
Abstract
Ultrasound (US) has played a role in MSK evaluation for over 50 years and has several advantages over other imaging modalities. Recent progress has expanded the scope of US in sports medicine to include other organ systems. US is an ideal imaging modality for injury evaluations at sporting events for its portability. Further, new programs enable physiologic and biological assessment of injured tissues to make return-to-play decisions. Its use in procedural guidance has improved the accuracy of existing office-based procedures while also opening the door for US-based micro-invasive surgical interventions. Ongoing research continues to expand the diagnostic and interventional capabilities of US, broadening the indications of US in the hands of skilled sports medicine physicians.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Elastography
- Hernia
- FAST
- Endofibrosis
- Nerve
- Neuropathy
- Exercise-induced laryngeal obstruction
- EILO
- ESCAPE
- Fracture
Introduction
The history of ultrasound (US) in sports medicine dates back to the 1940s when it was first used as a diagnostic imaging modality by Karl Dussik to image brain tumors [1]. That application expanded into musculoskeletal (MSK) evaluation in 1958 when US was used to measure the attenuation of articular and periarticular tissues [2]. The technology and image quality further improved over the following decade, eventually leading to a paper documenting the ability to differentiate a Baker’s cyst from thrombophlebitis [3]. From here, the use of US in athletes expanded beyond the MSK system. Echocardiography was first used in the 1970s to measure left ventricular end-diastolic volume and ventricular wall thickness and mass in an effort to diagnose athletic heart syndrome [4].
Ultrasound’s progress was eclipsed in the 1970s and 1980s by computed tomography (CT) and magnetic resonance imaging (MRI), both of which became the advanced imaging technologies of choice for the evaluation of MSK and sports medicine conditions. CT was most useful in identifying bony pathology typically missed on plain films including stress fractures and small intra-articular fractures. MRI became popular for its ability to delineate soft tissues better than any existing imaging technique [5,6,7,8,9,10,11,12]. Despite its early promise, the subpar spatial resolution and operator dependency of US during this period relegated it to a few specific applications outside of the MSK system.
However, further technological progress in the 1980s and 1990s led to renewed interest in applying US to the MSK system, particularly for muscle, ligament, and tendon pathology [13,14,15,16]. Rheumatologists were the first to widely adopt diagnostic US use and were the first to deploy it for procedural guidance during joint aspiration [17, 18]. Orthopedic surgeons soon recognized the value of US after several papers correlated sonographically identified rotator cuff pathology with arthrography [19] and postoperative function [20]. Subsequent studies documenting the superiority of US compared to standard radiographs in the diagnosis of transient synovitis of the hip in children also strengthened the case for its utility [21, 22].
The publication of the first MSK US textbooks in the 1990s led to broader awareness of the ways US could be used for diagnostic evaluation and interventional procedures in sports medicine and orthopedics [23, 24]. US was subsequently shown to make injections more accurate than similar injections done with landmark guidance for most peripheral joint and soft tissue injections, further boosting its popularity [25]. With increased interest, US imaging evolved in the early twenty-first century as spatial resolution improved and portability increased [26]. Between 2000 and 2009, there was a 316% increase in procedural use of MSK US [27].
Today, the term “sports US” refers to the use of US for both diagnostic and therapeutic indications in sports medicine and includes the diagnostic and interventional use of US for MSK conditions as well as the diagnostic use of US to evaluate non-MSK conditions in athletes [28,29,30,31,32]. The recent development of US-guided procedures indicates the ongoing interest in applying this technology to improve upon current procedural techniques [33,34,35]. This chapter will describe the current utility of diagnostic and interventional US in sports medicine. It will also review uses of US in procedures and emerging technologies addressing current limitations in US imaging.
Diagnostic Ultrasound in Sports Medicine
Advantages of Diagnostic Ultrasound in Sports Medicine
There are a number of advantages of diagnostic US compared to other imaging modalities such as x-ray, MRI, and CT (see Table 21.1). With increasing portability, US can be brought to the training rooms, injury clinics, or even athletic events to assist in a timely diagnosis and proper triaging for sports injuries from every organ system [36,37,38,39,40]. Advances in telecommunications, such as fifth-generation (5G) wireless, allow ultrasound scanning to be remotely guided by an experienced practitioner and real-time dynamic imaging for faster diagnosis [41, 42].
US also offers high spatial resolution of soft tissue and neurovascular pathology. A 10 Mhz US probe can achieve axial in-plane resolution of approximately 150 μm, significantly more than the resolution of common clinical MRI machines which only reach 450 μm [43]. One study compared MRI and US in detecting peripheral nerve pathology and found better sensitivity with US, while the two were equivalent in specificity [44]. Because of this high resolution, ultrasound has proven to be a cost-effective diagnostic tool for sports injuries, and if utilized for appropriate indications, it has been shown to potentially save billions of dollars [45,46,47,48,49]. Its real-time assessment allows for dynamic imaging of pathology that may be missed using static imaging such as CT or MRI [50, 51]. It has the benefit of providing imaging of the healthy contralateral side providing a control for comparison [52, 53].
Chronic musculoskeletal diseases such as knee OA, which are more prevalent in athletes, often require imaging to assess severity of disease [54, 55]. As the association of ionizing radiation exposure and cancer risk has become better understood, the potential for significant radiation exposure over athletes’ lifetimes has raised concern [56,57,58]. Ultrasound can provide equivalent imaging for the assessment of disease progression, such as OA-associated pathology, without any of the risks from ionizing radiation exposure [59,60,61].
Due to higher prevalence of chronic musculoskeletal diseases, athletes are more prone to joint replacement during their lifetime than in the general population [55, 62, 63]. Evaluation of peri-prosthetic soft tissue can be difficult using CT or MRI due to metal artifact obscuring structures [64, 65]. US is effective in detecting peri-prosthetic infections which are a leading cause of cause for revision of THAs and TKAs [66, 67]. Early identification of these infections to avoid revision due to septic loosening could reduce risk of prolonged postoperative pain due to septic joint replacement [68].
Ultrasound has the advantage of avoiding interference from motion artifact which are noted issues with CT and MRI assessment [69, 70]. It also has superior vascular imaging capability such as color and power Doppler which allow the identification of pathology such as muscle, tendon, and bone injury and permit the identification of vessels during ultrasound-guided procedures to limit complications [71, 72]. Neovascularization has been identified as a key finding in tendinosis, and advances in ultrasound technology such as superb microvascular imaging (SMI) have improved the identification of this pathology compared to color or power Doppler [73,74,75]. Other advances such as elastography or tissue characterization go beyond standard imaging with B mode and allow for a more thorough assessment of mechanical properties of soft tissues [76, 77].
Broad and Expanding Applicability of US Beyond Traditional MSK Applications
As discussed elsewhere in this book, US can be used to evaluate ligaments, muscles, nerves, tendons, and vessels at the point of care [78,79,80]. However, the use of US in the diagnosis and treatment of athletes has expanded beyond the MSK system. In a study of ultrasonography at the 2008 Beijing Olympics, US was found to be the imaging modality of choice in the Olympic village polyclinic and was most commonly used to evaluate abdominal complaints (41% of US exams performed) [81]. US’s portability, real-time results, and accuracy made it an ideal tool for initial imaging at a large sporting event where transportation to local imaging facilities may be complicated or lead to delayed diagnosis. The use in imaging abdominal complaints highlights the technology’s utility beyond evaluation of the MSK system.
US in Sports Medicine: Organ System Evaluation
Significant literature exists regarding the use of US for the evaluation of sports-related injuries. This section will highlight relevant organ systems and diagnoses for which US evaluation can be used in sports medicine and will include a discussion of the ways in which US evaluation can facilitate a more rapid and accurate diagnosis.
HEENT
Ocular Evaluation
Ocular examination with US is routinely used by radiologists, ophthalmologists, and emergency medicine physicians as a rapid, radiation-free, and accurate way to evaluate structures of the eye [82, 83]. Sports-related eye injuries account for approximately 1.5% of all sports injuries with higher rates in baseball, basketball, and racquet sports [84,85,86,87]. For some athletes, these injuries can lead to long-term vision loss [88]. US can serve as a triage tool on the sidelines to screen for severe eye injuries after trauma and is not hindered by hyphema or lid edema often present in these injuries.
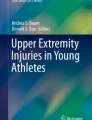
Frequent pathologies seen in sports settings amenable to US evaluation include retinal detachment, retinal hemorrhage, and lens dislocation or subluxation (Fig. 21.1). Retinal detachment requires rapid diagnosis and referral for intervention and can be readily visualized with US89. Untreated, symptomatic retinal detachment can progress to complete detachment within days and can result in complete loss of vision. Given the low incidence of retinal detachment among eye injuries in athletes, US is especially useful for ruling out a detachment in the setting of acute vision changes [90,91,92]. Research has shown that non-radiology specialists can be trained to reliably use US for the identification of retinal detachment with sensitivity ranging from 97 to 100% and specificity from 83 to 100% [89, 93, 94]. Retinal hemorrhage and lens dislocation or subluxation can also be visualized during the same examination, facilitating rapid triage for emergent care and early warning to the emergency department if urgent ophthalmologic evaluation is needed [82].

Ocular US: globe on the left reveals a detached retina which is visualized as a hyperechoic line anterior to the posterior wall; the right is normal
Ocular US can also be used for an assessment of elevated intracranial pressure (ICP) after head trauma. The optic nerve sheath is contiguous with the dura mater and expands when ICP is elevated. This expansion can be seen on US [95, 96]. A meta-analysis reviewing studies that compared optic nerve sheath diameters on US to CTs with findings suggestive of intracranial compression suggested a cutoff of sheath diameter of 5mm in adults was 95.6% sensitive and 92.3% specific for elevated ICP [97].
Exercise-Induced Laryngeal Obstruction
Exercise-induced laryngeal obstruction (EILO), often referred to as vocal fold dysfunction, is an uncommon and likely underrecognized cause of breathing complaints in sport [98, 99]. The precise etiology is not well understood and is believed to have multiple independent causes that result in partial obstruction of the airway during exercise [99,100,101]. The presenting symptoms of EILO are very similar to those of exercise-induced asthma, resulting in frequent misdiagnosis [99, 101]. These symptoms include difficulty breathing, chest discomfort, wheezing, dry cough, and a feeling of throat constriction that doesn’t respond to standard asthma treatment [102]. Fiber-optic video laryngoscopy is the gold standard for diagnosis, but requires specialized clinical space and equipment, which is often not available to sports medicine physicians, especially when symptoms are occurring [101]. Since symptoms may be context dependent and are transient, US offers the possibility of sideline evaluation and possible diagnosis while the athlete is symptomatic. One study demonstrated the ability to differentiate paradoxical vocal fold motion from normal vocal fold motion with US, but additional research is needed for confirmation [101].
Chest
Echocardiography
While rare, the most common cause of death in sport is sudden cardiac death [103]. These deaths are often preventable with adequate screening, but the type of screening and population to screen is debated [104, 105]. The history and physical exam (H&P) with or without electrocardiogram (EKG) are typically used as screening tools in the preparticipation evaluation (PPE) of athletes, but their effectiveness in disease identification is questioned [106]. A comprehensive review by Harmon et al. found that the pooled sensitivity for the history was 20% (range 7–44%) and 9% for the physical exam (range 3–24%). Both were more specific at 94% and 97%, respectively, but sole use of the H&P will likely omit athletes potentially at risk [106]. While EKG is both sensitive and specific at 94% (79–98%) and 93% (90–96%), respectively, it lacks portability and comes at a monetary cost [106]. Additionally, EKG may have a high false-positive rate, partly as a result of physiologic cardiac changes that occur in athletes and the variability in criteria used to define pathology in those settings [106, 107]. These false positives can exclude healthy athletes from play while subjecting them to prolonged and expensive workups [108, 109].
US has a long history of use in cardiology settings. While current data is insufficient to report well-defined sensitivity and specificity, some research has shown that echocardiography combined with EKG might decrease the false-positive rate and reduce the need for subsequent cardiology referrals [110,111,112]. One study of 3100 male soccer players who were screened with echocardiography found several cardiac anomalies missed by H&P and EKG, although most were mild valvular abnormalities with unclear clinical significance [113]. Severe abnormalities were rare in the study, and all that were present had an abnormal EKG [113].
The Early Screening for Cardiac Abnormalities with Preparticipation Echocardiography (ESCAPE) protocol was developed specifically to screen for the most concerning cardiac anomalies in athletes using US. It examines the end-diastolic interventricular septal thickness, left ventricular diameter, left ventricular wall thickness, and aortic root diameter [110, 114, 115]. Initial studies on this protocol have shown similar rates for the detection of anomalies between cardiologists and non-cardiologists [110, 116]. The role of screening echocardiography is still being debated and should not replace the H&P or EKG until more comprehensive and systematic research has been performed.
Rib Fracture and Pneumothorax
The etiology of chest pain after trauma can be difficult to determine acutely. Blunt trauma to the thorax can result in rib fracture, which is conventionally diagnosed with radiographs. However, US has been shown to be equivalent or superior to radiographs for rib fracture diagnosis, and its portability allows for rapid evaluation on the sideline or in the training room [117, 118]. On US evaluation, fracture is seen as a discontinuity in the usually smooth, hyperechoic contour of the rib [117].
Pneumothorax is a common sequelae of rib fractures and can be evaluated and diagnosed with US using several techniques [119]. The absence of lung sliding, absence of B lines, and presence of A lines indicate pneumothorax [119,120,121] (US findings described in Table 21.2) (Fig. 21.2). The absence of lung sliding and presence of A lines have a sensitivity and specificity of 94 and 95%, respectively, for the diagnosis of pneumothorax [119]. Evaluation can be performed by non-radiologists where x-ray equipment may not be readily available or ambient noise may be too loud to permit auscultation [121,122,123]. The diagnostic sensitivity and specificity of US evaluation are superior to upright anterior to posterior chest x-ray and similar to CT scan of the chest, which is the gold standard for the diagnosis of pneumothorax [90, 124]. The portability of US allows for point-of-care pneumothorax evaluation and rapid referral for care if present.

Lung US: comet tail artifact in the upper right extending downward from the pleura; A lines are notable throughout the image; no B lines are present
Abdomen
Extended FAST (eFAST)
The Focused Assessment with Sonography in Trauma (FAST) was developed in the 1990s to identify abnormal intraabdominal fluid or solid organ injury in the setting of blunt thoracoabdominal trauma [125, 126]. It includes evaluation for hemoperitoneum, liver injury, hemopericardium, pericardial or cardiac injury, and splenic or renal injury and should take the operator 5 minutes or less to perform [125, 127, 128]. The FAST examination was expanded to include the evaluation for pneumothorax and hemothorax and termed the extended FAST (or eFAST) examination. These exams can be performed rapidly, help to triage athletes, do not increase the time to intervention in the emergency department, and may decrease the number of missed life-threatening injuries [127]. However, further research is needed to support its use in sports-specific environments [29].
Splenomegaly Monitoring in Mononucleosis
Infectious mononucleosis is the clinical manifestation of Epstein-Barr viral infection. While common symptoms include fatigue and malaise, transient splenomegaly is the most concerning effect of mononucleosis for athletes [129, 130]. Splenic rupture is a rare, but potentially fatal, complication of return to sport in the setting of splenomegaly [130]. While contact sports are most commonly associated with reports of splenic rupture, rupture can rarely occur with significant Valsalva in non-contact sports [130]. As a result, athletes are often prevented from returning to play for 3 to 4 weeks after disease onset to ensure resolution of their transient splenomegaly [130].
US evaluation of the spleen has been proposed as a possible method to monitor splenomegaly and determine timing for safe return to play. However, there is significant interindividual sonographic variability of spleen size, making normal values difficult to establish [130, 131]. Without consistent baseline measurements, true splenomegaly is difficult to define and cannot guide return-to-play decisions as a result. It is possible that baseline measurements followed by serial scans would prove useful, but this is resource-intensive and likely impractical in many settings. More research is needed to determine the role of US in the evaluation of splenomegaly.
Abdominal Muscle Evaluation
Abdominal muscle pathology can often be visualized with US. Pathology can include herniation of abdominal musculature through its fascial plane or injury to the musculature itself with a resulting defect and herniation of fat or abdominal contents. Spigelian hernias are rare, occur at the edge of the rectus abdominis along the linea semilunaris, and may be difficult to identify with static imaging modalities [132, 133]. These hernias commonly contain fat, but can contain bowel and are seen on US protruding ventrally through the linea semilunaris with Valsalva [133]. Epigastric, umbilical, and incisional hernias can all be visualized as an outright defect in the abdominal wall or with ventral protrusion of abdominal contents with Valsalva [134]. Care should be taken to apply light transducer pressure when attempting to visualize herniation in these areas since it may be prevented or reduced with heavy pressure [135].
