
Abstract
Techniques for vagal and recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery have advanced significantly over the past 50 years. By empowering surgeons with data beyond the standard visual information, these techniques have steadily gained widespread acceptance as an adjunct for mapping and identifying the nerves, for confirming and elucidating mechanisms of laryngeal injury, for detecting anatomic variations, and for predicting the postoperative outcomes of vocal cord function. In this chapter, we discuss the pertinent anatomy of the carotid sheath, anatomy-based classifications, variations of the recurrent laryngeal nerve, the rationale for vagal and recurrent laryngeal nerve monitoring, indications for vagus/recurrent laryngeal nerve monitoring, basic laryngeal nerve monitoring equipment setup, the definition of loss of signal (LOS), classification to facilitate accurate intraoperative neural monitoring (IONM), and clinical applications as well as current standards and guidelines of IONM.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Vagus nerve
- Recurrent laryngeal nerve
- Surgical anatomic variations
- Intraoperative neural monitoring
- Loss of signal
- Vocal cord paralysis
Introduction
Recurrent laryngeal nerve (RLN) injury and vocal cord paralysis after thyroid surgery remain a significant source of morbidity and is a leading cause for medicolegal action [1]. Intraoperative neural monitoring (IONM) has gained widespread acceptance as a tool to assist in identifying and mapping the external branch of the superior laryngeal nerve (EBSLN), RLN, and vagus nerve (VN), detecting RLN anatomic variations, confirming and elucidating mechanisms of RLN injury, and predicting the outcome of vocal cord function [2,3,4,5,6,7,8,9,10,11,12,13]. By providing real-time functional information, IONM empowers surgeons beyond what is available to them through visual information alone. This chapter reviews the surgical anatomy of the VN, the carotid sheath, and the RLN as well as the surgical anatomy-based classifications and variations relevant to thyroid/parathyroid surgery, discusses the rationale and indications for VN and RLN monitoring, and also reviews basic laryngeal nerve monitoring equipment setup, standard procedures, and LOS definition and classification to facilitate accurate and efficient IONM. This chapter also summarizes the current standards and guidelines of VN and RLN monitoring.
Anatomy
Vagal Nerve and Carotid Sheath Anatomy
A better understanding of the anatomy and variability in the position of the VN within the carotid sheath is necessary not only to minimize complications but also to ensure accurate, efficient, and safe use of IONM [14]. The carotid sheath refers to the fibrous connective tissue that surrounds the vascular compartment of the neck and is part of the deep cervical fascia. The medial location of the common carotid artery (CCA) and anterolateral or lateral location of the internal jugular vein (IJV) are the most common configurations in the carotid sheath. Rare cases of medial IJV positions have been observed [15, 16]. In the largest series to date, Dionigi et al. [16] proposed an anatomical classification of the VN based on its position relative to the great vessels and offered a reproducible methodology for identifying the VN and its course in the carotid sheath. The relative location of the VN has been classified into various configurations where A denotes a VN anterior to the CCA and IJV (4%), P denotes a VN posterior to the CCA and the IJV (73%), Pj denotes a VN posterior to the internal jugular vein (8%), and Pc denotes a VN posterior to the CCA (15%) (Fig. 6.1). Such classification is useful in the intraoperative setting to localize the VN for IONM. During intermittent IONM, VN identification may also be expedited without formally dissecting the carotid sheath by placing the stimulation probe on the carotid sheath and blindly stimulating at 2–3 mA [11], as shown in Fig. 6.1.

Common locations of vagal nerve (VN) within the carotid sheath and procedure of VN stimulation by using the ball-tip stimulation probe mapping on the carotid sheath
RLN Surgical Anatomic Trajectory in the Neck Base
The RLN is a branch of VN that normally loops around the aorta at the ligamentum arteriosum on the left side and around the subclavian artery on the right side before coursing to the larynx. In 2016, Randolph et al. [14] published the basic classification of the RLN surgical anatomic pathway in the neck as it relates to thyroid surgery. This classification incorporates normal anatomy as well as embryological and acquired variations in the trajectory of the right and left RLN. It is simple and surgically relevant, presenting a valuable framework for the surgeon. This classification broadly categorizes the RLNs as having a(n):
-
1.
Normal trajectory
-
2.
Abnormal trajectory – acquired
-
3.
Abnormal trajectory – embryological
The details of the classification system and the estimated prevalence of each category are depicted in Fig. 6.2 and Table 6.1, respectively.

Basic classification of RLN surgical anatomic path in the neck base as it relates to the thyroid surgical procedure [14]
Normal Trajectory L1, R1
As the heart and great vessels descend during early embryologic life, the RLN is dragged down by the persistent aortic arch. The right VN runs from the posterior aspect of the carotid sheath in the neck base and crosses anterior to the first segment of the subclavian artery. The RLN branches off, traversing posterior to the subclavian artery (the fourth branchial arch remnant) to course supero-medially behind the CCA as it ascends through the right thoracic inlet to cross obliquely from lateral to medial as it ascends the neck. The left VN courses from the posterior aspect of the left carotid sheath in the left neck base anterior to the aortic arch (sixth arch ligament and arteriosus). The left RLN then branches underneath the aortic arch just lateral to the obliterated ductus arteriosus and ascends into the paratracheal region in a direct cranial-caudal trajectory within the tracheoesophageal (TE) groove. This should be distinguished from the more oblique path of its right counterpart. In general, the normal trajectory of the left RLN (L1) travels in a path that is parallel to the TE groove at an angle less than 30° in at least 80% of cases, whereas the normal trajectory of the right RLN (R1) travels in a path between 15 and 45° relative to the TE groove in approximately 80% of cases.
Acquired Variations of L2a/R2a (Lateral/Medial)
L2a If a goiter on the left side extends significantly into the TE groove, a more lateral displacement (more than 30°) of the left RLN may occur.
R2a Goitrous changes of certain aspects of the right normal thyroid lobe, especially the more dorsal aspects of the mid-inferior pole region, may displace the normally oblique nerve more medially into a newly acquired medial position more parallel to the TE groove (less than 15°).
Acquired Variations of L2b/R2b (Ventral)
L2b/R2b When thyroid tissue extends deep to the trachea due to a dorsally oriented tubercle of Zuckerkandl and forms a retrotracheal cervical goiter or posterior mediastinal goiter, the RLN may be excavated posteriorly by this segment of dorsal tissue. This can potentially result in a significant displacement of the RLN ventrally.
Embryologic Variations of L3/R3 (Nonrecurrent)
L3 A nonrecurrent left RLN embryologically requires a simultaneous occurrence of other anomalies, namely, situs invertus, aberrant subclavian artery, and ductus arteriosus. This is extraordinarily rare.
