
Abstract
Acute respiratory distress syndrome (ARDS) is a heterogeneous disease, which is defined by the acute onset of hypoxemic respiratory failure with bilateral infiltrates on chest radiography due primarily to non-cardiogenic pulmonary edema [1]. Only two supportive strategies have shown to improve survival in patients with acute lung injury (ALI)/ARDS, namely lung protective ventilation that reduces the stretch of the lungs and a conservative fluid strategy [2, 3]. The mortality of ARDS, however, remains high and no pharmacological therapies have effectively improved the outcome of these patients so far.
Studies of the pharmacologic management of ARDS, such as trials of anti-inflammatory agents, anticoagulants, surfactant, vasodilators, and β2 agonists, have shown conflicting results [4]. Potential reasons for such conflicting results may be: In the last decade, there has been extensive research into potential therapeutic targets and methods of drug administration that could help in the development of specific pharmacological drugs to prevent or mitigate the development of ARDS.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
- Acute Lung Injury
- Acute Respiratory Distress Syndrome
- Neutrophil Elastase
- Trefoil Factor Family
- Neutrophil Elastase Inhibitor
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Acute respiratory distress syndrome (ARDS) is a heterogeneous disease, which is defined by the acute onset of hypoxemic respiratory failure with bilateral infiltrates on chest radiography due primarily to non-cardiogenic pulmonary edema [1]. Only two supportive strategies have shown to improve survival in patients with acute lung injury (ALI)/ARDS, namely lung protective ventilation that reduces the stretch of the lungs and a conservative fluid strategy [2, 3]. The mortality of ARDS, however, remains high and no pharmacological therapies have effectively improved the outcome of these patients so far.
Studies of the pharmacologic management of ARDS, such as trials of anti-inflammatory agents, anticoagulants, surfactant, vasodilators, and β2 agonists, have shown conflicting results [4]. Potential reasons for such conflicting results may be:
-
1)
the heterogeneity of the pathophysiologic processes leading to lung injury;
-
2)
failure to apply therapies to subgroups of patients with an homogeneous disease process; and
-
3)
inappropriate dosing and route of administration of the drugs.
In the last decade, there has been extensive research into potential therapeutic targets and methods of drug administration that could help in the development of specific pharmacological drugs to prevent or mitigate the development of ARDS.
Pathophysiology
Early in ARDS, there is widespread neutrophilic alveolitis with disruption of the alveolar epithelial and endothelial barriers, which leads to the formation of protein-rich edema in the interstitium and alveolar spaces [5]. There is activation of alveolar macrophages and neutrophil recruitment, cell death in the alveolar epithelium and vascular endothelium, deposition of hyaline membranes on the denudated basement membrane, deficient surfactant production that contributes to alveolar collapse, and formation of microthrombi. This scenario evolves to a fibro-proliferative process that fills the airspaces with granulation tissue containing proliferating alveolar type II cells, as well as new blood vessels and extracellular matrix rich in collagen and fibrin. In some patients, this process progresses to irreversible lung fibrosis [6].
Modulation of Neutrophil Migration and Activation
A considerable quantity of neutrophils is present in the bronchoalveolar lavage (BAL) fluid from patients with ARDS. Persistence of elevated numbers of neutrophils correlates with worsening gas exchange and with poor prognosis [7]. The regulation of neutrophil lifespan is known to be critical for maintaining an effective host response and preventing excessive inflammation. One of the mechanisms that controls the number of neutrophils in the lung is the induction of apoptosis. Interestingly, neutrophils are less susceptible to undergo apoptosis under hypoxic conditions, as occurs in the alveoli in ARDS. In this line, the hypoxia-inducible factor (HIF) oxygen-sensing pathway has been shown to play a role in prolonging neutrophil survival during hypoxia. The expression and transcriptional activity of HIF are regulated by the oxygen-sensitive prolyl hydroxylases (PHD1-3) [8]. This suggests that modulation of HIF and PHD1-3 expression aimed at enhancing neutrophil apoptosis may be a potential approach to downregulate inflammation in the early phase of ARDS.