Injury to the abdominal musculature can also be visualized with US, including injury to the rectus abdominis, internal and external obliques, and transversus abdominis [136,137,138,139]. These injuries are often seen in throwers, who generate significant rotational forces in order to properly execute the throw [140]. These injuries appear on US as disruption of the fibrillar architecture of the muscle and areas of hypoechogenicity at the site of pain and are thought to represent hemorrhage, edema, and muscle fiber disruption [137].
Inguinal and Femoral Hernia Evaluation
US evaluation is often used to visualize hernias because they can be dynamically imaged during provocation maneuvers. Hernias may cause diffuse and nonspecific pain in the groin and lower abdomen, making it difficult to differentiate from other pain generators and difficult to diagnose based on physical exam alone [141, 142]. Inguinal hernias are most common in men and can be either indirect or direct [143]. Indirect hernias involve herniation of abdominal contents through the deep inguinal ring and are visualized on dynamic US as tissue extension lateral to the external iliac vessels or inferior epigastric vessels [133, 144]. Direct hernias involve herniation of abdominal contents directly through Hesselbach’s triangle in the abdominal wall, and dynamic US evaluation will show abnormal anterior movement of tissue medial to the inferior epigastric vessels [133, 144].
Femoral hernias are the most common type of hernia in women [145]. They occur below the level of the inguinal ligament, and dynamic US evaluation will reveal superior to inferior herniation of abdominal contents into the femoral canal medial to the femoral neurovasculature and ventral to the pectineus muscle [133, 144].
Hernia Mimickers: Groin Pain in the Athlete
Evaluation of groin pain in the athlete should include examination of pain generators in the area, particularly if a true hernia is absent. “Sports hernia” and “athletic pubalgia” are ambiguous terms often used to describe groin pain in athletes and generally do not reflect a hernia of any kind. Instead, they encompass the broad differential of gastrointestinal, MSK, or neurologic pathologies that may cause groin pain, including intraarticular and periarticular hip joint pathology, musculotendinous injuries (including abdominals, hip adductors, and iliopsoas), inflammatory bowel disease, or nerve entrapment syndromes [146, 147]. US can help narrow this broad differential diagnosis through its ability to evaluate the abdominal wall musculature (as described above), the rectus abdominis/adductor plate, and the adductor tendon origin dynamically at high resolution [141, 146] [148]. Additionally, the iliopsoas can be scanned dynamically to evaluate for snapping iliopsoas tendon [149, 150]. Nerves that can contribute to groin pain, including genitofemoral nerve, obturator nerve, or medial femoral cutaneous nerve, can also be evaluated [151,152,153].
MSK
US evaluation of the MSK system is covered in extensive detail in Chaps. 5, 6, 7, 8, 9, 10, and 11 of this book. US is effective for the evaluation of a wide variety of MSK complaints, including major joints, muscles, tendons, and ligaments in the extremities [28].
Peripheral Nerve Injuries
Peripheral nerve injuries are believed to be rare in athletes but may just be underrecognized by clinicians [154]. Peripheral nerve injuries can contribute to significant pain and inability to return to play [155, 156]. While electrodiagnostic testing (EDX) is the most common method to localize and determine the nature of these lesions, diagnosis is often delayed by the one to several weeks it takes for EDX to be positive [157]. During this time, athletes may be symptomatic and unable to return to play without an accurate diagnosis to guide effective treatment. While US is not a substitute for EDX, it can assist in localizing nerve injury and facilitate diagnosis and early management [158, 159]. The development of high-resolution US (HRUS), typically defined as 12 MHz or greater depending on the depth of evaluation, allows for the evaluation of nerve or fascicle enlargement indicating compression or irritation and visualization of small nerves that would be difficult or impossible to evaluate with EDX and that may not be adequately visualized on MRI [158, 160,161,162,163,164]. US examination is also less painful than EDX testing and may be better tolerated than EDX. Finally, US can supplement EDX since EDX is a physiologic test that evaluates the strength and speed of nerve conductions, while US evaluates other characteristics such as morphology of the nerve and nerve fascicles or nerves’ relationship to surrounding structures that might contribute to nerve irritation [165,166,167,168,169,170,171,172].
Characteristics of nerve injury seen on US include increased nerve or fascicle cross-sectional area due to edema, increased connective tissue formation from scarring, thickened and hyperechoic epineurium, or a hypoechoic internal appearance [169, 173, 174]. A study of nerve characteristics in peripheral nerve compression found increased transverse cross-sectional area (CSA) was most reliable for the diagnosis of nerve injury [175]. Several neuropathies that can be identified on US are described below, but this is not a comprehensive list, and research on peripheral nerve evaluation with US is ongoing.
Median Nerve
Carpal tunnel syndrome (CTS) is the most common mononeuropathy in the general population and is also common among wheelchair athletes [176, 177]. US has been used in the diagnosis of CTS and has shown sensitivity and specificity similar to EDX in several studies while also allowing immediate therapeutic injection or US-guided transverse carpal ligament release [178,179,180,181,182,183]. CSA of the median nerve at the inlet of the carpal tunnel has been found to be most sensitive and specific in diagnosing CTS [184]. While normal nerve size can vary and exact cutoffs are still debated, median nerve CSA between 9.0 and 12.6mm2 measured at the inlet has been shown to have sensitivity of 81% and specificity of 84% [184]. The color Doppler, power Doppler sonography, and contrast-enhanced ultrasonography can be used to identify median nerve hyperemia in the acute stage of CTS [185,186,187]. Superb microvascular imaging (SMI) is a novel technology which allows improved visualization of flow of both small and large vessels without requiring contrast enhancement and may be more sensitive to detecting blood flow changes due to CTS [188, 189].
Ulnar Nerve
The second most common upper extremity neuropathy is ulnar entrapment, often at the ulnar groove of the cubital tunnel, less frequently caused by the humeroulnar arcade [190]. This occurs with compression or recurrent subluxation of the nerve. While entrapment at the elbow occurs most commonly in baseball players, it can occur at the hand or wrist, especially in Guyon’s canal between the pisiform and the hook of hamate in wheelchair athletes, cyclists, and skiers [191, 192]. While EDX remains the gold standard for the localization of ulnar neuropathy, diagnostic accuracy improves when US is performed concomitantly [193, 194]. The normal ulnar nerve size varies between individuals and anatomic location, but some suggest a cutoff of 10 mm2 or greater as a diagnostic of cubital tunnel syndrome [195]. One study of patients in whom EDX was unsuccessful in localization found all injury locations were identifiable with HRUS [196].
Sciatic Nerve Branches
The common fibular nerve is frequently injured through direct trauma in football, hockey, and soccer players as it is superficial and prone to trauma at the lateral knee near the fibular head [197]. It is also susceptible to repetitive stress in runners [198, 199]. The tibial nerve can be injured in combination with the fibular nerve in acute ligamentous knee injuries, dislocations, fractures, or entrapment in tarsal tunnel syndrome at the medial ankle [200]. Both nerves can be visualized at the posterior distal thigh and can be traced to determine if and where injury occurred, providing diagnostic value comparable to that of MRI [201,202,203,204,205].
Lateral Femoral Cutaneous Nerve
Meralgia paresthetica, or neuropathy of the lateral femoral cutaneous nerve, is another commonly discussed focal mononeuropathy described in gymnasts, baseball players, and soccer players [206,207,208,209,210]. Diagnosis of this injury with EDX is possible, but can be technically difficult and may be significantly limited by body habitus [211]. Multiple reports have demonstrated HRUS is useful in identifying nerve entrapment at the lateral end of the inguinal ligament and for performing guidance diagnostic blocks and pain relief [212, 213].
Brachial Plexus
The brachial plexus is a common area for neuropathic injury in sports, especially those involving blunt trauma [214]. While most brachial plexus injuries are “stingers” that cause transient motor and sensory symptoms, others like neurogenic thoracic outlet syndrome (nTOS) result can also result in injuries to brachial plexus structures [215]. nTOS is the most common type of thoracic outlet syndrome comprising more than 95% of cases and can result from cervical trauma or from repetitive overhead activities that result in relative hypertrophy of muscles such as the pectoralis minor that can compress the brachial plexus and cause symptoms consistent with lower trunk brachial plexopathy [216]. While still under debate, US may be useful in identifying anomalous fibromuscular bands, sometimes referred to as “Roos ligaments,” compressing the lower trunk of the brachial plexus and causing nTOS [217]. It can also be useful in evaluating pectoral muscles for compression and tension placed upon the medial and lateral cord [218, 219]. Nerve compression between the clavicle, first rib, and scalene muscles due to muscle hypertrophy can cause brachial plexus compression and occurs more frequently among overhead athletes compared to the general population [220]. Ultrasound can identify the entrapment and guide anesthetic injection to the anterior scalene muscle to promote relaxation which correlates with good surgical outcomes [221, 222]. EDX can identify lesions that result in prolonged symptoms, but abnormalities will only appear after several weeks of persistent symptoms. US is capable of immediately visualizing nerve roots from the vertebral foramina through the trunks, divisions, cords, and branches to the axillary region, potentially providing earlier visualization of significant pathology and more rapid subsequent intervention although the clavicle can interrupt visualization from the supraclavicular area to the subpectoral area [223].
Vascular Injuries
While vascular injuries are uncommon in sports, they can cause significant symptoms in all extremities and should be considered when claudication symptoms are present. Vascular causes of exertional lower leg pain include external iliac artery endofibrosis and popliteal artery entrapment syndrome. External iliac artery endofibrosis results from intimal fibrosis of the arterial wall resulting in progressive stenosis and subsequent ischemic pain during exercise [224]. It is typically seen in endurance athletes such as cyclists and marathon runners [225]. Untreated, endofibrosis can lead to arterial dissection or thrombosis [226, 227]. US can be used to identify endofibrotic lesions, which appear as a segmental thickening of the intimal arterial wall with increased echogenicity of the arterial wall [228]. Doppler studies are normal at rest but show a decreased ankle brachial index (ABI) following exercise [229].
Popliteal artery entrapment occurs due to the compression of the artery by the anatomy of the gastrocnemius or popliteus muscles or dynamic compression by the soleus and can cause claudication symptoms [230, 231]. If undiagnosed, it can progress functional occlusion during activity, aneurysm, or thrombosis [232]. According to a meta-analysis, US Doppler ABI has a sensitivity of 90%, but specificity data is limited and may result in a high number of false-positive sonographic findings as a result [233]. This is supported by a study that found arterial occlusion induced with knee extension and subsequent plantarflexion and dorsiflexion in up to 50% of asymptomatic individuals [234].
Overhead athletes can also incur vascular injuries, especially aneurysms of the axillary artery and its branches including the posterior circumflex humeral artery (PCHA). This can lead to thrombosis or emboli causing subsequent digital ischemia [235,236,237]. Both symptomatic and asymptomatic volleyball players have been found to have PCHA aneurysms with a high prevalence of symptoms of digital ischemia thought to be secondary to microemboli [238, 239]. US has shown promise in the recognition of a PCHA aneurysm, which appears as a segmental vessel dilatation of greater than 50% compared to the closest normal-appearing vessel segment [240].
Overhead athletes are also susceptible to vasculogenic thoracic outlet syndrome, which can be of two forms: arterial thoracic outlet syndrome (aTOS) due to compression of the subclavian artery and venous thoracic outlet syndrome (vTOS) due to compression of the subclavian vein [241]. vTOS presents with fatigue or numbness that worsens when the arm is abducted and externally rotated [242, 243]. US has proven to have a role in diagnosis as episodes of occlusion have been identified by Doppler US, especially while observing during provocative maneuvers of the extremity [244, 245].
US in Sports Medicine: Physiologic Measures
US has been used experimentally to monitor physiologic parameters in an attempt to optimize training regimens and improve sports performance.
Muscle Glycogen
Evaluation of muscle glycogen content, an important source of energy for athletes, may help athletes evaluate their body’s response to training stimuli and assist with nutrition decisions. This might subsequently help prevent fatigue and overtraining syndrome while helping athletes and coaches optimize competition, training, recovery, and nutrition strategies [246,247,248]. Currently, muscle biopsy is the gold standard for determining glycogen quantity, but this is an invasive and uncomfortable procedure that is unrealistic for use during training. An application called MuscleSound (MuscleSound LLC, Denver, CO) has been developed using US to quantify and correlate the water content of muscles with glycogen content. Two studies funded by MuscleSound LLC have shown a strong correlation between muscle biopsy and MuscleSound measured glycogen content [249, 250]. An independently funded study found poor correlation between glycogen quantity measured by MuscleSound when compared to muscle biopsy [251]. More research is needed on the validity of this technology before the utility of noninvasive measure of muscle glycogen content can be established.
Body Composition
Many athletes, especially those in weight-sensitive sports, monitor and attempt to modulate body composition to improve performance [252]. US has been identified as a tool to assist in determining body fat measurements by measuring the thickness of adipose tissue [253]. This could replace the traditional use of fat calipers, which lack accuracy due to tissue compression during measurement [254, 255]. US was shown to have a better inter-rater reliability than the use of calipers for measuring body fat composition, but US scanning protocols for body composition are still under development [256].
Tendon Stiffness
Prior muscle or tendon injury has been identified as one of the major risk factors in the recurrence of injury and thus has been examined as a factor in determining return to play. Identifying weakened tissue is important in both diagnosing injury and determining timing for safe return to play without risking reinjury. Elastography estimates tissue hardness and can be used to estimate the mechanical properties of tissues. This may, in turn, help with early identification of at-risk individuals, outcome tracking, and treatment monitoring [257]. There are three types of elastography: acoustic radiation force impulse elastography, compression (strain) elastography, and shear wave elastography. Unfortunately, technical issues such as a lack of standardization and insufficient data on the characteristics of normal versus diseased tissues still limit the wide use of elastography [257]. The types of elastography and their respective utility in sports medicine are highlighted below.
Acoustic radiation force impulse (ARFI) elastography uses focused acoustic beams to convert acoustic compression waves to shear waves by absorbing acoustic energy [258]. The reaction of tissue to this process is monitored within the range of excitation, and images are generated from sequential data collection with lateral movement at given positions. The speed of shear wave propagation outside the range of excitation is used to estimate the tissue shear modulus [259]. While ARFI elastography has been used extensively in hepatic imaging, it has only recently received investigation in musculoskeletal evaluation [258, 260, 261].
SE uses US imaging to measure the amount of deformation following manual compression. Software then converts tissue hardness into a color map on the US machine. It has been used to evaluate tendon pathology including Achilles tendon [262,263,264], patellar tendon [264], epicondylar tendons of the elbow [265,266,267,268,269,270], rotator cuff tendons [268, 271,272,273,274], and biceps tendon [275]. Most studies have found that pathologic tendons are softer than normal tendon, with only one study finding that pathologic Achilles tendons are stiffer than normal tendons [276]. Additionally, SE has been used to show that healing Achilles tendons postoperatively are stiffer than normal tendons [277, 278]. Further studies are needed to validate the inter- and intra-rater reliability of SE and determine its role in the diagnosis of tendon injury and its use for monitoring recovery [279].
SWE uses an acoustic radiation force pulse to generate shear waves that propagate perpendicular to the US beam and can be converted to a measure of density using Young’s modulus [280]. SWE produces a more objective and quantitative assessment compared to strain elastography since the operator is not involved in stressing the tissues. Shear wave has been used to evaluate muscle, ligaments, and tendons [281, 282]. Findings have largely paralleled those seen with SE including softening of tendinopathic tendons [283, 284] and stiffening of post-surgical tendons [285]. SWE has also been used to monitor gastrocnemius, soleus, and Achilles tendon injuries and may be useful in guide return to play [286, 287]. As with SE, further studies on SWE are needed to validate inter- and intra-rater reliability and determine its role in the diagnosis of tendon injury, ability to monitor recovery, and usefulness in guiding return to play.
US tissue characterization (UTC) was developed to provide a standard assessment of tissue stiffness [77]. UTC utilizes a motorized device that guarantees a fixed US transducer position that obtains 600 contiguous transverse images in 45 seconds at intervals of 0.2 millimeters over a 12 centimeter distance to render a 3D block of US images [288]. After images are obtained, a complex algorithm characterizes each area of tendon into one of four echotypes based on pixel stability which is correlated to stiffness [288]. UTC has primarily been used for large tendons and ligaments, such as the Achilles tendon and patellar ligament [289,290,291,292,293]. Of note, the device used for standardized image acquisition in UTC has to be built specifically for each tendon. Similar to strain elastography (SE) and shear wave elastography (SWE), the role of UTC in the diagnosis of pathologic conditions and guiding return to play is yet to be determined, but shows promise in its ability to monitor the effect of load or treatment on tendon structure [77].
