
Abstract
In recent years, society has been growing and aging at accelerated rates. Consequently, it has been of great interest to develop rehabilitation and gait assistance solutions by medical and engineering professionals. Moreover, worldwide statistics report high incidence indicators of neurological and physical impairments, being a public health concern in several countries. In this sense, there are four types of assistive technologies that can be found in the field of rehabilitation engineering, focusing on human mobility: (1) wearable robots, (2) mobile robots, (3) social robots, and (4) combined platforms. Depending on the requirements of each user, these robotic devices aim to compensate, retrain, or provide the affected locomotion capabilities of the individual. This chapter defines these devices and describes their implementation in the context of gait assistance and rehabilitation. Similarly, it provides some evidence of applications in clinical scenarios.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Human mobility
- Gait rehabilitation
- Gait assistance
- Wearable robots
- Mobile robots
- Social robots
- Physical rehabilitation
- Rehabilitation robots
1.1 Human Gait
The ability to freely move and interact within a specific environment provides people with autonomy and independence during daily life activities. In this way, human mobility is one of the essential capacities for proper development and well-being. In general terms, human gait is a complex behavior that involves the musculoskeletal system, the nervous systems, and the cardio-respiratory system [1, 2]. Human gait requires the central nervous system (CNS) activation, the transmission of electrical signals to the muscles, muscular activation, and sensory information feedback [3]. Altogether, these systems enable gait initiation, planning, and execution, while being adapted to satisfy motivational and environmental demands of the individual [4]. The ability to walk is usually acquired at the first years of life [5]. During this stage, skills such as body weight balancing and upright standing are learned [6]. Once the individual learns to walk, this ability becomes spontaneous and unconscious, becoming an energy-efficient task [5, 6].
1.1.1 The Gait Cycle
The complexity of the human gait has become a topic of major interest within the field of human movement sciences. It is a key component in the investigation of pathological gait patterns. Human gait is a cyclic activity that can be described as a series of discrete events [7]. The gait cycle is often defined as the period of time from the initial contact of one foot with the ground to the following occurrence of the same event with the same foot (it is also known as stride). The gait cycle consists of two major phases: stance phase, which cover 60% of the cycle and swing phase that covers the remaining 40% [8]. Stance phase is the term used to designate the entire period during which the foot is on the ground. Whereas swing phase is defined as the period when the foot is in the air and the limb advances in preparation for subsequent foot contact [9]. The precise duration of these gait cycle intervals varies with the person’s cadence. The duration of both gait periods is shortened as gait velocity increases and becomes progressively greater as speed slows.
The gait cycle provides a means of correlating the simultaneous actions of the individual joints into patterns of total limb function and delineate in an orderly manner their specific biomechanical functions [10]. To this end, each pattern motion is related to a different functional demand that is why a more detailed breakdown of gait cycle is required, in such cases, four, six, or even eight different phases have been considered depending on the specific type of application. The most detailed gait cycle classification recognized by the literature is illustrated in Fig. 1.1 [10]. Stance phase consists of five events: heel strike (HS), Flat Foot (FF), midstance (MST), Heel-Off (HO), and preswing (PS). Swing phase, on the other hand, consists of the other three events: Toe-Off (TO), midswing (MSW), and terminal swing (TSW). Each gait phase has a functional objective and a critical pattern of selective synergistic motion to accomplish it [11].

Gait cycle is divided into seven phases. Illustrates seven periods that were summarized into one gait cycle based on 100% of the gait. One gait cycle can be described as a dynamic and continuous occurrence of seven phases from heel contact to the next heel contact. Different nomenclatures for the gait phases are used in the literature, this is the most used
Heel strike also known as initial contact begins when the foot strikes the ground and marks the beginning of stance phase [11]. It is essential to highlight that for individuals with some pathologies, heel contact may not occur; hence, the term initial contact is more appropriated to be used. Flat foot or loading response is the first period of double limb support defined from HS (0%) to approximately 8–12% of the gait cycle [10, 11]. During this phase, the body absorbs the impact of the foot. The foot is with its entire length in contact with the ground, and the body weight is fully transferred onto the stance limb that acts as a shock absorbent resulting in knee flexion, coincident with load acceptance and deceleration of the body. The period from HS trough FF enables the limb to accomplish a basic task denominated as weight acceptance. It is the most demanding task in the stride, because three functional patterns are needed, shock absorption, initial limb stability, and control of forward progression [10,11,12].
Midstance begins when the contralateral foot leaves the ground, initiating opposite limb swing phase, and ends at the instant when the body center of mass is decelerating until it is aligned over the forefoot. MST represents the first half of single limb support, which covers approximately 8–12% to 30%. Single limb support marks the period from MST through HO, when the opposite limb is in swing phase. During this period, one limb has the total responsibility for supporting body weight in both the sagittal and coronal planes. Heel off constitutes the second half of single limb support from 30 to 50% of the overall of the gait cycle [10,11,12]. This period begins at the time of heel leaves the ground and extends until the contralateral limb contacts the ground. During this event, the center of mass leads the forefoot and accelerates as it is falling forward towards the unsupported limb [11].
Preswing constitutes the last phase of the stance phase, i.e., it is the transition phase between stance phase and swing phase. During this event, the swinging leg acts as a compound pendulum [10, 13, 14]. The period of the pendulum is controlled by the mass moment of inertia. Variations in gait cadence are highly dependent on an individual’s ability to alter the period of this pendulum. Hence, this period is associated with limb advancement [10]. Limb advancement begins in the final phase of stance and then continues through the entire swing period. It means that during limb advancement four gait phases are involved: preswing (end of stance), initial swing, mid swing, and terminal swing. This period has the purpose to meet the high demands of advancing the limb. Therefore preparatory posturing begins in stance. Then the limb swings through three postures as it lifts itself, advances and prepares for the next stance interval.
Toe off is a short period when the toes leave the ground like their name said. During this period, the stance limb is unloaded, and body weight is transferred onto the contralateral limb. It is a period of modulated acceleration that covers the time from 62 to 75% of the overall gait cycle and usually occupies one-third of the swing phase [10, 12]. Midswing begins at the moment the foot leaves the ground and continues until maximum knee flexion occurs, when the swinging limb is aligned with the contralateral limb, and ends when the swinging limb is in front of the stance limb. This period covers the middle third of swing phase from 75 to 87% of the overall gait cycle. Terminal swing is the last event of the swing phase from 87 to 100%, which initiates with vertical tibial alignment and continues until HS [10,11,12].
1.1.2 Gait Assistance and Rehabilitation
Despite the evident complexity of gait, individuals usually exhibit smooth, regular, stable, and repeated movements during walking [1, 3]. However, affectations to these systems could result in disorders or limitations to mobility [15]. Particularly, as the human gait gathers almost of the muscles of the body, as well as involves several cortical and sub-cortical structures, the training processes after physical and neurological injuries are usually challenging and long [5]. In this sense, the gait quality and locomotion capacities constitute important indicators of the overall health of an individual [16]. Thus, the presence of neurological alterations or musculoskeletal pathologies might lead to atypical gait patterns, weakness or loss of motor control [17].
The most common causes of gait impairments include neurological conditions (e.g., cerebrovascular accidents, spinal cord injuries, Parkinson disease, and Huntington disease), orthopedic disorders (e.g., osteoarthritis, skeletal deformities, and muscular dystrophy), and several medical conditions (e.g., coronary heart disease, respiratory insufficiency, and obesity) [2, 15, 18]. With aging, the risk factor of health conditions that affects well-being and overall autonomy is increased. This effect includes gait disorders [19]. Older adults often exhibit cardiovascular complications, musculoskeletal diseases, cancer, and impaired proprioceptive functions [20,21,22]. In general, these conditions result in cognitive and physical limitations and can cause the partial loss or degradation of the upper and lower-limbs’ healthy functioning [23,24,25].
Physical rehabilitation aims at restoring people’s movement and functioning affected by injuries, illness, or disability [26]. Gait rehabilitation and assistance therapies focus on providing, compensating, increasing, or re-training the lost locomotion capacities and the affected cognitive abilities of the individual [18]. In general terms, rehabilitation interventions seek to improve walking performance by (1) eliciting voluntary muscular activation in lower limbs, (2) increasing muscle strength and coordination, (3) recovering walking speed and endurance (i.e., usually accompanied with cardiovascular training), and (4) maximizing lower-limbs range of motion [27, 28]. In this sense, physical rehabilitation includes several techniques and approaches, ranging from overground and conventional gait training to robot-assisted and machine-based therapies [29, 30]. These strategies emphasize weight support, body mass propulsion, as well as on balance and postural control during movement [31].
Bearing in mind the above mentioned, this chapter presents an introductory overview of robotics for human gait rehabilitation and assistance. Advances in engineering and healthcare have led to the development of rehabilitation devices based on multiple robotic principles. Therefore, throughout this chapter, as well as in the remainder of this book, the focus will be on (1) Wearable Robotics, (2) Mobile Robotics, (3) Social Robotics, and (4) Combined Robotic Platforms with a particular emphasis on gait rehabilitation and assistance. Thus, the following sections present a definition of these fields of robotics, a description of how they can be applied to healthcare and physical training, and evidences of their use in rehabilitation therapies and gait assistance.
1.2 Wearable Robotics
The first type of device studied in this chapter used in gait assistance and rehabilitation is wearable robotic devices. This section introduces them, focusing on lower-limb exoskeletons. The following topics are presented: (1) a description of wearable robotics, (2) an introduction to lower-limb exoskeletons and their main objectives in the field of assistance and rehabilitation, (3) their evidence in gait rehabilitation scenarios, and finally (4) their evidence in gait assistance scenarios.
1.2.1 Defining Wearable Robotics
The robotic devices were used to support and develop some tasks that require different interaction levels with humans [32]. This Human–Robot Interaction (HRI) has been involved in activities where the robot has physical interaction with various parts of the human body [33]. Therefore, these robotic devices are being developed according to some standards that consider the user’s safety when operating this device [34,35,36]. As a result, the definition of wearable robots emerges. As mentioned by Pons [37], “a wearable robot is person-oriented robots, that complement the limb primary movements or replace a human body limb”. Currently, the development of wearable robot is applied to different areas according to the user’s workspaces. For instance, applications where the user’s body supports high loads for a long time [38, 39], replacement of a human body limb [40], or robotic devices that complement or assist different human body movements [41,42,43,44].
As mentioned, the implementation of wearable robots involves the performance of a robotic device that supports and assists the user’s limbs movements. In the first case, the wearable robots are used in clinical scenarios. The user wears the device in the therapy sessions to recover different primary motor functions to the human body. In the second case, the user cannot generate the required muscle activity to execute the limb’s primary movements. For this reason, this device assists the limb’s movements. The wearable robots focus on factors such as the shape, weight, and kinematic of the robotic device [37]. Each of these factors is directly dependent on the number the links and joints that provide kinematic compatibility [45, 46], the different types of physical interfaces to ensure a mechanical power direct transfer [47], and the type of actuation system that provides the backdriveability condition to the wearable robot [48,49,50,51]. Finally, the estimation of the physical Human–Robot Interaction (pHRI) [52] allows the device to provide safety and comfort in support of different activities of daily living [53]. In this way, wearable robots are designed to apply the pHRI in various strategies depending on the user in developing different tasks in particular workspaces.
The assessment of the wearable is focused on critical aspects related to the functional performance applied on the interaction between the wearable robot and the user [54, 55]; the user experience focused on the embodiment [56]; the wearable robot usability [57]; and the methodology that comprises the reproducibility of the experiments executed with the wearable robot controlled by the user, the acquisition and the facility in interpreting the results [58]. This device is assessed in two aspects related to the electrical and mechanical structure [36]. In this sense, some international organizations have raised several standards to guarantee user safety. For instance, the International Organization for Standardization (ISO) in collaboration with the Electrotechnical Commission (IEC) identifies the particular hazards presented in the Human–Robot Interaction. Where the IEC 62061 formulates a safety standard for robots and robotics personal care [34], the ISO 13482 “Robots and robotic devices—Safety requirements for personal care robots” [34], and the ISO 22523 “External limb prostheses and external orthoses—Requirements and test methods” [35] focused in the requirements and test methods for lower-limb exoskeletons.
Currently, there are various wearable robots that have fulfilled all the relevant factors mentioned, offering different services according to the population. Some of these devices are robotic prostheses, aimed at replacing the limb of a user who has suffered limb loss [59, 60]; exoskeletons or orthoses focused on the industry whose purpose is to reduce the load perceived by the user [38, 39]; and finally, exoskeletons concentrate on the rehabilitation and assistance of activities of daily living that currently have been developed for various joints of the human body [42, 61, 62]. The development of these exoskeletons includes the use of different instruments for data acquisition from the user. Finally, the development of different control strategies has allowed the user to participate in the therapy sessions or improve the user’s quality of life with activity of daily living assistance.
1.2.2 Lower-Limb Exoskeletons
Lower-limb exoskeleton has been implemented for various applications related to increasing a person’s motor capabilities. As mentioned by Minchala et al. defined a lower-limb exoskeleton as an anthropomorphic mechanical device that conforms to the user’s anatomy. Where the movements generated by the device resemble various movements of the human body [63], therefore, its main objective is focused on three main aspects: increasing the strength of the human body [64,65,66,67], motor control rehabilitation of the human body [48, 68,69,70,71], and the assistance of the user’s movements in various activities [42, 61, 71,72,73]. Lower-limb exoskeletons classification can be executed from various viewpoints starting with the different control strategies, workspace settings, tasks assisted by the device, and actuation systems. This book focuses on lower-limb exoskeletons developed for the rehabilitation of people suffering from gait-associated pathologies and gait assistance.