Active neutrophils release a series of enzymes that contribute to lung damage. Neutrophil elastase is a serine protease stored in the azurophilic granules of leukocytes that has been implicated in the pathology of ARDS. Neutrophil elastase seems to promote inflammation, endothelial and epithelial cell injury, extracellular matrix damage and collagen deposition that leads pulmonary fibrosis [9–11]. Sivelestat was the first neutrophil elastase inhibitor tested in humans and it suppressed the production of neutrophil elastase and interleukin (IL)-8, resulting in improved respiratory function in patients with ARDS secondary to cardiopulmonary bypass [12]. In animal models of lung fibrosis, sivelestat not only decreased inflammatory cell recruitment in the acute phase, but also reduced collagen deposition in lung parenchyma in the fibroproliferative phase of ARDS resulting in less fibrosis and better static compliance of the lung. This beneficial effect was also associated with a decrease in transforming growth factor (TGF)-β1 activation and expression of phospho-SMAD2/3, which are mechanisms involved in lung fibrosis [9, 11]. AZD9668 (N-{[5-(methanesulfonyl)pyridin-2-yl]methyl}-6-methyl-5-(1-methyl-1H-pyrazol-5-yl)-2-oxo-1-[3-(trifluoromethyl)phenyl]-1,2-dihydropyridine-3-carboxamide) is another novel neutrophil elastase inhibitor that can be administered orally. It exerts selective and rapid inhibition of neutrophil elastase that is also reversible. Oral administration of AZD9668 to mice or rats prevented human neutrophil elastase-induced lung tissue injury as assessed by decreased matrix protein degradation products in BAL fluid and reduced inflammatory responses in the lung in acute and chronic lung injury models. Therefore, neutrophil elastase inhibitors may be drugs that could potentially reduce lung inflammation and diminish structural and functional pulmonary changes in human ARDS [13].
Endothelial Protection
Because the cardinal feature of ALI/ARDS is an increase in lung vascular permeability, often precipitated by an exuberant inflammatory response with subsequent endothelial barrier disruption, strategies aimed at promoting endothelial barrier function could serve as novel therapies in this setting. In this regard, several promising agonists have been identified, including lipid mediators (sphingosine 1-phosphate, resolvins), statins, ang-1/2-Tie2 system and activated protein C (APC). All these agonists have in common the ability to directly mediate endothelial cell signaling and induce characteristic actin cytoskeletal rearrangement leading to endothelial cell barrier protection [14].
Sphingosine 1-phosphate
There is increasing evidence that sphingolipids contribute to different pulmonary disorders, including ALI. Sphingolipids are essential constituents of plasma membranes and regulate many pathophysiological cellular responses inducing apoptosis and cell survival, vascular permeability, mast cell activation, and airway smooth muscle functions [15].
Sphingosine-1-phosphate (S1P) exerts a protective effect against ALI. S1P is a potent angiogenic factor that preserves human lung endothelial cell integrity and barrier function [16] preventing the alveolar flooding demonstrated in animal models of ARDS. S1P is a naturally occurring bioactive sphingolipid that acts extracellularly (via its G protein-coupled receptors, S1P1-5) and intracellularly on various targets. The synthesis of S1P is catalyzed by sphingosine kinases 1 and 2, and the degradation of S1P is mediated by lipid S1P phosphatases and S1P lyase, contributing to the control of the S1P cellular responses [15, 16] (Fig. 1). S1P enhances vascular barrier function through a series of cellular events initiated by activation of its G-protein coupled receptor, S1P1, and the subsequent downstream activation of Rho and Rac1. Activation of these intracellular signals results in endothelial cytoskeletal reorganization to form strong cortical actin rings in the cell periphery, and reinforcement of focal adhesions and paracellular junctional complexes (cadherin, paxillin, catenins, zona occludens), that prevent excessive vascular permeability [16, 17].


Overview of sphingolipid metabolism. Arrows indicate regulatory enzymes
Recent studies show that stimulating the S1P-SIP1 axis reduces vascular permeability, which can be of great value to treat ARDS. S1Ps and S1P analogs, such as FTY720 and ftysiponate, serve as protective agents limiting the disruption of the pulmonary microvascular endothelial barrier and lung edema formation, as well as attenuating parenchymal accumulation of inflammatory cells, which limit the development of ARDS [16, 18]. Another strategy is the prevention of degradation of S1P via inhibition of S1P lyase (S1PL). All these results can be particularly relevant as lung injury was associated with an enhanced S1PL expression and decreased S1P levels in lung tissue in some models of lipopolysaccharide (LPS)-induced ARDS. 2-acetyl-4(5)-[1(R),2(S),3(R),4-tetrahydroxybutyl]-imidazole inhibited S1PL in lung tissue and BAL fluid and reduced lung injury and inflammation in animal models [19].
