
Abstract
In the endovascular era, as newer and improved devices to treat intracranial aneurysms (IAs) continue to winnow the number of aneurysms treated by microsurgery, a substantial number of aneurysms will remain best treated by microsurgery. Currently, IAs most appropriate for microsurgical treatment include the following: multiple IAs most parsimoniously addressed by surgery, aneurysms in young patients, very small aneurysms, endovascular treatment failures, patients intolerant to or noncompliant with required antiplatelet agents for endovascular treatment, large and giant aneurysms with symptomatic mass effect, wide-necked aneurysms, fusiform aneurysms, aneurysms with complex anatomy, thrombotic aneurysms, infectious aneurysms that have failed antimicrobial treatment, and pseudoaneurysms among others. In this chapter, discussion of microsurgical considerations for each subtype is addressed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Intracranial aneurysm
- Microsurgery
- Indications
- Large
- Giant
- Very small
- Wide-necked
- Complex
- Thrombotic
- Fusiform
- Infectious
Introduction
The basic tenets for treatment of intracranial aneurysms (IAs) are to eliminate the aneurysm from the circulation completely, to preserve the patency of the parent vessels and associated branches, and to maintain or improve the patient’s neurologic function. Because of the complexity of aneurysm treatment, better outcomes are achieved in large volume centers where neurosurgical, endovascular, neurointensive care, and neuroanesthesia teams work together to care for these patients [1, 2]. The decision to treat and by which modality depends on factors of the patient (i.e., age, clinical status, and risk factors for hemorrhage) and the aneurysm (i.e., size, shape, configuration, multiplicity, and presence of thrombus). This chapter will focus on indications for surgical treatment of IAs in this era of rapid endovascular advancements.
History of Surgical Management of Aneurysms
As early as the 1800s, IAs were surgically treated by Hunterian ligation – or gradual occlusion of the carotid artery – to promote aneurysm thrombosis. Direct exposure of a ruptured IA and muscle wrapping was performed by Sir Norman Dott in 1931. The first aneurysm clip, a Cushing-McKenzie silver clip, was placed on the neck of a saccular IA in 1937 by Walter Dandy, while modern, spring-loaded aneurysm clips were first introduced in 1950 by Frank Mayfield and George Kees. Further design refinements were made by Charles Drake with the fenestrated clip, Thoralf Sundt Jr with the encircling clip, Gazi Yasargil, and Kenichiro Sugita. The pterional craniotomy was refined in the 1960s. In 1969, Yasargil described the superficial temporal artery to middle cerebral artery (STA-MCA) bypass as an adjunct in the treatment of complex IAs [3]. With the introduction of the operating microscope, refinements in microsurgical techniques, improved anesthetic and intensive care management, and development of diagnostic imaging, the risk of surgery for IAs decreased over time. Prior to 1991, when Guglielmi introduced detachable platinum coils, microsurgical clip ligation remained the primary treatment for IAs [1, 4].
Neuro-Imaging Evaluation
Imaging of IAs has improved tremendously over time. While axial angiography using computed tomography (CT) or magnetic resonance imaging (MRI) modalities is frequently used for screening and follow-up of both treated and observed aneurysms, noninvasive imaging is most sensitive for aneurysms >3 mm in size [2, 5]. Axial imaging may also provide complimentary and clinically important information regarding the presence of intraluminal thrombus and calcification of aneurysms [5]. Digital subtraction angiography (DSA) is the “gold standard” to evaluate IAs. Two- and three-dimensional DSAs are critical to evaluate the following features of the aneurysm and the surrounding vasculature: (1) parent vessel, (2) size, shape, and relationship to parent and adjacent arteries, (3) presence and location of vasospasm, (4) displacement of adjacent vessels, and (5) the presence of additional aneurysms or vascular malformations [5, 6].
Indications for Aneurysm Surgery in the Endovascular Era
Pediatric Patients
Considering the life expectancy of young adult and pediatric patients, optimal treatment for cerebral aneurysms remains unclear. Endovascular therapies confer reduced durability with recurrence reported to be as high at 20–40% [7,8,9]. Furthermore, the long-term outcomes of endovascular devices such as flow diverters are unknown due to lack of sufficient follow-up in the growing child or adolescent. Due to the rarity of pediatric aneurysms, only small clinical series have been published, which makes it difficult to make treatment recommendations.
Aneurysms in pediatric patients are more frequently large or giant or fusiform in morphology than adult aneurysms [7,8,9]. Complete occlusion of the aneurysm is achieved only for 80–82% after endovascular therapies [7,8,9]. Sanai et al. demonstrated a 14% recurrence after endovascular treatment (EVT) over a mean follow-up period of just 5.7 years [8]. Recurrence after surgery is documented to be around 2.5% or less [8, 9]. The clinical outcomes did not differ significantly between endovascular and microsurgical treatments with overall 7–14% long-term morbidity and low morality in this pediatric population [7,8,9].
Multiple Aneurysms
Multiple aneurysms are found in 20–34% of patients with intracranial aneurysms [10,11,12]. Female sex, smoking, and hypertension are all risk factors for developing multiple intracranial aneurysms [11, 12]. When possible, treatment of all aneurysms simultaneously in one procedure is ideal to reduce the number of invasive procedures. Though the overall length of the procedure and risk of complication is increased when treating multiple aneurysms at once, a one-staged operation has overall lower mortality than treating the patient in multiple stages or leaving an unruptured aneurysm untreated [13]. Additionally, one study compared surgical and endovascular treatment for multiple intracranial aneurysms and found similar complication rates (10.9% and 10.3%, respectively) but higher retreatment rates for the endovascular group (3% vs. 18%, respectively) [14]. In cases of multiplicity, microsurgical clip ligation should be considered to safely treat the highest number of aneurysms in the fewest number of procedures if EVT cannot address all of the aneurysms.
Very Small Aneurysms
Very small aneurysms (VSAs) are defined as aneurysms with a maximum diameter of 3 mm or smaller. Whether to treat unruptured VSAs remains controversial due to low reported risk of rupture in large epidemiological studies [15, 16]. Several reasons that may encourage treatment of unruptured VSAs include high risk patient populations, personal or family history of SAH, multiple aneurysms, and irregular shape or daughter sac, all of which portend higher risk of rupture. The International Subarachnoid Aneurysm Trial (ISAT) excluded small aneurysms (≤3 mm) from the trial, which leaves questions about the best treatment strategy for small ruptured aneurysms [17, 18].
Aneurysms ≤3 mm pose technical endovascular challenges for catheterizing the aneurysm, microcatheter stability, and deploying coils into a small volume. Endovascular failure (9.9–13.7%) or incomplete occlusion often results in cross over to surgery [19, 20]. Studies demonstrate that the risk of intraprocedural rupture during EVT is higher for VSAs (7.7%) than larger aneurysms (3.6%) and for ruptured (10.7%) over unruptured (5%) VSAs [19,20,21,22,23]. These data bias toward surgical management for VSAs when treatment is indicated.