US in Sports Medicine: Guiding Return to Play
As discussed above, the improving portability of US and the ability to perform serial examinations make US an ideal imaging modality for guiding return-to-play decisions. Many physicians utilize US both to immediately assess ability to return to play on the field (i.e., triage) and to help determine when an athlete is sufficiently healed to resume play. However, imaging criteria and published guidelines are lacking, and clinicians generally rely on a combination of clinical examination and functional performance measures correlated with imaging findings when returning athletes to sport. A few studies on muscle injuries in athletes have shown that evidence of disorganized fibrous tissue, intramuscular hematoma, intermuscular hematoma, and power Doppler signal on US examination predict longer time to return to play [294,295,296].
Interventional Use of Ultrasound for Procedural Guidance
Advantages of Interventional US in Sports Medicine
Ultrasound also has multiple advantages when used to assist with sports medicine procedures (see Table 21.3). If an interventional treatment is determined to be needed following diagnostic US, it can often be performed immediately after evaluation without the additional time delay required when obtaining an MRI or CT for diagnosis [80]. Injection accuracy is improved with the utilization of ultrasound for needle guidance for most structural targets [297, 298]. Doppler US can also be used to visualize blood vessels to evaluate vascular malformations as well as vascularity of soft tissue masses which can contribute to diagnosis [299,300,301]. The use of US guidance is even more important for advanced procedures such as barbotage and percutaneous fasciotomy and tenotomy (described in more detail below), which could not be performed accurately without US guidance [302,303,304]. Some US-guided interventions have additionally shown shorter recovery times with less post-procedural pain than open surgical procedures with similar clinical outcomes [305, 306]. Many peripheral nerve procedures exist and can relieve pain; however, they all require perineural needle placement which increases risk of nerve injury through intraneural injection or nerve penetration [307, 308].
The American Medical Society for Sports Medicine (AMSSM) has suggested that US-guided procedures can be divided into three different generations [309]. First-generation techniques are those that apply US guidance to improve accuracy of established procedures. Second-generation techniques are those that have been developed primarily as a result of US guidance and utilize commonly available needles. Examples include needle tenotomy for chronic or calcific tendinosis, neovessel ablation and tendon scraping, fenestration of the transverse carpal ligament, A1 pulley fenestration, and nerve hydrodissection. Third-generation techniques utilize specially designed surgical tools or devices to duplicate well-established surgical procedures under US guidance. These include A1 pulley release using a hook knife, carpal tunnel release using Guo wires or specially designed devices, and tenotomy or fasciotomy using meniscotomes, Guo wires, or hook knives [25].
First-Generation Procedures
Since the initial use of US by Karl Dussik to evaluate the MSK system, US’s ability to visualize both soft tissue and neurovascular structures has made it popular for procedural guidance. The use of US for diagnosis affords an easy transition to performance of US-guided procedures with superior accuracy to palpation guidance [302]. In a position statement on US-guided procedures, the AMSSM concluded that there is high-quality evidence that US-guided injections are more accurate than landmark-guided injections in large joints (accuracy 91–100% for US-guided and 64–81% for landmark-guided), intermediate joints (approximately 95% for US-guided and 78% for landmark-guided), small joints (accuracy 94–100% for US-guided and 0–96% for landmark-guided), and tendon sheaths (accuracy 87–100% for US-guided and 27–60% for landmark-guided), though the difference in efficacy and cost has not yet been determined [309]. Individual joint procedures are discussed in more detail in Chaps. 5, 6, 7, 8, 9, 10, and 11.
Historically, corticosteroid injection near the target structure was believed to be sufficient to provide therapeutic benefit. The local and systemic effects of corticosteroid allowed for therapeutic benefit even if the injection was not precisely placed. As corticosteroid use has fallen out of favor due to its toxic effects on tendon and cartilage, newer agents have arisen that are thought to require precise placement at the site of injury for maximum efficacy. These include autologous blood products, bone marrow, adipose tissue, allogenic amniotic membrane, or dextrose solutions [309]. As a result, it is recommended to perform these injections under US guidance to achieve the highest injection accuracy and best outcomes [309]. Further information on and discussion of regenerative medicine injectates can be found in Chaps. 1, 2, and 3, and procedures are reviewed in Chaps. 12 and 13.
Second-Generation Procedures
Greater spatial resolution has made it possible to perform procedures that require detailed needle visualization beyond mere guidance to a target. This includes using needles to fenestrate or cut a pathologic calcification, ligament, tendon, or retinaculum.
Calcific Barbotage
Calcific barbotage is used for the treatment of calcific tendinopathy [310, 311] and is most effective for intratendinous calcification rather than osseous extension [312]. The goal of the procedure is to break up the painful calcifications within the tendon. This involves lavage of the calcific particles using injection of normal saline and a needle (commonly 18-gauge) to repeatedly inject and aspirate the calcification under direct US guidance [313]. Soft and middle-sized calcifications generally respond best to this treatment [314]. Repeat barbotage may be required to fully address some calcific lesions [315] and may be combined with subacromial corticosteroid injection for greater relief [316]. Several reviews and meta-analyses describe calcific barbotage as safe and effective for the treatment of calcific rotator cuff tendinosis [313, 316,317,318]. Compiled results show up to 55% improvement in pain and indicate that it can be used as a first-line treatment [313, 316,317,318]. Calcific barbotage may also be used to treat calcific tendinopathy of the gluteal tendons [319] and the common extensor tendon at the elbow [320].
Neovessel Ablation
Neovessel ablation procedures include tendon scraping and high-volume image-guided injection (HVIGI) that can be performed together or in isolation under US guidance. The goal of these procedures is to disrupt the neovessels and neonerves that grow from fat pads like Hoffa’s or Kager’s fat pad that lie deep to large tendons. These neonerves and neovessels are thought to contribute to pain associated with patellar [321] and Achilles [322] tendinopathy. US with color Doppler allows for the visualization and targeting of these neovessels pre-procedurally with the hope of subsequently disrupting the accompanying neonerves. A significant advantage of these extra-tendinous procedures is that the integrity of the tendon is not compromised. This results in a more rapid return to activity after the procedure than what is recommended for intra-tendinous procedures.
The tendon scraping procedure can be performed entirely under US guidance through an 11-blade stab incision with an 18-gauge needle or meniscotome inserted perpendicular to the tendon under US guidance. This is then passed back and forth in a sweeping motion deep to the tendon at the area of neovascularization. While the utility of open and mini-open surgical tendon scraping to treat Achilles tendinosis is well documented, only one study has examined percutaneous Achilles tendon scraping under US guidance. In that study, percutaneous scraping of 19 tendons showed similar efficacy to an open procedure [322]. One case has been published on the use of tendon scraping to treat patellar tendinopathy that resulted in complete resolution of symptoms and full return to play at 4 weeks with no recurrence at 11-month follow-up321.
HVIGI typically consists of a 40–50mL injection of normal saline and aims to separate the tendon from the deep fat pad while disrupting neovessels and neonerves [323,324,325,326,327,328,329,330,331]. HVIGI has been shown to improve pain and physical function in multiple case reports, case series, one randomized controlled trial (RCT), and a retrospective cohort study, but rates of return to sport varied [323, 325,326,327,328,329,330, 332]. When compared to PRP or eccentric exercises alone, HVIGI had better results at 6 weeks than PRP and eccentric exercises alone, and both PRP and HVIGI were superior to eccentric exercises alone at 24 weeks [324]. HVIGI to treat greater trochanteric pain syndrome [333] and shoulder impingement [331] have been studied by one author, but found either no benefit or only short-term benefit, respectively.
Third-Generation Procedures
More recently, specific tools have been developed to perform procedures under US guidance that were historically performed by open or arthroscopic surgery. US-guided procedures allow for smaller incision sites that are associated with reduced post-procedure pain and improved function with a more rapid return to baseline activity. These procedures are also likely less costly with lower complication rates and increased patient satisfaction [334,335,336]. However, if these procedures are performed by practitioners with inadequate anatomical and procedural competence, they carry significantly higher risk for injury to surrounding structures. Correct identification of the anatomy and pathology is central to any US-guided procedure, and most third-generation procedures should be practiced on cadavers prior to use in patients. Use of cutting devices without adequate experience could lead to severe and irreversible injury to critical structures. Therefore, these procedures are best performed by experienced sonographers and proceduralists.
Ligament or Retinaculum Release
Ligament or retinaculum release can now be performed under US guidance through a very small incision. This has been demonstrated with release of the transverse carpal ligament (TCL) in carpal tunnel syndrome, release of the A1 pulley in trigger finger, release of the flexor retinaculum in tarsal tunnel syndrome, and release of the first dorsal compartment of the wrist to treat de Quervain’s tenosynovitis.
Release of the TCL under US guidance to treat carpal tunnel syndrome has evolved from a procedure done with US assistance to one done completely under US guidance through needle fenestration [337,338,339], use of a wire to cut the TCL [340,341,342], use of a hook knife to cut the TCL [305, 343,344,345,346,347], or use of commercially available devices such as the SX-ONE device [348,349,350,351]. US guidance allows for the direct visualization of pertinent anatomy that must be avoided during the procedure. This includes the transverse safe zone (bordered radially by the median nerve and ulnarly by the hook of the hamate or ulnar artery), palmar cutaneous branch of the median nerve, Berrettini branch, recurrent motor branch of the median nerve, and other neurovascular anomalies [352]. Overall, studies on US-guided carpal tunnel release with the SX-ONE device report successful release of the TCL in over 600 wrists with minimal complications and a 95% success rate [348].
Trigger finger release with a needle can be performed under US guidance with improved cosmesis and fewer days absent from work than open surgical release [306, 353, 354]. This is commonly performed after failure of a corticosteroid injection. Trigger finger release under US guidance can also be accomplished with use of a hook knife or wire to cut in a retrograde direction (intra or extra sheath) or use of a needle or needle knife (Nokor needle) to cut in an anterograde direction [355]. Cadaveric and clinical data have shown a higher complete pulley release rate when using a hook knife instead of a needle [355,356,357,358]. When compared to surgery, US-guided trigger finger release has a shorter procedure time, lower cost, and more rapid return to normal activities [306, 359].
US-guided tarsal tunnel release with a hook knife [360] and first dorsal compartment release with a needle have also been described. These procedures theoretically afford less pain, are lower cost, and have a more rapid recovery than their respective surgical procedures, but more research is needed [361].
Tendon, Muscle, or Fascial Release
Tendon, muscle, and fascial release can be performed under US guidance and is most beneficial for those who are poor surgical candidates or need a more rapid return to activities than that afforded by surgery. To date, several cadaveric and a few patient studies of these techniques have been published. Current limitations to these procedures include operator skill and lack of procedure-specific tools. The procedures are highlighted below, although a full description of these techniques is beyond the scope of this chapter.
Biceps tendon release using different devices (hook knife, scalpel, banana blade, retractable blade, serrated blade) with retrograde cutting of the biceps tendon at various locations (rotator interval, bicipital anchor, and bicipital groove) have been described [362,363,364]. Cases performed in the bicipital groove using a scalpel or hook knife were most successful in releasing the long head of the biceps in cadavers.
Plantaris tendon release using a hook knife [365] and adductor release using a Guo cutting wire [366] in a retrograde direction under US guidance have been described in cadavers and are thought to be safe.
Plantar fascia release under US guidance using a hook knife to cut in a retrograde medial to lateral direction [367] in cadavers or a beaver blade to cut in a deep to superficial direction in patients [368] have been found to be successful.
Fasciotomy of the anterior and lateral compartments of the lower leg for treatment of chronic exertional compartment syndrome has also been successfully performed on cadavers under US guidance using a meniscotome and anterograde release [34].
Although many of these procedures are still in development, the use of US to guide procedures offers a promising method to minimize the invasiveness of surgical procedures, decrease recovery time, and decrease cost. However, additional research is needed to develop specific tools to improve the ease of US-guided procedures and to directly compare outcomes between surgical and non-surgical procedures. The next step in the development of US-guided procedures is to determine if repair of tissues performed under US guidance has similar outcomes to open or arthroscopic surgical procedures and what differences in complications and rehabilitation protocols and timeline are noted. A protocol outlining US-guided repair of the lateral ligament complex of the ankle has been published and shows promise [369].
US in Orthopedics: Use of US in Preoperative Planning and in the Operating Room
In addition to assisting with diagnosis, US can be used to assist orthopedic surgeons during preoperative planning and intraoperatively to augment visualization of relevant structures. Several studies have shown that preoperative sonographic measurements of the patellar tendon [370], quadriceps tendon [371], and gracilis and semitendinosus tendons [372,373,374] predict ACL graft size. Preoperative US mapping of peripheral nerves targeted for surgical intervention has also been used to speed identification and access to the target, minimize tissue destruction, and decrease operating time [375]. US can also be utilized preoperatively to tag nerves commonly injured during certain procedures that are difficult to localize intraoperatively. This includes avoiding sensitive structures during Achilles tendon repair [376], plantar fascia repair [377], and medial elbow arthroscopy [378] and localizing the lateral femoral cutaneous nerve for operative decompression [379].
Current Limitations and Future Directions
In spite of the dramatic expansion of US technology over the last several decades, US still has several limitations (Table 21.4). Overcoming these limitations is the topic of ongoing research, and promising methods are discussed below.
While US is often touted as a portable imaging modality, especially compared to x-ray, MRI, and CT, companies continue to push the limits of portability to make US truly “pocket-portable.” The first US machine small enough to be used on the battlefield was developed in 1996 [380], and portable US machines have continued to demonstrate utility in field clinics after natural disasters [381]. Transducers that attach to phones and tablets are now commonplace. Transducers the size of a pen are actively in development, but several disadvantages and barriers to production remain for these small devices. Smaller probes and US machines often compromise image resolution, field of view, ability to employ multiple scanning modes (such as Doppler), machine durability, and battery life (although alternative battery sources, such as solar power, are also in development) [382]. In spite of that, technological progress continues to move toward a world where sideline US evaluation could be as simple as pulling out a durable, pocket-sized probe that syncs wirelessly with a mobile device or laptop.
The “operator dependency” of US is frequently cited as a weakness, but this is likely improving as US training increases. US training is being incorporated into medical school, residency programs, fellowships, and national workshops to improve and standardize operator skill [383, 384]. The number of articles cited in PubMed that utilize US to evaluate MSK conditions has increased exponentially since the 1970s with over 2800 articles published in 2018 alone. Despite this, inter-rater reliability in MSK and nerve evaluation still varies based on the site examined, whether the tissue is healthy or pathologic, and how much training the examiner has received [385,386,387,388,389]. New technology, such as UTC, attempts to standardize US evaluation by removing the human operator, but remains impractical for widespread implementation as described previously.
Additionally, US evaluation is limited by beam attenuation caused by superficial structures that impede deeper visualization. B-mode US relies on high-frequency sound waves to provide sufficient spatial resolution for tissue differentiation, but these high-frequency waves are attenuated when they pass through tissue layers, especially subcutaneous fat. This makes sonographic imaging of obese patients difficult. While deeper penetration can be achieved by using a lower-frequency transducer, this results in decreased resolution [390]. Tissue harmonic imaging (THI) is one attempt to overcome this problem. It utilizes higher-frequency harmonic sound waves produced by the original US wave interacting with nonlinear tissues of deep structures. These higher-frequency waves reflected from deep structures are captured by the probe, allowing for higher-resolution visualization of deep structures that would not be possible with standard B-mode US [391, 392]. In addition to THI, technological developments such as spatial compound imaging, speckle reduction, and tissue aberration correction are all image processing enhancements that improve image resolution [393,394,395].
US field of view is limited by the size of the transducer, which traditionally provides a two-dimensional view. As a result, the examiner must formulate a three-dimensional (3D) view in their mind using orthogonal planes and may need to gather multiple images to measure a long structure. To overcome this limitation, extended field of view US was developed in the late 1990s. It uses image registration technology to stitch together a larger field of view and allow for accurate measurement of larger objects including rotator cuff tears, fluid collections, and masses [396, 397]. 3D US has been developed to overcome the 2D nature of current US evaluation. It utilizes processing of data from multiple US images to form a 3D image. Though primarily used outside of the MSK system [398,399,400], it has also been trialed in the assessment of muscle volume and muscle fascicle length and architecture [48, 401].
Conclusion
US has played a role in MSK evaluation for over 50 years and has several advantages over other imaging modalities. Recent progress has expanded the scope of US in sports medicine to include other organ systems. US is an ideal imaging modality for injury evaluations at sporting events for its portability. Further, new programs enable physiologic and biological assessment of injured tissues to make return-to-play decisions. Its use in procedural guidance has improved the accuracy of existing office-based procedures while also opening the door for US-based micro-invasive surgical interventions. Ongoing research continues to expand the diagnostic and interventional capabilities of US, broadening the indications of US in the hands of skilled sports medicine physicians.
