
Abstract
Angiogenesis, sprouting of new vessels from pre-existing ones, occurs throughout life in both health (physiological angiogenesis) and disease (pathological angiogenesis). The process of angiogenesis is regulated by a delicate balance of pro- and anti-angiogenic stimuli including cell–cell interaction by endothelial cells and bystander cells, production of growth factors and their inhibitors, and the modulation of the extracellular matrix (ECM). One of the driving forces of angiogenesis is the shortage of oxygen (hypoxia) occurring in the tissues. Hypoxia regulates the production of many angiogenic growth factors but also stimulates cells to express proteins of the matrix and enzymes that modify the matrix. Here, we describe the effect of hypoxia on the modification of the ECM components. We particularly focus on the synthesis and modification of collagens, the major ECM molecules that dictate the physical and biochemical properties of the ECM. Finally, we discuss further clinical interest that might be hopeful in aberrant angiogenesis or/and hypoxic conditions that characterize many diseases (e.g. diabetes, cancer).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
8.1 Introduction
New blood vessel formation includes (a) vasculogenesis that refers to de novo formation of new vessels; (b) arteriogenesis, during which pre-existing vessels enlarge and mature, e.g., the remodelling of arterioles or collaterals into large high flow vessels; and (c) angiogenesis during which new capillaries derive from pre-existing vessels (Semenza 2007). Angiogenesis occurs throughout life in both health (physiological angiogenesis) and disease (pathological angiogenesis). During development, angiogenesis is required for the normal formation and function of a living organism. In the adult, physiological angiogenesis is limited and can be only enhanced during wound healing and the menstrual cycle. Pathological angiogenesis, on the other hand, is a major contributor to diseases such as cancer (Hanahan and Folkman 1996; Lugano et al. 2020; Zuazo-Gaztelu and Casanovas 2018), diabetic retinopathy (Capitão and Soares 2016; Patel et al. 2005), age-related macular degeneration (Yamamoto-Rodríguez et al. 2020), rheumatoid arthritis (Elshabrawy et al. 2015), endometriosis and psoriasis (Folkman 2006; Heidenreich et al. 2009).
In the blood vessel wall, three major cell types can be distinguished. A monolayer of endothelial cells is found towards the luminal surface of the vessels and sits on a basal lamina (basement membrane, BM), which is a thin and flexible sheet of extracellular matrix (ECM). In capillaries, scattered pericytes are wrapped around the BM, providing growth factors and cytokines that regulate functions of blood vessels and contribute to their stabilization. The wall of larger blood vessels, such as veins and arteries, are thicker and besides the BM, also contain one or more layers of smooth muscle cells and connective tissue (Ho-Tin-Noé and Michel 2011; Caporali et al. 2017; Marchand et al. 2019; Méndez-Barbero et al. 2021).
The first step in angiogenesis is the signal that comes from injury or disease characterized by a reduced oxygen level, often called hypoxia. Hypoxia upregulates the expression of several genes, including angiogenic growth factors, such as vascular endothelial growth factor A (VEGFA) that is relatively selective for endothelial cells. These angiogenic growth factors activate endothelial cells via binding to specific receptors on their cell surface. Initially, the pre-existing blood vessels vasodilate due to the production of nitric oxide (NO) and become hyperpermeable. In addition, the endothelial cells start to produce new molecules, including enzymes that degrade the BM, e.g. matrix metalloproteinases (MMPs) and members of the plasmin system. Partial degradation of the surrounding matrix facilitates the migration towards the stimulus (diseased tissue, tumour) and the proliferation of endothelial cells. Finally, the newly formed vessel tubes are stabilized by the synthesis of new BM, by recruiting supporting cells, such as pericytes and smooth muscle cells, and blood flow begins (Fong 2008; Senger and Davis 2011; Fraisl 2013; Schito 2019).
Under physiological conditions, the dynamic process of angiogenesis is strictly regulated by the co-ordinated function of numerous angiogenic stimulators and inhibitors that include growth factors, proteases and protease inhibitors, cytokines, and chemokines. This balance is disturbed in pathological conditions that are characterized by low pO2 and/or low pH, such as hypoglycaemia, mechanical stress, injury, inflammation, and cancer. In such cases, the effect of the stimulators exceeds that of the inhibitors and there is a dramatic increase in endothelial cell activity, a phenomenon known as “the angiogenic switch”.
Hypoxia is one of the major drivers of angiogenesis. When oxygen levels drop in inflamed tissues or tumours, either by an inadequate blood supply or an increased oxygen demand, a transcriptional response to hypoxia ensues. Among other transcriptional pathways that may also be activated, the major transcription pathway involved is that of the hypoxia-inducible factors (HIFs). HIFs have been shown to bind to a cis-acting hypoxia-response element in numerous genes that encode angiogenesis regulators, such as VEGFA, angiopoietin-2 (ANGPT2), platelet-derived growth factor beta (PDGFB), and fibroblast growth factor 2 (FGF2), and many others (Hickey and Simon 2006; Hirota and Semenza 2006; Gilkes et al. 2014).
In the present review, we describe the effect of hypoxia on the modification of angiogenesis-related ECM components, focusing on the synthesis and modification of collagens, the major matrix molecules that dictate the physical and biochemical properties of the ECM. Finally, we discuss further clinical interest that might be hopeful in aberrant angiogenesis or/and hypoxic conditions that characterize many diseases (e.g. diabetes, cancer).
8.1.1 Hypoxia Signalling Pathways
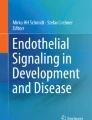
Hypoxia-inducible factors (HIFs) are heterodimeric transcription factors that consist of an oxygen-regulated HIF-α (HIF1α, HIF2α, and HIF3α) subunit and a constitutively expressed HIF-β subunit (Wang et al. 1995; Wang and Semenza 1995). In normoxia, hydroxylation of two proline residues (at positions 402 and 564) and acetylation of a lysine residue of HIF-α promote its interaction with the von Hippel-Lindau (pVHL) ubiquitin E3 ligase complex (Masson et al. 2001) that ubiquitinates HIF-α, which is then degraded in the proteasome (Fig. 8.1). Prolyl hydroxylation of HIF-α is catalysed by HIF prolyl hydroxylase domain-containing protein 1 (PHD1), PHD2, and PHD3, in a reaction that is dependent on oxygen, Fe2+, and α-ketoglutarate (Epstein et al. 2001; Kaelin and Ratcliffe 2008). Hydroxylation of an asparagine residue of HIF-α can also take place and inhibits its transcriptional activity (Lando et al. 2002). Under low oxygen conditions, HIF-α hydroxylation, ubiquitination and degradation is inhibited (Semenza 2012), and thereby a HIF-α stabilization and accumulation occurs in the cell (Fig. 8.1).

Oxygen-dependent regulation of HIF-α stabilization and transactivation. In normoxia (right), hydroxylated HIF-α proteins bind to the E3 ubiquitin ligase VHL complex (pVHL), leading to its degradation by the proteasome. In hypoxia (left), the activity of PHDs is reduced due to lack of O2, leading to HIF-α stabilization. CBP and p300 are co-activators that are required for transcriptional activation
The mechanisms through which hypoxia regulates angiogenesis are not entirely elucidated. It is well known that hypoxia, via HIF-α activation, rapidly induces VEGFA mRNA expression in all types of cells, and is the major mechanism through which hypoxia induces angiogenesis. However, hypoxia activates both HIF1α and HIF2α that although have several overlapping functions, also have distinct target genes and functions, adding to the complicated transcriptional response of endothelial cells to hypoxia (Nauta et al. 2017). Overall, HIF1α seems to induce the formation of tortuous and leaky vascular structures that are not adequately perfused, while HIF2α that is abundantly expressed in endothelial cells seems to induce the stabilization of new vessels (Skuli et al. 2012; Gong et al. 2015; Nauta et al. 2016).
Hypoxia is traditionally classified into acute and chronic that may differentially affect gene expression (Bayer et al. 2011). Acute hypoxia is mainly caused by temporary, local disturbances in tissue perfusion (Bayer et al. 2011) and has been shown to enhance the expression of the urokinase-type plasminogen activator receptor (uPAR), which—in part—explains the initial increased angiogenic response of endothelial cells, as demonstrated by the increased formation of capillary-like tubular structures in 3D fibrin matrices (Kroon et al. 2000). Chronic hypoxia lasts relatively long and can stop cell proliferation in the oxygen-depleted regions (Bayer et al. 2011; Saxena and Jolly 2019). It has been suggested that HIF1α predominates in acute hypoxia, whereas HIF2α is mostly responsible for responses to chronic hypoxia (Henze and Acker 2010), such as a more aggressive tumour phenotype through activation of genes such as MMP9, plasminogen activator inhibitor 1, or a 3.5-fold induction of the Vegfa gene (Weigand et al. 2012). On the other hand, HIF2α target genes that inhibit endothelial sprouting, such as peroxisome proliferator-activated receptor γ and membrane metalloendopeptidase, have also been found up-regulated during prolonged hypoxia in vitro (Nauta et al. 2017), supporting a shift towards a less aggressive phenotype.
8.1.2 The Structure and Function of the ECM
The ECM is a highly dynamic network that besides its structural role, it also regulates cellular functions dependent on its rigidity/elasticity and its composition. ECM continuously undergoes remodelling that is co-ordinated by the balance between production of new matrix components and degradation by matrix-degrading enzymes. Deregulation of such balance and changes in ECM composition associates with the development of several pathological conditions (Bonnans et al. 2014; Kastana et al. 2019; Mongiat et al. 2019; Yanagisawa and Yokoyama 2021; Kretschmer et al. 2021; Haller and Dudley 2022; Miller and Sewell-Loftin 2022).
The ECM varies between species and between tissues and is composed of structural biomolecules such as collagens, laminins, elastin, fibronectin, glycosaminoglycans (GAGs: hyaluronate, keratan sulphate, chondroitin sulphate, dermatan sulphate, and heparan sulphate), and proteoglycans. Most of these ECM molecules are synthesized and secreted locally by resident cells, among which endothelial cells. In addition to ECM structural components, there are other non-structural proteins called “matricellular” proteins that function as adaptors and modulators of cell–matrix interactions to guide ECM synthesis (Bonnans et al. 2014; Mongiat et al. 2019; Gopinath et al. 2022).