Overall, permanent morbidity and mortality are similar between endovascular and surgical treatment of VSAs, but procedure-related complications may be slightly higher for surgical intervention [19, 24, 25]. Data support that very small posterior circulation aneurysms should preferentially undergo endovascular therapy if amenable due to higher postoperative deficits compared to surgically treated anterior circulation aneurysms (45.5% vs. 3.9%, respectively) [22]. Figure 8.1 and Video 8.1 depict a case of young patient with multiple aneurysms including two VSAs.

The case of a young patient who was admitted for Hunt and Hess grade 1 subarachnoid hemorrhage is depicted. (a and b) Anteroposterior and lateral 2-D cerebral angiograms of the right internal carotid artery (ICA) reveal posterior communicating artery (Pcomm) and anterior choroidal artery (AchorA) origin aneurysms (open arrow). A double density at the proximal A1 segment of the ACA is suspicious for an aneurysm. (c) Three-dimensional reconstruction of the right ICA angiogram in the surgical orientation shows the Pcomm and AchorA aneurysms (open arrow) and the posterior wall A1 segment aneurysm (broken arrow). (d) Posteroanterior three-dimensional reconstruction better shows the A1 segment aneurysm (broken arrow). (e) Intraoperative photo of the ICA after dissection of the necks of the Pcomm and AchorA aneurysms. The “shoulder” of both the Pcomm and AchorA are well seen originating at the proximal neck of each aneurysm then taking their typical course behind the ICA. (f) Indocyanine green (ICG) video angiography reveals patency of the AchorA (arrow) – inset shows light microscopy of the selected ICG frame. (g and h) The posterior wall A1 segment aneurysm was occluded with a straight miniclip. (i and j) Intraoperative angiography reveals complete occlusion of the aneurysms and maintained patency of the normal vasculature, including the Pcomm and AchorA
Endovascular Treatment Failures
The volume of EVT failures that require retreatment either endovascularly or microsurgically will continue to grow as the number of endovascular procedures performed increases. In ISAT, 191 patients (17.4%) required retreatment in the endovascular cohort, and 54% of these patients required surgery [26]. Hayakawa et al. followed 73 aneurysms with residual necks an average of 17.3 months, and 49% showed recanalization on follow-up. Wide-neck (≥4 mm) and large or giant aneurysms were more likely to recur [27]. In one series of previously coiled aneurysms requiring microsurgical retreatment, 4 of 81 patients presented with rebleeding [28]. The Cerebral Aneurysm Rerupture After Treatment (CARAT) study demonstrated that rerupture rates increase as the percentage of aneurysm obliteration decreases [29]. Therefore, coiled aneurysms that are incompletely obliterated or recurrent should be monitored very closely and managed aggressively to prevent rerupture.
Aneurysms that have failed prior endovascular therapies may be more difficult to treat due to the biological changes that occur due to the coils or other endovascular device. Coils hold the aneurysm walls apart and induce intraluminal thrombus formation that hardens the aneurysms thus preventing the manipulation that can be afforded by collapsing the aneurysm sac with temporary clipping. Coils can erode through the aneurysm dome and extrude into the subarachnoid space which makes dissection of the aneurysm and branching arteries challenging. Coils can protrude into the neck of the aneurysm, the parent artery, or branching vessels complicating the placement of clips. Clipping is easiest when sufficient aneurysm recurrence is present to apply the aneurysm clip along the long axis of the parent vessel and occlude the neck below the coil mass. A ratio of the maximum transverse dimension of the coil mass to the height from the neck to the coil compaction of <2.5 has been correlated with successful clip application with limited complications [30].
The decision for retreatment of an endovascularly treated aneurysm must take into account the size and configuration of the remnant, location of the aneurysm, patient’s age and medical condition, and the endovascular techniques used. A recurrence is considered significant if it is progressively enlarging on serial imaging studies or the occlusion is <90% of the total aneurysm volume. Many endovascular recurrences or incomplete treatment may now be treated with more recent endovascular techniques, such as flow diversion. When surgery is determined to be the best option, most incompletely coiled and recurrent aneurysms are able to be treated with direct clipping with or without removal of coils (70–95%) [28, 31,32,33]. If surgery is performed shortly after coiling (i.e., within 1 month), coils are more easily removed; however, coils can be densely incorporated into thrombus after just 2 weeks rendering removal difficult or unsafe [28, 31]. Typically, coils should only be removed if the coil mass impedes clipping [33]. If coil removal is of too high risk and simple clipping is impossible, various bypass and trapping strategies can be employed to eliminate the aneurysm from the circulation [32]. Coils should not be removed if they are inside the parent artery or perforators due to the risk of injury to these vessels during extraction.
Good or excellent outcomes can be achieved in these patients after surgery (71–90%) with acceptable morbidity and mortality [28, 30,31,32,33]. Poor outcomes were related to the size of the aneurysm, location of the aneurysm in the posterior circulation, intraoperative rupture, and removal of coils during surgery [28]. Figure 8.2 depicts a case of a giant, recurrent, right MCA aneurysm that had been previously coiled.


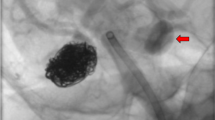
Microsurgical treatment of a giant, partially thrombosed right M1 segment aneurysm after endovascular treatment failure. A 36-year-old man presented with left-sided hemiparesis and 1 week of worsening headache with nausea. (a) Computed tomography scan showed a large recurrence of a previously coiled aneurysm with intraluminal hemorrhage. (b) Angiography showed only partial filling of the aneurysm and marked stenosis of the middle cerebral artery (MCA) beyond the neck of the aneurysm. The outline of the aneurysm is noted by red dots. Lenticulostriates draped over the lateral margin of the aneurysm are delineated by green arrows. (c) The surgical strategy was to perform a radial artery bypass graft from the common carotid artery to an M2 segment (red arrow – recipient site) with clip occlusion distal to the neck of the aneurysm (red bar). (d) Intraoperative image of the radial artery to M2 anastomosis. (e and f) One-month follow-up angiogram demonstrated the radial artery bypass filling the entire MCA distribution with back filling of the lenticulostriate arteries (green arrows), and complete occlusion of the aneurysm. Occlusion of the aneurysm and proximal M1 segment are demonstrated as the delayed angiogram shows that the internal carotid artery terminates at the A1
Contraindications to Dual Antiplatelet Therapies and Noncompliant Patients
Dual antiplatelet therapy (DAPT) is needed for the placement of an intracranial stent or flow diverter to minimize thromboembolic complications. Employing DAPT should be balanced with the risk of bleeding and individualized for each patient. Some patients have contraindications to DAPT which may make microsurgical clip ligation necessary. Contraindications to DAPT include known esophageal varices or gastric ulcers, thrombocytopenia (50,000/μL blood), decompensated liver disease or baseline INR >1.5, other coagulopathy, barriers to compliance (i.e., polysubstance abuse, dementia, and financial constraints), or imminent need for major surgery. While thrombocytopenia and coagulopathy are relative contraindications to cranial surgery, these can typically be corrected and maintained within normal limits in the short term to safely complete surgery.