References
Dussik KT. Ultraschall-Diagnostik, insbesondere bei Gehirnerkrankungen, mittels Hyperphonographie. Zeitschrift fur physikalische Therapie, Bader- und Klimaheilkunde. 1948;1(9-10):140–5.
Dussik KT, Fritch DJ, Kyriazidou M, Sear RS. Measurements of articular tissues with ultrasound. Am J Phys Med. 1958;37(3):160–5.
McDonald DG, Leopold GR. Ultrasound B-scanning in the differentiation of Baker's cyst and thrombophlebitis. Br J Radiol. 1972;45(538):729–32.
Morganroth J, Maron BJ, Henry WL, Epstein SE. Comparative left ventricular dimensions in trained athletes. Ann Intern Med. 1975;82(4):521–4.
Levinsohn EM. Computerized tomography of the musculoskeletal system. JAMA. 1980;244(3):278–80.
Sauser DD, Billimoria PE, Rouse GA, Mudge K. CT evaluation of hip trauma. AJR. Am J Roentgenol. 1980;135(2):269–74.
Danzig L, Resnick D, Greenway G. Evaluation of unstable shoulders by computed tomography. A preliminary study. Am J Sports Med. 1982;10(3):138–41.
Murcia M, Brennan RE, Edeiken J. Computed tomography of stress fracture. Skelet Radiol. 1982;8(3):193–5.
Somer K, Meurman KO. Computed tomography of stress fractures. J Comput Assist Tomogr. 1982;6(1):109–15.
Mandelbaum BR, Finerman GA, Reicher MA, et al. Magnetic resonance imaging as a tool for evaluation of traumatic knee injuries. Anatomical and pathoanatomical correlations. Am J Sports Med. 1986;14(5):361–70.
Verhaven EF, Shahabpour M, Handelberg FW, Vaes PH, Opdecam PJ. The accuracy of three-dimensional magnetic resonance imaging in the diagnosis of ruptures of the lateral ligaments of the ankle. Am J Sports Med. 1991;19(6):583–7.
Reinig JW, McDevitt ER, Ove PN. Progression of meniscal degenerative changes in college football players: evaluation with MR imaging. Radiology. 1991;181(1):255–7.
Fornage BD, Touche DH, Segal P, Rifkin MD. Ultrasonography in the evaluation of muscular trauma. Journal of Ultrasound in Medicine : Official Journal of the American Institute of Ultrasound in Medicine. 1983;2(12):549–54.
Fornage BD. Achilles tendon: US examination. Radiology. 1986;159(3):759–64.
Fornage BD, Rifkin MD, Touche DH, Segal PM. Sonography of the patellar tendon: preliminary observations. AJR. Am J Roentgenol. 1984;143(1):179–82.
Coral A, van Holsbeeck M, Adler RS. Imaging of meniscal cyst of the knee in three cases. Skelet Radiol. 1989;18(6):451–5.
Cooperberg PL, Tsang I, Truelove L, Knickerbocker WJ. Gray scale ultrasound in the evaluation of rheumatoid arthritis of the knee. Radiology. 1978;126(3):759–63.
De Flaviis L, Scaglione P, Nessi R, Ventura R, Calori G. Ultrasonography of the hand in rheumatoid arthritis. Acta radiologica (Stockholm, Sweden : 1987). 1988;29(4):457–60.
Crass JR, Craig EV, Thompson RC, Feinberg SB. Ultrasonography of the rotator cuff: surgical correlation. J Clin Ultrasound: JCU. 1984;12(8):487–91.
Harryman DT 2nd, Mack LA, Wang KY, Jackins SE, Richardson ML, Matsen FA 3rd. Repairs of the rotator cuff. Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am Vol. 1991;73(7):982–9.
Marchal GJ, Van Holsbeeck MT, Raes M, et al. Transient synovitis of the hip in children: role of US. Radiology. 1987;162(3):825–8.
van Holsbeeck M, van Holsbeeck K, Gevers G, et al. Staging and follow-up of rheumatoid arthritis of the knee. Comparison of sonography, thermography, and clinical assessment. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 1988;7(10):561–6.
van Holsbeeck M, Introcaso J. Musculoskeletal Ultrasound. St Louis: Mosby; 1991.
Fornage B. Musculoskeletal Ultrasound. New York: Churchill Livingstone; 1995.
Finnoff JT, Hall MM, Adams E, et al. American Medical Society for Sports Medicine (AMSSM) position statement: interventional musculoskeletal ultrasound in sports medicine. Br J Sports Med. 2015;49(3):145–50.
Jacobson JA. Musculoskeletal ultrasound and MRI: which do I choose? Semin Musculoskelet Radiol. 2005;9(2):135–49.
Sharpe RE, Nazarian LN, Parker L, Rao VM, Levin DC. Dramatically increased musculoskeletal ultrasound utilization from 2000 to 2009, especially by podiatrists in private offices. J Am Coll Radiol: JACR. 2012;9(2):141–6.
Finnoff JT. The evolution of diagnostic and interventional ultrasound in sports medicine. PM & R: The Journal of Injury, Function, and Rehabilitation. 2016;8(3 Suppl):S133–8.
Finnoff JT, Ray J, Corrado G, Kerkhof D, Hill J. Sports ultrasound: applications beyond the musculoskeletal system. Sports Health. 2016;8(5):412–7.
Blaivas M. Bedside emergency department ultrasonography in the evaluation of ocular pathology. Acad Emerg Med Off J Soc Acad Emerg Med. 2000;7(8):947–50.
Staub LJ, Biscaro RRM, Kaszubowski E, Maurici R. Chest ultrasonography for the emergency diagnosis of traumatic pneumothorax and haemothorax: a systematic review and meta-analysis. Injury. 2018;49(3):457–66.
Venckunas T, Mazutaitiene B. The role of echocardiography in the differential diagnosis between training induced myocardial hypertrophy versus cardiomyopathy. J Sports Sci Med. 2007;6(2):166–71.
Peck E, Jelsing E, Onishi K. Advanced ultrasound-guided interventions for tendinopathy. Phys Med Rehabil Clin N Am. 2016;27(3):733–48.
Lueders DR, Sellon JL, Smith J, Finnoff JT. Ultrasound-guided fasciotomy for chronic exertional compartment syndrome: a cadaveric investigation. PM & R: The Journal of Injury, Function, and Rehabilitation. 2017;9(7):683–90.
Smith J, Alfredson H, Masci L, Sellon JL, Woods CD. Sonographically guided plantaris tendon release: a cadaveric validation study. PM & R: The Journal of Injury, Function, and Rehabilitation. 2019;11(1):56–63.
Ojaghihaghighi S, Lombardi KM, Davis S, Vahdati SS, Sorkhabi R, Pourmand A. Diagnosis of traumatic eye injuries with point-of-care ocular ultrasonography in the emergency department. Ann Emerg Med. 2019;74(3):365–71.
Daniel MC, Restori M, Acheson J, Dahlmann-Noor A. Ocular ultrasound to detect raised intracranial pressure. Pediatr Emerg Care. 2017;33(3):e4.
Scharonow M, Weilbach C. Prehospital point-of-care emergency ultrasound: a cohort study. Scandinavian J Trauma Resuscitat Emerg Med. 2018;26(1):49.
Saranteas T, Mavrogenis AF, Mandila C, Poularas J, Panou F. Ultrasound in cardiac trauma. J Crit Care. 2017;38:144–51.
Miele V, Piccolo CL, Trinci M, Galluzzo M, Ianniello S, Brunese L. Diagnostic imaging of blunt abdominal trauma in pediatric patients. La Radiologia medica. 2016;121(5):409–30.
Editorial: 5G-based mhealth bringing healthcare convergence to reality. IEEE Rev Biomed Eng. 2019;12:2–3.
Nicholls M. Ultrasound scanning via a 5G network. 2019.; https://healthcare-in-europe.com/en/news/ultrasound-scanning-via-a-5g-network.html. Accessed 8 Aug, 2020.
Ali ZS, Pisapia JM, Ma TS, Zager EL, Heuer GG, Khoury V. Ultrasonographic evaluation of peripheral nerves. World neurosurgery. 2016;85:333–9.
Zaidman CM, Seelig MJ, Baker JC, Mackinnon SE, Pestronk A. Detection of peripheral nerve pathology: comparison of ultrasound and MRI. Neurology. 2013;80(18):1634–40.
Bureau NJ, Ziegler D. Economics of Musculoskeletal Ultrasound. Current Radiology Reports. 2016;4:44.
Mandeville R, Wali A, Park C, Groessl E, Walker FO, Cartwright MS. Cost-effectiveness of neuromuscular ultrasound in focal neuropathies. Neurology. 2019;92(23):e2674–8.
Parker L, Nazarian LN, Carrino JA, et al. Musculoskeletal imaging: medicare use, costs, and potential for cost substitution. J Am Coll Radiol: JACR. 2008;5(3):182–8.
Weide G, van der Zwaard S, Huijing PA, Jaspers RT, Harlaar J. 3D ultrasound imaging: fast and cost-effective morphometry of musculoskeletal tissue. J Visualized Experiments: JoVE. 2017;129
Guillin R, Botchu R, Bianchi S. Sonography of orthopedic hardware impingement of the extremities. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2012;31(9):1457–63.
Draghi F, Bortolotto C, Draghi AG, Gitto S. Intrasheath instability of the peroneal tendons: dynamic ultrasound imaging. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2018;37(12):2753–8.
Fisher CL, Rabbani T, Johnson K, Reeves R, Wood A. Diagnostic capability of dynamic ultrasound evaluation of supination-external rotation ankle injuries: a cadaveric study. BMC Musculoskelet Disord. 2019;20(1):502.
Rossi F, Zaottini F, Picasso R, Martinoli C, Tagliafico AS. Ankle and foot ultrasound: reliability of side-to-side comparison of small anatomic structures. J Ultrasound Med. 2019;38(8):2143–53.
Tagliafico A, Martinoli C. Reliability of side-to-side sonographic cross-sectional area measurements of upper extremity nerves in healthy volunteers. J Ultrasound Med. 2013;32(3):457–62.
Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502.
Tveit M, Rosengren BE, Nilsson J, Karlsson MK. Former male elite athletes have a higher prevalence of osteoarthritis and arthroplasty in the hip and knee than expected. Am J Sports Med. 2012;40(3):527–33.
Cross TM, Smart RC, Thomson JE. Exposure to diagnostic ionizing radiation in sports medicine: assessing and monitoring the risk. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine. 2003;13(3):164–70.
Pearce MS, Salotti JA, Little MP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet (London, England). 2012;380(9840):499–505.
Pijpe A, Andrieu N, Easton DF, et al. Exposure to diagnostic radiation and risk of breast cancer among carriers of BRCA1/2 mutations: retrospective cohort study (GENE-RAD-RISK). BMJ : British Medical Journal. 2012;345:e5660.
Adams JG, McAlindon T, Dimasi M, Carey J, Eustace S. Contribution of meniscal extrusion and cartilage loss to joint space narrowing in osteoarthritis. Clin Radiol. 1999;54(8):502–6.
Fife RS, Brandt KD, Braunstein EM, et al. Relationship between arthroscopic evidence of cartilage damage and radiographic evidence of joint space narrowing in early osteoarthritis of the knee. Arthritis Rheum. 1991;34(4):377–82.
Podlipská J, Guermazi A, Lehenkari P, et al. Comparison of diagnostic performance of semi-quantitative knee ultrasound and knee radiography with MRI: oulu knee osteoarthritis study. Sci Rep. 2016;6:22365.
Davies MAM, Kerr ZY, DeFreese JD, et al. Prevalence of and risk factors for total hip and knee replacement in retired national football league athletes. Am J Sports Med. 2019;47(12):2863–70.
Volpi P, Quaglia A, Carimati G, Petrillo S, Bisciotti GN. High incidence of hip and knee arthroplasty in former professional, male football players. J Sports Med Phys Fitness. 2019;59(9):1558–63.
Chun KA, Cho KH. Postoperative ultrasonography of the musculoskeletal system. Ultrasonography (Seoul, Korea). 2015;34(3):195–205.
Jacobson JA, Lax MJ. Musculoskeletal sonography of the postoperative orthopedic patient. Semin Musculoskelet Radiol. 2002;6(1):67–77.
Bureau NJ, Ali SS, Chhem RK, Cardinal E. Ultrasound of musculoskeletal infections. Semin Musculoskelet Radiol. 1998;2(3):299–306.
Bozic KJ, Kamath AF, Ong K, et al. Comparative epidemiology of revision arthroplasty: failed THA poses greater clinical and economic burdens than failed TKA. Clin Orthop Relat Res. 2015;473(6):2131–8.
van Kempen RW, Schimmel JJ, van Hellemondt GG, Vandenneucker H, Wymenga AB. Reason for revision TKA predicts clinical outcome: prospective evaluation of 150 consecutive patients with 2-years follow-up. Clin Orthop Relat Res. 2013;471(7):2296–302.
Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. Radiographics: A Review Publication of the Radiological Society of North America, Inc. 2004;24(6):1679–91.
Singh DR, Chin MS, Peh WC. Artifacts in musculoskeletal MR imaging. Semin Musculoskelet Radiol. 2014;18(1):12–22.
Boesen MI, Boesen M, Langberg H, et al. Musculoskeletal colour/power Doppler in sports medicine: image parameters, artefacts, image interpretation and therapy. Clin Exp Rheumatol. 2010;28(1):103–13.
Lambros V. Use of doppler ultrasound to avoid injection complications. Plastic Reconstruct Surg. 2019;144(4):724e.
Alfredson H, Ohberg L. Neovascularisation in chronic painful patellar tendinosis--promising results after sclerosing neovessels outside the tendon challenge the need for surgery. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA. 2005;13(2):74–80.
Hoksrud A, Ohberg L, Alfredson H, Bahr R. Color Doppler ultrasound findings in patellar tendinopathy (jumper's knee). Am J Sports Med. 2008;36(9):1813–20.
Arslan S, Karahan AY, Oncu F, Bakdik S, Durmaz MS, Tolu I. Diagnostic performance of superb microvascular imaging and other sonographic modalities in the assessment of lateral epicondylosis. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2018;37(3):585–93.
Domenichini R, Pialat JB, Podda A, Aubry S. Ultrasound elastography in tendon pathology: state of the art. Skelet Radiol. 2017;46(12):1643–55.
Rabello LM, Dams OC, van den Akker-Scheek I, Zwerver J, O'Neill S. Substantiating the use of ultrasound tissue characterization in the analysis of tendon structure: a systematic review. Clin J Sport Med. 2019;
Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42(2):311–9.
Patel DR, Yamasaki A, Brown K. Epidemiology of sports-related musculoskeletal injuries in young athletes in United States. Transl Pediatrics. 2017;6(3):160–6.
Smith J, Finnoff JT. Diagnostic and interventional musculoskeletal ultrasound: part 2. Clinical applications. PM & R: The Journal of Injury, Function, and Rehabilitation. 2009;1(2):162–77.
He W, Xiang DY, Dai JP. Sonography in the 29th olympic and paralympic games: a retrospective analysis. Clin Imaging. 2011;35(2):143–7.
Kilker BA, Holst JM, Hoffmann B. Bedside ocular ultrasound in the emergency department. European Journal of Emergency Medicine: Official Journal of the European Society for Emergency Medicine. 2014;21(4):246–53.
Kendall CJ, Prager TC, Cheng H, Gombos D, Tang RA, Schiffman JS. Diagnostic ophthalmic ultrasound for radiologists. Neuroimaging Clin N Am. 2015;25(3):327–65.
Jones NP. One year of severe eye injuries in sport. Eye (London, England). 1988;2(Pt 5):484–7.
Haring RS, Sheffield ID, Canner JK, Schneider EB. Epidemiology of sports-related eye injuries in the United States. JAMA ophthalmology. 2016;134(12):1382–90.
Miller KN, Collins CL, Chounthirath T, Smith GA. Pediatric sports- and recreation-related eye injuries treated in US emergency departments. Pediatrics. 2018;141(2).
Micieli JA, Easterbrook M. Eye and Orbital Injuries in Sports. Clin Sports Med. 2017;36(2):299–314.
Leivo T, Haavisto AK, Sahraravand A. Sports-related eye injuries: the current picture. Acta Ophthalmol. 2015;93(3):224–31.
Vrablik ME, Snead GR, Minnigan HJ, Kirschner JM, Emmett TW, Seupaul RA. The diagnostic accuracy of bedside ocular ultrasonography for the diagnosis of retinal detachment: a systematic review and meta-analysis. Annals Emerg Med. 2015;65(2):199–203.e191.
MacEwen CJ. Sport associated eye injury: a casualty department survey. Br J Ophthalmol. 1987;71(9):701.