Resolvins
Resolvins are docosahexaenoic acid (DHA)-derived lipid mediators that constitute novel endogenous pathways of local-acting mediators that possess both anti-inflammatory and pro-resolvin properties [19]. A novel resolvin D1 (RvD1) suppressed production of pro-inflammatory mediators by primary human cells, such as small airway epithelial cells and monocytes, in a dose-dependent manner in vitro [20] and attenuated inflammation in LPS-induced ALI in vivo [21]. This attenuated lung inflammation was mediated by the suppression of nuclear factor-kappa B (NF-κB) activation through a mechanism partly dependent on peroxisome proliferator-activated receptor gamma (PPARγ) activation. Also, RvD1 significantly reduced macrophages and neutrophil exocytosis and upregulated the expression of the anti-inflammatory cytokine, IL-10, which accelerated the resolution of lung inflammation [20]. In addition, these endogenous mediators seem to have anti-fibrotic and host-directed antimicrobial actions [19]. Thus, resolvins constitute a novel genus of chemical mediators that could be useful for the design of new therapies for ARDS.
Statins
Statins are a class of 3-hydroxy-3-methylglutaryl-coenzyme A-reductase inhibitors that have pleiotropic properties. Statins not only lower cholesterol, but also have other non-lipid-lowering effects that can be beneficial for the management of sepsis and sepsis-induced ARDS, particularly associated with pneumonia [22]. In this context, statins confer lung protection by preserving endothelial function and integrity, reducing vascular leak, and exerting anti-inflammatory and anti-thrombotic effects. In experimental studies of endotoxin-induced lung injury, simvastatin preserved protein permeability preventing lung edema formation, attenuated neutrophil migration to the lung, and reduced endothelial cell-derived cytokine expression (IL-6, IL-8, monocyte chemotactic protein [MCP]-1, regulated upon activation normal T cell expressed and presumably secreted [RANTES]). These protective effects of statins are mediated through the upregulation of the activity of integrin-β4 in endothelial cells. These findings support statins as useful drugs and integrin-β4 as a novel therapeutic target in patients with ALI [23].
Angiopoietin-1/2 System
The angiopoietin (Ang)-1/2 system has been recognized to play a major role in various features of human sepsis and ALI. Ang-1 and Ang-2 bind to the endothelial and the soluble form of the Tie2 receptor (sTie2). Ang-1 induces activation of the endothelial Tie2 receptor, and reduces pulmonary inflammation and endothelial cell permeability. Ang-2 prevents Ang-1 from binding to the endothelial Tie2 receptor, and consequently leads to pulmonary inflammation and increased endothelial cell permeability [24, 25]. This suggests that the Ang-1/2-Tie2 system should be further investigated as it constitutes a potential target for treating patients with ARDS.
Activated Protein C
APC, an endogenous protein that promotes fibrinolysis and inhibits thrombosis, can modulate the coagulation and inflammation associated with ALI. Restoring normal alveolar levels of APC was expected to prevent the progression of pulmonary coagulopathy and to mitigate the intensity of lung damage. However, a recent clinical trial demonstrated that APC did not improve outcomes in patients with ALI, suggesting that the method of APC administration may be important. It has been speculated that APC inhalation, instead of intravenous administration, might provide the expected benefit to patients with ARDS [26, 27]. Furthermore, combination of APC with other anticoagulant agents (including anti-thrombin and heparin) and pro-fibrinolytic agents (such as plasminogen activators) could be more effective in attenuating pulmonary coagulopathy and inflammation, but this has not been tested yet.
