
Abstract
Cigarette smoking remains the leading preventable cause of death and disease in the developed world. In this chapter, we review a behavior analytic approach to conceptualizing, assessing, and treating cigarette smoking. A behavior analytic perspective views cigarette smoking as operant behavior, or behavior that is selected and maintained by consequences. Most of the biological and environmental variables associated with the acquisition, maintenance, and successful treatment of cigarette smoking can be captured by the four-term operant unit. The four-term operant unit consists of motivating operations, discriminative stimuli, the target behavior of cigarette smoking, and consequent stimuli. Assessment of smoking includes consideration of reliable and valid methods to assess cigarette smoking, the functional assessment of the variables associated with the four-term unit, and characteristics such as degree of nicotine dependence and self-reported motivation that may be used to guide treatment decisions. A plethora of treatment options exist, and we discuss briefly pharmacotherapy, behavior therapy, and technology-based platforms to deliver behavior therapy. We focus on contingency management, including recent advances in technology-based contingency management interventions. We hope the chapter provides further evidence for the continued vitality and social relevance of a behavior analytic approach to cigarette smoking.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Smoking Cessation
Cigarette smoking continues to take an enormous toll on society. Since the first Surgeon General’s report on the health consequences of smoking in 1964, more than 20 million Americans have died prematurely from tobacco-related diseases (U.S. Department of Health and Human Services, 2014). An estimated 34.2 million people still smoke combustible cigarettes in the United States, and smoking remains the leading cause of premature death and preventable disease (Creamer et al., 2019). At least 70 chemicals in cigarette smoke are known carcinogens including arsenic, benzene, formaldehyde, lead, nitrosamines, and polonium 210 (Prochaska & Benowitz, 2019). Most adult smokers, 88%, smoked their first cigarette before the age of 18 (U.S. Department of Health and Human Services, 2012). Quitting cigarette smoking produces health benefits regardless of age (U.S. Department of Health and Human Services, 2014), and novel regulatory and treatment options continue to emerge to promote cessation (Bricker et al., 2018; Donny et al., 2014).
In this chapter, we review a behavior analytic approach to conceptualizing, assessing, and treating cigarette smoking. A behavior analytic perspective views cigarette smoking as operant behavior, or behavior that is selected and maintained by consequences (Thompson & Johanson, 1981; Silverman, 2004). Viewing cigarette smoking as operant behavior is tremendously useful in assessment and treatment (Henningfield & Higgins, 1989). The acquisition and maintenance of smoking can include social and non-social primary reinforcers, conditioned reinforcers, observational learning, the influence of advertising, social media, rules, and negative reinforcement. A behavior analytic account also entails contextual factors such as the availability of alternative sources of reinforcement and environmental stressors. It is also compatible with other biological and psychosocial theories to account for cigarette smoking. For example, genetic or acquired characteristics (e.g., family history of cigarette smoking or substance dependence, other psychiatric disorders) can affect the probability of cigarette smoking (Hatsukami et al., 2008). These characteristics may produce individual differences in sensitivity to reinforcement (to drug and/or social reinforcers), punishment, and delay to reinforcement that may contribute to cigarette smoking (Thompson, 2007). The operant view also incorporates private events such as craving and anxiety, as well as verbally mediated processes as part of a comprehensive account of the determinants and outcomes of smoking (DeGrandpre, 2000; Wilson & Hayes, 2000). Finally, a behavior analytic perspective also provides a useful framework to account for the effects of conventional treatments for smoking such as nicotine replacement, behavioral treatments focused on providing incentives contingent on abstinence, and novel regulatory and intervention efforts to prevent smoking and promote long-term cessation (Cassidy & Kurti, 2018).
Conceptual Framework: The Four-Term Operant Unit
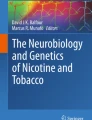
Most of the biological and environmental variables associated with the acquisition, maintenance, and successful treatment of cigarette smoking can be captured by the four-term operant unit (Dallery et al., 2013; Thompson, 2007). The four-term operant unit consists of motivating operations, discriminative stimuli, the target behavior of cigarette smoking, and consequent stimuli. Figure 41.1 presents a schematic of these units and some of their interactions. We have included examples of each term in the operant unit, but these nominal examples are not meant to apply universally across individuals. Also, the static nature of the figure belies the dynamic nature of how these units emerge over time, and how the influence of different variables may vary over time and across individuals.

The four-term functional unit of analysis
Upon inhalation, nicotine rapidly enters the lungs, undergoes dissolution in pulmonary fluid, and is transported to the heart and then to the brain (Hatsukami et al., 2008). It takes about 10 s for nicotine to enter the brain (Rupprecht et al., 2015). Daily smokers may smoke consistently throughout the day to maintain nicotine levels in a particular range (Benowitz, 1991). Cigarette smoke contains over 7000 chemicals, some of which may enhance the psychoactive effects of nicotine and some of which have independent psychoactive properties (Rupprecht et al., 2015). Evidence suggests that nicotine can serve as a positive reinforcer in non-humans and humans (Henningfield & Goldberg, 1983; Perkins et al., 2001). Laboratory research with non-human animals, however, suggests that nicotine serves as a weak primary reinforcer (Caggiula et al., 2009), and self-administration is increased by the presence of sensory stimuli such as illuminated cue lights during nicotine delivery (Palmatier et al., 2007). In humans, reinforcing consequences associated with smoking may include the physiological effects of nicotine, such as the arousal, increased energy, or appetite-suppressing effects of tobacco use (Hatsukami et al., 2008). Smoking can be acquired and maintained through other sources of positive reinforcement, such as social interaction (Friedman et al., 1985). Although nicotine may serve as a weak primary reinforcer, it may still confer conditioned reinforcing properties to stimuli associated with smoking such as the taste, smell, airway stimulation, and other sensory stimuli (Rose, 2006; Russel et al., 1974).
Negative reinforcement can also contribute to the origin and maintenance of smoking behavior (Eissenberg, 2004). Nicotine withdrawal is characterized by negative affect such as irritability, anger, cravings, and depression, and physiological symptoms such as constipation, coughing, dizziness, and even mouth sores (American Medical Association, 1994; Hughes et al., 1990). These symptoms peak in the first week of abstinence, but several studies have reported their persistence several months into abstinence (Gilbert et al., 2002; Piasecki et al., 2002). Although alleviation of negative affect is often endorsed by smokers, human laboratory research suggests that smoking relieves negative affect under limited conditions (Lerman & Audrain-McGovern, 2010; Perkins et al., 2010). For example, in the human laboratory, Perkins et al. found that smoking only reduced negative affect induced by abstinence, but not after other procedures to induce negative affect and anxiety (e.g., preparing for a speech, viewing negative mood slides). Interestingly, such effects were independent of nicotine: smoking denicotinized cigarettes had similar negative affect-reducing effects. Following smoking cessation in clinical contexts, negative affect has been found to characterize over 50% of all smoking lapses (Shiffman et al., 1996; Robinson et al., 2017). The role of negative affect on smoking is complicated, and may depend on factors such as nicotine content, stages of smoking (e.g., maintenance versus relapse), and other factors (see Kassel et al., 2003, for a review). Negative reinforcement associated with smoking can also occur when a smoker takes a break from work to smoke (Dunbar et al., 2018).
Establishing operations momentarily increase the value of a reinforcer and increase the likelihood of the response that produces that reinforcer (Laraway et al., 2003). In addition to serving as a reinforcer, nicotine may also function as an establishing operation. In laboratory animals, systemic injections or infusions of nicotine increase responding maintained by conditioned reinforcers such as an illuminated cue light (Charntikov et al., 2020; Donny et al., 2003; Chaudhri et al., 2006; Raiff & Dallery 2006; Palmatier et al., 2007; Liu et al., 2007). These findings, along with the findings that nicotine serves as a primary reinforcer, led to the dual reinforcement model of nicotine self-administration, which posits that nicotine has reinforcing and enhancement (establishing operation) effects on behavior (Caggiula et al., 2009). In humans, administration of nicotine has been shown to increase responding (e.g., under a progressive ratio schedule) maintained by access to music and video, and their self-reported pleasantness (Perkins & Karelitz, 2014; Perkins et al., 2017). Using electronic daily diaries, Piasecki et al. (2011) found that tobacco use increases the pleasure and subjective effects (e.g., “buzzed”) of alcohol use, and vice versa. In addition, a review by Martin and Sayette (2018) found that nicotine enhanced social behavior, meaning that it increased positive features of social functioning and decreased negative features. For example, participants exposed to nicotine were faster at identifying facial expressions than after abstinence and were less likely to engage in aggressive behavior after being provoked. Nicotine enhancement may be selective to certain types of reinforcing consequences such as sensory and social stimuli. Nicotine does not appear to enhance responding maintained by food reinforcers in animals (Raiff & Dallery, 2008) and monetary reinforcers in humans (Perkins et al., 2017). More work is needed to identify the generality of the establishing operation functions of nicotine across different types of reinforcers, and the extent of individual differences in these effects.
Antecedent events and stimuli are also associated with cigarette smoking (Niaura et al., 1988; Shiffman et al., 2004, 2014). For example, smoking may occur in the presence of specific people (peer smokers), places (outside, in car), and things (smoking paraphernalia). These stimuli may function as discriminative stimuli within the four-term unit, and they may also have additional Pavlovian effects (Thompson, 2007). The presence of certain peers may be associated with smoking-related reinforcement, and thus increase the probability of smoking. The presence of the same peers may also elicit physiological conditioned responses, and the same is true for other stimuli associated with smoking such as cigarettes, smoke, smoking paraphernalia, coffee, and so on (Conklin et al., 2013; Winkler et al., 2011). These physiological conditioned responses may set the occasion for the verbal responses characterized by “craving” (a full account of the origins and the multiple functions of verbal craving responses is beyond the scope of this paper). Nicotine itself can serve as a discriminative stimulus and increase responding maintained by ethanol in the animal laboratory (Ginsburg et al., 2018). Other environmental events may function as discriminative stimuli and alter the probability of smoking. For example, rules concerning the health consequences presented by parents, teachers, or the US Surgeon General may decrease smoking (Cerutti, 1989). Advertising may have discriminative stimulus effects (and establishing operation effects), as ads may signal the availability of social reinforcement for smoking. The role of advertising is particularly pernicious in light of the 26 million dollars per day spent on advertising cigarettes by tobacco companies in the United States (Centers for Disease Control, 2020).
Aversive consequences following smoking may also occur. Unless these consequences reduce the likelihood of smoking behavior, they cannot be termed “punishers.” Some aversive physiological stimuli may occur immediately following smoking, such as throat irritation, mouth dryness, shortness of breath, and cough (Şanli et al., 2016). Other consequences such as the increased likelihood of cancers and cardiovascular disease may be delayed and probabilistic (U.S. Department of Health and Human Services, 2010). Delaying the presentation of aversive stimuli reduces their punishing effects, as does reducing the certainty that they will occur (Green et al., 2014). Even when increased disease risk is communicated based on genomic information tailored for the individual, it does not appear to increase cessation (Ramsey et al., 2018).
The four-term unit comprising the operant determinants of smoking is also situated in the context of other biological vulnerabilities, previous operant learning, and current circumstances. Some of these will require consideration in assessment and treatment. Gene variation may increase the risk of dependence and treatment failure. Recent research suggests that individuals with genetically slow nicotine metabolism have higher cessation success with behavioral counseling and nicotine patch treatment (Chenoweth & Tyndale, 2017). In addition, the presence of comorbidities like depression, anxiety, post-traumatic stress, and schizophrenia requires effective management to increase the probability of cessation (Prochaska & Benowitz, 2019). The same is true with respect to the presence of other smokers and non-smokers in the individual’s environment, such as parents, partners, and friends (vanDellen et al., 2016). Additionally, individuals from lower socioeconomic classes and with lower educational attainment have been shown to smoke at higher rates and be less successful when they attempt to quit smoking (Garrett et al., 2019; Jarvis, 2004).
The availability of alternative sources of reinforcement may also influence smoking. Dallery and Raiff (2007) found that choice to smoke in the human laboratory decreased with the magnitude of the monetary alternative (see also Johnson & Bickel, 2003; Stoops et al., 2011), and Cassidy et al. (2015) found a similar pattern of decreasing smoking choices with increasing magnitude of an alternative monetary reinforcer in adolescents. In a non-lab, naturalistic setting, Audrain-McGovern et al. (2004) showed that school involvement, physical activity, academic performance, and sports team participation were associated with decreased risk of smoking. In a human laboratory choice arrangement, concurrent access to money and food decreased choice for cigarette puffs under some conditions (Epstein et al., 1991). In addition, Schnoll et al. (2016) found that the extent of alternative reinforcers predicted long-term abstinence following treatment. These findings suggest that enriched environments with a variety of opportunities to obtain alternative reinforcers may decrease smoking (Acuff et al., 2019; Correia et al., 2002; Vuchinich & Tucker, 1988).