1.2.2.1 Lower-Limb Exoskeletons in Gait Rehabilitation
Lower-limb exoskeletons for gait rehabilitation are designed for the medical field where they are considered a tool for use in therapy sessions. The application of these devices fulfills two objectives. The first one is focused on supporting the recovery motor control [74] in the lower limbs by stimulating neuronal plasticity [75,76,77]. Second, the use of these robotic devices in rehabilitation decreases the therapist’s workload to supervise the therapy session [68, 78,79,80]. In this way, the lower-limb exoskeletons support the user’s movements and assist in the performance of the therapy sessions proposed by the therapist.
The exoskeleton for gait rehabilitation applied in indoor environments is integrated into a robotic platform complemented by bodyweight support [81, 82] and a treadmill [49, 83]. This lower-limb exoskeleton design provides an environmentally controlled working area in the development of the walking activity. Lower-limb exoskeleton is generally composed of different degrees of freedom (DoF), providing movement in the three human body planes. As a result, these rehabilitation platforms assimilate the user’s lower-limb’s natural movements during the walking activity. Additionally, each platform has a sensory interface to monitor the gait speed [83] and the gait cycle [84, 85], the joint’s range of motion (RoM) [83], force/torque generated between the user and the wearable robot [50], the assistance level provided by the exoskeleton [81], and other kinetic and kinematic parameters to develop various control strategies, and to monitor the therapy session.
Different gait rehabilitation platforms use lower-limb exoskeletons to support the user’s lower-limb movements in walking activity. For instance, ALTACRO (Vrije University, Belgium) comprised of the MACCEPA actuation system provides adaptable compliance during the walking activity using 12 DoF in Hip, knee, and ankle joints [49, 86]. LOPES (University of Twente, Netherlands) exoskeleton applies a bowden cable system actuation [78, 83, 87] to implement the “Robot in charge”, “Patient in charge”, and the “Therapist in charge” modalities [83]. As a result, the exoskeleton allows movements in the leg and a free 3-D translation of the pelvis [87]. ALEX (University of Delaware, USA) applies force fields to guide the user’s foot trajectory into a prescribed gait pattern [82, 88]. Finally, a commercial rehabilitation such as Lokomat [68] is classified as a powered gait orthosis that can increase therapy session’s intensity and reduce the therapist burden and healthcare cost [89]. Figure 1.2a presents a lower-limb exoskeleton schematic for gait rehabilitation for indoor environments.

Lower-limb exoskeleton schematics; (a) lower-limb exoskeleton for gait rehabilitation in indoor environments example. Generally, this platform comprises a bodyweight support, Treadmill, and a lower-limb exoskeleton designed with various DoF that covers the movements in different human body planes; (b) lower-limb exoskeleton for gait rehabilitation/assistance in outdoor environment example. This wearable robot is composed of a lower-limb exoskeleton that generally supports the sagittal plane movements, instrumented crutches, and a human–machine interface
On the other hand, the literature presents different lower-limb exoskeleton types of gait rehabilitation where the user executes the walking activity in outdoor environments using a lower-limb exoskeleton [90]. In this sense, the device’s design changes compared to the exoskeletons mentioned in the last paragraph. The new design of these exoskeletons presents a portable design. This characteristic includes a portable power supply, processing module, and a sensory interface that the user could transport in various environments. Additionally, aspects such as the actuation system size [91], exoskeleton size [92], weight [74], and the kinematic configuration [45, 65] are taken into account to improve the interaction between the wearable robot and the user [93]. To fulfill the main objective of rehabilitating the walking activity in outdoor environments, some of the above aspects, such as design considerations regarding the number of DoF, generally, focus on the human body sagittal plane. Finally, considering that these exoskeletons do not have a bodyweight support, in some cases, the lower-limb exoskeletons are complemented using walkers [94] and crutches [95] to provide support and stability during the walking activity.
Currently, lower-limb exoskeletons have been implemented in the rehabilitation of activities of daily living employing different methodologies. For instance, the ALLOR (Federal University of Espirito Santo, Brazil) is a unilateral knee exoskeleton that changes the impedance components using virtual damping according to a detected gait phase during the walking activity [69, 94]. BioMot (Future and Emerging Technologies (FET), Spain) is a bilateral lower-limb exoskeleton that uses a MACCEPA to change the system stiffness through the Hook law [70]. BLEEX exoskeleton (University of California Berkeley, USA) now known as Ekso GT was designed in the rehabilitation and assistance of stroke patients and spinal cord injury, respectively [71, 91, 96, 97]. Figure 1.2b shows an example of a lower-limb exoskeleton for the rehabilitation of activities of daily living.
The exoskeletons mentioned above are based on a rigid mechanical structure to transfer the calculated torques to the users’ lower-limbs. However, the latest developments presented in the literature show different other wearable robot based on soft technology. In this field, the exosuits have been designed to fulfill the lower-limb exoskeleton purpose offering a lightweight device and an actuation system that generate the required torque profiles in the user’s lower limbs. For instance, XoSoft (Fondazione Istituto Italiano di Tecnologia, Italy) and Myosuit (ETH Zurich, Switzerland) are exosuits designed for activity of daily living rehabilitation using cable-driven actuation to complement the lower-limb movements [48, 98,99,100]. As a result, implementing these exosuits in therapy allows different joint lower-limb movements and decreases the exoskeleton weight.
1.2.2.2 Lower-Limb Exoskeletons in Gait Assistance
Another field where the lower-limb exoskeletons have been applied is in gait assistance. Compared to the exoskeleton mentioned in Sect. 1.2.2.1, these lower-limb exoskeletons’ primary objectives are to provide a high level of assistance in the human body’s primary movements [90, 95]. Figure 1.2b shows examples of lower-limb exoskeleton design for this end. For this reason, the control strategies proposed in these devices have not considered the force/torque between the user and the wearable robot [42, 71, 101]. In this case, the user that wearers the lower-limb exoskeleton operates the wearable robot. Therefore, these devices propose various human–robot interfaces such as wrist-watch style controller [42, 61], external computers [73], smartphone app [74], among others. The user can mobilize in outdoor environments employing this category of lower-limb exoskeletons. In this sense, some characteristics of lower-limb exoskeletons for activity of daily living rehabilitation are applied in these exoskeletons. For instance, actuation system size, exoskeleton size, weight, and kinematic configuration are considered. Parameters such as kinematic the joint angular position, the joint angular velocity are estimated, and other kinematic and kinetic parameters are required for control strategies applied in these devices [42, 72, 91, 101].
Lower-limb exoskeletons for assistance have been presented in the literature and some of these devices are patented for commercialization. Various of these devices demonstrated their feasibility and performance CYBATHLON [102], often mentioned in the literature as the Paralympic Games, where the paraplegic users compete in the development of various activities of daily living. As an example ReWalk (ReWalk Robotics, United Kingdom) [61, 103], REX (REX Bionics, New Zealand) [42], Indego (Vanderbilt University, USA) [42], VariLeg (ETH Zurich, Switzerland) [57, 73, 104], WalkON (Sogang University, South Korea) [72] are highlighted in these applications focused on the assistance of walking activity, sitting/standing activities, ascending/descending stairs, and walking on sloping surfaces.
Table 1.1 shows some relevant characteristics of the exoskeletons for gait assistance and rehabilitation reviewed in this section. There were mentioned some lower-limb exoskeletons classified by the category (gait rehabilitation/gait assistance), degree of freedom for each limb, the bilateral/unilateral exoskeleton, and some activities of daily living that the exoskeletons provide a user’s support and assistance.
In conclusion, this section presented the general definition of a wearable robot and relevant aspects for their development. For example, lower-limb exoskeletons are the product of the development of wearable robots that have been developed as tools for rehabilitation and assistance for users with pathologies associated with the lower limbs. Some characteristics that identify exoskeletons designed for rehabilitation and assistance were shown. Finally, the exoskeletons developed in the last decades were mentioned, considering the difference between exoskeletons designed for the rehabilitation environment and the user’s assistance environment.
1.3 Mobile Robotics
The second type of device used in gait assistance and rehabilitation therapies is mobile robotics. This section presents an introduction, concentrating on robotic or smart walkers. The following topics are presented: (1) a description of several mobile conventional devices, (2) a description of the smart walkers, from their overall structure to their functioning and interaction channels, (3) the evidence of smart walkers use in gait assistance and rehabilitation, with several applications in clinical scenarios, and finally (4) alternative mobile robots for gait rehabilitation, where other assistance platforms based on mobile robots will be showcased.
1.3.1 Defining Mobile Assistive Devices
Mobile devices for gait assistance often include ambulatory training tools and wheeled-based structures. For instance, these devices exploit the widely studied benefits of wheeled mobile robots, such as stability, balance, power autonomy, mechanical simplicity, among others. Mobile assistive devices intend to overcome physical limitations by maintaining or improving individuals’ functioning and independence in clinical and everyday scenarios [106]. Moreover, these devices can be classified into conventional and robotic devices. The most common conventional mobile devices are manual wheelchairs, walking sticks or canes, walking frames, and rollators [107] (See Fig. 1.3).

Illustration of standard mobile conventional devices based on wheeled or ambulatory frames. (a) Manual wheelchairs. (b) Walking sticks. (c) Walking frames. (d) Rollators
On the one hand, manual wheelchairs are a standard solution when lower-limb locomotion capacities are entirely lost. In their most straightforward configuration, these devices consist of a chair fitted with wheels, where the user is entirely in charge of the device’s propulsion [23]. The wheelchairs also provide proper fit and postural support based on each user’s biomechanical and environmental requirements. On the other hand, the walking sticks or canes are simple assistive devices that aim to increase the patients’ support base and improve their balance [108]. To provide weight support to the user, some variations include more than one support point to the floor. In this sense, multiple-legged canes or quad-canes are commonly found [108].
Finally, the walking frames or walkers are constituted by simple mechanical structures that improve overall balance, increase the users’ base of support, enhance lateral stability, and provide partial weight-bearing [108, 109]. The walkers offer support and use the patients’ remaining locomotion capability to move [109, 110]. These devices hold a rehabilitation potential as they encourage physical activity and social participation of people with mobility impairments [27]. Several types of conventional walkers can be found.
The standard walkers or walking frames are constituted by a four-legged frame with rubber tips that should simultaneously contact the floor [108, 110]. Although this configuration offers maximum stability, the patient must lift the frame and moved it forward during walking. In this sense, the use of standard walkers results in slower, and often abnormal gait patterns [108]. Moreover, this type of walker requires some degree of upper body strength and cognitive ability [110]. The front-wheeled walkers include wheels at the front legs making them more suitable for upper-limbs weakness [108]. These walkers reduce the risk for falling as lifting the device is not required, and it promotes forward displacements of the center of gravity [110]. The front-wheeled walkers facilitate more normal gait patterns and higher walking speeds [110]. The four-wheeled walker or rollators included wheels with pivot and rolling points requiring fewer users’ effort [108, 110]. Since these walkers provide minor stability, they are often used by higher functioning patients with minimal weight-bearing requirements [108, 110]. These walkers are intended to be used in community scenarios during daily living activities, as they provide the most natural gait patterns and highest walking speeds [110]. These devices are usually equipped with shopping baskets, a resting seat and hand brakes [110]. These rollators are also found in three-legged or u-shaped configurations [109].
Conventional walkers are widely used by older adults or neurological patients with high independence levels [18]. However, several issues restrict their implementation in rehabilitation settings, complex scenarios, or patients requiring higher degrees of assistance [107]. On the one hand, several studies have reported that the conventional walking frame does not ensure enough safety during walking, since there is a considerable risk for falls [111, 112]. Moreover, the users’ natural balance and energetic costs are often compromised with conventional walkers [107]. On the other hand, the user-walker interaction is entirely passive, so that the walker does not provide any additional physical and cognitive support [18, 107, 110]. For instance, patients with visual impairments may require assistance for safe navigation or guiding. Similarly, patients with reduced muscle capacity may require active assistance from the device [107, 113]. Other shortcomings associated with conventional walkers involve the inability of these devices to monitor the users’ condition or to track the quality of users’ gait. Additionally, these devices cannot provide any feedback to the users when there is an inappropriate interaction.
1.3.2 Smart Walkers
As previously stated, the walking frames or rollators exploit the patients’ remaining locomotion capacities to provide gait assistance. They are usually prescribed for patients in need of assistance during functional daily living tasks [107]. Similarly, literature evidence shows that walker-assisted gait often elicits essential psychological benefits, including increased confidence and safety perception during ambulation [27, 107]. However, critics regarding the use of these devices often point out the lack of safety measures, the increased energy expenditure, and the inability to track users’ progress and health status.
Bearing in mind the above mentioned, the possibility of improving and enhancing the functionalities of the conventional walkers through the inclusion of robotic technology has arisen. In general, there have been several research projects focused on creating robotic versions of canes, wheelchairs, and, particularly, walkers. The terms “robotic”, “intelligent”, or “smart walkers” (SWs) refer to those conventional walking frames and rollators that have been empowered with sensing interfaces, actuation technologies, and control strategies [27]. The inclusion of these technologies in the smart walkers allows providing more efficient and robust gait rehabilitation and assistance [27]. There are several benefits brought by the integration of technology and robotics, for instance (1) the execution of precise and repeatable tasks, (2) the implementation of intensive activities with programmable and measurable difficulty, (3) the online measurement of the performance and physiological state of the patients, (4) the implementation of more engaging rehabilitation environments through the use of virtual and augmented reality, (5) the assessment of the patients’ rehabilitation progress, and (6) the reduction of the physical effort of the therapists [25, 28, 31, 114].
