
Abstract
The craniovertebral junction (CVJ) can be affected by different pathologies, which may cause bulbomedullary compression. In recent years, the endoscope and the endoscopic endonasal approaches (EEAs) to the midline skull base have been proposed as an alternative to the classical microsurgical transoral approach (TOA), which has long been considered the ‘gold standard’ for anterior decompression. The EEA has permitted to minimize some technical challenges and surgical complications related with the procedure.
We report our surgical experience with the EEA for treatment of different CVJ pathologies and we will critically highlight the indications, the feasibility, advantages and limitations of this approach. The surgical technique is described together with some “tips and tricks”, either referred to the intraoperative maneuvers and the post-operative management of the patients operated upon with such technique. Moreover, the posterior occipito-cervical fusion, which, in most cases, completes the procedure and is performed during the same operation, is briefly described.
We report the results of the EEA on a series of five endonasal endoscopic odontoidectomies have been performed in our Centers. The patients were affects by bulbo-medullary compression due to different pathologies (rheumatoid pannus, complex CCJ malformation, odontoid misalignment following a previous C2 fracture). All patients were operated with the same surgical technique (endoscopic endonasal odontoidectomy and posterior fusion during the same surgical setting) and in all patients the preoperative symptoms improved postoperatively.
Endoscopic endonasal approach has proved to be a valid alternative to the classical transoral route for performing the removal of the odontoid process of C2 in cases of extradural bulbo-medullary compression. It permits to overcome or, at least, minimize some perioperative complications of the TOA but requires a special knowledge of the regional anatomy and the surgical technique.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Endoscope
- Endonasal odontoidectomy
- Cranio-cervical junction
- Occipito-cervical fixation
- Cranial base
- Extradural bulbo-medullary compression
Introduction
Anterior approach to the cranio-vertebral junction (CVJ) and, particularly, to the odontoid process of the second cervical vertebra has classically been performed, in neurosurgical settings, via a transoral route. Such technique is still considered the gold standard treatment for odontoid process diseases.
However, the advent of endoscopy in neurosurgery and the development and the refinement of the endonasal approaches to the entire midline skull base [1,2,3,4,5], has meant that also this field, once dominated by microsurgery, has become territory of exploration for neurosurgeons who have dedicated clinical and scientific efforts is this direction. As a matter of facts, the endoscopic endonasal approach to the cranio-cervical junction, and to the odontoid process, is among the areas of most interest to which endoscopic technique is developed.
Indeed, several studies either anatomical and/or clinical have been reported showing the interest of approaching the CCJ through the nasal corridor [6, 7]. In fact, the availability of new technologies, such as endoscopes, high definition endoscopic cameras, navigation systems, ultrasound micro-Doppler, dedicated endonasal instruments and bipolar forceps have opened new horizons to manage pathologies involving this complex region using the natural nasal corridors; this way/approach has demonstrated a remarkable improvement of the quality of disease resection as well of the functional outcome with a lower morbidity.
The endonasal route provides a direct access to the surgical field, minimizing the mucosal and the neurovascular manipulation: it follows a natural path road that goes from the nostrils to the mucosa covering the rhynopharynx, the rhinopharyngeal muscles, the anterior arch of C1 and, finally the odontoid process. As a consequence, the surgical invasiveness, of the endoscopic endonasal approach is lower and does not require additional surgical maneuvers, such as (1) mouth retraction, (2) tongue compression or even splitting, (3) possible injury to the teeth, (4) injury to the uvula and/or the soft palate and velupendulum, (5) neurovascular manipulation through the oropharynx. Theoretically, such facts imply a lower rate of postoperative complications related to invasiveness with a lower rate of post-operative dysphagia and respiratory complications, which are due to the possibility that, with the endoscopic approach, extubation coincides with the end of the procedure. All this involves, consequently, a more rapid mobilization and a reduction of recovery times for natural feeding, which then is reflected, of course, on hospitalization time. Seen in this light, the endoscopic endonasal approach offers a viable alternative to the more established transoral approach, especially for the clear advantages that the endoscopic technique offers in cases where there is full indication to execute it. On the other hand, in case of dural opening, there will be an important risk of CSF leak and meningitis; as a consequence, the endonasal approach is associated with a difficulty of dural closure with the related higher risk of postoperative CSF leakage and meningitis. Given the intrinsic features of the endoscope, the endonasal route provides a wider, panoramic and multi-angled view of the region favoring also a closer-up of the relevant anatomical structures of the surgical field.
Anterior Versus Posterior Approach
The decision making between an anterior or a posterior approach depends on different particular aspects: (1) the direction of the compression and, (2) the surgeon’s confidence and experience with the approaches, and thus, the possibility to perform the reduction of the compression with anterior, posterior or a combined approach. In general, unreducible anterior subluxation associated with spinal cord compression requires anterior approach, whereas a reducible posterior compression a posterior surgical route. However, different complex diseases, acquired or congenital, can cause an alteration of atlanto-axial relationships and anterior cervico-medullary junction compression. In these cases, a fixation or a posterior stabilization could be not sufficient to resolve the ventral compression. As matter of facts, in these last years, the option of a combined, anterior and posterior, approach has become the best choice for many authors.