Many patients presenting with ruptured aneurysms require external ventricular drain (EVD) or ventriculoperitoneal (VP) shunt placement for cerebrospinal fluid diversion. In one series, six of seven patients on DAPT for stent-assisted coiling who required placement of an EVD and/or VP shunt suffered a hemorrhagic complication. Four of these instances were due to placement or exchange of a ventricular catheter, and the remaining two patients suffered rebleeding events [34]. We are, therefore, hesitant to treat patients with aneurysmal SAH by endovascular methods that require DAPT. In the case of flow diversion, the aneurysm may not be immediately secured, which does not mitigate the risk of rebleeding.
Additionally, patients who may be noncompliant with DAPT regimen or unable to maintain the prescribed follow-up after EVT are better candidates for microsurgical treatment. Inability to correctly take a DAPT regimen after stent-assisted coiling or flow diversion could lead to disastrous thromboembolic complications. EVT requires diligent follow-up due to the higher rate of aneurysm recurrence and rerupture when compared to microsurgical treatment [29].
Associated Intracerebral Hemorrhage
Approximately 12–21% of patients with aneurysmal SAH present with concomitant intracerebral hemorrhage (ICH) [35, 36]. Patients with SAH and an associated ICH have worse Hunt and Hess grades on presentation and worse outcomes than those without ICH [36]. Aneurysms with associated ICH are more likely to be located on the middle cerebral artery (MCA) or anterior communicating artery (ACoA) [36]. Studies demonstrate substantial functional and mortality benefit in patients who undergo surgical evacuation of the associated ICH and clip ligation of the offending aneurysm compared to those treated without surgical decompression of the brain [37, 38]. The primary benefit of an endovascular procedure is avoidance of a craniotomy. If the patient needs surgery for evacuation of a life- or health-threatening hematoma, treatment of the aneurysm at the time of the craniotomy is the most parsimonious therapeutic strategy. Figure 8.3 demonstrates a case of a large, ruptured right MCA aneurysm with an associated ICH.


A middle-aged gentleman admitted with a Hunt and Hess grade 3 subarachnoid hemorrhage is shown. (a–c) Preoperative axial noncontrast computed tomography (CT) of the head shows a large intraparenchymal hemorrhage (IPH) in the right temporal lobe. (d–g) Two- and three-dimensional cerebral angiography revealed a large right middle cerebral artery (MCA) bifurcation aneurysm. (h) Intraoperative photo after clipping shows reconstruction of the MCA bifurcation and obliteration of the aneurysm using a side-angled clip placed parallel to the origins of the M2 segment takeoffs (M2f – frontal division; M2t – temporal division; M1 – M1 segment coming out of the Sylvian fissure). (i and j) Intraoperative angiography shows complete elimination of the aneurysm from the circulation. (k) Intraoperative photo after removal of the IPH. The IPH was removed from the point at which it broke through the temporal lobe surface anteriorly. The dome of the aneurysm is seen in the resection cavity (black arrows). (l–n) Postoperative CT shows near-complete evacuation of the IPH
Large Aneurysms with Mass Effect
Large (13–24 mm) and giant (≥25 mm) IAs pose technical challenges due to development of calcification at the neck and partial thrombosis of the dome, presence of perforators and branch vessels from the aneurysmal walls, and compression of adjacent brain or cranial nerves. Left untreated, giant aneurysms are associated with 70–80% morbidity and mortality rates over 2 years due to rupture, thromboembolic complications, or progressive compressive symptoms [39, 40].
Endovascular vessel sacrifice or surgical trapping is often not feasible for aneurysms that are at or distal to the internal carotid artery (ICA) bifurcation or for patients that fail a balloon test occlusion (BTO). Large and giant aneurysms have a well-documented low complete occlusion rate and high rate of recanalization after endovascular coiling, necessitating subsequent retreatment [41, 42]. Although well established to treat aneurysms of the petrocavernous and paraclinoid segments of the ICA, flow diversion does not immediately address the mass effect of large and giant IAs and can cause compressive symptoms to worsen [6, 43]. Consequently, surgical management remains a mainstay of treatment of large and giant IAs. Once the aneurysm is surgically occluded, it can be punctured or intrasaccular thrombus can be resected to immediately reduce the mass effect on critical structures, such as cranial nerves, the optic apparatus, or the brainstem. Figure 8.4 and Video 8.2 depict a case of a giant left ophthalmic artery origin ICA aneurysm treated by clipping followed by decompression of the optic apparatus.

Giant thrombotic internal carotid artery aneurysm arising at the ophthalmic segment causing mass effect. A 59-year-old man presented with progressive vision loss. Axial (a) and coronal (b) T1 pre-contrast magnetic resonance images with a large heterogeneous mass displacing the optic chiasm. (c) Angiography showed a partially thrombosed left ophthalmic artery aneurysm with residual filling measuring 5.3 mm × 6.7 mm × 5.6 mm with a 4.1 mm neck. (d and e) Intraoperative angiography demonstrated complete occlusion of the aneurysm after placement of single side-angled clip. (f) Follow-up computed tomography scan showed decreased mass effect after aneurysm debulking
Many large and giant aneurysms can be primarily clipped or clip reconstructed (40–60%) [39, 42, 44]. Simple clipping is the preferred treatment strategy but is often prevented by dolichoectatic morphology, aberrant branch anatomy, atherosclerosis at the aneurysm neck, and intraluminal thrombosis. Aneurysms that cannot be directly clipped require alternative techniques to indirectly occlude the aneurysm, which include distal occlusion, proximal occlusion, trapping, or excision with or without bypass. Overall, treatment-related surgical morbidity and mortality for giant IAs is approximately 20–30% with mortality comprising 8–22% [39, 42, 44].
When collateral circulation is inadequate to provide sufficient perfusion after permanent vessel occlusion, a revascularization procedure is required. BTO may be used in selected patients to determine which patients will not tolerate parent vessel occlusion. Many bypass techniques have been described, and the selection of bypass type depends on the location of the aneurysm, the need for low- versus high-flow revascularization, and surgeon preference. Special surgical considerations during bypass procedures include starting aspirin prior to surgery, giving intravenous heparin during the anastomosis, and inducing burst suppression and arterial pressure elevation to 20% above baseline during temporary clip occlusion.