More specifically, thanks to the sensors, actuators, and control strategies implemented in the SWs, they are capable of multiple high-level functions that can be grouped in the following categories:
-
Biomechanical and Health Monitoring: The smart walkers can gather information collected by their internal sensors and external sensors worn by the user. In this sense, the smart walkers can estimate biomechanical indicators from sensors such as Inertial Measurement Units (IMUs), Electromyography sensors (EMG), or sensors mounted on the device such as ultrasonic boards, Laser Rangefinders (LRF), cameras, among others [27, 107]. These sensors allow the estimation of gait spatiotemporal parameters such as cadence, speed, step length, stride length, gait symmetry, among others [115]. These parameters are relevant as they may help tracking and quantifying the users’ rehabilitation progress. Moreover, control strategies can also be implemented using this information [113, 116, 117]. Finally, the patients also wear heart rate sensors, oxygen saturation sensors, and other physiological sensors to estimate the overall health status.
-
Estimation of Movement’s Intention: An essential functionality that the smart walkers’ should provide is identifying the users’ intentions to move. This functionality allows the smart walkers to guarantee intuitive and natural interaction to their users. To this end, the smart walkers are often equipped with sensors on the forearm supports and handlebars to estimate the patients’ intention of movement [110]. The most common approaches exploit the resulting force and torque exerted on the walker by the user to generate linear and angular reference velocities [107, 118]. Other techniques are based on cognitive interaction, where the user can control the smart walker without physically interacting with it, using voice commands or body gestures [18, 113].
-
Guidance and Navigation: In the robotics field, navigation basically refers to a set of systems that allow a robot to safely move from one point to another within a specific environment [119]. In walker-assisted gait, navigation refers to safely guiding the users through different settings, while satisfying their social and motivational demands [107]. To this end, the smart walkers require obstacle detection and avoidance techniques, map building modules, autonomous localization algorithms, and path following strategies [107]. These functionalities can be implemented whether independently or in conjunction with user interaction modules, so that shared control strategies can be designed to regulate the users’ role during therapy [27, 120]. In this way, guidance and navigation modules help with patients with cognitive requirements or visual impairments.
-
Safety Provision: The smart walkers often assist the users in complex environments where dynamic situations might occur. Therefore, smart walkers equip redundant systems to react to hazardous situations rapidly. These modules commonly use rule-based algorithms, where different conditions and constraints are established to limit or stop the smart walker’s motion [107]. For instance, these modules allow the device to be blocked in presence of stairs, glass walls, and dangerous walkways. Using distance sensors, these modules can detect obstacles in front of the device and limit the speed depending on the proximity to the obstacles [27, 120]. Moreover, smart walkers are often remotely monitored and controlled by healthcare professionals. Thus, they can limit or stop the device’s movement in emergencies. Finally, along with these functionalities, the smart walkers also implement fall prevention strategies based on IMU sensors.
-
Feedback Strategies: The smart walkers implement multiple communication channels to provide cognitive assistance or communicate relevant information to the users. For example, during navigation tasks in patients with visual impairment, the smart walkers use haptic and auditory feedback to guide them [118, 120]. Other implementations are based on visual feedback to let the users know their performance and status during the therapy [110, 121].
-
Remote control: Gait rehabilitation therapies demand close accompanying of physiotherapists to provide postural corrections and therapy monitoring [55, 122]. In this sense, several smart walkers have implemented remote control strategies, so that the healthcare professionals can remotely assess the session data, override the device or control the smart walker’s behavior [107, 123].
According to their end purpose, smart walkers can be found in multiple configurations depending on their actuators’ type, the implemented sensory interfaces, the implemented functionalities and their mechanical structure. The smart walkers’ propulsion interface can be classified into active, passive or hybrid devices. This classification simply suggests if the propulsion is entirely accomplished by the user (i.e., passive), aided by actuators on the device’s wheels (i.e., active), or co-accomplished by the user and the device (i.e., hybrid). These topics will be further studied in the following sections and chapters.
1.3.3 Smart Walkers in Gait Assistance and Rehabilitation
Considering the above functionalities, the smart walkers have also proven helpful in gait assistance and rehabilitation therapies. Depending on each user’s specific needs, these functionalities can be adjusted to provide targeted tasks to meet the users’ clinical and personal requirements. In this sense, literature evidence shows that smart walkers have been successfully implemented in the following scenarios:
-
Smart walkers to provide stability and motion support: Similar to the conventional type, the smart walkers can provide partial body weight support, physical stability, and balance in active [107, 124] or passive configurations [120, 125]. It is worth mentioning that smart walkers in passive modality require a considerable amount of postural control and walking ability by the user. Thus, passive smart walkers can provide motion support in later stages of rehabilitation or home-based scenarios. The smart walkers in active modality require less energetic input from the user and can offer automatic context-aware propulsion. Active smart walkers tend to be used in the early stages of rehabilitation and in clinical scenarios. In both cases, the ability to provide motion support makes the smart walkers useful for individuals with partial mobility loss, presenting different residual motor capacity levels [126]. Moreover, passive or active smart walkers help the patients gain or increase their independence during daily tasks and may positively impact on self-esteem and social interaction [27, 126].
-
Smart walkers to provide functional and daily tasks assistance: The smart walkers are commonly characterized by forearm supports equipped with force sensors and pressure sensors, or devices to extract users’ intentions to move (e.g., joysticks, voice recognition modules) [27, 121]. The information extracted from such sensors (e.g., force signals) can be converted into navigation or velocity commands to make the smart walker move according to the users’ motivational demands [107, 118, 127]. This information is also used to detect undesired behaviors such as leaning more to one side of the walker, which is common in patients with hemiplegia or hemiparesis [128, 129]. In this sense, the smart walkers can cope with the users’ intentions to assist them during their daily living activities. Moreover, several robotic walkers use this information to detect the choice to perform sit-to-stand or stand-to-sit transfers by the user [130, 131]. The strategies implemented to aid the user during these transfers range from (1) simple activation of the braking system, to (2) active control of the smart walker in a forward direction to pull up the user, and (3) implementation of robotic supporting elements (e.g. forearm or chest support) to lift and guide the user [131]. Finally, smart walkers can also detect slopes, stairs or hazardous environments employing sensors such as laser rangefinders, ultrasonic sensors and cameras. With this information, the smart walkers can provide active propulsion to overcome rugged terrains such as slopes or ramps or completely stop their motion to avoid colliding with obstacles in the environment [107].
-
Smart walkers to provide guiding and safety: As previously stated, smart walkers can perform safe navigation and obstacle detection in multiple environments. These functionalities can be used to guide people with visual or cognitive impairments. Different robotic walkers use auditory feedback to indicate the obstacles or the path to follow in guiding tasks [124]. Similarly, other proposals include haptic feedback by causing the device to vibrate when there is an obstacle nearby or making the device heavier when the user deviates from the route [118, 120]. Visual feedback has also been explored in the literature, which uses lights, screens or virtual reality to indicate the route [118, 132].
-
Smart walkers to monitor health status and gait quality: The smart walkers can extract information from sensors worn by the users and onboard sensors [107]. This information is often processed to extract gait-related indicators such as speed, cadence, stride length, cycle duration, gait symmetry, among others [115]. The constant estimation of these indicators at every rehabilitation session allows the healthcare professionals to track the users’ progress and assess their gait quality. Moreover, the smart walkers also receive information related to heart rate, skin impedance, oxygen saturation, among others. The data provided by these sensors is of great relevance since it allows to monitor the overall health status of the users and detect emergencies [27].
As presented in Sierra et al., several smart walkers and on-going research projects involve the functionalities described above [107]. An updated and detailed description of some of these smart walkers is presented in Chap. 4. In the following section, some other devices based on mobile robots are presented.
1.3.4 Alternative Mobile Robots for Gait Rehabilitation
In case of total mobility impairment exhibited by the patient, several assistive devices based on mobile robots have been developed. Specifically, the conventional four-wheeled differential robots are commonly used to implement assistive devices such as robotic wheelchairs and autonomous vehicles for patients transportation (See Fig. 1.4).

(a) Illustration of a robotic wheelchair mounted on a four-wheeled mobile robot. (b) Illustration of an autonomous vehicle based on a robotic scooter
Robotic or smart wheelchairs employ actuators, sensory interfaces and advance processing algorithms to provide easier and safer navigation [133]. Moreover, considering the patients’ requirements, the robotic wheelchairs may include multimodal input interfaces, such as joysticks, touchscreens, voice recognition modules, image processing systems, and biosignals monitoring modules (e.g., electromyography and electroencephalography) [133].
Robotic scooters, standing vehicles and lifting robots are more commonly found around us [110]. These devices include several actuators and multimodal user interfaces to allow intuitive control and interaction. Moreover, these devices may be equipped with lifting mechanisms to provide sit-to-stand capabilities and partial body weight support [134].
At this point, the previous sections have highlighted and explained the benefits of employing wearable and mobile robotics in gait assistance and rehabilitation. However, there are other scenarios where robotics can foster physical training and gait assistance. In particular, patients can also benefit from social robots, in mobility and independence problems related to aging, cognitive syndromes, cardiac complications, depression, among others.
1.4 Social Robotics
In this section, a brief introduction to social robotics is presented. To achieve the complete understanding of social robots, this section provides: (1) the social robotics definition, where different definitions given to social robots are presented, (2) evidence of this type of robots in a healthcare context, and (3) applications of socially assistive robotics in gait assistance and rehabilitation.
1.4.1 Defining Social Robotics
Several definitions are given to social robotics through time. However, it is essential to clarify the meaning of “social”. This term represents two or more entities involved in the same context [135]. To illustrate a social robot’s definition, different researchers’ perspectives are currently used [136]. First, in 1999 Duffy et al. [135] defined a social robot as robots that can interact among more robots (social robots) or with humans (societal robots). The social robots according to these authors are composed of four layers: (1) physical layer, where the robot has a physic aspect within an environment and perform motor skills, (2) reactive layer to answer the stimulus of the environment through sensory interfaces, (3) deliberative layer that involves Beliefs-Desires Intention structure, and (4) the social layer in charge of the communication [135].
Afterward, in 2002 Fong et al. [137] define social robots as: embodied agents that are part of a heterogeneous group (robots or humans), and they can recognize and engage in social interactions. Moreover, Fong et al. established that social robots have environmental perceptions acquired from their own experience, i.e., they could learn a communicate within contexts. Thus, in 2004 Bartneck and Forlizzi [138] stated the Design-centered Approach of a social robot. Overall, they defined a social robot as an autonomous/semi-autonomous platform that interacts with humans following behavioral norms as in the human–human interaction. Bartneck and Forlizzi proposed two conditions to consider a platform as a social robot: (1) the robot has to be autonomous, it can interact cooperatively or non-cooperatively depending on the situation, (2) recognize human values, roles among others [138].
Finally, in 2018 Breazeal et al. [139] presented the sociable robot concept as a robot able to communicate and understand humans in social terms. In turn, human beings should be able to communicate and emphasize with sociable robots. In this case, Breazeal et al. established five fundamental characteristics to consider a robot sociable: (1) the embodiment in a situated manner (real or virtual), (2) has to have lifelike qualities, (3) the robot has to able of identifying the users, to create an interpersonal manner [139]. For instance, Theory of mind and empathy are essential to design human awareness. (4) The human has to understand the social robot’s role, and (5) the robot has to learn social situations (by imitation or mimicry), to shape its history.
1.4.2 Social Robots in Healthcare
Socially Assistive Robots (SAR) are being tested and accepted in healthcare areas, such as rehabilitation and clinical assistance. Social care sectors beyond the traditional scope of surgical and rehabilitation robots are poised to become one of the most significant technological innovations of the twenty-first century [140]. Social robots have been developed and used in multiple clinical settings and home-based areas, providing physical, cognitive and social support, as well as coaching activities, such as exercise training, education, and monitoring [141].
In this field, researchers are focused on developing social robots to perform tasks with a high degree of autonomy, while holding natural interaction with the patients and the clinical staff [142]. This has enabled social robots to provide support in healthcare scenarios through social interaction. Social robots are attractive and engaging to a wide range of children. Children often perceive social robots as something in between a pet and a friend [143]. This makes social robots an interesting play therapy tool, where children can take safe risks to learn new skills and abilities [143].
According to literature evidence, SAR have been studied in mainly four healthcare scenarios with children [141]:
-
Social robots to help emotionally cope with illness: They provide self-management tools as they help inform children about their medical conditions (e.g., cancer, diabetes) appropriately. Robots like NAO (SoftBank Robotics, France) are commonly used in this scenario, a significant emotional support tool for children [144, 145].
-
Social robots to support therapy or interventions in children with Autism Spectrum Disorder (ASD): They have been used as active agents of reinforcement in semi-structured behavior for children with ASD. They increase eye contact [146, 147], improve and develop children’s visual perspective-taking skills [148], enhance their joint attention [149], improve proprioception skills, improve in the production and recognition of children’s facial emotions [150]. Robots like NAO, CASTOR (Colombian School of Engineering, Colombia) [151, 152], Robonova (Hitec Robotics, South Korea) [153], Probo (Vrije Universiteit Brussel, Belgium) [154], Ono (Ghent University, Belgium) [149], and Kaspar (University of Hertfordshire, UK) [148] are commonly used in ASD therapies.
-
Social robots to enhance well-being during inpatient stays: They provide a positive effect on a child’s well-being through distraction, engagement, or a positive impulse on communication [155,156,157,158,159]. Pet-like robots such as Paro (AIST, Japan) and Huggable Bear (MIT, USA), or humanoid robots such as NAO are commonly used in this scenario.
-
Social robots that provide distraction during a medical procedure help decrease children’s anxiety and stress levels [158, 160, 161]. The robot most used in this scenario is NAO, which has a promising potential as a distraction during a medical procedure, especially in vaccination.