R3 A nonrecurrent right RLN occurs when the right subclavian artery arises from the distal aortic arch and extends to the right side in a retro-esophageal course. In this case, the right RLN runs in a more direct and medial course from the VN to its laryngeal entry point.
Clinically Important RLN Features
In addition to the L1–L3 and R1–R3 classes described above, other factors are also a crucial part of the surgical anatomic classification system. These can be denoted by additional lettering added to the L or R notations and can be classified as anatomical (F, fixed/splayed/entrapped; I, invaded; L, posterior ligament of Berry, entrapped; B, branched; T, thin caliber) or dynamic (LOS, loss of electrophysiologic signal; D, extensive nerve dissection) (Table 6.1).
Rationale of Vagus and Recurrent Laryngeal Nerve Monitoring
The RLN contains motor fibers that enable abduction and adduction of intrinsic vocal fold muscles and provides sensory fibers to the larynx. Intraoperative injury of the RLN or invasion of the nerve may result in RLN dysfunction, including vocal cord paralysis (VCP) with or without clinical symptoms [12, 14]. Unilateral RLN injury and VCP can cause significant dysphonia and dysphagia, while bilateral RLN injuries and VCP are potentially life-threatening due to airway compromise.
The use of VN and RLN IONM during thyroid and parathyroid surgery provides surgeons with a tool to better understand the possible mechanisms of RLN injury [6, 7, 17,18,19]. Previously, the surgeon was only aware of RLN injury if there were visible trauma to the identified nerve. Nerves that appear intact however are not always functionally intact. With IONM , the surgeon can confirm that nerve stimulation results in contraction of the laryngeal muscles, which can be palpated or recorded electrophysiologically. The amplitude of the vocal fold contraction can be measured in microvolts, and the latency of nerve conduction can be measured in microseconds [2, 20]. During intermittent IONM (IIONM), repeated stimulation of the VN or RLN during thyroidectomy can help the surgeon identify an impending RLN injury by identifying a decrease in the amplitude of the vocal fold contraction and increased latency of nerve conduction. A similar result may be obtained during continuous IONM (CIONM), which provides automated stimulation to the nerves. In the event of total loss or impending loss of nerve signal (LOS), the surgeon can evaluate the surgical maneuver that produced the impending or actual RLN injury and modify the maneuver [21,22,23]. Such real-time intraoperative feedback of RLN function also provides an opportunity to understand the mechanisms of RLN injury. Experience with IONM has demonstrated RLN injury occurs more frequently to a visually intact nerve than a visually damaged nerve [6, 7, 14, 17,18,19]. By enabling early detection of RLN injury and prediction of nerve outcome, IONM can help clinicians plan and modify intra- and postoperative treatments [2,3,4,5, 8, 14, 19].
Indications and Benefits of VN/RLN Monitoring
Appropriate use of VN/RLN monitoring during thyroid/parathyroid surgery should be considered for all cases. Certainly, cases that can be recognized preoperatively as likely having greater risk to the RLN should be monitored. However, many cases lacking these preoperative features may well present significant intraoperative difficulties and may benefit from monitoring. Routine application has been shown to shorten learning curves through greater experience in the interpretation of signal and troubleshooting system malfunction [24]. Although the impact of IONM on rates of RLN injury is generally accepted as lower, many studies have not shown statistical significance [25,26,27], possibly due to the power needed to detect a statistically significant difference (9 million patients per arm for benign goiter and 40 million per arm for malignant thyroid disease) [28].
In addition to thyroid/parathyroid surgery, RLN monitoring can be considered for open approaches to address Zenker’s diverticulum, carotid endarterectomy, surgery for laryngotracheal stenosis, anterior cervical approaches to the cervical spine, and certain skull base, cardiac, and upper chest procedures [29].
Given the potential implications on intraoperative decision-making, especially in total thyroidectomy, the use of IONM should be included in informed consent. Most patients appreciate and wish to actively take part in shared decision making regarding the management of their disease [30]. Adequate informed consent and use of IONM documentation have been reported to favorably impact malpractice suits against surgeons [31, 32].
Basic VN/RLN Monitoring Equipment Setup
Various methods have been applied to intraoperative VN and RLN monitoring during thyroid and parathyroid surgery. These different nerve monitoring formats include laryngeal palpation, glottic observation, glottic pressure monitoring, endoscopically placed intramuscular vocal cord electrodes (hookwires), intramuscular electrodes placed through the cricothyroid membrane, postcricoid surface electrodes, and endotracheal tube (ET)-based surface electrodes [2]. Basic VN/RLN monitoring involves multifaceted electronic stimulation and recording equipment (Fig. 6.3) which can be divided into the following categories: (i) the recording side and (ii) the stimulation side.

Multifaceted electronic stimulation and recording equipment for laryngeal nerve monitoring. Abbreviations: ETT, endotracheal tube; EMG, electromyogram; GND, ground
The recording side involves the recording electrodes (Figs. 6.3 and 6.4a, b), the grounding electrode, and associated connections at the interface-connector box and monitor [2]. ET-based surface electrodes are the most popular and have several advantages including the ease of setup, their noninvasive nature, and the large EMG potentials recordable with such electrodes. Electrodes are incorporated into the wall of the ET or fixed to the side of the endotracheal wall with adhesives and are exposed at the level of the glottis for optimal bilateral vocal cord mucosal contact. This allows evoked surface electromyography (EMG) monitoring of the vocal muscles’ contraction during stimulation of RLN and VN [2]. Several kinds of ET-based electrodes have been commercialized for recording during IONM, including adhesive, wire, and ink surface electrodes. A limitation of the clinical use of ET-based surface electrodes is the need to maintain constant contact between the electrodes and vocal cords during surgery to obtain a high-quality recording [33, 34]. Alternative electrode systems that can circumvent the factors affecting ET-based neural monitoring accuracy have been sought, such as anterior laryngeal transcutaneous or trans-cartilaginous surface electrodes [20, 35, 36].

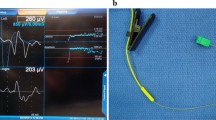
The multifaceted electronic equipment and principle of the IONM system. (a) The basic equipment included the neural stimulating electrodes (stimulator) and the recording electrodes (connected to the ETT). (b) The stimulating electrodes can be used to determine the location and functional status of the EBSLN, RLN, and VN during IONM. (c) The evoked EMG response is displayed on an LCD screen
The stimulation side includes the neural stimulating electrodes (Figs. 6.3 and 6.4a, b), its grounding electrode, and associated connections to the interface box-connector and stimulation current pulse generator within the monitor. Recording ground and nerve stimulator anode surface electrodes are placed on the patient’s shoulders and are interfaced with the monitor through a connector box. Stimulating electrodes may be monopolar or bipolar and may also be configured as dissecting instruments [37]. The selection of a stimulator can be based on the stimulation characteristics, the intended nerve monitoring application, and the surgeon’s preference [38]. During thyroid and parathyroid surgery, the stimulating electrode can be used for mapping, localization, and identification of the EBSLN, RLN, and VN (Fig. 6.4a). The evoked laryngeal EMG waveform may be viewed on the EMG monitor screen (Fig. 6.4c) and the amplitude and latency changes monitored during surgery.