8.2 Hypoxia-Induced Changes in the ECM
The effect of hypoxia on ECM remodelling is long known and follows the effect of hypoxia on the transcription of numerous genes and on cell functions, such as cell proliferation and migration. For example, hypoxia seems to affect fibroblast proliferation to a great degree, so that fibrosis is considered an important outcome of tissue hypoxia (Darby and Hewitson 2016; Xiong and Liu 2017; Valle-Tenney et al. 2020; Foglia et al. 2021; Romero and Aquino-Gálvez 2021). Hypoxia also stimulates vascular smooth muscle cell proliferation and collagen deposition, thus contributing to pulmonary vascular remodelling (Jeffery and Morrell 2002) mediated by endogenous transforming growth factor beta (TGFβ) (Chen et al. 2006) and reversed by ECM remodelling inhibition (Jeffery and Morrell 2002). Remodelling of the ECM following hypoxia has also been considered, at least partly, responsible for the cardiac dysfunction induced by sleep apnoea (Farré et al. 2018), tumour progression and metastasis (Labrousse-Arias et al. 2017), the stemness and differentiation potential of cancer stem cells involved in vasculogenic mimicry (Wei et al. 2021), and for angiogenesis (Germain et al. 2010; Rodriguez et al. 2021).
8.2.1 Hypoxia Effect on Collagen Gene Expression
Collagens, as major and abundantly expressed ECM proteins, provide tensile strength, regulate cell adhesion, support chemotaxis and migration, and direct tissue development. Among the numerous types of collagens, the main types of fibrillar collagens I, II, III, V, XI, and XXIV are found in connective tissues, whereas the networking collagens IV, VIII, and X are predominately found in the BM of epithelial and endothelial cells (Ricard-Blum 2011).
Numerous in vitro and in vivo studies have shown an increased rate of collagen synthesis under hypoxic conditions by fibroblasts (Norman et al. 2000; Liu et al. 2019; Kang et al. 2020), renal epithelial cells (Basu et al. 2011; Rozen-Zvi et al. 2013), and in hepatic stellate cells (Corpechot et al. 2002), contributing to tissue fibrosis, while at the same time it also stimulates angiogenesis (Corpechot et al. 2002). In most of the published data, it is not clarified whether hypoxia has a direct effect on collagen transcription, while there are some studies showing that it is a downstream effect mediated by other factors, such as connective tissue growth factor (CTGF) that promotes collagen I synthesis (Hong et al. 2006). Collagen I is known to positively regulate retinal endothelial cell angiogenic properties and seems to mediate hypoxia-induced retinopathy in zebrafish through α2 integrin (Liu et al. 2022).
In contrast to a positive effect of hypoxia on collagen synthesis, there are numerous studies in other types of cells that show a negative regulation of collagen I by hypoxia. Rabbit aortic smooth muscle cells under hypoxia produce less collagen, despite the increased synthesis of GAGs and hyaluronic acid (Pietilä and Jaakkola 1984). In human articular chondrocytes, HIF1α reduces Col1a1 gene transcription through the transcription factor Sp3 (Duval et al. 2016), verified by the decreased collagen synthesis observed in mouse growth plate chondrocytes (Stegen et al. 2019). In porcine aortic endothelial cells, hypoxia has been shown to cause a significant decrease in collagen synthesis (Levene et al. 1982) and to induce endothelial-to-mesenchymal transition as inferred by the increased expression of vimentin and α-smooth muscle actin and the decreased expression of VE-cadherin and CD31 (Liu et al. 2019).
Collagen XV has been recently shown to be positively regulated by hypoxia through HIF1α in human mesenchymal stromal cells and may be implicated in their osteogenic potential (Lambertini et al. 2018). In kidney cells, hypoxia suppresses collagen IV α2 expression through HIF1α (Sanaei-Ardekani et al. 2021). In both cases, it is unclear whether such effects occur in endothelial cells and/or if they may have an impact on angiogenesis.
8.2.2 Hypoxia Effect on Intracellular Collagen-Modifying Enzymes
Collagen mRNA is translated to procollagen that undergoes post-translational modifications within the endoplasmic reticulum (ER). Collagen proline hydroxylation is mediated by prolyl 4-hydroxylase α-subunit (P4HA). Three isoforms of P4HA have been identified, namely P4HA1, P4HA2, and P4HA3. All α-subunit isoforms form A2B2 tetramers with the prolyl 4-hydroxylase β-subunit (P4HB) and generate the P4H1, P4H2, and P4H3 holoenzymes, respectively. P4Hs modify proline to 4-hydroxyproline, and this step is essential for the thermal stability of the collagen triple helix (Rappu et al. 2019). Non-prolyl hydroxylated procollagen α-chains are improperly folded and degraded, leading to decreased collagen deposition (Yamauchi and Sricholpech 2012). Collagen lysine hydroxylation is mediated by the three procollagen-lysine 2-oxyglutarate 5-dioxygenase (PLOD1, PLOD2, and PLOD3) enzymes. Hydroxylated lysine residues contribute to increased stability of the collagen cross-links, leading to increased tissue stiffness (van der Slot et al. 2004) (Fig. 8.2).

Biosynthesis of fibrillar collagens. The intracellular steps involve the synthesis of procollagen polypeptides and the modification of these molecules in the ER and the Golgi apparatus by P4HA and PLOD enzymes. In the extracellular space, the non-helical termini are cleaved, and the mature collagen proteins form a collagen fibril. Collagen fibre formation is initiated by collagen crosslinking, catalysed by LOX family members
Hypoxia increases the expression of P4HA1, P4HA2, PLOD1, and/or PLOD2 in many cell types, e.g., fibroblasts (Gilkes et al. 2013; Rosell-García et al. 2019; Morimoto et al. 2021), chondrocytes (Grimmer et al. 2006), cytotrophoblasts (Highet et al. 2015), human gingival fibroblasts and human periodontal ligament cells (Morimoto et al. 2021), hepatic stellate cells (Copple et al. 2011), sarcoma cells (Eisinger-Mathason et al. 2013), and endothelial cells (Becker et al. 2021 and Table 8.1). This may lead to an increased hydroxylation of collagen and stabilization and stiffening of the collagen matrix. Abrogating the expression of HIF1α or P4HA1 and P4HA2 has been shown to reduce collagen deposition from fibroblasts in vitro (Gilkes et al. 2013). Similarly, a HIF1 pathway inhibitor has been shown to inhibit hypoxia-induced P4HA1 and P4HA2, decrease prolyl hydroxylation, and induce proteolytic cleavage of collagen VI, which is the main collagen produced in uveal melanoma, thus inhibiting uveal melanoma cell invasion (Kaluz et al. 2021). Hypoxia can also up-regulate P4H1 at the level of translation, independently of HIF1α, as has been shown in human fibroblasts (Fähling et al. 2006). It has been also suggested that HIF1α but not HIF2α mediates the stimulatory effect of hypoxia on P4H enzymes (Aro et al. 2012; Bentovim et al. 2012).
Collagen hydroxylation by P4H enzymes has been shown to regulate angiogenesis. Compounds that inhibit proline hydroxylation and maturation of collagen in endothelial cells have been shown to inhibit angiogenesis in vitro (Clement et al. 2002). In the same line, up-regulation of P4HA2 by p53 results in inhibition of angiogenesis (Teodoro et al. 2006). On the other hand, such inhibitors have been shown to enhance angiogenesis (Warnecke et al. 2003; Zhu et al. 2019) but the stimulatory effects seem to be attributed to non-collagen related effects of such inhibitors that may also inhibit the HIF PHDs or to a direct effect of P4H enzymes on HIF-α stability (Xiong et al. 2018).
Five different human microvascular endothelial cell isolations were cultured for 14 days at normoxic (20% of oxygen) or hypoxic (1% of oxygen) conditions and genome-wide sequencing was performed on a Illumina platform. For details, see Nauta et al. (2016, 2017).
8.2.3 Hypoxia Effect on Extracellular Collagen-Modifying Enzymes
Once secreted extracellularly and following cleavage of the two non-helical termini by proteinases, fibrillogenesis is initiated. During this process, specific lysine and hydroxylysine residues in the N- and C-telopeptides are oxidatively deaminated by lysyl oxidase (LOX), a step necessary for the formation of covalent intra- and inter-molecular cross-links (Yamauchi and Sricholpech 2012) (Fig. 8.2).
The expression of LOXs is induced by hypoxia in tumour cells (Wang et al. 2018; Calvo-Anguiano et al. 2018), in fibroblasts (van Vlimmeren et al. 2010), in adipocytes (Anvari and Bellas 2021), and in endothelial cells (Guadall et al. 2011; Becker et al. 2021; Table 8.1). LOX-cross linked collagen activates endothelial cells in vitro and angiogenesis in vivo and correlates with the number of blood vessels in colorectal and breast cancer (Baker et al. 2013), in oral squamous cell carcinoma (Shih et al. 2013), and in hepatocellular carcinoma (Yang et al. 2019). LOX expression has been found higher in tumour endothelial cells compared to normal endothelial cells and to regulate endothelial cell migration and tube formation (Osawa et al. 2013; Shi et al. 2018). In favour of a positive effect of LOX in the regulation of angiogenesis, it has been shown that in synovial membranes, the expression of LOX positively associates with the microvascular density (Wang et al. 2017). More recently, it was shown that an interplay between LOXs and VEGFA/TGFβ is essential for the maturation of blood vessels (Grunwald et al. 2021). Lysyl oxidase-like protein-2 (LOXL2) in endothelial cells has also been identified as a hypoxia target that is involved in the regulation of angiogenesis (Bignon et al. 2011) through its effect on collagen IV scaffolding in the BM of new blood vessels (Bignon et al. 2011), but also on the deposition of other ECM components, such as fibronectin (Umana-Diaz et al. 2020). It has been shown that LOXL2 modulates endothelial-to-mesenchymal transition and thus activates angiogenic functions of endothelial cells (de Jong et al. 2019), a mechanism that has also been described for hypoxia (Liu et al. 2019). It is also of interest that LOXL2 has been found on the exterior of endothelial cell-derived exosomes and is significantly up-regulated in exosomes derived from hypoxic endothelial cells (de Jong et al. 2016). Finally, LOXL2 has been shown to stabilize HIF1α from PHD-dependent hydroxylation, supporting the existence of a positive feedback loop that enhances the effects of hypoxia (Li et al. 2021).