Other compelling opportunities for social robots are in the context of eldercare. Regarding this population, their interaction includes educating, facilitating the older adults’ communication and social connection with others, and assisting with adherence to care regimen through social support [162]. Specifically, in the adults and older population, SAR have been used in two healthcare scenarios mainly [141]:
-
Social robots as companions for older adults with disease: They are widely used in mental health to aid and support loneliness, depression and anxiety [141]. Companion robots aim to enhance older people’s health and psychological factors by providing companionship [163]. Robots like Paro, NAO, Pepper (Softbank Robotics, France), and Buddy (Blue Frog Robotics, France) are currently used for this purpose, especially in elderly care for dementia and physical rehabilitation [164].
-
Social robots as service robots in elderly care and well-being: They are defined as assistive devices designed to support daily activities providing more independence to the users [163]. Service robots are mainly used to support older adults in home environments and healthcare centers. The most used robots in these areas are HOBBIT (Vienna University of Technology, Austria) [165], RiSH (Oklahoma State University, USA) [166], Robot Era (Project FP7/2007-2013) [167], and RAMCIP (Project EU Horizon 2020/643433) [168].
-
Social robots for exercising, coaching, and rehabilitation: They act as companions or assistants in specific scenarios, with the aim of improving user performance or increasing motivation during certain tasks. Some scenarios in which these social robots have been shown to play a fundamental role are cardiac rehabilitation and physical training. In both cases, humanoid robots have been used due to their similarity to human beings. For example, NAO [169,170,171,172], as shown in Fig. 1.5, has shown positive results by increasing people’s motivation to continue with their rehabilitation process. And ROBOVIE (Advanced Telecommunications Research Institute International, Japan) has shown positive results encouraging users to perform physical activity [173].
Fig. 1.5 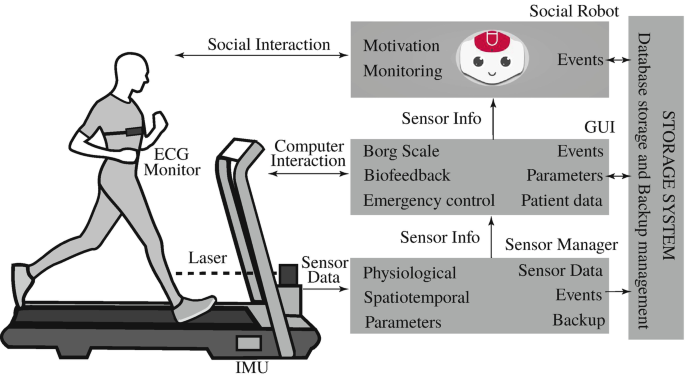
Architecture of the integration of a NAO social robot in the cardiac rehabilitation setting. This humanoid robot acts as a companion, improving user performance and increasing motivation during therapy

To summarizing, most of the studies reported positive effects of social robots within the older population. Nevertheless, some studies highlighted some issues and limitations about this technology [174], e.g., the novelty effect is decreased in some studies as the robots can become repetitive and predictable [175]. This issue can affect social interaction, which is reduced by time.
The studies identified in this section indicate that social robots can develop healthcare and well-being roles (i.e., assistance, companion, partner or coach/instructor). Social robots could be a valuable tool in healthcare personnel’s repertoire to support children, adults, and the elderly in a medical environment that deals with stresses and loneliness [141]. Besides, in the children’s population social robots might have the potential for engaging children, distracting, openness, develop their visual prospective-taking skills and decrease the level: of anger, fear, anxiety, and depression, among others. Such effects have also been noted for adults. The older under intervention with social robots, users showed improvements in social connections, communication, mood, and diminished loneliness, isolation, depression, and anxiety [141].
1.4.3 Social Robots in Gait Assistance and Rehabilitation
As presented previously, social robots have been developed and assessed in healthcare areas, showing positive effects regarding motivation, adherence and engagement to the treatments. Furthermore, in gait rehabilitation and assistance, social robotics have to support procedures from different approaches (see Table 1.2).
For instance, to assist elderly individuals in gait rehabilitation Scheidig et al. [176] developed a ROGER robot platform. This platform was used to assist elderly patients after surgery in hip endoprosthetic. ROGER’s role was to lead the patients during the therapy session and measured their gait patterns. The results showed that the platform was reliable in performing the gait assessments. Based on these results, Trinh et al. [177] conducted a study in which the ROGER platform was validated in more detail with 20 elderly patients. They considered three evaluation aspects: robust collision avoidance, user-centered navigation, and reliable person perception. The results suggested that the patients felt safe and motivated using the robot. Besides, ROGER was a valuable tool for the clinical staff as they managed and controlled the sessions. However, in regards to navigation, the results showed that further improvements are still needed for fully autonomous training, such as increasing the positional accuracy of the 3D obstacle and person detection, especially during situations where the robot is very close to the user.
Similarly, Piezzo et al. [178] presented a Pepper robot’s feasibility study to guide elderly individuals during walking. Qualitative study and gait analysis through the video analysis were performed to measure patients’ response to the robot’s role. Results showed that elderly patients trust the robot, and intrinsic motivation was influenced positively. Furthermore, the robot also aids the patients to complete their goals during the sessions (e.g., walking from a goal point to another). Moreover, the NAO robot has also been used to assist elderly patients in gait rehabilitation. Such can be illustrated in the research carried out by Cespedes et al. [179]. A human–robot interaction system that integrates sensors to measure physiological variables (heart rate, cervical and thoracic inclinations) and the exertion level perceived (Borg scale) was developed. This system allowed collaborating with the therapist’s tasks to decrease their work burden and motivate them to improve their self-performance through rehabilitation. The results suggest that the social robot has a positive and well-received effect on the robot regarding companionship, social interaction. Following this work, a long-term study showed that the robot’s support improves the patients’ physiological progress by reducing their unhealthy spinal posture time. Most patients described the platform as helpful and secure, with positive acceptance [180].
On the other hand, as far as assistance to children in gait rehabilitation is concerned, the most widely used social robot is also the NAO robot. An illustration of this is the research conducted by Buitrago et al. [181], which developed a motor learning therapeutic intervention using a social robot NAO for a child diagnosed with cerebral palsy. The researchers remark on the robot’s capability to facilitate the child’s persistence in walking and achieve the therapeutic objectives. Even they stated that after the fifth session, the children reached the proposed goal in the gait training. On the other hand, social robots are also used to support gait rehabilitation of patients who went under surgery procedures and need training during recovery phases. Therefore, Malik et al. [182] used the robot NAO in specific therapy for children with cerebral palsy. This consisted of four interactive scenarios in human–robot interaction based on the Gross Motor Functional Measure measurement items. However, the researchers reported a positive impact during therapy and effective engagement between child and robot. During the study, some mechanical errors occurred, e.g., the child did not understand what the robot said or answered the question correctly, but NAO did not detect the answer.
To summarizing, most of the studies reported positive effects of social robots to assist gait rehabilitation. They highlighted that patients feel more motivated, safe and comfortable during the session and, in turn, improved their rehabilitation performance during therapy. However, there are some issues and limitations about this technology regarding their configuration and operating setup in some gait rehabilitation scenarios.
1.5 Combined Platforms
The integration of different robotic devices, such as those mentioned throughout this chapter, has shown promising results in clinical applications, allowing to improve and accelerate the recovery of lost or diminished functions. As a result of this integration, this section presents an innovative concept called combined platforms, highlighting their use in gait assistance and rehabilitation. The following topics are presented: (1) a description of combined robotic platforms, (2) an overview of their deployments in healthcare, (3) the evidence of the use of these platforms in gait assistance and rehabilitation, with some conclusions resulting from their application in clinical scenarios, and finally (4) the general characteristics of existing combined platforms, where both electronic and mechanical characteristics will be described.
1.5.1 Defining Combined Robotic Platforms
As presented, several types of robotic devices, such as smart walkers, active joint orthosis, and lower and upper body exoskeletons, have been developed to provide rehabilitation, assistance or augmented physical capabilities in different scenarios (e.g. clinical, industry and military) [74]. Mainly, in the clinical setting, most of these devices focus on maintaining or improving an individual’s functioning and independence to facilitate participation and to enhance overall well-being [183]. Besides, in some cases, they can prevent deterioration and secondary health conditions such as bowel or bladder problems, depression, overweight, obesity, among other things [184, 185].
Because of the above, these devices have been integrated or combined to enhance and maximize their effects in rehabilitation therapies [27], being of great help for gait assistance and rehabilitation. That is why integrating two or more two robotic assistive devices can be defined as combined platforms, which aim to overcome and compensate for the physical limitations of those who suffer from them, applying to both clinical and everyday scenarios [106].
Although few studies refer to combined platforms, this new approach seeks to introduce new and reliable technologies in the rehabilitation process [186], offering interesting advantages such as the possibility of automated and personalized treatments reducing the fatigue associated with repetitive and monotonous exercises [187]. In addition to its ability to integrate sensors that provide a quantitative estimate of recovery [183].
For example, since 2006, a small number of combined platforms have been developed primarily aimed at gait rehabilitation in patients with neurological disorders [27, 188,189,190], and the clinical evaluation of these motor impairments using measures such as joint range of motion, strength, muscle reflexes, muscle activity and coordination [191, 192]. Among the studies already published, the AGoRA combined platform (Adaptable Robotic for Gait Rehabilitation and Assistance), shown below (see Fig. 1.6), stands out for being a clear example of a novel and affordable combined platform composed of two assistive devices [27].

AGoRA combined platform comprises a lower-limb exoskeleton and a smart walker oriented at gait rehabilitation of patients with mobility impairments
The combined platform concept is best exemplified in Fig. 1.6 with the AGoRA platform, composed of a lower-limb exoskeleton and a smart walker for mobility assistance and gait rehabilitation. Although this platform is one of the most recent examples, other similar combined platforms are found in the healthcare literature.
1.5.2 Combined Robotic Platforms in Healthcare
The deployment of combined platforms in the health area is considered a potential tool to improve the disabled and older population [193]. And even though robotic assistive devices are focused on helping humans, they will not replace humans’ roles in the setting [194]. In other words, these platforms have been introduced into the healthcare field to complement conventional therapeutic interventions, becoming an alternative treatment to improve the quality of life of older adults, persons with physical limitations or disabilities and those around them [195, 196].
These combined platforms’ clinical impact can be seen when the affected person can re-enter the workforce, reduce the burden on caregivers, and live at home, rather than in long-term care facilities. Some other benefits include prevention of medical complications and improved self-image and life satisfaction [193]. Therefore, in recent years, researchers have proposed and developed robotic platforms integrated by various robotic assistive devices. These efforts involved large and complex robotic systems, which evolved into more affordable systems that are both functional and aesthetically pleasing [193, 194].
Considering the above, most platforms today are integrated by an exoskeleton and a smart walker to assist people with reduced mobility. Next is a brief description of the existing combined platforms. Their use results are presented, allowing to offer a vision of the current situation of this new approach and the benefits that these can provide.
1.5.3 Combined Robotic Platforms in Gait Assistance and Rehabilitation
Combined platforms have shown positive effects in the area of rehabilitation and assistance in developing activities of daily living, helping to improve the independence and well-being of those who use them [81]. One of the first combined platforms developed was EXPOS [188]. This platform was proposed in 2006 by Sogang University as a viable solution to allow older people to live without the need for physical assistance from third parties. Furthermore, due to its ability to assist in the human body’s movement, this platform has potential use in the gait rehabilitation of patients with neuromuscular diseases.
As a combined platform, EXPOS consists of a lower-limb exoskeleton, which is as light as possible for comfort, and a smart walker, which is heavy enough to keep the body in balance when held by the user [188, 197, 198]. Although this platform typically works on flat-controlled surfaces within the laboratory, it can be adapted for everyday use. As a qualitative result, after using EXPOS in the laboratory, a user stated that this platform helped him walk, sit, and stand quite well, demonstrating its viability for the assistance of the elderly and patients with neuromuscular diseases [188].
Nine years later, in 2015, researchers from the Federal University of Espírito Santo proposed a combined platform composed of a lower-limb exoskeleton and a smart walker. This platform makes it possible to re-establish neuromotor control in subjects with neurological injuries, in addition to improving mobility and safety of those who use it while walking [199, 200].
As a combined platform, the lower-limb exoskeleton provides an assistive torque that alleviates the load and reduces the muscular effort. The smart walker guides the user and helps maintain a stable posture. As a differential factor, the researchers proposed a new control strategy based on recognizing the intention of human movement by analyzing biomedical signals such as brain signals (EEG) and surface myoelectric signals (sEMG), which turned out to be valuable and applicable in future work. So far, this combined platform does not report quantitative or qualitative results, although it is recognized as an innovative robotic system that can be adjusted to fatigue situations or according to the evolution of the user’s rehabilitation.
In 2017, researchers proposed the CPWalker platform aimed at gait training in children with cerebral palsy [189, 201]. As a combined platform, the CPWalker consists of a smart walker with bodyweight support and an exoskeleton for joint motion support [81], allowing the child to experience autonomous locomotion in a natural rehabilitation environment. Unlike the previous platforms presented, the use of CPWalker shows notable improvements in several physical skills as strength, stability, cadence, mean velocity, step length and symmetry in gait patterns [55]. All these improvements were achieved in the short term, so this research and its methodology could serve as an example for future clinical implementations of any robotic assistive device.
