
Abstract
The overhead throwing motion creates significant valgus and extension moments at the elbow, which can result in unique injury patterns seen in the throwing athlete. These abnormal forces can result in a multitude of distinct injuries, including ulnar collateral ligament tears and sprains, flexor-pronator mass tears and strains, ulnar neuritis, posteromedial impingement, olecranon stress fractures, osteochondritis dissecans (OCD) of the capitellum, and medial epicondyle apophyseal injuries. Accurate diagnosis and proper treatment of elbow injuries in the throwing athlete requires a thorough understanding of elbow function and anatomy, as well as an understanding of throwing mechanics and pathomechanics. The preoperative evaluation should focus on a thorough history and physical examination, followed by use of specific diagnostic imaging modalities. Recent advances in both nonoperative and operative treatment, including arthroscopic techniques, have afforded the athlete a successful return to competition.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Throwing athlete
- Thrower’s elbow
- Ulnar collateral ligament
- Posteromedial impingement
- Capitellar osteochondritis dissecans
25.1 Introduction
With the growing popularity of overhead throwing sports, and the increasing involvement in year-round competition, overuse injuries to the elbow have become an epidemic among throwing athletes. As more attention has been directed toward this population, a better understanding of throwing biomechanics and the associated pathology has been obtained, and numerous unique injury patterns have been identified.
As the arm passes through the late cocking and early acceleration phases of the throwing motion, tensile stress is placed upon the medial soft tissues, while the lateral and posterior compartments of the elbow experience compressive and medially directed sheer forces, respectively. These abnormal forces can result in a multitude of distinct injuries relating to the thrower’s elbow, including ulnar collateral ligament (UCL) tears, flexor-pronator mass injuries, ulnar neuritis, posteromedial impingement, olecranon stress fractures, osteochondritis dissecans (OCD) of the capitellum, and medial epicondyle apophyseal injuries. Accurate diagnosis and proper care of elbow injuries in the throwing athlete require a thorough understanding of elbow anatomy and function, and numerous unique injury patterns have been identified.
25.2 Functional Anatomy
The elbow is a ginglymus, or hinged, joint, which is comprised of three separate articulations: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The ulnohumeral joint provides the primary bony support of the elbow via a constrained articulation between the distal humeral trochlea and the sigmoid notch of the ulna. In particular, it is the largest contributor to elbow stability at less than 20° of flexion and greater than 120° of flexion, when the coronoid process and olecranon engage their respective fossae on the distal humerus. The radiocapitellar joint provides a lesser degree of valgus stability through resistance of compressive forces at the lateral elbow. Between 20° and 120° of flexion, the majority of the static and dynamic stability of the elbow is provided by surrounding soft tissue structures.
The ulnar collateral ligament (UCL) is the most important static soft tissue contributor to elbow stability in the throwing athlete. The UCL is composed of three distinct components: an anterior bundle, a posterior bundle, and a transverse ligament. The anterior bundle originates on the anteromedial edge of the medial epicondyle of the humerus and inserts on the sublime tubercle of the ulna. The posterior bundle is a fan-shaped fascicle that originates on the posteroinferior medial epicondyle and attaches on the medial aspect of the ulna. The transverse ligament, or Cooper’s ligament, extends from the olecranon to the base of the coronoid process. Previous studies have shown that the anterior bundle of the UCL serves as the primary restraint to valgus force throughout the functional range of motion, between 20° and 120° of flexion [1–3]. The posterior bundle is thinner and weaker, and it provides secondary elbow stability at greater degrees of flexion, while the transverse ligament serves to expand the greater sigmoid notch as a thickening of the joint capsule.
Important dynamic stabilizers of the elbow include the flexor-pronator mass (FPM). This muscular group shares a common origin on the medial epicondyle of the humerus and, from proximal to distal, consists of the pronator teres, flexor carpi radialis (FCR), palmaris longus (when present), flexor digitorum superficialis (FDS), and flexor carpi ulnaris (FCU). Altogether, the flexor-pronator mass assists the UCL in creating the varus torque required to counteract the valgus force generated in the throwing motion. However, biomechanical data has shown that the FCU serves as the primary dynamic restraint to valgus force, as a result of its position in line with the UCL [4].
In throwing athletes, the ulnar nerve can be prone to symptomatology and must be evaluated. The ulnar nerve runs along the medial upper arm and crosses from the anterior to the posterior compartment at the arcade of Struthers before passing through the cubital tunnel at the elbow. The nerve then exits the cubital tunnel between the humeral and ulnar heads of the FCU and runs superficial to the flexor digitorum profundus (FDP) in the forearm.
25.3 Pathophysiology and Biomechanics
The throwing motion has been divided into six phases: windup, early cocking, late cocking, acceleration, deceleration, and follow-through [5–9]. The late cocking/early acceleration and deceleration phases have been identified as being particularly injurious to the thrower’s elbow, as the joint moves from approximately 110 to 20° of flexion with extension velocities approaching 3,000°/s [10]. This violent motion creates significant valgus and extension moments at the elbow, which produce tensile stress on the medial stabilizing structures and compression and medially directed shear forces in the lateral and posterior compartments of the elbow, respectively. This combination of forces may subsequently result in overload of the valgus stabilizers of the elbow resulting in pathologic changes in the medial aspect of the elbow, and it serves as the basic underlying etiology for most pathologic conditions in the thrower’s elbow [11–14].
Tensile stress at the medial elbow is primarily resisted by the anterior bundle of the UCL. Previous studies have shown that the UCL produces approximately 54 % of the varus torque necessary to counteract valgus force on the elbow at 90° of flexion [1]. The maximum valgus torque generated in the overhead throw can exceed 64 N-m, which is roughly twice the ultimate tensile strength of the UCL (32.1 ± 9.6 N-m) [10]. Repetition of these near-tensile failure loads during the overhead throwing motion in the presence of flexor-pronator fatigue can lead to attritional injury or acute rupture of the UCL. Depending upon the throwing athlete’s age, increased stress to the static stabilizers of the medial aspect of the elbow can result in UCL injuries, flexor-pronator injuries, olecranon stress fractures, medial epicondylitis, medial epicondyle apophysitis, and medial epicondyle avulsion injuries [12, 13, 15].
The ulnar nerve is also susceptible to injury secondary to its position at the medial elbow. Even in healthy arms, the overhead throwing motion has been shown to cause increases in ulnar nerve intraneural pressure and cubital tunnel pressure [16–18]. In addition, the throwing motion places upon the nerve a significant amount of strain, which approaches the elastic and circulatory limits of the nerve [19]. This suggests that repetition of the throwing motion can lead to intraneural injury and ischemia, and the nerve could be particularly vulnerable in the presence of concomitant valgus instability. In addition, the presence of osteophytes, flexor-pronator mass hypertrophy, and/or thickening of medial elbow soft tissues can lead to direct compression of the nerve, as well as to restriction of the nerve’s mobility [20].
On the lateral side of the elbow, compressive forces measuring upwards of 500 N have been observed at the radiocapitellar joint during the late cocking and early acceleration phases of throwing [10]. It has been theorized that such pathologic overloading of the lateral elbow compartment leads to changes in the subchondral blood supply, which may result in radiocapitellar chondromalacia, cartilage degeneration, and formation of osteochondral fractures and loose bodies [21].
At the posterior elbow, the combined valgus and extension forces result in a “windshield wiper” effect, where the tip of the olecranon translates medially on the humeral trochlea. During normal kinematics in a healthy elbow, the FPM and UCL function to prevent excessive medial translation and consequential impingement between the olecranon and olecranon fossa. However, in the setting of valgus instability, further impingement may occur at the posteromedial elbow, possibly leading to chondromalacia and osteophyte formation. Classically, this phenomenon has been described during the deceleration phase of the throwing motion at low elbow flexion angles [11, 12, 22–25]. However, recent biomechanical data from Osbahr et al. has confirmed that there are increased contact forces in the posteromedial UCL-deficient elbow at 90° of flexion during the acceleration phase of throwing [13]. This study introduced the concept of ulnohumeral chondral and ligamentous overload (UCLO), which suggests that there is a continuum of abnormal contact forces and resultant posteromedial ulnohumeral impingement throughout the entire arc of the throwing motion in the setting of UCL insufficiency.
25.4 History and Physical Examination
Evaluation of the throwing athlete with elbow pain begins with a thorough history and physical examination. When obtaining the history, it is important to note details regarding sport participation, previous injuries, recent changes in training regimen, and aggravating factors. For pitchers, particular attention should be paid to pitch count, innings pitched, and types of pitches thrown. Any changes in velocity, accuracy, strength, or stamina should also be documented, as these could suggest a chronic UCL injury. If possible, it is also important to determine the phase of throwing during which pain is experienced, as the majority of athletes with valgus instability will report experiencing pain during the late cocking/early acceleration and deceleration phases of the throwing motion [10]. Mechanical symptoms may suggest the presence of intra-articular loose bodies, radiocapitellar osteochondral lesions, posteromedial chondromalacia, or posteromedial olecranon osteophytes.
Inquiry should also be made regarding vascular or neurologic complaints. Numbness or tingling in the hand or fingers, cold intolerance, subjective loss of grip strength, and frequent dropping of objects may indicate an ulnar neuropathy [17, 26]. Ulnar nerve symptoms can present in the setting of nerve subluxation or chronic overuse, or they may provide a clue to additional underlying pathology, such as valgus instability.