Continuous intraoperative nerve monitoring (CIONM) uses a newly configured electrode positioned on the VN to indirectly stimulate the RLN [39,40,41]. A laryngeal adductor reflex (LAR-C-IONM) EMG tube [42] has the advantage of assessing real-time nerve integrity and thus better indicates impending nerve injury compared to intermittent (IONM) stimulation techniques. A more complete description of alternative techniques and methods of IIONM and CIONM is presented in the following chapters.
Basic Standard VN and RLN Monitoring Procedures
According to current literature and international standards and guidelines [2], the standard procedure for performing IONM should include the following six steps: (i) preoperative laryngoscopy (L1); (ii) VN stimulation before surgical dissection (V1); (iii) RLN stimulation at initial identification (R1); (iv) RLN stimulation after completion of thyroid dissection and hemostasis (R2); (v) VN stimulation after completion of thyroidectomy and confirmation of hemostasis (V2); and (vi) postoperative laryngoscopy (L2) (Table 6.2).
Preoperative laryngoscopy (L1) provides the baseline functional status of the vocal cords prior to surgery. Pre-RLN dissection vagal stimulation (V1) allows for the verification of system function and RLN mapping so that a negative stimulation can be interpreted as a true negative. Post-RLN dissection vagal stimulation (V2) is the most accurate prognostic test available for postoperative glottic function and has been shown to have higher sensitivity, slightly higher specificity, higher positive predictive value, and slightly higher negative predictive value compared to RLN stimulation [2, 8]. VN stimulation typically can be performed successfully without direct vagal dissection by placing the stimulator probe between the jugular vein and carotid artery at a level of stimulation between 1 and 2 mA (Fig. 6.1) [11]. On the right side a pattern of high vagal positive stimulation and lower vagal negative stimulation is the diagnostic for nonrecurrent right RLN [43]. Following the V1-R1-R2-V2 procedure during surgery, three evaluative events can be observed [6, 17]:
-
1.
Stable signal: Improved or unchanged amplitude of R2 and V2 signals as compared with R1 and V1 signals confirms no RLN injury due to surgical dissection. It indicates normal intraoperative RLN function and postoperative vocal cord function.
-
2.
Weak or incomplete loss of signal (LOS): The RLN can be partially injured by certain surgical maneuvers including traction, compression, clamping, mechanical trauma, or cauterization . Despite a visually intact nerve, these maneuvers can lead to focally absent or weak points of nerve conduction, where the amplitude of proximal RLN stimulation is over 100 μV compared to a substantial amplitude reduction of the distal RLN stimulation [6, 7, 18]. The correlation between the percentage of EMG amplitude reduction and postoperative vocal cord function is highly variable, and vocal cord mobility can be normal, weak, or paralyzed. Recent studies recommend that if the final EMG amplitude reduction reaches 50–60% or more, surgeons should consider the possibility of postoperative VCP [44, 45]. However, an incomplete LOS may occur if the recording electrodes are not contacting properly the vocal cords possibly due to surgical manipulation of the thyroid or trachea. This displacement can result in a substantial change of EMG amplitude. Thus, it is important to verify and when needed adjust the EMG tube and electrode position if a significant reduction in amplitude is noted [46].
-
3.
Loss of signal (LOS): LOS is defined in part as an amplitude of 100 μV or less (see Section VII). When R2 and V2 signals become lost after complete dissection of the RLN, it should be assumed that the RLN might have been injured during surgical manipulation. An effort should be made to identify the disrupted point of nerve conduction and elucidate the mechanism of injury. The disrupted point of nerve conduction may be located by testing the RLN from the distal portion near the entry point of the larynx. If a signal is obtained, the lower portion of the nerve should be tested until a response can no longer be elicited. In this manner, the disrupted point of nerve conduction may be located more precisely. If no disrupted point of nerve conduction is detected, contralateral VN stimulation should be used to exclude the possibility of false LOS, such as monitoring equipment dysfunction, EMG tube malposition, or misuse of neuromuscular blocking agents [2, 12, 14, 47].
Loss of Signal: Definition and Classifications
According to the 2011 International Neural Monitoring Study Group (INMSG) guidelines [2], the three basic criteria for LOS are (1) an EMG change from an initially satisfactory EMG, (2) absence of response or low response (i.e., 100 μV or less) to 1–2 mA stimulation on a dry field, and (3) absence of laryngeal and/or glottic twitch. According to a recent 2018 INMSG guideline for interpreting LOS [4], the optimal normative baseline at the beginning of surgery is an initial V1/R1 waveform with an amplitude of 500 μV or greater obtained under a stimulation current of 1–2 mA.
INMSG Impending Adverse EMG (IA-EMG) and Adverse EMG (A-EMG)
In the setting of continuous vagal IONM , the surgeon can use repeated pulsed stimulation to obtain the real-time EMG change during surgical dissection. The surgeon can set the threshold to a percentage (%) of amplitude reduction (fewer nerve fibers participating in the response) and latency increase (slower response) as an indicator of adverse EMG changes. The surgeon can then correct certain maneuvers immediately to prevent irreversible nerve injury. Animal studies using continuous IONM have demonstrated that amplitude and latency degradation under ongoing traction has potential for recovery if traction is released [23, 48,49,50,51]. Two clinical studies that have explored concordant amplitude decrease and latency increase indicate that these “combined events” are reliable early indicators of impending neurapraxia [21, 22]. Therefore, according to the recent INMSG LOS guideline [4], an amplitude decrease of >50% (with absolute amplitude >100 μV) and latency increase of >10% should be interpreted as an Impending Adverse EMG (IA-EMG) because they imply that the nerve is approaching a combined event status in which VCP risk is elevated. Immediate cessation of the surgical maneuver is recommended. The INMSG has also proposed that Adverse EMG (A-EMG) should be defined as 100 μV or less as this drop indicates a progression from the preceding IA-EMG and is known to have a strong association with subsequent VCP with limited recoverability of 17–23% [4].
