
Abstract
There is no universally accepted etiological factor of temporomandibular disorders according to the recent literature. Some studies suggested that partial edentulism has only a minor role in the etiology of temporomandibular disorders (TMD). Although some cadaver studies are able to show the relationship between posterior tooth loss and arthritic changes in temporomandibular joint, there is a consensus in the literature that the causal relationship between occlusion and TMD does not appear. Tooth loss and osteoarthritis (OA) is a natural progression of aging. Thus, the weak correlation between OA and tooth loss has to be reconsidered according to this fact. The historical studies especially from the 1970s speculated a close relationship of the above-mentioned topic using mostly the biomechanical theory. Later studies however confuted this theory. The clinical signs and symptoms of TMD are not always correlated with the anatomical changes in TMJ. Therefore, the results of the clinical researches are more important compared to the cadaver and radiological studies. These studies are also not able to evaluate muscle symptoms of the patients.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Occlusal splint
- Temporomandibular joint
- Edentulism
- Tooth loss
- Temporomandibular disorders
- Removable partial denture
1 Definitions
- Grinding:
-
A term used to denote the act of correcting occlusal disharmonies by grinding the natural or artificial teeth.
- Maximal intercuspal position (MIP):
-
The complete intercuspation of the opposing teeth independent of condylar position, sometimes referred to as the best fit of the teeth regardless of the condylar position—called also maximal intercuspation.
- Occlusal splint or device:
-
Any removable artificial occlusal surface used for diagnosis or therapy affecting the relationship of the mandible to the maxillae. It may be used for occlusal stabilization, for treatment of temporomandibular disorders, or to prevent wear of the dentition.
- Retruded contact position (RCP):
-
That guided occlusal relationship occurring at the most retruded position of the condyles in the joint cavities. A position that may be more retruded than the centric relation position.
- Temporomandibular disorders (TMD):
-
1: Conditions producing abnormal, incomplete, or impaired function of the temporomandibular joint(s). 2: A collection of symptoms frequently observed in various combinations first described by Costen (1997), which he claimed to be reflexes due to irritation of the auriculotemporal and/or chorda tympanic nerves as they emerged from the tympanic plate caused by altered anatomic relations and derangements of the temporomandibular joint associated with loss of occlusal vertical dimension, loss of posterior tooth support, and/or other malocclusions. The symptoms can include headache about the vertex and occiput, tinnitus, pain about the ear, impaired hearing, and pain about the tongue.
2 Relationship Between Partial Edentulism and TMD
There is no universally accepted etiological factor of temporomandibular disorders according to the recent literature. Some studies suggested that partial edentulism has only a minor role in the etiology of temporomandibular disorders (TMD). Although some cadaver studies are able to show the relationship between posterior tooth loss and arthritic changes in temporomandibular joint, there is a consensus in the literature that the causal relationship between occlusion and TMD does not appear. Tooth loss and osteoarthritis (OA) is a natural progression of aging. Thus, the weak correlation between OA and tooth loss has to be reconsidered according to this fact. The historical studies especially from the 1970s speculated a close relationship of the above-mentioned topic using mostly the biomechanical theory. Later studies however confuted this theory. The clinical signs and symptoms of TMD are not always correlated with the anatomical changes in TMJ. Therefore, the results of the clinical researches are more important compared to the cadaver and radiological studies. These studies are also not able to evaluate muscle symptoms of the patients. Consequently, recent clinical studies show weak or no correlation between TMD symptoms and lack of molar support. Additionally, the studies analyzing “shortened dental arch theory” are in consensus that the lack of molar support is not a risk for the development of TMD. This topic was explained in Chap. 5 in detail.