The physical examination involves a standardized approach to evaluation of the entire kinetic chain, including the shoulder and elbow, with an intent to truly comprehend how to improve the pathological process relating to the injured throwing athlete. Both upper extremities are first inspected to detect any asymmetry in the forearm musculature, the resting position of the elbow, and the elbow carrying angle. In particular, a more valgus carrying angle may be due to adaptive changes to repetitive abnormal valgus stress placed upon the elbow [27]. While the normal carrying angle is 11° of valgus in men and 13° of valgus in women, King et al. noted that the throwing athlete is commonly found to have a carrying angle >15° [27].
It is important to assess both passive and active range of motion of the elbow compared to the contralateral upper extremity. The normal flexion/extension arc should range from 0° to 140°, while normal pronation and supination should both range approximately 80–90° from neutral. As pointed out by Cain et al., particular attention should be paid to the “end-feel” with the flexion/extension motion arc [12]. The normal “end-feel” of flexion should be that of the soft tissue of the upper arm contacting the soft tissue of the forearm, while extension should conclude with the firm sensation of the olecranon engaging the olecranon fossa. A soft end-feel at terminal extension may indicate a flexion contracture, which is present in approximately half of professional pitchers and not necessarily indicative of an injury [27–29]. Conversely, a firm end-feel that interrupts terminal flexion is generally a pathologic finding, related to osteophytic changes or loose bodies [12].
Palpation of the elbow should employ a systematic approach and investigate both bony landmarks and soft tissue structures. Important bony landmarks include the olecranon, the medial epicondyle, and the radial head. Pain with palpation of the olecranon may indicate an olecranon stress fracture or inflammation due to underlying posteromedial impingement [30, 31]. Tenderness at the medial epicondyle may indicate apophysitis or, in the immature athlete, an avulsion fracture or growth plate injury. The radial head is palpated while the forearm is passively rotated, and the presence of pain may provide a diagnostic clue to an underlying fracture or OCD lesion [21].
Palpation of the soft tissue begins with the UCL. This is performed with the elbow in approximately 50–70° of flexion to displace the FPM anterior to the ligament [12]. The UCL should be palpated from its origin on the medial epicondyle to its insertion on the sublime tubercle of the ulna. Pain with palpation has high sensitivity (81–94 %) but poor specificity (22 %) for ligamentous injury [32, 33]. Tenderness with palpation of the FPM can indicate a muscular strain, which may be an isolated injury or an indication of increased stress due to underlying valgus instability.
The ulnar nerve should be palpated along its course at the medial elbow. Any pain with palpation or paresthesias with percussion at the cubital tunnel should alert the examiner to the possibility of ulnar neuropathy. The nerve should also be examined for subluxation at the medial epicondyle, which can be a source of pain and paresthesias [26, 30, 34].
Provocative maneuvers are an important part of the physical examination of throwing athletes. Maneuvers designed to test for medial instability include the valgus stress test, the moving valgus stress test, and the “milking maneuver.” With the valgus stress test, the patient’s arm is stabilized, the elbow is flexed to approximately 30°, and a valgus stress is applied. In this position, most of the stress is placed on the anterior band of the UCL [15]. The test is positive if there is loss of a firm end point and increased medial sided joint opening when compared to the contralateral upper extremity. The test produces pain in approximately 50 % of patients with a torn UCL, and it has a sensitivity and specificity of 66 and 60 %, respectively [32, 35]. The moving valgus stress test was initially described by O’Driscoll and colleagues and was designed to simulate the valgus force experienced during the overhead throwing motion [36]. The maneuver begins with the patient’s elbow placed in full flexion, and the examiner maintains a constant valgus torque on the elbow while the elbow is quickly extended to approximately 30°. The test is positive if it reproduces the patient’s medial elbow pain between 70° and 120° of flexion. The original study describing the technique reported high sensitivity (100 %) and specificity (75 %) for UCL insufficiency [36]. The “milking maneuver,” however, is performed by pulling on the patient’s thumb with the forearm fully supinated, the shoulder flexed forward, and the elbow flexed beyond 90°. This exam places valgus torque on the elbow in a higher degree of flexion and better assesses the integrity of the posterior band of the UCL. A positive test reveals medial sided elbow pain and instability [37, 38]. For the purpose of valgus stress testing, a cadaveric study by Safran et al. showed that neutral rotation is the best forearm position to reveal valgus laxity [39].
The valgus extension overload test is similar to the moving valgus stress test, but is performed at lower degrees of elbow flexion. The elbow is placed in approximately 20–30° of flexion, a constant valgus force is applied, and the elbow is repeatedly forced into terminal extension [11, 40]. This test attempts to recreate the impingement of the posteromedial olecranon in the olecranon fossa, and the test is positive if it reproduces the pain that the patient experiences during throwing. The active radiocapitellar compression test is used to detect OCD lesions of the radiocapitellar joint. The test is performed by applying an axial load on the fully extended arm, while the patient actively pronates and supinates the forearm. The test is positive if there is pain or crepitus at the lateral compartment of the elbow [21, 40].
25.5 Diagnostic Imaging
Diagnostic imaging should begin with standard anteroposterior and lateral radiographs of the injured elbow, which may reveal osteochondral lesions in the radiocapitellar joint, loose bodies, or changes consistent with chronic instability, such as calcification of the UCL. One may also consider including internal and external oblique views to obtain a full “thrower’s series” of the elbow, as well as an oblique axial view with the elbow in 110° of flexion to visualize posteromedial olecranon osteophytes [11]. Anteroposterior valgus stress views can reveal excessive medial joint line opening. An opening greater than 3 mm has been considered diagnostic of valgus instability [32, 41], while a difference of >0.5 mm compared to the non-injured upper extremity has been shown to be consistent with a UCL tear [42].
Bone scintigraphy and computed tomography (CT) are useful in the assessment of bony pathology, including stress fractures and avulsion fractures. The soft tissue structures around the elbow may be assessed with the use of ultrasound or CT arthrography. In particular, a study by Timmerman et al. showed that CT arthrogram has a high sensitivity (86 %) and specificity (91 %) for UCL injury [35]. However, MRI is largely considered the gold standard for evaluation of soft tissue injuries about the elbow, including ligamentous injury and tendinopathy, as well as injury to the articular cartilage. Standard MRI without contrast has been reported to have a sensitivity of 57–79 % and a specificity of 100 % for diagnosing UCL tears [35, 43]. Enhancement of the MRI with intra-articular saline or gadolinium increases the sensitivity to greater than 90 % and improves diagnosis of partial tears, but it comes with the limitations of being a more invasive and costly test [44, 45]. Standard and enhanced MRI also has an important role in the classification and management of capitellar OCD lesions, as these studies can help identify unstable and high-grade lesions, which may respond poorly to nonoperative treatment [46, 47].
25.6 Prevention
With the growing popularity of overhead throwing sports, and the increasing involvement in year-round competition, overuse injuries to the elbow have become an epidemic among throwing athletes. Coincident with the rise in such injuries has been an increased interest in their prevention. To this end, the USA Baseball Medical & Safety Advisory Committee was created to provide scientifically based information and recommendations to help reduce injury. In 2004, this committee established guidelines for youth baseball players in an effort to reduce the incidence of such injuries [48]. These guidelines, which were partly based on research by the American Sports Medicine Institute, included recommendations for pitch counts, pitch types, pitching mechanics, multiple appearances, multiple leagues, year-round baseball, and physical conditioning [49, 50] (Table 25.1). Adherence to these guidelines has been shown to correlate with the incidence of pitching-related arm pain and pitching-related injuries in multiple studies [50–54]. In particular, a follow-up study by Olsen et al. noted that athletes pitching more than 8 months per year were five times more likely to require shoulder or elbow surgery, and athletes pitching more than 80 pitches per game were four times more likely to require surgery [50]. Additionally, those who only occasionally pitched with a fatigued arm were four times more likely to undergo surgery, while those who regularly pitched with a fatigued arm were 36 times more likely to have an injury that required surgery [50].
Despite the literature supporting the US baseball injury prevention guidelines and the implementation of injury prevention programs, additional research shows that further work must be done to raise public awareness of high-risk throwing activities. A recent study by Ahmad et al. investigated the public perception of UCL reconstruction and found that 31 % of coaches, 28 % of players, and 25 % of parents did not believe that the number of pitches thrown was a risk factor for injury [55]. In addition, 51 % of high school athletes, 37 % of parents, 30 % of coaches, and 26 % of collegiate athletes thought that UCL reconstruction should be performed on players without elbow injury in order to enhance performance. These studies highlight the need for continued endeavors to better educate players, parents, and coaches regarding prevention of overuse throwing injuries [55].
25.7 Valgus Instability/Ulnar Collateral Ligament Injuries
Injury to the UCL was first described in javelin throwers by Waris in 1946 [56]. Since that time, UCL injuries have been reported in increasing frequency among other overhead athletes, particularly baseball pitchers. The UCL is the primary restraint to valgus stress throughout the functional range of motion, between 20° and 120° of flexion, and it is subjected to enormous valgus forces during the throwing motion. These forces approach the ultimate tensile strength of the UCL, and repetition of the overhead throwing motion can lead to attritional injury and/or acute rupture. The most well-studied treatment options for UCL injury include nonoperative management with formal rehabilitation, direct ligament repair, and ligament reconstruction.