Filipe JA, Barros H, Castro-Correia J. Sports-related ocular injuries. A three-year follow-up study. Ophthalmology. 1997;104(2):313–8.
Barr A, Baines PS, Desai P, MacEwen CJ. Ocular sports injuries: the current picture. Br J Sports Med. 2000;34(6):456.
Baker N, Amini R, Situ-LaCasse EH, et al. Can emergency physicians accurately distinguish retinal detachment from posterior vitreous detachment with point-of-care ocular ultrasound? Am J Emerg Med. 2018;36(5):774–6.
Shinar Z, Chan L, Orlinsky M. Use of ocular ultrasound for the evaluation of retinal detachment. J Emergency Med. 2011;40(1):53–7.
Major R, Girling S, Boyle A. Ultrasound measurement of optic nerve sheath diameter in patients with a clinical suspicion of raised intracranial pressure. Emergency medicine journal : EMJ. 2011;28(8):679–81.
Tayal VS, Neulander M, Norton HJ, Foster T, Saunders T, Blaivas M. Emergency department sonographic measurement of optic nerve sheath diameter to detect findings of increased intracranial pressure in adult head injury patients. Ann Emerg Med. 2007;49(4):508–14.
Ohle R, McIsaac SM, Woo MY, Perry JJ. Sonography of the optic nerve sheath diameter for Detection of Raised Intracranial Pressure Compared to Computed tomography: a systematic review and meta-analysis. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2015;34(7):1285–94.
Halvorsen T, Walsted ES, Bucca C, et al. Inducible laryngeal obstruction: an official joint European Respiratory Society and European Laryngological Society statement. The European Respiratory Journal. 2017;50(3).
Christensen PM, Thomsen SF, Rasmussen N, Backer V. Exercise-induced laryngeal obstructions: prevalence and symptoms in the general public. European Archives of Oto-Rhino-Laryngology: Official Journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS): Affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2011;268(9):1313–9.
Wilson JJ, Wilson EM. Practical management: vocal cord dysfunction in athletes. Clinical Journal of Sport Medicine : Official Journal of the Canadian Academy of Sport Medicine. 2006;16(4):357–60.
Finnoff JT, Orbelo DM, Ekbom DC. Can ultrasound identify paradoxical vocal fold movement? a pilot study. Clinical Journal of Sport Medicine : Official Journal of the Canadian Academy of Sport Medicine. 2018;
Griffin SA, Walsted ES, Hull JH. Infographic. The breathless athlete: EILO. Br J Sports Med. 2019;53(10):616–7.
Harmon KG, Drezner JA, Wilson MG, Sharma S. Incidence of sudden cardiac death in athletes: a state-of-the-art review. Br J Sports Med. 2014;48(15):1185–92.
Boden BP, Breit I, Beachler JA, Williams A, Mueller FO. Fatalities in high school and college football players. Am J Sports Med. 2013;41(5):1108–16.
Corrado D, Pelliccia A, Bjornstad HH, et al. Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J. 2005;26(5):516–24.
Harmon KG, Zigman M, Drezner JA. The effectiveness of screening history, physical exam, and ECG to detect potentially lethal cardiac disorders in athletes: a systematic review/meta-analysis. J Electrocardiol. 2015;48(3):329–38.
Drezner JA, Sharma S, Baggish A, et al. International criteria for electrocardiographic interpretation in athletes: Consensus statement. Br J Sports Med. 2017;51(9):704–31.
Maron BJ, Friedman RA, Kligfield P, et al. Assessment of the 12-lead ECG as a screening test for detection of cardiovascular disease in healthy general populations of young people (12-25 Years of Age): a scientific statement from the American Heart Association and the American College of Cardiology. Circulation. 2014;130(15):1303–34.
Malhotra R, West JJ, Dent J, et al. Cost and yield of adding electrocardiography to history and physical in screening Division I intercollegiate athletes: a 5-year experience. Heart Rhythm. 2011;8(5):721–7.
Yim ES, Basilico F, Corrado G. Early screening for cardiovascular abnormalities with preparticipation echocardiography: utility of focused physician-operated echocardiography in preparticipation screening of athletes. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2014;33(2):307–13.
Gleason CN, Kerkhof DL, Cilia EA, et al. Early screening for cardiovascular abnormalities with preparticipation echocardiography: feasibility study. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine. 2017;27(5):423–9.
Lucas C, Kerkhof DL, Briggs JE, Corrado GD. The use of echocardiograms in preparticipation examinations. Curr Sports Med Rep. 2017;16(2):77–83.
Rizzo M, Spataro A, Cecchetelli C, et al. Structural cardiac disease diagnosed by echocardiography in asymptomatic young male soccer players: implications for pre-participation screening. Br J Sports Med. 2012;46(5):371–3.
Kerkhof DL, Gleason CN, Basilico FC, Corrado GD. Is there a role for limited echocardiography during the preparticipation physical examination? PM & R: The Journal of Injury, Function, and Rehabilitation. 2016;8(3 Suppl):S36–44.
Yim ES, Kao D, Gillis EF, Basilico FC, Corrado GD. Focused physician-performed echocardiography in sports medicine: a potential screening tool for detecting aortic root dilatation in athletes. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2013;32(12):2101–6.
Yim ES, Gillis EF, Ojala K, MacDonald J, Basilico FC, Corrado GD. Focused transthoracic echocardiography by sports medicine physicians: measurements relevant to hypertrophic cardiomyopathy. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2013;32(2):333–8.
Griffith JF, Rainer TH, Ching AS, Law KL, Cocks RA, Metreweli C. Sonography compared with radiography in revealing acute rib fracture. AJR. Am J Roentgenol. 1999;173(6):1603–9.
Battle C, Hayward S, Eggert S, Evans PA. Comparison of the use of lung ultrasound and chest radiography in the diagnosis of rib fractures: a systematic review. Emergency Med J: EMJ. 2019;36(3):185–90.
Lichtenstein DA, Meziere G, Lascols N, et al. Ultrasound diagnosis of occult pneumothorax. Crit Care Med. 2005;33(6):1231–8.
Lichtenstein D, Meziere G, Biderman P, Gepner A. The comet-tail artifact: an ultrasound sign ruling out pneumothorax. Intensive Care Med. 1999;25(4):383–8.
Berkoff DJ, English J, Theodoro D. Sports medicine ultrasound (US) beyond the musculoskeletal system: use in the abdomen, solid organs, lung, heart and eye. Br J Sports Med. 2015;49(3):161–5.
Lichtenstein DA, Menu Y. A bedside ultrasound sign ruling out pneumothorax in the critically ill. Lung sliding Chest. 1995;108(5):1345–8.
Lyon M, Walton P, Bhalla V, Shiver SA. Ultrasound detection of the sliding lung sign by prehospital critical care providers. Am J Emerg Med. 2012;30(3):485–8.
Soldati G, Testa A, Sher S, Pignataro G, La Sala M, Silveri NG. Occult traumatic pneumothorax: diagnostic accuracy of lung ultrasonography in the emergency department. Chest. 2008;133(1):204–11.
Rozycki GS, Ochsner MG, Schmidt JA, et al. A prospective study of surgeon-performed ultrasound as the primary adjuvant modality for injured patient assessment. J Trauma. 1995;39(3):492–8; discussion 498-500.
Kirkpatrick AW, Sirois M, Laupland KB, et al. Hand-held thoracic sonography for detecting post-traumatic pneumothoraces: the Extended Focused Assessment with Sonography for Trauma (EFAST). J Trauma. 2004;57(2):288–95.
Brun PM, Bessereau J, Chenaitia H, et al. Stay and play eFAST or scoop and run eFAST? That is the question! Am J Emerg Med. 2014;32(2):166–70.
Bloom BA, Gibbons RC. Focused Assessment with Sonography for Trauma (FAST). StatPearls. Treasure Island (FL): StatPearls Publishing LLC; 2019.
Ceraulo AS, Bytomski JR. Infectious mononucleosis management in athletes. Clin Sports Med. 2019;38(4):555–61.
Putukian M, O'Connor FG, Stricker P, et al. Mononucleosis and athletic participation: an evidence-based subject review. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine. 2008;18(4):309–15.
Hosey RG, Mattacola CG, Kriss V, Armsey T, Quarles JD, Jagger J. Ultrasound assessment of spleen size in collegiate athletes. Br J Sports Med. 2006;40(3):251–4; discussion 251-254.
Smereczynski A, Kolaczyk K, Lubinski J, Bojko S, Galdynska M, Bernatowicz E. Sonographic imaging of Spigelian hernias. J Ultrasonography. 2012;12(50):269–75.
Jacobson JA. Fundamentals of musculoskeletal ultrasound. 3rd ed. Philadelphia, PA: Elsevier; 2018.
Bradley MJ, Cosgrove DO. Chapter 41 - The abdominal wall, peritoneum and retroperitoneum. In: Allan PL, Baxter GM, Weston MJ, editors. Clinical ultrasound. 3rd ed. Edinburgh: Churchill Livingstone; 2011. p. 798–827.
Gokhale S. Three-dimensional sonography of muscle hernias. J Ultrasound Med. 2007;26(2):239–42.
Connell D, Ali K, Javid M, Bell P, Batt M, Kemp S. Sonography and MRI of rectus abdominis muscle strain in elite tennis players. AJR. Am J Roentgenol. 2006;187(6):1457–61.
Obaid H, Nealon A, Connell D. Sonographic appearance of side strain injury. AJR. Am J Roentgenol. 2008;191(6):W264–7.
Stevens KJ, Crain JM, Akizuki KH, Beaulieu CF. Imaging and ultrasound-guided steroid injection of internal oblique muscle strains in baseball pitchers. Am J Sports Med. 2010;38(3):581–5.
Minardi J, Shaver E, Monseau A, Pratt A, Layman SM. Right lower quadrant pain in a young female: ultrasound diagnosis of rectus abdominis tear. J Emergency Med. 2015;49(5):623–6.
Nealon AR, Kountouris A, Cook JL. Side strain in sport: a narrative review of pathomechanics, diagnosis, imaging and management for the clinician. J Sci Med Sport. 2017;20(3):261–6.
Thorborg K, Reiman MP, Weir A, et al. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. J Orthopaedic Sports Phys Therapy. 2018;48(4):239–49.
Niebuhr H, Konig A, Pawlak M, Sailer M, Kockerling F, Reinpold W. Groin hernia diagnostics: dynamic inguinal ultrasound (DIUS). Langenbeck's Arch Surg. 2017;402(7):1039–45.
Jenkins JT, O'Dwyer PJ. Inguinal hernias. BMJ. 2008;336(7638):269–72.
Vasileff WK, Nekhline M, Kolowich PA, Talpos GB, Eyler WR, van Holsbeeck M. Inguinal hernia in athletes: role of dynamic ultrasound. Sports health. 2017;9(5):414–21.
HerniaSurge G. International guidelines for groin hernia management. Hernia. 2018;22(1):1–165.
Weir A, Brukner P, Delahunt E, et al. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br J Sports Med. 2015;49(12):768–74.
Omar IM, Zoga AC, Kavanagh EC, et al. Athletic pubalgia and "sports hernia": optimal MR imaging technique and findings. Radiographics: A Review Publication of the Radiological Society of North America, Inc. 2008;28(5):1415–38.
Brandon CJ, Jacobson JA, Fessell D, et al. Groin pain beyond the hip: how anatomy predisposes to injury as visualized by musculoskeletal ultrasound and MRI. AJR. Am J Roentgenol. 2011;197(5):1190–7.
Tagliafico A, Bignotti B, Rossi F, Sconfienza LM, Messina C, Martinoli C. Ultrasound of the hip joint, soft tissues, and nerves. Semin Musculoskelet Radiol. 2017;21(05):582–8.
Jacobson JA, Khoury V, Brandon CJ. Ultrasound of the groin: techniques, pathology, and pitfalls. Am J Roentgenol. 2015;205(3):513–23.
Tagliafico A, Bignotti B, Cadoni A, Perez MM, Martinoli C. Anatomical study of the iliohypogastric, ilioinguinal, and genitofemoral nerves using high-resolution ultrasound. Muscle Nerve. 2015;51(1):42–8.
Martinoli C, Miguel-Perez M, Padua L, Gandolfo N, Zicca A, Tagliafico A. Imaging of neuropathies about the hip. Eur J Radiol. 2013;82(1):17–26.
Pivec C, Bodner G, Mayer JA, et al. Novel demonstration of the anterior femoral cutaneous nerves using ultrasound. Ultraschall Med, 2018. https://doi.org/10.1055/s-0043-121628.
Zuckerman SL, Kerr ZY, Pierpoint L, Kirby P, Than KD, Wilson TJ. An 11-year analysis of peripheral nerve injuries in high school sports. Physician Sports Med. 2019;47(2):167–73.
Takazawa H, Sudo N, Akoi K. Statistical observation of nerve injuries in athletes. Brain Nerve Injuries. 1971;3:11–7.
Lorei MP, Hershman EB. Peripheral nerve injuries in athletes. Treatment and prevention. Sports Med (Auckland, N.Z.). 1993;16(2):130–47.
Robinson LR. Traumatic injury to peripheral nerves. Muscle Nerve. 2000;23(6):863–73.
Smith JK, Miller ME, Carroll CG, et al. High-resolution ultrasound in combat-related peripheral nerve injuries. Muscle Nerve. 2016;54(6):1139–44.
Padua L, Di Pasquale A, Liotta G, et al. Ultrasound as a useful tool in the diagnosis and management of traumatic nerve lesions. Clinical Neurophysiology: Official Journal of the International Federation of Clinical Neurophysiology. 2013;124(6):1237–43.
Moritz T, Prosch H, Pivec CH, et al. High-resolution ultrasound visualization of the subcutaneous nerves of the forearm: a feasibility study in anatomic specimens. Muscle Nerve. 2014;49(5):676–9.
Bianchi S, Becciolini M, Urigo C. Ultrasound imaging of disorders of small nerves of the extremities: less recognized locations. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2019;38(11):2821–42.
Mifune Y, Inui A, Sakata R, et al. High-resolution ultrasound in the diagnosis of trigger finger and evaluation of response to steroid injection. Skelet Radiol. 2016;45(12):1661–7.
Riegler G, Brugger PC, Gruber GM, Pivec C, Jengojan S, Bodner G. High-resolution ultrasound visualization of pacinian corpuscles. Ultrasound Med Biol. 2018;44(12):2596–601.
Riegler G, Lieba-Samal D, Brugger PC, et al. High-resolution ultrasound visualization of the deep branch of the ulnar nerve. Muscle Nerve. 2017;56(6):1101–7.
De Maeseneer M, Brigido MK, Antic M, et al. Ultrasound of the elbow with emphasis on detailed assessment of ligaments, tendons, and nerves. Eur J Radiol. 2015;84(4):671–81.
Deimel GW, Hurst RW, Sorenson EJ, Boon AJ. Utility of ultrasound-guided near-nerve needle recording for lateral femoral cutaneous sensory nerve conduction study: does it increase reliability compared with surface recording? Muscle Nerve. 2013;47(2):274–6.
Gans P, Van Alfen N. Nerve ultrasound showing Martin–Gruber anastomosis. Muscle Nerve. 2017;56(5):E46–7.
Lucchetta M, Liotta GA, Briani C, et al. Ultrasound diagnosis of peroneal nerve variant in a child with compressive mononeuropathy. J Pediatr Surg. 2011;46(2):405–7.
van Alfen N, Mah JK. Neuromuscular ultrasound: a new tool in your toolbox. Canadian Journal of Neurological Sciences / Journal Canadien des Sciences Neurologiques. 2018;45(5):504–15.
Baute V, Strakowski JA, Reynolds JW, et al. Neuromuscular ultrasound of the brachial plexus: a standardized approach. Muscle Nerve. 2018;58(5):618–24.
Bignotti B, Cadoni A, Assini A, Martinoli C, Tagliafico A. Fascicular involvement in common fibular neuropathy: evaluation with ultrasound. Muscle Nerve. 2016;53(4):532–7.
Jelsing EJ, Presley JC, Maida E, Hangiandreou NJ, Smith J. The effect of magnification on sonographically measured nerve cross-sectional area. Muscle Nerve. 2015;51(1):30–4.
Kalia V, Jacobson JA. Imaging of peripheral nerves of the upper extremity. Radiol Clin N Am. 2019;57(5):1063–71.
Silvestri E, Martinoli C, Derchi LE, Bertolotto M, Chiaramondia M, Rosenberg I. Echotexture of peripheral nerves: correlation between US and histologic findings and criteria to differentiate tendons. Radiology. 1995;197(1):291–6.
Azman D, Hrabac P, Demarin V. Use of multiple ultrasonographic parameters in confirmation of carpal tunnel syndrome. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2018;37(4):879–89.