Lastly, other behavioral tendencies or processes have also shown to be correlated with smoking status, such as the degree of delay discounting and distress tolerance (MacKillop & Munafò, 2017; Veilleux, 2019). For example, individual differences in delay discounting, or the rate at which a future outcome loses value with increasing delays, have been reliably associated with smoking status and severity (Bickel et al., 1999; DeHart et al., 2020). Research suggests that rapid discounting increases the later propensity to smoke compared to those who discount at lower rates (Audrain-McGovern et al., 2009; Dallery & Raiff, 2007), and nicotine and other drugs of abuse may increase impulsive and risky choice (Dallery & Locey, 2005; Locey & Dallery, 2011; Perry & Carroll, 2008).
Assessment
Assessment of smoking includes consideration of reliable and valid methods to assess cigarette smoking, the functional assessment of the variables associated with the four-term unit, and characteristics such as degree of nicotine dependence and self-reported motivation that may be used to guide treatment decisions.
Cigarette Smoking
Self-report of smoking, as operant verbal behavior, is influenced by a variety of social contingencies. The self-report may vary depending on the contingencies associated with the age of the smoker (adolescent versus adult), the reasons for quitting (pressure from spouse or personal health reasons), and whether quitting may result in a positive consequence such as a monetary incentive. As such, no unitary statement about the validity of self-report is possible. Clinicians must assess and possibly attenuate the influence of social and non-social contingencies operating on the form of the self-report (Critchfield et al., 1998). One method to increase the accuracy of self-report is to count smoking episodes within a time period (Frederiksen et al., 1979; McFall & Hammen, 1971). These self-monitoring methods can vary in precision from simply counting the number of cigarettes smoked in one day to recording the number, time, and behaviors or environments relevant to each smoking episode. These methods involve discrimination of the smoking episode and recording of that episode. As such, measurement error can occur in both of these steps. Another method involves counting the permanent product of a smoking episode, that is, the smoked cigarette (Schwartz, 1992). Similarly, Timeline Follow-Back (TLFB) procedures may be used to increase accuracy. These methods are also well-suited to collect information about smoking over longer periods (e.g., 30 days) and with non-daily smokers (Harris et al., 2009). Briefly, the TLFB procedure uses key events (such as birthdays) to prompt respondents to provide daily retrospective estimates over a specified time period (Lewis-Esquerre et al., 2005). The TLFB procedure may have limits in terms of accuracy, particularly for heavy smokers (Griffith et al., 2009; Shiffman, 2009).
More objective methods include biochemical assessments of the metabolites of nicotine in saliva or urine, or exhaled breath carbon monoxide (CO; Benowitz et al., 2020). Benowitz et al. reported that up to one in ten who self-report abstinence do not meet biochemical abstinence criteria in research settings. Not only are biochemical methods often more accurate than self-report, but also they may be useful in populations in which smoking may occur surreptitiously such as with adolescents. Cotinine is the primary result of the metabolization of nicotine in the body and is most easily measured via saliva or urine. One consideration for the use of cotinine as an objective measure for smoking is that cotinine may also be present in the body if the individual is using other nicotine-containing products, such as electronic cigarettes (ECs) or nicotine replacement. Commercially available products such as NicAlert® for salivary testing may be useful in clinical settings. NicAlert® is advantageous in that it is inexpensive, and results are available within minutes of collecting the (urine or saliva) sample. In addition, cotinine’s long half-life (10–30 h) permits detection for several days after cessation (Benowitz et al., 2020).
An alternative objective method is the measurement of breath carbon monoxide (CO). Commercially available devices (e.g., Pico Smokerlyzer®; Bedfont Scientific Ltd) measure the rate of conversion of CO to carbon dioxide when the smoker exhales air over a catalytically active electrode. Breath CO measurement is highly correlated with blood nicotine levels (Jaffe et al., 1981). Optimal cutpoints for abstinence range between 4 and 6 ppm and will depend on the manufacturer of the CO meter (Perkins et al., 2013). Another consideration is the short half-life of CO, which is about 4 h, which may necessitate twice-daily measurements to provide an index of daily abstinence. Breath CO may reach a “non-smoking” cutpoint in a regular smoker in 6–24 h, and can depend on other factors such as activity level, sleep, and ambient sources of CO (Benowitz et al., 2020). Recently available CO monitors, such as the Smokerlyzer®, can be connected directly to a smoker’s smartphone. For detailed consideration of biochemical confirmation procedures and cutpoints for CO and cotinine, the reader is directed to Benowitz et al. (2020).
Functional Assessment
In contrast to the ubiquity of functional assessment methods in other areas of Applied Behavior Analysis (Hanley, 2012), there are relatively few examples of functional assessment methods in the area of cigarette smoking (Cole & Bonem, 2000; Epstein & Collins, 1977; Pomerleau et al., 2003). Many treatment guidelines recommend assessment of “triggers” for smoking, but they do not assess the full range of functions as exemplified in modern assessment methods. Axelrod (1991) reported on one of the first approximations to a functional assessment that included both antecedents and consequences. It was not developed by behavior analysts but rather by physicians and published in a medically oriented encyclopedia. The questionnaire asked smokers their reasons for smoking (e.g., to relax, deal with anger, to get a lift), and then various activities were recommended based on the responses (e.g., deep breathing, going for a walk).
Burrows et al. (2020) developed the Functional Assessment for Smoking Treatment Recommendations (FASTR). The FASTR is a 30-item questionnaire designed to identify 5 potential functions of smoking derived from the four-term unit: automatic positive reinforcement, automatic negative reinforcement, social positive reinforcement, social negative reinforcement, and antecedent stimuli. The questionnaire is divided into five subscales, one for each function, and each item was rated on a 5-point Likert scale, from strongly disagree to strongly agree. Although Burrows et al. found that the measure has good psychometric properties, it has not been evaluated as a method to improve cessation treatment.
Ecological Momentary Assessment (EMA) is a common self-report method to assess smoking behavior along with its antecedents, and less commonly its consequences (Shiffman et al., 2008). EMAs involve the delivery of short questionnaires throughout the day, directly to an individual’s smart phone or other mobile device. These questionnaires typically include measures of the individuals’ covert behaviors and states, overt behaviors, and environmental conditions (e.g., location, social context). As such, EMAs provide a way to sample behavior over long periods of time in a way that reduces recall bias and maximizes ecological validity (Shiffman et al., 2008). They are particularly useful in identifying social and situational factors that contribute to smoking, and thus may offer a functional approach to the assessment of smoking. Lag analyses between antecedents and smoking behavior found that the presence of cigarettes significantly predicted smoking both before and after a quit date, while the presence of other smokers predicted a smoking lapse, with the likelihood increasing with days after the quit date, though non-significantly (Koslovsky et al., 2018). Using a similar analysis with recently abstinent smokers, alcohol use (within 15 min) predicted smoking lapses for low-nicotine-dependent smokers up to 25 days after quitting (Dermody & Shiffman, 2020). Although EMA represents an improvement over global retrospective self-reports, there is a dearth of work comparing EMA to direct observation (Dallery et al., 2013; Shiffman et al., 2008).
Assessing Nicotine Dependence and Motivation
Assessing nicotine dependence may suggest different kinds or levels of treatment. The most common method to assess dependence is the Fagerström Test for Nicotine Dependence (FTND) (Heatherton et al., 1991). The FTND is comprised of six yes/no items, and higher scores reflect a greater degree of dependence. Physical dependence is the result of chronic smoking, with the individual showing signs of withdrawal that are ameliorated by smoking. Two questions seem to be particularly important indicators of dependence: cigarettes per day and time to first cigarette of the day (West, 2004). The FTND has been shown to predict treatment outcomes. Results may also indicate different intensities or doses of behavior therapy or pharmacotherapy, respectively (Fiore et al., 2008; West, 2004).
Finally, assessing self-reported motivation may be used to select treatment approaches. West (2004) recommends simple direct questioning about a smoker’s interest and intent to quit in clinical contexts. More structured, brief questionnaires are also available (Hall et al., 1990). For behavior analytic clinicians, assessing motivation may be a precursor to assessing the contingencies that lead to the different responses. For example, high motivation to quit smoking may be a result of threat of divorce and health problems. These factors could also be addressed or harnessed in treatment. In addition, if a smoker reports low motivation to quit smoking, strategies such as motivational interviewing may be warranted before (or in addition to) recommending other treatments. However, evidence is inconclusive about the effects of motivational interviewing on smoking (Lindson et al., 2019b). Furthermore, as West (2004) notes, the degree of nicotine dependence is a much better predictor of treatment outcome than motivation once treatment has commenced.
Treatment
Although over 70% of smokers express some desire to stop smoking and 45% actually make a quit attempt per year, only about 5% are successful (Hatsukami et al., 2008). The United States Public Health Service endorses a variety of pharmacological and counseling therapies for smoking cessation (Fiore et al., 2008). Most patients, however, relapse within six months, even when various treatments are used together (Cahill et al., 2014, 2016; Hartmann-Boyce et al., 2014; Hughes et al., 2014; Stead et al., 2015, 2016). Although smoking cessation rates are higher following these treatments compared to placebo, the high relapse rate, in absolute numbers, presents a formidable challenge for smoking reduction efforts. A review of smoking cessation interventions designed to prevent relapse found that no psychosocial interventions were effective in preventing relapse (Hajek et al., 2013). Treatment of cigarette smoking should not be viewed as a behavior problem treated acutely, but rather as a chronic, relapsing condition that is likely to require long-term behavior management. Most smokers try to quit several times, and thus repeated intervention may be necessary to support this dynamic process (Hughes, 2003; Niaura, 2008).
Accessible, effective smoking cessation programs are needed. Stitzer (1999) argued that increasing the acceptability and accessibility of behavior therapy in particular is critical: “Greater use of behavior therapy is especially important in view of the research findings that support its dose-related ability to improve cessation” (p. 186). The goal of treatment is cessation. Smoking reductions may increase the probability of later cessation, but there is no evidence that smoking reduction leads to decreases in health risks (Hughes & Carpenter, 2006). In addition, smokers who reduce their smoking engage in compensatory smoking (e.g., deeper inhalation per cigarette). A reduction in cigarette consumption of 50% or more results only in a 30% decrease in biomarkers for toxicant exposure (Hatsukami et al., 2008). In this section, we discuss briefly pharmacotherapy, behavior therapy, and technology-based platforms to deliver behavior therapy. The focus will be on contingency management (CM).
Pharmacological Therapy
The most common pharmacological therapy is nicotine replacement therapy (NRT). NRT can be administered transdermally with a patch, orally (gum, lozenge or sublingual tablets, inhaler), or nasally (Hatsukami et al., 2008). As the name implies, NRT replaces nicotine in tobacco to maintain some of its effects while also reducing its abuse liability (i.e., by reducing the amount and speed of nicotine delivery). Evidence suggests that all forms of NRT are equally effective, and approximately doubles the probability of cessation relative to placebo control conditions (Lindson et al., 2019a, b). In addition, a recent systematic review indicates that combination NRT versus single-form NRT, and 4 mg versus 2 mg nicotine gum, can increase the chances of cessation (Lindson et al., 2019a, b). A common combination is a fast-acting NRT such as gum with a nicotine patch. There is also some evidence for more success with higher-dose nicotine patches, such as 21 mg patches relative to 14 mg patches. The review also suggested that there is some evidence that using NRT prior to quitting may improve quit rates when compared to starting on the quit date.
Other common pharmacological treatments include bupropion and varenicline. Both are non-nicotine-based drugs. Bupropion is also used as an anti-depressant, but its effects appear to be similar in depressed and non-depressed smokers (Hughes et al., 2014). Varenicline targets a specific nicotinic receptor subtype (technically, varenicline is a potent α4 β2 partial agonist). Overall, bupropion produces similar rates of cessation compared to NRT (Cahill et al., 2016), while varenicline increases cessation relative to NRT and bupropion. Cahill et al. concluded that compared to those not treated with varenicline, the use varenicline produces one extra successful quitter for every 11 people treated. Some side-effects associated with varenicline may be of concern (e.g., nausea). More significant side-effects associated with all forms of pharmacotherapy (e.g., cardiovascular events) have not been supported in large, systematic studies (Benowitz et al., 2018)
Pharmacological interventions influence the effects of positive and negative reinforcement associated with smoking. For example, NRT leads to a decrease in withdrawal symptoms. Research also suggests that medicinal nicotine, particularly transdermal patches, results in reduced reinforcement from cigarette smoking, at least as measured by ad libitum cigarette smoking and self-reports of satisfaction derived from smoking (Hatsukami et al., 2008). As such, NRT may function as an abolishing operation to the extent it attenuates the reinforcing value of smoking cigarettes (Laraway et al., 2003). Interestingly, recent research also suggests that adhering to NRT may prevent the loss of the establishing operation effects of nicotine on sensory stimuli (Perkins et al., 2019). Varenicline also has effects that can be understood within the four-term unit. It provides relief from tobacco withdrawal (via its agonist action) and it also attenuates the reinforcing effects of nicotine (via its antagonist action; Hatsukami et al., 2008).
