
Abstract
Introduction
Parastomal hernia in patients with a permanent colostomy is common. The aim of this study was to evaluate the reliability of the diagnosis based on clinical examination and to compare this examination with the result of a specially designed questionnaire and computerised tomography (CT) scan.
Methods
Forty-one patients operated upon with an abdominoperineal resection due to rectal cancer at three hospitals between 1996 and 2002 were included. At minimum of 4 years after the operation, they underwent clinical examination by two or three independent surgeons, answered a colostomy questionnaire and were offered a CT scan of the abdominal wall.
Result
At Hospital I, 17 patients were examined by three surgeons, with inter-observer kappa values between 0.35 and 0.64. At Hospital II, 13 patients were examined by three surgeons, the kappa values ranged between 0.29 and 0.43. At Hospital III, 11 patients were examined by two surgeons, with kappa value of 0.73. The kappa value between CT scan and the colostomy questionnaire was 0.45.
Conclusion
The inter-observer reliability was low, indicating that parastomal hernia is difficult to diagnose by patient history and clinical examination. Some herniae may not be detected by CT scan, and the correlation to patient-reported complaints is low. A more sensitive radiological method to detect parastomal hernia is needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Approximately one third of all patients with rectal carcinoma will end up with a permanent colostomy [1]. Parastomal hernia or a bulge around the stoma is a common complication. The frequency of parastomal hernia in the literature has been reported to range between 3% and 81% partly depending on diagnostic criteria and when the hernia is evaluated in relation to time after surgery [2–4]. The majority of all parastomal herniae develops within a few years, but can appear as late as 20 years after surgery [5, 6]. The definition of parastomal hernia is not uniform, and the distinction between a bulge of the abdominal wall and a parastomal hernia is vague. Thus, calculations of prevalence in the literature are based on different criteria, and sometimes these criteria are not even reported or described [7]. In some publications, it is not obvious whether the observers were independent of each other during the examination, and the data concerning inter-observer reliability are missing. Validated questionnaires have not been utilised, and the duration of follow-up of patients is often short. Moreover, there are few comparisons between clinical examination and radiology. Of these, one [3] showed that the incidence increased from 52% to 78% when computerised tomography (CT) scan was added to the physical examination.
The aim of the present study was to evaluate the reliability of the diagnosis based on clinical examination and to compare this examination with the result of a specially designed questionnaire and CT scan.
Materials and methods
Patients
Six hundred and thirty-eight patients, coming from the three Swedish hospitals represented by the authors, were abdominally operated on for rectal carcinoma between 1996 and 2002. An abdominoperineal resection was performed in 163 patients and a Hartmann´s procedure in 43 patients. Accordingly, 32% (206/638) received a primary permanent colostomy. A cross-check was performed against the population register to exclude patients who had died during the follow-up period. The patients were identified from the Swedish Rectal Cancer Register [1] at a minimum of 3 years postoperatively.
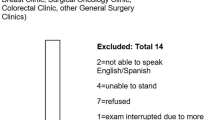
A total of 56 patients fulfilled the criteria. In total, 15 patients were excluded; nine patients gave no informed consent, four suffered from dementia, and two were only partially examined due to logistic failure. Thus, 41 patients (17 women and 24 men) answered the questionnaire, had a complete clinical examination, and were included in the study (Fig. 1).

Flow chart of patients who were included in the study
Forty patients were operated with abdominoperineal resection and one with Hartmann’s procedure. The median time from surgery to follow-up with this clinical examination was 5 years (range, 4–10 years).
Clinical examination
The clinical examination was performed in the supine and erect position while performing the Valsalva manoeuvre, and included intrastomal palpation. The clinical examination had three options: no hernia, bulge or parastomal hernia. The patients were examined by two or three independent surgeons who were blinded to each other’s findings and to the result of the questionnaire. The surgeons were resident (Dr A) and four senior consultant colorectal surgeons (Dr B, Dr C, Dr D and Dr E). Dr A examined all 41 patients, Dr B 28 patients, Dr C 17 patients, whereas Dr D and Dr E examined 13 patients. The examination results were documented in a structured case report form.
Questionnaire
A colostomy questionnaire comprising 29 questions was developed for this study. It contained questions about the patients’ attitude to the stoma before and after surgery, the function of the stoma, any problems with the stoma, if they considered that they had a bulge/parastomal hernia, and if the stoma was considered a disability for them.
BMI
BMI was calculated for each patient to observe if there was a clear connexion between BMI and parastomal hernia.