Transoral Approach and Transnasal Approach
Several surgical routes have been described for the cranio-vertebral junction (CVJ) region because of its complex anatomy and vital surrounding structures. During the last decades, the transoral approach with microscopic assistance has been proposed as the standard procedure to perform the anterior odontoidectomy, considering the etiology of the disease, the mechanism of compression and finally its reducibility [8,9,10,11]. The transoral approach has been considered the gold standard approach for the surgical treatment of pathologies at the anterior CVJ. Specifically, in the absence of spinal cord contusion or progressive myelopathy, the posterior decompression and fusion are sufficient alone to achieve an acceptable outcome. Odontoidectomy is necessary when there is a non reducible bony compression of spinal cord or soft tissue pannus, causing severe ventral compression and resulting in progressive myelopathy.
The risk of bacterial contamination, prolonged post operative intubation, nasogastric tube feeding, tongue swelling, and nasopharyngeal incompetence after transoral surgery have led authors to identify alternative routes to approach this region.
The anterior aspect of the cranio-cervical region can be exposed also via a transnasal despite the fact that some anatomical limits exist. In the transnasal route, the exposure of the C2 body below the odontoid process is limited by the posterior part of the hard palate; however, angled endoscopes, drills, and dedicated instruments provide access downwards to the lower edge of the C2 body [12,13,14,15]. On the other hand, the transoral approach is limited by the degree of mouth opening, the size of the patient’s tongue, and the position of the uvula and the soft palate. The inferior limit of the access, usually the C3 vertebra, is determined by the degree of mouth opening, the size of the patient’s oral cavity and the prominence of the incisors. However, also for the transoral approach, the use of angled endoscopes and instruments, directs the approach superiorly increasing the rostral access above the anterior arch of the atlas to the lower clivus and C2 [16, 17]. One of the main anatomical landmarks to consider, especially in transoral route, is the course of vertebral artery (VA). The VA, after ascending through the transverse foramen of the axis and atlas, approximately 15 mm from the midline, courses medially along the upper surface of the posterior arch of the atlas to reach its dural entrance. It is mandatory to preserve the segment of the vertebral artery ascending between the C1 and C2 transverse processes.
Once the anterior arch of C1 is exposed, its drilling is necessary to expose the odontoid process of C2. Another difference between transoral and transnasal approach is the visualization of the ligamentous complex. For instance, the apical ligament, is easily visualized directly straight ahead of the endoscope in the transnasal route but is seen later, after removal of the odontoid, in the transoral approach. The main step of the anterior odontoidectomy is represented by the drilling of the dens. In the transnasal approach, the dens is seen directly ahead. The anterior cortical surface and core of the dens is drilled, whereas the cortical shell is removed. On the other hand, the base of the dens is more easily accessed for drilling by the transoral route. In addition, a different view is offered by these two approach regarding as the exposure of the upper, middle or lower clivus. The standard endoscopic transnasal transsphenoidal approach allows to reach the upper clivus, which corresponds to the posterior wall of the sphenoid sinus. Thus the middle and lower clivus are viewed directly straight ahead in the transnasal approach. The access to the middle and lower clivus generally does not require opening the sphenoid sinus. On the other hand, in the transoral approach the middle and the upper clivus are not usually accessible because of it would be necessary the soft and hard palates opening, the splitting of the tongue or mandible to gain an upward angulation. However, such maneuvers as using an angled endoscope, retracting sufficientlythe uvula, and widely opening the mouth provide a safe access to the lower clivus.
Indications
Odontoidectomy is a procedure that is necessary in all cases in which there is an impairment of the nervous structures of the cranio-cervical junction due to an irreducible alteration of the relations that the odontoid process contracts with neighboring neurovascular structures.
Various pathologies may cause atlanto-axial misalignment and bulbo-medullary junction compression, among them, congenital malformation—such as Arnold Chiari type II—, genetic degenerative transformation—such as in Down’s syndrome—, chronic inflammation related to rheumatoid arthritis and/or metabolic disorders and, finally, post-traumatic alterations (Fig. 18.1).

Preoperative neuroimaging studies. T2-weighted sagittal (a) and axial (b) MRI of the CVJ showing a bulbo-medullary compression by an extradural mass lesion of the odontoid process (rheumatoid pannus). (c, d) 3D reconstruction of an angio-CT of the same patient
The irreducibility is a crucial concept in the path that leads to the indication for surgery. In fact, several studies confirmed that, when feasible, the reduction of the compression by putting in traction the cranio-cervical junction and the subsequent fixation, as well as, in cases of compression due to the rheumatoid pannus, posterior stabilization of the cranio-cervical junction leads, in some cases, the improvement or even the resolution of the ventral compression.