Electronic cigarettes (ECs) have also emerged as a potential pharmacological treatment for cigarette smoking (Glasser et al., 2017; Martner & Dallery, 2019). ECs are battery-operated devices that contain a liquid consisting mainly of water, propylene glycol, vegetable glycerin, nicotine, and flavorings. ECs can deliver nicotine at doses and rates that are similar to what is observed with combustible cigarettes. In addition, they both involve similar patterns of inhaling, exhaling, and hand-to-mouth gestures (Farsalinos, et al., 2013), and as such may substitute for the conditioned reinforcing stimuli associated with smoking. Several studies suggest that ECs may function as a substitute for cigarettes in laboratory settings (Grace et al., 2015; Johnson et al., 2017; Pope et al., 2019; Quisenberry et al., 2016, 2017; Snider et al., 2017; Stein et al., 2018), and a small number of randomized controlled studies suggest that vaping may promote smoking cessation (Adriaens et al., 2014; Bullen et al., 2013; Caponnetto et al., 2013). Although the use of cigarettes among youth has declined over the past decade, the use of electronic cigarettes in this population is increasing (Singh et al., 2016). EC use in youth may increase the chances of initiation of cigarette smoking and affect brain development (U.S. Department of Health and Human Services, 2016).
Behavior Therapy
A plethora of counseling and talk-therapies exist to treat cigarette smoking. These range from brief counseling such as the 5 As (Ask, Advise, Assess, Assist, Arrange) that can be used by clinicians mostly in a primary care setting (Fiore et al., 2008), to individual and group cognitive-behavioral therapy (Niaura, 2008). Cognitive-behavioral approaches include components such as learning to cope with craving and withdrawal induced by nicotine deprivation, learning and avoiding antecedent “triggers” for smoking, stress management, social support, and motivational enhancement (e.g., listing reasons for quitting) techniques. There is good evidence of a dose–response increase in efficacy, at least as measured by total minutes in contact (Fiore et al., 2008; Niaura, 2008). Overall, according to systematic reviews and expert panels, there is moderate evidence for efficacy of these treatment approaches.
Technology-based platforms also deliver cognitive-behavioral approaches along with social support and other components (Taylor et al., 2017). For example, BecomeAnEx.org focuses on teaching strategies to identify and cope with smoking cues, along with providing social support and pharmacotherapy resources. The website contains an online forum for smokers to communicate with one another, videos, interactive content, and a personalized quit plan. The social network component has been found to increase cessation, but only for those who actively participate in the forum. In a large sample (n = 2657), Graham et al. (2017) found abstinence rates of 7.7% in non-users of the forum, 10.7% in passive users, and 20.7% in active users. A theme in research on technology-based platforms is that although they provide access to evidence-based treatment components, users generally do not engage with relevant content and adherence is poor (Eysenbach, 2005). Recent research has explored how specific intervention components may increase engagement. For example, Graham et al. found that increasing engagement in the social network component of BecomeAnEx and provision of free NRT increased adherence across all three recommended components of an evidence-based smoking cessation program (skills training, social support, and pharmacotherapy use).
Bricker and colleagues developed a web-based Acceptance and Commitment Therapy (ACT) called WebQuit (Bricker et al., 2014, 2018). ACT for smoking focuses on acknowledging and accepting emotions, thoughts, and other antecedents for smoking without allowing them to control subsequent behavior. ACT uses six core processes to develop such “psychological flexibility”: acceptance, cognitive diffusion, being present, self as context, values, and committed action. Without going into detail, these processes focus on two main activities: mindfulness and acceptance of thoughts and feelings, and identifying values and behavior change procedures to commit to these values (e.g., smoking cessation). Core processes of ACT were embedded in the website by using personalized quit plans along with videos of former smokers sharing success stories and modeling acceptance. A pilot randomized controlled trial indicated that WebQuit outperformed the Department of Health and Human Services’ website, Smokefree.gov. Cessation rates were higher for the web-based ACT intervention than the Smokefree (23% versus 10%) at a 3-month follow-up (Bricker et al., 2014). However, in a larger randomized controlled trial involving 2637 smokers (Bricker et al., 2018), there were no differences in abstinence at a 12-month follow-up: 24% (278 of 1141) for WebQuit.org and 26% (305 of 1168) for Smokefree.gov. The authors point out the increase in the Smokefree.gov group relative to the previous trial, and they suggest that several new elements of the site may have bolstered efficacy (e.g., new content and front-page placement of coping with depression, an interactive feature to select pharmacotherapy). In addition, in both trials, participants in the ACT group reported increased acceptance of internal experiences (e.g., cravings), and this acceptance was also related to the impact of ACT on smoking. Despite the lack of group differences in the second study, both platforms resulted in positive outcomes. The public health impact of both sites can be estimated based on the product of reach and efficacy. As such, for every 1 million smokers reached, approximately 250,000 would stop smoking (Bricker et al., 2018).
Contingency Management
Contingency management (CM) interventions emerged from basic research on operant behavior and drug reinforcement (Silverman, 2004; Silverman et al., Chap. 65, this volume). Specifically, CM incorporated the finding that linking the absence of a problem behavior with contingent delivery of a reinforcer can lead to decreases in or elimination of problem behavior (Hunt & Azrin, 1973; Miller, 1975; Stitzer et al., 1977). Under contingency management procedures for cigarette smoking, smokers receive desirable consequences contingent on objective evidence (CO or cotinine) of smoking reductions and abstinence. Several early studies provided the initial evidence of the feasibility of using CM to reduce smoking (Tighe & Elliot, 1968; Paxton, 1980, 1981, 1983; Winett, 1973). These studies generally offered rewards, such as the return of monetary deposits, contingent upon self-reports of smoking abstinence and showed that CM could reduce levels of smoking. These studies suffered from several limitations, however, including reliance upon self-reports of abstinence (versus biochemical verification of abstinence) for implementing the contingencies or insufficient monitoring of smoking status. Subsequent studies, using more rigorous experimental methods, provided persuasive demonstrations that CM could reduce smoking (Sigmon & Patrick, 2012; Stitzer & Bigelow, 1982, 1983, 1985; Stitzer et al., 1986; Rand et al., 1989). For example, Stitzer and Bigelow (1982) delivered $5 payments to participants who submitted CO samples with at least a 50% decrease from the average baseline readings. This contingency effectively decreased CO levels, decreased number of self-reported cigarettes per day, and increased the latency to the first cigarette of the day.
A 2019 Cochrane review of CM for cigarette smoking concluded that incentives improve smoking cessation rates at long-term follow-up (i.e., at least six months from treatment onset) in mixed population studies (Notley et al., 2019). The review also highlighted that effects were sustained even after withdrawal of incentives. There was considerable diversity across studies, which included 33 studies and more than 21,600 participants. Settings included workplaces, clinics, hospitals, and community programs, and monetary consequences ranged from 0 (under deposit contract procedures, which are discussed below) to $1185. Interestingly, the review found no discernable effect of reward magnitude on outcomes. Notley et al. also examined CM targeting pregnant women who continue to smoke and found higher cessation rates compared to control groups both at the end of the pregnancy and after the birth of the baby. Smoking during pregnancy is the leading cause of infant morbidity and mortality (U.S. Department of Health and Human Services, 2001). Another major review of extant interventions revealed that incentive-based CM interventions were the most efficacious in promoting cessation among pregnant women (Chamberlain et al., 2013; see also Higgins et al., 2012; Ierfino et al., 2015; Tappin et al., 2015). Furthermore, the benefits of incentive-based interventions extend beyond smoking outcomes. Higgins et al. (2012) found incentive-based interventions improved estimated fetal growth, average birth weight, percentage of low-birth-weight deliveries, and breastfeeding duration. In several recent studies, Higgins et al. (2014) found that CM increased estimated fetal weight and abdominal circumference, and Lopez et al. (2015) revealed a reduction in the severity of postpartum depression.
Technology-Based Contingency Management
Despite the well-established efficacy of CM to promote cessation, there remain several challenges in adopting, implementing, and ensuring the fidelity of CM interventions (Dallery & Raiff, 2011). Making weekly or daily visits to a clinic to provide evidence of smoking status may also represent a substantial burden to various patient populations. To address these challenges, Dallery and colleagues developed a smoking cessation intervention that employed remote, web-based technology to allow for frequent (twice daily) and convenient breath CO collection (Dallery et al., 2008, 2013, 2017; Dallery & Glenn, 2005; Jarvis & Dallery, 2017; Reynolds et al., 2015; Stoops et al., 2009). Individuals provided CO samples in front of a video camera connected to the Internet. The video was time stamped, sent across the Internet, and evaluated by staff. An incentive was delivered electronically if the sample was valid and if the CO level displayed on the CO meter met the criterion for incentive delivery. This intervention has been effective in promoting smoking cessation (Dallery et al., 2015a, b), including in a nationwide study of smokers (n = 94) from around the United States (Dallery et al., 2017). In the nationwide study, the treatment lasted seven weeks, and there were significant differences in negative COs between the treatment group and a group that received incentives for submitting CO samples: 54% versus 25%, respectively. Although group differences persisted at the three- and six-month follow-ups, these differences were not statistically significant.
Technology-based CM has also been used to arrange group contingencies, where small groups of smokers must collectively achieve cessation goals to receive consequences (Dallery et al., 2015a, b; Meredith et al., 2011; Meredith & Dallery, 2013). Participants also provided and/or received encouragement, feedback, and support via a discussion board. Some evidence suggests that social networks influence smoking abstinence (Christakis & Fowler, 2008; Mermelstein et al., 1986; Mermelstein & Turner, 2006). Moreover, research suggests that practitioners are more willing to adopt treatments that use social components relative to those that use only tangible reinforcers (Kirby et al., 2006). Overall, group-based and individual CM appear to generate similar rates of abstinence, but there are individual differences in preferences for individual or group arrangements. One advantage of technology is that one size need not fit all: a variety of group or individual contingency arrangements could be delivered in a single platform.
To facilitate dissemination, basic cell phones and smartphones have been used to implement similar incentive-based interventions in adults (Alessi et al., 2017; Carpenter et al., 2015; Dallery et al., in press; Dan et al., 2016; Hertzberg et al., 2013; Kendzor et al., 2020; Kurti et al., 2020) and adolescents (Kong et al., 2017). For example, Alessi et al. used a CM procedure and basic cell phones to obtain visual evidence of the CO sampling procedure. CM plus usual care (n = 45) was compared to usual care alone (n = 45), which consisted of pharmacotherapy (i.e., nicotine patch) and twice-weekly counseling sessions conducted remotely via telephone. Results indicated that 82% of mobile CM versus 41% of usual care participants were abstinent at 4 weeks, and 21% versus 16% at 24 weeks. Smartphones have even greater reach relative to Internet-based methods. Compared to white Americans in the United States, black and Hispanic groups report equivalent rates of smartphone ownerships: 77% for whites, 72% for blacks, and 75% for Hispanics (Perrin, 2017). African Americans and Hispanics use their smartphones more often for health-related activities like searching for health information compared to whites (Perrin, 2017). As such, mobile technology could further reduce the “access gap” to the receipt of evidence-based interventions to promote cessation.
Monetary consequences may limit the application of CM interventions. To address this limitation, Dallery et al. (2008) used a deposit contract method that we introduced in the early CM studies noted above. Smoking status was verified via CO and Internet-based procedures. The procedure required an up-front deposit of $50 by the participant, which could be recouped based on evidence of abstinence. The deposit contract procedure produced equivalent rates of abstinence relative to a no-deposit group, and it resulted in cost savings. Jarvis and Dallery (2017) also investigated self-selected deposits rather than a fixed deposit. In Experiment 1 of their study, 47% of the CO samples met the criterion for abstinence, compared to 1% during baseline. Experiment 2 evaluated the impact of an additional clinic “match” of the participant’s deposit. No samples met the criterion during baseline but 41.5% met it during treatment. The average deposit was $82 in Experiment 1 and $49 in Experiment 2. Participants rated the intervention favorably, and sample submission rates were high. The deposit arrangements completely eliminated voucher costs, even when incorporating a clinic-match. After payments to 19 participants, $332.66 was left in surplus and donated to charity.