Wide-Necked Aneurysms
The most commonly used definition for wide-necked aneurysms (WNAs) is neck size ≥4 mm or dome-to-neck ratio <2. Many endovascular techniques exist for the treatment of WNAs including balloon-assisted coiling, stent-assisted coiling, complex neck support devices (i.e., PulseRider and pCONus), parent artery flow diversion (i.e., Pipeline, FRED, and Surpass), and intra-saccular flow diversion (i.e., Woven EndoBridge). Brinjikji et al. found that aneurysms with aspect (height-to-neck) and dome-to-neck ratios >1.6 typically did not require the use of adjunctive techniques during EVT [45]. WNAs are more likely to have a neck remnant and more likely to have recanalization on follow-up than aneurysms with narrow necks after coil embolization [27, 41].
Few studies have examined the results of microsurgical clipping of WNAs while a large number of studies have examined EVT. A post hoc subgroup analysis in the Barrow Ruptured Aneurysm Trial (BRAT) examined WNAs. WNAs comprised 54.1% of the aneurysms treated; were more likely to arise from the MCA, basilar tip, or internal carotid artery (ICA) other than the ICA-posterior communicating artery (PCoA) junction; and were more common in older patients with worse clinical presentation. Complete obliteration on postoperative imaging was lower and retreatment rate was higher for coiling compared with clipping (51.2% vs. 84.3% and 26.8% vs. 0%, respectively), but clinical outcomes after either treatment were not significantly different at any time point [46]. A meta-analysis comparing EVT to surgical clipping for wide-necked bifurcation aneurysms showed similar adverse events (21.1% vs. 24.3%) but lower complete occlusion with EVT (39.8% vs. 52.5%) [47].
Complex Configuration
Numerous factors can make an IA “complex” including deep location, wide neck, large size, inclusion of branching vessels, dolichoectactic morphology, presence of intraluminal thrombus or atherosclerotic walls, or previous endovascular or surgical treatments. Simple aneurysms are readily treated with current endovascular techniques including stand-alone coiling, balloon- or stent-assisted coiling, or parent artery and intra-saccular flow diversion. As this field develops, vascular neurosurgeons are left with more complex aneurysms deemed unsuitable for endovascular therapies. Microsurgical treatment of complex IAs requires careful planning and innovative thinking, expanding the exposure with skull base approaches, temporary occlusion or hypothermic circulatory arrest, the use of a variety of bypass techniques, and, sometimes, the combination of microsurgical and endovascular treatments.
Aneurysms with complex configurations are often located at branch points and have efferent arteries arising from the aneurysm walls. Clip reconstruction is the preferred strategy to obliterate the aneurysm and maintain patency of the parent and branching arteries. When this is not feasible, vessel occlusion (i.e., distal, proximal, or both [trapping]) or aneurysm excision with or without bypass can be performed. Many bypass techniques have been described for the treatment of complex aneurysms including extracranial-intracranial (EC-IC) bypass, EC-IC interpositional bypass, reimplantation, reanastamosis, in situ bypass, IC-IC interpositional bypass, and combination bypass [48]. When microsurgical and endovascular techniques are used together, the number of possible treatment strategies increases drastically to include the following possibilities: coil embolization after partial aneurysm clipping to narrow the neck, endovascular parent vessel and aneurysm occlusion after surgical bypass, proximal endovascular occlusion after distal surgical occlusion and bypass for complete trapping of aneurysm, aneurysm debulking after endovascular parent vessel occlusion, and balloon catheter placement for temporary proximal occlusion and/or suction decompression to allow for surgical clipping [49,50,51,52,53].
Several clinical series have been published examining the combination of endovascular and microsurgical management for complex aneurysms. Aneurysm occlusion was obtained in 95% of cases [49, 51]. Good or excellent outcomes were seen in 77.1–86% of patients, permanent morbidity occurred in 5.2–8.3%, and procedural mortality was 9.1–14.3% [49, 51, 52]. As seen previously, death or poor outcome was more common after the treatment of a posterior circulation aneurysm than an anterior circulation aneurysm [51, 52].
Thrombotic Aneurysms
Cerebral aneurysms with significant intraluminal thrombus are poorly described in the literature because they are often included in larger series along with fusiform or giant aneurysms, but account for up to 16.8% of aneurysms [54]. These aneurysms should be studied with CT and/or MRI plus catheter angiography due to the discrepancies between aneurysm size and luminal filling. Most patients present with symptoms from mass effect (32%), which is indicative of their predilection to be larger in size. Only 10% of patients with thrombotic aneurysms present with embolic symptoms [55].
Surgical treatment is often preferred to endovascular therapies for thrombosed aneurysms, for which recanalization after coiling is up to five times greater than in non-thrombosed aneurysms [54]. Recurrence of thrombotic aneurysms is multifactorial and likely related to their large or giant size, coil migration into the adjacent thrombus, and failure to endothelialize across the neck [41, 56].
Microsurgical approaches include direct clipping, thrombectomy with clip reconstruction, bypass with aneurysm occlusion, and trapping without bypass. The best surgical results were achieved with direct clipping, which is dependent on compliance of the neck of the aneurysm. Concentric and complete thrombotic aneurysms have noncompliant necks, and canalized thrombotic aneurysms do not have a defined neck. Eccentric thrombotic aneurysms or coiled thrombotic aneurysms with eccentric coil compaction were more likely to be amenable to direct clipping. For unclippable thrombotic aneurysms, better results were achieved with bypass and parent vessel occlusion over thrombectomy with clip reconstruction [55]. Observation is recommended for completely thrombosed aneurysms.
Fusiform or Dolichoectatic Aneurysms
Fusiform aneurysms comprise <0.1% of IAs [57]. They are defined based on appearance of fusiform arterial ectasia at a nonbranching site. In contrast to saccular aneurysms, fusiform aneurysms are more often found in younger patients and more frequently in males [57,58,59]. The proposed mechanism of formation starts with arterial dissection [58]. The acute dissecting type typically presents with rupture, whereas the chronic type presents with continual growth [60, 61]. Patients may be diagnosed incidentally due to compressive symptoms related to mass effect on the brain or cranial nerves, thromboembolic events, or rupture. Patients with fusiform aneurysms associated with atherosclerosis, symptomatic presentation, or size >7 mm are at higher risk for progression [62]. A select group of patients can tolerate conservative management or anticoagulation alone with good results.
These lesions are extremely difficult to treat whether by endovascular techniques, microsurgery, or a multidisciplinary approach. Surgical treatment carries a morbidity and mortality rate of approximately 25% [57,58,59, 62]. Surgical options include clip reconstruction, clip wrapping, bypass and trapping, proximal or distal occlusion only, or excision with reanastomosis [57, 61].
Infectious Aneurysms
Infectious IAs (I-IAs) account for approximately 2% of all IAs [6, 63]. Infective endocarditis is responsible for 70-80% of infectious aneurysms, which typically occur in the distal MCA territory [63, 64]. Extravascular infections such as meningitis, cavernous sinus thrombophlebitis, cerebral abscess, subdural empyema, osteomyelitis of the skull, and sinus infections can also cause infectious aneurysms. These aneurysms typically occur in more proximal locations due to direct infectious spread at the base of the brain.