Other Absolute and Relative Threshold Criteria
Different criteria for using LOS to predict VCP are reported in the literature, including absolute threshold values and relative threshold values. Absolute threshold value criteria include the occurrence of LOS (intraoperative LOS episodes [21, 52, 53] or persistent LOS at the end of surgery [2, 6, 17, 54,55,56]) and specific final V2 value (200 μV [57] or 280 μV [58]). Relative threshold value criteria involve comparing the signals from the most distal (R2d) and the most proximal (R2p) ends of the exposed RLN as a simple and useful method to evaluate type I LOS (or segmental RLN injury) after completion of thyroid lobectomy and for predicting RLN functional outcome [13, 59]. The positive predictive value of a R2p/R2d ratio >63% for postoperative VCP was 79.4% [59]. Therefore, when the relative threshold value R2p/R2d reduction exceeds 60%, the surgeon should consider the possibility of postoperative VCP, even if the EMG value exceeds 100 μV [13].
False LOS
Normal RLN function with no or very low EMG signal is called false LOS . False LOS is characterized by a lack of a point of injury on the exposed RLN and a lack of response to contralateral VN stimulation [2].
The most common three causes of false LOS are:
-
1.
Monitoring equipment malfunction. The grounding, recording/stimulating electrodes and associated connections at the interface-connector box and monitor should be checked to ensure that they are not displaced, dislodged, or broken. The use of electrocauterization can also cause a broken fuse.
-
2.
ET malposition. During ET-based recording, displacement of the EMG tube (up- or downward or due to rotation) during surgical manipulation may cause false LOS due to insufficient contact between EMG tube electrodes and vocal folds [46, 60, 61]. To correct a displaced ET EMG tube, the surgeon can perform vagal stimulation, while the anesthesiologist readjusts the tube [2]. If false LOS is suspected, fiber-optic laryngoscopy can be used to confirm the presence of laryngeal twitch and to adjust the electrode position [17].
-
3.
Repeated use of neuromuscular blocking agents (NMBAs). Repeated intraoperative administration of NMBAs can cause a false LOS. Preoperative discussion with the anesthesiologist enables proper anesthetic planning. Intraoperatively, when LOS occurs, the surgeon should consult the anesthesiologist regarding any NMBA use. If an NMBA has been inadvertently administered intraoperatively, NMBA reversals (e.g., sugammadex) may be needed for rapid restoration of normal muscle twitch activity [62,63,64,65].
True LOS: Type I and Type II
True LOS is defined as an RLN injury resulting in an elicited EMG signal <100 μV. According to the troubleshooting algorithm described in the INSMSG guidelines [2, 4], a negative laryngeal/glottic twitch combined with a positive contralateral VN evoked EMG signal should be interpreted as an ipsilateral neural injury and the possibility of postoperative VCP.
Currently, true LOS and RLN injury are usually classified into two subtypes [2, 6, 17] according to the electrophysiology results observed during IONM. Type 1 LOS or RLN injury (i.e., segmental or localized RLN injury) is characterized by a nerve injury at a specific site, and it usually results from direct stress on the nerve. In type 1 LOS, distal RLN stimulation induces normal evoked activity, whereas proximal stimulation to the injured segment elicits a waveform no greater than 100 μV. In type 2 LOS, the exposed RLN shows no specific disruption site (i.e., diffuse or global RLN injury) and no visible change in appearance [2, 6, 17].
The reported proportion of type I and type II RLN LOS varies in the literature. Dionigi reported greater type I than type II LOS (I = 71% vs. II = 29%) [18] as did Snyder (I = 92% vs. II = 8%) [7]. In contrast, Schneider reported fewer type I LOS lesions (I = 44% vs. II = 56%) [45] as did Chiang (I = 33% vs. II = 67%) [6]. Differences in the reported prevalence may be due to differences in the extent of RLN exposure and whether the disrupted point of the RLN is checked routinely, surgical experience and technique or the use of certain surgical maneuvers, as well as variations in RLN anatomy (i.e., branching patterns, relationship to the ligament of Berry) among different study populations (e.g., different ethnicities) [66].
To establish true LOS with high certainty, the surgeon must use IONM LOS troubleshooting algorithms to exclude all possible causes of false LOS [2].
When a true LOS is confirmed, the following management principles should be applied: (1) Map lesion (type I or II) and elucidate the possible injury mechanism (2) Consider a staged contralateral procedure in cases of LOS with no or incomplete intraoperative recovery. Detailed information on the management of LOS and its troubleshooting algorithms will be introduced and discussed in the following chapters.
Clinically Significant Monitoring Applications
There is increasing adoption of nerve monitoring in endocrine and other head and neck surgery. In a recent survey of practice patterns in the United States, IONM is utilized in roughly 80% of thyroid surgeries performed by otolaryngology-head and neck surgeons and over 65% performed by general surgeons with the number rising significantly over the last 5 years [67, 68]. Over 95% of endocrine surgery fellows (general surgery and otolaryngology-head and neck surgery), exposed to nerve monitoring during their endocrine surgery fellowship, report utilizing IONM in some or all of their cases upon completion of fellowship [69]. Large survey studies suggest higher-volume surgeons more commonly utilize neural monitoring [70]. Strict adherence to IONM standards improves implementation [71].
The 2018 INMSG Guidelines [4] identified the following clinically significant IONM applications and benefits :
-
1.
RLN mapping before its visual identification to facilitate subsequent visual identification and help avoid RLN injury [72]. Snyder et al. reported that electrical RLN neural identification preceded visual identification in nearly 35% of cases [73]. RLN identification speed is improved with IONM [74].
-
2.
Identification of RLN anatomical variants with increased potential for iatrogenic injury.
-
3.
Reducing the rate of tracheotomy in total thyroidectomy based on the prognostication of RLN function [75, 76].
-
4.
Intraoperative alteration of surgical maneuver in case of impending neural injury [22, 77].
-
5.
Identification and preservation of superior laryngeal nerve (SLN) [3, 78].
-
6.
IONM may help younger or less experienced surgeons achieve outcomes similar to experienced surgeons [79].
-
7.
IONM may assist in early and definitive intraoperative identification of nonrecurrent laryngeal nerve variations [80].
The 2018 INMSG Guidelines [4] further outlined the following conceptual domains for the use of IONM during thyroidectomy
-
1.
Intraoperative nerve identification and nerve mapping
-
2.
Differentiation between neural and non-neural structures
-
3.
Identification of impeding nerve injury as well as the mechanism and site of injury
-
4.