Regulation of the Renin-angiotensin System
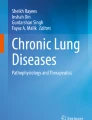
Recent studies indicate that the renin-angiotensin system plays a critical role in acute lung diseases. Angiotensin II, a key effector peptide of the system, causes vasoconstriction and exerts multiple biological functions. Angiotensin-converting enzyme (ACE) and ACE2 are homologs with different key functions in the renin-angiotensin system. ACE cleaves angiotensin I to generate angiotensin II, whereas ACE2 reduces angiotensin II levels and thereby functions as a negative regulator of the angiotensin system (Fig. 2). Capillary blood vessels in the lung are a major site of ACE expression and angiotensin II production in the human body [28]. ACE, angiotensin II and the angiotensin II type 1 receptor (AT1) induce apoptosis in the alveolar wall, alter alveolar capillary barrier integrity leading to lung edema, and promote collagen deposition, which can result in lung fibrosis with the consequent impairment of lung function. In contrast, ACE2 and the angiotensin II type 2 receptor (AT2) protect against all these effects (Fig. 2). Indeed, inhibiting ACE and AT1 as well as increasing ACE2 and AT2 activity attenuated lung injury in several animal models of ARDS, and may represent novel approaches for the treatment of ARDS [29–32].


Schematic of the renin-angiotensin system. ACE: angiotensin-converting enzyme; ACE2: angiotensin-converting enzyme 2; AT1: angiotensin II type 1 receptor; AT2: angiotensin II type 2 receptor
Endotoxin Signaling
Many drugs targeting endotoxin or the endotoxin-induced cytokine storm have been developed with therapeutic purposes in sepsis and sepsis-induced ARDS. Toll-like receptor 4 (TLR4) is activated by LPS or endotoxin, the major component of the outer membrane of Gram-negative bacteria, and constitutes a potent inflammatory stimulus implicated in septic shock and septic-induced ARDS. Activation of TLR4 by LPS depends on LPS binding protein (LBP)-catalyzed extraction and transfer of individual LPS molecules from aggregated LPS to CD14 and then from CD14 to MD2, followed by engagement and dimerization of TLR4. TLR4 signaling may also be activated by stimuli other than LPS. Chemical (acid aspiration) or virus (influenza) insults may cause ALI via the generation of host-derived, oxidized phospholipids that potently stimulate TLR-4 [33]. Eritoran is a potent, well-tolerated, synthetic TLR4 antagonist that protects against influenza-induced ARDS in mice, improving the survival of these animals even when administered as late as 6 days post-infection. Eritoran binds to CD14, which inhibits ligand binding to MD2:TLR4 complexes preventing TLR4 dimerization and activation [34]. In viral infection, eritoran blocks oxidized phospholipid-induced TLR4 signaling, mitigates the subsequent cytokine storm, and also helps to control viral titer. Despite the lack of benefit in severe septic patients (ACCESS trial) [38], eritoran could still be effective in influenza infection and, perhaps, in ALI mediated by non-infectious agents, but its most effective timing and dosing remain unknown. Based on endotoxin challenge studies in animals, the prophylactic or very early administration of eritoran in patients at-risk or with ARDS could be more effective in controlling the ‘sepsis cascade’. Antagonism of TLR4 signaling could therefore become a useful therapy for ARDS [35, 36].
Cell Adhesion Molecules
The cell adhesion molecules, integrins and selectins, are transmembrane cell surface receptors that regulate leukocyte migration and activation, endothelial/epithelial cytokine expression and alveolar-capillary protein permeability in the lung [37]. The αvβ5 and αvβ6 integrins have an important role on pulmonary endothelial and epithelial cells, respectively. Dysfunction of these molecules alters alveolar endothelial- and epithelial-cell functions and barrier integrity, leading to alveolar flooding. In addition, αvβ6 integrin, which is upregulated in injured epithelial cells, plays a robust role in the development of lung fibrosis via activation of the TGF-β (a pro-fibrotic cytokine). Prevention of leukocyte-epithelial adhesion by using antagonists of integrins, such as XVA143 (antagonist of α-L/β-2 integrin) or BIO1211 (antagonist of α-4/β-1 integrin), protects alveolar epithelial cells from injury in inflammatory lung diseases [38].
