
Abstract
Complex intracranial aneurysms remain challenging to treat using standard microsurgical or endovascular techniques. These aneurysms often require a combination of deconstructive and reconstructive procedures, such as parent artery occlusion, flow alteration, and blind-alley formation with or without bypass surgery, for effective and enduring therapeutic effects. It is important to determine the type of bypass based on the site of occlusion of the patent artery, anatomical features of the distal vessels, and expected adequate blood flow. In this chapter, we describe the “Standards,” “Advances,” and “Controversies” in the context of a microsurgical treatment strategy for complex intracranial aneurysms. “Standards” include a combination of frequent and commonly used procedures that have been gathering a certain consensus on their effectiveness. “Advances” include infrequent, demanding, and/or uncertain surgical procedures that are currently under debate. Finally, “Controversies” discuss a number of unsolved issues.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Complex intracranial aneurysm
- Balloon test occlusion
- Bypass surgery
- Patent artery occlusion
- Flow alteration
- Blind-alley formation
12.1 Introduction
Several characteristics of complex intracranial aneurysms have been reported: (1) large or giant; (2) broad neck; (3) intra–aneurysmal thrombus; (4) calcified or atherosclerotic neck; (5) branches or perforators originating from the aneurysmal dome or neck; (6) recurrence after previous clipping or coil embolization; (7) absence of collateral circulation; and (8) non-saccular morphology, such as in the case of, for example, fusiform/serpentine, mycotic, or dissecting/blood-blister-like aneurysms [1]. In most cases, these aneurysms are unsuitable for standard microsurgical clipping or endovascular coil embolization.
Although recent advances in endovascular procedures, including stent-assisted coil embolization and flow diverter stenting, may yield favorable outcomes in some cases [2, 3], there remain many challenging cases in which microsurgical management may represent the optimal form of treatment. Most of these complex aneurysms require parent artery occlusion (PAO) [4], flow alteration [5], and blind-alley formation [6] with cerebral revascularization to prevent ischemic complications and maintain the cerebral blood flow in the distal territory. Herein, we describe microsurgical aneurysmal clipping and PAO/flow alteration/blind-alley formation procedures using various bypass techniques to treat complex intracranial aneurysms.
12.2 Standards
12.2.1 Giant/Large Middle Cerebral Artery Bifurcation Aneurysms
Giant/large middle cerebral artery (MCA) bifurcation aneurysms are often difficult to treat with simple clipping due to the cortical branches or lenticulostriate arteries (LSA) arising from the aneurysm neck or dome. Such aneurysms may also have a sclerotic aneurysmal wall that precludes clipping.
When clipping is not indicated, a superficial temporal artery (STA)-MCA bypass to the distal MCA branches followed by PAO is usually the next best choice. Complex MCA bifurcation aneurysms may be treated by clipping the neck together with one of the M2 branches arising from the aneurysm dome following protection with a bypass. This strategy of preserving the outflow of M1 to one of the M2 branches can effectively prevent infarction in the LSA territory. On the other hand, PAO at the most distal part of M1, occluding its anterograde flow, may cause infarction in the LSA territory due to abrupt blood flow reduction of M1 [7]. It is important to plan a bypass and PAO strategy such as to maintain adequate blood flow in the LSAs.
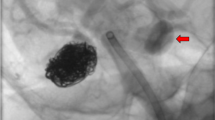
Case presentation (Fig. 12.1): A 59-year-old man suffered a World Federation of Neurosurgical Societies (WFNS) Grade IV subarachnoid hemorrhage (SAH). Initial computed tomography (CT) revealed right-dominant SAH. Preoperative digital subtraction angiography (DSA) demonstrated a giant MCA aneurysm (45 mm in diameter). The distal branches and perforators were unclear on angiography. Because the brain damage was minimal on diffusion-weighted imaging (DWI), surgery to exclude the aneurysm was performed on the same day. Intraoperatively, the M2 inferior trunk originated from the aneurysm dome, and neck clipping was considered difficult. Following the STA-MCA double bypass to both the M2 areas, the aneurysm was investigated under temporary occlusion of the most distal part of M1 (26 min) to finally perform clipping on the neck of the aneurysm with occlusion of the M2 inferior trunk while maintaining anterograde blood flow to the M2 superior trunk. Postoperative DWI revealed an acute infarction in the right LSA territory, probably due to a prolonged temporary occlusion of the distal M1 which caused blood flow reduction of M1 to make the LSA territories ischemia. The patient’s condition improved postoperatively, and he was transferred to a rehabilitation hospital with a modified Rankin scale (mRS) score of 3.