Therefore, the indications for the odontoidectomy arise in all those cases in which there is irreducible atlanto-axial subluxation, associated with severe brainstem and/or spinal cord compression causing progressive neurological dysfunction. In most cases, the pathological process can be due to: (1) irreducible basilar impression [18,19,20,21,22,23]; (2) ventral compression, as in the cases of rheumatoid pannus, not resolved after posterior stabilization [24,25,26]; (3) significant retroflexion of the odontoid process or basilar invagination associated with Chiari disease; [27] (4) presence of os odontoideum [28,29,30]; (5) post-traumatic pseudoartrosis or misalignment; (6) several recent experiences have enlarged the indications of endoscopic endonasal odontoidectomy for the treatment of intradural lesions [3, 5, 31,32,33].
Feasibility of the Endoscopic Endonasal Odontoidectomy
The goal of the surgical operation is to completely remove the odontoid process of C2 and obtain a sufficient decompression of the ventral brainstem and CVJ. In the debate between microsurgery and endoscopic technique, a remark is done to the eventuality, in the endonasal approach, to have difficulty in reaching the lower portion of the cranio-cervical junction and, namely, the base of the dens. To understanding this aspect, numerous studies on cadavers and on radiological images were performed, with the purpose of delimiting the limits and then the indications to endoscopic approach to the odontoid process pathology. However, leading authors widely reported the feasibility of the endoscopic endonasal approach (EEA) to the CVJ [3, 6].
In cases low junction, located far below the level of the hard palate, it could be quite difficult if not impossible to reach anterior arch of C1 and the base of the odontoid process. Such cases can represent still an indication for the transoral approach. On the other hand, in a higher junction, the dens is more easily reachable and removable by the nasal route.
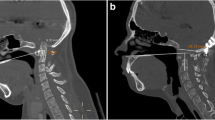
In order to preoperatively assess the feasibility of the odontoidectomy via an endoscopic endonasal route, in a midline sagittal CT slice with bone window, it’s possible to draw four lines representing possible paths, to depart from piriform aperture of the nasal bones, which target the odontoid process and lead to assess the inferior limit for surgical exposure. Predicting the inferior limit of the CVJ is crucial to choose the appropriate approach in an aerea which is considered a transitional area between endonasal and transoral route.
Nasopalatine Line
One of the criticisms of the EEA to the upper cervical spine is the limited exposure inferiorly. Endonasal dissection of the upper cervical spine is limited superiorly by the nasal bones and soft tissues of the nose, and inferiorly by the hard palate and soft palate [34, 35]. The line created by connecting the most inferior point of the nasal bone to the posterior edge of the hard palate in the midsagittal plane is defined the naso-palatine line (NPL), and considered a limitation of caudal dissection with straight endoscopic instruments. The angle created by this line and the plane of the hard palate, the nasopalatine angle (NPA) provides the window of exposure to the skull base and upper cervical spine. The mean nasopalatine angle is 27.1° ± 0.7° . The mean point of intersection between the nasopalatine line and the vertebral column is reported to be 8.9 ± 1.8 mm above the base of the C2 vertebral body. The NPL is considered by several authors, a controversial predictor of the maximal extent of inferior dissection in endoscopic endonasal resection of odontoid process [34], considering that the inferior limit predicted by the NPL was found by a mean value of 12.7 mm, below the real inferior extent of surgical dissection. Various pathologic (basilar invagination) and physiologic factors (head positioning) affect the point of intersection of the NPL with the cervical spine. In order to improve caudal exposure, the use of angled instruments or drills may be of value. Additionally, the retraction of the soft palate and drilling the posterior edge of the hard palate may improve the exposure but may increase the risks of palatal dehiscence and velopharyngeal insufficiency.
Naso-Axial Line
The naso-axial line (NAxL) is defined as the line constructed in the midsagittal plane using a starting point that corresponds to the midpoint of the distance from the rhinion to the anterior nasal spine of the maxillary bone and a second point at the tip of the posterior nasal spine of the palatine bone. It is extended posteriorly and inferiorly to the cervical spine. Some authors, in order to predict more accurately, than using NPL,the lower limit of the EEA to reach the CVJ through the correspondence between CT measurements and the real surgical limit, performed a cadaveric study evaluating the predictive value of NAxL. Their findings supported the close correspondence between the NAxL, drawn in preoperative CT images, and the anatomic surgical extent [36].
Hard-Palate Line
The hard-palate line (HPL) is defined as the line that passes through the anterior and posterior edges of the hard palate (anterior nasal spine of the maxillary bone and posterior nasal spine of the palatine bone, respectively) and intersects the cranio-vertebral junction posteriorly. This line represents the long axis of the hard palate [37]. It is considered a realible marker of the inferior extension of CVJ especially in congenital abnormalities, such as platybasia with associated basilar invagination, where the tip of odontoid is often above the plane of the hard palate [38].