These results identify integrins and selectins as promising therapeutic targets for ALI, in particular in sepsis-induced ARDS [39]. Inhibition of these integrins by specific antibodies has shown therapeutic effects in models of septic shock [40, 41]. In fact, these families of adhesion molecules have been under intense investigation by the pharmaceutical industry. In this regard, antagonists of integrin αvβ3 (e. g., abciximab), integrin αLβ2 (efalizumab), and integrin α4β1 (natalizumab) are currently US FDA-approved for acute coronary syndromes, psoriasis and multiple sclerosis, respectively. However, none has been approved for indications related to ARDS. Recently, positive results in phase II clinical trials with a small-molecule selectin antagonist (bimosiamose) and a small-molecule integrin α4β1 antagonist (valategrast, R411) for the management of asthma and chronic obstructive pulmonary disease (COPD) have generated great enthusiasm [37]. The efficacy of these molecules against the development of ARDS may therefore warrant further investigation.
MicroRNA
ARDS is a disease affected by various genetic and non-genetic factors. MicroRNAs (miRNAs) have emerged as a novel class of gene regulators which play critical roles in complex diseases including ARDS. From animal models of ALI, including LPS- and ventilator-induced lung injury (VILI), several miRNAs (e. g., miR-146a, miR-155, miR-16) have been identified as important regulators of inflammatory responses in the lung. For example, upregulation of miR-16 significantly downregulates IL-6 and TNF-α expression in LPS-induced lung injury [42]. In addition, some miRNAs (hsa-miR-374a, hsa-miR-374b, hsa-miR-520c-3p, and hsa-miR-1290) have been involved in endothelial cell barrier dysfunction and in the increased vascular permeability and formation of lung edema in injured lungs. These miRNAs seem to control endothelial cell barrier via regulation of non-muscle myosin light chain kinase (nmMLCK) expression in human lung endothelium in vitro. Thereby, modulation of miRNAs could have important beneficial effects on controlling the development and progression of ARDS [43].
Antihistamines
Endogenous histamine is widely distributed in the lungs and is an important mediator of early and late inflammatory responses. Histamine promotes neutrophil migration, increases cytokine expression, and enhances capillary permeability leading to protein leak. In animal models of ALI, inhaled endotoxin causes an increase in histamine concentration in BAL fluid. Administration of mepyramine (H1-receptor antagonist) or ranitidine (H2-receptor antagonist) attenuates the increased histamine concentration, but only the administration of ranitidine was associated with a significant reduction in neutrophil numbers and in protein permeability. This study suggests that endogenous histamine may be involved in the recruitment of neutrophils and protein leaks in endotoxin-induced ALI via the H2 receptors [44]. Also, scavenging of endogenous histamine by the arthropod-derived histamine binding protein, EV131, mitigates endotoxin-induced lung injury, supporting the notion that histamine-mediated signaling could be a potential target in ARDS [45].
Stimulators of Lung Repair
Growth Factors
A series of growth factors, such as keratinocyte-, epithelial-, basic fibroblast-, hepatocyte- and vascular endothelial-growth factor, are emerging as important candidates to repair the damaged pulmonary alveolar capillary membrane. To this end, the synergistic interaction of these growth factors, which directly or indirectly affect pulmonary endothelial and epithelial cells, appears to promote the repair process of lung damage. As an example, the combined effect of trefoil factor family peptides and growth factors, such as epithelial growth factor (EGF), stimulated epithelial proliferation and repair [46].
Erythropoietin
A number of preclinical studies have revealed beneficial effects of exogenous erythropoietin (EPO) administration in various experimental models of ARDS. EPO provides protection by modulating multiple early signaling pathways involved in apoptosis, inflammation and peroxidation. Furthermore, EPO appears to confer vascular protection by promoting angiogenesis. However, only preliminary studies exist and more experimental and clinical data are necessary to clarify the efficacy and cytoprotective mechanisms of EPO [47].
Hyaluronan
Hyaluronan constitutes the major glycosaminoglycan in lung tissue and has diverse functions in normal lung homeostasis and pulmonary disease. Hyaluronan and its degradation products, produced by hyaluronidase enzymes and reactive oxygen species (ROS), are implicated in different aspects of the ALI process. The different activities of hyaluronan and its degradation products are regulated by multiple hyaluronan-binding proteins, including CD44, TLR4, hyaluronan-binding protein 2 (HABP2), and receptor for hyaluronan-mediated motility (RHAMM). Recent research indicates that exogenous administration of high molecular weight hyaluronan can serve as a novel therapeutic intervention for lung diseases, including LPS-induced ALI, sepsis/VILI, and airway hyperactivity [48].