More recently, in 2018, Colombian researchers proposed and developed a new combined platform called AGoRA, aimed at gait assistance and rehabilitation [27, 202,203,204]. As shown in Fig. 1.6, AGoRA consists of a lower-limb exoskeleton with a bioinspired design [205], and a smart walker [202]. Although as a combined platform it has not been tested, both devices that compose it have already been assessed separately. For instance, stationary approaches such as the use of an ankle exoskeleton for motor recovery [206], the use of a lower-limb exoskeleton for knee rehabilitation [207], and their evaluations during walking have shown improvements in spatiotemporal and kinematic parameters, as well as their usability and performance through a natural interaction between users and devices [43, 46]. This platform will integrate the measurement of kinematic, physiological, and cognitive parameters to monitor the patient’s condition, his evolutionary rehabilitation process and evaluate the effects of the platform’s assistance. AGoRA platform presents interesting capabilities, such as the integration of the clinician the control loop [208] and multimodal capabilities to enhance the navigation and the interaction with the environment [107]. In this sense, it is being studied the integration of cloud computing capabilities to empower the sensor processing and control strategies [209].
During that same year, Colombian researchers proposed a new combined platform that, unlike the previous ones, integrates a social robot and a robotic gait orthosis. Since then, the researchers have been developing innovative social robot interfaces to empower gait rehabilitation in patients with spinal cord injury or stroke [179, 180, 210]. This study is focused on studying the effectiveness of socially assistive robotics during gait training with Lokomat after suffering a neurological disease to maximize the probability of success of the rehabilitation. Different variables such as heart rate, spinal posture, spatiotemporal parameters, and perceived exertion are measured, providing a feedback mechanism through a socially assistive robot. As a result of the long-term study, two patients who suffered spinal cord injury have presented remarkable improvements in motor, cognitive and emotional processes [180].
All the platforms mentioned above have the main objective of being an effective tool for the assistance and rehabilitation of gait through robot-assisted therapy, especially in patients with neuromuscular disorders or also in older adults [211,212,213,214]. For this reason, these platforms have become a new alternative to help people with motor disabilities to recover or compensate for the loss of motor control, and re-establish their independence and well-being [215, 216].
In addition to sharing the same objective, these platforms have similarities at a structural level. Next, general aspects of their mechanical and electronic architecture will be delved into understanding their operation better.
1.5.4 General Features of Existing Combined Platforms
A combined platform’s construction requires a high level of specialization in various scientific areas such as electronic control, mechanical design, and ergonomics [217]. The joint work of these different areas for the assembly of robotic devices for gait assistance and rehabilitation has advantages over conventional devices. It offers the user the opportunity to move autonomously, increasing his motivation and improving his physical capacities [7, 199, 218].
Some robotic devices such as exoskeletons and smart walkers, which are shown in Fig. 1.7, have presented promising results since they are equipped with different types of electronic sensors, such as kinematic sensors (angular position, speed, and acceleration) and kinetic (interaction force between the limb and each robotic device), which allow collecting relevant information to know the user’s evolution or to control the robotic device [219,220,221]. This last idea has become an innovative feature implemented by some existing robotic devices, ensuring better controllability by analyzing biosignals such as EEG and sEMG for human motion intention detection [199, 218].

Illustration of the most common robotic devices that make up the currently existing combined platforms. (a) Robotic lower-limb exoskeleton. (b) Smart robotic walker
That is why, considering the electronic operation and potential of these robotic devices, most of the existing combined platforms for mobility assistance and gait rehabilitation integrate an exoskeleton and a smart walker. On a mechanical level, as shown in Fig. 1.7a, exoskeletons are designed for the lower extremities, providing the ability to assist and support the gait process. Depending on the pathological conditions or the needs of each user, the exoskeletons can be unilateral or bilateral. Besides, the ergonomic design allows them to be adapted according to each user’s anthropometry [219, 221].
On the other hand, most smart walkers, as shown in Fig. 1.7b, have been developed on mobile platforms, allowing to guarantee a gait pattern that is as natural as possible [110, 218, 222]. Furthermore, considering that its movement is carried out on wheels, less force must be exerted to move it, since no lifting is necessary [110, 218, 223, 224]. However, since the wheels can run freely, this type of walker requires from the user better control and a good balance [110, 218, 223,224,225].
These general mechanical and electronic aspects make integrating two or more than two robotic assistive devices a potential, innovative, and affordable solution to help people with motor disabilities regain or compensate for the loss of motor control. Although most existing combined platforms for gait rehabilitation integrate an exoskeleton and a robotic walker, rapid advances in the technology area will make it possible in the short term to innovate and integrate new platforms with different devices that are increasingly lighter, smarter, more sophisticated, and aesthetically pleasing.
1.6 Scope of the Book
This book is organized in 13 thematic chapters (Chaps. 2 – 14 ), addressing relevant robotic technologies that have been integrated into healthcare and physical training environments to provide gait assistance and rehabilitation. Chapter 2 introduces the basic concepts of kinematic modelling, actuation systems, and sensing architectures of the different type of robotic devices here explained: lower-limb exoskeletons, social robots, and smart walkers. That chapter reviews the most common configurations for both commercial and research devices on the field.
Chapter 3 introduces the design process for lower-limb exoskeletons, from which the main modules and considerations of design can be extracted to analyze all other robotic devices presented. Through the definition of user-centered and device-centered features, the platforms are broken down into several modules that are addressed in the next chapters.
Similarly, Chap. 4 explores the design of smart walkers. From physical structures to sensory interfaces and control strategies, that chapter presents the different smart walkers developed until now, and their main characteristics.
Chapter 5 describes some of the most relevant spatial and temporal indicators that are used to characterize human gait, and therefore, track and report a patient’s rehabilitation progress, and detect anomalies in their gait patterns. That chapter also presents some wearable sensors that allow the acquisition of such indicators and methodologies that make use of them to develop high-level controllers in wearable and mobile robotic devices.
Chapter 6 focuses on the module of actuators, specifically in the area of flexible and soft actuators for the development of assistive robotic devices. It presents the steps involved in their characterization and the understanding of their capacities and limitations to correctly implement them in assistive and rehabilitation applications. The chapter finishes with concrete examples of robotics devices that include each type of actuation.
Chapter 7 centers in the field of flexible actuators and presents an overview of the variable stiffness actuators in terms of their principles, setups, and characteristics. The chapter introduces T-FLEX, an ankle exoskeleton based on this technology, and shows two preliminary case studies with healthy participants using this device.
Having the sensor and actuator modules explained. Chap. 8 explores control strategies in lower-limb exoskeletons. Two controllers are developed for the AGoRA exoskeleton based on the principle of impedance, as methodologies for gait assistance. The controllers are implemented in two case studies.
Chapter 9 introduces the relevance of using the Brain–Computer Interface for neurorehabilitation and the stages in the universal design of a BCI system. That chapter also analyzes some of the most relevant works related to BCI-based control for lower-limb exoskeletons. Finally, a study case of a stroke survivor commanding T-FLEX through a BCI interface is presented.
Similar to Chap. 8 , Chap. 10 presents control strategies for smart walkers. These strategies contemplate smart walkers’ interaction with both humans and the environment and allow smart walkers to respond to the user’s movement intentions, to guide a user between two points or along a trajectory, among many others behaviors.
Chapter 11 explores the incorporation of socially assistive robotics to gait rehabilitation scenarios. That chapter provides an introduction to the benefits of including social interaction in rehabilitation processes, through relevant characteristics of social robotics and their role in patient-robot interfaces.
Chapter 12 introduces one of the new trends in this challenging field of rehabilitation robotics. Serious games in robot-assisted therapies are covered in terms of their interaction technology and feedback and incentive strategies. That chapter presents the development of Jumping Guy, a serious game for ankle rehabilitation therapy with T-FLEX.
After understanding of the different modules and strategies available in the robotic devices, Chap. 13 addresses the methods, metrics, and equipment used to assess their performance in gait assistance and rehabilitation scenarios. It starts by explaining the basic concepts to characterize a motor skill and finishes with practical examples of assessments in the field.
Finally, Chap. 14 is devoted to the compilation and evaluation of the experiences of clinicians using the rehabilitation robotics presented along the book. That chapter collects several techniques that can be used to analyze clinicians and patients opinions and to quantify this qualitative information. The book concludes with an analysis of the importance of using these techniques and the new opportunities that arise for robotics in rehabilitation and clinical programs.
References
C.L. Vaughan, Theories of bipedal walking: an odyssey. J. Biomech. 36, 513–523 (2003)
W. Pirker, R. Katzenschlager, Gait disorders in adults and the elderly. Wien. klin. Wochenschr. 129, 81–95 (2017)
L.M. Decker, F. Cignetti, N. Stergiou, Complexity and human gait. Rev. Andal. Med. Deport. 3(1), 2–12 (2010)
A.S. Buchman, P.A. Boyle, S.E. Leurgans, L.L. Barnes, D.A. Bennett, Cognitive function is associated with the development of mobility impairments in community-dwelling elders. Am. J. Geriatr. Psychiatry 19(6), 571–580 (2011)
É. Watelain, Human gait: from clinical gait analysis to diagnosis assistance. Mov. Sport Sci. 98(4), 3 (2017)
K.E. Adolph, W.G. Cole, M. Komati, J.S. Garciaguirre, D. Badaly, J.M. Lingeman, G.L.Y. Chan, R.B. Sotsky, How do you learn to walk? Thousands of steps and dozens of falls per day. Psychol. Sci. 23, 1387–1394 (2012)
A. Kuo, M. Donelan, Dynamic principles of gait and their clinical implications. Phys. Ther. 90, 157–174 (2009)
Z.O. Abu-Faraj, G.F. Harris, P.A. Smith, S. Hassani, Human gait and clinical movement analysis, in Wiley Encyclopedia of Electrical and Electronics Engineering (Wiley, Hoboken, 2015), pp. 1–34
C. Vaughan, B. Davis, J. O’Connor, The three-dimensional and cyclic nature of gait, in Dynamics of Human Gait, vol. 168 (Kiboho Publishers, Cape Town, 1999), pp. 16–17
J. Perry, J.R. Davids et al., Gait analysis: normal and pathological function. J. Pediatr. Orthop. 12(6), 815 (1992)
J.R. Gage, Gait analysis. An essential tool in the treatment of cerebral palsy. Clin. Orthop. Relat. Res. 288, 126–134 (1993)
M.W. Whittle, Clinical gait analysis: a review. Hum. Mov. Sci. 15(3), 369–387 (1996)
R. Hicks, S. Tashman, J. Cary, R. Altman, J. Gage, Swing phase control with knee friction in juvenile amputees. J. Orthop. Res. 3(2), 198–201 (1985)
S. Tashman, R. Hicks, D. Jendrzejczyk, Evaluation of a prosthetic shank with variable inertial properties. Clin. Prosthet. Orthot. 9(3), 23–28 (1985)
I. Carrera, H.A. Moreno, S. Sierra, A. Campos, M. Munera, C.A. Cifuentes, Technologies for therapy and assistance of lower limb disabilities: sit to stand and walking, in Exoskeleton Robots for Rehabilitation and Healthcare Devices, chap. 4 (Springer, Berlin, 2020), pp. 43–66
S. Schmid, K. Schweizer, J. Romkes, S. Lorenzetti, R. Brunner, Secondary gait deviations in patients with and without neurological involvement: a systematic review. Gait Posture 37, 480–493 (2013).