Nonoperative management of an isolated UCL injury begins with short-term immobilization to control pain and inflammation, as well as to limit valgus stress on the elbow. This is followed by a comprehensive rehabilitation program as described by Wilk et al., which consists of functional exercises and plyometrics and focuses on pitching mechanics, shoulder kinematics, and motion deficits, as well as strengthening of the core, upper extremities, and lower extremities [57–60]. Once the throwing athlete is pain-free and kinetic chain deficits have been addressed, they may transition to an interval throwing program. This conservative approach is generally indicated in non-throwing athletes and similarly low-demand individuals, and it may also be considered in the immature throwing athlete with a partial tear of the ligament [61]. Skeletally mature, UCL-deficient athletes involved in high-demand throwing sports may not respond well to nonoperative treatment [62, 63]. A study by Rettig reported that 42 % of throwing athletes were able to return to their sport at or above their pre-injury level of play following nonoperative management with appropriate rehabilitation [64]. An injection of platelet-rich plasma (PRP) may be considered, although the data is limited for use in UCL tears. Podesta et al. treated 34 overhead athletes (including 27 professional baseball players) with partial UCL tears with injections of platelet-rich plasma (PRP) and rehabilitation [65]. They reported 88 % excellent results with return to their previous level of competition or higher.
Direct repair of the UCL was initially the treatment of choice for UCL injuries, as early data showed better clinical outcomes when compared to nonoperative treatment [66]. However, additional studies that compared UCL repair to reconstruction found that overhead athletes are more likely to achieve better outcomes and return to their previous level of competition with reconstruction of the ligament [15, 67, 68]. A recent study by Savoie et al. showed that a good indication for UCL repair may be the young athlete with a proximal or distal UCL tear with a good quality ligament. In their retrospective case series of 60 young amateur athletes (mean age, 17.2 years), they reported 93 % good or excellent outcomes following direct repair of proximal or distal UCL tears using suture anchors or suture plication with repair to bone drill holes [69].
Reconstruction of the UCL is often indicated in the high-level overhead throwing athlete who sustains a complete tear of the UCL and wishes to return to throwing sports. Ligament reconstruction is also considered in the throwing athlete who sustains a partial tear of the UCL and continues to have pain and/or instability despite an appropriate course of nonoperative treatment, including a comprehensive rehabilitation program as noted above. Jobe et al. described the first reconstruction technique that afforded players a successful return to competition, utilizing a free-tendon graft placed through bone tunnels in the ulna and medial epicondyle of the humerus in a figure-of-eight fashion [5]. The flexor-pronator origin was detached for the surgical approach, and submuscular transposition of the ulnar nerve was performed. Ten of 16 (63 %) throwing athletes were able to return to their previous level of competition; however, roughly one half of the patients had complications, including five ulnar neuropraxias and one flexor-pronator mass rupture [41].
Since the original figure-of-eight technique was described, multiple modifications have been made in an effort to facilitate anatomic reconstruction, obtain strength similar to the native UCL, and expedite secure graft fixation, all while decreasing morbidity associated with disruption of the flexor-pronator mass and transposition of the ulnar nerve [32, 70–74]. To this end, most modifications have addressed the surgical approach and/or the method of graft fixation on both the ulnar and humeral sides. With regard to the surgical approach, Jobe himself transitioned to a flexor-pronator muscle splitting approach, as described by Smith and Altchek [75], and abandoned obligatory transposition of the ulnar nerve. This modified Jobe technique exhibited improved results with a greater proportion of patients returning to their previous level of play (82 %), as well as a decreased complication rate (12 %) [32].
In 1995, Andrews and Timmerman introduced the American Sports Medicine Institute (ASMI) modification, which utilizes a posterior approach between the two heads of the flexor carpi ulnaris, with elevation of the flexor-pronator mass and obligatory subcutaneous ulnar nerve transposition [67]. This approach leaves the flexor-pronator origin intact and avoids morbidity associated with takedown and repair of the flexor-pronator mass. Cain et al. evaluated the clinical outcome of the ASMI modification in 1,281 throwing athletes and found that 83 % of athletes were able to return to their pre-injury level of competition [76]. Complications occurred in approximately 20 % of the patients, but most (96 %) of these were considered minor, including transient ulnar nerve symptoms.
Modifications for graft fixation have included the docking technique [70], interference screw fixation [71], suture anchor fixation [72], and cortical suspensory fixation [73]. The DANE TJ technique (named in acknowledgement of Drs. David Altchek and Neal ElAttrache, as well as the first professional baseball player to undergo UCL reconstruction and successfully return to competition, Tommy John) is one modification which employs two modern fixation techniques, utilizing interference screw fixation on the ulnar side and the docking technique on the humeral side [74]. To date, the figure-of-eight and docking techniques remain the most well-studied reconstruction techniques with reported long-term outcomes [23, 24, 76–79]. However, regardless of the fixation used, most modern techniques have similar outcomes, with 80–90 % of athletes returning to their previous level of play. An overall complication rate has been reported of between 15 and 20 %, with most consisting of transient ulnar neuropathy and superficial wound infection at either the graft harvest site or the elbow [23, 24, 76–79].
Following surgery, the patient should engage in a four-phase rehabilitation program as described by Wilk et al. and noted above [57–60]. The first phase begins immediately after surgery and continues for 3 weeks. Following the UCL reconstruction, the patient’s arm is placed in a posterior splint to immobilize the elbow at 90° of flexion. The splint is kept in place for 1 week to allow for initial wound healing, and the patient is permitted to perform wrist and hand range of motion and hand grasping exercises during this time. After 1 week, a hinged brace is applied and adjusted to allow motion from 30° to 100° of elbow flexion. The elbow motion is increased in a stepwise fashion until the patient achieves full range of motion by the end of the fifth to sixth week after surgery. The hinged elbow brace is discontinued at the end of the 8th week. During phase II (weeks 4–10) and phase III (weeks 10–16), the patient works on progressive strengthening and continued stretching and flexibility exercises. By week 12 the patient is permitted to begin an isotonic lifting program, including bench press, latissimus dorsi pull downs, seated rows, triceps push downs, and biceps curls. Week 12 also marks the time when the throwing athlete may begin a plyometric throwing program. The first 2 weeks of the plyometric program consist of two-hand throws, such as chest passes, soccer throws, and side throws. During the following 2 weeks, the patient is allowed to transition to one-hand throws. Phase IV (weeks 16 and beyond), the return to activity phase, consists of a formal interval throwing program. Throwing athletes are permitted to begin throwing from the mound approximately 6–8 weeks after initiation of the interval throwing program, and return to competitive throwing can be expected 9–12 months after surgery [57–60].
25.8 Ulnar Neuritis
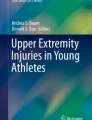
Ulnar nerve neuritis can also occur in overhead throwing athletes secondary to the nerve’s position at the medial elbow, where it is susceptible to compression and traction as well as to inflammation of nearby stabilizing structures. On presentation, athletes typically complain of pain at the medial elbow and sensory disturbance in the ulnar aspect of the hand as well as the ring and small fingers. Overt motor weakness is rare in the thrower, but it can instead present as loss of ball control or difficulty with performance of complex hand tasks. On exam, the physician should determine if there is subluxation or dislocation of the nerve with palpation or elbow range of motion (Fig. 25.1). Patients may also exhibit a positive Tinel sign at the cubital tunnel, as well as a positive elbow flexion test, which reproduces pain, numbness, and tingling in the ulnar nerve distribution with maintained maximum elbow flexion and wrist extension for at least 1 min [80].

(a) Intraoperative examination of the ulnar nerve (dashed line) with the arm in extension identifies the nerve located in its anatomic position behind the medial epicondyle (*). (b) In the setting of ulnar nerve instability, flexion of the arm at the elbow results in dislocation of the nerve (dashed line) anterior to the medial epicondyle (Copyright Daryl C. Osbahr)
In addition to standard radiographic imaging, electrodiagnostic studies including electromyography (EMG) and nerve conduction velocities (NCV) may be obtained as part of the diagnostic work-up in cases with equivocal findings on the physical examination. However, results of such studies must be interpreted with caution, as negative test results do not rule out the diagnosis of ulnar neuritis and symptoms of dynamic compression or traction. Rather, positive findings are typically seen only with chronic or advanced nerve entrapment [18, 26, 33]. Symptoms of ulnar nerve inflammation or compression should alert the physician to possible underlying elbow instability. In a systematic review of athletes undergoing UCL reconstruction, approximately 30 % endorsed concomitant ulnar neuropathy [81]. Similarly, ulnar nerve symptoms are reported in as many as 60 % of throwing athletes with medial epicondylitis. Treatment options for ulnar neuritis include nonoperative management, decompression, medial epicondylectomy, and anterior submuscular or subcutaneous transposition.
Treatment of isolated ulnar neuritis should begin with nonoperative management, including cessation of sports activities, rest, ice, and nonsteroidal anti-inflammatory drugs (NSAIDs). In the presence of nerve subluxation or dislocation, a 2-week trial of immobilization may be indicated, as well. Once the patient is asymptomatic, a stretching routine may be established for the elbow, forearm, and wrist, followed by a progressive isometric strengthening program and gradual return to sport-specific functions [33]. Greater duration and severity of symptoms, as well as presence of concomitant valgus instability, may predict decreased success with nonoperative treatment [82, 83].