Halpern et al. (2015) evaluated incentive treatments for smoking cessation, including deposit contracting, in a large (N = 2538) randomized six-month intervention. Sustained abstinence for those who accepted the programs (i.e., participants could refuse the group assignment) was 52.3% in the deposit groups compared to 17.1% in the reward groups. However, the rate at which participants selected the deposit was low: only 13.7% accepted the deposit. The acceptability of a deposit—or the number of individuals who actually make a deposit—will depend on a host of factors (Halpern et al., 2012; Stedman-Falls et al., 2018). More research is needed to assess variables that influence acceptability. A technology-based method to enable a deposit (e.g., via PayPal) may lower the response effort associated with making deposits and therefore increase acceptability for some individuals (Stedman-Falls & Dallery, 2020). Deposit contracts may not only offset voucher costs, but also they may mitigate a public policy concern with paying people to change behavior (Madison et al., 2011). A deposit contract method may be acceptable and efficacious for a sizeable enough portion of smokers and stakeholders to deliver a public health impact, and it could be used in individual treatment in clinical settings.
There is certainly more work to be done to further promote cessation. Qualitative data from a recent mobile phone CM study revealed that participants wanted help learning personally relevant new skills or information about smoking cessation, and several reported significant life stressors (Dallery et al., in press). Multi-component technology-based interventions hold promise. Several mobile phone CM interventions have included skills building, stress management, and/or motivational enhancement treatment components (Carpenter et al., 2015; Hertzberg et al., 2013). For example, Carpenter et al. (2015) included weekly cognitive-behavioral therapy and pharmacotherapy, and they found smoking abstinence rates of 65% and 60% at 3 and 6 months after the mobile CM intervention, respectively. Mobile interventions have also been designed to provide intervention components such as stress management on demand based on participant input (Heron & Smyth, 2010). Such “ecological momentary interventions” may be useful adjuncts to CM (Businelle et al., 2016). In addition, methods to assess the functions of cigarette smoking should be explored to tailor intervention components to promote cessation (Burrows et al., 2020).
Considerations in the Delivery of CM in Clinical Settings
CM interventions are comprised of several components that can be implemented in a variety of ways (Meredith et al., 2014; Petry, 2000). Once a reliable and valid monitoring system is selected, either CO or cotinine in saliva or urine, the clinician must select a CM intervention (e.g., voucher or prize-based in which reinforcers are available intermittently). In addition, several specific parameters of the CM intervention must be selected to maximize cost-effectiveness and access to treatment. For example, the clinician must select parameters of reinforcement (e.g., delay, magnitude) to maximize the probability of successful outcomes (Lussier et al., 2006; Stitzer & Bigelow, 1983). As noted above, however, a major Cochrane review found little evidence of magnitude effects across smoking cessation studies. It may have been the case that the magnitudes were all sufficiently high, which means that care should be taken to ensure that the magnitude selected is above an empirically informed threshold. In clinical practice, the parameters of a specific CM program may need to be modified iteratively, using experimental methods, to reveal the optimal program for a specific individual (Dallery & Raiff, 2014).
Another consideration in designing a CM intervention in a clinical setting is the schedule of reinforcement. The most common schedule of reinforcement used in CM interventions is the ascending schedule of reinforcer delivery with resets of the voucher value for evidence of lapses or missed samples (Roll & Higgins, 2000; McPherson et al., 2018). One study found that a schedule that included ascending values plus resets resulted in greater rates of smoking abstinence than an ascending schedule without resets, and greater rates of abstinence compared to a fixed schedule in which the same amount was available for each negative sample (Roll & Higgins, 2000). Prize-based procedures also involve escalation (Petry, 2000), but because rewards are available intermittently, they may represent a lower-cost method to deliver incentives.
One potential problem with an ascending schedule of reinforcement is the low initial value of the consequence for abstinence. Several researchers have noted that some participants never contact the monetary reinforcers for abstinence (Correia et al., 2005). One reason some participants do not achieve abstinence is that most CM interventions require an abrupt transition to complete abstinence. Gradual reductions in drug use may permit greater contact with monetary reinforcers for changing drug use behavior. Several studies suggest that gradual reductions, or shaping procedures, can generate high initial rates of abstinence in nicotine-dependent individuals (Lamb et al., 2004, 2010). Shaping procedures are only possible if some quantitative or semi-quantitative monitoring of drug status is available, which is the case for CO- and several cotinine-based measures.
Conclusions
Cigarette smoking remains a vexing problem, or what some have called a wicked problem (Wallace et al., 2015). Although smoking rates overall have declined, there remain substantial disparities in smoking prevalence. Smoking remains high among people who have less education, American Indians/Alaska Natives, those who experience serious psychological distress, those experiencing socioeconomic disadvantage, people with a disability, and those who are lesbian, gay, or bisexual, to name a few examples. Population-level interventions are responsible for most of the reductions in smoking such as increased taxes, smoking bans, and mass media campaigns, especially those interventions targeting youth initiation. Nevertheless, a role still exists for treatments focused on individuals, and as such behavior analytically derived interventions are justified and require further development. This development will need to be sensitive to the changing landscape of tobacco control policies. For example, in 2017, the U.S. Food and Drug Administration announced a focus on reducing nicotine in cigarettes to levels low enough that cigarettes would be minimally or non-addictive (Gottlieb & Zeller, 2017). If new policy is implemented, it would mean that only very low nicotine content (VLNC) cigarettes would be sold in the United States. Research has found that VLNC cigarettes lead to lower dependence, fewer cigarettes smoked per day, and increased quit attempts compared to standard nicotine level cigarettes (Donny et al., 2015; Hatsukami et al., 2010), and that VLNC reduced abuse liability compared to higher nicotine content cigarettes in adolescent smokers (Cassidy et al., 2018).
As we have reviewed in this chapter, a behavior analytic framework of the etiology, maintenance, and treatment of smoking has proven to be robust and pragmatic. Many researchers and clinicians have lamented the limited scope of behavioral interventions, despite their potential to address a wide range of socially relevant behavior (e.g., Friman, 2010; Normand & Kohn, 2013). Cigarette smoking is a case example of how behavior analysis has been broadened to inform understanding and treatment of the leading preventable cause of death in the developed world. Indeed, Henningfield and Higgins (1989) noted the important contributions of behavior analysis to the 1988 Annual Report of the Surgeon General on the Health Consequences of Smoking (U.S. Department of Health and Human Services, 1988). Specifically, the contributions included research on the cross-species similarities in drug taking behavior, research showing drug taking follows the same general laws as other operant behavior, and research on behavioral treatments for cigarette smoking. We hope that the current chapter provides further evidence for the continued vitality and social relevance of behavior analytic research on cigarette smoking.
References
Acuff, S. F., Dennhardt, A. A., Correia, C. J., & Murphy, J. G. (2019). Measurement of substance-free reinforcement in addiction: A systematic review. Clinical Psychology Review, 70, 79–90. https://doi.org/10.1016/j.cpr.2019.04.003
Adriaens, K., Van Gucht, D., Declerck, P., & Baeyens, F. (2014). Effectiveness of the electronic cigarette: An eight-week Flemish study with six-month follow-up on smoking reduction, craving and experienced benefits and complaints. International Journal of Environmental Research and Public Health, 11(11), 11220–11248. https://doi.org/10.3390/ijerph111111220
Alessi, S. M., Rash, C. J., & Petry, N. M. (2017). A randomized trial of adjunct mHealth abstinence reinforcement with transdermal nicotine and counseling for smoking cessation. Nicotine and Tobacco Research, 19(3), 290–298. https://doi.org/10.1093/ntr/ntw155
American Psychiatric Association (Ed.). (1994). Diagnostic and statistical manual of mental disorders (4th ed.). American Psychiatric Association.
Audrain-McGovern, J., Rodriguez, D., Epstein, L. H., Tercyak, K. P., Goldman, P., & Wileyto, E. P. (2004). Applying a behavioral economic framework to understanding adolescent smoking. Psychology of Addictive Behaviors, 18(1), 64–73. https://doi.org/10.1037/0893-164X.18.1.64
Audrain-McGovern, J., Rodriguez, D., Epstein, L. H., Cuevas, J., Rodgers, K., & Wileyto, E. P. (2009). Does delay discounting play an etiological role in smoking or is it a consequence of smoking? Drug and Alcohol Dependence, 103(3), 99–106. https://doi.org/10.1016/j.drugalcdep.2008.12.019
Axelrod, S. (1991). Smoking cessation through functional analysis. Journal of Applied Behavior Analysis, 24(4), 717–718. https://doi.org/10.1901/jaba.1991.24-717
Benowitz, N. L. (1991). Pharmacodynamics of nicotine: Implications for rational treatment of nicotine addiction. British Journal of Addiction, 86(5), 495–499. https://doi.org/10.1111/j.1360-0443.1991.tb01796.x
Benowitz, N. L., Pipe, A., West, R., Hays, J. T., Tonstad, S., McRae, T., Lawrence, D., St Aubin, L., & Anthenelli, R. M. (2018). Cardiovascular safety of varenicline, bupropion, and nicotine patch in smokers: A randomized clinical trial. JAMA Internal Medicine, 178(5), 622–631. https://doi.org/10.1001/jamainternmed.2018.0397
Benowitz, N. L., Bernert, J. T., Foulds, J., Hecht, S. S., Jacob, P., Jarvis, M. J., Joseph, A., Oncken, C., & Piper, M. E. (2020). Biochemical verification of tobacco use and abstinence: 2019 Update. Nicotine and Tobacco Research, 22(7), 1086–1097. https://doi.org/10.1093/ntr/ntz132
Bickel, W. K., Odum, A. L., & Madden, G. J. (1999). Impulsivity and cigarette smoking: Delay discounting in current, never, and ex-smokers. Psychopharmacology, 146, 447–454.
Bricker, J. B., Bush, T., Zbikowski, S. M., Mercer, L. D., & Heffner, J. L. (2014). Randomized trial of telephone-delivered acceptance and commitment therapy versus cognitive behavioral therapy for smoking cessation: A pilot study. Nicotine and Tobacco Research, 16(11), 1446–1454. https://doi.org/10.1093/ntr/ntu102
Bricker, J. B., Mull, K. E., McClure, J. B., Watson, N. L., & Heffner, J. L. (2018). Improving quit rates of web-delivered interventions for smoking cessation: Full-scale randomized trial of WebQuit.org versus Smokefree.gov. Addiction, 113(5), 914–923. https://doi.org/10.1111/add.14127
Bullen, C., Howe, C., Laugesen, M., McRobbie, H., Parag, V., Williman, J., & Walker, N. (2013). Electronic cigarettes for smoking cessation: A randomised controlled trial. Lancet, 382(9905), 1629–1637. https://doi.org/10.1016/S0140-6736(13)61842-5
Burrows, C., Dallery, J., Kim, S., & Raiff, B. R. (2020). Validity of a functional assessment for smoking treatment recommendations questionnaire. Psychological Record, 70, 215–226. https://doi.org/10.1007/s40732-020-00375-5
Businelle, M. S., Ma, P., Kendzor, D. E., Frank, S. G., Vidrine, D. J., & Wetter, D. W. (2016). An ecological momentary intervention for smoking cessation: Evaluation of feasibility and effectiveness. Journal of Medical Internet Research, 18(12), e321. https://doi.org/10.2196/jmir.6058
Caggiula, A. R., Donny, E. C., Palmatier, M. I., Liu, X., Chaudhri, N., & Sved, A. F. (2009). The role of nicotine in smoking: A dual-reinforcement model. Nebraska Symposium on Motivation, 55, 91–109. https://doi.org/10.1007/978-0-387-78748-0_6
Cahill, K., Stevens, S., & Lancaster, T. (2014). Pharmacological treatments for smoking cessation. JAMA, 311(2), 193–194. https://doi.org/10.1001/jama.2013.283787
Cahill, K., Lindson-Hawley, N., Thomas, K. H., Fanshawe, T. R., & Lancaster, T. (2016). Nicotine receptor partial agonists for smoking cessation. The Cochrane Database of Systematic Reviews, CD006103. https://doi.org/10.1002/14651858.CD006103.pub7
Caponnetto, P., Campagna, D., Cibella, F., Morjaria, J. B., Caruso, M., Russo, C., & Polosa, R. (2013). EffiCiency and Safety of an eLectronic cigAreTte (ECLAT) as tobacco cigarettes substitute: A prospective 12-month randomized control design study. PloS One, 8(6), e66317. https://doi.org/10.1371/journal.pone.0066317
Carpenter, V. L., Hertzberg, J. S., Kirby, A. C., Calhoun, P. S., Moore, S. D., Dennis, M. F., et al. (2015). Multicomponent smoking cessation treatment including mobile contingency management in homeless veterans. Journal of Clinical Psychiatry, 76(7), 959–964. https://doi.org/10.4088/JCP.14m09053
Cassidy, R. N., & Kurti, A. N. (2018). Behavioral economic research in addiction as an area of growth for the experimental analysis of behavior. Behavior Analysis and Practice, 18(4), 333–339. https://doi.org/10.1037/bar0000105
Cassidy, R. N., Tidey, J. W., Kahler, C. W., Wray, T. B., & Colby, S. M. (2015). Increasing the value of an alternative monetary reinforcer reduces cigarette choice in adolescents. Nicotine and Tobacco Research, 17(12), 1449–1455. https://doi.org/10.1093/ntr/ntv033
Cassidy, R. N., Colby, S. M., Tidey, J. W., Jackson, K. M., Cioe, P. A., Krishnan-Sarin, S., & Hatsukami, D. (2018). Adolescent smokers’ response to reducing the nicotine content of cigarettes: Acute effects on withdrawal symptoms and subjective evaluations. Drug and Alcohol Dependence, 188, 153–160. https://doi.org/10.1016/j.drugalcdep.2018.04.006
Center for Disease Control. (2020). Economic trends in tobacco. https://www.cdc.gov/tobacco/data_statistics/fact_sheets/economics/econ_facts/index.htm
Cerutti, D. T. (1989). Discrimination theory of rule-governed behavior. Journal of the Experimental Analysis of Behavior, 51(2), 259–276. https://doi.org/10.1901/jeab.1989.51-259
Chamberlain, C., O’mara-Eves, A., Oliver, S., Caird, J. R., Perlen, S. M., Eades, S. J., & Thomas, J. (2013). Psychosocial interventions for supporting women to stop smoking in pregnancy. Cochrane Database of Systematic Reviews, 10, Article CD001055. doi:https://doi.org/10.1002/14651858.cd001055.pub4
Charntikov, S., Pittenger, S. T., Swalve, N., Barrett, S. T., & Bevins, R. A. (2020). Conditioned enhancement of the nicotine reinforcer. Experimental and Clinical Psychopharmacology, Advance online publication. https://doi.org/10.1037/pha0000370
Chaudhri, N., Caggiula, A. R., Donny, E. C., Palmatier, M. I., Liu, X., & Sved, A. F. (2006). Complex interactions between nicotine and nonpharmacological stimuli reveal multiple roles for nicotine in reinforcement. Psychopharmacology, 184(3-4), 353–366. https://doi.org/10.1007/s00213-005-0178-1
Chenoweth, M. J., & Tyndale, R. F. (2017). Pharmacogenetic optimization of smoking Cessation treatment. Trends in Pharmacological Sciences, 38(1), 55–66. https://doi.org/10.1016/j.tips.2016.09.006
Christakis, N. A., & Fowler, J. H. (2008). The collective dynamics of smoking in a large social network. The New England Journal of Medicine, 358(21), 2249–2258. https://doi.org/10.1056/NEJMsa0706154
Cole, M., & Bonem, M. (2000). The A-B-C’s of smoking cessation: Using behavioral strategies to help undergraduates stop smoking. The Behavior Analyst Today, 1(4), 89–101.