8.2.4 Hypoxia Effect on ECM Remodelling Enzymes
Proteolytic cleavage of the ECM is part of its remodelling and is important for regulating its composition and structure, as well as for releasing biologically active molecules. During angiogenesis, endothelial cells produce numerous enzymes that cleave ECM proteins to support various critical steps of the process: (a) BM breakdown at the initiation of angiogenesis to favour endothelial cell mobility; (b) invasion into collagen I or fibrin matrices; and (c) new lumen formation. Besides degradation of endothelial BM to allow for endothelial cell migration and new lumen formation, proteases also liberate and/or modify pro- and anti-angiogenic factors that are stored in the ECM, contribute to ectodomain shedding of growth factor receptors that are thus activated, cleave and liberate cytokines from membrane-bound precursors, and generate ECM protein fragments that inhibit or activate angiogenesis (Davis et al. 2002; Gonias et al. 2000; Selvarajan et al. 2001; Davis and Bayless 2003; van Hinsbergh and Koolwijk 2008).
MMPs are a major group of enzymes involved in ECM degradation. They are produced either as soluble or as cell membrane-anchored proteinases and have wide substrate specificities towards many ECM proteins (Laronha and Caldeira 2020). Hypoxia has been shown to increase the expression and activity of both MMP2 and MMP9 in pulmonary arterial endothelial cells in vitro and pulmonary artery endothelium in vivo (Liu et al. 2018). Hypoxia has been also shown to stimulate MMP9 expression in brain endothelial cells but not pericytes (Boroujerdi et al. 2015). MMP9 has been implicated in the hypoxia-induced blood–brain barrier disruption and its inhibition has been suggested as a potential basis for therapeutic strategies to treat brain oedema (Bauer et al. 2010). Interestingly, MMP9 seems to not be essential for hypoxic-induced cerebral angiogenesis, but it affects the post-hypoxic vascular pruning following degradation of laminin and claudin-5 (Boroujerdi et al. 2015). Hypoxic pre-treatment of bone marrow mesenchymal stem cells has led to enhanced MMP9 expression levels, among others, and after being transplanted into rats with diabetic lower limb ischaemia, these cells significantly improved angiogenesis (Liu et al. 2015). In monkey choroid-retinal endothelial cells, hypoxia has been shown to primarily induce MMP2 activity (Ottino et al. 2004) and enhancement of MMP2 by hypoxia in endothelial cells has been linked to their enhanced migration and apoptosis but not tube formation; at the same time, hypoxia decreased membrane type 1 MMP (MT1-MMP) and tissue inhibitor of MMP 2 (TIMP2) mRNA and protein levels, suggesting an MT1-MMP-independent MMP2 activation (Ben-Yosef et al. 2005). The decrease of MT1-MMP and TIMP2 by hypoxia has been observed in both short (6 h) and prolong (24 h) hypoxia, while MMP2 has been found up-regulated only at prolonged hypoxia (Ben-Yosef et al. 2002). As has been shown for collagen, the effect of hypoxia on MMPs may be mediated by CTGF that increases the expression of MMPs and decreases the expression of TIMPs by vascular endothelial cells (Kondo et al. 2002). The effect of hypoxia on MMP2 expression and neovascularization in retinas exposed to hypoxia has also been shown to be mediated by ANGPT2 (Feng et al. 2009).
Besides a direct effect of hypoxia on MMPs in endothelial cells, hypoxia can also regulate MMP expression and activity in other cells that subsequently affect tissue angiogenesis. For example, hypoxia in rheumatoid arthritis fibroblasts has been shown to up-regulate MMPs 2, 8, and 9, as well as MT1-MMP, but to have no effect on TIMPs 1 and 2 and to decrease MMP13. Conditioned medium of these cells stimulated angiogenesis in vitro (Akhavani et al. 2009). In human intervertebral disc cells, hypoxia has been shown to significantly increase MMPs 1 and 3 and decrease TIMPs 1 and 2, thus enhancing the angiogenic ability of intervertebral disc cells during inflammatory reactions in vitro (Kwon et al. 2017). In human cancer cells, MT4-MMP has been shown to be up-regulated by hypoxia or overexpression of HIF1α through activation of the transcription factor SLUG (Huang et al. 2009), and such up-regulation has been linked to invasiveness, metastasis, and angiogenesis (Huang et al. 2009; Host et al. 2012). In glioblastoma cell lines, hypoxia has been shown to significantly enhance MMPs 2 and 9, as well as collagen I. Interestingly, expression levels of angiostatins, MMP-dependent proteolytic products of plasminogen/plasmin, were also increased by hypoxia, despite the pro-angiogenic phenotype of these cells (Emara and Allalunis-Turner 2014). On the other hand, plasma levels of MMP2 and angiostatin, but not plasminogen/plasmin or MMP9, were found significantly decreased in a swine model of neonatal hypoxia compared to the normoxic group (Emara et al. 2007). Angiostatin has been shown to decrease MMP2 expression in human microvascular endothelial cells exposed to hypoxia, thus inhibiting endothelial cell migration (Radziwon-Balicka et al. 2013). Besides angiostatin, the anti-angiogenic cleavage product of collagen XVIII, endostatin, has been also found increased in extracts from tissues exposed to hypoxia and the elevated amounts of endostatin within the aortic wall of mice exposed to hypobaric hypoxia might contribute to the hypoxia-induced development of pulmonary hypertension due to decreased angiogenesis (Paddenberg et al. 2006).
Another enzyme family that is important in ECM remodelling is that of the serine proteases. The plasminogen activators, urokinase-type (uPA) and tissue-type (tPA), target plasminogen to generate plasmin, an enzyme that degrades many ECM proteins e.g., fibrin, fibronectin, and laminin (Engelse et al. 2004). The uPAR on many cells, including endothelial cells, not only binds uPA and thereby localizes its activity, but can also activate intracellular signalling pathways to coordinate ECM proteolysis (Fig. 8.3). Since uPAR lacks transmembrane and intracellular domains, transmembrane co-receptors, such as integrins, are required for its signalling (Smith and Marshall 2010).

The uPAR is an important regulator of ECM proteolysis. uPAR regulates the activity of the plasminogen activation system, an extracellular proteolytic cascade, by binding the serine protease uPA and its zymogen form, scu-PA. Plasminogen-derived plasmin cleaves and activates MMPs. Both plasmin and MMPs degrade many ECM components leading to proteolytic fragments with pro- or anti-angiogenic activities and activate or liberate growth factors that are sequestered in the ECM
Hypoxia through HIF1α has been shown to up-regulate the expression of both uPA and u-PAR in cancer cells, thus enhancing the proteolytic activity at the invasive front (Krishnamachary et al. 2003; Sullivan and Graham 2007) and promoting the epithelial-to-mesenchymal transition (Gupta et al. 2011), thus favouring invasiveness and metastasis. uPAR expression is also enhanced by hypoxia in endothelial cells and has been linked to enhanced angiogenesis in vitro (Graham et al. 1998; Kroon et al. 2000; Kroon et al. 2001; Choi et al. 2008). Hypoxia has been also shown to increase tPA and plasmin in human retinal microvascular endothelial cells (Valapala et al. 2011) through HIF1α (Huang et al. 2011). PAI1 mRNA and protein levels are also enhanced by hypoxia in bovine aortic endothelial cells (Uchiyama et al. 2000). On the other hand, prolonged hypoxia has decreased the production of uPA without affecting PAI1 (Nauta et al. 2016).
Besides the above-mentioned main families of proteolytic enzymes, several other proteases that play roles during the modulation of the matrix may be affected by hypoxia. For example, hypoxia stimulates the pro-angiogenic heparanase secretion in human retinal microvascular endothelial cells (Hu et al. 2012). Heparanase specifically cleaves cell surface and ECM heparan sulphates at intra-chain sites and its mRNA levels have been correlated with enhanced angiogenesis in the adult rat hippocampus following repeated hypoxia exposures (Navarro et al. 2008). Some members of the ADAM (a disintegrin and metalloproteinase) protein family have also been shown to be up-regulated by hypoxia in other than endothelial cells. Examples include increased expression of ADAM17 following hypoxia treatment of various cancer cell lines (Rzymski et al. 2012). ADAM17 seems to be involved in hypoxia-induced CTGF expression in human lung fibroblasts and may thus play a crucial role in the development of lung fibrosis (Chen et al. 2017). In human glioblastoma specimens, HIF1α expression has been found strongly correlated with endothelial cell markers and ADAM10 expression, implying a potential effect of hypoxia on ADAM10 expression (Musumeci et al. 2015). Hypoxia also enhances ADAM8 expression and activation in human pancreatic cells (Gao et al. 2019).
8.2.5 Hypoxia Effect on Integrins
Integrins on endothelial cells serve as receptors for various ECM molecules, including collagens or collagen fragments, and regulate angiogenesis. Hypoxia has been shown to enhance expression of ανβ3 but not ανβ5 integrin in human umbilical vein endothelial cells (Walton et al. 2000; Ben-Yosef et al. 2005). In human microvascular endothelial cells, hypoxia enhances expression of αv, β1, β3, and β5 but not α5 integrins (Befani and Liakos 2017). Hypoxia also increases ανβ3 integrin expression in other types of cells, such as melanoma cells (Cowden Dahl et al. 2005) and in myocardium early after infarction (Kalinowski et al. 2008). In human glioblastoma cells, hypoxia recruits ανβ3 and ανβ5 integrins to the cell membrane, required for the activation of HIF1α through focal adhesion kinase and for angiogenesis stimulation (Skuli et al. 2009). In the developing mouse central nervous system, hypoxia enhances expression of both fibronectin and its receptor α5β1 integrin localized on brain capillaries (Milner et al. 2008) and this has been correlated with brain endothelial cell proliferation (Li et al. 2012) or spinal cord vessel formation (Halder et al. 2018b) in response to hypoxia. On the other hand, HIF1α has been shown to decrease α5 integrin subunit expression in human gastric cancer cells, thus regulating anoikis and metastasis (Rohwer et al. 2008). Chronic mild hypoxia in the central nervous system enhances vascular integrity by increasing the expression of laminins 111 and 411 and the laminin receptor α6β1 integrin on endothelial cells, without affecting α1β1 integrin (Halder et al. 2018a).