Surgical intervention may be considered when nonoperative management fails or when the patient presents with advanced symptoms, such as motor weakness or muscular wasting. There is limited data on use of simple decompression or medial epicondylectomy to treat ulnar neuritis in throwing athletes. However, in the throwing athlete, decompression alone is generally not recommended, as it does not eliminate traction force on the ulnar nerve, and medial epicondylectomy may destabilize the UCL or FPM as well as predispose to ulnar nerve subluxation or dislocation [37, 83, 84]. Most of the available literature focuses on anterior submuscular or subcutaneous transposition of the nerve. Historically, some authors have recommended submuscular transposition for the potential advantage of better protection of the ulnar nerve from direct and indirect trauma [17, 18, 20, 33, 34, 41]. More recently, there has been increasing support for subcutaneous transposition in throwing athletes, as this avoids morbidity associated with disruption of the flexor-pronator mass, especially in overhead athletes [23, 67, 68, 85, 86].
Regardless of the method of surgically addressing the ulnar nerve, the nerve must be adequately released and mobilized to ensure that there is no tethering or compression of the nerve along its entire course. Particular attention should be made to free the nerve proximally from the arcade of Struthers and distally from the fascia between the two heads of the FCU, as these areas have been identified as common causes of incomplete release and recurrent ulnar nerve symptoms [87–89].
We prefer subcutaneous transposition for the aforementioned reasons. The surgical approach is similar to that used for UCL reconstruction, and it begins with a 4–5 cm incision centered over the medial epicondyle. The medial antebrachial cutaneous nerve is identified and protected, and the ulnar nerve is released from the cubital tunnel, as well as its proximal and distal restraints, as noted above. A fascial sling is created from a strip of the medial intermuscular septum. The ulnar nerve is transposed anterior to the medial epicondyle, and the fascial sling is laid loosely over the nerve and sutured to the fascia of the FPM. The elbow is then taken through a gentle range of motion to ensure that the ulnar nerve is able to move freely without compression or tethering. The cubital tunnel and fascia of the FCU are both closed. Meticulous hemostasis is obtained using electrocautery, and a drain is placed with plans for removal before discharge home the same day. The wound is closed in two layers, including a subcuticular closure reinforced with Steri-Strips (3 M, St. Paul, Minnesota). The elbow is splinted at 90° of flexion for 1 week. Following splint removal, the patient is permitted to begin progressive range of motion exercises and rehabilitation.
25.9 Flexor-Pronator Injuries
The flexor-pronator musculature provides dynamic stability to the medial elbow, and it assists the UCL in creating the varus torque necessary to counteract the valgus forces created during the overhead throwing motion. Repetition of the throwing motion can lead to muscular fatigue, chronic tendinosis, attritional injury, and acute rupture of the FPM [12, 90]. On presentation, the throwing athlete will typically describe pain during the late cocking and acceleration phases of the throwing motion. Examination usually reveals tenderness just distal to the FPM origin on the medial epicondyle, and resisted wrist flexion and forearm pronation exacerbate pain. The most significant differential diagnosis which must be ruled out is concomitant injury to the UCL. Studies have shown that FPM injuries accompany approximately 4.3 % of UCL injuries, and the risk of combined FPM and UCL injuries among baseball players increases after 30 years of age [15, 91].
The vast majority of FPM injuries respond well to conservative treatment, including rest, ice, and a course of anti-inflammatory medication, followed by physical therapy and a gradual return to throwing. Surgery is considered in throwers with chronic tendinosis, which does not respond to at least 3–6 months of nonoperative treatment, and in the rare case of complete rupture with associated valgus instability.
The literature on operative treatment and outcomes of FPM injuries is limited. A study by Vangsness showed that approximately 90 % of patients with isolated chronic tendinosis have a good or excellent result, and >95 % of athletes are able to return to sports activities, following detachment of the FPM origin, excision of abnormal tissue, and reattachment of FPM [92]. A more recent case series by Osbahr et al. identified a population of baseball players undergoing UCL reconstruction who sustained concomitant flexor-pronator injuries [91] (Fig. 25.2). Compared to baseball players with isolated UCL injuries, baseball players with combined flexor-pronator and UCL injuries were found to be significantly older (33.4 years versus 20.1 years) and had a significantly lower rate of return to prior level of play (12.5 %) [91].

Coronal T2-weighted MR arthrogram of the elbow demonstrating combined injury to the ulnar collateral ligament (solid arrow) and flexor-pronator mass (dashed arrow). Note the abnormal proximal extension of intra-articular contrast (*) to the level of the medial epicondyle (Copyright Daryl C. Osbahr)
25.10 Medial Epicondyle Apophyseal Injuries
Recent decades have seen an increase in elbow injuries in youth baseball pitchers [53]. This has been attributed to high pitch counts and increased sport participation, including year-round league play, involvement in concurrent leagues, and travel team play [51, 52]. While adolescent athletes are susceptible to UCL injuries, the substantial valgus forces created by the overhead throw more typically affect the relatively weak medial epicondyle apophyseal plate, resulting in medial epicondyle apophysitis and avulsion injuries [12].
Classically, medial epicondyle apophyseal injuries have been thought to result from repetitive microtrauma over a prolonged time period. Early studies by Bennett and Brogdon introduced the concept of “Little Leaguer’s elbow” to describe the clinical and radiographic findings discovered in the throwing arms of youth baseball players [93, 94]. Their patients were noted to present with a prior history of pain, swelling, and tenderness at the medial elbow, and radiographs revealed fragmentation and physeal widening at the medial epicondyle. More recent studies have corroborated their initial reports; however, the aforementioned chronic radiographic findings have since been seen among asymptomatic adolescent baseball athletes, including both pitchers and position players [95–100]. This has created some controversy regarding the overall significance of these findings, as well as their exact incidence among asymptomatic youth throwers. Depending on the study population, the incidence of radiographic widening and fragmentation of the medial epicondyle has been reported to range from 4 to 50 % [95, 97–100].
While medial epicondyle apophysitis generally presents with chronic complaints and findings, medial epicondyle avulsion fractures may occur with a characteristic acute presentation while throwing. A case series by Osbahr et al. reported on eight previously asymptomatic youth baseball players who experienced a sudden acute avulsion fracture during the act of throwing [95]. Patients typically reported a sudden pain or “pop” while throwing and presented with acute pain, swelling, and tenderness, as well as decreased range of motion [95]. Plain radiographs are usually sufficient for diagnosis and most often reveal a Salter-Harris type I fracture, but fragmentation of the epicondyle may be observed. A CT scan may be considered to determine total fracture displacement, as well as to assist with treatment decision making.
As previously noted, prevention is key in the management of elbow injuries in youth athletes, and adherence to the USA Baseball Medical & Safety Advisory Committee guidelines has been shown to correlate with the incidence of youth pitching-related arm pain and pitching-related injuries [48–54]. Beyond prevention, the management of medial epicondyle apophysitis is generally straightforward, and good results have been achieved with rest, ice, and activity modification with occasional bracing or splinting [97]. However, there is still much debate within the literature about the optimal treatment of medial epicondyle fractures [12, 91, 101–104]. Many authors agree that non-displaced fractures may be adequately treated with a brief period of immobilization in a long-arm splint or cast with the elbow flexed to 90°, yet there [12, 103]. Considerable controversy regarding treatment of minimally displaced (2–5 mm) medial epicondyle fractures in throwing athletes, as based upon the notion that minimal degrees of valgus instability may be less tolerable in this population. Surgical decision making is further complicated by the fact that the magnitude of fracture displacement may be underestimated by standard radiographs, and the fact that there is low interobserver and intraobserver agreement as based upon standard radiograph measurements [105, 106]. A CT scan may be obtained if there is uncertainty regarding fracture displacement and optimal treatment, but it comes with the risk of increased radiation exposure. Absolute surgical indications typically include open fractures, gross elbow instability, incarceration of the fracture fragment, or entrapment of the ulnar nerve [103, 107].
When operative treatment is indicated, most authors support open reduction and internal fixation with a single screw, with or without a washer [95, 103, 104]. Postoperatively, the elbow is immobilized at 70–90° of flexion with the forearm in neutral rotation for a maximum of 3 weeks. Patients are then placed in a hinged elbow brace to resist valgus forces. Rehabilitation begins at 3 weeks with physical and occupational therapy to work on range of motion, followed by progressive strengthening and gradual return to physical activity. A throwing program may begin once there is radiographic evidence of fracture union, good upper extremity strength, and pain-free range of motion [95].
25.11 Osteochondritis Dissecans of the Capitellum
Osteochondritis dissecans of the capitellum is another condition that is seen primarily in the adolescent overhead athlete. The exact etiology of this disorder remains controversial, but it is believed to be multifactorial and strongly associated with repeated microtrauma to the poorly vascularized immature capitellum [21, 108, 109]. Vascular studies have shown that the capitellum is primarily supplied by posterior end arteries that traverse the articular cartilage, and there is an absence of significant metaphyseal collateral blood flow [21–111]. The overhead throwing motion produces significant compression forces in the lateral compartment of the elbow, which are believed to cause injury to the aforementioned subchondral end arteries, resulting in ischemia, osteonecrosis, and formation of loose bodies [12, 21, 109, 112].