I-IAs are most commonly due to Streptococcus species or Staphylococcus aureus, but can be caused by a variety of bacterial, fungal, spirochetal, amebic, or viral pathogens [63, 65]. Pathologic changes show infiltration of the adventitia and tunica media by polymorphonuclear leukocytes, marked intimal proliferation, and destruction of the internal elastic lamina. They are typically friable and thin-walled with a wide or absent neck and are often not easy to separate from the brain parenchyma.
No trials exist comparing surgical and endovascular treatment of I-IAs; therefore, treatment recommendations are based on large case series and systematic reviews. Unruptured infectious aneurysms should initially be treated with appropriate antibiotic therapy for at least 4-6 weeks. Repeat imaging can be performed at 1-week intervals initially to determine stability or change in aneurysm size. Surgical or endovascular treatment should be pursued if an unruptured aneurysm increases in size despite antibiotic therapy, or if a patient presents with a ruptured aneurysm. Rupture of I-IAs may occur in as high as 75% of cases [64]. Morbidity and mortality from infectious aneurysms are 36% and 20%, respectively, though this is likely an underestimate due to death before presentation to neurosurgical attention [63]. If hospitalized for endocarditis, mortality in patients with unruptured I-IAs is 30% but is 80% if ruptured [66]. Fungal etiologies are more frequently fatal despite medical or surgical therapy [65].
Surgical clipping, trapping, or excision of an I-IA is preferred if a symptomatic hematoma is present, if eloquent territory is at risk from parent artery occlusion, or if inaccessible by endovascular means. Surgery offers the opportunity to perform an anastomotic procedure if eloquent, distal circulation will be affected by vessel sacrifice. If the I-IA is proximal to ineloquent brain and is on a sufficiently small vessel, the diseased parent artery may be sacrificed, particularly if a long segment of the artery is diseased, as in the case presented in Fig. 8.5 and Video 8.3. Frameless stereotactic guidance is helpful when the aneurysm is buried within unusual locations. Open surgical treatment confers a higher rate of success than medical therapy and similar complication rate to EVT [64, 65]. EVT may be favored in cases in which the patient has severe cardiac dysfunction and anesthesia risks are too great.

An elderly gentleman with infectious endocarditis was admitted with a left frontoparietal intraparenchymal hemorrhage (IPH). (a) Axial noncontrast head computed tomography (CT) shows the IPH, while CT angiography demonstrated a M4 segment middle cerebral artery (MCA) aneurysm. (b) Sequential intraoperative photos show removal of the IPH, which unveils the dome of the aneurysm (open arrow). Further dissection reveals the diseased M4 branch proximal to the aneurysm (green arrows). The aneurysm is noted to involve 360° of the vessel lumen with no neck, which rendered clip reconstruction impossible. Aneurysm clips were applied and the aneurysm was excised (open arrowhead). After complete removal of the IPH and sacrifice of the diseased segment the brain is relaxed (blue circle). Shown in the accompanying video, but not here, primary reanastomosis was attempted, but the vessel was under too much tension and given that the branch supplied blood to brain posterior to the primary motor area, the decision was made to excise the aneurysm without reanastamosis. (c) Postoperative CT and magnetic resonance images show the clips, complete IPH evacuation, and no ischemic changes distal to the vessel sacrifice
Pseudoaneurysms
Pseudoaneurysms represent <1% of all IAs, but constitute as high as 20% of pediatric IAs [67, 68]. Pseudoaneurysm rupture is associated with mortality as high at 30% [69]. The most common cause of pseudoaneurysms is penetrating or blunt trauma. Other causes include iatrogenic (i.e., trans-sphenoidal surgery, sinus surgery, ventricular taps, stereotactic brain biopsy, endoscopic third ventriculostomy), infectious, radiation-associated, and connective tissue disease. False aneurysms or pseudoaneurysms are distinct from true aneurysms because they are caused by complete disruption of the vessel wall. A contained hematoma outside the vessel then develops a false lumen. The lack of well-formed walls in pseudoaneurysms makes both clipping and coiling difficult.
Despite advancements of EVTs, several limitations remain, including inaccessible distal locations, risk of intraprocedural rupture due to the lack of aneurysm wall, and coil extrusion through the false lumen leading to recurrence of the aneurysm. EVTs are most useful in locations where there are bony confines, like the petrous or cavernous segments of the internal carotid artery, and subacute pseudoaneurysms where the walls are more mature [70]. While the use of DAPT can be limiting, flow diversion has gained traction in the treatment of these lesions, particularly as they provide an intraluminal scaffold for endothelialization.
Many surgical techniques have been used to treat pseudoaneurysms including clipping, vascular reconstruction and revascularization, trapping, wrapping, or simple excision with or without arterial bypass. Direct clipping is possible only in 10–15% [63]. As previously stated, surgery is the preferred treatment strategy for ruptured pseudoaneurysms with associated large ICHs that need urgent evacuation.
Basic Principles of Surgery
Considerations for surgical approach to specific aneurysms are addressed elsewhere; however, the basic tenets of microsurgical clipping of IAs are reviewed in the ensuing text.
Anesthetic Considerations
Optimal management of the patient in the operating room depends on open communication between the surgical and anesthesia teams. Generally, the anesthetic used should be short acting, not reduce cerebral blood flow or increase intracranial pressure, and allow for careful blood pressure control. When using motor and somatosensory evoked potentials, total intravenous anesthesia may be necessary. The anesthesiologist should employ measures to decrease the intracranial pressure including mild hyperventilation, osmotic diuresis with mannitol, and monitoring output from the EVD if present. During temporary occlusion, the blood pressure should be augmented (i.e., goal mean arterial pressure [MAP] >90 mmHg) and burst suppression may be induced to limit the risk of cerebral ischemia [1, 6]. Systemic mild hypothermia is widely used during aneurysm surgery for brain protection. In rare circumstances, deep hypothermic circulatory arrest can prolong the duration of cessation of blood flow during the final aneurysm dissection and clip reconstruction. The anesthesiologist should have adenosine readily available to induce transient cardiac arrest in the event of an untimely intraoperative rupture. Finally, the anesthesia team should closely monitor glucose and electrolytes to prevent hyperglycemia, hyponatremia, or hyperkalemia. Typed and cross-matched blood should be available for all aneurysm surgery.
Positioning and Craniotomy
The chosen craniotomy should maximize surgical exposure and shorten the surgical corridor as much as possible. No matter the surgical approach, the head should be positioned above the heart and as neutral as possible to aid in venous drainage and prevent hyperemia. In addition, the surgeon should use gravity to enhance exposure where possible. Adequate bony exposure minimizes the need for fixed retractors and provides sufficient room to obtain distal and proximal control while providing sufficient degrees of freedom to maximize clip application angle.