Some studies have shown that the loss of a specific tooth may be associated with the development of TMD. Kirveskari and Alanen (1985) have shown that loss of maxillary first premolar tooth has an association with TMD. In another study by Abdel-Fattah (1996), it was shown that the loss of first molar tooth is related with TMD signs and symptoms. In a clinical study with better statistical analyses, Wang et al. are able to show that not only the number of missing posterior teeth but the number of dental quadrants with missing posterior teeth has an effect on the development of TMD. These studies based their results on the premature contacts and loss of the biomechanical balance as a result of drifting and tipping of the remaining teeth.
As a conclusion, recent literature does not support a sound relationship between partial edentulism and TMD. However, there are some good researches to point out that tooth loss and occlusal discrepancies may have an impact on the development of the functional disorder of the stomatognathic system. In future, the scientists have to focus more on longitudinal studies to show the long-term effect of occlusal changes and the lack of biomechanical stability on the masticatory system disorders.
Now the question is: Should we focus on the replacement of missing posterior teeth to treat the patients with TMD, even though there is no evidence to show such a relation? First of all, we have to discuss the effect of occlusal therapy in the treatment of TMD. Recent literature can show only a short-term success of occlusal therapy. Longitudinal studies are not enough to demonstrate a distinction of irreversible occlusal corrections (occlusal grinding or restoration) to more conservative and simple treatment modalities like occlusal splints or physical therapies. There are however a lot of studies that support the success of occlusal splint therapy in rehabilitation of the patients with TMD. Other studies are also not able to show a positive effect of placing fixed or removable prosthesis in the treatment of TMDs, especially if the patient has lost only his/her molar teeth. Thus, there is no need to choose a sophisticated prosthodontic treatment modality for the rehabilitation of the signs and symptoms of TMD. However in some cases with partial edentulism, there is a need of replacement of missing teeth to make a stabilization appliance. The aim of this chapter is to make clear how to construct an occlusal appliance in various partial edentulism situations.
3 Occlusal Splints
The occlusal splint therapy is based on changing the occlusal relations. However, that does not mean that the occlusal relations have to be restored or be adjusted in similar ways. In many cases, there is no need for a definite occlusal rehabilitation after the occlusal splint therapy. The occlusal splint therapy is finished after the symptoms of the patient diminish. The treatment should be restarted when the symptoms are returned after the end of the splint therapy. If a definitive therapy with occlusal splint is not possible, an irreversible occlusal rehabilitation should be evaluated. Yet, it should be kept in mind that there is no scientific evidence in dental literature that irreversible changes in dental occlusion help to reduce the symptoms of TMD.
3.1 How Do Occlusal Splints Rehabilitate TMD
-
1.
The increase of the occlusal vertical dimension
The occlusal splints are interocclusal devices which increase the occlusal vertical dimension of the patient for a temporary period. This is a very important characteristic of the occlusal splints. This increase elongates the masseter, temporal, and medial pterygoid muscles, which reduce the isometric contractions. It is well known that the isometric contractions of the muscles can expose myogenic pain. In contracted muscles, the blood circulation is blocked. That means the muscle cannot be nourished and purged. And the pain revealing particles collect in the muscle and expose pain. The physical therapy modalities generally function with this mechanism. The muscle is heated using infrared, laser, massage, etc., and the blood circulation is regenerated. Therefore, occlusal splints achieve this goal without using any physical therapy if the patient has bruxism.
-
2.
The change of the condyle position
Placing an occlusal splint into the mouth of the patient creates a new position of the condyles in the glenoid fossa which is more anterior and caudal to the centric position. Thus, the overload in the articular soft tissues is reduced.
-
3.
New occlusal relations
An occlusal splint should have a flat occlusal surface which eliminates the occlusal interferences and builds point contacts with each antagonist teeth. These kinds of splints create a harmonic slide between maximal intercuspal position (MIP) and retruded contact position (RCP). Additionally, a stabilization splint should have a canine guided eccentric occlusal balance. Especially the occlusal point contacts are perceived from the proprioceptive receptors in periodontium, and this information is sent as an impulse to the central pattern generator (CPG) in the brain. Thus, a decrease of muscle contraction is achieved.