Reduction of tracheotomy risk based on the prognostication of nerve injury before proceeding with the contralateral side
Guidelines and Current Standards
In 2006, The International Neural Monitoring Study Group (INMSG) was founded as an international multidisciplinary collaboration to serve the emerging field of neurophysiologic monitoring of laryngeal nerves in head and neck endocrine surgery. Comprised of experts in the field of head and neck endocrine surgery, laryngology, electromyography, anesthesiology, and neurophysiology, the group has published several guidelines to promote uniform and standard IONM technique, to define standardized references of normative and pathological RLN neurophysiology parameters, to evaluate new technological developments, and to support standardized educational and research activities in the field of IONM for head and neck surgeries. It has published guidelines on basic RLN and EBSLN monitoring techniques and interpretations for monitored thyroid and parathyroid surgery [2, 3]. More recently, INMSG has published a two-part consensus guideline discussing nerve monitoring for thyroid and parathyroid surgery with a specific focus of its application on intraoperative strategy and disease management. Part I discusses the management of LOS including its relevance to the staging of thyroid surgery. Part II discusses optimal IONM in the setting of invasive thyroid cancer [4, 5].
These guidelines together with continued advances in monitoring equipment as well as the increasing body of literature supporting the application of IONM in head and neck surgery have led to increasing organizational support for IONM in thyroid and parathyroid surgeries. Both INMSG Guidelines and the German Association of Endocrine Surgery guidelines recommend neural monitoring in all cases of thyroid and parathyroid surgery [2,3,4,5, 81]. Updating the 2009 American Thyroid Association (ATA) Thyroid Nodules and Differentiated Thyroid Cancer guidelines, the 2015 Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer included seven surgical recommendations pertaining to voice optimization laryngeal exam, neural management, and IONM [82]. In addition, the ATA Surgical Affairs Committee Consensus Statement on Outpatient Thyroid Surgery and the ATA Statement on Optimal Surgical Management of Goiter highlight the role of neural monitoring in confirming intact neural function at the end of surgery including its role in discharge planning particularly in cases of bilateral LOS [83, 84]. The American Academy of Otolaryngology Head and Neck Surgery (AAOHNS) Clinical Practice Guideline: Improving Voice Outcomes After Thyroid Surgery as well as the Evidence-Based American Head and Neck Society (AHNS) Consensus Statement on the Management of Locally Invasive Well-Differentiated Thyroid Cancer discuss the utility of neural monitoring in neural identification, reduction of transient nerve paralysis rates, prognostication of nerve function, and avoidance of bilateral VCP [76, 85]. The AAOHNS supports the use of IONM in cases of (i) total thyroidectomy, (ii) revision surgery for thyroid cancer , and (iii) thyroid surgery on an only functioning nerve.
Conclusion
There has been much progress in the application of VN/RLN monitoring during thyroid and parathyroid surgery. Standardization and organizational support has been instrumental in promoting the use of IONM. This chapter provides an overview of the rationale and indications of IONM. Detailed information on the monitoring of the EBSLN and CIONM, troubleshooting system integrity, managing LOS, incorporating IONM into the intraoperative management of invasive thyroid cancer, and nerve monitoring in remote access thyroid surgery and parathyroid surgery are described in other chapters.
References
Swonke ML, Shakibai N, Chaaban MR. Medical malpractice trends in thyroidectomies among general surgeons and otolaryngologists. OTO Open. 2020;4(2):2473974x20921141.
Randolph GW, Dralle H, Abdullah H, Barczynski M, Bellantone R, Brauckhoff M, Carnaille B, Cherenko S, Chiang FY, Dionigi G, et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011;121(Suppl 1):S1–16.
Barczynski M, Randolph GW, Cernea CR, Dralle H, Dionigi G, Alesina PF, Mihai R, Finck C, Lombardi D, Hartl DM, et al. External branch of the superior laryngeal nerve monitoring during thyroid and parathyroid surgery: International Neural Monitoring Study Group standards guideline statement. Laryngoscope. 2013;123(Suppl 4):S1–14.
Schneider R, Randolph GW, Dionigi G, Wu CW, Barczynski M, Chiang FY, Al-Quaryshi Z, Angelos P, Brauckhoff K, Cernea CR, et al. International neural monitoring study group guideline 2018 part I: staging bilateral thyroid surgery with monitoring loss of signal. Laryngoscope. 2018;128(Suppl 3):S1–s17.
Wu CW, Dionigi G, Barczynski M, Chiang FY, Dralle H, Schneider R, Al-Quaryshi Z, Angelos P, Brauckhoff K, Brooks JA, et al. International neuromonitoring study group guidelines 2018: Part II: optimal recurrent laryngeal nerve management for invasive thyroid cancer-incorporation of surgical, laryngeal, and neural electrophysiologic data. Laryngoscope. 2018;128(Suppl 3):S18–s27.
Chiang FY, Lu IC, Kuo WR, Lee KW, Chang NC, Wu CW. The mechanism of recurrent laryngeal nerve injury during thyroid surgery–the application of intraoperative neuromonitoring. Surgery. 2008;143(6):743–9.
Snyder SK, Lairmore TC, Hendricks JC, Roberts JW. Elucidating mechanisms of recurrent laryngeal nerve injury during thyroidectomy and parathyroidectomy. J Am Coll Surg. 2008;206(1):123–30.
Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg. 2008;32(7):1358–66.
Chiang FY, Lu IC, Tsai CJ, Hsiao PJ, Lee KW, Wu CW. Detecting and identifying nonrecurrent laryngeal nerve with the application of intraoperative neuromonitoring during thyroid and parathyroid operation. Am J Otolaryngol. 2012;33(1):1–5.
Chiang FY, Lu IC, Chen HC, Chen HY, Tsai CJ, Hsiao PJ, Lee KW, Wu CW. Anatomical variations of recurrent laryngeal nerve during thyroid surgery: how to identify and handle the variations with intraoperative neuromonitoring. Kaohsiung J Med Sci. 2010;26(11):575–83.
Wu CW, Dionigi G, Chen HC, Chen HY, Lee KW, Lu IC, Chang PY, Hsiao PJ, Ho KY, Chiang FY. Vagal nerve stimulation without dissecting the carotid sheath during intraoperative neuromonitoring of the recurrent laryngeal nerve in thyroid surgery. Head Neck. 2013;35(10):1443–7.
Wu CW, Wang MH, Chen CC, Chen HC, Chen HY, Yu JY, Chang PY, Lu IC, Lin YC, Chiang FY. Loss of signal in recurrent nerve neuromonitoring: causes and management. Gland Surg. 2015;4(1):19–26.
Wu CW, Hao M, Tian M, Dionigi G, Tufano RP, Kim HY, Jung KY, Liu X, Sun H, Lu IC, et al. Recurrent laryngeal nerve injury with incomplete loss of electromyography signal during monitored thyroidectomy-evaluation and outcome. Langenbecks Arch Surg. 2017;402(4):691–9.