Rhinopalatine Line
The rhinopalatine line is defined as the line constructed in the midsagittal plane using a starting point that corresponds to the two-thirds point of the distance from the rhinion to the anterior nasal spine of the maxillary bone and a second point at the posterior nasal spine of palatine bone. The line is extended posteriorly and inferiorly, ending to the cervical spine. There have been great efforts from different groups to study the inferior limit of the endoscopic endonasal approach (EEA) . De Almeida et al. [34] described the nasopalatine (NPL) as a good and accurate predictor of the inferior limit of the EEA, but in their study, the NPL resulted always below the inferior extent of surgical dissection with a mean value of 12.7 mm. Consequently, the naso-axial line was reported to predict more accurately and reliably the inferior caudal exposure of the EEA to the CVJ. Similarly, it was been found that the NAxL also overpredicted the lower limits of the approach [37]. The rhino-palatine line (RPL) seemed to be a most accurate predictor in several studies.
This predictor accounts also for patient anatomical variability, such as the presence of nasal and palatal osseous and soft structures, together with the hard palate’s direction and length, which represent the most significant factors that limit the inferior extension of the EEA. The RPL cannot be used to predict the lateral limits of the EEA to the CVJ.
Operative Tecnique
According to different pathologies we perform an endoscopic endonasal odontoidectomy followed by posterior decompression and fusion in a single stage surgery.
In order to accurately choose the correct approach, we consider on sagittal CT scan the relationship between naso- and rhino-palatine line and the upper cervical spine.
We routinely use the neuronavigation system (StealthStation S7, Medtronic, Minneapolis [MN], USA), based on contrast enhanced MR with angiographic TOF sequences merged with a 1 mm layer CT of the brain and cervical spine in unique volume. Generally, we use the optical tracking of the StealthStation S7® in order merged with the angiographic TOF sequencesin order to provide feasible pre-operative images regarding the relationship between bone CVJ bone and vascular structures such as vertebral and carotid arteries. Somatosensory evoked potential neuromonitoring is routinely used.
Patient Positioning and Preparation
Following general anesthesia and oro-tracheal intubation, the patient is placed in supine position with the trunk elevated of about 20°. The head is slightly turned on the right of, maximum 10°, not flexed, and fixed in a radiolucent Mayfield-Kees three-pin head-clamp. The head is kept parallel to the floor and maintained without flexion or extension during the posterior fusion when the patient is turned by supine to prone position. In all cases we used the O-arm® system (Medtronic, Minneapolis [MN], USA) in the phase of posterior fusion. On this, the optical reference of the neuronavigator is mounted, should the optical system be used. On the contrary, the magnetic reference is positioned on the patient’s head, in case the electromagnetic system is employed. We use antibiotic prophylaxis with Cefazolin 2 g 1 h before the procedure.
Nasal Phase
The nose is prepped with cottonoids soaked with diluted iodopovidone 5% solution inside the two nostrils. A 0° angled lens and 18 cm endoscope associated with an HD camera (Karl Storz, Tuttlingen, Germany) is introduced inside the right nostril. The identification of usual anatomical nasal landmarks is performed (inferior turbinate laterally and nasal septum medially). As a standard endoscopic endonasal procedure, above the inferior turbinate, the middle turbinate is identified and luxated laterally putting cottonoids soaked with diluted adrenaline between middle turbinate and nasal septum, to prevent bleeding of the nasal mucosa. The same maneuvers are carried out in the left nostril. The endoscope advances parallel to the floor of the nasal cavity until the choana is reached. With the aid of the neuronavigation system, the anatomical landmarks are verified. The mucosa over the posterior and inferior aspect of the nasal septum is cauterized with monopolar coagulation or, better, with bipolar forceps. We do not routinely perform the removal of the anterior wall of the sphenoid sinus since a transsphenoidal corridor is rarely needed, unless an higher exposure should be required in case of the tip of the dens goes quite high or when more space is required for the surgical maneuvers, due to patient’s individual anatomy. Afterwards, an inferior septectomy is performed, removing sufficiently the vomer bone and extending inferiorly, down to the hard palate. The most superior limit reached is the clivus-nasal septum junction. At this stage few important anatomical landmark should be identified, which guide the surgeons to stay oriented: (1) the clivus-septum junction superiorly, (2) the Eustachian tubes laterally, (3) the nasal floor/soft palate inferiorly as marked by the hard and soft palate. The neuronavigation will confirm the position of such surgical landmarks and give the correct direction for the subsequent surgical steps.