Microsurgical Technique
Mannitol is given prior to skin incision to improve rheology and relax the brain to facilitate subarachnoid dissection. The intradural component of aneurysm surgery is completed using a surgical microscope to maximize illumination and magnification. The CSF cisterns are then opened sequentially from superficial to deep taking care not to breach the pia, which may be injurious to the surrounding brain. Microdissection is carried out both sharply, to cut recalcitrant bands of arachnoid, and with gentle spreading using micro-forceps. Blunt dissection is generally directed along the long axis of the sulcus or fissure to be opened with force applied perpendicular to the brain surfaces (e.g., the Sylvian fissure is opened parallel to its overall course, either distal to proximal, or vice versa, but application of force applied by the tips and shaft of the micro-forceps are directed outward from the middle of the Sylvian fissure to gently separate the frontal and temporal lobes). Temporary clipping is a useful surgical adjunct to make final dissection of the aneurysm neck and clip application safer. In addition, temporary clipping softens large, turgid aneurysms to allow for complete reconstruction. Blind or excessive blunt dissection should be minimized or completely avoided, particularly around the aneurysm neck, to prevent tearing of the aneurysm, which may be challenging to repair. Permanent clips come in a variety of sizes and configurations, making clipping versatile and durable. In general, the simplest possible clipping strategy should be employed to maximize the likelihood of complete aneurysm occlusion while limiting the chance of parent or branch vessel compromise. When possible, the long axis of the clip(s) should be placed parallel to the long access of the parent vessel to limit vessel wall stress at the neck. In the face of intraoperative rupture, calm on the part of the surgeon is paramount. The field is cleared of blood with large-bore suctions, proximal and distal vessel control is achieved, neck dissection is completed, and permanent clips are applied. Cotton tamponade can be gently applied over the site of rupture, either using a suction or by applying light pressure with a fixed retractor to act as a “third hand.” The surgeon must consciously avoid the temptation to prematurely “jam” permanent clips across the aneurysm before complete dissection and visualization is achieved. So doing may worsen the rent in the aneurysm and/or parent artery, or avulse small perforating arteries. Once the aneurysm is occluded, temporary clips are removed sequentially from distal to proximal. Each temporary clip is opened partially and the field is closely inspected to assure no residual bleeding before the clip is completely removed. Finally, the surgeon must be prepared for a variety of bailout options, such as cotton-clipping used in the setting of a neck tear, or bypass to revascularize permanently compromised vessels.
Conclusion
As endovascular technology advances, the pool of IAs treated surgically continues to ebb. However, the complexity of aneurysms referred for surgical treatment has increased as a result. Indubitably, the need for well-trained, capable cerebrovascular surgeons will continue into the future. IAs currently considered for microsurgical treatment in the current era include those in the very young, geometries not amenable to EVT, endovascular failures, patients intolerant to or noncompliant with DAPT required for EVT, ruptured aneurysms with associated ICH, very small aneurysms, large and giant aneurysms – particularly those with thrombus – and infectious aneurysms among others.
References
Connolly ES, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. Stroke. 2012;43(6):1711–37.
Thompson BG, Brown RD Jr, Amin-Hanjani S, Broderick JP, Cockroft KM, Connolly ES Jr, et al. Guidelines for the management of patients with unruptured intracranial aneurysms: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46(8):2368–400.
Lai LT, O'Neill AH. History, evolution, and continuing innovations of intracranial aneurysm surgery. World Neurosurg. 2017;102:673–81.
Cowan JA Jr, Ziewacz J, Dimick JB, Upchurch GR Jr, Thompson BG. Use of endovascular coil embolization and surgical clip occlusion for cerebral artery aneurysms. J Neurosurg. 2007;107(3):530–5.
Howard BM, Hu R, Barrow JW, Barrow DL. Comprehensive review of imaging of intracranial aneurysms and angiographically negative subarachnoid hemorrhage. Neurosurg Focus. 2019;47(6):E20.
Winn HR. Youmans and Winn neurological surgery. Philadelphia: Elsevier; 2017.
Gross BA, Smith ER, Scott RM, Orbach DB. Intracranial aneurysms in the youngest patients: characteristics and treatment challenges. Pediatr Neurosurg. 2015;50(1):18–25.
Sanai N, Quinones-Hinojosa A, Gupta NM, Perry V, Sun PP, Wilson CB, et al. Pediatric intracranial aneurysms: durability of treatment following microsurgical and endovascular management. J Neurosurg. 2006;104(2 Suppl):82–9.
Kakarla UK, Beres EJ, Ponce FA, Chang SW, Deshmukh VR, Bambakidis NC, et al. Microsurgical treatment of pediatric intracranial aneurysms: long-term angiographic and clinical outcomes. Neurosurgery. 2010;67(2):237–49; discussion 50.
Rinne J, Hernesniemi J, Puranen M, Saari T. Multiple intracranial aneurysms in a defined population: prospective angiographic and clinical study. Neurosurgery. 1994;35(5):803–8.
Juvela S. Risk factors for multiple intracranial aneurysms. Stroke. 2000;31(2):392–7.
Jabbarli R, Dinger TF, Darkwah Oppong M, Pierscianek D, Dammann P, Wrede KH, et al. Risk factors for and clinical consequences of multiple intracranial aneurysms: a systematic review and meta-analysis. Stroke. 2018;49(4):848–55.
Rinne J, Hernesniemi J, Niskanen M, Vapalahti M. Management outcome for multiple intracranial aneurysms. Neurosurgery. 1995;36(1):31–7; discussion 7–8.
Dong QL, Gao BL, Cheng ZR, He YY, Zhang XJ, Fan QY, et al. Comparison of surgical and endovascular approaches in the management of multiple intracranial aneurysms. Int J Surg (London, England). 2016;32:129–35.
Greving JP, Wermer MJ, Brown RD Jr, Morita A, Juvela S, Yonekura M, et al. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol. 2014;13(1):59–66.
Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet (London, England). 2003;362(9378):103–10.
Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet (London, England). 2002;360(9342):1267–74.
Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet (London, England). 2005;366(9488):809–17.
Chalouhi N, Penn DL, Tjoumakaris S, Jabbour P, Gonzalez LF, Starke RM, et al. Treatment of small ruptured intracranial aneurysms: comparison of surgical and endovascular options. J Am Heart Assoc. 2012;1(4):e002865.
Pierot L, Barbe C, Spelle L. Endovascular treatment of very small unruptured aneurysms: rate of procedural complications, clinical outcome, and anatomical results. Stroke. 2010;41(12):2855–9.
Brinjikji W, Lanzino G, Cloft HJ, Rabinstein A, Kallmes DF. Endovascular treatment of very small (3 mm or smaller) intracranial aneurysms: report of a consecutive series and a meta-analysis. Stroke. 2010;41(1):116–21.
Bruneau M, Amin-Hanjani S, Koroknay-Pal P, Bijlenga P, Jahromi BR, Lehto H, et al. Surgical clipping of very small unruptured intracranial aneurysms: a multicenter international study. Neurosurgery. 2016;78(1):47–52.
van Rooij WJ, Keeren GJ, Peluso JP, Sluzewski M. Clinical and angiographic results of coiling of 196 very small (< or = 3 mm) intracranial aneurysms. AJNR Am J Neuroradiol. 2009;30(4):835–9.