Randolph GW, Wu CW, Dionigi G, Kamani D, Modi RR, Chiang FY, Henry JF. The international RLN anatomic classification system. In: Randolph GW, editor. The recurrent and superior laryngeal nerves. Cham: Springer International Publishing; 2016. p. 125–38.
Shoja MM, Ardalan MR, Tubbs RS, Loukas M, Vahedinia S, Jabbary R, Jalilvand M, Shakeri A. The relationship between the internal jugular vein and common carotid artery in the carotid sheath: the effects of age, gender and side. Ann Anat. 2008;190(4):339–43.
Dionigi G, Chiang FY, Rausei S, Wu CW, Boni L, Lee KW, Rovera F, Cantone G, Bacuzzi A. Surgical anatomy and neurophysiology of the vagus nerve (VN) for standardised intraoperative neuromonitoring (IONM) of the inferior laryngeal nerve (ILN) during thyroidectomy. Langenbecks Arch Surg. 2010;395(7):893–9.
Chiang FY, Lee KW, Chen HC, Chen HY, Lu IC, Kuo WR, Hsieh MC, Wu CW. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg. 2010;34(2):223–9.
Dionigi G, Alesina PF, Barczynski M, Boni L, Chiang FY, Kim HY, Materazzi G, Randolph GW, Terris DJ, Wu CW. Recurrent laryngeal nerve injury in video-assisted thyroidectomy: lessons learned from neuromonitoring. Surg Endosc. 2012;26(9):2601–8.
Dionigi G, Wu CW, Kim HY, Rausei S, Boni L, Chiang FY. Severity of recurrent laryngeal nerve injuries in thyroid surgery. World J Surg. 2016;40(6):1373–81.
Chiang F-Y, Lu IC, Chang P-Y, Dionigi G, Randolph GW, Sun H, Lee K-D, Tae K, Ji YB, Kim SW, et al. Comparison of EMG signals recorded by surface electrodes on endotracheal tube and thyroid cartilage during monitored thyroidectomy. Kaohsiung J Med Sci. 2017;33(10):503–9.
Schneider R, Randolph GW, Sekulla C, Phelan E, Thanh PN, Bucher M, Machens A, Dralle H, Lorenz K. Continuous intraoperative vagus nerve stimulation for identification of imminent recurrent laryngeal nerve injury. Head Neck. 2013;35(11):1591–8.
Phelan E, Schneider R, Lorenz K, Dralle H, Kamani D, Potenza A, Sritharan N, Shin J. G WR: continuous vagal IONM prevents recurrent laryngeal nerve paralysis by revealing initial EMG changes of impending neuropraxic injury: a prospective, multicenter study. Laryngoscope. 2014;124(6):1498–505.
Wu CW, Dionigi G, Sun H, Liu X, Kim HY, Hsiao PJ, Tsai KB, Chen HC, Chen HY, Chang PY, et al. Intraoperative neuromonitoring for the early detection and prevention of RLN traction injury in thyroid surgery: a porcine model. Surgery. 2014;155(2):329–39.
Dionigi G, Bacuzzi A, Boni L, Rovera F, Dionigi R. What is the learning curve for intraoperative neuromonitoring in thyroid surgery? Int J Surg. 2008;6(Suppl 1):S7–12.
Cirocchi R, Arezzo A, D’Andrea V, et al. Intraoperative neuromonitoring versus visual nerve identification for prevention of recurrent laryngeal nerve injury in adults undergoing thyroid surgery. Cochrane Database Syst Rev. 2019;1(1):CD012483. https://doi.org/10.1002/14651858.CD012483.pub2.
Zheng S, Xu Z, Wei Y, Zeng M, He J. Effect of intraoperative neuromonitoring on recurrent laryngeal nerve palsy rates after thyroid surgery–a meta-analysis. J Formos Med Assoc. 2013;112(8):463–72. https://doi.org/10.1016/j.jfma.2012.03.003.
Higgins TS, Gupta R, Ketcham AS, Sataloff RT, Wadsworth JT, Sinacori JT. Recurrent laryngeal nerve monitoring versus identification alone on post-thyroidectomy true vocal fold palsy: a meta-analysis. Laryngoscope. 2011;121(5):1009–17. https://doi.org/10.1002/lary.21578.
Dralle H, Sekulla C, Haerting J, et al. Risk factors of paralysis and functional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery. 2004;136(6):1310–22. https://doi.org/10.1016/j.surg.2004.07.018.
Roberts JR, Wadsworth J. Recurrent laryngeal nerve monitoring during mediastinoscopy: predictors of injury. Ann Thorac Surg. 2007;83(2):388–91. discussion 391-382
Uldry E, Schafer M, Saadi A, Rousson V, Demartines N. Patients’ preferences on information and involvement in decision making for gastrointestinal surgery. World J Surg. 2013;37(9):2162–71.
Horne SK, Gal TJ, Brennan JA. Prevalence and patterns of intraoperative nerve monitoring for thyroidectomy. Otolaryngol Head Neck Surg. 2007;136(6):952–6.
Dralle H, Lorenz K, Machens A. Verdicts on malpractice claims after thyroid surgery: emerging trends and future directions. Head Neck. 2012;34(11):1591–6.
Randolph GW, Shin JJ, Grillo HC, Mathisen D, Katlic MR, Kamani D, Zurakowski D. The surgical management of goiter: part II. Surgical treatment and results. Laryngoscope. 2011;121(1):68–76.
Kim HY, Tufano RP, Randolph G, Barczynski M, Wu CW, Chiang FY, Liu X, Masuoka H, Miyauchi A, Park SY, et al. Impact of positional changes in neural monitoring endotracheal tube on amplitude and latency of electromyographic response in monitored thyroid surgery: results from the Porcine Experiment. Head Neck. 2016;38(Suppl 1):E1004–8.
Liddy W, Lawson BR, Barber SR, Kamani D, Shama M, Soylu S, Wu CW, Chiang FY, Scharpf J, Barczynski M, et al. Anterior laryngeal electrodes for recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: new expanded options for neural monitoring. Laryngoscope. 2018;128(12):2910–5.
Lee HS, Oh J, Kim SW, Jeong YW, Wu CW, Chiang FY, Lee KD. Intraoperative neuromonitoring of recurrent laryngeal nerve during thyroidectomy with adhesive skin electrodes. World J Surg. 2020;44(1):148–54.
Chiang FY, Lu IC, Chang PY, Sun H, Wang P, Lu XB, Chen HC, Chen HY, Kim HY, Dionigi G, et al. Stimulating dissecting instruments during neuromonitoring of RLN in thyroid surgery. Laryngoscope. 2015;125(12):2832–7.