Nasopharynx Phase
The key points of the nasal phase allow the widest exposure of the rhinopharynx and to avoid any conflict among the instruments during the next surgical steps. The nasopharynx muchosa is incised on the midline (Fig. 18.2a) and the muscles are dissected bilaterally in order to expose the anterior arch of C1 (Fig. 18.2b). Several authors reported a reverse “U”-shaped flap of nasopharyngeal prepared with monopolar electrocautery, elevated and reflected caudally to the level of the soft palate in order to improve the surgical field.The cranio-caudal extension of the flap involves the inferior third of the clivus superiorly, the C2 vertebral body inferiorly, and the lateral margin of the operative exposure included the lateral masses of the C1 vertebra. The U-shaped nasopharynx flap extends the surgical corridor laterally, but on the other hand increases the risk of injuries to parapharyngeal carotids which are located laterally to the superior pharyngeal constrictor muscle. We prefer doing a straight midline opening of the nasopharynx because of guarantees a sufficient exposure and a lower risk of vascular damage. Then, we proceed with skeletonizing of the anterior arch of C1 and of the odontoid process in a subperiosteal fashion.

Intraoperative pictures of the endoscopic endonasal approach. (a) Incision into the rhinopharynx; (b) drilling of the anterior arch of C1; (c) drilling of the odontoid process of C2; (d) freeing of the remaining part of the dens from the ligaments. rPh rhinopharynx, ET Eustachian tubes, C1 tub anterior tubercle of C1, OP odontoid process, lig ligaments
C1 Anterior Arch Preservation in Selected Cases
Recently, several authors reported their experience in matter of endoscopic endonasal odontoidectomy, focusing on the preservation of C1 anterior arch during the craniovertebral junction phase, avoiding the posterior fixation [32, 39]. Particularly, in case of rheumatoid arthritis or other inflammatory diseases, the anterior arch of the atlas is preserved by drilling the odontoid base, weakening its apical, and leading to the pulling downward of the dens in the working area. The following removal of the axis with other remaining compressive inflammatory lesions is performed using a combination of high-speed drill, ultrasonic bone curette and standard Kerrison’s rongeurs [32, 39]. According to such authors, working above and below the C1 anterior arch and its preservation represent not only an element of stability, but also give an important opportunity for reconstruction and to reinforce the closure. Additionally, the same groups, in case of inveterate D’Alonzo II fractures or in the combination of odontoid fracture associated with fracture of anterior arch of C1, proposed their tecnique of anterior fixation and anterior C1 arch reconstruction [40].
Craniovertebral Junction Phase and Closure
In our tecnique, the anterior arch of the atlas is exposed and removed through the high speed drill with diamond burrs and Kerrison’s rongeurs (Fig. 18.2c). Posteriorly, the odontoid process of C2, is exposed, separated from the alar and apical ligaments, dissected from the transverse ligament, thinned using the microdrill and finally removed (Fig. 18.2d). At this point, a wide surgical corridor is created. The odontoidectomy is performed carefully by using high speed drill, Kerrison’s, and in case of lesions with soft consistency, curettes and pounches or ultrasound aspiration. When the removal is complete the dural plane appears pulsating and indicates an optimal decompression of the brainstem (Fig. 18.3a, b).

Intraoperative pictures of the endoscopic endonasal approach. (a) removal of the pannus causing the compression; (b) dura mater of the CVJ; (c) closure of the muscle and mucosal incision with the aid of the fibrin glue; (d) endoscopic control of the surgical field 3 days later showing the optimal closure of the incision. p pannus, C2 base of the dens (body of C2), DM dura mater of the CVJ, ET Eustachian tube, rPh rhinopharynx, fg fibrin glue, SP soft palate; asterisk: nasogastric tube
After having obtained a satisfying hemostasis, the closure is guaranteed with a layer of fibrin glue only in the absence of a possible dural tearing (Fig. 18.3c). In case of CSF leak, a packing with Gelfoam/Surgicel and fibrin glue is realized to reinforce the closure. In these cases we consider the possibility to position and extended lumbar drain (ELD) at the end of the operation. We close the nasopharynx muchosa by a single stich because of the median opening allows a faster closure of the muscles at the end of endoscopic time. Generally, we position a nasogastric tube under endoscopic control.
Posterior Fusion
The second step of the operation is characterized by the posterior occipito-cervical fusion. The patient, already fixed to the Mayfield-Kees three-pin carbon fibers radiolucent head-holder, is turned by supine to prone position with the head parallel to the floor and with a slight degree of extension. This position considers the C0–C2 angle which is formed by the posterior extension of the hard palate and the vertical line passing through the dens and avoids the breath impairment related to the flexion. A midline incision is performed starting from the inion to the spinous process of C6. The fascia is exposed and incised on the midline with monopolar cautery. The muscle dissection is performed along the raphe in a subperiosteal fashion from the basiocciput to the posterior complex of C5. The bone landmarks are clearly visible: (1) the occipital bone; (2) posterior arch and lateral masses of C1; (3) posterior complex from C1 to C5.
