1):24–6. 8–32; quiz 3–4.
Armstrong E. Practical aspects of stoma care. Nurs Times. 2001;97(12):40–2.
Kane M, McErlean D, McGrogan M, Thompson MJ, Haughey S. Clinical protocols for stoma care: 6. Management of parastomal hernia. Nurs Stand. 2004;18(19):43–4.
Berger D, Bientzle M. Laparoscopic repair of parastomal hernias: a single surgeon’s experience in 66 patients. Dis Colon Rectum. 2007;50(10):1668–73.
Hansson BM, Slater NJ, van der Velden AS, Groenewoud HM, Buyne OR, de Hingh IH, et al. Surgical techniques for parastomal hernia repair: a systematic review of the literature. Ann Surg. 2012;255(4):685–95.
Sugarbaker PH. Peritoneal approach to prosthetic mesh repair of paraostomy hernias. Ann Surg. 1985;201(3):344–6.
Bayer I, Kyzer S, Chaimoff C. A new approach to primary strengthening of colostomy with Marlex mesh to prevent paracolostomy hernia. Surg Gynecol Obstet. 1986;163(6):579–80.
Figel NA, Rostas JW, Ellis CN. Outcomes using a bioprosthetic mesh at the time of permanent stoma creation in preventing a parastomal hernia: a value analysis. Am J Surg. 2012;203(3):323–6. discussion 6.
Gogenur I, Mortensen J, Harvald T, Rosenberg J, Fischer A. Prevention of parastomal hernia by placement of a polypropylene mesh at the primary operation. Dis Colon Rectum. 2006;49(8):1131–5.
Martinek L, Dostalik J, Gunkova P, Gunka I, Mazur M. Prevention of parastomal hernia using laparoscopic introduction of a prosthetic mesh--initial experience. Rozhl Chir. 2012;91(4):216–8.
Nagy A, Kovacs T, Bognar J, Mohos E, Loderer Z. Parastomal hernia repair and prevention with PHSL type mesh after abdomino-perineal rectum extirpation. Zentralbl Chir. 2004;129(2):149–52.
Marimuthu K, Vijayasekar C, Ghosh D, Mathew G. Prevention of parastomal hernia using preperitoneal mesh: a prospective observational study. Colorectal Dis. 2006;8(8):672–5.
Vijayasekar C, Marimuthu K, Jadhav V, Mathew G. Parastomal hernia: Is prevention better than cure? Use of preperitoneal polypropylene mesh at the time of stoma formation. Tech Coloproctol. 2008;12(4):309–13.
Lee L, Saleem A, Landry T, Latimer E, Chaudhury P, Feldman LS. Cost effectiveness of mesh prophylaxis to prevent parastomal hernia in patients undergoing permanent colostomy for rectal cancer. J Am Coll Surg. 2013;29.
Lopez-Cano M, Lozoya-Trujillo R, Quiroga S, Sanchez JL, Vallribera F, Marti M, et al. Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection: a randomized controlled trial. Hernia. 2012;16(6):661–7.
Hammond TM, Huang A, Prosser K, Frye JN, Williams NS. Parastomal hernia prevention using a novel collagen implant: a randomised controlled phase 1 study. Hernia. 2008;12(5):475–81.
Janes A, Cengiz Y, Israelsson LA. Preventing parastomal hernia with a prosthetic mesh. Arch Surg. 2004;139(12):1356–8.
Serra-Aracil X, Bombardo-Junca J, Moreno-Matias J, Darnell A, Mora-Lopez L, Alcantara-Moral M, et al. Randomized, controlled, prospective trial of the use of a mesh to prevent parastomal hernia. Ann Surg. 2009;249(4):583–7.
Sajid MS, Kalra L, Hutson K, Sains P. Parastomal hernia as a consequence of colorectal cancer resections can prophylactically be controlled by mesh insertion at the time of primary surgery: a literature based systematic review of published trials. Minerva Chir. 2012;67(4):289–96.
Shabbir J, Chaudhary BN, Dawson R. A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation. Colorectal Dis. 2012;14(8):931–6.
Tam KW, Wei PL, Kuo LJ, Wu CH. Systematic review of the use of a mesh to prevent parastomal hernia. World J Surg. 2010;34(11):2723–9.
Fleshman JW, Beck DE, Hyman N, Wexner SD, Bauer J, George V, PRISM Study Group. A prospective, multicenter, randomized, controlled study of non-cross-linked porcine acellular dermal matrix fascial sublay for parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies. Dis Colon Rectum. 2014;57(5):623–31.
Mancini GJ, McClusky 3rd DA, Khaitan L, Goldenberg EA, Heniford BT, Novitsky YW, et al. Laparoscopic parastomal hernia repair using a nonslit mesh technique. Surg Endosc. 2007;21(9):1487–91.
McLemore EC, Harold KL, Efron JE, Laxa BU, Young-Fadok TM, Heppell JP. Parastomal hernia: short-term outcome after laparoscopic and conventional repairs. Surg Innov. 2007;14(3):199–204.
Craft RO, Huguet KL, McLemore EC, Harold KL. Laparoscopic parastomal hernia repair. Hernia. 2008;12(2):137–40.
Berger D, Bientzle M. Polyvinylidene fluoride: a suitable mesh material for laparoscopic incisional and parastomal hernia repair! A prospective, observational study with 344 patients. Hernia. 2009;13(2):167–72.
Hansson BM, de Hingh IH, Bleichrodt RP. Laparoscopic parastomal hernia repair is feasible and safe: early results of a prospective clinical study including 55 consecutive patients. Surg Endosc. 2007;21(6):989–93.
Hansson BM, Bleichrodt RP, de Hingh IH. Laparoscopic parastomal hernia repair using a keyhole technique results in a high recurrence rate. Surg Endosc. 2009;23(7):1456–9.
Liu F, Li J, Wang S, Yao S, Zhu Y. Effectiveness analysis of laparoscopic repair of parastomal hernia using CK Parastomal patch. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2011;25(6):681–4.
Wara P, Andersen LM. Long-term follow-up of laparoscopic repair of parastomal hernia using a bilayer mesh with a slit. Surg Endosc. 2011;25(2):526–30.
Mizrahi H, Bhattacharya P, Parker MC. Laparoscopic slit mesh repair of parastomal hernia using a designated mesh: long-term results. Surg Endosc. 2012;26(1):267–70.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Electronic Supplementary Material
Laparoscopic Parastomal (Sugarbaker) repair, by Harold (WMV 137,831 kb)
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Garvey, E.M., Harold, K.L. (2016). Laparoscopic Parastomal Hernia Repair. In: Novitsky, Y. (eds) Hernia Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-27470-6_23
Download citation
DOI: https://doi.org/10.1007/978-3-319-27470-6_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27468-3
Online ISBN: 978-3-319-27470-6
eBook Packages: MedicineMedicine (R0)