Nanomedicine
Novel long-acting biocompatible and biodegradable phospholipid micelles have been developed to inhibit different targets implicated in ALI. For example, nano-sized micelles have been developed to trigger receptor expressed on myeloid cells 1 (TREM-1), ROS and heat shock protein (Hsp)90, all effectors thought to be involved in ALI. The main limitations of some peptide drugs for clinical use are the short half-life (minutes) and their water-insolubility. To overcome these limitations, some groups have developed micellar-targeted peptides in which the peptide drug remains in its active form for longer (hours) and increases its stability and bioavailability [49]. These long-acting micellar nanomedicines have provided significant advancement in the treatment of ARDS in experimental models, which could be extended to the clinical setting. Another advance is the novel nanovesicle aerosols composed of non-lamellar phospholipids that were developed as pulmonary surfactant aerosols and have been successfully used as therapy in mice with acid-induced lung injury. Currently existing intratracheal surfactants are ineffective because they are inactivated by albumin leakage and other mechanisms. The nanovesicle aerosols of non-lamellar lipids improve the resistance of pulmonary surfactants to inhibition, and may therefore be promising as a non-invasive aerosol therapy in ALI [50].
Conclusions
Despite decades of clinical trials and experimental research, there is no effective pharmacologic therapy for the treatment of all patients with ARDS. Multiple biochemical and biological targets, however, have been identified that could give rise to future drug discovery and development. Several aspects should be taken into account in order to guarantee the efficacy of those potential new drugs. Better stratification may help to identify subgroups of patients with ARDS that benefit from targeted interventions, given the heterogeneity of patients with ARDS and the multiple etiologies of this disease (direct versus indirect ARDS). Combinations of different therapeutic strategies could also improve outcomes for these patients compared with therapies based on single agents. Finally, we also need to optimize the dose, timing and route of administration as well as to determine the potential toxicity of the novel pharmacologic agents for their future use in the management of patients with ARDS.
Acknowledgements
This work was funded by the Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES) and the Instituto de Salud Carlos III (Fondo de Investigación Sanitaria, FIS PI12/0245, PI0902624, PI0902644, PI1102791).
References
Ranieri VM, Rubenfeld GD, Thompson BT et al (2012) Acute respiratory distress syndrome: the Berlin Definition. JAMA 307:2526–2533
Wiedemann HP, Wheeler AP, Bernard GR et al (2006) Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 354:2564–2575
Petrucci N, Iacovelli W (2004) Ventilation with lower tidal volumes versus traditional tidal volumes in adults for acute lung injury and acute respiratory distress syndrome. Cochrane Database Syst Rev CD003844
Frank AJ, Thompson BT (2010) Pharmacological treatments for acute respiratory distress syndrome. Curr Opin Crit Care 16:62–68
Ware LB, Matthay MA (2000) The acute respiratory distress syndrome. N Engl J Med 342:1334–1349
Thille AW, Esteban A, Fernandez-Segoviano P et al (2013) Comparison of the Berlin definition for acute respiratory distress syndrome with autopsy. Am J Respir Crit Care Med 187:761–767
Steinberg KP, Milberg JA, Martin TR, Maunder RJ, Cockrill BA, Hudson LD (1994) Evolution of bronchoalveolar cell populations in the adult respiratory distress syndrome. Am J Respir Crit Care Med 150:113–122
Walmsley SR, Chilvers ER, Thompson AA et al (2011) Prolyl hydroxylase 3 (PHD3) is essential for hypoxic regulation of neutrophilic inflammation in humans and mice. J Clin Invest 121:1053–1063