8.3 Summary and Future Perspectives
The ECM is important for diverse physiological and pathological processes and is altered in many disease states and following hypoxia. As summarized above, hypoxia enhances ECM stiffness to facilitate endothelial cell proliferation and migration; however, a hypoxia-induced increase of ECM stiffness above a certain level inhibits the formation of new blood vessels and induces fibrosis. Similarly, hypoxia affects the expression and activation of various proteases to remodel ECM, but the physiological consequences of such effects depend on the microenvironment of cells/tissues and the final balance between the pro- and anti-angiogenic molecules produced.
One concern in the interpretation of the data related to the effect of hypoxia on the ECM is the inherent complexity related to the variations in the duration and levels of hypoxia and its categorization as acute or chronic in all the in vitro and in vivo experimental models. It has been shown that in various in vitro studies, acute hypoxia lasts between 0.5 and 72 h, while chronic hypoxia between 4 h to several weeks (Bayer and Vaupel 2012) and it remains unclear whether and how any of such settings resemble pathologies in vivo. Besides chronic and acute, cycling hypoxia (also called intermittent hypoxia) is of interest since it also appears in tumours and needs to be mimicked in vitro and in vivo (Saxena and Jolly 2019). In all cases, a strategy to control the effects of hypoxia would be the regulation of the expression and activity of HIFs, thus affecting ECM remodelling and angiogenesis (Gilkes et al. 2014; LaGory and Giaccia 2016; Lee et al. 2022).
References
Akhavani MA, Madden L, Buysschaert I, Sivakumar B, Kang N, Paleolog EM (2009) Hypoxia upregulates angiogenesis and synovial cell migration in rheumatoid arthritis. Arthritis Res Ther 11(3):R64. https://doi.org/10.1186/ar2689
Anvari G, Bellas E (2021) Hypoxia induces stress fiber formation in adipocytes in the early stage of obesity. Sci Rep 11(1):21473. https://doi.org/10.1038/s41598-021-00335-1
Aro E, Khatri R, Gerard-O'Riley R, Mangiavini L, Myllyharju J, Schipani E (2012) Hypoxia-inducible factor-1 (HIF-1) but not HIF-2 is essential for hypoxic induction of collagen prolyl 4-hydroxylases in primary newborn mouse epiphyseal growth plate chondrocytes. J Biol Chem 287(44):37134–37144. https://doi.org/10.1074/jbc.M112.352872
Baker AM, Bird D, Welti JC, Gourlaouen M, Lang G, Murray GI, Reynolds AR, Cox TR, Erler JT (2013) Lysyl oxidase plays a critical role in endothelial cell stimulation to drive tumor angiogenesis. Cancer Res 73(2):583–594. https://doi.org/10.1158/0008-5472.CAN-12-2447
Basu RK, Hubchak S, Hayashida T, Runyan CE, Schumacker PT, Schnaper HW (2011) Interdependence of HIF-1α and TGF-β/Smad3 signaling in normoxic and hypoxic renal epithelial cell collagen expression. Am J Physiol Renal Physiol 300(4):F898–F905. https://doi.org/10.1152/ajprenal.00335.2010
Bauer AT, Bürgers HF, Rabie T, Marti HH (2010) Matrix metalloproteinase-9 mediates hypoxia-induced vascular leakage in the brain via tight junction rearrangement. J Cereb Blood Flow Metab 30(4):837–848. https://doi.org/10.1038/jcbfm.2009.248
Bayer C, Vaupel P (2012) Acute versus chronic hypoxia in tumors: controversial data concerning time frames and biological consequences. Strahlenther Onkol 188(7):616–627. https://doi.org/10.1007/s00066-012-0085-4
Bayer C, Shi K, Astner ST, Maftei CA, Vaupel P (2011) Acute versus chronic hypoxia: why a simplified classification is simply not enough. Int J Radiat 80(4):965–968. https://doi.org/10.1016/j.ijrobp.2011.02.049
Becker J, Schwoch S, Zelent C, Sitte M, Salinas G, Wilting J (2021) Transcriptome analysis of hypoxic lymphatic endothelial cells indicates their potential to contribute to extracellular matrix rearrangement. Cells 10(5):1008. https://doi.org/10.3390/cells10051008
Befani C, Liakos P (2017) Hypoxia upregulates integrin gene expression in microvascular endothelial cells and promotes their migration and capillary-like tube formation. Cell Biol Int 41(7):769–778. https://doi.org/10.1002/cbin.10777
Bentovim L, Amarilio R, Zelzer E (2012) HIF1α is a central regulator of collagen hydroxylation and secretion under hypoxia during bone development. Development 139(23):4473–4483. https://doi.org/10.1242/dev.083881
Ben-Yosef Y, Lahat N, Shapiro S, Bitterman H, Miller A (2002) Regulation of endothelial matrix metalloproteinase-2 by hypoxia/reoxygenation. Circ Res 90(7):784–791. https://doi.org/10.1161/01.res.0000015588.70132.dc
Ben-Yosef Y, Miller A, Shapiro S, Lahat N (2005) Hypoxia of endothelial cells leads to MMP-2-dependent survival and death. Am J Physiol Cell Physiol 289(5):C1321–C1331. https://doi.org/10.1152/ajpcell.00079.2005
Bignon M, Pichol-Thievend C, Hardouin J, Malbouyres M, Bréchot N, Nasciutti L, Barret A, Teillon J, Guillon E, Etienne E, Caron M, Joubert-Caron R, Monnot C, Ruggiero F, Muller L, Germain S (2011) Lysyl oxidase-like protein-2 regulates sprouting angiogenesis and type IV collagen assembly in the endothelial basement membrane. Blood 118(14):3979–3989. https://doi.org/10.1182/blood-2010-10-313296
Bonnans C, Chou J, Werb Z (2014) Remodelling the extracellular matrix in development and disease. Nat Rev Mol Cell Biol 15(12):786–801. https://doi.org/10.1038/nrm3904
Boroujerdi A, Welser-Alves JV, Milner R (2015) Matrix metalloproteinase-9 mediates post-hypoxic vascular pruning of cerebral blood vessels by degrading laminin and claudin-5. Angiogenesis 18(3):255–264. https://doi.org/10.1007/s10456-015-9464-7
Calvo-Anguiano G, Lugo-Trampe JJ, Camacho A, Said-Fernández S, Mercado-Hernández R, Zomosa-Signoret V, Rojas-Martínez A, Ortiz-López R (2018) Comparison of specific expression profile in two in vitro hypoxia models. Exp Ther Med 15(6):4777–4784. https://doi.org/10.3892/etm.2018.6048
Capitão M, Soares R (2016) Angiogenesis and inflammation crosstalk in diabetic retinopathy. J Cell Biochem 117(11):2443–2453. https://doi.org/10.1002/jcb.25575
Caporali A, Martello A, Miscianinov V, Maselli D, Vono R, Spinetti G (2017) Contribution of pericyte paracrine regulation of the endothelium to angiogenesis. Pharmacol Ther 171:56–64. https://doi.org/10.1016/j.pharmthera.2016.10.001
Chen YF, Feng JA, Li P, Xing D, Zhang Y, Serra R, Ambalavanan N, Majid-Hassan E, Oparil S (2006) Dominant negative mutation of the TGF-beta receptor blocks hypoxia-induced pulmonary vascular remodeling. J Appl Physiol 100(2):564–571. https://doi.org/10.1152/japplphysiol.00595.2005
Chen JY, Lin CH, Chen BC (2017) Hypoxia-induced ADAM 17 expression is mediated by RSK1-dependent C/EBPβ activation in human lung fibroblasts. Mol Immunol 88:155–163. https://doi.org/10.1016/j.molimm.2017.06.029
Choi HJ, Eun JS, Kim DK, Li RH, Shin TY, Park H, Cho NP, Soh Y (2008) Icariside II from Epimedium koreanum inhibits hypoxia-inducible factor-1alpha in human osteosarcoma cells. Eur J Pharmacol 579(1-3):58–65. https://doi.org/10.1016/j.ejphar.2007.10.010
Clement PM, Hanauske-Abel HM, Wolff EC, Kleinman HK, Park MH (2002) The antifungal drug ciclopirox inhibits deoxyhypusine and proline hydroxylation, endothelial cell growth and angiogenesis in vitro. Int J Cancer 100(4):491–498. https://doi.org/10.1002/ijc.10515
Copple BL, Bai S, Burgoon LD, Moon JO (2011) Hypoxia-inducible factor-1α regulates the expression of genes in hypoxic hepatic stellate cells important for collagen deposition and angiogenesis. Liver Int 31(2):230–244. https://doi.org/10.1111/j.1478-3231.2010.02347.x
Corpechot C, Barbu V, Wendum D, Kinnman N, Rey C, Poupon R, Housset C, Rosmorduc O (2002) Hypoxia-induced VEGF and collagen I expressions are associated with angiogenesis and fibrogenesis in experimental cirrhosis. Hepatology 35(5):1010–1021. https://doi.org/10.1053/jhep.2002.32524
Cowden Dahl KD, Robertson SE, Weaver VM, Simon MC (2005) Hypoxia-inducible factor regulates alphavbeta3 integrin cell surface expression. Mol Biol Cell 16(4):1901–1912. https://doi.org/10.1091/mbc.e04-12-1082
Darby IA, Hewitson TD (2016) Hypoxia in tissue repair and fibrosis. Cell Tissue Res 365(3):553–562. https://doi.org/10.1007/s00441-016-2461-3