Also, the cognitive awareness of the patient and the placebo effect of the occlusal devices are also important factors for the relief of the sign and symptoms of TMD.
3.2 Occlusal Splint Design in Partial Edentulism
First of all, the clinician should decide which jaw is appropriate for fabricating an occlusal splint. Therefore, the position, number, and size of the edentulous places should be analyzed. The following rules are helpful for a clinician to make the decision:
-
1.
In cases with single (maxillary or mandibular) long free-ending edentulous arches (unilateral or bilateral), the antagonist jaw (full dentate or with a dentition which is explained in third entry) is ideal to place an occlusal splint and the edentulous jaw should be rehabilitated using an RPD (Fig. 21.1a–c). It is not suitable to make a stabilization splint over an RPD and it is also not correct to place a splint to a dental arch with a long free-ending edentulism. It may produce a tilting force on the anterior teeth because of the resilience of the mucosa (Fig. 21.2a, b). An alternative is to make a special designed occlusal splint for only night time use (Fig. 21.3a–f).
Fig. 21.1 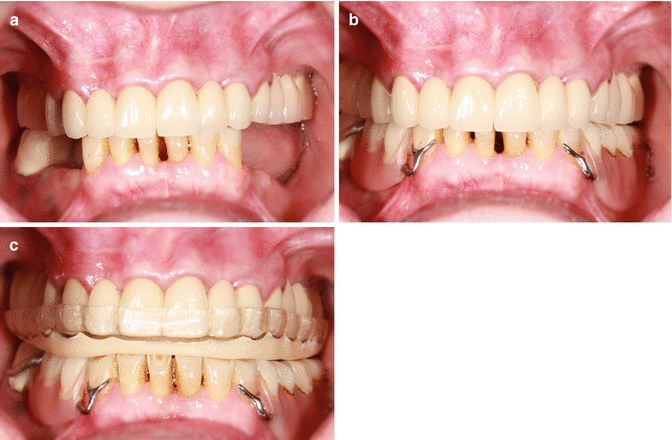
(a) A temporomandibular disorder (TMD) patient with mandibular partial edentulism. Intraoral view in occlusion. (b) A removable partial denture (RPD) is fabricated for the patient first. (c) Then a maxillary occlusal splint is fabricated
Fig. 21.2 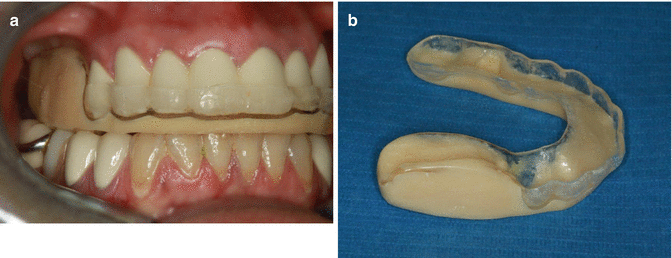
(a) An occlusal splint is fabricated to a patient with a long free-ending partial edentulism. (b) Notice the long distal part of the occlusal splint, which may produce a tilting force on the anterior teeth
-
2.
In cases with both maxillary and mandibular long free-ending edentulous crest (unilateral or bilateral), the patient should be rehabilitated first with RPDs. Afterward, a specially designed maxillary occlusal splint should be prepared for nighttime use.