M. Roberts, D. Mongeon, F. Prince, Biomechanical parameters for gait analysis: a systematic review of healthy human gait. Phys. Ther. Rehabil. 4(1), 6 (2017)
C.A. Cifuentes, A. Frizera, Human-Robot Interaction Strategies for Walker-Assisted Locomotion. Springer Tracts in Advanced Robotics, vol. 115 (Springer International Publishing, Cham, 2016)
A.H. Snijders, B.P. van de Warrenburg, N. Giladi, B.R. Bloem, Neurological gait disorders in elderly people: clinical approach and classification. Lancet Neurol. 6(1), 63–74 (2007)
R. Gheno, J. Cepparo, C. Rosca, A. Cotten, Musculoskeletal disorders in the elderly. J. Clin. Imaging Sci. 2(3), 39 (2012)
MedlinePlus, Bone diseases (2016). https://medlineplus.gov/bonediseases.html
S.N. Nabili, C.P. Davis, Senior health: successful aging (2019)
Disabled World, Physical and Mobility Impairment: Information & News (2019). https://www.disabled-world.com/disability/types/mobility/
G. Sammer, T. Uhlmann, W. Unbehaun, A. Millonig, B. Mandl, J. Dangschat, R. Mayr, Identification of mobility-impaired persons and analysis of their travel behavior and needs. Transp. Res. Rec. J. Transp. Res. Board 2320, 46–54 (2012)
T. Mikolajczyk, I. Ciobanu, D.I. Badea, A. Iliescu, S. Pizzamiglio, T. Schauer, T. Seel, P.L. Seiciu, D.L. Turner, M. Berteanu, Advanced technology for gait rehabilitation: an overview. Adv. Mech. Eng. 10, 168781401878362 (2018)
National Health Service UK, Physiotherapy (2018). https://www.nhs.uk/conditions/physiotherapy/
S. Sierra, L. Arciniegas, F. Ballen-Moreno, D. Gomez-Vargas, M. Munera, C.A. Cifuentes, Adaptable robotic platform for gait rehabilitation and assistance: design concepts and applications, in Exoskeleton Robots for Rehabilitation and Healthcare Devices (Springer, Berlin, 2020), pp. 67–93
S.L. Chaparro-Cárdenas, A.A. Lozano-Guzmán, J.A. Ramirez-Bautista, A. Hernández-Zavala, A review in gait rehabilitation devices and applied control techniques. Disabil. Rehabil. Assist. Technol. 13(8), 819–834 (2018)
R.A. States, E. Pappas, Y. Salem, Overground physical therapy gait training for chronic stroke patients with mobility deficits. Cochrane Database Syst. Rev. 2009(3), CD006075 (2009)
A. Pollock, G. Baer, P. Campbell, P.L. Choo, A. Forster, J. Morris, V.M. Pomeroy, P. Langhorne, Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst. Rev. 2014(4), CD001920 (2014)
L.R. Sheffler, J. Chae, Technological advances in interventions to enhance poststroke gait. Phys. Med. Rehabil. Clin. N. Am. 24, 305–323 (2013)
S. Haddadin, E. Croft, Physical human–robot interaction, in Springer Handbook of Robotics (Springer International Publishing, Cham, 2016), pp. 1835–1874
A.Q. Keemink, H. van der Kooij, A.H. Stienen, Admittance control for physical human–robot interaction. Int. J. Robot. Res. 37, 1421–1444 (2018)
ISO 13482:2014(en) Robots and robotic devices — Safety requirements for personal care robots (2014). https://www.iso.org/obp/ui/#iso:std:iso:13482:ed-1:v1:en
ISO 22523:2006 External limb prostheses and external orthoses - Requirements and test methods (2006). https://www.iso.org/standard/37546.html
J.F. Veneman, Wearable robotics: challenges and trends, in Challenges and Trends. Biosystems & Biorobotics (2016), pp. 189–193
L. Bueno, F. Brunetti, A. Frizera, J.L. Pons, J.C. Moreno, E. Rocon, J.M. Carmena, E. Farella, L. Benini, Human–robot cognitive interaction, in Wearable Robots (Wiley, Chichester, 2008), pp. 87–125
E. Bionics, EVO (2020). https://eksobionics.com/ekso-evo/
Lockheed Martin, FORTIS (2014). https://www.lockheedmartin.com/en-us/products/exoskeleton-technologies/industrial.html
R. Alturkistani, A. Kavin, S. Devasahayam, R. Thomas, E.L. Colombini, C.A. Cifuentes, S. Homer-Vanniasinkam, H.A. Wurdemann, M. Moazen, Affordable passive 3D-printed prosthesis for persons with partial hand amputation. Prosthet. Orthot. Int. 44(2), 92–98 (2020)
H. Lee, P.W. Ferguson, J. Rosen, Lower limb exoskeleton systems—overview, in Wearable Robotics, Chap. 11 (Academic, London, 2020)
R. Bionics, REX (2019). https://www.rexbionics.com/
D. Gomez-Vargas, F. Ballen-Moreno, P. Barria, R. Aguilar, J.M. Azorín, M. Múnera, C.A. Cifuentes, The actuation system of the ankle exoskeleton T-FLEX: first use experimental validation in people with stroke. Brain Sci. 11(4), 412 (2021)
A. Peñas, J. Maldonado, O. Ramos, M. Munera, P. Barria, M. Moazen, H.A. Wurdemann, C.A. Cifuentes, Towards a fabric-based soft hand exoskeleton for various grasp taxonomies, in The International Symposium on Wearable Robotics (WeRob2020) and WearRAcon Europe (2020)
J. Beil, C. Marquardt, T. Asfour, Self-aligning exoskeleton hip joint: kinematic design with five revolute, three prismatic and one ball joint. IEEE Int. Conf. Rehabil. Robot. 2017, 1349–1355 (2017)
F. Ballen-Moreno, C. Cifuentes, T. Provot, M. Bourgain, M. Munera, 3D relative motion assessment in lower-limb exoskeletons: a case of study with AGoRA exoskeleton, in The International Symposium on Wearable Robotics (WeRob2020) and WearRAcon Europe (2020)
A.F. Ruiz, A. Forner-Cordero, E. Rocon, J.L. Pons, Exoskeletons for rehabilitation and motor control, in Proceedings of the First IEEE/RAS-EMBS International Conference on Biomedical Robotics and Biomechatronics, 2006, BioRob 2006, vol. 2006 (2006), pp. 601–606
K. Schmidt, J.E. Duarte, M. Grimmer, A. Sancho-Puchades, H. Wei, C.S. Easthope, R. Riener, The Myosuit: bi-articular anti-gravity exosuit that reduces hip extensor activity in sitting transfers. Front. Neurorobot. 11, 1–16 (2017)
P. Cherelle, V. Grosu, P. Beyl, A. Mathys, R. Van Ham, M. Van Damme, B. Vanderborght, D. Lefeber, The MACCEPA actuation system as torque actuator in the gait rehabilitation robot ALTACRO, in 2010 3rd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (IEEE, Piscataway, 2010), pp. 27–32
W. Huo, S. Mohammed, J.C. Moreno, Y. Amirat, Lower limb wearable robots for assistance and rehabilitation: a state of the art. IEEE Syst. J. 10, 1–14 (2016)
M. Bortole, A. del Ama, E. Rocon, J.C. Moreno, F. Brunetti, J.L. Pons, A robotic exoskeleton for overground gait rehabilitation, in 2013 IEEE International Conference on Robotics and Automation (IEEE, Piscataway, 2013), pp. 3356–3361
A. Schiele, F.C. van der Helm, Influence of attachment pressure and kinematic configuration on pHRI with wearable robots. Appl. Bionics Biomech. 6(2), 157–173 (2009)
R. Alami, A. Albu-Schaeffer, A. Bicchi, R. Bischoff, R. Chatila, A. De Luca, A. De Santis, G. Giralt, J. Guiochet, G. Hirzinger, F. Ingrand, V. Lippiello, R. Mattone, D. Powell, S. Sen, B. Siciliano, G. Tonietti, L. Villani, Safe and dependable physical human-robot interaction in anthropic domains: state of the art and challenges, in IEEE International Conference on Intelligent Robots and Systems (2006)
E. Pirondini, M. Coscia, S. Marcheschi, G. Roas, F. Salsedo, A. Frisoli, M. Bergamasco, S. Micera, Evaluation of the effects of the Arm Light Exoskeleton on movement execution and muscle activities: a pilot study on healthy subjects. J. NeuroEng. Rehabil. 13(1), 1–21 (2016)
L.F. Aycardi, C.A. Cifuentes, M. Múnera, C. Bayón, O. Ramírez, S. Lerma, A. Frizera, E. Rocon, Evaluation of biomechanical gait parameters of patients with Cerebral Palsy at three different levels of gait assistance using the CPWalker. J. NeuroEng. Rehabil. 16, 15 (2019)
M. Pazzaglia, M. Molinari, The embodiment of assistive devices-from wheelchair to exoskeleton. Phys. Life Rev. 16, 163–175 (2016)
J.T. Meyer, S.O. Schrade, O. Lambercy, R. Gassert, User-centered design and evaluation of physical interfaces for an exoskeleton for paraplegic users, in 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR) (2019), pp. 1159–1166
D. Torricelli, C. Rodriguez-Guerrero, J.F. Veneman, S. Crea, K. Briem, B. Lenggenhager, P. Beckerle, Benchmarking wearable robots: challenges and recommendations from functional, user experience, and methodological perspectives. Front. Robot. AI 7, 168 (2020)
Ossur, Proprio foot. https://www.ossur.com/en-us/prosthetics/feet/proprio-foot
Ottobock, Empower (2020). https://www.ottobockus.com/products/empower-ankle/
A. Esquenazi, M. Talaty, A. Packel, M. Saulino, The ReWalk powered exoskeleton to restore ambulatory function to individuals with thoracic-level motor-complete spinal cord injury. Am. J. Phys. Med. Rehabil. 91(11), 911–921 (2012)
Myoswiss, Myosuit (2020). https://myo.swiss/myosuit/
L.I. Minchala, F. Astudillo-Salinas, K. Palacio-Baus, A. Vazquez-Rodas, Mechatronic design of a lower limb exoskeleton, in Design, Control and Applications of Mechatronic Systems in Engineering (2017)
B.J. Makinson, Research and development prototype for machine augmentation of human strength and endurance. Hardiman I Project (1971)
H. Kim, Y.J. Shin, J. Kim, Kinematic-based locomotion mode recognition for power augmentation exoskeleton. Int. J. Adv. Robot. Syst. 14(5), 1–14 (2017)
S. Galle, P. Malcolm, S.H. Collins, D. De Clercq, Reducing the metabolic cost of walking with an ankle exoskeleton: interaction between actuation timing and power. J. NeuroEng. Rehabil. 14(1), 1–16 (2017)
L.M. Mooney, H.M. Herr, Biomechanical walking mechanisms underlying the metabolic reduction caused by an autonomous exoskeleton. J. NeuroEng. Rehabil. 13(1), 1–12 (2016)
G. Colombo, M. Joerg, R. Scheier, V. Dietz, Treadmill training of paraplegic patients using a robotic orthosis. Percept. Mot. Skills 73(1), 146 (2000)
A.C. Villa-Parra, D. Delisle-Rodriguez, T. Botelho, J.J.V. Mayor, A.L. Delis, R. Carelli, A. Frizera Neto, T.F. Bastos, Control of a robotic knee exoskeleton for assistance and rehabilitation based on motion intention from sEMG. Res. Biomed. Eng. 34(3), 198–210 (2018)
T. Bacek, M. Moltedo, K. Langlois, G.A. Prieto, M.C. Sanchez-Villamañan, J. Gonzalez-Vargas, B. Vanderborght, D. Lefeber, J.C. Moreno, BioMot exoskeleton - towards a smart wearable robot for symbiotic human-robot interaction. IEEE Int. Conf. Rehabil. Robot. 2017, 1666–1671 (2017)
E. Bionics, Ekso GT. https://eksobionics.com/
J. Choi, B. Na, P.-G. Jung, D.-w. Rha, K. Kong, Walkon suit: a medalist in the powered exoskeleton race of Cybathlon 2016. IEEE Robot. Autom. Mag. 24(4), 75–86 (2017)
S.O. Schrade, K. Dätwyler, M. Stücheli, K. Studer, D.A. Türk, M. Meboldt, R. Gassert, O. Lambercy, Development of VariLeg, an exoskeleton with variable stiffness actuation: first results and user evaluation from the CYBATHLON 2016 Olivier Lambercy; Roger Gassert. J. NeuroEng. Rehabil. 15(1), 1–18 (2018)
B. Chen, H. Ma, L.-Y. Qin, F. Gao, K.-M. Chan, S.-W. Law, L. Qin, W.-H. Liao, Recent developments and challenges of lower extremity exoskeletons. J. Orthop. Translat. 5, 26–37 (2016)
J.D. Schaechter, Motor rehabilitation and brain plasticity after hemiparetic stroke. Prog. Neurobiol. 73(1), 61–72 (2004)
G. Chen, C.K. Chan, Z. Guo, H. Yu, A review of lower extremity assistive robotic exoskeletons in rehabilitation therapy. Crit. Rev. Biomed. Eng. 41(4–5), 343–363 (2013)
R.S. Calabró, A. Naro, M. Russo, P. Bramanti, L. Carioti, T. Balletta, A. Buda, A. Manuli, S. Filoni, A. Bramanti, Shaping neuroplasticity by using powered exoskeletons in patients with stroke: a randomized clinical trial. J. Neuroeng. Rehabil. 15(1), 35 (2018)
B. Koopman, E.H. van Asseldonk, H. van der Kooij, Selective control of gait subtasks in robotic gait training: foot clearance support in stroke survivors with a powered exoskeleton. J. NeuroEng. Rehabil. 10(1), 3 (2013)
L.D. da Silva, T.F. Pereira, V.R. Leithardt, L.O. Seman, C.A. Zeferino, Hybrid impedance-admittance control for upper limb exoskeleton using electromyography. Appl. Sci. (Switzerland) 10(20), 1–19 (2020)
E. Fosch-Villaronga, B. Ozcan, The progressive intertwinement between design, human needs and the regulation of care technology: the case of lower-limb exoskeletons. Int. J. Soc. Robot. 12, 959–972 (2020)
C. Bayon, R. Raya, S. Lerma Lara, O. Ramirez, J.I. Serrano, E. Rocon, Robotic therapies for children with cerebral palsy: a systematic review. Transl. Biomed. 7(1), 44 (2016)
S. Banala, S.H. Kim, S. Agrawal, J. Scholz, Robot assisted gait training with active leg exoskeleton (ALEX). IEEE Trans. Neural Syst. Rehabil. Eng. 17, 2–8 (2009)