Davis GE, Bayless KJ (2003) An integrin and Rho GTPase-dependent pinocytic vacuole mechanism controls capillary lumen formation in collagen and fibrin matrices. Microcirculation 10(1):27–44. https://doi.org/10.1038/sj.mn.7800175
Davis GE, Bayless KJ, Mavila A (2002) Molecular basis of endothelial cell morphogenesis in three-dimensional extracellular matrices. Anat Rec 268(3):252–275. https://doi.org/10.1002/ar.10159
de Jong OG, van Balkom BW, Gremmels H, Verhaar MC (2016) Exosomes from hypoxic endothelial cells have increased collagen crosslinking activity through up-regulation of lysyl oxidase-like 2. J Cell Mol Med 20(2):342–350. https://doi.org/10.1111/jcmm.12730
de Jong OG, van der Waals LM, Kools FRW, Verhaar MC, van Balkom BWM (2019) Lysyl oxidase-like 2 is a regulator of angiogenesis through modulation of endothelial-to-mesenchymal transition. J Cell Physiol 234(7):10260–10269. https://doi.org/10.1002/jcp.27695
Duval E, Bouyoucef M, Leclercq S, Baugé C, Boumédiene K (2016) Hypoxia inducible factor 1 alpha down-regulates type I collagen through Sp3 transcription factor in human chondrocytes. IUBMB Life 68(9):756–763. https://doi.org/10.1002/iub.1539
Eisinger-Mathason TS, Zhang M, Qiu Q, Skuli N, Nakazawa MS, Karakasheva T, Mucaj V, Shay JE, Stangenberg L, Sadri N, Puré E, Yoon SS, Kirsch DG, Simon MC (2013) Hypoxia-dependent modification of collagen networks promotes sarcoma metastasis. Cancer Discov 3(10):1190–1205. https://doi.org/10.1158/2159-8290.CD-13-0118
Elshabrawy HA, Chen Z, Volin MV, Ravella S, Virupannavar S, Shahrara S (2015) The pathogenic role of angiogenesis in rheumatoid arthritis. Angiogenesis 18(4):433–448. https://doi.org/10.1007/s10456-015-9477-2
Emara M, Allalunis-Turner J (2014) Effect of hypoxia on angiogenesis related factors in glioblastoma cells. Oncol Rep 31(4):1947–1953. https://doi.org/10.3892/or.2014.3037
Emara M, Obaid L, Johnson S, Bigam DL, Cheung PY (2007) Expression of angiostatin and its related factors in the plasma of newborn pigs with hypoxia and reoxygenation. Arch Biochem Biophys 466(1):136–144. https://doi.org/10.1016/j.abb.2007.07.009
Engelse MA, Hanemaaijer R, Koolwijk P, van Hinsbergh VW (2004) The fibrinolytic system and matrix metalloproteinases in angiogenesis and tumor progression. Semin Thromb Hemost 30(1):71–82. https://doi.org/10.1055/s-2004-822972
Epstein AC, Gleadle JM, McNeill LA, Hewitson KS, O'Rourke J, Mole DR, Mukherji M, Metzen E, Wilson MI, Dhanda A, Tian YM, Masson N, Hamilton DL, Jaakkola P, Barstead R, Hodgkin J, Maxwell PH, Pugh CW, Schofield CJ, Ratcliffe PJ (2001) C. elegans EGL-9 and mammalian homologs define a family of dioxygenases that regulate HIF by prolyl hydroxylation. Cell 107(1):43–54. https://doi.org/10.1016/s0092-8674(01)00507-4
Fähling M, Mrowka R, Steege A, Nebrich G, Perlewitz A, Persson PB, Thiele BJ (2006) Translational control of collagen prolyl 4-hydroxylase-alpha(I) gene expression under hypoxia. J Biol Chem 281(36):26089–26101. https://doi.org/10.1074/jbc.M604939200
Farré N, Otero J, Falcones B, Torres M, Jorba I, Gozal D, Almendros I, Farré R, Navajas D (2018) Intermittent hypoxia mimicking sleep apnea increases passive stiffness of myocardial extracellular matrix. A multiscale study. Front Physiol 9:1143. https://doi.org/10.3389/fphys.2018.01143
Feng Y, Wang Y, Pfister F, Hillebrands JL, Deutsch U, Hammes HP (2009) Decreased hypoxia-induced neovascularization in angiopoietin-2 heterozygous knockout mouse through reduced MMP activity. Cell Physiol Biochem 23(4-6):277–284. https://doi.org/10.1159/000218174
Foglia B, Novo E, Protopapa F, Maggiora M, Bocca C, Cannito S, Parola M (2021) Hypoxia, hypoxia-inducible factors and liver fibrosis. Cells 10(7):1764. https://doi.org/10.3390/cells10071764
Folkman J (2006) Angiogenesis. Annu Rev Med 57:1–18. https://doi.org/10.1146/annurev.med.57.121304.131306
Fong GH (2008) Mechanisms of adaptive angiogenesis to tissue hypoxia. Angiogenesis 11(2):121–140. https://doi.org/10.1007/s10456-008-9107-3
Fraisl P (2013) Crosstalk between oxygen- and nitric oxide-dependent signaling pathways in angiogenesis. Exp Cell Res 319(9):1331–1339. https://doi.org/10.1016/j.yexcr.2013.02.010
Gao Y, Yu X, Zhang F, Dai J (2019) Propofol inhibits pancreatic cancer progress under hypoxia via ADAM8. J Hepatobiliary Pancreat Sci 26(6):219–226. https://doi.org/10.1002/jhbp.624
Germain S, Monnot C, Muller L, Eichmann A (2010) Hypoxia-driven angiogenesis: role of tip cells and extracellular matrix scaffolding. Curr Opin Hematol 17(3):245–251. https://doi.org/10.1097/MOH.0b013e32833865b9
Gilkes DM, Bajpai S, Chaturvedi P, Wirtz D, Semenza GL (2013) Hypoxia-inducible factor 1 (HIF-1) promotes extracellular matrix remodeling under hypoxic conditions by inducing P4HA1, P4HA2, and PLOD2 expression in fibroblasts. J Biol Chem 288(15):10819–10829. https://doi.org/10.1074/jbc.M112.442939
Gilkes DM, Semenza GL, Wirtz D (2014) Hypoxia and the extracellular matrix: drivers of tumour metastasis. Nat Rev Cancer 14(6):430–439. https://doi.org/10.1038/nrc3726
Gong H, Rehman J, Tang H, Wary K, Mittal M, Chaturvedi P, Zhao YY, Komarova YA, Vogel SM, Malik AB (2015) HIF2α signaling inhibits adherens junctional disruption in acute lung injury. J Clin Invest 125(2):652–664. https://doi.org/10.1172/JCI77701
Gonias SL, Carmichael A, Mettenburg JM, Roadcap DW, Irvin WP, Webb DJ (2000) Identical or overlapping sequences in the primary structure of human α2-macroglobulin are responsible for the binding of nerve growth factor-β, platelet-derived growth factor-BB, and transforming growth factor-β. J Biol Chem 275(8):5826–5831. https://doi.org/10.1074/jbc.275.8.5826
Gopinath P, Natarajan A, Sathyanarayanan A, Veluswami S, Gopisetty G (2022) The multifaceted role of Matricellular Proteins in health and cancer, as biomarkers and therapeutic targets. Gene 815:146137. https://doi.org/10.1016/j.gene.2021.146137
Graham CH, Fitzpatrick TE, McCrae KR (1998) Hypoxia stimulates urokinase receptor expression through a heme protein-dependent pathway. Blood 91(9):3300–3307. https://doi.org/10.1182/blood.V91.9.3300
Grimmer C, Balbus N, Lang U, Aigner T, Cramer T, Müller L, Swoboda B, Pfander D (2006) Regulation of type II collagen synthesis during osteoarthritis by prolyl-4-hydroxylases: possible influence of low oxygen levels. Am J Pathol 169(2):491–502. https://doi.org/10.2353/ajpath.2006.050738
Grunwald H, Hunker KL, Birt I, Aviram R, Zaffryar-Eilot S, Ganesh SK, Hasson P (2021) Lysyl oxidase interactions with transforming growth factor-β during angiogenesis are mediated by endothelin 1. FASEB J 35(9):e21824. https://doi.org/10.1096/fj.202001860RR
Guadall A, Orriols M, Alcudia JF, Cachofeiro V, Martinez-Gonzalez J, Rodriguez C (2011) Hypoxia-induced ROS signaling is required for LOX up-regulation in endothelial cells. Front Biosci (Elite Ed) 3(3):955–967. https://doi.org/10.2741/e301
Gupta R, Chetty C, Bhoopathi P, Lakka S, Mohanam S, Rao JS, Dinh DE (2011) Downregulation of uPA/uPAR inhibits intermittent hypoxia-induced epithelial-mesenchymal transition (EMT) in DAOY and D283 medulloblastoma cells. Int J Oncol 38(3):733–744. https://doi.org/10.3892/ijo.2010.883
Halder SK, Kant R, Milner R (2018a) Chronic mild hypoxia increases expression of laminins 111 and 411 and the laminin receptor α6β1 integrin at the blood-brain barrier. Brain Res 1700:78–85. https://doi.org/10.1016/j.brainres.2018.07.012
Halder SK, Kant R, Milner R (2018b) Chronic mild hypoxia promotes profound vascular remodeling in spinal cord blood vessels, preferentially in white matter, via an α5β1 integrin-mediated mechanism. Angiogenesis 21(2):251–266. https://doi.org/10.1007/s10456-017-9593-2
Haller SJ, Dudley AT (2022) Extracellular mechanotransduction. J Gen Physiol 154(3):e202113026. https://doi.org/10.1085/jgp.202113026
Hanahan D, Folkman J (1996) Patterns and emerging mechanisms of the angiogenic switch during tumorigenesis. Cell 86(3):353–364. https://doi.org/10.1016/s0092-8674(00)80108-7
Heidenreich R, Röcken M, Ghoreschi K (2009) Angiogenesis drives psoriasis pathogenesis. Int J Exp Pathol 90(3):232–248. https://doi.org/10.1111/j.1365-2613.2009.00669.x