Historically, the management of capitellar OCD has been based upon multiple factors, including the grade and size of the lesion, as well as the state of the capitellar physis [108, 109, 112–114]. Multiple grading systems have been established and are based upon the appearance of the OCD lesion on plain radiographs, CT, MRI, and arthroscopy [112, 115–117]. In general, each of these systems grades the lesion as stable, unstable but attached, or detached and loose. Nonoperative management is typically reserved for patients with stable lesions and an open capitellar physis, and it includes activity modification, use of nonsteroidal anti-inflammatory drugs (NSAIDs), and cessation of sports participation for 3–6 months. Recent data has shown that approximately 90 % of such patients can expect spontaneous healing with nonoperative management [112, 113].
Operative management is indicated in patients with stable lesions that have failed 6 months of nonoperative management and in patients who present with unstable lesions, articular loose bodies, or mechanical symptoms. The goals of surgery are stimulation of a healing response, removal of loose bodies, and resolution of mechanical symptoms. Surgical treatment options include arthroscopic versus open removal of loose bodies, capitellum debridement, abrasion chondroplasty, fragment excision, fragment fixation, microfracture, humeral osteotomy, or osteochondral autograft transplantation surgery (OATS procedure). Most of the outcome data for surgical treatment of capitellar OCD comes from retrospective case series, which had small sample sizes and/or did not utilize modern arthroscopic techniques [118–126]. This makes it difficult to draw significant conclusions or recommend one procedure over another. A systematic review by de Graaff et al. reported on the findings of nine such studies with 219 total patients undergoing arthroscopic treatment for OCD of the capitellum [127]. This included 41 patients who underwent osteochondral autografting and 178 patients who underwent debridement, drilling, microfracture, and/or fragment fixation depending on the grade of their osteochondral lesion. Those patients undergoing osteochondral autografting had a return to sport rate ranging from 77–90 %, and 94 % were pain-free, while all other patients had a return to sport ranging from 80–100 %, and 84–100 % were pain-free [127].
Ruchelsman et al. provided a useful algorithm on capitellar OCD treatment [21]. They recommend retrograde drilling for lesions with intact overlying cartilage and arthroscopic debridement with marrow stimulation (microfracture) for lesions with unstable cartilage caps or loose bodies. Open osteochondral autograft and allograft procedures are reserved for large defects that involve more than 50 % of the width of the articular surface or that engage the radial head [21]. When an open approach is desired, either a direct lateral or posterolateral approach to the elbow may be used, depending on the location of the lesion.
25.12 Posteromedial Impingement
Impingement of the posteromedial bony and soft tissue structures may occur with the repetitive elbow extension and valgus forces created by the overhead throwing motion, particularly in the setting of UCL insufficiency. Such impingement can result in soft tissue swelling, osteophyte formation, chondromalacia, and the development of intra-articular loose bodies. Athletes may complain of pain at the posterior elbow, swelling, crepitus, locking, and/or loss of terminal extension, and they are likely to present with a positive valgus extension overload test [14, 128–130]. Plain radiographs, especially axial and oblique views, can help identify posterior elbow osteophytic changes, and MRI with intra-articular contrast can be performed to detect loose bodies and inflammation of soft tissue structures.
Treatment of posteromedial impingement begins with prevention, including the early recognition and prompt treatment of UCL insufficiency. Nonoperative management typically consists of NSAIDs and active rest, followed by rehabilitation focusing on the entire kinetic chain, including the lower extremities, core, scapular shoulder, and elbow. Elbow rehabilitation should focus on range of motion, flexibility, and flexor-pronator strengthening. As symptoms resolve, the athlete may be permitted to begin a throwing mechanics program followed by a progressive interval throwing program and a gradual return to competition. If the patient does not obtain relief despite adequate rehabilitation, they may be considered a candidate for arthroscopic or open debridement of the elbow with focus on osteophyte excision, treatment of chondromalacia, and removal of loose bodies.
Arthroscopic debridement has become the treatment of choice, as it allows excision of loose bodies, direct visualization of articular surfaces, drilling of osteochondral defects, and evaluation of the UCL for undersurface tears (Fig. 25.3). To date, there have been very few studies which have specifically investigated the outcomes of arthroscopic debridement for the treatment of posteromedial impingement. Rahusen et al. reported on 16 athletes with isolated posterior impingement who underwent arthroscopic debridement of the olecranon and posterior fossa [131]. There was no comparison group, but their cohort had statistically significant improvement in the modified Andrews elbow scoring system (69/100 preoperatively versus 93/100 postoperatively) and the visual analog scale for pain, both at rest (3/10 versus 0/10) and with activity (7/10 versus 2/10) [131]. Outcome data from other studies has shown that arthroscopic treatment with debridement, olecranon osteophyte excision, and loose body removal has permitted 72–85 % athletes to return to play at their previous level of competition [31, 132, 133]. Additionally, the American Sports Medicine Institute’s 2-year follow-up data on UCL reconstruction showed that athletes had an equivalent or higher return to play rate (86 % versus 82 %) when olecranon osteophyte excision was performed at the same time as their UCL reconstruction, compared to performing UCL reconstruction alone [76]. In the same study, arthroscopic debridement of an olecranon osteophyte was the most common reason for additional surgery, and reoperation for olecranon osteophyte excision after UCL reconstruction carried a worse prognosis for return to play at the same level of competition or higher (71 %) [76].

(a) Arthroscopic examination of an athlete with posteromedial impingement reveals a large posteromedial olecranon osteophyte (*) and associated chondromalacia of the humeral trochlea (circle). (b) Removal of the olecranon osteophyte (dashed line) reveals more extensive cartilage damage and allows further evaluation and treatment of the posterior humeral trochlea (Copyright Daryl C. Osbahr)
When planning to perform arthroscopic excision of olecranon osteophytes, it is important to discuss with the athlete the risk of unmasking or creating valgus instability. A study by Andrews and Timmerman noted that approximately 25 % of professional baseball players who had previously undergone a posteromedial olecranon osteophyte excision required a subsequent UCL reconstruction [67]. This phenomenon may be due to an unmasking of preexisting subclinical valgus instability caused by an insufficient UCL, such as that seen in the setting of ulnohumeral chondral and ligamentous overload, and highlights the importance of early recognition of UCL insufficiency. Similarly, when osteophyte excision is performed, care must be taken to limit the removal of bone to the osteophytic overgrowth, only, as recent studies have shown that overzealous excision involving the native olecranon may result in medial elbow instability [134–137]. A biomechanical study by Kamineni et al. found that resections of the posteromedial aspect of the olecranon >3 mm may jeopardize the function of the anterior bundle of the UCL because it places increased strain upon the ligament [136].
25.13 Olecranon Stress Fractures
Olecranon stress fractures in overhead throwing athletes are thought to be related to the interaction of the osseous and soft tissue restraints of the elbow as they respond to the repetitive, enormous valgus, and extension loads, which are generated during the throwing motion [10, 15]. This includes impingement of the posteromedial olecranon, as well as excessive tensile stress of the triceps tendon and an intact UCL [10, 30]. Patients will typically present with tenderness upon palpation of the posterior olecranon, particularly the posteromedial aspect [30]. Conventional radiographs are an important first step in imaging for stress fractures; however, radiographic findings may not be apparent early in the disease process resulting in a delay in diagnosis [138–143]. For this reason, advanced imaging including bone scintigraphy, MRI, or CT may be necessary to establish a diagnosis.
To further guide diagnosis and treatment, Osbahr et al. established a classification system, which expanded upon previous work by Nakaji et al., to include both skeletally immature and skeletally mature injury patterns [144, 145] (Table 25.2). In general, olecranon stress injuries without a discrete fracture line on imaging will heal well with conservative management, including throwing cessation and active rest with or without use of a bone stimulator, followed by a three-phase rehabilitation program focusing on progressive range of motion, strengthening, and a throwing program [30, 144, 146, 147]. However, in throwing athletes, olecranon stress injuries with a fracture line demonstrated on conventional radiographs may require operative treatment to ensure successful healing and return to play [144, 145, 148–150]. When operative treatment is indicated, many authors support open reduction and internal fixation with the use of a single, cannulated cancellous screw (6.5–7.3 mm) for transverse fracture patterns, while more proximal oblique fracture patterns may require two 4.0 mm screws placed perpendicular to the fracture line [144, 150–152]. Figure-of-eight tension band wiring with either high strength suture or metal wire may be used to supplement the fixation, but may increase the likelihood of reoperation for painful retained hardware [152–154]. Elbow arthroscopy may be employed to aid in fracture reduction, as well as to address other intra-articular pathologies, including loose bodies, osteophytes, and chondromalacia. Additionally, olecranon tip fractures can be treated via arthroscopic debridement with isolated olecranon tip excision [12, 144].
In the largest case series to date, Paci et al. reported on the outcomes of 18 baseball players with olecranon stress fractures, which were treated by open reduction and internal fixation with a single, titanium, cannulated compression screw [152]. All patients went on to successful union, and 17 of the 18 patients (94 %) were able to return to baseball at or above their prior level of play. However, six (33 %) patients required hardware removal, including two for infection. Their series also highlighted the incidence of concomitant and future throwing injuries, including UCL tears (11 %), and the value of using titanium screws to reduce MRI interference should future MRI be warranted [152].
25.14 Summary
The overhead throwing motion creates significant valgus and extension moments at the elbow, which can result in unique injury patterns seen in the throwing athlete. These abnormal forces can result in a multitude of distinct injuries, including ulnar collateral ligament tears and sprains, flexor-pronator mass tears and strains, ulnar neuritis, posteromedial impingement, olecranon stress fractures, osteochondritis dissecans (OCD) of the capitellum, and medial epicondyle apophyseal injuries. Accurate diagnosis and proper treatment of elbow injuries in the throwing athlete requires a thorough understanding of elbow function and anatomy, as well as an understanding of throwing mechanics and pathomechanics. The preoperative evaluation should focus on a thorough history and physical examination, followed by use of specific diagnostic imaging modalities. Recent advances in both nonoperative and operative treatment, including arthroscopic techniques, have afforded the athlete a successful return to competition.