Wu CW, Liu X, Barczynski M, Kim HY, Dionigi G, Sun H, Chiang FY, Kamani D, Randolph GW. Optimal stimulation during monitored thyroid surgery: EMG response characteristics in a porcine model. Laryngoscope. 2017;127(4):998–1005.
Lamade W, Ulmer C, Seimer A, Molnar V, Meyding-Lamade U, Thon KP, Koch KP. A new system for continuous recurrent laryngeal nerve monitoring. Minim Invasive Ther Allied Technol. 2007;16(3):149–54.
Ulmer C, Koch KP, Seimer A, Molnar V, Meyding-Lamade U, Thon KP, Lamade W. Real-time monitoring of the recurrent laryngeal nerve: an observational clinical trial. Surgery. 2008;143(3):359–65.
Schneider R, Przybyl J, Pliquett U, Hermann M, Wehner M, Pietsch UC, Konig F, Hauss J, Jonas S, Leinung S. A new vagal anchor electrode for real-time monitoring of the recurrent laryngeal nerve. Am J Surg. 2010;199(4):507–14.
Sinclair CF, Téllez MJ, Ulkatan S. Noninvasive, tube-based, continuous vagal nerve monitoring using the laryngeal adductor reflex: feasibility study of 134 nerves at risk. Head Neck. 2018;40(11):2498–506.
Brauckhoff M, Walls G, Brauckhoff K, Thanh PN, Thomusch O, Dralle H. Identification of the non-recurrent inferior laryngeal nerve using intraoperative neurostimulation. Langenbecks Arch Surg. 2002;386(7):482–7.
Wu CW, Hao M, Tian M, Dionigi G, Tufano RP, Kim HY, Jung KY, Liu X, Sun H, Lu IC, et al. Recurrent laryngeal nerve injury with incomplete loss of electromyography signal during monitored thyroidectomy-evaluation and outcome. Langenbecks Arch Surg. 2016; https://doi.org/10.1007/s00423-00016-01381-00428.
Schneider R, Sekulla C, Machens A, Lorenz K, Thanh PN, Dralle H. Dynamics of loss and recovery of the nerve monitoring signal during thyroidectomy predict early postoperative vocal fold function. Head Neck. 2016;38(Suppl 1):E1144–51.
Lu IC, Chu KS, Tsai CJ, Wu CW, Kuo WR, Chen HY, Lee KW, Chiang FY. Optimal depth of NIM EMG endotracheal tube for intraoperative Neuromonitoring of the recurrent laryngeal nerve during thyroidectomy. World J Surg. 2008;32(9):1935–9.
Randolph GW. Surgery of the thyroid and parathyroid glands. Philadelphia: Saunders, Elsevier; 2013.
Puram SV, Chow H, Wu CW, Heaton JT, Kamani D, Gorti G, Chiang FY, Dionigi G, Barczynski M, Schneider R, et al. Posterior cricoarytenoid muscle electrophysiologic changes are predictive of vocal cord paralysis with recurrent laryngeal nerve compressive injury in a canine model. Laryngoscope. 2016;126(12):2744–51.
Puram SV, Chow H, Wu CW, Heaton JT, Kamani D, Gorti G, Chiang FY, Dionigi G, Barczynski M, Schneider R, et al. Vocal cord paralysis predicted by neural monitoring electrophysiologic changes with recurrent laryngeal nerve compressive neuropraxic injury in a canine model. Head Neck. 2016;38(Suppl 1):E1341–50.
Brauckhoff K, Svendsen OS, Stangeland L, Biermann M, Aas T, Husby PJA. Injury mechanisms and electromyographic changes after injury of the recurrent laryngeal nerve: experiments in a porcine model. Head Neck. 2018;40(2):274–82.
Wu C-W, Randolph GW, Lu I-C, Chang P-Y, Chen Y-T, Hun P-C, Lin Y-C, Dionigi G, Chiang F-Y. Intraoperative neural monitoring in thyroid surgery: lessons learned from animal studies. Gland Surg. 2016;5(5):473–80.
Jonas J. Continuous vagal nerve stimulation for recurrent laryngeal nerve protection in thyroid surgery. Eur Surg Res. 2010;44(3-4):185–91.
Sitges-Serra A, Fontane J, Duenas JP, Duque CS, Lorente L, Trillo L, Sancho JJ. Prospective study on loss of signal on the first side during neuromonitoring of the recurrent laryngeal nerve in total thyroidectomy. Br J Surg. 2013;100(5):662–6.
Cernea CR, Brandao LG, Hojaij FC, De Carlucci D, et al. Negative and positive predictive values of nerve monitoring in thyroidectomy. Head Neck. 2012;34(2):175–9.
Melin M, Schwarz K, Lammers BJ, Goretzki PE. IONM-guided goiter surgery leading to two-stage thyroidectomy--indication and results. Langenbecks Arch Surg. 2013;398(3):411–8.
Caragacianu D, Kamani D, Randolph GW. Intraoperative monitoring: normative range associated with normal postoperative glottic function. Laryngoscope. 2013;123(12):3026–31.
Genther DJ, Kandil EH, Noureldine SI, Tufano RP. Correlation of final evoked potential amplitudes on intraoperative electromyography of the recurrent laryngeal nerve with immediate postoperative vocal fold function after thyroid and parathyroid surgery. JAMA Otolaryngol Head Neck Surg. 2014;140(2):124–8.
Pavier Y, Saroul N, Pereira B, Tauveron I, Gilain L, Mom T. Acute prediction of laryngeal outcome during thyroid surgery by electromyographic laryngeal monitoring. Head Neck. 2015;37(6):835–9.
Yuan Q, Wu G, Hou J, Liao X, Liao Y, Chiang FY. Correlation between electrophysiological changes and outcomes of vocal cord function in 1764 recurrent laryngeal nerves with visual integrity during thyroidectomy. Thyroid. 2020;30(5):739–45.
Tsai CJ, Tseng KY, Wang FY, Lu IC, Wang HM, Wu CW, Chiang HC, Chiang FY. Electromyographic endotracheal tube placement during thyroid surgery in neuromonitoring of recurrent laryngeal nerve. Kaohsiung J Med Sci. 2011;27(3):96–101.
Chang PY, Hu PY, Lin YC, Chen HY, Chiang FY, Wu CW, Dionigi G, Lu IC. Trachway video intubating stylet allows for optimization of electromyographic endotracheal tube placement for monitored thyroidectomy. Gland Surg. 2017;6(5):464–8.
Lu IC, Wu CW, Chang PY, Chen HY, Tseng KY, Randolph GW, Cheng KI, Chiang FY. Reversal of rocuronium-induced neuromuscular blockade by sugammadex allows for optimization of neural monitoring of the recurrent laryngeal nerve. Laryngoscope. 2016;126(4):1014–9.