Fujino N, Kubo H, Suzuki T et al (2012) Administration of a specific inhibitor of neutrophil elastase attenuates pulmonary fibrosis after acute lung injury in mice. Exp Lung Res 38:28–36
Chua F, Dunsmore SE, Clingen PH et al (2007) Mice lacking neutrophil elastase are resistant to bleomycin-induced pulmonary fibrosis. Am J Pathol 170:65–74
Takemasa A, Ishii Y, Fukuda T (2012) A neutrophil elastase inhibitor prevents bleomycin-induced pulmonary fibrosis in mice. Eur Respir J 40:1475–1482
Ryugo M, Sawa Y, Takano H et al (2006) Effect of a polymorphonuclear elastase inhibitor (sivelestat sodium) on acute lung injury after cardiopulmonary bypass: findings of a double-blind randomized study. Surg Today 36:321–326
Stevens T, Ekholm K, Granse M et al (2011) AZD9668: pharmacological characterization of a novel oral inhibitor of neutrophil elastase. J Pharmacol Exp Ther 339:313–320
Jacobson JR (2009) Pharmacologic therapies on the horizon for acute lung injury/acute respiratory distress syndrome. J Investig Med 57:870–873
Uhlig S, Gulbins E (2008) Sphingolipids in the lungs. Am J Respir Crit Care Med 178:1100–1114
Abbasi T, Garcia JG (2013) Sphingolipids in lung endothelial biology and regulation of vascular integrity. Handb Exp Pharmacol 201–226
Wang L, Dudek SM (2009) Regulation of vascular permeability by sphingosine 1-phosphate. Microvasc Res 77:39–45
Natarajan V, Dudek SM, Jacobson JR et al (2013) Sphingosine-1-phosphate, FTY720, and sphingosine-1-phosphate receptors in the pathobiology of acute lung injury. Am J Respir Cell Mol Biol 49:6–17
Serhan CN, Chiang N (2008) Endogenous pro-resolving and anti-inflammatory lipid mediators: a new pharmacologic genus. Br J Pharmacol 153(1):200–215
Hsiao HM, Sapinoro RE, Thatcher TH et al (2013) A novel anti-inflammatory and pro-resolving role for resolvin D1 in acute cigarette smoke-induced lung inflammation. PLoS One 8:e58258
Liao Z, Dong J, Wu W et al (2012) Resolvin D1 attenuates inflammation in lipopolysaccharide-induced acute lung injury through a process involving the PPARgamma/NF-kappaB pathway. Respir Res 13:110
Chalmers JD, Short PM, Mandal P, Akram AR, Hill AT (2010) Statins in community acquired pneumonia: Evidence from experimental and clinical studies. Respir Med 104:1081–1091
Chen W, Sammani S, Mitra S, Ma SF, Garcia JG, Jacobson JR (2012) Critical role for integrin-beta4 in the attenuation of murine acute lung injury by simvastatin. Am J Physiol Lung Cell Mol Physiol 303:L279–L285
van der Heijden M, van Nieuw Amerongen GP, Koolwijk P, van Hinsbergh VW, Groeneveld AB (2008) Angiopoietin-2, permeability oedema, occurrence and severity of ALI/ARDS in septic and non-septic critically ill patients. Thorax 63:903–909
van der Heijden M, van Nieuw Amerongen GP, van Hinsbergh VW, Groeneveld AB (2010) The interaction of soluble Tie2 with angiopoietins and pulmonary vascular permeability in septic and nonseptic critically ill patients. Shock 33:263–268
Glas GJ, Van Der Sluijs KF, Schultz MJ, Hofstra JJ, Van Der Poll T, Levi M (2013) Bronchoalveolar hemostasis in lung injury and acute respiratory distress syndrome. J Thromb Haemost 11:17–25
Bo L, Bian J, Li J, Wan X, Zhu K, Deng X (2011) Activated protein C inhalation: a novel therapeutic strategy for acute lung injury. Med Sci Monit 17:HY11–HY13
Imai Y, Kuba K, Penninger JM (2007) Angiotensin-converting enzyme 2 in acute respiratory distress syndrome. Cell Mol Life Sci 64:2006–2012
Imai Y, Kuba K, Rao S et al (2005) Angiotensin-converting enzyme 2 protects from severe acute lung failure. Nature 436:112–116
Wang R, Ibarra-Sunga O, Verlinski L, Pick R, Uhal BD (2000) Abrogation of bleomycin-induced epithelial apoptosis and lung fibrosis by captopril or by a caspase inhibitor. Am J Physiol Lung Cell Mol Physiol 279:L143–L151