Resources
Morrey BF, An KN (1983) Articular and ligamentous contributions to the stability of the elbow joint. Am J Sports Med 11:315–319
Schwab GH, Bennett JB, Woods GW, Tullos HS (1980) Biomechanics of elbow instability: the role of the medial collateral ligament. Clin Orthop 146:42–52
Morrey BF, Tanaka S, An KN (1991) Valgus stability of the elbow: a definition of primary and secondary constraints. Clin Orthop 265:187–195
Park MC, Ahmad CS (2004) Dynamic contributions of the flexor-pronator mass to elbow valgus stability. J Bone Joint Surg Am 86:2268–2274
Jobe FW, Moynes DR, Tibone JE, Perry J (1984) An EMG analysis of the shoulder in pitching: a second report. Am J Sports Med 12:218–220
Sisto DJ, Jobe FW, Moynes DR, Antoneli DJ (1987) An electromyographic analysis of the elbow in pitching. Am J Sports Med 15:260–263
Glousman RE, Barron J, Jobe FW, Perry J, Pink M (1992) An electromyographic analysis of the elbow in normal injured pitchers with medial collateral ligament insufficiency. Am J Sports Med 20:311–317
DiGiovine NM, Jobe FW, Pink M, Perry J (1992) An electromyographic analysis of the upper extremity in pitching. J Shoulder Elbow Surg 1:15–25
Hamilton CD, Glousman RE, Jobe FW, Brault J, Pink M, Perry J (1996) Dynamic stability of the elbow: electromyographic analysis of the flexor pronator group and the extensor group in pitchers with valgus instability. J Shoulder Elbow Surg 5:347–354
Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF (1995) Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 23:233–239
Wilson FD, Andrews JR, Blackburn TA, McCluskey G (1983) Valgus extension overload in the pitching elbow. Am J Sports Med 11:83–88
Cain EL Jr, Dugas JR, Wolf RS, Andrews JR (2003) Elbow injuries in throwing athletes: a current concepts review. Am J Sports Med 31(4):621–635
Osbahr DC, Dines JS, Breazeale NM, Deng XH, Altchek DW (2010) Ulnohumeral chondral and ligamentous overload: biomechanical correlation for posteromedial chondromalacia of the elbow in throwing athletes. Am J Sports Med 38:2535–2541
Osbahr DC, Dines JS, Rosenbaum AJ, Nguyen JT, Altchek DW (2012) Does posteromedial chondromalacia reduce rate of return to play after ulnar collateral ligament reconstruction. Clin Orthop Relat Res 470:1558–1564
Conway JE, Jobe FW, Glousman RE, Pink M (1992) Medial instability of the elbow in throwing athletes. Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am 74:67–83
Pechan J, Julis I (1975) The pressure measurement in the ulnar nerve: a contribution to the pathophysiology of the cubital tunnel syndrome. J Biomech 8:75–79
Glousman RE (1990) Ulnar nerve problems in the athlete’s elbow. Clin Sports Med 9:365–377
Rokito AS, McMahon PJ, Jobe FW (1996) Cubital tunnel syndrome. Oper Tech Sports Med 4:15–20
Aoki M, Takasaki H, Muraki T, Uchiyama E, Murakami G, Yamashita T (2005) Strain on the ulnar nerve at the elbow and wrist during throwing motion. J Bone Joint Surg Am 87:2508–2514
Boatright JR, D’Alessandro DF (1996) Nerve entrapment syndromes at the elbow. In: Jobe FW, Pink MM, Glousman RE, Kvitne RE, Zemel MP (eds) Operative techniques in upper extremity sports injuries. Mosby-Year Book, St Louis, pp 518–537
Ruchelsman DE, Hall MP, Youm T (2010) Osteochondritis dissecans of the capitellum: current concepts. J Am Acad Orthop Surg 18:557–567
Hyman J, Breazeale NM, Altchek DW (2001) Valgus instability of the elbow in athletes. Clin Sports Med 20:25–45
Dodson CC, Thomas A, Dines JS, Nho SJ, Williams RJ 3rd, Altchek DW (2006) Medial ulnar collateral ligament reconstruction of the elbow in throwing athletes. Am J Sports Med 34:1926–1932
Vitale MA, Ahmad CS (2008) The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med 36:1193–1205
Marshall KW, Marshall DL, Busch MT, Williams JP (2009) Osteochondral lesions of the humeral trochlea in the young athlete. Skeletal Radiol 38:479–491
Del Pizzo W, Jobe FW, Norwood L (1977) Ulnar nerve entrapment syndrome in baseball players. Am J Sports Med 5:182
King JW, Brelsford HJ, Tullos HS (1969) Analysis of the pitching arm of the professional baseball player. Clin Orthop 67:116–123
Brown LP, Niehues SL, Harrah A, Yavorsky P, Hirshman HP (1988) Upper extremity range of motion and isokinetic strength of the internal and external shoulder rotators in major league baseball players. Am J Sports Med 16:577–585
Wright RW, Steger-May K, Wasserlauf BL, O’Neal ME, Weinberg BW, Paletta GA (2006) Elbow range of motion in professional baseball pitchers. Am J Sports Med 34:190–193
Schickendantz MS, Ho CP, Koh J (2002) Stress injury of the proximal ulna in professional baseball players. Am J Sports Med 30(5):737–741
Fideler BM, Kvitne RS, Jordan S (1997) Posterior impingement of the elbow in professional baseball players. J Shoulder Elbow Surg 6:169–170
Thompson WH, Jobe FW, Yocum LA, Pink MM (2001) Ulnar collateral ligament reconstruction in athletes: muscle-splitting approach without transposition of the ulnar nerve. J Shoulder Elbow Surg 10:152–157
Hariri S, Safran MR (2010) Ulnar collateral ligament injury in the overhead athlete. Clin Sports Med 29:619–644
Childress HM (1975) Recurrent ulnar nerve dislocation at the elbow. Clin Orthop 108:168–173
Timmerman LA, Schwartz ML, Andrews JR (1994) Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography. Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med 22:26–32
O’Driscoll SW, Lawton RL, Smith AM (2005) The “moving valgus stress test” for medial collateral ligament tears of the elbow. Am J Sports Med 33(2):231–239
Chen FS, Rokito AS, Jobe FW (2001) Medial elbow problems in the overhead throwing athlete. J Am Acad Orthop Surg 9:99–113
Jones KJ, Osbahr DO, Schrumpf MA, Dines JS, Altcheck DW (2012) Ulnar collateral ligament reconstruction in throwing athletes: a review of current concepts. J Bone Joint Surg Am 94:e49(1–12)
Safran MR, McTarry MH, Shin S, Han S, Lee TQ (2005) Effects of elbow flexion and forearm rotation on valgus laxity of the elbow. J Bone Joint Surg Am 87(9):2065–2074
Dugas JR (2010) Valgus extension overload: diagnosis and treatment. Clin Sports Med 29(4):645–654
Jobe FW, Stark H, Lombardo SJ (1986) Reconstruction of the ulnar collateral ligament in athletes. J Bone Joint Surg Am 68(8):1158–1163
Rijke AM, Goltz HT, McCue FC, Andrews JR, Berr SS (1994) Stress radiography of the medial elbow ligaments. Radiology 191:213–216
Ouellette H, Bredella M, Labis J, Palmer WE, Torriani M (2008) MR imaging of the elbow in baseball pitchers. Skeletal Radiol 37:115–121
Schwartz ML, Al-Zahrani S, Morwessel RM, Andrews JR (1995) Ulnar collateral ligament injury in the throwing athlete: evaluation with saline-enhanced MR arthrography. Radiology 197:297–299
Hill NB Jr, Bucchieri JS, Shon F, Miller TT, Rosenwasser MP (2000) Magnetic resonance imaging of injury to the medial collateral ligament of the elbow: a cadaver model. J Shoulder Elbow Surg 9:418–422
Kijowski R, De Smet AA (2005) MRI findings of osteochondritis dissecans of the capitellum with surgical correlation. Am J Roentgenol 185(6):1453–1459
Takahara M, Mura N, Sasaki J, Harada M, Ogino T (2007) Classification, treatment, and outcome of osteochondritis dissecans of the humeral capitellum. J Bone Joint Surg Am 89(6):1205–1214
USA Baseball Medical & Safety Advisory Committee. Youth baseball pitching injuries. 30 Nov 2008. http://web.usabaseball.com. Accessed 10 June 2014
Lyman S, Fleisig GS, Andrews JR, Osinski ED (2002) Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med 30:463–468
Olsen SJ 2nd, Fleisig GS, Dun S, Loftice J, Andrews JR (2006) Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med 34:905–912
Register-Mihalik JK, Oyama S, Marshall SW, Mueller FO (2012) Pitching practices and self-reported injuries among youth baseball pitchers: a descriptive study. Athl Train Sports Health Care 4:11–20
Fleisig GS, Andrews JR, Cutter GR et al (2011) Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med 39:253–257
Flesig GS, Andrews JR (2012) Prevention of elbow injuries in youth baseball pitchers. Sports Health 4(5):419–424