Generally, we remove the posterior arch of C1, because of, in most of our cases, it contributed to the bulbo-pontine compression. The lateral masses of C3 and C4 are identified and verified through the O-arm® system. The fixation system we used in all cases was the Vertex titanium system (Medtronic, Minneapolis [MN], USA). The high speed drill is used to prepare the position of the screws within the lateral masses of C3 and C4. The polyaxial screws are inserted according to Magerl technique [41] in order to avoid vascular injuries. Differently, in the basiocciput the monoaxial screws are positioned 2 cm from the inion on both sides and 1 cm above the sinuses. The length of the screws we use is 8 mm. After screws are positioned, the two rods are pulled to obtain the correct alignment of the cervical spine, and finally fixed through the wrench of wing nuts. The bone fusion is improved with the addition of bone substitutes. The last verification with the O-arm® system is done at the end of the procedure. At the discharge we recommend the use of cervical collar for 2 months (Fig. 18.4).

Postoperative neuroimaging studies of the same patient of Fig. 18.1. The T2-weighted sagittal (a) MRI of the CVJ shows an optimal decompression of the bulbo-medullary junction. (b, c) intraoperative O-arm® images showing the removal of the odontoid process. (d–f) 3D reconstruction of the post-operative CT scan of the CVJ
Series Presentation
A series of five endonasal endoscopic odontoidectomies have been performed in our centers. Demographic, clinical, and management details are summarized in Tables 18.1 and 18.2.
All patients were female, ranging between 62 and 82 years (mean age 68.8 years). Four patients were admitted with a neurological onset characterized by tetraparesis; in one patient, motor deficits were prevalent on the right arm. Urinary incontinence was present in two patients. Was present in two patients. One patient presented severe dysphagia for either solids or liquids. In three patients, symptoms were related to the presence of a rheumatoid synovial pannus, while the other two cases showed signs and symptoms due to a complex malformation of the craniocervical junction and to a misalignment of the odontoid process following a previous non-fused Anderson-D’Alonzo type II frac- ture, respectively. Interestingly, the patient affected by the complex CVJ malforma- tion underwent previously to aoccipital-cervical stabilization to another institution. Subsequently, she underwent an attempt of transoral odontoidectomy, which failed due to the higher position of the dens. She was referred in our clinic for an anterior decompression performed through an endoscopic endonasal odontoidectomy. In the remaining three patients, in the same single-stage surgery, anterior decompression and posterior stabilization were performed during the same operation.
The length of stay ranges from 9 to 19 days (including the first period of rehabili- tation). In all patients, there was an improvement of the neurological conditions, compared to the preoperative one. In one patient the swallowing dysfunction resolved, allowing an early oral feeding. In two cases an implementation with par- enteral nutrition was necessary for a few days.
Postoperative Management
In our practice, according to the general clinical condition of patient and the lenght of sedation, we preferred leaving the patient in our intensive care unit for 24 h. This occurred in two of the four cases treated. In our department, the primary aim is the early mobilization of the patient, to lower the risks of an extended bed rest. In addition, the use of the nasogastric tube guaranteed a sufficient patient’s caloric intake, with the addition of parenteral nutrition, when required. We performed at least two endoscopic postoperative controls: one in the first 24 h and one before the discharge (Fig. 18.3d). During such checks we verified the proper closure of the surgical wound and the possible presence of CSF leak, and thus we removed the nasogastric tube under endoscopic control. This maneuver can be performed only after testing the function of lower cranial nerves by and otolaryngologist. In our series, the removal of nasogastric tube occurred in three patients, in the eighth postoperative day, in two patients, and in the seventh postoperative day, in the other one. In our series patients performed before discharge, a CT scan of the head and cervical spine in order to assess the degree of the odontoidectomy and the correct position of screws and rods of the posterior fusion, and an MRI to evaluate the decompression of neurovascular structures. A further control was performed after 3 months. All patients started a physical rehabilitation program, which also continued after discharge.
References
Cappabianca P, Cavallo LM, Esposito F, de Divitiis O, Messina A, de Divitiis E. Extended endoscopic endonasal approach to the midline skull base: the evolving role of transsphenoidal surgery. In: Pickard JD, Akalan N, Di Rocco C, Dolenc VV, Lobo Antunes J, Mooij JJA, Schramm J, Sindou M, editors. Advances and technical standards in neurosurgery. Wien: Springer; 2008. p. 152–99.
Cavallo LM, De Divitiis O, Aydin S, Messina A, Esposito F, Iaconetta G, Talat K, Cappabianca P, Tschabitscher M. Extended endoscopic endonasal transsphenoidal approach to the suprasellar area: anatomic considerations—part 1. Neurosurgery. 2008;62:1202–12.
Cavallo LM, Messina A, Cappabianca P, Esposito F, de Divitiis E, Gardner P, Tschabitscher M. Endoscopic endonasal surgery of the midline skull base: anatomical study and clinical considerations. Neurosurg Focus. 2005;19(1):E2.