Li J, Su L, Ma J, Kang P, Ma L, Ma L. Endovascular coiling versus microsurgical clipping for patients with ruptured very small intracranial aneurysms: management strategies and clinical outcomes of 162 cases. World Neurosurg. 2017;99:763–9.
Zhao B, Xing H, Fan L, Tan X, Zhong M, Pan Y, et al. Endovascular coiling versus surgical clipping of very small ruptured anterior communicating artery aneurysms. World Neurosurg. 2019;126:e1246–e50.
Campi A, Ramzi N, Molyneux AJ, Summers PE, Kerr RS, Sneade M, et al. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT). Stroke. 2007;38(5):1538–44.
Hayakawa M, Murayama Y, Duckwiler GR, Gobin YP, Guglielmi G, Viñuela F. Natural history of the neck remnant of a cerebral aneurysm treated with the Guglielmi detachable coil system. J Neurosurg. 2000;93(4):561–8.
Romani R, Lehto H, Laakso A, Horcajadas A, Kivisaari R, von und zu Fraunberg M, et al. Microsurgery for previously coiled aneurysms: experience with 81 patients. Neurosurgery. 2011;68(1):140–53; discussion 53–4.
CARAT Investigators. Rates of delayed rebleeding from intracranial aneurysms are low after surgical and endovascular treatment. Stroke. 2006;37(6):1437–42.
Owen CM, Montemurro N, Lawton MT. Microsurgical management of residual and recurrent aneurysms after coiling and clipping: an experience with 97 patients. Neurosurgery. 2015;62 Suppl 1:92–102.
Gurian JH, Martin NA, King WA, Duckwiler GR, Guglielmi G, Viñuela F. Neurosurgical management of cerebral aneurysms following unsuccessful or incomplete endovascular embolization. J Neurosurg. 1995;83(5):843–53.
Waldron JS, Halbach VV, Lawton MT. Microsurgical management of incompletely coiled and recurrent aneurysms: trends, techniques, and observations on coil extrusion. Neurosurgery. 2009;64(5 Suppl 2):301–15; discussion 15–7.
Zhang YJ, Barrow DL, Cawley CM, Dion JE. Neurosurgical management of intracranial aneurysms previously treated with endovascular therapy. Neurosurgery. 2003;52(2):283–93; discussion 93–5.
Tumialán LM, Zhang YJ, Cawley CM, Dion JE, Tong FC, Barrow DL. Intracranial hemorrhage associated with stent-assisted coil embolization of cerebral aneurysms: a cautionary report. J Neurosurg. 2008;108(6):1122–9.
Wan A, Jaja BN, Schweizer TA, Macdonald RL. Clinical characteristics and outcome of aneurysmal subarachnoid hemorrhage with intracerebral hematoma. J Neurosurg. 2016;125(6):1344–51.
Abbed KM, Ogilvy CS. Intracerebral hematoma from aneurysm rupture. Neurosurg Focus. 2003;15(4):E4.
Wheelock B, Weir B, Watts R, Mohr G, Khan M, Hunter M, et al. Timing of surgery for intracerebral hematomas due to aneurysm rupture. J Neurosurg. 1983;58(4):476–81.
Heiskanen O, Poranen A, Kuurne T, Valtonen S, Kaste M. Acute surgery for intracerebral haematomas caused by rupture of an intracranial arterial aneurysm. A prospective randomized study. Acta Neurochir. 1988;90(3-4):81–3.
Kodama N, Suzuki J. Surgical treatment of giant aneurysms. Neurosurg Rev. 1982;5(4):155–60.
Gonzalez NR, Duckwiler G, Jahan R, Murayama Y, Viñuela F. Challenges in the endovascular treatment of giant intracranial aneurysms. Neurosurgery. 2006;59(5 Suppl 3):S113–24; discussion S3–13.
Murayama Y, Nien YL, Duckwiler G, Gobin YP, Jahan R, Frazee J, et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years’ experience. J Neurosurg. 2003;98(5):959–66.
Sughrue ME, Saloner D, Rayz VL, Lawton MT. Giant intracranial aneurysms: evolution of management in a contemporary surgical series. Neurosurgery. 2011;69(6):1261–70; discussion 70–1.
Malisch TW, Guglielmi G, Viñuela F, Duckwiler G, Gobin YP, Martin NA, et al. Unruptured aneurysms presenting with mass effect symptoms: response to endosaccular treatment with Guglielmi detachable coils. Part I. Symptoms of cranial nerve dysfunction. J Neurosurg. 1998;89(6):956–61.
Cantore G, Santoro A, Guidetti G, Delfinis CP, Colonnese C, Passacantilli E. Surgical treatment of giant intracranial aneurysms: current viewpoint. Neurosurgery. 2008;63(4 Suppl 2):279–89; discussion 89–90.
Brinjikji W, Cloft HJ, Kallmes DF. Difficult aneurysms for endovascular treatment: overwide or undertall? AJNR Am J Neuroradiol. 2009;30(8):1513–7.
Mascitelli JR, Lawton MT, Hendricks BK, Nakaji P, Zabramski JM, Spetzler RF. Analysis of wide-neck aneurysms in the barrow ruptured aneurysm trial. Neurosurgery. 2019;85(5):622–31.
Fiorella D, Arthur AS, Chiacchierini R, Emery E, Molyneux A, Pierot L. How safe and effective are existing treatments for wide-necked bifurcation aneurysms? Literature-based objective performance criteria for safety and effectiveness. J Neurointerv Surg. 2017;9(12):1197–201.
Lawton MT, Lang MJ. The future of open vascular neurosurgery: perspectives on cavernous malformations, AVMs, and bypasses for complex aneurysms. J Neurosurg. 2019;130(5):1409–25.
Lawton MT, Quinones-Hinojosa A, Sanai N, Malek JY, Dowd CF. Combined microsurgical and endovascular management of complex intracranial aneurysms. Neurosurgery. 2003;52(2):263–74; discussion 74–5.
Choudhri O, Mukerji N, Steinberg GK. Combined endovascular and microsurgical management of complex cerebral aneurysms. Front Neurol. 2013;4:108.
Ponce FA, Albuquerque FC, McDougall CG, Han PP, Zabramski JM, Spetzler RF. Combined endovascular and microsurgical management of giant and complex unruptured aneurysms. Neurosurg Focus. 2004;17(5):E11.
Hoh BL, Putman CM, Budzik RF, Carter BS, Ogilvy CS. Combined surgical and endovascular techniques of flow alteration to treat fusiform and complex wide-necked intracranial aneurysms that are unsuitable for clipping or coil embolization. J Neurosurg. 2001;95(1):24–35.