R. Ekkelenkamp, J. Veneman, H. van der Kooij, LOPES: a lower extremity powered exoskeleton, in Proceedings 2007 IEEE International Conference on Robotics and Automation (IEEE, Piscataway, 2007), pp. 3132–3133
M.D. Sánchez-Manchola, M.J. Bernal, M. Munera, C.A. Cifuentes, Gait phase detection for lower-limb exoskeletons using foot motion data from a single inertial measurement unit in hemiparetic individuals. Sensors (Switzerland) 19(13), 2988 (2019)
C. Di Natali, T. Poliero, M. Sposito, E. Graf, C. Bauer, C. Pauli, E. Bottenberg, A. De Eyto, L. O’sullivan, A.F. Hidalgo, D. Scherly, K.S. Stadler, D.G. Caldwell, J. Ortiz, Design and evaluation of a soft assistive lower limb exoskeleton. Robotica 37(12), 2014–2034 (2019)
B. Brackx, V. Grosu, D. Lefeber, ALTACRO: design of the gait rehabilitation robot, in Symposium on Robot-Assisted Gait Rehabilitation (ALTACRO) (2013)
J.F. Veneman, R. Kruidhof, E.E. Hekman, R. Ekkelenkamp, E.H. Van Asseldonk, H. Van Der Kooij, Design and evaluation of the LOPES exoskeleton robot for interactive gait rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 15(3), 379–386 (2007)
S.K. Banala, S.K. Agrawal, J. Scholz, Active leg exoskeleton (ALEX) for gait rehabilitation of motor-impaired patients, in 2007 IEEE 10th International Conference on Rehabilitation Robotics (2007), pp. 401–407
C.R. Salvatore, A. Cacciola, F. Berté, A. Manuli, A. Leo, A. Bramanti, A. Naro, D. Milardi, P. Bramanti, Robotic gait rehabilitation and substitution devices in neurological disorders: where are we now?. Neurol. Sci. 37(4), 503–514 (2016)
K. Han, J. Lee, W.K. Song, Application scenarios for assistive robots based on in-depth focus group interviews and clinical expert meetings, in 2013 44th International Symposium on Robotics, ISR 2013, no. C (2013)
A.B. Zoss, H. Kazerooni, A. Chu, Biomechanical design of the Berkeley Lower Extremity Exoskeleton (BLEEX). IEEE/ASME Trans. Mechatron. 11(2), 128–138 (2006)
C. Velandia, H. Celedon, D.A. Tibaduiza, C. Torres-Pinzon, J. Vitola, Design and control of an exoskeleton in rehabilitation tasks for lower limb, in 2016 21st Symposium on Signal Processing, Images and Artificial Vision, STSIVA 2016 (2016), pp. 1–6
M. Cempini, S.M.M. De Rossi, T. Lenzi, N. Vitiello, M.C. Carrozza, Self-alignment mechanisms for assistive wearable robots: a kinetostatic compatibility method. IEEE Trans. Robot. 29(1), 236–250 (2013)
A.C. Villa-Parra, D. Delisle-Rodriguez, J.S. Lima, A. Frizera-Neto, T. Bastos, Knee impedance modulation to control an active orthosis using insole sensors. Sensors (Switzerland) 17(12), 2751 (2017)
B. Chen, C.H. Zhong, X. Zhao, H. Ma, X. Guan, X. Li, F.Y. Liang, J.C.Y. Cheng, L. Qin, S.W. Law, W.H. Liao, A wearable exoskeleton suit for motion assistance to paralysed patients. J. Orthop. Translat. 11, 7–18 (2017)
R. Steger, S.H. Kim, H. Kazerooni, Control scheme and networked control architecture for the Berkeley Lower Extremity Exoskeleton (BLEEX), in Proceedings - IEEE International Conference on Robotics and Automation, vol. 2006, May 2006, pp. 3469–3476
H. Kazerooni, R. Steger, L. Huang, Hybrid control of the Berkeley Lower Extremity Exoskeleton (BLEEX). Int. J. Rob. Res. 25(5–6), 561–573 (2006)
T. Poliero, C. Di Natali, M. Sposito, J. Ortiz, E. Graf, C. Pauli, E. Bottenberg, A. De Eyto, D.G. Caldwell, Soft wearable device for lower limb assistance: assessment of an optimized energy efficient actuation prototype. 2018 IEEE International Conference on Soft Robotics, RoboSoft 2018 (2018), pp. 559–564
J.E. Duarte, K. Schmidt, R. Riener, J.E. Duarte, K. Schmidt, R. Riener, J.E. Duarte, K. Schmidt, R. Riener, The Myosuit : textile-powered mobility The Myosuit : Myosuit : textile-powered. IFAC-PapersOnLine 51(34), 242–243 (2019)
F.L. Haufe, A.M. Kober, K. Schmidt, A. Sancho-puchades, J.E. Duarte, P. Wolf, R. Riener, User-driven walking assistance: first experimental results using the MyoSuit ∗, in 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR) (2019), pp. 944–949
Indego, Indego Exoskeleton (2012). http://www.indego.com/indego/us/en/home
C.E. Zurich, CYBATHLON (2020). https://cybathlon.ethz.ch/en
M. Talaty, A. Esquenazi, J.E. Briceno, Differentiating ability in users of the ReWalkTM powered exoskeleton: an analysis of walking kinematics. IEEE Int. Conf. Rehabil. Robot. 2013, 6650469 (2013)
S.O. Schrade, Y. Nager, A.R. Wu, R. Gassert, A. Ijspeert, Bio-inspired control of joint torque and knee stiffness in a robotic lower limb exoskeleton using a central pattern generator. Int. Conf. Rehabil. Robot. 2017, 1387–1394 (2017)
A. Roy, H.I. Krebs, S.L. Patterson, T.N. Judkins, I. Khanna, L.W. Forrester, R.M. Macko, N. Hogan, Measurement of human ankle stiffness using the anklebot, in 2007 IEEE 10th International Conference on Rehabilitation Robotics, ICORR’07, vol. 00, no. c (2007), pp. 356–363
H. Bateni, B.E. Maki, Assistive devices for balance and mobility: Benefits, demands, and adverse consequences. Arch. Phys. Med. Rehabil. 86(1), 134–145 (2005)
S.D. Sierra M., M. Garzón, M. Múnera, C.A. Cifuentes, Human–robot–environment interaction interface for smart walker assisted gait: AGoRA walker. Sensors 19, 2897 (2019)
F.W. Van Hook, D. Demonbreun, B.D. Weiss, Ambulatory devices for chronic gait disorders in the elderly. Am. Fam. Physician 67(8), 1717–1724 (2003)
R. Constantinescu, C. Leonard, C. Deeley, R. Kurlan, Assistive devices for gait in Parkinson’s disease. Parkinsonism Relat. Disord. 13, 133–138 (2007)
M. Martins, C. Santos, A. Frizera, R. Ceres, Assistive mobility devices focusing on smart walkers: classification and review. Rob. Auton. Syst. 60, 548–562 (2012)
M. Amboni, P. Barone, J.M. Hausdorff, Cognitive contributions to gait and falls: evidence and implications. Mov. Disord. 28, 1520–1533 (2013)
M. Montero-Odasso, J. Verghese, O. Beauchet, J.M. Hausdorff, Gait and cognition: a complementary approach to understanding brain function and the risk of falling. J. Am. Geriatr. Soc. 60, 2127–2136 (2012)
W.M. Scheidegger, R.C. de Mello, S.D. Sierra M., M.F. Jimenez, M.C. Munera, C.A. Cifuentes, A. Frizera-Neto, A novel multimodal cognitive interaction for walker-assisted rehabilitation therapies, in 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR) (IEEE, Piscataway, 2019), pp. 905–910
J.-M. Belda-Lois, S. Mena-del Horno, I. Bermejo-Bosch, J.C. Moreno, J.L. Pons, D. Farina, M. Iosa, M. Molinari, F. Tamburella, A. Ramos, A. Caria, T. Solis-Escalante, C. Brunner, M. Rea, Rehabilitation of gait after stroke: a review towards a top-down approach. J. NeuroEng. Rehabil. 8(1), 66 (2011)
A. Aguirre, S.D. Sierra M., M. Munera, C.A. Cifuentes, Online system for gait parameters estimation using a LRF sensor for assistive devices. IEEE Sens. J. 1 (2020). https://doi.org/10.1109/JSEN.2020.3028279
J. Ballesteros, C. Urdiales, A.B. Martinez, M. Tirado, Online estimation of rollator user condition using spatiotemporal gait parameters, in International Conference on Intelligent Robots and Systems (IROS) (2016), pp. 3180–3185
C.A. Cifuentes, C. Rodriguez, A. Frizera, T. Bastos, Sensor Fusion to control a robotic walker based on upper-limbs reaction forces and gait kinematics. in 5th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (2014), pp. 1098–1103
M.F. Jiménez, M. Monllor, A. Frizera, T. Bastos, F. Roberti, R. Carelli, Admittance controller with spatial modulation for assisted locomotion using a smart walker. J. Intell. Robot. Syst. 94(7), 1–17 (2019)
S.F.R. Alves, J.M. Rosario, H. Ferasoli, L.K.A. Rincon, R.A.T. Yamasaki, Conceptual bases of robot navigation modeling, control and applications, in Advances in Robot Navigation (InTech, London, 2011)
A. Wachaja, P. Agarwal, M. Zink, M.R. Adame, K. Möller, W. Burgard, Navigating blind people with walking impairments using a smart walker. Auton. Robot. 41, 555–573 (2017)
M. Martins, C. Santos, A. Frizera, R. Ceres, A review of the functionalities of smart walkers. Med. Eng. Phys. 37, 917–928 (2015)
M. Belas Dos Santos, C. Barros de Oliveira, A. Dos Santos, C. Garabello Pires, V. Dylewski, R.M. Arida, A comparative study of conventional physiotherapy versus robot-assisted gait training associated to physiotherapy in individuals with ataxia after stroke. Behav. Neurol. 2018, 2892065 (2018)
S.D. Sierra, M.F. Jimenez, M.C. Munera, A. Frizera-Neto, C.A. Cifuentes, Remote-operated multimodal interface for therapists during walker-assisted gait rehabilitation: a preliminary assessment, in 2019 14th ACM/IEEE International Conference on Human-Robot Interaction (HRI) (IEEE, Piscataway, 2019), pp. 528–529
G.J. Lacey, D. Rodriguez-Losada, The evolution of Guido. IEEE Robot. Autom. Mag. 15(4), 75–83 (2008)
C. Huang, G. Wasson, M. Alwan, P. Sheth, Shared navigational control and user intent detection in an intelligent walker, in AAAI Fall 2005 (2005)
A.F. Neto, A. Elias, C.A. Cifuentes, C. Rodriguez, T. Bastos, R. Carelli, Smart walkers: advanced robotic human walking-aid systems, in Intelligent Assistive Robots. Springer Tracts in Advanced Robotics (Springer, Berlin, 2015), pp. 103–131
W.-H. Mou, M.-F. Chang, C.-K. Liao, Y.-H. Hsu, S.-H. Tseng, L.-C. Fu, Context-aware assisted interactive robotic walker for Parkinson’s disease patients, in 2012 IEEE/RSJ International Conference on Intelligent Robots and Systems (IEEE, Piscataway, 2012), pp. 329–334
T. Hellström, O. Lindahl, T. Bäcklund, M. Karlsson, P. Hohnloser, A. Bråndal, X. Hu, P. Wester, An intelligent rollator for mobility impaired persons, especially stroke patients. J. Med. Eng. Technol. 40, 270–279 (2016)
K.-H. Cho, S. Pyo, G.-S. Shin, S.-D. Hong, S.-H. Lee, D. Lee, S. Song, G. Lee, A novel one arm motorized walker for hemiplegic stroke survivors: a feasibility study. BioMed. Eng. OnLine 17, 14 (2018)
D. Chugo, T. Asawa, T. Kitamura, S. Jia, K. Takase, A moving control of a robotic walker for standing, walking and seating assistance, in 2008 IEEE International Conference on Robotics and Biomimetics (IEEE, Piscataway, 2009), pp. 692–697
C. Werner, M. Geravand, P.Z. Korondi, A. Peer, J.M. Bauer, K. Hauer, Evaluating the sit-to-stand transfer assistance from a smart walker in older adults with motor impairments. Geriatr. Gerontol. Int. 20, 312–316 (2020)
L. Palopoli, A. Argyros, J. Birchbauer, A. Colombo, D. Fontanelli, A. Legay, A. Garulli, A. Giannitrapani, D. Macii, F. Moro, P. Nazemzadeh, P. Padeleris, R. Passerone, G. Poier, D. Prattichizzo, T. Rizano, L. Rizzon, S. Scheggi, S. Sedwards, Navigation assistance and guidance of older adults across complex public spaces: the DALi approach. Intell. Serv. Robot. 8, 77–92 (2015)
J. Leaman, H.M. La, A comprehensive review of smart wheelchairs: past, present, and future. IEEE Trans. Hum. Mach. Syst. 47, 486–499 (2017)
R. Bostelman, J. Albus, Robotic patient lift and transfer, in Service Robot Applications (InTech, London, 2008)
B.R. Duffy, C.F.B. Rooney, G.M.P.O. Hare, R.P.S.O. Donoghue, What is a social robot? Computer 1–3 (1999)
F. Hegel, C. Muhl, B. Wrede, M. Hielscher-Fastabend, G. Sagerer, Understanding social robots, in 2009 Second International Conferences on Advances in Computer-Human Interactions, pp. 169–174 (IEEE, Piscataway, 2009)
T. Fong, I. Nourbakhsh, K. Dautenhahn, A survey of socially interactive robots: concepts, design and applications. Des. Appl. Robot. Auton. Syst. 42(3), 142–166 (2002)
C. Bartneck, J. Forlizzi, A design-centred framework for social human-robot interaction, in RO-MAN (2004), pp. 591–594
C. Breazeal, Designing Sociable Robots (The MIT Press, Cambridge, 2018)
T.S. Dahl, M.N.K. Boulos, Robots in health and social care: a complementary technology to home care and telehealthcare? Robotics 3(1), 1–21 (2014)
C.A. Cifuentes, M.J. Pinto, N. Céspedes, M. Múnera, Social robots in therapy and care, in Current Robotics Reports (2020), pp. 1–16
T. Dahl, M. Kamel Boulos, Robots in health and social care: a complementary technology to home care and telehealthcare?, in Robotics (MDPI, ISSN 2218-6581), vol. 3 (2014), pp. 1–21
I. Leite, C. Martinho, A. Paiva, Social robots for long-term interaction: a survey. Int. J. Soc. Robot. 5(2), 291–308 (2013)