(a) Preoperative computed tomography image representing a right-dominant subarachnoid hemorrhage. A giant right middle cerebral artery (MCA) aneurysm was suspected in the right temporal lobe (arrow). (b) Digital subtraction angiography (DSA) showing a giant MCA aneurysm (45 mm in diameter). The M2 superior trunk originated from the aneurysm neck (arrow), but the M2 inferior trunk was unclear. (c–e) Intraoperative photographs and the schema showing that the M2 inferior trunk originated from the aneurysm dome (c); neck clipping was performed with occlusion of the M2 inferior trunk while maintaining anterograde blood flow to the M2 superior trunk following superior temporal artery-MCA double bypasses (d, e). (f) Postoperative diffusion-weighted image showing the right lenticulostriate artery territory infarction, probably due to prolonged temporary occlusion of the M1. (g) Postoperative magnetic resonance angiography showing a patent bypass and disappearance of the aneurysm
12.2.2 Unruptured Symptomatic Intracavernous Giant/Large Internal Carotid Artery Aneurysms
Giant/large internal carotid artery (ICA) aneurysms of the intracavernous portion may cause visual dysfunction and cranial nerve (III, IV, and VI) palsy [8]. Whether cranial nerve palsy improves after treatment depends on the duration of symptoms [9], and the best early surgical indication is recommended.
Following microsurgical clipping, the symptoms caused by the aneurysms may be alleviated by a decrease in the mass effect and loss of pulsation due to aneurysmal size reduction. Such effects are difficult to achieve with coil embolization [10]. Although flow diversion is a superior treatment that can improve cranial nerve palsy, it has been reported to be associated with 5.3% morbidity and 10.7% mortality [11]. Therefore, PAO, which can immediately and reliably obliterate the blood flow on the proximal side of the aneurysm, remains an effective surgical option.
Case presentation (Fig. 12.2 [12]): A 56-year-old man presented with left abducens nerve palsy. Magnetic resonance angiography (MRA) revealed bilateral ICA aneurysms and a right vertebral artery (VA) fusiform aneurysm. The left symptomatic giant ICA aneurysm (50 mm in diameter) of the intracavernous portion was treated with PAO (ligation of the ICA at the cervical portion) following a saphenous vein graft bypass from the cervical external carotid artery to M2. An STA–MCA bypass to the distal branch of the M2 was performed prior to the vein graft bypass to minimize ischemia during temporary occlusion of the recipient M2 [13]. The patient was discharged without any complications.

(a) A T2-weighted image showing the bilateral internal carotid artery (ICA) aneurysms of the intracavernous portion (arrow and dot arrow). (b) Magnetic resonance angiography (MRA) showing the bilateral ICA aneurysms and the right vertebral artery aneurysm. (c, d) Intraoperative photographs showing cervical external carotid artery (ECA)-vein graft anastomosis (c) and M2-vein graft anastomosis (d). (e) Postoperative MRA demonstrating a patent vein graft between the left ECA and M2, and disappearance of the left ICA aneurysm (Reprinted from reference [12] under permission)
12.2.3 Ruptured Intradural Vertebral Artery Dissecting Aneurysms
This type of aneurysm has been reported to have a high incidence of rebleeding and a high mortality rate in a previous study [14]. Therefore, the treatment of such aneurysms should be carried out as early as possible, as previously emphasized. In recent years, endovascular internal trapping has been increasingly selected as a first-line treatment because it is less invasive and can be performed immediately following a diagnosis [15]. However, this procedure includes a risk of medullary infarction (MI) due to perforator occlusion, which may affect patient outcomes [16]. Although microsurgical trapping may often prevent ischemic complications by avoiding occlusion of the perforators from the VA or posterior inferior cerebellar artery (PICA) to the medulla, it is not always possible depending on the anatomical structures.