Boninger ML, Robertson RN, Wolff M, Cooper RA. Upper limb nerve entrapments in elite wheelchair racers. Am J Phys Med Rehabil. 1996;75(3):170–6.
Burnham RS, Steadward RD. Upper extremity peripheral nerve entrapments among wheelchair athletes: prevalence, location, and risk factors. Arch Phys Med Rehabil. 1994;75(5):519–24.
Duncan I, Sullivan P, Lomas F. Sonography in the diagnosis of carpal tunnel syndrome. AJR. Am J Roentgenol. 1999;173(3):681–4.
El Miedany YM, Aty SA, Ashour S. Ultrasonography versus nerve conduction study in patients with carpal tunnel syndrome: substantive or complementary tests? Rheumatology (Oxford, England). 2004;43(7):887–95.
Lee D, van Holsbeeck MT, Janevski PK, Ganos DL, Ditmars DM, Darian VB. Diagnosis of carpal tunnel syndrome. Ultrasound versus electromyography. Radiol Clin N Am. 1999;37(4):859–72. x
Visser LH, Smidt MH, Lee ML. High-resolution sonography versus EMG in the diagnosis of carpal tunnel syndrome. J Neurol Neurosurg Psychiatry. 2008;79(1):63–7.
Wiesler ER, Chloros GD, Cartwright MS, Smith BP, Rushing J, Walker FO. The use of diagnostic ultrasound in carpal tunnel syndrome. J Hand Surg. 2006;31(5):726–32.
Yesildag A, Kutluhan S, Sengul N, et al. The role of ultrasonographic measurements of the median nerve in the diagnosis of carpal tunnel syndrome. Clin Radiol. 2004;59(10):910–5.
Torres-Costoso A, Martinez-Vizcaino V, Alvarez-Bueno C, Ferri-Morales A, Cavero-Redondo I. Accuracy of ultrasonography for the diagnosis of carpal tunnel syndrome: a systematic review and meta-analysis. Arch Phys Med Rehab. 2018;99(4):758–65.e710.
Rahmani M, Ghasemi Esfe AR, Vaziri-Bozorg SM, Mazloumi M, Khalilzadeh O, Kahnouji H. The ultrasonographic correlates of carpal tunnel syndrome in patients with normal electrodiagnostic tests. La Radiologia medica. 2011;116(3):489–96.
Vanderschueren GA, Meys VE, Beekman R. Doppler sonography for the diagnosis of carpal tunnel syndrome: a critical review. Muscle Nerve. 2014;50(2):159–63.
Volz KR, Evans KD, Kanner CD, Dickerson JA. Detection of intraneural median nerve microvascularity using contrast-enhanced sonography: a pilot study. Journal of Ultrasound in Medicine : Official Journal of the American Institute of Ultrasound in Medicine. 2016;35(6):1309–16.
Chen J, Chen L, Wu L, et al. Value of superb microvascular imaging ultrasonography in the diagnosis of carpal tunnel syndrome: compared with color Doppler and power Doppler. Medicine. 2017;96(21):e6862.
Karahan AY, Arslan S, Ordahan B, Bakdik S, Ekiz T. Superb microvascular imaging of the median nerve in carpal tunnel syndrome: an electrodiagnostic and ultrasonographic study. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2018;37(12):2855–61.
Campbell WW. Ulnar neuropathy at the elbow. Muscle Nerve. 2000;23(4):450–2.
Olivo R, Tsao B. Peripheral nerve injuries in sport. Neurol Clin. 2017;35(3):559–72.
Łasecki M, Olchowy C, Pawluś A, Zaleska-Dorobisz U. The Snapping elbow syndrome as a reason for chronic elbow neuralgia in a tennis player - MR, US and sonoelastography evaluation. Pol J Radiol. 2014;79:467–71.
Ellegaard HR, Fuglsang-Frederiksen A, Hess A, Johnsen B, Qerama E. High-resolution ultrasound in ulnar neuropathy at the elbow: a prospective study. Muscle Nerve. 2015;52(5):759–66.
Schertz M, Mutschler C, Masmejean E, Silvera J. High-resolution ultrasound in etiological evaluation of ulnar neuropathy at the elbow. Eur J Radiol. 2017;95:111–7.
Chang KV, Wu WT, Han DS, Özçakar L. Ulnar nerve cross-sectional area for the diagnosis of cubital tunnel syndrome: a meta-analysis of ultrasonographic measurements. Arch Phys Med Rehabil. 2018;99(4):743–57.
Alrajeh M, Preston DC. Neuromuscular ultrasound in electrically non-localizable ulnar neuropathy. Muscle Nerve. 2018;58(5):655–9.
Peer S, Kovacs P, Harpf C, Bodner G. High-resolution sonography of lower extremity peripheral nerves: anatomic correlation and spectrum of disease. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Med. 2002;21(3):315–22.
Masakado Y, Kawakami M, Suzuki K, Abe L, Ota T, Kimura A. Clinical neurophysiology in the diagnosis of peroneal nerve palsy. Keio J Med. 2008;57(2):84–9.
Hainline BW. Peripheral nerve injury in sports. Continuum (Minneapolis, Minn.). 2014;20(6 Sports Neurology):1605–28.
Krivickas LS, Wilbourn AJ. Peripheral nerve injuries in athletes: a case series of over 200 injuries. Semin Neurol. 2000;20(2):225–32.
Bucklan JN, Morren JA, Shook SJ. Ultrasound in the diagnosis and management of fibular mononeuropathy. Muscle Nerve. 2019;60(5):544–8.
Bignotti B, Assini A, Signori A, Martinoli C, Tagliafico A. Ultrasound versus MRI in common fibular neuropathy. Muscle Nerve. 2017;55(6):849–57.
Fantino O. Role of ultrasound in posteromedial tarsal tunnel syndrome: 81 cases. J Ultrasound. 2014;17(2):99–112.
Tsukamoto H, Granata G, Coraci D, Paolasso I, Padua L. Ultrasound and neurophysiological correlation in common fibular nerve conduction block at fibular head. Clinical Neurophysiology: Official Journal of the International Federation of Clinical Neurophysiology. 2014;125(7):1491–5.
Wu WT, Chang KV, Özçakar L. Ultrasound facilitates the diagnosis of tarsal tunnel syndrome: intraneural ganglion cyst of the tibial nerve. J Ultrasound. 2019;22(1):95–8.
Kho KH, Blijham PJ, Zwarts MJ. Meralgia paresthetica after strenuous exercise. Muscle Nerve. 2005;31(6):761–3.
Macgregor J, Moncur JA. Meralgia paraesthetica--a sports lesion in girl gymnasts. Br J Sports Med. 1977;11(1):16–9.
Otoshi K, Itoh Y, Tsujino A, Kikuchi S. Case report: meralgia paresthetica in a baseball pitcher. Clin Orthop Relat Res. 2008;466(9):2268–70.
Ulkar B, Yildiz Y, Kunduracioglu B. Meralgia paresthetica: a long-standing performance-limiting cause of anterior thigh pain in a soccer player. Am J Sports Med. 2003;31(5):787–9.
Esser S, Thurston M, Nalluri K, Muzaurieta A. "Numb-Leg" in a crossfit athlete: a case presentation. PM & R: The Journal of Injury, Function, and Rehabilitation. 2017;9(8):834–6.
Seror P. Somatosensory evoked potentials for the electrodiagnosis of meralgia paresthetica. Muscle Nerve. 2004;29(2):309–12.
Aravindakannan T, Wilder-Smith EP. High-resolution ultrasonography in the assessment of meralgia paresthetica. Muscle Nerve. 2012;45(3):434–5.
Tagliafico A, Serafini G, Lacelli F, Perrone N, Valsania V, Martinoli C. Ultrasound-guided treatment of meralgia paresthetica (lateral femoral cutaneous neuropathy): technical description and results of treatment in 20 consecutive patients. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2011;30(10):1341–6.
Cunnane M, Pratten M, Loughna S. A retrospective study looking at the incidence of ‘stinger' injuries in professional rugby union players. Br J Sports Med 2011;45(15):A19.
Safran MR. Nerve injury about the shoulder in athletes, part 2: long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med. 2004;32(4):1063–76.
Stewman C, Vitanzo PC Jr, Harwood MI. Neurologic thoracic outlet syndrome: summarizing a complex history and evolution. Curr Sports Med Rep. 2014;13(2):100–6.
Arányi Z, Csillik A, Böhm J, Schelle T. Ultrasonographic identification of fibromuscular bands associated with neurogenic thoracic outlet syndrome: the "wedge-sickle" sign. Ultrasound Med Biol. 2016;42(10):2357–66.
Pesser N, Teijink JAW, Vervaart K, et al. Value of ultrasound in the diagnosis of neurogenic thoracic outlet syndrome. European Journal of Vascular and Endovascular Surgery: The Official Journal of the European Society for Vascular Surgery. 2020;59(5):852–3.
Sucher BM. Thoracic outlet syndrome-postural type: ultrasound imaging of pectoralis minor and brachial plexus abnormalities. PM & R: The Journal of Injury, Function, and Rehabilitation. 2012;4(1):65–72.
Shutze W, Richardson B, Shutze R, et al. Midterm and long-term follow-up in competitive athletes undergoing thoracic outlet decompression for neurogenic thoracic outlet syndrome. J Vasc Surg. 2017;66(6):1798–805.
Jordan SE, Ahn SS, Gelabert HA. Combining ultrasonography and electromyography for botulinum chemodenervation treatment of thoracic outlet syndrome: comparison with fluoroscopy and electromyography guidance. Pain physician. 2007;10(4):541–6.
Torriani M, Gupta R, Donahue DM. Sonographically guided anesthetic injection of anterior scalene muscle for investigation of neurogenic thoracic outlet syndrome. Skelet Radiol. 2009;38(11):1083–7.
Graif M, Martinoli C, Rochkind S, et al. Sonographic evaluation of brachial plexus pathology. Eur Radiol. 2004;14(2):193–200.
Abraham P, Saumet JL, Chevalier JM. External iliac artery endofibrosis in athletes. Sports Med (Auckland, N.Z.). 1997;24(4):221–6.
Menon D, Onida S, Davies AH. Overview of arterial pathology related to repetitive trauma in athletes. J Vasc Surg. 2019;70(2):641–50.
Nakamura KM, Skeik N, Shepherd RF, Wennberg PW. External iliac vein thrombosis in an athletic cyclist with a history of external iliac artery endofibrosis and thrombosis. Vasc Endovasc Surg. 2011;45(8):761–4.
Willson TD, Revesz E, Podbielski FJ, Blecha MJ. External iliac artery dissection secondary to endofibrosis in a cyclist. J Vasc Surg. 2010;52(1):219–21.
Abraham P, Leftheriotis G, Bourre Y, Chevalier JM, Saumet JL. Echography of external iliac artery endofibrosis in cyclists. Am J Sports Med. 1993;21(6):861–3.
Fernandez-Garcia B, Alvarez Fernandez J, Vega Garcia F, et al. Diagnosing external iliac endofibrosis by postexercise ankle to arm index in cyclists. Med Sci Sports Exerc. 2002;34(2):222–7.
Joy SM, Raudales R. Popliteal artery entrapment syndrome. Curr Sports Med Reports. 2015;14(5):364–7.
Cho KJ, Kang S, Ko S, Baek J, Kim Y, Park NK. Neurovascular compression caused by popliteus muscle enlargement without discrete trauma. Ann Rehabil Med. 2016;40(3):545–50.
Levien LJ, Veller MG. Popliteal artery entrapment syndrome: more common than previously recognized. J Vasc Surg. 1999;30(4):587–98.
Sinha S, Houghton J, Holt PJ, Thompson MM, Loftus IM, Hinchliffe RJ. Popliteal entrapment syndrome. J Vascular Surg. 2012;55(1):252–62.e230.
Erdoes LS, Devine JJ, Bernhard VM, Baker MR, Berman SS, Hunter GC. Popliteal vascular compression in a normal population. J Vasc Surg. 1994;20(6):978–86.
Jackson MR. Upper extremity arterial injuries in athletes. Semin Vasc Surg. 2003;16(3):232–9.
Rohrer MJ, Cardullo PA, Pappas AM, Phillips DA, Wheeler HB. Axillary artery compression and thrombosis in throwing athletes. J Vasc Surg. 1990;11(6):761–8; discussion 768-769.
Schneider K, Kasparyan NG, Altchek DW, Fantini GA, Weiland AJ. An aneurysm involving the axillary artery and its branch vessels in a major league baseball pitcher. A case report and review of the literature. Am J Sports Med. 1999;27(3):370–5.
van de Pol D, Kuijer PP, Langenhorst T, Maas M. High prevalence of self-reported symptoms of digital ischemia in elite male volleyball players in the Netherlands: a cross-sectional national survey. Am J Sports Med. 2012;40(10):2296–302.
van de Pol D, Maas M, Terpstra A, et al. Ultrasound assessment of the posterior circumflex humeral artery in elite volleyball players: aneurysm prevalence, anatomy, branching pattern and vessel characteristics. Eur Radiol. 2017;27(3):889–98.
van de Pol D, Maas M, Terpstra A, Pannekoek-Hekman M, Kuijer PP, Planken RN. B-Mode sonographic assessment of the posterior circumflex humeral artery: the SPI-US Protocol-A technical procedure in 4 steps. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2016;35(5):1015–20.
Nichols AW. Diagnosis and management of thoracic outlet syndrome. Curr Sports Med Rep. 2009;8(5):240–9.
Daniels B, Michaud L, Sease F Jr, Cassas KJ, Gray BH. Arterial thoracic outlet syndrome. Curr Sports Med Rep. 2014;13(2):75–80.
Farrar TA, Rankin G, Chatfield M. Venous thoracic outlet syndrome: approach to diagnosis and treatment with focus on affected athletes. Curr Sports Med Reports. 2014;13(2):81–5.
Demondion X, Vidal C, Herbinet P, Gautier C, Duquesnoy B, Cotten A. Ultrasonographic assessment of arterial cross-sectional area in the thoracic outlet on postural maneuvers measured with power Doppler ultrasonography in both asymptomatic and symptomatic populations. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2006;25(2):217–24.
Longley DG, Yedlicka JW, Molina EJ, Schwabacher S, Hunter DW, Letourneau JG. Thoracic outlet syndrome: evaluation of the subclavian vessels by color duplex sonography. AJR. Am J Roentgenol. 1992;158(3):623–30.
Coggan AR, Coyle EF. Reversal of fatigue during prolonged exercise by carbohydrate infusion or ingestion. J Appl Physiol (Bethesda, Md. : 1985). 1987;63(6):2388–95.
Coggan AR, Coyle EF. Carbohydrate ingestion during prolonged exercise: effects on metabolism and performance. Exerc Sport Sci Rev. 1991;19:1–40.
Coyle EF, Coggan AR, Hemmert MK, Ivy JL. Muscle glycogen utilization during prolonged strenuous exercise when fed carbohydrate. J Appl Physiol (Bethesda, Md. : 1985). 1986;61(1):165–72.
Hill JC, Millan IS. Validation of musculoskeletal ultrasound to assess and quantify muscle glycogen content. A novel approach. Phys Sportsmed. 2014;42(3):45–52.
Nieman DC, Shanely RA, Zwetsloot KA, Meaney MP, Farris GE. Ultrasonic assessment of exercise-induced change in skeletal muscle glycogen content. BMC Sports Sci Med Rehab. 2015;7:9.
Bone JL, Ross ML, Tomcik KA, Jeacocke NA, Hawley JA, Burke LM. Ultrasound technology fails to provide indirect estimate of muscle glycogen concentration: 1891 Board #43 June 2, 2: 00 PM - 3: 30 PM. Med Sci Sports Exercise. 2016;48(5S).
Fogelholm M. Effects of bodyweight reduction on sports performance. Sports Medicine (Auckland, N.Z.). 1994;18(4):249–67.
Ramirez ME. Measurement of subcutaneous adipose tissue using ultrasound images. Am J Phys Anthropol. 1992;89(3):347–57.
Muller W, Lohman TG, Stewart AD, et al. Subcutaneous fat patterning in athletes: selection of appropriate sites and standardisation of a novel ultrasound measurement technique: ad hoc working group on body composition, health and performance, under the auspices of the IOC Medical Commission. Br J Sports Med. 2016;50(1):45–54.
Storchle P, Muller W, Sengeis M, et al. Standardized ultrasound measurement of subcutaneous fat patterning: high reliability and accuracy in groups ranging from lean to obese. Ultrasound Med Biol. 2017;43(2):427–38.
Müller W, Horn M, Fürhapter-Rieger A, et al. Body composition in sport: a comparison of a novel ultrasound imaging technique to measure subcutaneous fat tissue compared with skinfold measurement. Br J Sports Med. 2013;47(16):1028.