Henze AT, Acker T (2010) Feedback regulators of hypoxia-inducible factors and their role in cancer biology. Cell Cycle 9(14):2749–2763. https://doi.org/10.4161/cc.9.14.12591
Hickey MM, Simon MC (2006) Regulation of angiogenesis by hypoxia and hypoxia-inducible factors. Curr Top Dev Biol 76:217–257. https://doi.org/10.1016/S0070-2153(06)76007-0
Highet AR, Khoda SM, Buckberry S, Leemaqz S, Bianco-Miotto T, Harrington E, Ricciardelli C, Roberts CT (2015) Hypoxia induced HIF-1/HIF-2 activity alters trophoblast transcriptional regulation and promotes invasion. Eur J Cell Biol 94(12):589–602. https://doi.org/10.1016/j.ejcb.2015.10.004
Hirota K, Semenza GL (2006) Regulation of angiogenesis by hypoxia-inducible factor 1. Crit Rev Oncol Hematol 59(1):15–26. https://doi.org/10.1016/j.critrevonc.2005.12.003
Hong KH, Yoo SA, Kang SS, Choi JJ, Kim WU, Cho CS (2006) Hypoxia induces expression of connective tissue growth factor in scleroderma skin fibroblasts. Clin Exp Immunol 146(2):362–370. https://doi.org/10.1111/j.1365-2249.2006.03199.x
Host L, Paye A, Detry B, Blacher S, Munaut C, Foidart JM, Seiki M, Sounni NE, Noel A (2012) The proteolytic activity of MT4-MMP is required for its pro-angiogenic and pro-metastatic promoting effects. Int J Cancer 131(7):1537–1548. https://doi.org/10.1002/ijc.27436
Ho-Tin-Noé B, Michel JB (2011) Initiation of angiogenesis in atherosclerosis: smooth muscle cells as mediators of the angiogenic response to atheroma formation. Trends Cardiovasc Med 21(7):183–187. https://doi.org/10.1016/j.tcm.2012.05.007
Hu J, Song X, He YQ, Freeman C, Parish CR, Yuan L, Yu H, Tang S (2012) Heparanase and vascular endothelial growth factor expression is increased in hypoxia-induced retinal neovascularization. Invest Ophthalmol Vis Sci 53(11):6810–6817. https://doi.org/10.1167/iovs.11-9144
Huang CH, Yang WH, Chang SY, Tai SK, Tzeng CH, Kao JY, Wu KJ, Yang MH (2009) Regulation of membrane-type 4 matrix metalloproteinase by SLUG contributes to hypoxia-mediated metastasis. Neoplasia 11(12):1371–1382. https://doi.org/10.1593/neo.91326
Huang B, Deora AB, He KL, Chen K, Sui G, Jacovina AT, Almeida D, Hong P, Burgman P, Hajjar KA (2011) Hypoxia-inducible factor-1 drives annexin A2 system-mediated perivascular fibrin clearance in oxygen-induced retinopathy in mice. Blood 118(10):2918–2929. https://doi.org/10.1182/blood-2011-03-341214
Jeffery TK, Morrell NW (2002) Molecular and cellular basis of pulmonary vascular remodeling in pulmonary hypertension. Prog Cardiovasc Dis 45(3):173–202. https://doi.org/10.1053/pcad.2002.130041
Kaelin WG Jr, Ratcliffe PJ (2008) Oxygen sensing by metazoans: the central role of the HIF hydroxylase pathway. Mol Cell 30(4):393–402. https://doi.org/10.1016/j.molcel.2008.04.009
Kalinowski L, Dobrucki LW, Meoli DF, Dione DP, Sadeghi MM, Madri JA, Sinusas AJ (2008) Targeted imaging of hypoxia-induced integrin activation in myocardium early after infarction. J Appl Physiol 104(5):1504–1512. https://doi.org/10.1152/japplphysiol.00861.2007
Kaluz S, Zhang Q, Kuranaga Y, Yang H, Osuka S, Bhattacharya D, Devi NS, Mun J, Wang W, Zhang R, Goodman MM, Grossniklaus HE, Van Meir EG (2021) Targeting HIF-activated collagen prolyl 4-hydroxylase expression disrupts collagen deposition and blocks primary and metastatic uveal melanoma growth. Oncogene 40(33):5182–5191. https://doi.org/10.1038/s41388-021-01919-x
Kang Y, Roh MR, Rajadurai S, Rajadurai A, Kumar R, Njauw CN, Zheng Z, Tsao H (2020) Hypoxia and HIF-1α regulate collagen production in keloids. J Invest Dermatol 140(11):2157–2165. https://doi.org/10.1016/j.jid.2020.01.036
Kastana P, Choleva E, Poimenidi E, Karamanos N, Sugahara K, Papadimitriou E (2019) Insight into the role of chondroitin sulfate E in angiogenesis. FEBS J 286(15):2921–2936. https://doi.org/10.1111/febs.14830
Kondo S, Kubota S, Shimo T, Nishida T, Yosimichi G, Eguchi T, Sugahara T, Takigawa M (2002) Connective tissue growth factor increased by hypoxia may initiate angiogenesis in collaboration with matrix metalloproteinases. Carcinogenesis 23(5):769–776. https://doi.org/10.1093/carcin/23.5.769
Kretschmer M, Rüdiger D, Zahler S (2021) Mechanical aspects of angiogenesis. Cancers (Basel) 13(19):4987. https://doi.org/10.3390/cancers13194987
Krishnamachary B, Berg-Dixon S, Kelly B, Agani F, Feldser D, Ferreira G, Iyer N, LaRusch J, Pak B, Taghavi P, Semenza GL (2003) Regulation of colon carcinoma cell invasion by hypoxia-inducible factor 1. Cancer Res 63(5):1138–1143
Kroon ME, Koolwijk P, van der Vecht B, van Hinsbergh VW (2000) Urokinase receptor expression on human microvascular endothelial cells is increased by hypoxia: implications for capillary-like tube formation in a fibrin matrix. Blood 96(8):2775–2783. https://doi.org/10.1182/blood.V96.8.2775
Kroon ME, Koolwijk P, van der Vecht B, van Hinsbergh VW (2001) Hypoxia in combination with FGF-2 induces tube formation by human microvascular endothelial cells in a fibrin matrix: involvement of at least two signal transduction pathways. J Cell Sci 114(Pt 4):825–833. https://doi.org/10.1242/jcs.114.4.825
Kwon WK, Moon HJ, Kwon TH, Park YK, Kim JH (2017) The role of hypoxia in angiogenesis and extracellular matrix regulation of intervertebral disc cells during inflammatory reactions. Neurosurgery 81(5):867–875. https://doi.org/10.1093/neuros/nyx149
Labrousse-Arias D, Martínez-Ruiz A, Calzada MJ (2017) Hypoxia and redox signaling on extracellular matrix remodeling: from mechanisms to pathological implications. Antioxid Redox Signal 27(12):802–822. https://doi.org/10.1089/ars.2017.7275
LaGory EL, Giaccia AJ (2016) The ever-expanding role of HIF in tumour and stromal biology. Nat Cell Biol 18(4):356–365. https://doi.org/10.1038/ncb3330
Lambertini E, Penolazzi L, Angelozzi M, Bergamin LS, Manferdini C, Vieceli Dalla Sega F, Paolella F, Lisignoli G, Piva R (2018) Hypoxia preconditioning of human MSCs: a direct evidence of HIF-1α and collagen type XV correlation. Cell Physiol Biochem 51(5):2237–2249. https://doi.org/10.1159/000495869
Lando D, Peet DJ, Gorman JJ, Whelan DA, Whitelaw ML, Bruick RK (2002) FIH-1 is an asparaginyl hydroxylase enzyme that regulates the transcriptional activity of hypoxia-inducible factor. Genes Dev 16(12):1466–1471. https://doi.org/10.1101/gad.991402
Laronha H, Caldeira J (2020) Structure and function of human matrix metalloproteinases. Cells 9(5):1076. https://doi.org/10.3390/cells9051076
Lee D, Miwa Y, Kunimi H, Ibuki M, Shoda C, Nakai A, Kurihara T (2022) HIF inhibition therapy in ocular diseases. Keio J Med 71(1):1–12. https://doi.org/10.2302/kjm.2021-0004-IR
Levene CI, Kapoor R, Heale G (1982) The effect of hypoxia on the synthesis of collagen and glycosaminoglycans by cultured pig aortic endothelium. Atherosclerosis 44(3):327–337. https://doi.org/10.1016/0021-9150(82)90007-7
Li L, Welser-Alves J, van der Flier A, Boroujerdi A, Hynes RO, Milner R (2012) An angiogenic role for the α5β1 integrin in promoting endothelial cell proliferation during cerebral hypoxia. Exp Neurol 237(1):46–54. https://doi.org/10.1016/j.expneurol.2012.06.005
Li R, Li H, Zhu L, Zhang X, Liu D, Li Q, Ni B, Hu L, Zhang Z, Zhang Y, Wang X, Jiang SH (2021) Reciprocal regulation of LOXL2 and HIF1α drives the Warburg effect to support pancreatic cancer aggressiveness. Cell Death Dis 12(12):1106. https://doi.org/10.1038/s41419-021-04391-3
Liu J, Hao H, Xia L, Ti D, Huang H, Dong L, Tong C, Hou Q, Zhao Y, Liu H, Fu X, Han W (2015) Hypoxia pretreatment of bone marrow mesenchymal stem cells facilitates angiogenesis by improving the function of endothelial cells in diabetic rats with lower ischemia. PLoS One 10(5):e0126715. https://doi.org/10.1371/journal.pone.0126715
Liu Y, Zhang H, Yan L, Du W, Zhang M, Chen H, Zhang L, Li G, Li J, Dong Y, Zhu D (2018) MMP-2 and MMP-9 contribute to the angiogenic effect produced by hypoxia/15-HETE in pulmonary endothelial cells. J Mol Cell Cardiol 121:36–50. https://doi.org/10.1016/j.yjmcc.2018.06.006
Liu C, Zhou X, Lu J, Zhu L, Li M (2019) Autophagy mediates 2-methoxyestradiol-inhibited scleroderma collagen synthesis and endothelial-to-mesenchymal transition induced by hypoxia. Rheumatology 58(11):1966–1975. https://doi.org/10.1093/rheumatology/kez159