Fig. 21.3 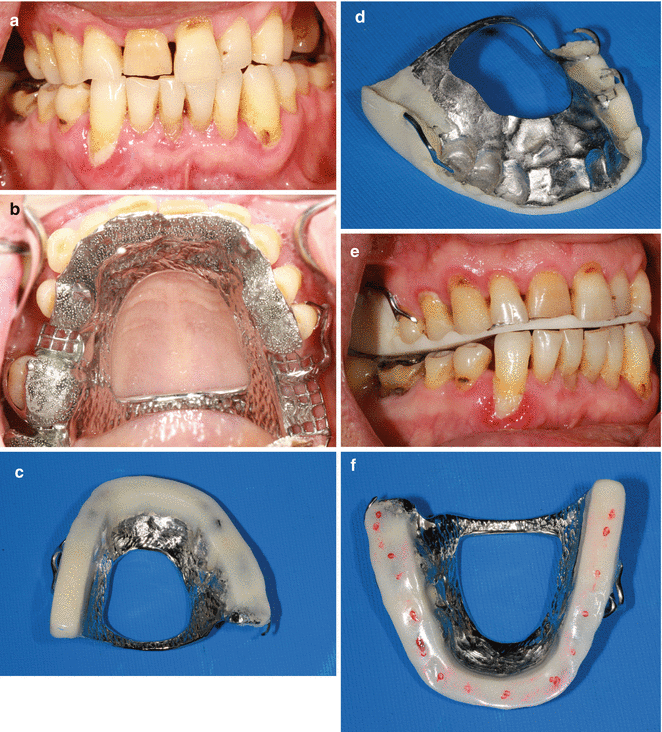
(a) A temporomandibular disorder (TMD) patient with maxillary partial edentulism. Intraoral view in occlusion. (b) The metal framework of the specially designed occlusal splint. Occlusal view. (c) Occlusal splint after positioning using cold curing resin. Occlusal view. (d) Occlusal splint after positioning using cold curing resin. Inner view. (e) Specially designed occlusal splint in the mouth of the patient in occlusion. (f) The occlusal point contacts for each antagonist teeth
-
3.
In cases with edentulous gaps or short free-ending situations (e.g., absence of second molar tooth unilateral or bilateral), the replacement of tooth loss can be done by using the occlusal splint. In such cases, the splint should be placed to the jaw with more tooth loss (Fig. 21.4a, b).
Fig. 21.4 
(a) A mandibular occlusal splint that also replaces the second molar tooth. (b) The occlusal splint in the mouth of the patient
-
4.
In cases with mandibular partial and maxillary complete edentulism, a mandibular RPD and maxillary complete denture should be prepared if the patient has no prosthesis at all. For nighttime use, an additional upper denture (so-called Shore denture) should be placed to function as an occlusal splint (Fig. 21.5a, b).
Fig. 21.5 
A case with maxillary complete and mandibular partial edentulism that needs temporomandibular disorder (TMD) management. (a) A maxillary complete and mandibular removable partial denture is fabricated. (b) A maxillary Shore prosthesis is fabricated for nighttime use as an occlusal splint
-
5.
In cases with mandibular full edentulous arch and maxillary partial edentulism, occlusal splint therapy is contraindicated because of the poor support of mandibular alveolar crest. If the mandibular denture is supported with implants, Shore prosthesis could be constructed for the lower jaw.





Bibliography
Abdel-Fattah RA. Intraoral appliances in management of temporomandibular disorders, revised. Cranio. 1996;14:344–5.
Al-Jabrah O, Al-Shumailan YR. Prevalence of temporomandibular disorder signs in patients with complete versus partial dentures. Clin Oral Investig. 2006;10:167–73.
Amorim VC, Laganá DC, de Paula Eduardo JV, Zanetti AL. Analysis of the condyle/fossa relationship before and after prosthetic rehabilitation with maxillary complete denture and mandibular removable partial denture. J Prosthet Dent. 2003;89:508–14.
Aras K, Hasanreisoğlu U, Shinogaya T. Masticatory performance, maximum occlusal force, and occlusal contact area in patients with bilaterally missing molars and distal extension removable partial dentures. Int J Prosthodont. 2009;22:204–9.
Bessadet M, Nicolas E, Sochat M, Hennequin M, Veyrune JL. Impact of removable partial denture prosthesis on chewing efficiency. J Appl Oral Sci. 2013;21:392–6.
Carlsson GE. Some dogmas related to prosthodontics, temporomandibular disorders and occlusion. Acta Odontol Scand. 2010;68:313–22.