Prado-Costa R, Rebelo J, Monteiro-Barroso J, Preto AS. Ultrasound elastography: compression elastography and shear-wave elastography in the assessment of tendon injury. Insights Into Imaging. 2018;9(5):791–814.
Karatekin YS, Karaismailoglu B, Kaynak G, et al. Does elasticity of Achilles tendon change after suture applications? Evaluation of repair area by acoustic radiation force impulse elastography. J Orthop Surg Res. 2018;13(1):45.
Nightingale K. Acoustic Radiation Force Impulse (ARFI) imaging: a review. Curr Med Imaging Rev. 2011;7(4):328–39.
Cho SH, Lee JY, Han JK, Choi BI. Acoustic radiation force impulse elastography for the evaluation of focal solid hepatic lesions: preliminary findings. Ultrasound Med Biol. 2010;36(2):202–8.
Kural Rahatli F, Turnaoglu H, Haberal KM, et al. Acoustic radiation force impulse elastography findings of achilles tendons in patients on chronic hemodialysis and in renal transplant patients. Experimental and Clinical Transplantation: Official Journal of the Middle East Society for Organ Transplantation. 2018;
De Zordo T, Chhem R, Smekal V, et al. Real-time sonoelastography: findings in patients with symptomatic achilles tendons and comparison to healthy volunteers. Ultraschall in der Medizin (Stuttgart, Germany: 1980). 2010;31(4):394–400.
Klauser AS, Miyamoto H, Tamegger M, et al. Achilles tendon assessed with sonoelastography: histologic agreement. Radiology. 2013;267(3):837–42.
Ooi CC, Richards PJ, Maffulli N, et al. A soft patellar tendon on ultrasound elastography is associated with pain and functional deficit in volleyball players. J Sci Med Sport. 2016;19(5):373–8.
De Zordo T, Lill SR, Fink C, et al. Real-time sonoelastography of lateral epicondylitis: comparison of findings between patients and healthy volunteers. AJR. Am J Roentgenol. 2009;193(1):180–5.
Ahn KS, Kang CH, Hong SJ, Jeong WK. Ultrasound elastography of lateral epicondylosis: clinical feasibility of quantitative elastographic measurements. AJR. Am J Roentgenol. 2014;202(5):1094–9.
Park G, Kwon D, Park J. Diagnostic confidence of sonoelastography as adjunct to greyscale ultrasonography in lateral elbow tendinopathy. Chin Med J. 2014;127(17):3110–5.
Kocyigit F, Kuyucu E, Kocyigit A, Herek DT, Savkin R, Aslan UB. Investigation of biomechanical characteristics of intact supraspinatus tendons in subacromial impingement syndrome: a cross-sectional study with real-time sonoelastography. Am J Phys Med Rehabil. 2016;95(8):588–96.
Klauser AS, Pamminger M, Halpern EJ, et al. Extensor tendinopathy of the elbow assessed with sonoelastography: histologic correlation. Eur Radiol. 2017;27(8):3460–6.
Klauser AS, Pamminger MJ, Halpern EJ, et al. Sonoelastography of the common flexor tendon of the elbow with histologic agreement: a cadaveric study. Radiology. 2017;283(2):486–91.
Seo JB, Yoo JS, Ryu JW. The accuracy of sonoelastography in fatty degeneration of the supraspinatus: a comparison of magnetic resonance imaging and conventional ultrasonography. J Ultrasound. 2014;17(4):279–85.
Seo JB, Yoo JS, Ryu JW. Sonoelastography findings of supraspinatus tendon in rotator cuff tendinopathy without tear: comparison with magnetic resonance images and conventional ultrasonography. J Ultrasound. 2015;18(2):143–9.
Tudisco C, Bisicchia S, Stefanini M, Antonicoli M, Masala S, Simonetti G. Tendon quality in small unilateral supraspinatus tendon tears. Real-time sonoelastography correlates with clinical findings. Knee Surgery, Sports Traumatology, Arthroscopy : Official Journal of the ESSKA. 2015;23(2):393–8.
Lee SU, Joo SY, Kim SK, Lee SH, Park SR, Jeong C. Real-time sonoelastography in the diagnosis of rotator cuff tendinopathy. J Shoulder Elb Surg. 2016;25(5):723–9.
Seo JB, Yoo JS, Ryu JW. Sonoelastography findings of biceps tendinitis and tendinosis. J Ultrasound. 2014;17(4):271–7.
Sconfienza LM, Silvestri E, Cimmino MA. Sonoelastography in the evaluation of painful Achilles tendon in amateur athletes. Clin Exp Rheumatol. 2010;28(3):373–8.
Tan S, Kudas S, Ozcan AS, et al. Real-time sonoelastography of the Achilles tendon: pattern description in healthy subjects and patients with surgically repaired complete ruptures. Skelet Radiol. 2012;41(9):1067–72.
Busilacchi A, Olivieri M, Ulisse S, et al. Real-time sonoelastography as novel follow-up method in Achilles tendon surgery. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA. 2016;24(7):2124–32.
Brage K, Hjarbaek J, Kjaer P, Ingwersen KG, Juul-Kristensen B. Ultrasonic strain elastography for detecting abnormalities in the supraspinatus tendon: an intra- and inter-rater reliability study. BMJ Open. 2019;9(5):e027725.
Gennisson JL, Deffieux T, Fink M, Tanter M. Ultrasound elastography: principles and techniques. Dia Intervent Imaging. 2013;94(5):487–95.
Dirrichs T, Quack V, Gatz M, Tingart M, Kuhl CK, Schrading S. Shear Wave Elastography (SWE) for the evaluation of patients with tendinopathies. Acad Radiol. 2016;23(10):1204–13.
Coombes BK, Tucker K, Vicenzino B, et al. Achilles and patellar tendinopathy display opposite changes in elastic properties: A shear wave elastography study. Scand J Med Sci Sports. 2018;28(3):1201–8.
Aubry S, Nueffer JP, Tanter M, Becce F, Vidal C, Michel F. Viscoelasticity in Achilles tendonopathy: quantitative assessment by using real-time shear-wave elastography. Radiology. 2015;274(3):821–9.
Chen XM, Cui LG, He P, Shen WW, Qian YJ, Wang JR. Shear wave elastographic characterization of normal and torn achilles tendons: a pilot study. Journal of Ultrasound in Medicine : Official Journal of the American Institute of Ultrasound in Medicine. 2013;32(3):449–55.
Zhang LN, Wan WB, Wang YX, et al. Evaluation of elastic stiffness in healing achilles tendon after surgical repair of a tendon rupture using in vivo ultrasound shear wave elastography. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research. 2016;22:1186–91.
Yoshida K, Itoigawa Y, Maruyama Y, Kaneko K. Healing Process of Gastrocnemius Muscle Injury on Ultrasonography Using B-Mode Imaging, Power Doppler Imaging, and Shear Wave Elastography. Journal of Ultrasound in Medicine : Official Journal of the American Institute of Ultrasound in Medicine. 2019;38(12):3239–46.
Washburn N, Onishi K, Wang JH. Ultrasound elastography and ultrasound tissue characterisation for tendon evaluation. J Orthopaedic Transl. 2018;15:9–20.
van Schie HT, Bakker EM, Jonker AM, van Weeren PR. Efficacy of computerized discrimination between structure-related and non-structure-related echoes in ultrasonographic images for the quantitative evaluation of the structural integrity of superficial digital flexor tendons in horses. Am J Vet Res. 2001;62(7):1159–66.
Docking SI, Cook J. Pathological tendons maintain sufficient aligned fibrillar structure on ultrasound tissue characterization (UTC). Scand J Med Sci Sports. 2016;26(6):675–83.
Rosengarten SD, Cook JL, Bryant AL, Cordy JT, Daffy J, Docking SI. Australian football players' Achilles tendons respond to game loads within 2 days: an ultrasound tissue characterisation (UTC) study. Br J Sports Med. 2015;49(3):183–7.
Docking SI, Rosengarten SD, Cook J. Achilles tendon structure improves on UTC imaging over a 5-month pre-season in elite Australian football players. Scand J Med Sci Sports. 2016;26(5):557–63.
van Ark M, Rio E, Cook J, et al. Clinical improvements are not explained by changes in tendon structure on ultrasound tissue characterization after an exercise program for patellar tendinopathy. Am J Phys Med Rehabil. 2018;97(10):708–14.
Pereira CS, Santos RCG, Whiteley R, Finni T. Reliability and methodology of quantitative assessment of harvested and unharvested patellar tendons of ACL injured athletes using ultrasound tissue characterization. BMC Sports Science, Medicine & Rehabilitation. 2019;11:12.
Torres RJL, Hattori S, Kato Y, Yamada S, Ohuchi H. Ultrasonography and return to play of the different clinical grading of quadriceps contusions: a case series. J Med Ultrasonics (2001). 2018;45(2):375–80.
Guillodo Y, Bouttier R, Saraux A. Value of sonography combined with clinical assessment to evaluate muscle injury severity in athletes. J Athl Train. 2011;46(5):500–4.
Yoshida K, Itoigawa Y, Maruyama Y, Kaneko K. Healing process of gastrocnemius muscle injury on ultrasonography using B-mode imaging, power doppler imaging, and shear wave elastography. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2019;
Lee JH, Lee JU, Yoo SW. Accuracy and efficacy of ultrasound-guided pes anserinus bursa injection. J Clin Ultrasound: JCU. 2019;47(2):77–82.
Hashiuchi T, Sakurai G, Morimoto M, Komei T, Takakura Y, Tanaka Y. Accuracy of the biceps tendon sheath injection: ultrasound-guided or unguided injection? A randomized controlled trial. J Shoulder Elb Surg. 2011;20(7):1069–73.
Brull R, Perlas A, Cheng PH, Chan VW. Minimizing the risk of intravascular injection during ultrasound-guided peripheral nerve blockade. Anesthesiology. 2008;109(6):1142; author reply 1144, 1144-1145.
Zhang M, Pessina MA, Higgs JB, Kissin EY. A vascular obstacle in ultrasound-guided hip joint injection. J Med Ultrasound. 2018;26(2):77–80.
Carra BJ, Bui-Mansfield LT, O'Brien SD, Chen DC. Sonography of musculoskeletal soft-tissue masses: techniques, pearls, and pitfalls. Am J Roentgenol. 2014;202(6):1281–90.
Lento PH, Strakowski JA. The use of ultrasound in guiding musculoskeletal interventional procedures. Phys Med Rehabil Clin N Am. 2010;21(3):559–83.
Jacobson JA, Kim SM, Brigido MK. Ultrasound-guided percutaneous tenotomy. Semin Musculoskelet Radiol. 2016;20(5):414–21.
Koh JS, Mohan PC, Howe TS, et al. Fasciotomy and surgical tenotomy for recalcitrant lateral elbow tendinopathy: early clinical experience with a novel device for minimally invasive percutaneous microresection. Am J Sports Med. 2013;41(3):636–44.
Rojo-Manaute JM, Capa-Grasa A, Chana-Rodríguez F, et al. Ultra-minimally invasive ultrasound-guided carpal tunnel release: a randomized clinical trial. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2016;35(6):1149–57.
Nikolaou VS, Malahias MA, Kaseta MK, Sourlas I, Babis GC. Comparative clinical study of ultrasound-guided A1 pulley release vs open surgical intervention in the treatment of trigger finger. World J Orthopedics. 2017;8(2):163–9.
Strakowski JA. Ultrasound-guided peripheral nerve procedures. Phys Med Rehabil Clin N Am. 2016;27(3):687–715.
Brull R, Hadzic A, Reina MA, Barrington MJ. Pathophysiology and etiology of nerve injury following peripheral nerve blockade. Reg Anesth Pain Med. 2015;40(5):479–90.
Finnoff JT, Hall MM, Adams E, et al. American medical society for sports medicine position statement: interventional musculoskeletal ultrasound in sports medicine. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine. 2015;25(1):6–22.
de Witte PB, Kolk A, Overes F, Nelissen R, Reijnierse M. Rotator cuff calcific tendinitis: ultrasound-guided needling and lavage versus subacromial corticosteroids: five-year outcomes of a randomized controlled trial. Am J Sports Med. 2017;45(14):3305–14.
de Witte PB, Selten JW, Navas A, et al. Calcific tendinitis of the rotator cuff: a randomized controlled trial of ultrasound-guided needling and lavage versus subacromial corticosteroids. Am J Sports Med. 2013;41(7):1665–73.
Klontzas ME, Vassalou EE, Karantanas AH. Calcific tendinopathy of the shoulder with intraosseous extension: outcomes of ultrasound-guided percutaneous irrigation. Skelet Radiol. 2017;46(2):201–8.
Lanza E, Banfi G, Serafini G, et al. Ultrasound-guided percutaneous irrigation in rotator cuff calcific tendinopathy: what is the evidence? A systematic review with proposals for future reporting. Eur Radiol. 2015;25(7):2176–83.
Bazzocchi A, Pelotti P, Serraino S, et al. Ultrasound imaging-guided percutaneous treatment of rotator cuff calcific tendinitis: success in short-term outcome. Br J Radiol. 2016;89(1057):20150407.
Oudelaar BW, Schepers-Bok R, Ooms EM. Huis In 't Veld R, Vochteloo AJ. Needle aspiration of calcific deposits (NACD) for calcific tendinitis is safe and effective: Six months follow-up of clinical results and complications in a series of 431 patients. Eur J Radiol. 2016;85(4):689–94.
Arirachakaran A, Boonard M, Yamaphai S, Prommahachai A, Kesprayura S, Kongtharvonskul J. Extracorporeal shock wave therapy, ultrasound-guided percutaneous lavage, corticosteroid injection and combined treatment for the treatment of rotator cuff calcific tendinopathy: a network meta-analysis of RCTs. European Journal of Orthopaedic Surgery & Traumatology: Orthopedie Traumatologie. 2017;27(3):381–90.
Gatt DL, Charalambous CP. Ultrasound-guided barbotage for calcific tendonitis of the shoulder: a systematic review including 908 patients. Arthroscopy. 2014;30(9):1166–72.
Wu YC, Tsai WC, Tu YK, Yu TY. Comparative effectiveness of nonoperative treatments for chronic calcific tendinitis of the shoulder: a systematic review and network meta-analysis of randomized controlled trials. Arch Physical Med Rehab. 2017;98(8):1678–92.e1676.
Jo H, Kim G, Baek S, Park HW. Calcific tendinopathy of the gluteus medius mimicking lumbar radicular pain successfully treated with barbotage: a case report. Ann Rehabil Med. 2016;40(2):368–72.
Abate M, Salini V, Schiavone C. Ultrasound-guided percutaneous lavage in the treatment of calcific tendinopathy of elbow extensor tendons: a case report. Malaysian Orthopaedic J. 2016;10(2):53–5.
Hall MM, Rajasekaran S. Ultrasound-guided scraping for chronic patellar tendinopathy: a case presentation. PM & R: the Journal of Injury, Function, and Rehabilitation. 2016;8(6):593–6.
Alfredson H. Ultrasound and Doppler-guided mini-surgery to treat midportion Achilles tendinosis: results of a large material and a randomised study comparing two scraping techniques. Br J Sports Med. 2011;45(5):407–10.
Humphrey J, Chan O, Crisp T, et al. The short-term effects of high volume image guided injections in resistant non-insertional Achilles tendinopathy. J Sci Med Sport. 2010;13(3):295–8.
Boesen AP, Hansen R, Boesen MI, Malliaras P, Langberg H. Effect of high-volume injection, platelet-rich plasma, and sham treatment in chronic midportion achilles tendinopathy: a randomized double-blinded prospective study. Am J Sports Med. 2017;45(9):2034–43.
Chan O, O'Dowd D, Padhiar N, et al. High volume image guided injections in chronic Achilles tendinopathy. Disabil Rehabil. 2008;30(20-22):1697–708.
Maffulli N, Spiezia F, Longo UG, Denaro V, Maffulli GD. High volume image guided injections for the management of chronic tendinopathy of the main body of the Achilles tendon. Physical Therapy in Sport: Official Journal of the Association of Chartered Physiotherapists in Sports Medicine. 2013;14(3):163–7.
Abate M, Di Carlo L, Verna S, Di Gregorio P, Schiavone C, Salini V. Synergistic activity of platelet rich plasma and high volume image guided injection for patellar tendinopathy. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA. 2018;26(12):3645–51.
Crisp T, Khan F, Padhiar N, et al. High volume ultrasound guided injections at the interface between the patellar tendon and Hoffa's body are effective in chronic patellar tendinopathy: a pilot study. Disabil Rehabil. 2008;30(20-22):1625–34.