Conklin, C. A., Salkeld, R. P., Perkins, K. A., & Robin, N. (2013). Do people serve as cues to smoke? Nicotine and Tobacco Research, 15(12), 2081–2087. https://doi.org/10.1093/ntr/ntt104
Correia, C. J., Carey, K. B., & Borsari, B. (2002). Measuring substance-free and substance-related reinforcement in the natural environment. Psychology of Addictive Behaviors, 16(1), 28–34.
Correia, C. J., Sigmon, S. C., Silverman, K., Bigelow, G., & Stitzer, M. L. (2005). A comparison of voucher-delivery schedules for the initiation of cocaine abstinence. Experimental and Clinical Psychopharmacology, 13(3), 253–258. https://doi.org/10.1037/1064-1297.13.3.253
Creamer, M. R., Wang, T. W., Babb, S., Cullen, K. A., Day, H., Willis, G., Jamal, A., & Neff, L. (2019). Tobacco product use and cessation indicators among adults - United States, 2018. Morbidity and Mortality Weekly Report, 68(45), 1013–1019. https://doi.org/10.15585/mmwr.mm6845a2
Critchfield, T. S., Tucker, J. A., & Vuchinich, R. E. (1998). Self-report methods. In K. A. Lattal & M. Perone (Eds.), Applied Clinical Psychology. Handbook of research methods in human operant behavior (pp. 435–470). Plenum Press. https://doi.org/10.1007/978-1-4899-1947-2_14
Dallery, J., & Glenn, I. M. (2005). Effects of an Internet-based voucher reinforcement program for smoking abstinence: A feasibility study. Journal of Applied Behavior Analysis, 38(3), 349–357. https://doi.org/10.1901/jaba.2005.150-04
Dallery, J., & Locey, M. L. (2005). Effects of acute and chronic nicotine on impulsive choice in rats. Behavioural Pharmacology, 16(1), 15–23. https://doi.org/10.1097/00008877-200502000-00002
Dallery, J., & Raiff, B. R. (2007). Delay discounting predicts cigarette smoking in a laboratory model of abstinence reinforcement. Psychopharmacology, 190(4), 485–496. https://doi.org/10.1007/s00213-006-0627-5
Dallery, J., & Raiff, B. R. (2011). Contingency management in the 21st century: Technological innovations to promote smoking cessation. Substance Use and Misuse, 46(1). https://doi.org/10.3109/10826084.2011.521067
Dallery, J., & Raiff, B. R. (2014). Optimizing behavioral health interventions with single-case designs: From development to dissemination. Translational Behavioral Medicine, 4(3), 290–303. https://doi.org/10.1007/s13142-014-0258-z
Dallery, J., Meredith, S., & Glenn, I. M. (2008). A deposit contract method to deliver abstinence reinforcement for cigarette smoking. Journal of Applied Behavior Analysis, 41(4), 609–615. https://doi.org/10.1901/jaba.2008.41-609
Dallery, J., Raiff, B. R., & Grabinski, M. J. (2013). Internet-based contingency management to promote smoking cessation: A randomized controlled study. Journal of Applied Behavior Analysis, 46(4), 750–764. https://doi.org/10.1002/jaba.89
Dallery, J., Kurti, A., & Erb, P. (2015a). A new frontier: Integrating behavioral and digital technology to promote health behavior. The Behavior Analyst, 38(1), 19–49. https://doi.org/10.1007/s40614-014-0017-y
Dallery, J., Meredith, S., Jarvis, B., & Nuzzo, P. A. (2015b). Internet-based group contingency management to promote smoking abstinence. Experimental and Clinical Psychopharmacology, 23(3), 176–183. https://doi.org/10.1037/pha0000013
Dallery, J., Raiff, B. R., Kim, S. J., Marsch, L. A., Stitzer, M., & Grabinski, M. J. (2017). Nationwide access to an internet-based contingency management intervention to promote smoking cessation: A randomized controlled trial. Addiction, 112(5). https://doi.org/10.1111/add.13715
Dallery, J., Stinson, L., Bolivar, H., Modave, F., Salloum, R. G., Mendoza, T. M., & Rohilla, P. (in press). mMotiv8: A smartphone-based contingency management intervention to promote smoking cessation. Journal of Applied Behavior Analysis
Dan, M., Grabinski, M. J., & Raiff, B. R. (2016). Smartphone-based contingency management for smoking cessation with smokers diagnosed with attention-deficit/hyperactivity disorder. Translational Issues in Psychological Science, 2(2), 116–127. https://doi.org/10.1037/tps0000062
DeGrandpre, R. J. (2000). A science of meaning. Can behaviorism bring meaning to psychological science? The American Psychologist, 55(7), 721–739.
DeHart, W. B., Friedel, J. E., Berry, M., Frye, C., Galizio, A., & Odum, A. L. (2020). Comparison of delay discounting of different outcomes in cigarette smokers, smokeless tobacco users, e-cigarette users, and non-tobacco users. Journal of the Experimental Analysis of Behavior, Advance online publication. https://doi.org/10.1002/jeab.623
Dermody, S. S., & Shiffman, S. (2020). The time-varying effect of alcohol use on cigarette smoking relapse risk. Addictive Behaviors, 102, 106192. https://doi.org/10.1016/j.addbeh.2019.106192
Donny, E. C., Chaudhri, N., Caggiula, A. R., Evans-Martin, F. F., Booth, S., Gharib, M. A., Clements, L. A., & Sved, A. F. (2003). Operant responding for a visual reinforcer in rats is enhanced by noncontingent nicotine: Implications for nicotine self-administration and reinforcement. Psychopharmacology, 169(1), 68–76. https://doi.org/10.1007/s00213-003-1473-3
Donny, E. C., Hatsukami, D. K., Benowitz, N. L., Sved, A. F., Tidey, J. W., & Cassidy, R. N. (2014). Reduced nicotine product standards for combustible tobacco: Building an empirical basis for effective regulation. Preventive Medicine, 68, 17–22. https://doi.org/10.1016/j.ypmed.2014.06.020
Donny, E. C., Denlinger, R. L., Tidey, J. W., Koopmeiners, J. S., Benowitz, N. L., Vandrey, R. G., al’Absi, M., Carmella, S. G., Cinciripini, P. M., Dermody, S. S., Drobes, D. J., Hecht, S. S., Jensen, J., Lane, T., Le, C. T., McClernon, F. J., Montoya, I. D., Murphy, S. E., Robinson, J. D., Stitzer, M. L., et al. (2015). Randomized trial of reduced-nicotine standards for cigarettes. The New England Journal of Medicine, 373(14), 1340–1349. https://doi.org/10.1056/NEJMsa1502403
Dunbar, M. S., Shiffman, S., & Chandra, S. (2018). Exposure to workplace smoking bans and continuity of daily smoking patterns on workdays and weekends. Addictive Behaviors, 80, 53–58. https://doi.org/10.1016/j.addbeh.2018.01.006
Eissenberg, T. (2004). Measuring the emergence of tobacco dependence: The contribution of negative reinforcement models. Addiction, 99(Suppl 1), 5–29. https://doi.org/10.1111/j.1360-0443.2004.00735.x
Epstein, L. H., & Collins, F. L., Jr. (1977). The measurement of situational influences of smoking. Addictive Behaviors, 2(1), 47–53. https://doi.org/10.1016/0306-4603(77)90008-9
Epstein, L. H., Bulik, C. M., Perkins, K. A., Caggiula, A. R., & Rodefer, J. (1991). Behavioral economic analysis of smoking: Money and food as alternatives. Pharmacology, Biochemistry and Behavior, 38(4), 715–721. https://doi.org/10.1016/0091-3057(91)90232-Q
Eysenbach, G. (2005). The law of attrition. Journal of Medical Internet Research, 7(1), e11. https://doi.org/10.2196/jmir.7.1.e11
Farsalinos, K. E., Romagna, G., Tsiapras, D., Kyrzopoulos, S., & Voudris, V. (2013). Evaluating nicotine levels selection and patterns of electronic cigarette use in a group of “vapers” who had achieved complete substitution of smoking. Substance Abuse: Research and Treatment, 7, 139–146. https://doi.org/10.4137/SART.S12756
Fiore, M. C., Jaén, C. R., Baker, T. B., et al. (2008). Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. U.S. Department of Health and Human Services. Public Health Service.