Radiology
The CT scan was performed in the supine position and included a Valsalva manoeuvre during the examination. CT scans were performed without oral contrast and contrast instilled in the colon. A senior radiologist who was blinded to the clinical examination evaluated all the scans. Twenty-six of the patients included underwent a CT scan of the abdomen, and two patients had recently been examined by CT scan of the abdomen.
The evaluations of the CT scans had two options, no hernia and parastomal hernia, comparatively to the surgeons, who had three options, no hernia, bulge and parastomal hernia. A parastomal hernia was defined as a defect in the fascia through which intraabdominal contents such as omentum or bowel could be extruded out. A finding of intact fascia with dilated or elongated stoma bowel in the subcutaneous area was considered not to be a hernia.
Statistical methods
To measure the congruence between surgeons, surgeons vs. CT scan, and CT scan vs. questionnaire, kappa values were used [8]. Calculation of the kappa value was performed with the VasarStats programme [9].
Ethics
The study was approved by the Ethics Committee of Uppsala University, Dnr 2005:287.
Results
In 26 of the 41 (63%) patients, the surgeons reached full agreement on classification of the stomata by clinical examination. Eleven of those patients had a hernia by all diagnostic criteria, whereas 15 patients, of whom two had a bulge, did not have a definite hernia.
The remaining 15 patients (37%) were difficult to classify by clinical examination. In six patients, disagreement was between a bulge and no hernia, whereas in five patients, disagreement was between a bulge and a hernia. The results from the remaining four patients were more diverging (Table 1). Three patients were examined by three surgeons and judged to have no hernia, bulge and hernia, and for the last patient, there was disagreement whether there was no hernia or hernia.
Clinical examination
At Hospital I, 17 patients were examined by three surgeons, Dr A, Dr B and Dr C. In 11 patients, full agreement was reached on classification of the stomas (Table 2). All agreed that none of the 17 patients required a reconstruction of the stoma.
At Hospital II, 13 patients were examined by three surgeons, Dr A, Dr D and Dr E, with full agreement on classification of the stomata in six patients (Table 2). All agreed that two patients required reconstruction of the stoma, Dr D and Dr E each had another patient in whom there was disagreement on this point.
At Hospital III, 11 patients were examined by two surgeons, Dr A and Dr B, with full agreement on classification of the stomata in nine patients (Table 2). Both agreed that none of the 11 patients required a reconstruction of the stoma.
Questionnaire
The attitude to receive a stoma was positive in 20% of the patients, negative in 43% and no opinion in 37%. This attitude changed after surgery to 66%, 17% and 17%, respectively. Two patients (5%) had been re-operated due to parastomal hernia, one had a stoma on a new location and one had a repair with a mesh. The majority was affected by the stoma in everyday life (64%) including mental wellbeing (54%). Forty of 41(97.5%) patients were satisfied with their function of the stoma, although some had pain occasionally (20%) or had pain most of the time (5%). Forty-four percent of the patients considered that they had a hernia or bulge, and 44% denied a bulge or hernia. Twelve percent did not answer that specific question (Table 1).
BMI
BMI greater than 25 is considered as overweight, and BMI greater than 30 is considered as obesity [10]. BMI greater than 25 was found in six of the 15 patients with diagnostic difficulties (Table 3). A total of 22 patients had a BMI greater than 25, and seven greater than BMI 30.
CT scan
Nineteen patients (67%) had a CT scan, which was in full agreement with the surgical assessment. Here, bulge was considered as no hernia. Twelve of 28 (43%) CT scans were classified as identifying a parastomal hernia. Eight of 12 patients diagnosed with a parastomal hernia at CT scan had a BMI greater than 25. In eight of 16 CT scans in which a parastomal hernia could not be detected, the patient had a BMI greater than 25. Three patients had a parastomal hernia according to three investigating surgeons, but the CT scan did not detect a parastomal hernia.
Examiners, CT scan and questionnaire compared
Kappa values for inter-observer reliability, comparison with results of CT scans, and with results from the questionnaire are shown in Table 2. The kappa value between CT scan and the colostomy questionnaire was 0.45.
Discussion
The low inter-observer reliability between the investigating surgeons is the most striking result from the present study, despite the fact that four of the five examiners were experienced colorectal surgeons with a special interest in parastomal hernia. Accordingly, it appears that clinical examination is not enough to diagnose parastomal hernia, and judgements based on examination only are not stable and reliable. The wide range of the kappa values for surgeons, questionnaire results and CT scans (Table 2) may explain the wide range of incidence of parastomal herniae reported in the literature [2–4].