Revascularization surgery, such as an occipital artery (OA)-PICA bypass or PICA-PICA bypass, is often required if the PICA is involved in the dissection of the VA [17]. When patient conditions do not allow for a surgical intervention, PAO proximal to the dissection may be the treatment of choice; however, it carries the risk of rebleeding due to retrograde flow from the contralateral VA.
Case presentation (Fig. 12.3): A 55-year-old man suffered a WFNS Grade I SAH. Initial MRA and DSA demonstrated a right VA dissecting aneurysm located on the midline. An OA-PICA bypass was performed because the large PICA originated from the aneurysm wall. Subsequently, the dissecting part was completely occluded by internal trapping using a coil. Postoperative DWI showed right dorso-lateral MI, and the patient presented with dysphagia and right ataxia. The patient was transferred to a rehabilitation hospital with an mRS score of 2.

(a) Preoperative computed tomography showing subarachnoid hemorrhage and intra-fourth ventricle hemorrhage. (b) Digital subtraction angiography (DSA) showing a right vertebral artery (VA) dissecting aneurysm located on the midline. The surgical strategy included an internal trapping following an occipital artery (OA)-posterior inferior cerebellar artery (PICA) bypass given that the large PICA originated from the aneurysm wall. (c, d) Postoperative DSA showing complete occlusion of the right VA dissecting part (c) and a patent bypass (d). The region distal from the VA union was well supplied by the left VA. (e) Postoperative diffusion-weighted image showing the right dorso-lateral medullary infarction
12.3 Advances
12.3.1 Recurrent Intradural ICA Aneurysms Following Previous Coil Embolization
As long-term follow-ups after coil embolization increase, recurrent aneurysms due to incomplete obliteration and coil compaction are being increasingly reported [18]. Surgical procedures may be challenging in most cases because it is difficult to identify the entire structure of the aneurysm due to the previously placed coil mass [19]. A bypass surgery to prevent ischemic complications is often carried out either to prolong temporary occlusion time or to permanently provide alternative blood flow following sacrifice of the related arterial branch.
Case presentation (Fig. 12.4): A 61-year-old woman had suffered from SAH 4 years prior. The ruptured left ICA-posterior communicating (IC-PC) aneurysm was successfully treated using simple coil embolization. However, the IC-PC aneurysm gradually enlarged and rebled to cause SAH as well as right hemiparesis due to infarction in the left anterior choroidal artery (AchA) 4 years later. Removal of a part of the coil followed by neck clipping was planned. Bypass and PAO were the second choice of treatment when clipping was not possible. STA-MCA double bypass to the M3 portions was first performed. Because the AchA was already obstructed, the aneurysm neck was clipped after coil removal, including the origin of the AchA, and the anterograde flow of the ICA was preserved. No adverse events were observed during the postoperative period, and the patient was discharged to a rehabilitation hospital with an mRS score of 3.

(a) Digital subtraction angiography (DSA) showing a ruptured left internal carotid artery-posterior communicating artery (IC-PC) aneurysm which was successfully treated by simple coil embolization. (b) DSA 4 years after the surgery showing the left IC-PC aneurysm that had regrown and rebleeding. (c) A fluid-attenuated inversion-recovery image showing the left anterior choroidal artery territory infarction (arrow) and the left intraventricular hemorrhage (dot arrow). (d–f) Intraoperative photographs showing the superficial temporal artery-middle cerebral artery double bypasses as an insurance bypass (d) and aneurysm neck clipping following partial removal of the previous coil (e, f)
12.3.2 Giant/Large Distal ACA Aneurysms
Giant/large distal ACA aneurysms that require distal revascularization surgery are difficult to treat using standard bypass techniques. In such cases, A3-A3 bypass is useful when the recipient artery and contralateral A3 are sufficiently close. A short interposition STA graft may be useful for anastomosing bilateral A3s, which are apart [20].
Case presentation (Fig. 12.5 [12]): A 68-year-old man presented with multiple infarctions in the right ACA territory. DSA revealed a right giant ACA aneurysm. Notably, both ACAs were supplied by the unpaired ACA, and there was stenosis of the right ACA just proximal to the aneurysm. Intra-aneurysmal thrombus was suspected as the embolic source, and microsurgical obliteration of the aneurysm was performed. The aneurysm was trapped following an A3-A3 bypass using a short-interpositioned STA graft. The postoperative course was favorable, and the patient was discharged with no clinical symptoms.