Frederiksen, L. W., Martin, J. E., & Webster, J. S. (1979). Assessment of smoking behavior. Journal of Applied Behavior Analysis, 12(4), 653–664. https://doi.org/10.1901/jaba.1979.12-653
Friedman, L. S., Lichtenstein, E., & Biglan, A. (1985). Smoking onset among teens: An empirical analysis of initial situations. Addictive Behaviors, 10(1), 1–13. https://doi.org/10.1016/0306-4603(85)90048-6
Friman, P. C. (2010). Come on in, the water is fine: Achieving mainstream relevance through integration with primary medical care. The Behavior Analyst, 33(1), 19–36. https://doi.org/10.1007/BF03392201
Garrett, B. E., Martell, B. N., Caraballo, R. S., & King, B. A. (2019). Socioeconomic differences in cigarette smoking among sociodemographic groups. Preventing Chronic Disease, 16(6), 180553. https://doi.org/10.5888/pcd16.180553
Gilbert, D. G., McClernon, F. J., Rabinovich, N. E., Plath, L. C., Masson, C. L., Anderson, A. E., & Sly, K. F. (2002). Mood disturbance fails to resolve across 31 days of cigarette abstinence in women. Journal of Consulting and Clinical Psychology, 70(1), 142–152. https://doi.org/10.1037//0022-006x.70.1.142
Ginsburg, B. C., Levy, S. A., & Lamb, R. J. (2018). Nicotine as a discriminative stimulus for ethanol use. Drug and Alcohol Dependence, 182, 98–102. https://doi.org/10.1016/j.drugalcdep.2017.11.004
Glasser, A. M., Collins, L., Pearson, J. L., Abudayyeh, H., Niaura, R. S., Abrams, D. B., & Villanti, A. C. (2017). Overview of electronic nicotine delivery systems: A systematic review. American Journal of Preventive Medicine, 52(2), e33–e66. https://doi.org/10.1016/j.amepre.2016.10.036
Gottlieb, S., & Zeller, M. (2017). A nicotine-focused framework for public health. The New England Journal of Medicine, 377(12), 1111–1114. https://doi.org/10.1056/NEJMp1707409
Grace, R. C., Kivell, B. M., & Laugesen, M. (2015). Estimating cross-price elasticity of e-cigarettes using a simulated demand procedure. Nicotine and Tobacco Research, 17(5), 592–598. https://doi.org/10.1093/ntr/ntu268
Graham, A. L., Papandonatos, G. D., Cha, S., Erar, B., Amato, M. S., Cobb, N. K., Niaura, R. S., & Abrams, D. B. (2017). Improving adherence to smoking cessation treatment: Intervention effects in a web-based randomized trial. Nicotine and Tobacco Research, 19(3), 324–332. https://doi.org/10.1093/ntr/ntw282
Green, L., Myerson, J., Oliveira, L., & Chang, S. E. (2014). Discounting of delayed and probabilistic losses over a wide range of amounts. Journal of the Experimental Analysis of Behavior, 101(2), 186–200. https://doi.org/10.1901/jeab.2014.101-186
Griffith, S. D., Shiffman, S., & Heitjan, D. F. (2009). A method comparison study of timeline followback and ecological momentary assessment of daily cigarette consumption. Nicotine and Tobacco Research, 11(11), 1368–1373. https://doi.org/10.1093/ntr/ntp150
Hajek, P., Stead, L. F., West, R., Jarvis, M., Hartmann-Boyce, J., & Lancaster, T. (2013). Relapse prevention interventions for smoking cessation. The Cochrane Database of Systematic Reviews, 8, CD003999. https://doi.org/10.1002/14651858.CD003999.pub4
Hall, S. M., Havassy, B. E., & Wasserman, D. A. (1990). Commitment to abstinence and acute stress in relapse to alcohol, opiates, and nicotine. Journal of Consulting and Clinical Psychology, 58(2), 175–181. https://doi.org/10.1037//0022-006x.58.2.175
Halpern, S. D., Asch, D. A., & Volpp, K. G. (2012). Commitment contracts as a way to health. BMJ (Clinical research ed.), 344, e522. https://doi.org/10.1136/bmj.e522
Halpern, S. D., French, B., Small, D. S., Saulsgiver, K., Harhay, M. O., Audrain-McGovern, J., Loewenstein, G., Brennan, T. A., Asch, D. A., & Volpp, K. G. (2015). Randomized trial of four financial-incentive programs for smoking cessation. The New England Journal of Medicine, 372(22), 2108–2117. https://doi.org/10.1056/NEJMoa1414293
Hanley, G. P. (2012). Functional assessment of problem behavior: Dispelling myths, overcoming implementation obstacles, and developing new lore. Behavior Analysis in Practice, 5(1), 54–72. https://doi.org/10.1007/BF03391818
Harris, K. J., Golbeck, A. L., Cronk, N. J., Catley, D., Conway, K., & Williams, K. B. (2009). Timeline follow-back versus global self-reports of tobacco smoking: A comparison of findings with nondaily smokers. Psychology of Addictive Behaviors, 23(2), 368–372. https://doi.org/10.1037/a0015270
Hartmann-Boyce, J., Stead, L. F., Cahill, K., & Lancaster, T. (2014). Efficacy of interventions to combat tobacco addiction: Cochrane update of 2013 reviews. Addiction, 109(9), 1414–1425. https://doi.org/10.1111/add.12633
Hatsukami, D. K., Stead, L. F., & Gupta, P. C. (2008). Tobacco addiction. The Lancet, 371(9629), 2027–2038. https://doi.org/10.1016/S0140-6736(08)60871-5
Hatsukami, D. K., Kotlyar, M., Hertsgaard, L. A., Zhang, Y., Carmella, S. G., Jensen, J. A., Allen, S. S., Shields, P. G., Murphy, S. E., Stepanov, I., & Hecht, S. S. (2010). Reduced nicotine content cigarettes: Effects on toxicant exposure, dependence and cessation. Addiction, 105(2), 343–355. https://doi.org/10.1111/j.1360-0443.2009.02780.x
Heatherton, T. F., Kozlowski, L. T., Frecker, R. C., & Fagerström, K. O. (1991). The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. British Journal of Addiction, 86(9), 1119–1127. https://doi.org/10.1111/j.1360-0443.1991.tb01879.x
Henningfield, J. E., & Goldberg, S. R. (1983). Control of behavior by intravenous nicotine injections in human subjects. Pharmacology, Biochemistry, and Behavior, 19(6), 1021–1026. https://doi.org/10.1016/0091-3057(83)90409-4
Henningfield, J. E., & Higgins, S. T. (1989). The influence of behavior analysis on the surgeon general’s report, the health consequences of smoking: Nicotine addiction. The Behavior Analyst, 12(1), 99–101. https://doi.org/10.1007/BF03392485
Heron, K. E., & Smyth, J. M. (2010). Ecological momentary interventions: Incorporating mobile technology into psychosocial and health behaviour treatments. British Journal of Health Psychology, 15(Pt 1), 1–39. https://doi.org/10.1348/135910709X466063
Hertzberg, J. S., Carpenter, V. L., Kirby, A. C., Calhoun, P. S., Moore, S. D., Dennis, M. F., et al. (2013). Mobile contingency management as an adjunctive smoking cessation treatment for smokers with posttraumatic stress disorder. Nicotine and Tobacco Research, 15(11), 1934–1938. https://doi.org/10.1093/ntr/ntt060
Higgins, S. T., Washio, Y., Heil, S. H., Solomon, L. J., Gaalema, D. E., Higgins, T. M., & Bernstein, I. M. (2012). Financial incentives for smoking cessation among pregnant and newly postpartum women. Preventive Medicine, 55 Suppl(Suppl), S33–S40. https://doi.org/10.1016/j.ypmed.2011.12.016
Higgins, S. T., Washio, Y., Lopez, A. A., Heil, S. H., Solomon, L. J., Lynch, M. E., Hanson, J. D., Higgins, T. M., Skelly, J. M., Redner, R., & Bernstein, I. M. (2014). Examining two different schedules of financial incentives for smoking cessation among pregnant women. Preventive Medicine, 68, 51–57. https://doi.org/10.1016/j.ypmed.2014.03.024
Hughes, J. R. (2003). Motivating and helping smokers to stop smoking. Journal of General Internal Medicine, 18(12), 1053–1057. https://doi.org/10.1111/j.1525-1497.2003.20640.x
Hughes, J. R., & Carpenter, M. J. (2006). Does smoking reduction increase future cessation and decrease disease risk? A qualitative review. Nicotine and Tobacco Research, 8(6), 739–749. https://doi.org/10.1080/14622200600789726
Hughes, J. R., Higgins, S. T., & Hatsukami, D. (1990). Effects of Abstinence from Tobacco. In Research Advances in Alcohol and Drug Problems (pp. 317–398). Springer US. https://doi.org/10.1007/978-1-4899-1669-3_10
Hughes, J. R., Stead, L. F., Hartmann-Boyce, J., Cahill, K., & Lancaster, T. (2014). Antidepressants for smoking cessation. The Cochrane Database of Systematic Reviews, 2014(1), CD000031. https://doi.org/10.1002/14651858.CD000031.pub4
Hunt, G. M., & Azrin, N. H. (1973). A community-reinforcement approach to alcoholism. Behaviour Research and Therapy, 11(1), 91–104. https://doi.org/10.1016/0005-7967(73)90072-7
Ierfino, D., Mantzari, E., Hirst, J., Jones, T., Aveyard, P., & Marteau, T. M. (2015). Financial incentives for smoking cessation in pregnancy: A single-arm intervention study assessing cessation and gaming. Addiction, 110(4), 680–688. https://doi.org/10.1111/add.12817
Jaffe, J. H., Kanzler, M., Friedman, L., Stunkard, A. J., & Verebey, K. (1981). Carbon monoxide and thiocyanate levels in low tar/nicotine smokers. Addictive Behaviors, 6(4), 337–343. https://doi.org/10.1016/0306-4603(81)90049-6
Jarvis, M. J. (2004). Why people smoke. BMJ, 328(7434), 277. https://doi.org/10.1136/bmj.328.7434.277
Jarvis, B. P., & Dallery, J. (2017). Internet-based self-tailored deposit contracts to promote smoking reduction and abstinence. Journal of Applied Behavior Analysis, 50(2). https://doi.org/10.1002/jaba.377
Johnson, M. W., & Bickel, W. K. (2003). The behavioral economics of cigarette smoking: The concurrent presence of a substitute and an independent reinforcer. Behavioural Pharmacology, 14(2), 137–144. https://doi.org/10.1097/00008877-200303000-00005
Johnson, M. W., Johnson, P. S., Rass, O., & Pacek, L. R. (2017). Behavioral economic substitutability of e-cigarettes, tobacco cigarettes, and nicotine gum. Journal of Psychopharmacology, 31(7), 851–860. https://doi.org/10.1177/0269881117711921
Kassel, J. D., Stroud, L. R., & Paronis, C. A. (2003). Smoking, stress, and negative affect: Correlation, causation, and context across stages of smoking. Psychological Bulletin, 129(2), 270–304. https://doi.org/10.1037/0033-2909.129.2.270
Kendzor, D. E., Businelle, M. S., Waring, J. J. C., Mathews, A. J., Geller, D. W., Barton, J. M., et al. (2020). Automated mobile delivery of financial incentives for smoking cessation among socioeconomically disadvantaged adults: Feasibility study. JMIR MHealth and UHealth. https://doi.org/10.2196/15960
Kirby, K. C., Benishek, L. A., Dugosh, K. L., & Kerwin, M. E. (2006). Substance abuse treatment providers’ beliefs and objections regarding contingency management: Implications for dissemination. Drug and Alcohol Dependence, 85(1), 19–27. https://doi.org/10.1016/j.drugalcdep.2006.03.010
Kong, G., Goldberg, A. L., Dallery, J., & Krishnan-Sarin, S. (2017). An open-label pilot study of an intervention using mobile phones to deliver contingency management of tobacco abstinence to high school students. Experimental and Clinical Psychopharmacology, 25(5). https://doi.org/10.1037/pha0000151
Koslovsky, M. D., Hébert, E. T., Swartz, M. D., Chan, W., Leon-Novelo, L., Wilkinson, A. V., Kendzor, D. E., & Businelle, M. S. (2018). The time-varying relations between risk factors and smoking before and after a quit attempt. Nicotine and Tobacco Research, 20(10), 1231–1236. https://doi.org/10.1093/ntr/ntx225
Kurti, A. N., Tang, K., Bolivar, H. A., Evemy, C., Medina, N., Skelly, J., Nighbor, T., & Higgins, S. T. (2020). Smartphone-based financial incentives to promote smoking cessation during pregnancy: A pilot study. Preventive Medicine, 106201. Advance online publication. https://doi.org/10.1016/j.ypmed.2020.106201
Lamb, R. J., Morral, A. R., Kirby, K. C., Iguchi, M. Y., & Galbicka, G. (2004). Shaping smoking cessation using percentile schedules. Drug and Alcohol Dependence, 76(3), 247–259. https://doi.org/10.1016/j.drugalcdep.2004.05.008
Lamb, R. J., Kirby, K. C., Morral, A. R., Galbicka, G., & Iguchi, M. Y. (2010). Shaping smoking cessation in hard-to-treat smokers. Journal of Consulting and Clinical Psychology, 78(1), 62–71. https://doi.org/10.1037/a0018323
Laraway, S., Snycerski, S., Michael, J., & Poling, A. (2003). Motivating operations and terms to describe them: Some further refinements. Journal of Applied Behavior Analysis, 36(3), 407–414. https://doi.org/10.1901/jaba.2003.36-407
Lerman, C., & Audrain-McGovern, J. (2010). Reinforcing effects of smoking: More than a feeling. Biological Psychiatry, 67(8), 699–701. https://doi.org/10.1016/j.biopsych.2010.02.014
Lewis-Esquerre, J. M., Colby, S. M., Tevyaw, T. O., Eaton, C. A., Kahler, C. W., & Monti, P. M. (2005). Validation of the timeline follow-back in the assessment of adolescent smoking. Drug and Alcohol Dependence, 79(1), 33–43. https://doi.org/10.1016/j.drugalcdep.2004.12.007
Lindson, N., Chepkin, S. C., Ye, W., Fanshawe, T. R., Bullen, C., & Hartmann-Boyce, J. (2019a). Different doses, durations and modes of delivery of nicotine replacement therapy for smoking cessation. The Cochrane Database of Systematic Reviews, 4(4), CD013308. https://doi.org/10.1002/14651858.CD013308
Lindson, N., Thompson, T. P., Ferrey, A., Lambert, J. D., & Aveyard, P. (2019b). Motivational interviewing for smoking cessation. The Cochrane Database of Systematic Reviews, 7(7), CD006936. Advance online publication. https://doi.org/10.1002/14651858.CD006936.pub4
Liu, X., Palmatier, M. I., Caggiula, A. R., Donny, E. C., & Sved, A. F. (2007). Reinforcement enhancing effect of nicotine and its attenuation by nicotinic antagonists in rats. Psychopharmacology, 194(4), 463–473. https://doi.org/10.1007/s00213-007-0863-3