Esposito F, Becker DP, Villablanca JP, Kelly DF. Endonasal transsphenoidal transclival removal of prepontine epidermoid tumors: technical note. Neurosurgery. 2005;56(2 Suppl):E443.
Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL. Expanded endonasal approach: the rostrocaudal axis. Part II. Posterior clinoids to the foramen magnum. Neurosurg Focus. 2005;19(1):E4.
Cavallo LM, Cappabianca P, Messina A, Esposito F, Stella L, de Divitiis E, Tschabitscher M. The extended endoscopic endonasal approach to the clivus and cranio-vertebral junction: anatomical study. Childs Nerv Syst. 2007;23(6):665–71.
Messina A, Bruno MC, Decq P, Coste A, Cavallo LM, de Divittis E, Cappabianca P, Tschabitscher M. Pure endoscopic endonasal odontoidectomy: anatomical study. Neurosurg Rev. 2007;30(3):189–94. discussion 194
Crockard HA. The transoral approach to the base of the brain and upper cervical cord. Ann R Coll Surg Engl. 1985;67(5):321–5.
Crockard HA, Pozo JL, Ransford AO, Stevens JM, Kendall BE, Essigman WK. Transoral decompression and posterior fusion for rheumatoid atlanto-axial subluxation. J Bone Joint Surg Br. 1986;68(3):350–6.
Perrini P, Benedetto N, Guidi E, Di Lorenzo N. Transoral approach and its superior extensions to the craniovertebral junction malformations: surgical strategies and results. Neurosurgery. 2009;64(5 Suppl 2):331–42. https://doi.org/10.1227/01.NEU.0000334430.25626.DC.
Perrini P, Benedetto N, Di Lorenzo N. Transoral approach to extradural non-neoplastic lesions of the craniovertebral junction. Acta Neurochir. 2014;156(6):1231–6.
Cappabianca P, Cavallo LM, Esposito F, de Divitiis E. Endoscopic endonasal transsphenoidal surgery: procedure, endoscopic equipment and instrumentation. Childs Nerv Syst. 2004;20(11–12):796–801.
Cappabianca P, de Divitiis O, Esposito F, Cavallo LM, de Divitiis E. Endoscopic skull base instrumentation. In: Anand VK, Schwartz TH, editors. Practical endoscopic skull base surgery. San Diego: Plural Publishing; 2007. p. 45–56.
Cappabianca P, Esposito F, Cavallo LM, Corriero OV. Instruments. In: Cranial, craniofacial and skull base surgery. Wien: Springer; 2010. p. 7–15.
Esposito F, Di Rocco F, Zada G, Cinalli G, Schroeder HWS, Mallucci C, Cavallo LM, Decq P, Chiaramonte C, Cappabianca P. Intraventricular and skull base neuroendoscopy in 2012: a global survey of usage patterns and the role of intraoperative neuronavigation. World Neurosurg. 2013;80(6):709–16.
de Divitiis O, Conti A, Angileri FF, Cardali S, La Torre D, Tschabitscher M. Endoscopic transoral-transclival approach to the brainstem and surrounding cisternal space: anatomic study. Neurosurgery. 2004;54(1):125–30. discussion 130
Visocchi M, Doglietto F, Della Pepa GM, Esposito G, La Rocca G, Di Rocco C, Maira G, Fernandez E. Endoscope-assisted microsurgical transoral approach to the anterior craniovertebral junction compressive pathologies. Eur Spine J. 2011;20(9):1518–25.
Goel A, Bhatjiwale M, Desai K. Basilar invagination: a study based on 190 surgically treated patients. J Neurosurg. 1998;88(6):962–8.
Karam YR, Menezes AH, Traynelis VC. Posterolateral approaches to the craniovertebral junction. Neurosurgery. 2010;66(3 Suppl):135–40. https://doi.org/10.1227/01.NEU.0000365828.03949.D0.
Menezes AH. Craniocervical developmental anatomy and its implications. Childs Nerv Syst. 2008;24(10):1109–22.
Menezes AH, VanGilder JC. Transoral-transpharyngeal approach to the anterior craniocervical junction. Ten-year experience with 72 patients. J Neurosurg. 1988;69(6):895–903.
Smoker WR. Craniovertebral junction: normal anatomy, craniometry, and congenital anomalies. Radiographics. 1994;14(2):255–77.
Smoker WRK, Khanna G. Imaging the craniocervical junction. Childs Nerv Syst. 2008;24(10):1123–45.
Joaquim AF, Appenzeller S. Cervical spine involvement in rheumatoid arthritis—a systematic review. Autoimmun Rev. 2014;13(12):1195–202.
Pare MC, Currier BL, Ebersold MJ. Resolution of traumatic hypertrophic periodontoid cicatrix after posterior cervical fusion: case report. Neurosurgery. 1995;37(3):531–3.