(a) A diffusion-weighted image showing the right frontal lobe infarction. (b) Digital subtraction angiography (DSA) showing the right anterior cerebral artery (ACA) aneurysm. Bilateral ACAs are supplied by the unpaired ACA and a stenotic lesion is observed in the right ACA just proximal to the aneurysm. The surgical strategy included trapping of the aneurysm (dot arrows) followed by an A3-A3 bypass (double arrow). (c, d) Intraoperative photograph (c) and schema (d) showing the A3-A3 bypass using an interposed superficial temporal artery graft due to the differences in depth of both A3s. (e) Postoperative DSA showing a patent bypass and disappearance of the aneurysm (Reprinted from reference [12] under permission)
12.3.3 Unruptured Symptomatic Giant/Large Basilar Trunk Saccular Aneurysms
Giant/large basilar trunk saccular aneurysms may cause neurological symptoms due to compression of the brainstem or surrounding cranial nerves and are sometimes life-threatening. Such aneurysms are mostly challenging for microsurgical clipping while preserving perforators or other branches. Although flow diverter stents have recently become a new treatment option, they lack long-term follow-up data. According to previously published literature [21], a flow alteration method using various bypasses to the superior cerebellar artery and/or posterior cerebral artery (PCA) combined with PAO can be effective in reducing the aneurysm and improving the symptoms.
Case presentation (Fig. 12.6 [12]): A 46-year-old man presented with progressive dysphagia, dysarthria, and right upper motor paresis over the course of 3 months. Magnetic resonance T2-weighted imaging showed an aneurysm that severely compressed the brainstem. DSA revealed a giant basilar trunk aneurysm protruding from basilar fenestration. The right anterior inferior cerebellar artery (AICA) originated just proximal to the aneurysm. Because both curative clipping and coiling were considered difficult, a flow alteration strategy was selected for aneurysmal flow reduction. Maintenance of adequate flow to the basilar perforators was thought to be a key of this surgery.

(a) A T2-weighted image showing an aneurysm which severely compressed the brainstem. (b) Digital subtraction angiography (DSA) showing the giant basilar trunk aneurysm protruding from a basilar fenestration. The right anterior inferior cerebellar artery (AICA) originates just distal to the aneurysm (arrow). (c–e) Intraoperative photographs showing left posterior cerebral artery-vein graft anastomosis (c) and superficial temporal artery-vein graft anastomosis (d). The basilar trunk was occluded just proximal to the origin of the right AICA (e) to create an outflow of the bypass flow toward to the AICA and preserve basilar perforators. (f) A T2-weighted image 1 month after the surgery showing the decreased aneurysm size. (g) Left carotid angiogram showing a patent bypass graft and an occluded basilar trunk just proximal to the origin of the right AICA. The right AICA made an outflow of the bypass flow and the aneurysm decreased in size (Reprinted from reference [12] under permission)
Using a transpetrosal presigmoid approach, a left STA short saphenous vein graft--PCA bypass was performed to introduce sufficient blood flow to replace basilar artery blood flow. The basilar trunk was occluded just proximal to the origin of the right AICA to make an outflow of the bypass flow toward the AICA and preserve basilar perforators. Postoperative images revealed a decrease in the size of the aneurysm, and the patient’s clinical symptoms gradually improved.
12.4 Controversies
12.4.1 Bypass Selection upon Therapeutic ICA Occlusion
Simple ICA ligation without distal revascularization resulted in cerebral infarction in 26% of patients, 46% of which were fatal according to an analysis of several reports [22]; therefore, the PAO procedure is usually combined with reconstructive bypass surgery, such as a STA-MCA bypass or high-flow bypass using a saphenous vein graft or a radial artery graft [23, 24].
There are two approaches to planning which type of bypass surgery should be performed prior to PAO of the ICA. The selective approach uses preoperative balloon test occlusion (BTO) of the parent ICA to simulate an ischemic condition and selects either a low-or high-flow bypass according to the residual blood flow during BTO [25].