Locey, M. L., & Dallery, J. (2011). Nicotine and the behavioral mechanisms of intertemporal choice. Behavioural Processes, 87(1), 18–24. https://doi.org/10.1016/j.beproc.2011.02.006
Lopez, A. A., Skelly, J. M., & Higgins, S. T. (2015). Financial incentives for smoking cessation among depression-prone pregnant and newly postpartum women: Effects on smoking abstinence and depression ratings. Nicotine and Tobacco Research, 17(4), 455–462. https://doi.org/10.1093/ntr/ntu193
Lussier, J. P., Heil, S. H., Mongeon, J. A., Badger, G. J., & Higgins, S. T. (2006). A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Addiction, 101(2), 192–203. https://doi.org/10.1111/j.1360-0443.2006.01311.x
MacKillop, J., & Munafò, M. R. (2017). Commentary: Delay discounting and smoking: Robust correlation, but uncertain causation. International Journal of Epidemiology, 46(3), 870–871. https://doi.org/10.1093/ije/dyw303
Madison, K. M., Volpp, K. G., & Halpern, S. D. (2011). The law, policy, and ethics of employers’ use of financial incentives to improve health. The Journal of Law, Medicine and Ethics: A Journal of the American Society of Law, Medicine & Ethics, 39(3), 450–468. https://doi.org/10.1111/j.1748-720X.2011.00614.x
Martin, L. M., & Sayette, M. A. (2018). A review of the effects of nicotine on social functioning. Experimental and Clinical Psychopharmacology, 26(5), 425–439. https://doi.org/10.1037/pha0000208
Martner, S. G., & Dallery, J. (2019). Technology-based contingency management and e-cigarettes during the initial weeks of a smoking quit attempt. Journal of Applied Behavior Analysis, 52(4), 928–943. https://doi.org/10.1002/jaba.641
Mcfall, R. M., & Hammen, C. L. (1971). Motivation, structure, and self-monitoring: Role of nonspecific factors in smoking reduction. Journal of Consulting and Clinical Psychology, 37(1), 80–86. https://doi.org/10.1037/h0031279
McPherson, S. M., Burduli, E., Smith, C. L., Herron, J., Oluwoye, O., Hirchak, K., Orr, M. F., McDonell, M. G., & Roll, J. M. (2018). A review of contingency management for the treatment of substance-use disorders: Adaptation for underserved populations, use of experimental technologies, and personalized optimization strategies. Substance Abuse and Rehabilitation, 9, 43–57. https://doi.org/10.2147/SAR.S138439
Meredith, S. E., & Dallery, J. (2013). Investigating group contingencies to promote brief abstinence from cigarette smoking. Experimental and Clinical Psychopharmacology, 21(2), 144–154. https://doi.org/10.1037/a0031707
Meredith, S. E., Grabinski, M. J., & Dallery, J. (2011). Internet-based group contingency management to promote abstinence from cigarette smoking: A feasibility study. Drug and Alcohol Dependence, 118(1), 23–30. https://doi.org/10.1016/j.drugalcdep.2011.02.012
Meredith, S. E., Jarvis, B. P., Raiff, B. R., Rojewski, A. M., Kurti, A., Cassidy, R. N., Erb, P., Sy, J. R., & Dallery, J. (2014). The ABCs of incentive-based treatment in health care: A behavior analytic framework to inform research and practice. Psychology Research and Behavior Management, 7, 103–114. https://doi.org/10.2147/PRBM.S59792
Mermelstein, R., & Turner, L. (2006). Web-based support as an adjunct to group-based smoking cessation for adolescents. Nicotine and Tobacco Research, 8 Suppl 1(Suppl 1), S69–S76. https://doi.org/10.1080/14622200601039949
Mermelstein, R., Cohen, S., Lichtenstein, E., Baer, J. S., & Kamarck, T. (1986). Social support and smoking cessation and maintenance. Journal of Consulting and Clinical Psychology, 54(4), 447–453. https://doi.org/10.1037//0022-006x.54.4.447
Miller, P. M. (1975). A behavioral intervention program for chronic public drunkenness offenders. Archives of General Psychiatry, 32(7), 915–918. https://doi.org/10.1001/archpsyc.1975.01760250107012
Niaura, R. (2008). Nonpharmacologic therapy for smoking cessation: Characteristics and efficacy of current approaches. The American Journal of Medicine, 121(4 Suppl 1), S11–S19. https://doi.org/10.1016/j.amjmed.2008.01.021
Niaura, R. S., Rohsenow, D. J., Binkoff, J. A., Monti, P. M., Pedraza, M., & Abrams, D. B. (1988). Relevance of cue reactivity to understanding alcohol and smoking relapse. Journal of Abnormal Psychology, 97(2), 133–152. https://doi.org/10.1037//0021-843x.97.2.133
Normand, M. P., & Kohn, C. S. (2013). Don’t wag the dog: Extending the reach of applied behavior analysis. The Behavior Analyst, 36(1), 109–122. https://doi.org/10.1007/BF03392294
Notley, C., Gentry, S., Livingstone-Banks, J., Bauld, L., Perera, R., & Hartmann-Boyce, J. (2019). Incentives for smoking cessation. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.cd004307.pub6
Palmatier, M. I., Matteson, G. L., Black, J. J., Liu, X., Caggiula, A. R., Craven, L., Donny, E. C., & Sved, A. F. (2007). The reinforcement enhancing effects of nicotine depend on the incentive value of non-drug reinforcers and increase with repeated drug injections. Drug and Alcohol Dependence, 89(1), 52–59. https://doi.org/10.1016/j.drugalcdep.2006.11.020
Paxton, R. (1980). The effects of a deposit contract as a component in a behavioral programme for stopping smoking. Behaviour Research and Therapy, 18(1), 45–50.
Paxton, R. (1981). Deposit contracts with smokers: Varying frequency and amount of repayments. Behaviour Research and Therapy, 19, 117–123.
Paxton, R. (1983). Prolonging the effect of deposit contracts with smokers. Behaviour Research and Therapy, 21, 425–433.
Perkins, K. A., & Karelitz, J. L. (2014). Sensory reinforcement-enhancing effects of nicotine via smoking. Experimental and Clinical Psychopharmacology, 22(6), 511–516. https://doi.org/10.1037/a0037823
Perkins, K. A., Fonte, C., Meeker, J., White, W., & Wilson, A. (2001). The discriminative stimulus and reinforcing effects of nicotine in humans following nicotine pretreatment. Behavioural Pharmacology, 12(1), 35–44. https://doi.org/10.1097/00008877-200102000-00004
Perkins, K. A., Karelitz, J. L., Conklin, C. A., Sayette, M. A., & Giedgowd, G. E. (2010). Acute negative affect relief from smoking depends on the affect situation and measure but not on nicotine. Biological Psychiatry, 67(8), 707–714. https://doi.org/10.1016/j.biopsych.2009.12.017
Perkins, K. A., Karelitz, J. L., & Jao, N. C. (2013). Optimal carbon monoxide criteria to confirm 24-hr smoking abstinence. Nicotine and Tobacco Research, 15(5), 978–982. https://doi.org/10.1093/ntr/nts205
Perkins, K. A., Karelitz, J. L., & Boldry, M. C. (2017). Nicotine acutely enhances reinforcement from non-drug rewards in humans. Frontiers in Psychiatry, 8, 65. https://doi.org/10.3389/fpsyt.2017.00065
Perkins, K. A., Karelitz, J. L., & Boldry, M. C. (2019). Reinforcement Enhancing Effects of Nicotine Via Patch and Nasal Spray. Nicotine & Tobacco Research, 21(6), 778–783. https://doi.org/10.1093/ntr/nty038
Perrin, A. (2017, June 28). 10 facts about smartphones as the iPhone turns 10. Pew Research Center. https://www.pewresearch.org/fact-tank/2017/06/28/10-facts-about-smartphones/
Perry, J. L., & Carroll, M. E. (2008). The role of impulsive behavior in drug abuse. Psychopharmacology, 200(1), 1–26. https://doi.org/10.1007/s00213-008-1173-0
Petry, N. M. (2000). A comprehensive guide to the application of contingency management procedures in clinical settings. Drug and Alcohol Dependence, 58(1-2), 9–25. https://doi.org/10.1016/s0376-8716(99)00071-x
Piasecki, T. M., Fiore, M. C., McCarthy, D. E., & Baker, T. B. (2002). Have we lost our way? The need for dynamic formulations of smoking relapse proneness. Addiction, 97(9), 1093–1108. https://doi.org/10.1046/j.1360-0443.2002.00216.x
Piasecki, T. M., Jahng, S., Wood, P. K., Robertson, B. M., Epler, A. J., Cronk, N. J., Rohrbaugh, J. W., Heath, A. C., Shiffman, S., & Sher, K. J. (2011). The subjective effects of alcohol-tobacco co-use: An ecological momentary assessment investigation. Journal of Abnormal Psychology, 120(3), 557–571. https://doi.org/10.1037/a0023033
Pomerleau, O. F., Fagerström, K. O., Marks, J. L., Tate, J. C., & Pomerleau, C. S. (2003). Development and validation of a self-rating scale for positive- and negative-reinforcement smoking: The Michigan Nicotine Reinforcement Questionnaire. Nicotine and Tobacco Research, 5(5), 711–718. https://doi.org/10.1080/1462220031000158627
Pope, D. A., Poe, L., Stein, J. S., Kaplan, B. A., Heckman, B. W., Epstein, L. H., & Bickel, W. K. (2019). Experimental tobacco marketplace: Substitutability of e-cigarette liquid for cigarettes as a function of nicotine strength. Tobacco Control, 28(2), 206–211. https://doi.org/10.1136/tobaccocontrol-2017-054024
Prochaska, J. J., & Benowitz, N. L. (2019). Current advances in research in treatment and recovery: Nicotine addiction. Science Advances, 5(10), eaay9763. https://doi.org/10.1126/sciadv.aay9763
Quisenberry, A. J., Koffarnus, M. N., Hatz, L. E., Epstein, L. H., & Bickel, W. K. (2016). The Experimental Tobacco Marketplace I: Substitutability as a function of the price of conventional cigarettes. Nicotine and Tobacco Research, 18(7), 1642–1648. https://doi.org/10.1093/ntr/ntv230
Quisenberry, A. J., Koffarnus, M. N., Epstein, L. H., & Bickel, W. K. (2017). The Experimental Tobacco Marketplace II: Substitutability and sex effects in dual electronic cigarette and conventional cigarette users. Drug and Alcohol Dependence, 178, 551–555. https://doi.org/10.1016/j.drugalcdep.2017.06.004
Raiff, B. R., & Dallery, J. (2006). Effects of acute and chronic nicotine on responses maintained by primary and conditioned reinforcers in rats. Experimental and Clinical Psychopharmacology, 14(3), 296–305. https://doi.org/10.1037/1064-1297.14.3.296
Raiff, B. R., & Dallery, J. (2008). The generality of nicotine as a reinforcer enhancer in rats: Effects on responding maintained by primary and conditioned reinforcers and resistance to extinction. Psychopharmacology, 201(2), 305–314. https://doi.org/10.1007/s00213-008-1282-9
Ramsey, A. T., Chen, L. S., Hartz, S. M., Saccone, N. L., Fisher, S. L., Proctor, E. K., & Bierut, L. J. (2018). Toward the implementation of genomic applications for smoking cessation and smoking-related diseases. Translational Behavioral Medicine, 8(1), 7–17. https://doi.org/10.1093/tbm/ibx060
Rand, C. S., Stitzer, M. L., Bigelow, G. E., & Mead, A. M. (1989). The effects of contingent payment and frequent workplace monitoring on smoking abstinence. Addictive Behaviors, 14(2), 121–128. https://doi.org/10.1016/0306-4603(89)90041-5
Reynolds, B., Harris, M., Slone, S. A., Shelton, B. J., Dallery, J., Stoops, W., & Lewis, R. (2015). A feasibility study of home-based contingency management with adolescent smokers of rural appalachia. Experimental and Clinical Psychopharmacology, 23(6). https://doi.org/10.1037/pha0000046
Robinson, J. D., Kypriotakis, G., Karam-Hage, M., Green, C. E., Hatsukami, D. K., Cinciripini, P. M., & Donny, E. C. (2017). Cigarette nicotine content as a moderator of the relationship between negative affect and smoking. Nicotine and Tobacco Research, 19(9), 1080–1086. https://doi.org/10.1093/ntr/ntx068
Roll, J. M., & Higgins, S. T. (2000). A within-subject comparison of three different schedules of reinforcement of drug abstinence using cigarette smoking as an exemplar. Drug and Alcohol Dependence, 58(1-2), 103–109. https://doi.org/10.1016/s0376-8716(99)00073-3
Rose, J. E. (2006). Nicotine and nonnicotine factors in cigarette addiction. Psychopharmacology, 184(3-4), 274–285. https://doi.org/10.1007/s00213-005-0250-x
Rupprecht, L. E., Smith, T. T., Schassburger, R. L., Buffalari, D. M., Sved, A. F., & Donny, E. C. (2015). Behavioral mechanisms underlying nicotine reinforcement. Current Topics in Behavioral Neurosciences, 24, 19–53. https://doi.org/10.1007/978-3-319-13482-6_2
Russel, M., Peto, J., & Patel, U. (1974). The classification of smoking by factorial structure of motives. Journal of the Royal Statistical Society, 137(3), 313–346. https://doi.org/10.2307/2344953
Şanli, A., Bekmez, E., Yildiz, G., Erdoğan, B. A., Yilmaz, H. B., & Altin, G. (2016). Relationship between smoking and otorhinolaryngological symptoms. Journal of Ear, Nose, and Throat, 26(1), 28–33. https://doi.org/10.5606/kbbihtisas.2016.87059
Schnoll, R. A., Hitsman, B., Blazekovic, S., Veluz-Wilkins, A., Wileyto, E. P., Leone, F. T., & Audrain-McGovern, J. E. (2016). Longitudinal changes in smoking abstinence symptoms and alternative reinforcers predict long-term smoking cessation outcomes. Drug and Alcohol Dependence, 165, 245–252. https://doi.org/10.1016/j.drugalcdep.2016.06.017
Schwartz, J. L. (1992). Methods of smoking cessation. The Medical Clinics of North America, 76(2), 451–476. https://doi.org/10.1016/s0025-7125(16)30362-5
Shiffman, S. (2009). How many cigarettes did you smoke? Assessing cigarette consumption by global report, Time-Line Follow-Back, and ecological momentary assessment. Health Psychology, 28(5), 519–526. https://doi.org/10.1037/a0015197
Shiffman, S., Hickcox, M., Paty, J. A., Gnys, M., Kassel, J. D., & Richards, T. (1996). Progression from a smoking lapse to relapse: Prediction from abstinence violation effects, nicotine dependence, and lapse characteristics. Journal of Consulting and Clinical Psychology, 64(5), 993–1002.