Hanel RA, Spetzler RF. Surgical treatment of complex intracranial aneurysms. Neurosurgery. 2008;62(6 Suppl 3):1289–97; discussion 97–9.
Kim SJ, Choi IS. Midterm outcome of partially thrombosed intracranial aneurysms treated with guglielmi detachable coils. Interv Neuroradiol. 2000;6(1):13–25.
Lawton MT, Quiñones-Hinojosa A, Chang EF, Yu T. Thrombotic intracranial aneurysms: classification scheme and management strategies in 68 patients. Neurosurgery. 2005;56(3):441–54; discussion -54.
Molyneux AJ, Ellison DW, Morris J, Byrne JV. Histological findings in giant aneurysms treated with Guglielmi detachable coils. Report of two cases with autopsy correlation. J Neurosurg. 1995;83(1):129–32.
Anson JA, Lawton MT, Spetzler RF. Characteristics and surgical treatment of dolichoectatic and fusiform aneurysms. J Neurosurg. 1996;84(2):185–93.
Day AL, Gaposchkin CG, Yu CJ, Rivet DJ, Dacey RG Jr. Spontaneous fusiform middle cerebral artery aneurysms: characteristics and a proposed mechanism of formation. J Neurosurg. 2003;99(2):228–40.
Drake CG, Peerless SJ. Giant fusiform intracranial aneurysms: review of 120 patients treated surgically from 1965 to 1992. J Neurosurg. 1997;87(2):141–62.
Nakatomi H, Segawa H, Kurata A, Shiokawa Y, Nagata K, Kamiyama H, et al. Clinicopathological study of intracranial fusiform and dolichoectatic aneurysms : insight on the mechanism of growth. Stroke. 2000;31(4):896–900.
Safavi-Abbasi S, Kalani MYS, Frock B, Sun H, Yagmurlu K, Moron F, et al. Techniques and outcomes of microsurgical management of ruptured and unruptured fusiform cerebral aneurysms. J Neurosurg. 2017;127(6):1353–60.
Sacho RH, Saliou G, Kostynskyy A, Menezes R, Tymianski M, Krings T, et al. Natural history and outcome after treatment of unruptured intradural fusiform aneurysms. Stroke. 2014;45(11):3251–6.
Quiñones-Hinojosa A, Schmidek HH. Schmidek & Sweet operative neurosurgical techniques: indications, methods, and results. Philadelphia: Elsevier/Saunders; 2012.
Alawieh A, Chaudry MI, Turner RD, Turk AS, Spiotta AM. Infectious intracranial aneurysms: a systematic review of epidemiology, management, and outcomes. J Neurointerv Surg. 2018;10(7):708–16.
Barrow DL, Prats AR. Infectious intracranial aneurysms: comparison of groups with and without endocarditis. Neurosurgery. 1990;27(4):562–72; discussion 72–3.
Bohmfalk GL, Story JL, Wissinger JP, Brown WE Jr. Bacterial intracranial aneurysm. J Neurosurg. 1978;48(3):369–82.
Chen R, Zhang S, Guo R, You C, Ma L. Pediatric intracranial pseudoaneurysms: a report of 15 cases and review of the literature. World Neurosurg. 2018;116:e951–e9.
Zheng Y, Lu Z, Shen J, Xu F. Intracranial pseudoaneurysms: evaluation and management. Front Neurol. 2020;11:582.
Buckingham MJ, Crone KR, Ball WS, Tomsick TA, Berger TS, Tew JM Jr. Traumatic intracranial aneurysms in childhood: two cases and a review of the literature. Neurosurgery. 1988;22(2):398–408.
Lempert TE, Halbach VV, Higashida RT, Dowd CF, Urwin RW, Balousek PA, et al. Endovascular treatment of pseudoaneurysms with electrolytically detachable coils. AJNR Am J Neuroradiol. 1998;19(5):907–11.
Copyright Clause
Please note that the Department of Neurosurgery at Emory University School of Medicine owns and retains copyright to the figures and videos. Permission to publish these figures and videos is enclosed with this submission and has been so addended in the publishing agreement.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Electronic Supplementary Material
Microsurgical clip ligation of multiple aneurysms after subarachnoid hemorrhage (Fig. 8.1). The aneurysms included a ruptured right posterior communicating artery (Pcomm) aneurysm and two unruptured very small aneurysms at the right anterior choroidal artery (AchorA) origin and proximal A1 segment. The approach was performed via a standard right-sided pterional craniotomy. The video depicts microsurgical technique for dissection of the proximal portion of the Sylvian fissure and definition of the neck and dome of all three aneurysms. The Pcomm aneurysm is clipped with a slightly curved miniclip, and AchorA and A1 segment aneurysms are treated with a single straight miniclip each. Indocyanine green video angiography and intraoperative angiography confirmed complete occlusion of the aneurysms and maintained patency of the normal vasculature (MP4 212990 kb)
Microsurgical clip ligation of a giant thrombotic aneurysm arising on the ophthalmic segment of the internal carotid artery (Fig. 8.4). The exposure was performed through a standard left frontotemporal craniotomy. Indocyanine green video angiography shows the narrow neck of the aneurysm. A single side angled clip was placed at the neck of the aneurysm after microsurgical dissection. The flattened optic nerve is gently dissected from the aneurysm sac. The aneurysm is opened and an aneurysmorrhaphy performed with microsurgical instruments, suction, and an ultrasonic aspirator to decompress the optic apparatus. Intraoperative angiography confirmed complete occlusion of the aneurysm and maintained patency of the distal circulation. Postoperative computed tomography shows the decompressed aneurysm sac (MP4 179034 kb)
Microsurgical resection of a ruptured left M4 segment infectious intracranial aneurysm and evacuation of the associated intraparenchymal hemorrhage (IPH) (Fig. 8.5). A standard frontotemporal parietal craniotomy was completed for exposure. The IPH is removed with gentle mechanical debridement and irrigation. The dome of aneurysm is noted within the middle of the clot cavity. After IPH removal, microsurgical dissection of the aneurysm is completed, including identification of the inflow and outflow of the aneurysm, and indocyanine green video angiography confirms the inflow vessel. The aneurysm is fusiform in configuration and encompasses 360° of the diseased arterial segment, which made clip reconstruction impossible. The aneurysm is resected, and the diseased artery is dissected both proximally and distally to prepare for an anastomosis. Primary reanastomosis is attempted but abandoned due to excessive tension on the proximal and distal ends of the vessel artery. The vessel is sacrificed by permanent clip placement and coagulation (MP4 125960 kb)
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Eshraghi, S.R., Howard, B.M., Barrow, D.L. (2022). Microsurgical Aneurysm Treatment. In: Mascitelli, J.R., Binning, M.J. (eds) Introduction to Vascular Neurosurgery. Springer, Cham. https://doi.org/10.1007/978-3-030-88196-2_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-88196-2_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-88195-5
Online ISBN: 978-3-030-88196-2
eBook Packages: MedicineMedicine (R0)