The universal approach uses a high-flow bypass for all patients who undergo PAO [26]. This is based on the consideration of possible errors in the selection and complications due to BTO.
We have applied a selective approach using preoperative BTO. Figure 12.7 demonstrates our criteria for bypass selection based on a previous study [4]. High-flow bypass is indicated for all patients with ischemic symptoms during BTO. In the absence of any ischemic symptoms, the bypass procedure was selected based on the percentage of residual flow, which was quantitatively assessed by single photon emission computed tomography (SPECT) during BTO. Residual flow of less than 70–75% indicated a high-flow bypass, while residual flow between 75 and 90% indicated a STA-MCA bypass. Simple PAO without bypass may be possible for patients with residual flow exceeding 90% in terms of immediate good outcomes; however, considering the long-term risk of aneurysm induction on collateral arteries, a STA-MCA bypass was applied in most patients, except in elderly patients or patients with systemic surgical risks.

Balloon test occlusion criteria in our institution for bypass selection in parent artery occlusion
Postoperative quantitative SPECT demonstrated that cerebral blood flow and cerebrovascular reactivity to acetazolamide on the surgical and non–surgical sides did not differ significantly [4].
However, BTO is associated with a 3.2% complication rate [6], and the process is cumbersome because of the use of SPECT during BTO. Further improvements in bypass selection are warranted.
12.4.2 PAO Strategy: Coiling or Clipping?
12.4.2.1 Intracavernous Giant/Large ICA Aneurysms
In most cases of intracavernous giant/large ICA aneurysms, a cervical ICA ligation is appropriate as a PAO after EC-IC bypass. Usually, there are no major branches arising from the cervical ICA to the origin of the ophthalmic artery, and spontaneous thrombotic formation is expected. However, in approximately 10–20% of cases, several collateral circulations, such as the meningohypophyseal trunk or vidian artery, may be observed between the external carotid artery and the ICA during BTO, providing intense aneurysmal opacification [27]. In these cases, coil embolization of the ICA just proximal to the aneurysm was used to avoid residual blood flow to the aneurysm in our institution. However, it has not been clarified if this strategy is correct and further evaluation is necessary.
12.4.2.2 Paraclinoid Giant/Large ICA Aneurysms
In cases of paraclinoid giant/large ICA (C2) aneurysms, cervical ICA ligation is unsuitable for PAO due to the remaining collateral circulation via the ophthalmic artery to the aneurysm. In these cases, PAO of the ICA between the ophthalmic artery and aneurysm is theoretically necessary. This can be achieved either by clip occlusion after anterior clinoidectomy or coil embolization, usually together with the aneurysm.
On the other hand, PAO for C1 portion aneurysms should be performed with clip occlusion because the critical branches, including the posterior communicating artery, anterior choroidal artery, and direct ICA perforators originate from the C1 portion of the ICA. If a coil is used for PAO of the C1 portion of the ICA, thromboembolic infarction of these branches may occur [28]. Clip trapping or proximal clipping is preferred for PAOs in C1 portion aneurysms.
12.4.2.3 Intradural VA Dissecting Aneurysms
Although endovascular internal trapping is frequently chosen as the first-line treatment for this type of aneurysm, postoperative MI may occur in 30–47% of cases [16, 29, 30]. Several risk factors for MI have been previously reported. Endo et al. reported that the long segment of the VA coiling (15.7 ± 6.0 mm) was significantly associated with MI [29]. Ikeda et al. reported that the length of the coil mass proximal to the dilated portion of more than 5.8 mm was associated with a higher incidence of MI [30]. In contrast, Aihara et al. reported that the length of trapping was not the primary risk factor for MI, and proximal VA stumps were associated with MI. Preservation of the origin of the anterior spinal artery may also reduce the risk of MI [16].
In some cases, clip ligation of the dissected VA may outperform internal trapping with a coil to preserve perforators to the medulla; however, this is not necessarily possible in all patients, and it remains controversial which method is the best to occlude dissected VA.