Shiffman, S., Paty, J. A., Gwaltney, C. J., & Dang, Q. (2004). Immediate antecedents of cigarette smoking: An analysis of unrestricted smoking patterns. Journal of Abnormal Psychology, 113(1), 166–171. https://doi.org/10.1037/0021-843X.113.1.166
Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momentary assessment. Annual Review of Clinical Psychology, 4, 1–32. https://doi.org/10.1146/annurev.clinpsy.3.022806.091415
Shiffman, S., Dunbar, M. S., Li, X., Scholl, S. M., Tindle, H. A., Anderson, S. J., & Ferguson, S. G. (2014). Smoking patterns and stimulus control in intermittent and daily smokers. PloS One, 9(3), e89911. https://doi.org/10.1371/journal.pone.0089911
Sigmon, S. C., & Patrick, M. E. (2012). The use of financial incentives in promoting smoking cessation. Preventive Medicine, 55 Suppl(Suppl), S24–S32. https://doi.org/10.1016/j.ypmed.2012.04.007
Silverman, K. (2004). Exploring the limits and utility of operant conditioning in the treatment of drug addiction. The Behavior Analyst, 27(2), 209–230. https://doi.org/10.1007/BF03393181
Singh, T., Arrazola, R. A., Corey, C. G., Husten, C. G., Neff, L. J., Homa, D. M., & King, B. A. (2016). Tobacco use among middle and high school students--United States, 2011-2015. Morbidity and mortality weekly report, 65(14), 361–367. https://doi.org/10.15585/mmwr.mm6514a1
Snider, S. E., Cummings, K. M., & Bickel, W. K. (2017). Behavioral economic substitution between conventional cigarettes and e-cigarettes differs as a function of the frequency of e-cigarette use. Drug and Alcohol Dependence, 177, 14–22. https://doi.org/10.1016/j.drugalcdep.2017.03.017
Stead, L. F., Koilpillai, P., & Lancaster, T. (2015). Additional behavioural support as an adjunct to pharmacotherapy for smoking cessation. The Cochrane Database of Systematic Reviews, 10, CD009670. https://doi.org/10.1002/14651858.CD009670.pub3
Stead, L. F., Koilpillai, P., Fanshawe, T. R., & Lancaster, T. (2016). Combined pharmacotherapy and behavioural interventions for smoking cessation. The Cochrane Database of Systematic Reviews, 3, CD008286. https://doi.org/10.1002/14651858.CD008286.pub3
Stedman-Falls, L. M., & Dallery, J. (2020). Technology-based versus in-person deposit contract treatments for promoting physical activity. Journal of Applied Behavior Analysis, 53(4), 1904–1921. https://doi.org/10.1002/jaba.776
Stedman-Falls, L. M., Dallery, J., & Salloum, R. G. (2018). Discrete choice experiments on the acceptability of monetary-based health treatments: A replication and extension to deposit contracts. The Psychological Record, 68, 501–512. https://doi.org/10.1007/s40732-018-0296-x
Stein, J. S., Koffarnus, M. N., Stepanov, I., Hatsukami, D. K., & Bickel, W. K. (2018). Cigarette and e-liquid demand and substitution in e-cigarette-naïve smokers. Experimental and Clinical Psychopharmacology, 26(3), 233–243. https://doi.org/10.1037/pha0000192
Stitzer, M. L. (1999). Combined behavioral and pharmacological treatments for smoking cessation. Nicotine & Tobacco Research, 1(Suppl 2), S181–S210. https://doi.org/10.1080/14622299050012041
Stitzer, M. L., & Bigelow, G. E. (1982). Contingent reinforcement for reduced carbon monoxide levels in cigarette smokers. Addictive Behaviors, 7(4), 403–412. https://doi.org/10.1016/0306-4603(82)90010-7
Stitzer, M. L., & Bigelow, G. E. (1983). Contingent payment for carbon monoxide reduction: Effects of pay amount. Behavior Therapy, 14(5), 647–656. https://doi.org/10.1016/S0005-7894(83)80057-4
Stitzer, M. L., & Bigelow, G. E. (1985). Contingent reinforcement for reduced breath carbon monoxide levels: Target-specific effects on cigarette smoking. Addictive Behaviors, 10(4), 345–349. https://doi.org/10.1016/0306-4603(85)90030-9
Stitzer, M., Bigelow, G., Lawrence, C., Cohen, J., D’Lugoff, B., & Hawthorne, J. (1977). Medication take-home as a reinforcer in a methadone maintenance program. Addictive Behaviors, 2(1), 9–14. https://doi.org/10.1016/0306-4603(77)90003-x
Stitzer, M. L., Rand, C. S., Bigelow, G. E., & Mead, A. M. (1986). Contingent payment procedures for smoking reduction and cessation. Journal of Applied Behavior Analysis, 19, 197–202. https://doi.org/10.1901/jaba.1986.19-197
Stoops, W., Dallery, J., Fields, N. M., Nuzzo, P. A., Schoenberg, N. E., Martin, C. A., et al. (2009). An Internet-based abstinence reinforcement smoking cessation intervention in rural smokers. Drug and Alcohol Dependence, 105(1–2), 56–62. https://doi.org/10.1016/j.drugalcdep.2009.06.010
Stoops, W. W., Poole, M. M., Vansickel, A. R., Hays, K. A., Glaser, P. E., & Rush, C. R. (2011). Methylphenidate increases choice of cigarettes over money. Nicotine & Tobacco Research, 13(1), 29–33. https://doi.org/10.1093/ntr/ntq198
Tappin, D., Bauld, L., Purves, D., Boyd, K., Sinclair, L., MacAskill, S., McKell, J., Friel, B., McConnachie, A., de Caestecker, L., Tannahill, C., Radley, A., Coleman, T., & Cessation in Pregnancy Incentives Trial Team. (2015). Financial incentives for smoking cessation in pregnancy: Randomised controlled trial. BMJ (Clinical research ed.), 350, h134. https://doi.org/10.1136/bmj.h134
Taylor, G., Dalili, M. N., Semwal, M., Civljak, M., Sheikh, A., & Car, J. (2017). Internet-based interventions for smoking cessation. The Cochrane Database of Systematic Reviews, 9(9), CD007078. https://doi.org/10.1002/14651858.CD007078.pub5
Thompson, T. (2007). Relations among functional systems in behavior analysis. Journal of the Experimental Analysis of Behavior, 87(3), 423–440. https://doi.org/10.1901/jeab.2007.21-06
Thompson, T., & Johanson, C. E. (1981). Behavioral pharmacology of human drug dependence (NIDA Research Monograph No. 37). U.S. Department of Health and Human Services, (ADM) 81-1137.
Tighe, T. J., & Elliott, R. (1968). A technique for controlling behavior in natural life settings. Journal of Applied Behavior Analysis, 1(3), 263–266. https://doi.org/10.1901/jaba.1968.1-263
U.S. Department of Health and Human Services. (1988). The health consequences of smoking: Nicotine addiction. A report of the Surgeon General. U.S. Department of Health and Human Services, CDC, 88-8406.
U.S. Department of Health and Human Services. (2001). 2001 surgeon general’s report highlights: Tobacco use and reproductive outcomes. US Department of Health and Human Services, CDC. https://www.cdc.gov/tobacco/data_statistics/sgr/2001/highlights/outcomes/index.htm
U.S. Department of Health and Human Services. (2010). How tobacco smoke causes disease: The biology and behavioral basis for smoking-attributable disease. In How tobacco smoke causes disease: The biology and behavioral basis for smoking-attributable disease: A report of the surgeon general. Centers for Disease Control and Prevention (US). https://www.ncbi.nlm.nih.gov/books/NBK53017/
U.S. Department of Health and Human Services. (2012). Preventing tobacco use among youth and young adults: A report of the surgeon general. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
U.S. Department of Health and Human Services. (2014). The health consequences of smoking—50 years of progress: A report of the Surgeon General. US Department of Health and Human Services, CDC. https://www.cdc.gov/tobacco/data_statistics/sgr/50th-anniversary/index.htm
U.S. Department of Health and Human Services. (2016). E-Cigarette use among youth and young adults. A report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
vanDellen, M. R., Boyd, S. M., Ranby, K. W., MacKillop, J., & Lipkus, I. M. (2016). Willingness to provide support for a quit attempt: A study of partners of smokers. Journal of Health Psychology, 21(9), 1840–1849. https://doi.org/10.1177/1359105314567209
Veilleux, J. C. (2019). The relationship between distress tolerance and cigarette smoking: A systematic review and synthesis. Clinical Psychology Review, 71, 78–89. https://doi.org/10.1016/j.cpr.2019.01.003
Vuchinich, R. E., & Tucker, J. A. (1988). Contributions from behavioral theories of choice to an analysis of alcohol abuse. Journal of Abnormal Psychology, 97(2), 181–195. https://doi.org/10.1037//0021-843x.97.2.181
Wallace, R., Geller, A., & Ogawa, V. A. (2015). Committee on the assessment of agent-based models to inform tobacco product regulation. In Board on Population Health and Public Health Practice, & Institute of Medicine (Eds.), Assessing the Use of Agent-Based Models for Tobacco Regulation. National Academies Press (US).
West, R. (2004). Assessment of dependence and motivation to stop smoking. BMJ (Clinical research ed.), 328(7435), 338–339. https://doi.org/10.1136/bmj.328.7435.338
Wilson, K. G., & Hayes, S. C. (2000). Why it is crucial to understand thinking and feeling: An analysis and application to drug abuse. The Behavior Analyst, 23(1), 25–43. https://doi.org/10.1007/BF03391997
Winett, R. A. (1973). Parameters of deposit contracts in the modification of smoking. The Psychological Record, 23(1), 49–60.
Winkler, M. H., Weyers, P., Mucha, R. F., Stippekohl, B., Stark, R., & Pauli, P. (2011). Conditioned cues for smoking elicit preparatory responses in healthy smokers. Psychopharmacology, 213(4), 781–789. https://doi.org/10.1007/s00213-010-2033-2
Acknowledgment
We thank Lindsey Ives and Alexandra Knerr for comments on a previous draft of this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Dallery, J., Stinson, L., Villegas, A. (2023). Smoking Cessation. In: Matson, J.L. (eds) Handbook of Applied Behavior Analysis. Autism and Child Psychopathology Series. Springer, Cham. https://doi.org/10.1007/978-3-031-19964-6_41
Download citation
DOI: https://doi.org/10.1007/978-3-031-19964-6_41
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-19963-9
Online ISBN: 978-3-031-19964-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)