Maffulli N, Del Buono A, Oliva F, Testa V, Capasso G, Maffulli G. High-volume image-guided injection for recalcitrant patellar tendinopathy in athletes. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine. 2016;26(1):12–6.
Morton S, Chan O, King J, et al. High volume image-guided Injections for patellar tendinopathy: a combined retrospective and prospective case series. Muscles Ligaments Tendons J. 2014;4(2):214–9.
Morton S, Chan O, Ghozlan A, Price J, Perry J, Morrissey D. High volume image guided injections and structured rehabilitation in shoulder impingement syndrome: a retrospective study. Muscles Ligaments Tendons J. 2015;5(3):195–9.
Wheeler PC, Mahadevan D, Bhatt R, Bhatia M. A comparison of two different high-volume image-guided injection procedures for patients with chronic noninsertional achilles tendinopathy: a pragmatic retrospective cohort study. J Foot Ankle Surg. 2016;55(5):976–9.
Morton S, Chan O, Price J, et al. High volume image-guided injections and structured rehabilitation improve greater trochanter pain syndrome in the short and medium term: a combined retrospective and prospective case series. Muscles Ligaments Tendons J. 2015;5(2):73–87.
Gilberts EC, Beekman WH, Stevens HJ, Wereldsma JC. Prospective randomized trial of open versus percutaneous surgery for trigger digits. J Hand Surg. 2001;26(3):497–500.
Nakamichi K, Tachibana S. Ultrasonographically assisted carpal tunnel release. J Hand Surg. 1997;22(5):853–62.
Nakamichi K, Tachibana S, Yamamoto S, Ida M. Percutaneous carpal tunnel release compared with mini-open release using ultrasonographic guidance for both techniques. J Hand Surg. 2010;35(3):437–45.
McShane JM, Slaff S, Gold JE, Nazarian LN. Sonographically guided percutaneous needle release of the carpal tunnel for treatment of carpal tunnel syndrome: preliminary report. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2012;31(9):1341–9.
Guo XY, Xiong MX, Lu M, et al. Ultrasound-guided needle release of the transverse carpal ligament with and without corticosteroid injection for the treatment of carpal tunnel syndrome. J Orthop Surg Res. 2018;13(1):69.
Guo XY, Xiong MX, Zhao Y, et al. Comparison of the clinical effectiveness of ultrasound-guided corticosteroid injection with and without needle release of the transverse carpal ligament in carpal tunnel syndrome. Eur Neurol. 2017;78(1-2):33–40.
Guo D, Guo D, Guo J, Malone DG, Wei N, McCool LC. A cadaveric study for the improvement of thread carpal tunnel release. J Hand Surg. 2016;41(10):e351–7.
Guo D, Guo D, Guo J, Schmidt SC, Lytie RM. A clinical study of the modified thread carpal tunnel release. Hand (New York, N.Y.). 2017;12(5):453–60.
Burnham R, Playfair L, Loh E, Roberts S, Agur A. Evaluation of the effectiveness and safety of ultrasound-guided percutaneous carpal tunnel release: a cadaveric study. Am J Phys Med Rehabil. 2017;96(7):457–63.
Capa-Grasa A, Rojo-Manaute JM, Rodriguez FC, Martin JV. Ultra minimally invasive sonographically guided carpal tunnel release: an external pilot study. Orthopaedics & Traumatology, Surgery & Research: OTSR. 2014;100(3):287–92.
Rojo-Manaute JM, Capa-Grasa A, Rodriguez-Maruri GE, Moran LM, Martinez MV, Martin JV. Ultra-minimally invasive sonographically guided carpal tunnel release: anatomic study of a new technique. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2013;32(1):131–42.
Chern TC, Kuo LC, Shao CJ, Wu TT, Wu KC, Jou IM. Ultrasonographically guided percutaneous carpal tunnel release: early clinical experiences and outcomes. Arthroscopy: The Journal of Arthroscopic & Related Surgery : Official Publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2015;31(12):2400–10.
Petrover D, Hakime A, Silvera J, Richette P, Nizard R. Ultrasound-guided surgery for carpal tunnel syndrome: a new interventional procedure. Semin Interv Radiol. 2018;35(4):248–54.
Petrover D, Silvera J, De Baere T, Vigan M, Hakime A. Percutaneous ultrasound-guided carpal tunnel release: study upon clinical efficacy and safety. Cardiovasc Intervent Radiol. 2017;40(4):568–75.
Henning PT, Yang L, Awan T, Lueders D, Pourcho AM. Minimally invasive ultrasound-guided carpal tunnel release: preliminary clinical results. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2018;37(11):2699–706.
Henning T, Lueders D, Chang K, Yang L. Ultrasound-Guided carpal tunnel release using dynamic expansion of the transverse safe zone in a patient with postpolio syndrome: a case report. PM & R: The Journal of Injury, Function, and Rehabilitation. 2018;10(10):1115–8.
Latzka EW, Henning PT, Pourcho AM. Sonographic changes after ultrasound-guided release of the transverse carpal ligament: a case report. PM & R: The Journal of Injury, Function, and Rehabilitation. 2018;10(10):1125–9.
Beckman JP, Sellon JL, Lachman N, Smith J. Sonographically detected transligamentous median nerve branch. Am J Phys Med Rehabil. 2018;97(9):e87–8.
Sytsma TT, Ryan HS, Lachman N, Kakar S, Smith J. Anatomic relationship between the hook of the hamate and the distal transverse carpal ligament: implications for ultrasound-guided carpal tunnel release. Am J Phys Med Rehabil. 2018;97(7):482–7.
Rajeswaran G, Healy JC, Lee JC. Percutaneous release procedures: trigger finger and carpal tunnel. Semin Musculoskelet Radiol. 2016;20(5):432–40.
Rajeswaran G, Lee JC, Eckersley R, Katsarma E, Healy JC. Ultrasound-guided percutaneous release of the annular pulley in trigger digit. Eur Radiol. 2009;19(9):2232–7.
Smith J, Rizzo M, Lai JK. Sonographically guided percutaneous first annular pulley release: cadaveric safety study of needle and knife techniques. J Ultrasound Med. 2010;29(11):1531–42.
Rojo-Manaute JM, Rodriguez-Maruri G, Capa-Grasa A, Chana-Rodriguez F, Soto Mdel V, Martin JV. Sonographically guided intrasheath percutaneous release of the first annular pulley for trigger digits, part 1: clinical efficacy and safety. Journal of Ultrasound in Medicine : Official Journal of the American Institute of Ultrasound in Medicine. 2012;31(3):417–24.
Guo D, Guo D, Guo J, McCool LC, Tonkin B. A cadaveric study of the thread trigger finger release: the first annular pulley transection through thread transecting technique. Hand (New York, N.Y.). 2018;13(2):170–5.
Pan M, Sheng S, Fan Z, et al. Ultrasound-guided percutaneous release of A1 pulley by using a needle knife: a prospective study of 41 cases. Front Pharmacol. 2019;10:267.
Rojo-Manaute JM, Capa-Grasa A, Del Cerro-Gutierrez M, Martinez MV, Chana-Rodriguez F, Martin JV. Sonographically guided intrasheath percutaneous release of the first annular pulley for trigger digits, part 2: randomized comparative study of the economic impact of 3 surgical models. Journal of Ultrasound in Medicine : Official Journal of the American Institute of Ultrasound in Medicine. 2012;31(3):427–38.
Marcos AI, Villanueva-Martinez M, Barrett SL, Rodriguez-Collazo ER, Sanz-Ruiz P. Ultrasound-guided release of the tibial nerve and its distal branches: a cadaveric study. J Ultrasound Med. 2018;
Lapegue F, Andre A, Pasquier Bernachot E, et al. US-guided percutaneous release of the first extensor tendon compartment using a 21-gauge needle in de Quervain’s disease: a prospective study of 35 cases. Eur Radiol. 2018;28(9):3977–85.
Levy B, Ducat A, Gaudin P, et al. Ultrasound-guided percutaneous tenotomy of the long head of the biceps tendon: a non-reliable technique. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA. 2012;20(6):1027–30.
Aly AR, Rajasekaran S, Mohamed A, Beavis C, Obaid H. Feasibility of ultrasound-guided percutaneous tenotomy of the long head of the biceps tendon--A pilot cadaveric study. J Clin Ultrasound: JCU. 2015;43(6):361–6.
Sconfienza LM, Mauri G, Messina C, et al. Ultrasound-guided percutaneous tenotomy of biceps tendon: technical feasibility on cadavers. Ultrasound Med Biol. 2016;42(10):2513–7.
Smith J, Alfredson H, Masci L, Sellon JL, Woods CD. Sonographically guided plantaris tendon release: a cadaveric validation study. PM & R: The Journal of Injury, Function, and Rehabilitation. 2018.
Boettcher BJ, Hollman JH, Stuart MJ, Finnoff JT. Ultrasound-guided cutting wire release of the proximal adductor longus tendon: a feasibility study. Orthopaedic J Sports Med. 2019;7(8):2325967119866010.
Vohra PK, Japour CJ. Ultrasound-guided plantar fascia release technique: a retrospective study of 46 feet. J Am Podiatr Med Assoc. 2009;99(3):183–90.
Debrule MB. Ultrasound-guided weil percutaneous plantar fasciotomy. J Am Podiatr Med Assoc. 2010;100(2):146–8.
Hattori S, Alvarez CAD, Canton S, Hogan MV, Onishi K. Ultrasound-guided ankle lateral ligament stabilization. Curr Rev Musculoskel Med. 2019;12(4):497–508.
Seijas R, Rius M, Barastegui D, Ares O, Rivera E, Alvarez-Diaz P. Sonographic measurement of the patellar tendon should predict autograft Bone Patellar Tendon Bone (BPTB) size: comparison of anatomical and clinical findings. Journal of Investigative Surgery: The Official Journal of the Academy of Surgical Research. 2019:1–6.
Takeuchi S, Rothrauff B, Taguchi M, Fu F, Onishi K. Prediction of quadriceps tendon autograft diameter with preoperative ultrasonography for individualized anterior cruciate ligament reconstruction. Paper presented at: Orthopaedic Research Society2020; Phoenix, Arizona.
Takenaga T, Yoshida M, Albers M, et al. Preoperative sonographic measurement can accurately predict quadrupled hamstring tendon graft diameter for ACL reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA. 2019;27(3):797–804.
Rodriguez-Mendez LM, Martinez-Ruiz JJ, Perez-Manzo R, Corona-Hernandez JL, Alcala-Zermeno JL, Sanchez-Enriquez S. Preoperative ultrasonographic prediction of hamstring tendon diameter for anterior cruciate ligament repair. J Knee Surg. 2017;30(6):544–8.
Sumanont S, Mahaweerawat C, Boonrod A, Thammaroj P, Boonrod A. Preoperative ultrasound evaluation of the semitendinosus tendon for anterior cruciate ligament reconstruction. Orthopaedic J Sports Med. 2019;7(1):2325967118822318.
Gofeld M, Bristow SJ, Chiu S, Kliot M. Preoperative ultrasound-guided mapping of peripheral nerves. J Neurosurg. 2013;119(3):709–13.
Chavez J, Hattori S, Kato Y, Takazawa S, Yamada S, Ohuchi H. The use of ultrasonography during minimally invasive Achilles tendon repair to avoid sural nerve injury. J Med Ultrasonics (2001). 2019;46(4):513–4.
Ohuchi H, Ichikawa K, Shinga K, Hattori S, Yamada S, Takahashi K. Ultrasound-assisted endoscopic partial plantar fascia release. Arthroscopy Tech. 2013;2(3):e227–30.
Ohuchi H, Torres RJL, Shinga K, et al. Ultrasound-assisted posteromedial portal placement of the elbow joint to prevent ulnar nerve injury. Arthroscopy Tech. 2017;6(4):e1087–91.
Hanna AS, Ehlers ME, Lee KS. Preoperative ultrasound-guided wire localization of the lateral femoral cutaneous nerve. Operative Neurosurgery (Hagerstown, Md.). 2017;13(3):402–8.
Hwang J-J, Quistgaard J, Souquet J, Crum LA. Portable ultrasound device for battlefield trauma. Paper presented at: 1998 IEEE Ultrasonics Symposium. Proceedings (Cat. No. 98CH36102)1998.
Shorter M, Macias DJ. Portable handheld ultrasound in austere environments: use in the Haiti disaster. Prehospital Disaster Med. 2012;27(2):172–7.
Nolting L, Baker D, Hardy Z, Kushinka M, Brown HA. Solar-powered point-of-care sonography: our himalayan experience. Journal of Ultrasound in Medicine: Official Journal of the American Institute of Ultrasound in Medicine. 2019;38(9):2477–84.
Berko NS, Goldberg-Stein S, Thornhill BA, Koenigsberg M. Survey of current trends in postgraduate musculoskeletal ultrasound education in the United States. Skelet Radiol. 2016;45(4):475–82.
Wu WT, Chang KV, Han DS, Ozcakar L. Musculoskeletal ultrasound workshops in postgraduate physician training: a pre- and post-workshop survey of 156 participants. BMC Med Education. 2019;19(1):362.
Drolet P, Martineau A, Lacroix R, Roy JS. Reliability of ultrasound evaluation of the long head of the biceps tendon. J Rehabil Med. 2016;48(6):554–8.
Fowler JR, Hirsch D, Kruse K. The reliability of ultrasound measurements of the median nerve at the carpal tunnel inlet. J Hand Surg. 2015;40(10):1992–5.
Garcia-Santibanez R, Dietz AR, Bucelli RC, Zaidman CM. Nerve ultrasound reliability of upper limbs: Effects of examiner training. Muscle Nerve. 2018;57(2):189–92.
Ishida H, Suehiro T, Suzuki K, Watanabe S. Muscle thickness and echo intensity measurements of the rectus femoris muscle of healthy subjects: Intra and interrater reliability of transducer tilt during ultrasound. J Bodyw Mov Ther. 2018;22(3):657–60.
Tamborrini G, Marx C, Micheroli R. Inter-rater reliability in the classification of supraspinatus tendon tears using 3D ultrasound - a question of experience? J Ultrasonography. 2016;16(66):252–9.
Modica MJ, Kanal KM, Gunn ML. The obese emergency patient: imaging challenges and solutions. Radiographics: A Review Publication of the Radiological Society of North America, Inc. 2011;31(3):811–23.
Averkiou MA, Roundhill DN, Powers JE. A new imaging technique based on the nonlinear properties of tissues. Paper presented at. 1997 IEEE Ultrasonics Symposium Proceedings. An International Symposium (Cat. No.97CH36118); 5-8 Oct. 1997, 1997.
Ward B, Baker AC, Humphrey VF. Nonlinear propagation applied to the improvement of resolution in diagnostic medical ultrasound. J Acoustical Soc Am. 1997;101(1):143–54.
Meuwly JY, Thiran JP, Gudinchet F. Application of adaptive image processing technique to real-time spatial compound ultrasound imaging improves image quality. Investig Radiol. 2003;38(5):257–62.
Barr RG, Maldonado RL, Georgian-Smith D. Comparison of conventional, compounding, computer enhancement, and compounding with computer enhancement in ultrasound imaging of the breast. Ultrasound Quarterly. 2009;25(3):129–34.
McLaughlin GW. Practical aberration correction methods. Ultrasound. 2007;15(2):99–104.
Weng L, Tirumalai AP, Lowery CM, et al. US extended-field-of-view imaging technology. Radiology. 1997;203(3):877–80.
Lin EC, Middleton WD, Teefey SA. Extended field of view sonography in musculoskeletal imaging. J Ultrasound Med. 1999;18(2):147–52.
Lang RM, Addetia K, Narang A, Mor-Avi V. 3-dimensional echocardiography: latest developments and future directions. J Am Coll Cardiol Img. 2018;11(12):1854–78.
Merz E, Abramowicz JS. 3D/4D ultrasound in prenatal diagnosis: is it time for routine use? Clin Obstet Gynecol. 2012;55(1):336–51.
Fenster A, Blake C, Gyacskov I, Landry A, Spence JD. 3D ultrasound analysis of carotid plaque volume and surface morphology. Ultrasonics. 2006;44(Suppl 1):e153–7.
Rana M, Wakeling JM. In-vivo determination of 3D muscle architecture of human muscle using free hand ultrasound. J Biomech. 2011;44(11):2129–35.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Smith, J., Schroeder, A.N., Lloyd, A.R., Onishi, K. (2022). Evolution of Sports Ultrasound. In: El Miedany, Y. (eds) Musculoskeletal Ultrasound-Guided Regenerative Medicine. Springer, Cham. https://doi.org/10.1007/978-3-030-98256-0_21
Download citation
DOI: https://doi.org/10.1007/978-3-030-98256-0_21
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-98255-3
Online ISBN: 978-3-030-98256-0
eBook Packages: MedicineMedicine (R0)