Liu X, Xing Y, Liu X, Zeng L, Ma J (2022) Opticin ameliorates hypoxia-induced retinal angiogenesis by suppression of integrin α2-I domain-collagen complex formation and RhoA/ROCK1 signaling. Invest Ophthalmol Vis Sci 63(1):13. https://doi.org/10.1167/iovs.63.1.13
Lugano R, Ramachandran M, Dimberg A (2020) Tumor angiogenesis: causes, consequences, challenges and opportunities. Cell Mol Life Sci 77(9):1745–1770. https://doi.org/10.1007/s00018-019-03351-7
Marchand M, Monnot C, Muller L, Germain S (2019) Extracellular matrix scaffolding in angiogenesis and capillary homeostasis. Semin Cell Dev Biol 89:147–156. https://doi.org/10.1016/j.semcdb.2018.08.007
Masson N, Willam C, Maxwell PH, Pugh CW, Ratcliffe PJ (2001) Independent function of two destruction domains in hypoxia-inducible factor-α chains activated by prolyl hydroxylation. EMBO J 20(18):5197–5206. https://doi.org/10.1093/emboj/20.18.5197
Méndez-Barbero N, Gutiérrez-Muñoz C, Blanco-Colio LM (2021) Cellular crosstalk between endothelial and smooth muscle cells in vascular wall remodeling. Int J Mol Sci 22(14):7284. https://doi.org/10.3390/ijms22147284
Miller B, Sewell-Loftin MK (2022) Mechanoregulation of vascular endothelial growth factor receptor 2 in angiogenesis. Front Cardiovasc Med 8:804934. https://doi.org/10.3389/fcvm.2021.804934
Milner R, Hung S, Erokwu B, Dore-Duffy P, LaManna JC, del Zoppo GJ (2008) Increased expression of fibronectin and the alpha 5 beta 1 integrin in angiogenic cerebral blood vessels of mice subject to hypobaric hypoxia. Mol Cell Neurosci 38(1):43–52. https://doi.org/10.1016/j.mcn.2008.01.013
Mongiat M, Buraschi S, Andreuzzi E, Neill T, Iozzo RV (2019) Extracellular matrix: the gatekeeper of tumor angiogenesis. Biochem Soc Trans 47(5):1543–1555. https://doi.org/10.1042/BST20190653
Morimoto C, Takedachi M, Kawasaki K, Shimomura J, Murata M, Hirai A, Kawakami K, Sawada K, Iwayama T, Murakami S (2021) Hypoxia stimulates collagen hydroxylation in gingival fibroblasts and periodontal ligament cells. J Periodontol 92(11):1635–1645. https://doi.org/10.1002/JPER.20-0670
Musumeci G, Castorina A, Magro G, Cardile V, Castorina S, Ribatti D (2015) Enhanced expression of CD31/platelet endothelial cell adhesion molecule 1 (PECAM1) correlates with hypoxia inducible factor-1 alpha (HIF-1α) in human glioblastoma multiforme. Exp Cell Res 339(2):407–416. https://doi.org/10.1016/j.yexcr.2015.09.007
Nauta TD, Duyndam MC, Weijers EM, van Hinsbergh VM, Koolwijk P (2016) HIF-2α expression regulates sprout formation into 3D fibrin matrices in prolonged hypoxia in human microvascular endothelial cells. PLoS One 11(8):e0160700. https://doi.org/10.1371/journal.pone.0160700
Nauta TD, van den Broek M, Gibbs S, van der Pouw-Kraan TC, Oudejans CB, van Hinsbergh VW, Koolwijk P (2017) Identification of HIF-2α-regulated genes that play a role in human microvascular endothelial sprouting during prolonged hypoxia in vitro. Angiogenesis 20(1):39–54. https://doi.org/10.1007/s10456-016-9527-4
Navarro FP, Fares RP, Sanchez PE, Nadam J, Georges B, Moulin C, Morales A, Pequignot JM, Bezin L (2008) Brain heparanase expression is up-regulated during postnatal development and hypoxia-induced neovascularization in adult rats. J Neurochem 105(1):34–45. https://doi.org/10.1111/j.1471-4159.2007.05116.x
Norman JT, Clark IM, Garcia PL (2000) Hypoxia promotes fibrogenesis in human renal fibroblasts. Kidney Int 58(6):2351–2366. https://doi.org/10.1046/j.1523-1755.2000.00419.x
Osawa T, Ohga N, Akiyama K, Hida Y, Kitayama K, Kawamoto T, Yamamoto K, Maishi N, Kondoh M, Onodera Y, Fujie M, Shinohara N, Nonomura K, Shindoh M, Hida K (2013) Lysyl oxidase secreted by tumour endothelial cells promotes angiogenesis and metastasis. Br J Cancer 109(8):2237–2247. https://doi.org/10.1038/bjc.2013.535
Ottino P, Finley J, Rojo E, Ottlecz A, Lambrou GN, Bazan HE, Bazan NG (2004) Hypoxia activates matrix metalloproteinase expression and the VEGF system in monkey choroid-retinal endothelial cells: involvement of cytosolic phospholipase A2 activity. Mol Vis 10:341–350
Paddenberg R, Faulhammer P, Goldenberg A, Kummer W (2006) Hypoxia-induced increase of endostatin in murine aorta and lung. Histochem Cell Biol 125(5):497–508. https://doi.org/10.1007/s00418-006-0158-5
Patel JI, Hykin PG, Gregor ZJ, Boulton M, Cree IA (2005) Angiopoietin concentrations in diabetic retinopathy. Br J Ophthalmol 89(4):480–483. https://doi.org/10.1136/bjo.2004.049940
Pietilä K, Jaakkola O (1984) Effect of hypoxia on the synthesis of glycosaminoglycans and collagen by rabbit aortic smooth muscle cells in culture. Atherosclerosis 50(2):183–190. https://doi.org/10.1016/0021-9150(84)90021-2
Radziwon-Balicka A, Ramer C, Moncada de la Rosa C, Zielnik-Drabik B, Jurasz P (2013) Angiostatin inhibits endothelial MMP-2 and MMP-14 expression: a hypoxia specific mechanism of action. Vasc Pharmacol 58(4):280–291. https://doi.org/10.1016/j.vph.2012.11.003
Rappu P, Salo AM, Myllyharju J, Heino J (2019) Role of prolyl hydroxylation in the molecular interactions of collagens. Essays Biochem 63(3):325–335. https://doi.org/10.1042/EBC20180053
Ricard-Blum S (2011) The collagen family. Cold Spring Harb Perspect Biol 3(1):a004978. https://doi.org/10.1101/cshperspect.a004978
Rodriguez D, Watts D, Gaete D, Sormendi S, Wielockx B (2021) Hypoxia pathway proteins and their impact on the blood vasculature. Int J Mol Sci 22(17):9191. https://doi.org/10.3390/ijms22179191
Rohwer N, Welzel M, Daskalow K, Pfander D, Wiedenmann B, Detjen K, Cramer T (2008) Hypoxia-inducible factor 1alpha mediates anoikis resistance via suppression of alpha5 integrin. Cancer Res 68(24):10113–10120. https://doi.org/10.1158/0008-5472.CAN-08-1839
Romero Y, Aquino-Gálvez A (2021) Hypoxia in cancer and fibrosis: part of the problem and part of the solution. Int J Mol Sci 22(15):8335. https://doi.org/10.3390/ijms22158335
Rosell-García T, Palomo-Álvarez O, Rodríguez-Pascual F (2019) A hierarchical network of hypoxia-inducible factor and SMAD proteins governs procollagen lysyl hydroxylase 2 induction by hypoxia and transforming growth factor β1. J Biol Chem 294(39):14308–14318. https://doi.org/10.1074/jbc.RA119.007674
Rozen-Zvi B, Hayashida T, Hubchak SC, Hanna C, Platanias LC, Schnaper HW (2013) TGF-β/Smad3 activates mammalian target of rapamycin complex-1 to promote collagen production by increasing HIF-1α expression. Am J Physiol Renal Physiol 305(4):F485–F494. https://doi.org/10.1152/ajprenal.00215.2013
Rzymski T, Petry A, Kračun D, Rieß F, Pike L, Harris AL, Görlach A (2012) The unfolded protein response controls induction and activation of ADAM17/TACE by severe hypoxia and ER stress. Oncogene 31(31):3621–3634. https://doi.org/10.1038/onc.2011.522
Sanaei-Ardekani M, Kamal S, Handy W, Alam S, Salaheldin A, Moore A, Movafagh S (2021) Suppression of collagen IV alpha-2 subunit by prolyl hydroxylase domain inhibition via hypoxia-inducible factor-1 in chronic kidney disease. Pharmacol Res Perspect 9(5):e00872. https://doi.org/10.1002/prp2.872
Saxena K, Jolly MK (2019) Acute vs. chronic vs. cyclic hypoxia: their differential dynamics, molecular mechanisms, and effects on tumor progression. Biomolecules 9(8):339. https://doi.org/10.3390/biom9080339
Schito L (2019) Hypoxia-dependent angiogenesis and lymphangiogenesis in cancer. Adv Exp Med Biol 1136:71–85. https://doi.org/10.1007/978-3-030-12734-3_5
Selvarajan S, Lund LR, Takeuchi T, Craik CS, Werb Z (2001) A plasma kallikrein-dependent plasminogen cascade required for adipocyte differentiation. Nat Cell Biol 3(3):267–275. https://doi.org/10.1038/35060059
Semenza GL (2007) Vasculogenesis, angiogenesis, and arteriogenesis: mechanisms of blood vessel formation and remodeling. J Cell Biochem 102(4):840–847. https://doi.org/10.1002/jcb.21523
Semenza GL (2012) Hypoxia-inducible factors in physiology and medicine. Cell 148(3):399–408. https://doi.org/10.1016/j.cell.2012.01.021
Senger DR, Davis GE (2011) Angiogenesis. Cold Spring Harb Perspect Biol 3(8):a005090. https://doi.org/10.1101/cshperspect.a005090