Yang J, Mann BJ, Guettler JH, Dugas JR, Irrgang JJ, Fleisig GS, Albright JP (2014) Risk-prone pitching activities and injuries in youth baseball: findings from a national sample. Am J Sports Med 42:1456–1463
Ahmad CS, Grantham WJ, Greiwe RM (2012) Public perceptions of Tommy John surgery. Phys Sportsmed 40(2):64–72
Waris W (1946) Elbow injuries of javelin-throwers. Acta Chir Scand 93:563–575
Wilk KE, Arrigo CA, Andrews JR (1993) Rehabilitation of the elbow in the throwing athlete. J Orthop Sports Phys Ther 17:305–317
Wilk KE, Arrigo CA, Andrews JR et al (1996) Rehabilitation following elbow surgery in the throwing athlete. Oper Tech Sports Med 4:114–132
Wilk KE, Arrigo CA, Andrews JR et al (1996) Preventative and rehabilitation exercises for the shoulder and elbow, 4th edn. American Sports Medicine Institute, Birmingham
Wilk KE, Azar FM, Andrews JR (1995) Conservative and operative rehabilitation of the elbow in sports. Sports Med Arthrosc Rev 3:237–258
Bruce JR, Andrews JR (2014) Ulnar collateral ligament injuries in the throwing athlete. J Am Acad Orthop Surg 22:315–325
Arendt EA (ed) (1999) Orthopaedic knowledge update: sports medicine. American Academy of Orthopaedic Surgeons, Rosemont, pp 225–235
Kenter K, Behr CT, Warren RF, O’Brien SJ, Barnes R (2000) Acute elbow injuries in the national football league. J Shoulder Elbow Surg 9:1–5
Rettig AC, Sherrill C, Snead DS, Mendler JC, Mieling P (2001) Nonoperative treatment of ulnar collateral ligament injuries in throwing athletes. Am J Sports Med 29:15–17
Podesta L, Crow SA, Volkmer D, Bert T, Yocum LA (2013) Treatment of partial ulnar collateral ligament tears in the elbow with platelet-rich plasma. Am J Sports Med 41(7):1689–1694
Barnes DA, Tullos HS (1978) An analysis of 100 symptomatic baseball players. Am J Sports Med 6:62–67
Andrews JR, Timmerman LA (1995) Outcome of elbow surgery in professional baseball players. Am J Sports Med 23:407–413
Azar FM, Andrews JR, Wilk KE, Groh D (2000) Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 28:16–23
Savoie FH 3rd, Trenhaile SW, Roberts J, Field LD, Ramsey JR (2008) Primary repair of ulnar collateral ligament injuries of the elbow in young athletes: a case series injuries to the proximal and distal ends of the ligament. Am J Sports Med 36:1066–1072
Rohrbough JT, Altchek DW, Hyman J, Williams RJ 3rd, Botts JD (2002) Medial collateral ligament reconstruction of the elbow using the docking technique. Am J Sports Med 30(4):541–548
Ahmad CS, Lee TQ, ElAttrache NS (2003) Biomechanical evaluation of a new ulnar collateral ligament reconstruction technique with interference screw fixation. Am J Sports Med 31(3):332–337
Hechtman KS, Zvijac JE, Wells ME, Botto-van Bemden A (2011) Long-term results of ulnar collateral ligament reconstruction in throwing athletes based on a hybrid technique. Am J Sports Med 39(2):342–347
Jackson TJ, Adamson GJ, Peterson A, Patton J, McGarry MH, Lee TQ (2013) Ulnar collateral ligament reconstruction using bisuspensory fixation: a biomechanical comparison with the docking technique. Am J Sports Med 41(5):1158–1164
Dines JS, ElAttrache NS, Conway JE, Smith W, Ahmad CS (2007) Clinical outcomes of the DANE TJ technique to treat ulnar collateral ligament insufficiency of the elbow. Am J Sports Med 35(12):2039–2044
Smith GR, Altchek DW, Pagnani MJ, Keeley JR (1996) A muscle-splitting approach to the ulnar collateral ligament of the elbow. Neuroanatomy and operative technique. Am J Sports Med 24:575–580
Cain EL Jr, Andrews JR, Dugas JR, Wilk KE, McMichael CS, Walter JC, Riley RS, Arthur ST (2010) Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: results in 743 athletes with minimum 2-year follow-up. Am J Sports Med 38:2426–2434
Koh JL, Schafer MF, Keuter G, Hsu JE (2006) Ulnar collateral ligament reconstruction in elite throwing athletes. Arthroscopy 22:1187–1191
Paletta GA Jr, Wright RW (2006) The modified docking procedure for elbow ulnar collateral ligament reconstruction: 2-year follow-up in elite throwers. Am J Sports Med 34:1594–1598
Bowers AL, Dines JS, Dines DM, Altchek DW (2010) Elbow medial ulnar collateral ligament reconstruction: clinical relevance and the docking technique. J Shoulder Elbow Surg 19(2 Suppl):110–117
Buehler MJ, Thayer DT (1988) The elbow flexion test: a clinical test for the cubital tunnel syndrome. Clin Orthop 233:213–216
Watson JN, McQueen P, Hutchinson MR (2014) A systematic review of ulnar collateral ligament reconstruction techniques. Am J Sports Med 42:2510–2516
Grana W (2001) Medial epicondylitis and cubital tunnel syndrome in the throwing athlete. Clin Sports Med 20:541–548
Cummins CA, Schneider DS (2009) Peripheral nerve injuries in baseball players. Phys Med Rehabil Clin N Am 20:175–193
Aldridge JW, Bruno RJ, Strauch RJ, Rosenwasser MP (2001) Nerve entrapment in athletes. Clin Sports Med 20(1):95–122
Rettig AC, Ebben JR (1993) Anterior subcutaneous transfer of the ulnar nerve in the athlete. Am J Sports Med 21:836–840
Petty DH, Andrews JR, Fleisig GS, Cain EL (2004) Ulnar collateral ligament reconstruction in high school baseball players: clinical results and injury risk factors. Am J Sports Med 32:1158–1164
Gabel GT, Amadio PC (1990) Reoperation for failed decompression of the ulnar nerve in the region of the elbow. J Bone Joint Surg 72A:213–219
Kleinman WB (1994) Revision ulnar neuroplasty. Hand Clin 10:461–477
Mackinnon SE, Novak CB (2007) Operative findings in reoperation of patients with cubital tunnel syndrome. Hand (N Y) 2:137–143
Norwood LA, Shook JA, Andrews JR (1981) Acute medial elbow ruptures. Am J Sports Med 9:16–19
Osbahr DC, Swaminathan SS, Allen AA, Dines JS, Coleman SH, Altchek DW (2010) Combined flexor-pronator mass and ulnar collateral ligament injuries in the elbows of older baseball players. Am J Sports Med 38:733–739
Vangsness CT, Jobe FW (1991) Surgical treatment of medial epicondylitis. Results in 35 elbows. J Bone Joint Surg Br 73:409–411
Brogdon BG, Crow NE (1960) Little Leaguer’s elbow. Am J Roentgenol Radium Ther Nucl Med 83:671–675
Bennett GE (1959) Elbow and shoulder lesions of baseball players. Am J Surg 98:484–492
Osbahr DC, Chalmers PN, Frank JS, Williams RJ III, Widmann RF, Green DW (2010) Acute, avulsion fractures of the medial epicondyle while throwing in youth baseball players: a variant of Little League elbow. J Shoulder Elbow Surg 19:951–957
Adams JE (1973) Little league elbow. Calif Med 118:34–35
Torg JS, Pollack H, Sweterlitsch P (1972) The effect of competitive pitching on shoulders and elbows of preadolescent baseball players. Pediatrics 49:267–272
Gugenheim JJ Jr, Stanley RF, Woods GW, Tullos HS (1976) Little League survey: the Houston study. Am J Sports Med 4:189–200
Hang DW, Chao CM, Hang YS (2004) A clinical and roentgenographic study of Little League elbow. Am J Sports Med 32:79–84
Larson RL, Singer KM, Bergstrom R, Thomas S (1976) Little League survey: the Eugene study. Am J Sports Med 4:201–209
Farsetti P, Potenza V, Caterini R, Ippolito E (2001) Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 83:1299–1305
Lee HH, Shen HC, Chang JH, Lee CH, Wu SS (2005) Operative treatment of medial epicondyle fractures in children and adolescents. J Shoulder Elbow Surg 14:178–185
Gottschalk HP, Eisner E, Hosalkar HS (2012) Medial epicondyle fractures in the pediatric population. J Am Acad Orthop Surg 20:223–232
Lawrence JTR, Neeraj PM, Macknin J, Flynn JM, Cameron D, Wolfgruber JC, Ganley TJ (2013) Return to competitive sports after medial epicondyle fractures in adolescent athletes: results of operative and nonoperative treatment. Am J Sports Med 41:1152–1157
Patel NM, Ganley TJ (2012) Medial epicondyle fractures of the humerus: how to evaluate and when to operate. J Pediatr Orthop 32(Suppl 1):S10–S13
Edmonds EW (2010) How displaced are “nondisplaced” fractures of the medial humeral epicondyle in children? Results of a three-dimensional computed tomography analysis. J Bone Joint Surg Am 92(17):2785–2791