12.4.3 Surgical Strategy for Fusiform Giant Partially Thrombosed Basilar Trunk Aneurysms
Unclippable fusiform giant partially thrombosed basilar trunk aneurysms are among the most challenging types in the treatment of neurovascular disorders. Although the optimal therapeutic strategy for these aneurysms remains unclear, flow alteration or blind-alley methods have been reported to be effective treatments by several authors [5, 6]. The purpose of both methods is to reduce the intra-aneurysmal flow or aneurysmal wall shear stress by altering the pathological hemodynamics. If collateral circulation is insufficient to maintain an adequate distal blood supply, a bypass surgery for one or more distal main vessels is required. However, it remains difficult to predict how much bypass flow is appropriate to preserve distal blood flow and how rapidly intraluminal thrombus formation progresses.
Recently, computational fluid dynamics (CFD) models have become available to predict the territories that are likely to be ischemic upon PAO and simulate postoperative flows following a planned flow alteration procedure [31]. Further advances in this field are expected to create a universal prediction model for the treatment of challenging complex aneurysms in the future.
12.5 Conclusion
We have described various treatments such as PAO, flow alteration, and blind-alley formation combined with bypass surgery. To prevent aneurysmal rupture and ischemic complications, case-by-case multi-modal evaluations and careful surgical strategy planning are indispensable.
References
Nussbaum ES, Kallmes KM, Lassig JP, et al. Cerebral revascularization for the management of complex intracranial aneurysms: a single-center experience. J Neurosurg. 2018;131:1–11.
Roh H, Kim J, Bae H, et al. Comparison of stent-assisted and no-stent coil embolization for safety and effectiveness in the treatment of ruptured intracranial aneurysms. J Neurosurg. 2019;30:1–7.
Becske T, Brinjikji W, Potts MB, et al. Long-term clinical and angiographic outcomes following pipeline embolization device treatment of complex internal carotid artery aneurysms: five-year results of the Pipeline for Uncoilable or Failed Aneurysms Trial. Neurosurgery. 2017;80:40–8.
Shimizu H, Matsumoto Y, Tominaga T. Parent artery occlusion with bypass surgery for the treatment of internal carotid artery aneurysms: clinical and hemodynamic results. Clin Neurol Neurosurg. 2010;112:32–9.
Lee SH, Ahn JS, Kwun BD, et al. Surgical flow alteration for the treatment of intracranial aneurysms that are unclippable, untrappable, and uncoilable. J Korean Neurosurg Soc. 2015;58:518–27.
Wongsuriyanan S, Sriamornrattanakul K. Blind-alley formation and occipital artery-posterior inferior cerebellar artery bypass for the treatment of unclippable vertebral artery aneurysms with posterior inferior cerebellar artery involvement. W Neurosurg. 2020;138:e539–50.
Kivipelto L, Niemelä M, Meling T, et al. Bypass surgery for complex middle cerebral artery aneurysms: impact of the exact location in the MCA tree. J Neurosurg. 2014;120:398–408.
Date I. Symptomatic unruptured cerebral aneurysms: features and surgical outcome. Neurol Med Chir (Tokyo). 2010;50:788–99.
Yanaka K, Matsumaru Y, Mashiko R, et al. Small Unruptured cerebral aneurysms presenting with oculomotor nerve palsy. Neurosurgery. 2003;52:553–7; discussion 556.
Tan H, Huang G, Zhang T, et al. A retrospective comparison of the influence of surgical clipping and endovascular embolization on recovery of oculomotor nerve palsy in patients with posterior communicating artery aneurysms. Neurosurgery. 2015;76:687–94; discussion 694.
Raymond J, Gentric JC, Darsaut TE, et al. Flow diversion in the treatment of aneurysms: a randomized care trial and registry. J Neurosurg. 2017;127:454–62.
Shimizu H. Deep bypass surgery: basic techniques and tips. Jpn J Neurosurg (Tokyo). 2015;24:846–54.
Hongo K, Horiuchi T, Nitta J, et al. Double-insurance bypass for internal carotid aneurysm surgery. Neurosurgery. 2013;52:597–602; discussion 600.
Mizutani T, Aruga T, Kirino T, et al. Recurrent subarachnoid hemorrhage from untreated ruptured vertebrobasilar dissecting aneurysms. Neurosurgery. 1995;36:905–11; discussion 912.
Iihara K, Sakai N, Murao K, et al. Dissecting aneurysms of the vertebral artery: a management strategy. J Neurosurg. 2002;97:259–67.