Bechara RI, Pelaez A, Palacio A et al (2005) Angiotensin II mediates glutathione depletion, transforming growth factor-beta1 expression, and epithelial barrier dysfunction in the alcoholic rat lung. Am J Physiol Lung Cell Mol Physiol 289:L363–L370
Marshall RP, Gohlke P, Chambers RC et al (2004) Angiotensin II and the fibroproliferative response to acute lung injury. Am J Physiol Lung Cell Mol Physiol 286:L156–L164
Imai Y, Kuba K, Neely GG et al (2008) Identification of oxidative stress and Toll-like receptor 4 signaling as a key pathway of acute lung injury. Cell 133:235–249
Kim HM, Park BS, Kim JI et al (2007) Crystal structure of the TLR4-MD-2 complex with bound endotoxin antagonist Eritoran. Cell 130:906–917
Wong YN, Rossignol D, Rose JR, Kao R, Carter A, Lynn M (2003) Safety, pharmacokinetics, and pharmacodynamics of E5564, a lipid A antagonist, during an ascending single-dose clinical study. J Clin Pharmacol 43:735–742
Mullarkey M, Rose JR, Bristol J et al (2003) Inhibition of endotoxin response by e5564, a novel Toll-like receptor 4-directed endotoxin antagonist. J Pharmacol Exp Ther 304:1093–1102
Woodside DG, Vanderslice P (2008) Cell adhesion antagonists: therapeutic potential in asthma and chronic obstructive pulmonary disease. BioDrugs 22:85–100
Sheppard D (2012) Modulation of acute lung injury by integrins. Proc Am Thorac Soc 9:126–129
Su G, Hodnett M, Wu N et al (2007) Integrin alphavbeta5 regulates lung vascular permeability and pulmonary endothelial barrier function. Am J Respir Cell Mol Biol 36:377–386
Puthawala K, Hadjiangelis N, Jacoby SC et al (2008) Inhibition of integrin alpha(v)beta6, an activator of latent transforming growth factor-beta, prevents radiation-induced lung fibrosis. Am J Respir Crit Care Med 177:82–90
Kyriakides C, Austen W Jr, Wang Y, Favuzza J, Moore FD Jr, Hechtman HB (2000) Endothelial selectin blockade attenuates lung permeability of experimental acid aspiration. Surgery 128:327–331
Cai ZG, Zhang SM, Zhang Y, Zhou YY, Wu HB, Xu XP (2012) MicroRNAs are dynamically regulated and play an important role in LPS-induced lung injury. Can J Physiol Pharmacol 90:37–43
Adyshev DM, Moldobaeva N, Mapes B, Elangovan V, Garcia JG (2013) MicroRNA regulation of nonmuscle myosin light chain kinase expression in human lung endothelium. Am J Respir Cell Mol Biol 49:58–66
Kim TH, Yoon HJ, Lim CM, Kim EK, Kim MJ, Koh Y (2005) The role of endogenous histamine on the pathogenesis of the lipopolysaccharide (LPS)-induced, acute lung injury: a pilot study. Inflammation 29:72–80
Ryffel B, Couillin I, Maillet I et al (2005) Histamine scavenging attenuates endotoxin-induced acute lung injury. Ann NY Acad Sci 1056:197–205
Lindsay CD (2011) Novel therapeutic strategies for acute lung injury induced by lung damaging agents: the potential role of growth factors as treatment options. Hum Exp Toxicol 30:701–724
Kakavas S, Demestiha T, Vasileiou P, Xanthos T (2011) Erythropoetin as a novel agent with pleiotropic effects against acute lung injury. Eur J Clin Pharmacol 67:1–9
Lennon FE, Singleton PA (2011) Role of hyaluronan and hyaluronan-binding proteins in lung pathobiology. Am J Physiol Lung Cell Mol Physiol 301:L137–L147
Sadikot RT, Rubinstein I (2009) Long-acting, multi-targeted nanomedicine: addressing unmet medical need in acute lung injury. J Biomed Nanotechnol 5:614–619
Kaviratna AS, Banerjee R (2012) Nanovesicle aerosols as surfactant therapy in lung injury. Nanomedicine 8:665–672
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Herrero, R., Rojas, Y., Esteban, A. (2014). Novel Pharmacologic Approaches for the Treatment of ARDS. In: Vincent, JL. (eds) Annual Update in Intensive Care and Emergency Medicine 2014. Annual Update in Intensive Care and Emergency Medicine, vol 2014. Springer, Cham. https://doi.org/10.1007/978-3-319-03746-2_18
Download citation
DOI: https://doi.org/10.1007/978-3-319-03746-2_18
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-03745-5
Online ISBN: 978-3-319-03746-2
eBook Packages: MedicineMedicine (R0)