Pappas N, Lawrence JT, Donegan D, Ganley T, Flynn JM (2010) Intraobserver and interobserver agreement in the measurement of displaced humeral medial epicondyle fractures in children. J Bone Joint Surg Am 92(2):322–327
Schenck RC Jr, Goodnight JM (1996) Osteochondritis dissecans. J Bone Joint Surg Am 78(3):439–456
Bradley JP, Petrie RS (2001) Osteochondritis dissecans of the humeral capitellum: diagnosis and treatment. Clin Sports Med 20(3):565–590
Yadao MA, Field LD, Savoie FH III (2004) Osteochondritis dissecans of the elbow. Instr Course Lect 53:599–606
Yamaguchi K, Sweet FA, Bindra R, Morrey BF, Gelberman RH (1997) The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 79(11):1653–1662
Takahara M, Ogino T, Takagi M, Tsuchida H, Orui H, Nambu T (2000) Natural progression of osteochondritis dissecans of the humeral capitellum: initial observations. Radiology 216(1):207–212
Mihara K, Tsutsui H, Nishinaka N, Yamaguchi K (2009) Nonoperative treatment for osteochondritis dissecans of the capitellum. Am J Sports Med 37(2):298–304
Ahmad C, El Attrache N (2006) Treatment of capitellar osteochondritis dissecans. Tech Should Elbow Surg 7(4):169–174
Minami M, Nakashita K, Ishii S et al (1979) Twenty-five cases of osteochondritis dissecans of the elbow. Rinsho Seikei Geka 14:805–810
Nelson DW, DiPaola J, Colville M, Schmidgall J (1990) Osteochondritis dissecans of the talus and knee: prospective comparison of MR and arthroscopic classifications. J Comput Assist Tomogr 14(5):804–808
Baumgarten TE, Andrews JR, Satterwhite YE (1998) The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 26(4):520–523
Micheli LJ, Luke AC, Mintzer CM, Waters PM (2001) Elbow arthroscopy in the pediatric and adolescent population. Arthroscopy 17:694–699
Takeda H, Watarai K, Matsushita T, Saito T, Terashima Y (2002) A surgical treatment for unstable osteochondritis lesions of the humeral capitellum in adolescent baseball players. Am J Sports Med 30:713–717
Rahusen FT, Brinkman JM, Eygendaal D (2006) Results of arthroscopic debridement for osteochondritis dissecans of the elbow. Br J Sports Med 40:966–969
Brownlow HC, O’Connor-Read LM, Perko M (2006) Arthroscopic treatment of osteochondritis dissecans of the capitellum. Knee Surg Sports Traumatol Arthrosc 14:198–202
Yamamoto Y, Ishibashi Y, Tsuda E, Sato H, Toh S (2006) Osteochondral autograft transplantation for osteochondritis dissecans of the elbow in juvenile baseball players: minimum 2-year follow-up. Am J Sports Med 34:714–720
Nobuta S, Ogawa K, Sato K, Nakagawa T, Hatori M, Itoi E (2008) Clinical outcome of fragment fixation for osteochondritis dissecans of the elbow. Ups J Med Sci 113:201–208
Iwasaki N, Kato H, Ishikawa J, Masuko T, Funakoshi T, Minami A (2009) Autologous osteochondral mosaicplasty for osteochondritis dissecans of the elbow in teenage athletes. J Bone Joint Surg Am 91:2359–2366
Mihara K, Suzuki K, Makiuchi D, Mishinaka N, Yamaguchi K, Tsutsui H (2010) Surgical treatment for osteochondritis dissecans of the humeral capitellum. J Shoulder Elbow Surg 19:31–37
Jones KJ, Wiesel BB, Sankar WN, Ganley TJ (2010) Arthroscopic management of osteochondritis dissecans of the capitellum: mid-term results in adolescent athletes. J Pediatr Orthop 30:8–13
de Graaff F, Krijnen MR, Poolman RW, Willems WJ (2011) Arthroscopic surgery in athletes with osteochondritis dissecans of the elbow. Arthroscopy 27(7):986–993
Andrews JR, Wilk KE, Satterwhite YE, Tedder JI (1993) Physical examination of the thrower’s elbow. J Orthop Sports Phys Ther 17(6):296–304
Miller CD, Savoie FH 3rd (1994) Valgus extension injuries of the elbow in the throwing athlete. J Am Acad Orthop Surg 2:261–269
Moskal MJ (2001) Arthroscopic treatment of posterior impingement of the elbow in athletes. Clin Sports Med 20:11–24
Rahusen FT, Brinkman JM, Eygendaal D (2009) Arthroscopic treatment of posterior impingement of the elbow in athletes: a medium-term follow-up in 16 cases. J Shoulder Elbow Surg 18(2):279–282
Eygendaal D, Safran MR (2006) Postero-medial elbow problems in the adult athlete. Br J Sports Med 40(5):430–434
Reddy AS, Kvitne RS, Yocum LA, ElAttrache NS, Glousman RE, Jobe FW (2000) Arthroscopy of the elbow: a long-term clinical review. Arthroscopy 16(6):588–594
Andrews JR, Heggland EJH, Fleisig GS, Zheng N (2001) Relationship of ulnar collateral ligament strain to amount of medial olecranon osteotomy. Am J Sports Med 29(6):716–721
Kamineni S, Hirahara H, Pomianowski S, Neale PG, O’Driscoll SW, ElAttrache N, An KN, Morrey BF (2003) Partial posteromedial olecranon resection: a kinematic study. J Bone Joint Surg Am 85-A(6):1005–1011
Kamineni S, ElAttrache NS, O’Driscoll SW, Ahmad CS, Hirohara H, Neale PG, An KN, Morrey BF (2004) Medial collateral ligament strain with partial posteromedial olecranon resection. A biomechanical study. J Bone Joint Surg Am 86-A(11):2424–2430
Inagaki K (2013) Current concepts of elbow-joint disorders and their treatment. J Orthop Sci 18:1–7
Greaney RB, Gerber FH, Laughlin RL, Kmet JP, Metz CD, Kilcheski TS, Rao BR, Silverman ED (1983) Distribution and natural history of stress fractures in U.S. Marine recruits. Radiology 146(2):339–346
Stafford SA, Rosenthal DI, Gebhardt MC, Brady TJ, Scott JA (1986) MRI in stress fracture. AJR Am J Roentgenol 147(3):553–556
Daffner RH, Pavlov H (1992) Stress fractures: current concepts. AJR Am J Roentgenol 159(2):245–252
Anderson MW, Greenspan A (1996) Stress fractures. Radiology 199(1):1–12
Spitz DJ, Newberg AH (2002) Imaging of stress fractures in the athlete. Radiol Clin North Am 40(2):313–331
Sofka CM (2006) Imaging of stress fractures. Clin Sports Med 25(1):53–62
Osbahr DC, Bedi A, Conway JE (2012) Olecranon stress fractures. In: Dines JS, ElAttrache NS, Altchek DW, Andrews JR, Yocum LA, Wilk KE (eds) Sports medicine in baseball. Lippincott Williams and Wilkins, Philadelphia
Nakaji N, Fujioka H, Tanaka J, Sugimoto K, Yoshiya S, Fujita K, Kurosaka M (2006) Stress fracture of the olecranon in an adult baseball player. Knee Surg Sports Traumatol Arthrosc 14(4):390–393
Mamanee P, Neira C, Martire JR, McFarland EG (2000) Stress lesion of the proximal medial ulna in a throwing athlete. A case report. Am J Sports Med 28(2):261–263
Blake JJ, Block JJ, Hannah GA, Kan JH (2008) Unusual stress fracture in an adolescent baseball pitcher affecting the trochlear groove of the olecranon. Pediatr Radiol 38(7):788–790
Nuber GW, Diment MT (1992) Olecranon stress fractures in throwers. A report of two cases and a review of the literature. Clin Orthop Relat Res 278:58–61
Suzuki K, Minami A, Suenaga N, Kondoh M (1997) Oblique stress fracture of the olecranon in baseball pitchers. J Shoulder Elbow Surg 6(5):491–494
Rettig AC, Wurth TR, Mieling P (2006) Nonunion of olecranon stress fractures in adolescent baseball pitchers: a case series of 5 athletes. Am J Sports Med 34(4):653–656
Hutchinson DT, Horwitz DS, Ha G, Thomas CW, Bachus KN (2003) Cyclic loading of olecranon fracture fixation constructs. J Bone Joint Surg Am 85-A(5):831–837
Paci JM, Dugas JR, Guy JA, Cain EL, Fleisig GS, Hurst C, Wilk KE, Andrews JR (2012) Cannulated screw fixation of refractory olecranon stress fractures with and without associated injuries allows a return to baseball. Am J Sports Med 41(2):306–312
Carofino BC, Santangelo SA, Kabadi M, Mazzocca AD, Browner BD (2007) Olecranon fractures repaired with FiberWire or metal wire tension banding: a biomechanical comparison. Arthroscopy 23(9):964–970
Sahajpal D, Wright TW (2009) Proximal ulna fractures. J Hand Surg Am 34(2):357–362
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Warrell, C.S., Osbahr, D.C., Andrews, J.R. (2016). Thrower’s Elbow. In: Volpi, P. (eds) Arthroscopy and Sport Injuries. Springer, Cham. https://doi.org/10.1007/978-3-319-14815-1_25
Download citation
DOI: https://doi.org/10.1007/978-3-319-14815-1_25
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-14814-4
Online ISBN: 978-3-319-14815-1
eBook Packages: MedicineMedicine (R0)