Aihara M, Naito I, Shimizu T, et al. Predictive factors of medullary infarction after endovascular internal trapping using coils for vertebral artery dissecting aneurysms. J Neurosurg. 2018;129:107–13.
Shi L, Xu K, Sun X, et al. Therapeutic progress in treating vertebral dissecting aneurysms involving the posterior inferior cerebellar artery. Int J Med Sci. 2016;13:540–55.
Kole MK, Pelz DM, Kalapos P, et al. Endovascular coil embolization of intracranial aneurysms: important factors related to rates and outcomes of incomplete occlusion. J Neurosurg. 2005;102:607–15.
Daou B, Chalouhi N, Starke RM, et al. Clipping of previously coiled cerebral aneurysms: efficacy, safety, and predictors in a cohort of 111 patients. J Neurosurg. 2016;125:1337–43.
Labib MA, Gandhi S, Cavallo C, et al. Anterior cerebral artery bypass for complex aneurysms: advances in intracranial-intracranial bypass techniques. World Neurosurg. 2020;141:e42–54.
Yanagisawa T, Kinouchi H, Sasajima T, et al. Long-term follow-up for a giant basilar trunk aneurysm surgically treated by proximal occlusion and external carotid artery to posterior carotid artery bypass using a saphenous vein graft. J Stroke Cerebrovasc Dis. 2016;25:e212–3.
Linskey ME, Jungreis CA, Yonas H, et al. Stroke risk after abrupt internal carotid artery sacrifice: accuracy of preoperative assessment with balloon test occlusion and stable xenon-enhanced CT. AJNR Am J Neuroradiol. 1994;15:829–43.
Jafar JJ, Russell SM, Woo HH. Treatment of giant intracranial aneurysms with saphenous vein extracranial-to-intracranial bypass grafting: indications, operative technique, and results in 29 patients. Neurosurgery. 2002;51:138–44; discussion 144.
Sekhar LN, Duff JM, Kalavakonda C, et al. Cerebral revascularization using radial artery grafts for the treatment of complex intracranial aneurysms: techniques and outcomes for 17 patients. Neurosurgery. 2001;49:646–58; discussion 658.
Surdell DL, Hage ZA, Eddleman CS, et al. Revascularization for complex intracranial aneurysms. Neurosurg Focus. 2008;24:E21.
Mohit AA, Sekhar LN, Natarajan SK, et al. High-flow bypass grafts in the management of complex intracranial aneurysms. Neurosurgery. 2007;60(Suppl 1):ONS105–22; discussion ONS122: ONS105–122.
Allen JW, Alastra AJ, Nelson PK. Proximal intracranial internal carotid artery branches: prevalence and importance for balloon occlusion test. J Neurosurg. 2005;102:45–52.
Murakami K, Shimizu H, Matsumoto Y, et al. Acute ischemic complications after therapeutic parent artery occlusion with revascularization for complex internal carotid artery aneurysms. Surg Neurol. 2009;71:434–41; discussion 441.
Endo H, Matsumoto Y, Kondo R, et al. Medullary infarction as a poor prognostic factor after internal coil trapping of a ruptured vertebral artery dissection. J Neurosurg. 2013;118:131–9.
Ikeda H, Imamura H, Mineharu Y, et al. Effect of coil packing proximal to the dilated segment on postoperative medullary infarction and prognosis following internal trapping for ruptured vertebral artery dissection. Interv Neuroradiol. 2016;22:67–75.
Tsuji M, Ishikawa T, Ishida F, et al. Stagnation and complex flow in ruptured cerebral aneurysms: a possible association with hemostatic pattern. J Neurosurg. 2017;126:1566–72.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Togashi, S., Shimizu, H. (2022). Complex Intracranial Aneurysms. In: Kato, Y., Ansari, A. (eds) Cerebrovascular Surgery. Advances and Technical Standards in Neurosurgery, vol 44. Springer, Cham. https://doi.org/10.1007/978-3-030-87649-4_12
Download citation
DOI: https://doi.org/10.1007/978-3-030-87649-4_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-87648-7
Online ISBN: 978-3-030-87649-4
eBook Packages: MedicineMedicine (R0)