Description of parastomal herniae in the literature is sparse, and to our knowledge inter -observer reliability and correlation between patient-reported signs and complaints and radiological examination for parastomal hernia has not been studied in detail before. The study design with a total of five investigating surgeons reflects the stability of the diagnosis in common clinical praxis and the variability in kappa values between those underlines the low inter-observer reliability. Although the limited number (41) of patients included, they represent in total 112 observations and may allow for a reliable estimate of the inter-observer reliability. Moreover, the follow-up time was at least 4 years. Other studies have considered 1 to 2 years to be enough to detect parastomal hernia; few studies have a long-term follow-up period [2–4]. Overweight and obese also pose diagnostic problems. In the group in which it was difficult to classify the stoma, six of 15 patients had a BMI greater than 25 and were subsequently difficult to evaluate by clinical examination.
Parastomal hernia may be seen as a graded diagnosis based on clinical criteria ranging from bulging at the stoma site to obvious herniation of abdominal contents into the parastomal space. Further radiological investigation is necessary to carefully evaluate symptoms and the patient’s complaints before reconstructive surgery.
The CT scan was undertaken while the patient performed Valsalva manoeuvre, in the supine position. It is well-known that a hernia is easier to detect during the Valsalva manoeuvre, and in the erect position. This could be the reason why CT scan did not detect a hernia, detected by all three examiners in three patients. Thus, CT scan in its present form cannot serve as a reference for the diagnosis of parastomal hernia. It may detect herniae missed in clinical examination but obviously also miss herniae diagnosed by independent surgeons. The logical conclusion is that refinement of the CT technique is required.
As a result of the discordance between clinical investigation and CT, we have started a project aimed at developing an endostomal ultrasound technique using a standardised protocol to detect parastomal herniae.
The questionnaire showed that 97.5% of the patients were satisfied with their stoma function; however, 24.5% had problem with pain, and 44% considered that they had a bulge or a hernia. The majority of the patients thought that the stoma had affected their lives. This sheds light on the fact that a permanent stoma has a major impact on quality of life and should be used only when deemed unavoidable (Table 4).
An important finding is that some of the patients have no more than a bulge in the abdominal wall, and it is often difficult to distinguish this bulge from a parastomal hernia by clinical examination only. The evaluation of the CT scans could only classify no hernia and parastomal hernia; bulging of the abdominal wall is very hard to diagnose on the images. All in all, in 37% of the patients we had disagreement in classification. Obviously, it is important to define reliable and reproducible criteria for the diagnosis of parastomal hernia, probably including a modality of radiological technique which remains to be developed and evaluated.
References
Påhlman L, Bohe M, Cedermark B, Dahlberg M, Lindmark G, Sjödahl R, Öjerskog B, Damber L, Johansson R (2007) The Swedish Rectal Cancer Registry. Br J Surg 94:1285–1292
Sjödahl R, Anderberg B, Bolin T (1988) Parastomal hernia in relation to site of the abdominal wall. Br J Surg 75:339–341
Cingi A, Cakir T, Sever A, Aktan AO (2006) Enterostomy site hernias: A clinical and computerized tomographic evaluation. Dis Colon Rectum 49:1559–1563
Jänes A, Cengiz Y, Israelsson L (2009) Preventing parastomal hernia with prosthetic mesh: a 5-year follow-up of a randomized study. World J Surg 33:118–121
Carne PWG, Robertson GM, Frizelle FA (2003) Parastomal hernia. Br J Surg 90:784–793
London-Schimmer EE, Leong APK, Phillips RKS (1994) Life table analysis of stomal complications following colostomy. Dis Colon Rectum 37:916–920
Ortiz H, Sara MJ, Armendariz P, de Miguel M, Marti J, Chocarro C (1994) Does the frequency of parastomal hernias depend on the position of the colostomy in the abdominal wall? Int J Colorectal Dis 9:65–67
Boyd NF, Pater JF, Ginsburg AD (1979) Observer variation in the classification of information from medical records. J Chronic Dis 32:327–332
Vassar Stats: Web Site for Statistical computation. http://faculty.vassar.edu/lowry/VassarStats.html
http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html#Interpreted
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gurmu, A., Matthiessen, P., Nilsson, S. et al. The inter-observer reliability is very low at clinical examination of parastomal hernia. Int J Colorectal Dis 26, 89–95 (2011). https://doi.org/10.1007/s00384-010-1050-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-010-1050-2