Costen JB. A syndrome of ear and sinus symptoms dependent upon disturbed function of the temporomandibular joint. 1934. Ann Otol Rhinol Laryngol. 1997;106:805–19.
Creugers NH, Witter DJ, Van’t Spijker A, Gerritsen AE, Kreulen CM. Occlusion and temporomandibular function among subjects with mandibular distal extension removable partial dentures. Int J Dent. 2010;2010:807850. doi:10.1155/2010/807850.
Davies SJ, Gray RM, McCord JF. Good occlusal practice in removable prosthodontics. Br Dent J. 2001;191:497–502.
De Boever JA, Carlsson GE, Klineberg IJ. Need for occlusal therapy and prosthodontic treatment in the management of temporomandibular disorders. J Oral Rehabil. 2000;27:647–59.
Farias-Neto A, Martins AP, Sánchez-Ayala A, Rabie AB, Novaes PD, Rizzatti-Barbosa CM. The effect of posterior tooth loss on the expression of type II collagen, IL-1β and VEGF in the condylar cartilage of growing rats. Arch Oral Biol. 2012;57:1551–7.
Kirveskari P, Alanen P. Association between tooth loss and TMJ dysfunction. J Oral Rehabil. 1985;12:189–94.
Krzemień J, Baron S. Axiographic and clinical assessment of temporomandibular joint function in patients with partial edentulism. Acta Bioeng Biomech. 2013;15:19–26.
Kurt H, Erdelt KJ, Cilingir A, Mumcu E, Sülün T, Tuncer N, Gernet W, Beuer F. Two-body wear of occlusal splint materials. J Oral Rehabil. 2012;39:584–90.
Mahönen KT, Virtanen KK. Occlusion and craniomandibular function among patients treated with removable partial dentures. J Oral Rehabil. 1994;21:233–40.
Reissmann DR, Heydecke G, Schierz O, Marré B, Wolfart S, Strub JR, Stark H, Pospiech P, Mundt T, Hannak W, Hartmann S, Wöstmann B, Luthardt RG, Böning KW, Kern M, Walter MH. The randomized shortened dental arch study: temporomandibular disorder pain. Clin Oral Investig. 2014;18:2159–69.
Rues S, Lenz J, Türp JC, Schweizerhof K, Schindler HJ. Muscle and joint forces under variable equilibrium states of the mandible. Clin Oral Investig. 2011;15:737–47.
Sulun T, Geckili O. A simple technique for increasing the occlusal vertical dimension of removable denture wearers. J Calif Dent Assoc. 2011;39:881–3.
Tallents RH, Macher DJ, Kyrkanides S, Katzberg RW, Moss ME. Prevalence of missing posterior teeth and intraarticular temporomandibular disorders. J Prosthet Dent. 2002;87:45–50.
The glossary of prosthetic terms. J Prosthet Dent. 2005;94:10–92.
Türp JC, Schindler H. The dental occlusion as a suspected cause for TMDs: epidemiological and etiological considerations. J Oral Rehabil. 2012;39:502–12.
Wang MQ, Xue F, He JJ, Chen JH, Chen CS, Raustia A. Missing posterior teeth and risk of temporomandibular disorders. J Dent Res. 2009;88:942–5.
Zoidis P, Polyzois G. Removable dental prosthesis splint. An occlusal device for nocturnal bruxing partial denture users. J Prosthodont. 2013;22:652–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Sülün, T. (2016). Management of Temporomandibular Disorders (TMD) in Partially Edentulous Patients. In: Şakar, O. (eds) Removable Partial Dentures. Springer, Cham. https://doi.org/10.1007/978-3-319-20556-4_21
Download citation
DOI: https://doi.org/10.1007/978-3-319-20556-4_21
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-20555-7
Online ISBN: 978-3-319-20556-4
eBook Packages: MedicineMedicine (R0)