Sandhu FA, Pait TG, Benzel E, Henderson FC. Occipitocervical fusion for rheumatoid arthritis using the inside-outside stabilization technique. Spine (Phila Pa 1976). 2003;28(4):414–9.
Klekamp J. Chiari I malformation with and without basilar invagination: a comparative study. Neurosurg Focus. 2015;38(4):E12.
Arvin B, Fournier-Gosselin MP, Fehlings MG. Os Odontoideum: etiology and surgical management. Neurosurgery. 2010;66(3 Suppl):22–31. https://doi.org/10.1227/01.NEU.0000366113.15248.07.
Matsui H, Imada K, Tsuji H. Radiographic classification of Os odontoideum and its clinical significance. Spine (Phila Pa 1976). 1997;22(15):1706–9.
Vargas TM, Rybicki FJ, Ledbetter SM, MacKenzie JD. Atlantoaxial instability associated with an orthotopic os odontoideum: a multimodality imaging assessment. Emerg Radiol. 2005;11(4):223–5.
Cappabianca P, Cavallo LM, Esposito F, de Divitiis O, Messina A, de Divitiis E. Extended endoscopic endonasal approach to the midline skull base: the evolving role of transsphenoidal surgery. In: Pickard JD, editor. Advances and technical standards in neurosurgery. Wien: Springer; 2007. p. 1–48.
Iacoangeli M, Gladi M, Alvaro L, Di Rienzo A, Specchia N, Scerrati M. Endoscopic endonasal odontoidectomy with anterior C1 arch preservation in elderly patients affected by rheumatoid arthritis. Spine J. 2013;13(5):542–8.
Kassam AB, Gardner PA, Snyderman CH, Carrau RL, Mintz AH, Prevedello DM. Expanded endonasal approach, a fully endoscopic transnasal approach for the resection of midline suprasellar craniopharyngiomas: a new classification based on the infundibulum. J Neurosurg. 2008;108(4):715–28.
De Almeida JR, Zanation AM, Snyderman CH, Carrau RL, Prevedello DM, Gardner PA, Kassam AB. Defining the nasopalatine line: the limit for endonasal surgery of the spine. Laryngoscope. 2009;119(2):239–44.
Kassam AB, Snyderman C, Gardner P, Carrau R, Spiro R. The expanded endonasal approach: a fully endoscopic transnasal approach and resection of the odontoid process: technical case report. Neurosurgery. 2005;57(1 Suppl):E213.
Aldana PR, Naseri I, La Corte E. The naso-axial line: a new method of accurately predicting the inferior limit of the endoscopic endonasal approach to the craniovertebral junction. Neurosurgery. 2012;71:ons308-14. https://doi.org/10.1227/NEU.0b013e318266e488.
La Corte E, Aldana PR, Ferroli P, Greenfield JP, Hartl R, Anand VK, Schwartz TH. The rhinopalatine line as a reliable predictor of the inferior extent of endonasal odontoidectomies. Neurosurg Focus. 2015;38(4):E16.
El-Sayed IH, Wu J-C, Ames CP, Balamurali G, Mummaneni PV. Combined transnasal and transoral endoscopic approaches to the craniovertebral junction. J Craniovertebr Junction Spine. 2010;1(1):44–8.
Gladi M, Iacoangeli M, Specchia N, Re M, Dobran M, Alvaro L, Moriconi E, Scerrati M. Endoscopic transnasal odontoid resection to decompress the bulbo-medullary junction: a reliable anterior minimally invasive technique without posterior fusion. Eur Spine J. 2012;21(Suppl 1):S55–60. https://doi.org/10.1007/s00586-012-2220-4.
Re M, Iacoangeli M, Di Somma L, Alvaro L, Nasi D, Magliulo G, Gioacchini FM, Fradeani D, Scerrati M. Endoscopic endonasal approach to the craniocervical junction: the importance of anterior C1 arch preservation or its reconstruction. Acta Otorhinolaryngol Ital. 2016;36(2):107–18.
Suchomel P, Stulik J, Klezl Z, Chrobok J, Lukas R, Krbec M, Magerl F. [Transarticular fixation of C1-C2: a multicenter retrospective study]. Acta Chir Orthop Traumatol Cechoslov. 2004;71(1):6–12.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Esposito, F., Angileri, F.F., Cavallo, L.M., Cacciola, F., Germanò, A., Cappabianca, P. (2022). Endoscopic Endonasal Odontoidectomy. In: Menchetti, P.P.M. (eds) Cervical Spine. Springer, Cham. https://doi.org/10.1007/978-3-030-94829-0_18
Download citation
DOI: https://doi.org/10.1007/978-3-030-94829-0_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-94828-3
Online ISBN: 978-3-030-94829-0
eBook Packages: MedicineMedicine (R0)