Lu IC, Lin IH, Wu CW, Chen HY, Lin YC, Chiang FY, Chang PY. Preoperative, intraoperative and postoperative anesthetic prospective for thyroid surgery: what’s new. Gland Surg. 2017;6(5):469–75.
Lu IC, Wu SH, Wu CW. Neuromuscular blockade management for intraoperative neural monitoring. Kaohsiung J Med Sci. 2020;36(4):230–5.
Lu IC, Wu SH, Chang PY, Ho PY, Huang TY, Lin YC, Kamani D, Randolph GW, Dionigi G, Chiang FY, et al. Precision neuromuscular block management for neural monitoring during thyroid surgery. J Invest Surg. 2020:1–8. https://doi.org/10.1080/08941939.2020.1805055.
Wu CW, Lee KD, Tae K, Ji YB, Kim SU, Lee HS, Lee KW, Chiang FY. Recurrent laryngeal nerve (RLN) injury in thyroid surgery: lessons learned from the intraoperative neural monitoring (IONM). Int J Head Neck Sci. 2017;1(1):19–26.
Singer MC, Rosenfeld RM, Sundaram K. Laryngeal nerve monitoring: current utilization among head and neck surgeons. Otolaryngol Head Neck Surg. 2012;146(6):895–9.
Ho Y, Carr MM, Goldenberg D. Trends in intraoperative neural monitoring for thyroid and parathyroid surgery amongst otolaryngologists and general surgeons. Eur Arch Otorhinolaryngol. 2013;270(9):2525–30.
Marti JL, Holm T, Randolph G. Universal use of intraoperative nerve monitoring by recently fellowship-trained thyroid surgeons is common, associated with higher surgical volume, and impacts intraoperative decision-making. World J Surg. 2016;40(2):337–43.
Sturgeon C, Sturgeon T, Angelos P. Neuromonitoring in thyroid surgery: attitudes, usage patterns, and predictors of use among endocrine surgeons. World J Surg. 2009;33(3):417–25.
Schneider R, Randolph GW, Barczynski M, Dionigi G, Wu C-W, Chiang F-Y, Machens A, Kamani D, Dralle H. Continuous intraoperative neural monitoring of the recurrent nerves in thyroid surgery: a quantum leap in technology. Gland Surg. 2016;5(6):607–16.
Chiang FY, Lu IC, Chen HC, Chen HY, Tsai CJ, Hsiao PJ, Lee KW, Wu CW. Intraoperative neuromonitoring for early localization and identification of the recurrent laryngeal nerve during thyroid surgery. Kaohsiung J Med Sci. 2010;26(12):633–9.
Snyder SK, Sigmond BR, Lairmore TC, Govednik-Horny CM, Janicek AK, Jupiter DC. The long-term impact of routine intraoperative nerve monitoring during thyroid and parathyroid surgery. Surgery. 2013;154(4):704–11. discussion 711–703
Sari S, Erbil Y, Sumer A, Agcaoglu O, Bayraktar A, Issever H, Ozarmagan S. Evaluation of recurrent laryngeal nerve monitoring in thyroid surgery. Int J Surg. 2010;8(6):474–8.
Goretzki PE, Schwarz K, Brinkmann J, Wirowski D, Lammers BJ. The impact of intraoperative neuromonitoring (IONM) on surgical strategy in bilateral thyroid diseases: is it worth the effort? World J Surg. 2010;34(6):1274–84.
Chandrasekhar SS, Randolph GW, Seidman MD, Rosenfeld RM, Angelos P, Barkmeier-Kraemer J, Benninger MS, Blumin JH, Dennis G, Hanks J, et al. Clinical practice guideline: improving voice outcomes after thyroid surgery. Otolaryngol Head Neck Surg. 2013;148(6 Suppl):S1–37.
Schneider R, Lamade W, Hermann M, Goretzki P, Timmermann W, Hauss J. Continuous intraoperative neuromonitoring of the recurrent laryngeal nerve in thyroid surgery (CIONM) – Where are we now? An update to the European Symposium of Continuous Neuromonitoring in Thyroid Surgery. Zentralbl Chir. 2012;137(1):88–90.
Cernea CR, Ferraz AR, Furlani J, Monteiro S, Nishio S, Hojaij FC, Dutra Junior A, Marques LA, Pontes PA, Bevilacqua RG. Identification of the external branch of the superior laryngeal nerve during thyroidectomy. Am J Surg. 1992;164(6):634–9.
Alesina PF, Hinrichs J, Meier B, Cho EY, Bolli M, Walz MK. Intraoperative neuromonitoring for surgical training in thyroid surgery: its routine use allows a safe operation instead of lack of experienced mentoring. World J Surg. 2014;38(3):592–8.
Kamani D, Potenza AS, Cernea CR, Kamani YV, Randolph GW. The nonrecurrent laryngeal nerve: anatomic and electrophysiologic algorithm for reliable identification. Laryngoscope. 2015;125(2):503–8.
Musholt TJ, Clerici T, Dralle H, Frilling A, Goretzki PE, Hermann MM, Kussmann J, Lorenz K, Nies C, Schabram J, et al. German Association of Endocrine Surgeons practice guidelines for the surgical treatment of benign thyroid disease. Langenbecks Arch Surg. 2011;396(5):639–49.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133.
Chen AY, Bernet VJ, Carty SE, Davies TF, Ganly I, Inabnet WB III, Shaha AR. American thyroid association statement on optimal surgical management of goiter. Thyroid. 2014;24(2):181–9.
Terris DJ, Snyder S, Carneiro-Pla D, Inabnet WB, Kandil E, Orloff LA, Shindo M, Tufano RP, Tuttle RMM, Urken ML, et al. American thyroid association statement on outpatient thyroidectomy. Thyroid. 2013;23(10):1193–202.
Shindo ML, Caruana S, Kandil E, McCaffrey JC, Orloff L, Porterfield JR, Randolph G, Shaha A, Shin J, Terris D. Management of invasive well-differentiated thyroid cancer an American Head and Neck society consensus statement. Head Neck. 2014;36(10):1379–90.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Wu, CW., Chiang, FY., Karcioglu, A.S., Iwata, A.J., Abdelhamid Ahmed, A.H., Randolph, G.W. (2022). Rationale and Indications for Vagus/Recurrent Laryngeal Nerve Monitoring. In: Scharpf, J., Randolph, G.W. (eds) Intraoperative Cranial Nerve Monitoring in Otolaryngology-Head and Neck Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-84916-0_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-84916-0_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-84915-3
Online ISBN: 978-3-030-84916-0
eBook Packages: MedicineMedicine (R0)