Shi L, Zhang N, Liu H, Zhao L, Liu J, Wan J, Wu W, Lei H, Liu R, Han M (2018) Lysyl oxidase inhibition via β-aminoproprionitrile hampers human umbilical vein endothelial cell angiogenesis and migration in vitro. Mol Med Rep 17(4):5029–5036. https://doi.org/10.3892/mmr.2018.8508
Shih YH, Chang KW, Chen MY, Yu CC, Lin DJ, Hsia SM, Huang HL, Shieh TM (2013) Lysyl oxidase and enhancement of cell proliferation and angiogenesis in oral squamous cell carcinoma. Head Neck 35(2):250–256. https://doi.org/10.1002/hed.22959
Skuli N, Monferran S, Delmas C, Favre G, Bonnet J, Toulas C, Cohen-Jonathan Moyal E (2009) Alphavbeta3/alphavbeta5 integrins-FAK-RhoB: a novel pathway for hypoxia regulation in glioblastoma. Cancer Res 69(8):3308–3316. https://doi.org/10.1158/0008-5472.CAN-08-2158
Skuli N, Majmundar AJ, Krock BL, Mesquita RC, Mathew LK, Quinn ZL, Runge A, Liu L, Kim MN, Liang J, Schenkel S, Yodh AG, Keith B, Simon MC (2012) Endothelial HIF-2α regulates murine pathological angiogenesis and revascularization processes. J Clin Invest 122:1427–1443. https://doi.org/10.1172/JCI57322
Smith HW, Marshall CJ (2010) Regulation of cell signalling by u-PAR. Nat Rev Mol Cell Biol 11(1):23–36. https://doi.org/10.1038/nrm2821
Stegen S, Laperre K, Eelen G, Rinaldi G, Fraisl P, Torrekens S, Van Looveren R, Loopmans S, Bultynck G, Vinckier S, Meersman F, Maxwell PH, Rai J, Weis M, Eyre DR, Ghesquière B, Fendt SM, Carmeliet P, Carmeliet G (2019) HIF-1α metabolically controls collagen synthesis and modification in chondrocytes. Nature 565(7740):511–515. https://doi.org/10.1038/s41586-019-0874-3
Sullivan R, Graham CH (2007) Hypoxia-driven selection of the metastatic phenotype. Cancer Metastasis Rev 26(2):319–331. https://doi.org/10.1007/s10555-007-9062-2
Teodoro JG, Parker AE, Zhu X, Green MR (2006) p53-mediated inhibition of angiogenesis through up-regulation of a collagen prolyl hydroxylase. Science 313(5789):968–971. https://doi.org/10.1126/science.1126391
Uchiyama T, Kurabayashi M, Ohyama Y, Utsugi T, Akuzawa N, Sato M, Tomono S, Kawazu S, Nagai R (2000) Hypoxia induces transcription of the plasminogen activator inhibitor-1 gene through genistein-sensitive tyrosine kinase pathways in vascular endothelial cells. Arterioscler Thromb Vasc Biol 20(4):1155–1161. https://doi.org/10.1161/01.atv.20.4.1155
Umana-Diaz C, Pichol-Thievend C, Marchand MF, Atlas Y, Salza R, Malbouyres M, Barret A, Teillon J, Ardidie-Robouant C, Ruggiero F, Monnot C, Girard P, Guilluy C, Ricard-Blum S, Germain S, Muller L (2020) Scavenger receptor cysteine-rich domains of Lysyl oxidase-Like2 regulate endothelial ECM and angiogenesis through non-catalytic scaffolding mechanisms. Matrix Biol 88:33–52. https://doi.org/10.1016/j.matbio.2019.11.003
Valapala M, Thamake SI, Vishwanatha JK (2011) A competitive hexapeptide inhibitor of annexin A2 prevents hypoxia-induced angiogenic events. J Cell Sci 124(Pt 9):1453–1464. https://doi.org/10.1242/jcs.079236
Valle-Tenney R, Rebolledo D, Acuña MJ, Brandan E (2020) HIF-hypoxia signaling in skeletal muscle physiology and fibrosis. J Cell Commun Signal 14(2):147–158. https://doi.org/10.1007/s12079-020-00553-8
van der Slot AJ, Zuurmond AM, van den Bogaerdt AJ, Ulrich MM, Middelkoop E, Boers W, Karel Ronday H, DeGroot J, Huizinga TW, Bank RA (2004) Increased formation of pyridinoline cross-links due to higher telopeptide lysyl hydroxylase levels is a general fibrotic phenomenon. Matrix Biol 23(4):251–257. https://doi.org/10.1016/j.matbio.2004.06.001
van Hinsbergh VW, Koolwijk P (2008) Endothelial sprouting and angiogenesis: matrix metalloproteinases in the lead. Cardiovasc Res 78(2):203–212. https://doi.org/10.1093/cvr/cvm102
van Vlimmeren MA, Driessen-Mol A, van den Broek M, Bouten CV, Baaijens FP (2010) Controlling matrix formation and cross-linking by hypoxia in cardiovascular tissue engineering. J Appl Physiol 109(5):1483–1491. https://doi.org/10.1152/japplphysiol.00571.2010
Walton HL, Corjay MH, Mohamed SN, Mousa SA, Santomenna LD, Reilly TM (2000) Hypoxia induces differential expression of the integrin receptors alpha(vbeta3) and alpha(vbeta5) in cultured human endothelial cells. J Cell Biochem 78(4):674–680. https://doi.org/10.1002/1097-4644(20000915)78:4<674::aid-jcb16>3.0.co;2-g
Wang GL, Semenza GL (1995) Purification and characterization of hypoxia-inducible factor 1 (∗). J Biol Chem 270(3):1230–1237. https://doi.org/10.1074/jbc.270.3.1230
Wang GL, Jiang BH, Rue EA, Semenza GL (1995) Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS heterodimer regulated by cellular O2 tension. Proc Natl Acad Sci U S A 92(12):5510–5514. https://doi.org/10.1073/pnas.92.12.5510
Wang F, Wan J, Li Q, Zhang M, Wan Q, Ji C, Li H, Liu R, Han M (2017) Lysyl oxidase is involved in synovial hyperplasia and angiogenesis in rats with collagen-induced arthritis. Mol Med Rep 16(5):6736–6742. https://doi.org/10.3892/mmr.2017.7436
Wang Y, Mirza S, Wu S, Zeng J, Shi W, Band H, Band V, Duan B (2018) 3D hydrogel breast cancer models for studying the effects of hypoxia on epithelial to mesenchymal transition. Oncotarget 9(63):32191–32203. https://doi.org/10.18632/oncotarget.25891
Warnecke C, Griethe W, Weidemann A, Jürgensen JS, Willam C, Bachmann S, Ivashchenko Y, Wagner I, Frei U, Wiesener M, Eckardt KU (2003) Activation of the hypoxia-inducible factor-pathway and stimulation of angiogenesis by application of prolyl hydroxylase inhibitors. FASEB J 17(9):1186–1188. https://doi.org/10.1096/fj.02-1062fje
Wei X, Chen Y, Jiang X, Peng M, Liu Y, Mo Y, Ren D, Hua Y, Yu B, Zhou Y, Liao Q, Wang H, Xiang B, Zhou M, Li X, Li G, Li Y, Xiong W, Zeng Z (2021) Mechanisms of vasculogenic mimicry in hypoxic tumor microenvironments. Mol Cancer 20(1):7. https://doi.org/10.1186/s12943-020-01288-1
Weigand JE, Boeckel JN, Gellert P, Dimmeler S (2012) Hypoxia-induced alternative splicing in endothelial cells. PLos One 7(8):e42697. https://doi.org/10.1371/journal.pone.0042697
Xiong A, Liu Y (2017) Targeting hypoxia inducible factors-1α As a novel therapy in fibrosis. Front Pharmacol 8:326. https://doi.org/10.3389/fphar.2017.00326
Xiong G, Stewart RL, Chen J, Gao T, Scott TL, Samayoa LM, O'Connor K, Lane AN, Xu R (2018) Collagen prolyl 4-hydroxylase 1 is essential for HIF-1α stabilization and TNBC chemoresistance. Nat Commun 9(1):4456. https://doi.org/10.1038/s41467-018-06893-9
Yamamoto-Rodríguez L, Zarbin MA, Casaroli-Marano RP (2020) New frontiers and clinical implications in the pathophysiology of age-related macular degeneration. Med Clin 154(12):496–504. https://doi.org/10.1016/j.medcli.2020.01.023
Yamauchi M, Sricholpech M (2012) Lysine post-translational modifications of collagen. Essays Biochem 52:113–133. https://doi.org/10.1042/bse0520113
Yanagisawa H, Yokoyama U (2021) Extracellular matrix-mediated remodeling and mechanotransduction in large vessels during development and disease. Cell Signal 86:110104. https://doi.org/10.1016/j.cellsig.2021.110104
Yang M, Liu J, Wang F, Tian Z, Ma B, Li Z, Wang B, Zhao W (2019) Lysyl oxidase assists tumor-initiating cells to enhance angiogenesis in hepatocellular carcinoma. Int J Oncol 54(4):1398–1408. https://doi.org/10.3892/ijo.2019.4705
Zhu Y, Wang Y, Jia Y, Xu J, Chai Y (2019) Roxadustat promotes angiogenesis through HIF-1α/VEGF/VEGFR2 signaling and accelerates cutaneous wound healing in diabetic rats. Wound Repair Regen 27(4):324–334. https://doi.org/10.1111/wrr.12708
Zuazo-Gaztelu I, Casanovas O (2018) Unraveling the role of angiogenesis in cancer ecosystems. Front Oncol 8:248. https://doi.org/10.3389/fonc.2018.00248
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Karavasili, K., Koolwijk, P. (2023). Hypoxia: A Potent Regulator of Angiogenesis Through Extracellular Matrix Remodelling. In: Papadimitriou, E., Mikelis, C.M. (eds) Matrix Pathobiology and Angiogenesis. Biology of Extracellular Matrix, vol 12. Springer, Cham. https://doi.org/10.1007/978-3-031-19616-4_8
Download citation
DOI: https://doi.org/10.1007/978-3-031-19616-4_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-19615-7
Online ISBN: 978-3-031-19616-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)