O.A. Henkemans, B.P. Bierman, J. Janssen, R. Looije, M.A. Neerincx, M.M. van Dooren, J.L. de Vries, G.J. van der Burg, S.D. Huisman, Design and evaluation of a personal robot playing a self-management education game with children with diabetes type 1. Int. J. Hum. Comput. Stud. 106, 63–76 (2017)
R. Looije, M.A. Neerincx, J.K. Peters, O.A. Henkemans, Integrating robot support functions into varied activities at returning hospital visits: supporting child’s self-management of diabetes. Int. J. Soc. Robot. 8(4), 483–497 (2016)
S.S. Yun, J.S. Choi, S.K. Park, G.Y. Bong, H.J. Yoo, Social skills training for children with autism spectrum disorder using a robotic behavioral intervention system. Autism Res. 10(7), 1306–1323 (2017)
Z. Zheng, H. Zhao, A.R. Swanson, A.S. Weitlauf, Z.E. Warren, N. Sarkar, Design, development, and evaluation of a noninvasive autonomous robot-mediated joint attention intervention system for young children with ASD. IEEE Trans. Hum. Mach. Syst. 48(2), 125–135 (2018)
L.J. Wood, B. Robins, G. Lakatos, D.S. Syrdal, A. Zaraki, K. Dautenhahn, Developing a protocol and experimental setup for using a humanoid robot to assist children with autism to develop visual perspective taking skills. Paladyn 10(1), 167–179 (2019)
A.A. Ramírez-Duque, T. Bastos, M. Munera, C.A. Cifuentes, A. Frizera-Neto, Robot-Assisted Intervention for children with special needs: a comparative assessment for autism screening. Robot. Auton. Syst. 127, 103484 (2020)
W.C. So, M.K.Y. Wong, C.K.Y. Lam, W.Y. Lam, A.T.F. Chui, T.L. Lee, H.M. Ng, C.H. Chan, D.C.W. Fok, Using a social robot to teach gestural recognition and production in children with autism spectrum disorders. Disabil. Rehabil. Assist. Technol. 13(6), 527–539 (2018)
D. Casas-Bocanegra, D. Gomez-Vargas, M.J. Pinto-Bernal, J. Maldonado, M. Munera, A. Villa-Moreno, M.F. Stoelen, T. Belpaeme, C.A. Cifuentes, An open-source social robot based on compliant soft robotics for therapy with children with ASD. Actuators 9(3), 1–22 (2020)
A. Ramirez-Duque, L. Aycardi, A. Villa, M. Munera, T. Freire, T. Belpaeme, A. Frizera, C.A. Cifuentes, Collaborative and inclusive process with the autism community: a case study in Colombia about social robot design. Int. J. Soc. Robot. 13(2), 153–167 (2021)
A. Peca, R. Simut, S. Pintea, B. Vanderborght, Are children with ASD more prone to test the intentions of the Robonova robot compared to a human? Int. J. Soc. Robot. 7(5), 629–639 (2015)
B. Vanderborght, R. Simut, J. Saldien, C. Pop, A.S. Rusu, S. Pintea, D. Lefeber, D.O. David, Using the social robot probo as a social story telling agent for children with ASD. Interact. Stud. 13(3), 348–372 (2012)
Y. Nakadoi, Usefulness of animal type robot assisted therapy for autism spectrum disorder in the child and adolescent psychiatric ward, in New Frontiers in Artificial Intelligence, ed. by M. Otake, S. Kurahashi, Y. Ota, K. Satoh, D. Bekki (Springer International Publishing, Cham, 2017), pp. 478–482
S. Jeong, D.E. Logan, M.S. Goodwin, S. Graca, B. O’Connell, H. Goodenough, L. Anderson, N. Stenquist, K. Fitzpatrick, M. Zisook, L. Plummer, C. Breazeal, P. Weinstock, A social robot to mitigate stress, anxiety, and pain in hospital pediatric care, in ACM/IEEE International Conference on Human-Robot Interaction, vol. 02, no. 1, March 2015, pp. 103–104
S. Jeong, C. Breazeal, D. Logan, P. Weinstock, Huggable: impact of embodiment on promoting verbal and physical engagement for young pediatric inpatients, in RO-MAN 2017 - 26th IEEE International Symposium on Robot and Human Interactive Communication, vol. 2017-Janua (2017), pp. 121–126
L.A. Jibb, K.A. Birnie, P.C. Nathan, T.N. Beran, V. Hum, J.C. Victor, J.N. Stinson, Using the MEDiPORT humanoid robot to reduce procedural pain and distress in children with cancer: a pilot randomized controlled trial. Pediatr. Blood Cancer 65(9), e27242 (2018)
N. Céspedes Gómez, A.V. Calderon Echeverria, M. Munera, E. Rocon, C.A. Cifuentes, First interaction assessment between a social robot and children diagnosed with cerebral palsy in a rehabilitation context, in Companion of the 2021 ACM/IEEE International Conference on Human-Robot Interaction, HRI ’21 Companion (Association for Computing Machinery, New York, 2021), pp. 484–488
T.N. Beran, A. Ramirez-Serrano, O.G. Vanderkooi, S. Kuhn, Humanoid robotics in health care: an exploration of children’s and parents’ emotional reactions. J. Health Psychol. 20(7), 984–989 (2015)
S. Rossi, M. Larafa, M. Ruocco, Emotional and behavioural distraction by a social robot for children anxiety reduction during vaccination. Int. J. Soc. Robot. 12(3), 765–777 (2020)
O. Korn, Social Robots: Technological, Societal and Ethical Aspects of Human-Robot Interaction (Springer, Berlin, 2019)
E. Martinez-Martin, A.P. del Pobil, Personal robot assistants for elderly care: an overview, in Personal Assistants: Emerging Computational Technologies (2018), pp. 77–91
W. Moyle, M. Bramble, C. Jones, J. Murfield, Care staff perceptions of a social robot called paro and a look-alike plush toy: a descriptive qualitative approach. Aging Ment. Health 22(3), 330–335 (2018)
M. Bajones, D. Fischinger, A. Weiss, D. Wolf, M. Vincze, P. de la Puente, T. Körtner, M. Weninger, K. Papoutsakis, D. Michel et al., Hobbit: providing fall detection and prevention for the elderly in the real world. J. Robot. 2018 (2018). https://doi.org/10.1155/2018/1754657
H.M. Do, M. Pham, W. Sheng, D. Yang, M. Liu, Rish: a robot-integrated smart home for elderly care. Robot. Auton. Syst. 101, 74–92 (2018)
F. Cavallo, R. Limosani, A. Manzi, M. Bonaccorsi, R. Esposito, M. Di Rocco, F. Pecora, G. Teti, A. Saffiotti, P. Dario, Development of a socially believable multi-robot solution from town to home. Cogn. Comput. 6(4), 954–967 (2014)
G. Peleka, A. Kargakos, E. Skartados, I. Kostavelis, D. Giakoumis, I. Sarantopoulos, Z. Doulgeri, M. Foukarakis, M. Antona, S. Hirche et al., Ramcip-a service robot for MCI patients at home, in 2018 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS) (IEEE, Piscataway, 2018), pp. 1–9
J. Casas, N. Cespedes, M. Múnera, C.A. Cifuentes, Chapter one - human-robot interaction for rehabilitation scenarios, in Control Systems Design of Bio-Robotics and Bio-mechatronics with Advanced Applications, ed. by A.T. Azar (Academic, London, 2020), pp. 1–31
J. Casas, E. Senft, L. Gutiérrez, M. Rincón-Rocancio, M. Munera, T. Belpaeme, C.A. Cifuentes, Social assistive robots: assessing the impact of a training assistant robot in cardiac rehabilitation. Int. J. Soc. Robot. 1–15 (2020). https://doi.org/10.1007/s12369-020-00708-y
J. Casas, N. Céspedes, C.A. Cifuentes G., L. Gutierrez, M. Rincón-Roncancio, M. Munera, Expectation vs. reality: attitudes towards a socially assistive robot in cardiac rehabilitation. Appl. Sci. 9, 4651 (2019)
N. Céspedes, B. Irfan, E. Senft, C.A. Cifuentes, L.F. Gutierrez, M. Rincon-Roncancio, T. Belpaeme, M. Múnera, A socially assistive robot for long-term cardiac rehabilitation in the real world. Front. Neurorobot. 15, 21 (2021)
D.J. Rea, S. Schneider, T. Kanda, “Is this all you can do? harder!”: The effects of (im)polite robot encouragement on exercise effort, in Proceedings of the 2021 ACM/IEEE International Conference on Human-Robot Interaction, HRI ’21 (Association for Computing Machinery, New York, 2021), pp. 225–233
M.F. Damholdt, M. Nørskov, R. Yamazaki, R. Hakli, C.V. Hansen, C. Vestergaard, J. Seibt, Attitudinal change in elderly citizens toward social robots: the role of personality traits and beliefs about robot functionality. Front. Psychol. 6, 1701 (2015)
D. Portugal, P. Alvito, E. Christodoulou, G. Samaras, J. Dias, A study on the deployment of a service robot in an elderly care center. Int. J. Soc. Robot. 11(2), 317–341 (2019)
A. Scheidig, B. Jaeschke, B. Schuetz, T.Q. Trinh, A. Vorndran, A. Mayfarth, H.M. Gross, May I keep an eye on your training? gait assessment assisted by a mobile robot, in IEEE International Conference on Rehabilitation Robotics, vol. 2019, June 2019, pp. 701–708
T.Q. Trinh, A. Vorndran, B. Schuetz, B. Jaeschke, A. Mayfarth, A. Scheidig, H.-M. Gross, Autonomous mobile gait training robot for orthopedic rehabilitation in a clinical environment, in 2020 29th IEEE International Conference on Robot and Human Interactive Communication (RO-MAN), pp. 580–587 (IEEE, Piscataway, 2020)
C. Piezzo, K. Suzuki, Feasibility study of a socially assistive humanoid robot for Guiding elderly individuals during walking. Future Internet 9(3), 30 (2017)
N. Céspedes, M. Munera, C. Gomez, C. Cifuentes G., Social human-robot interaction for gait rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. PP, 1 (2020)
N. Céspedes, D. Raigoso, M. Munera, C.A. Cifuentes, Long-term social human-robot interaction for neurorehabilitation: robots as a tool to support gait therapy in the pandemic. Front. Neurorobot. 15, 612034 (2021)
J.A. Buitrago, A.M. Bolaños, E. Caicedo Bravo, A motor learning therapeutic intervention for a child with cerebral palsy through a social assistive robot. Disabil. Rehabil. Assist. Technol. 15(3), 357–362 (2020)
N.A. Malik, H. Yussof, F.A. Hanapiah, R.A.A. Rahman, H.H. Basri, Human-robot interaction for children with cerebral palsy: reflection and suggestion for interactive scenario design. Procedia Comput. Sci. 76, 388–393 (2015)
J.C. Pulido, C. Suárez, J.C. González Dorado, A. Dueñas-Ruiz, P. Ferri, M. Encarnación, M. Sahuquillo, C. Echevarría, R. Vargas, P. Infante-Cossio, C. Luis, C. Parra Calderón, F. Fernández, A socially assistive robotic platform for upper-limb rehabilitation: a longitudinal study with pediatric patients. IEEE Robot. Autom. Mag. 26, 24–39 (2019)
G. Krahn, D. Walker, R. Correa-de Araujo, Persons with disabilities as an unrecognized health disparity population. Am. J. Public Health 105, e1–e9 (2015)
S. Gulley, E. Rasch, C. Bethell, A. Carle, B. Druss, A. Houtrow, A. Reichard, L. Chan, At the intersection of chronic disease, disability and health services research: a scoping literature review. Disabil. Health J. 11, 192–203 (2018)
V. Haung, J. Krakauer, Robotic neurorehabilitation: a computational motor learning perspective. J. NeuroEng. Rehabil. 6, 1–13 (2009)
M. Gilliaux, A. Renders, D. Dispa, D. Holvoet, J. Sapin, B. Dehez, C. Detrembleur, T. Lejeune, G. Stoquart, Upper limb robot-assisted therapy in cerebral palsy: a single-blind randomized controlled trial. Neurorehabil. Neural Repair 29, 183–192 (2014)
K. Kong, D. Jeon, Design and control of an exoskeleton for the elderly and patients. IEEE/ASME Trans. Mechatron. 11, 428–432 (2006)
C. Bayon, T. Martín Lorenzo, B. Moral, O. Ramírez, A. Moreno, S. Lerma Lara, I. Martínez, E. Rocon, A robot-based gait training therapy for pediatric population with cerebral palsy: goal setting, proposal and preliminary clinical implementation. J. NeuroEng. Rehabil. 15, 69 (2018)
D. Delisle Rodriguez, A. Villa-Parra, J. Lima, L. Vargas-Valencia, A. Frizera, T. Bastos, Assessment of an assistive control approach applied in an active knee orthosis plus walker for post-stroke gait rehabilitation. Sensors 20, 2452 (2020)
X. Giralt, L. Amigo, A. Casals, J. Amat, Robotic platform to evaluate the assistance and assessment on the rehabilitation loop, in Converging Clinical and Engineering Research on Neurorehabilitation, ed. by J.L. Pons, D. Torricelli, M. Pajaro. Biosystems & Biorobotics, vol. 1 (Springer, Berlin, 2013), pp. 1031–1035
S. Scott, S. Dukelow, Potential of robots as next-generation technology for clinical assessment of neurological disorders and upper-limb therapy. J. Rehabil. Res. Dev. 48, 335–353 (2011)
S. Brose, D. Weber, B. Salatin, G. Grindle, H. Wang, J. Vazquez, R. Cooper, The role of assistive robotics in the lives of persons with disability. Am. J. Phys. Med. Rehabil. 89, 509–521 (2010)
A.S. Prabuwono, K. Allehaibi, K. Kurnianingsih, Assistive robotic technology: a review. Comput. Eng. Appl. J. 6, 71–78 (2017)
A. Meyer-Heim, H.J. van Hedel, Robot-assisted and computer-enhanced therapies for children with cerebral palsy: current state and clinical implementation. Semin. Pediatr. Neurol. 20(2), 139–145 (2013)
D. Damiano, K. Alter, H. Chambers, New clinical and research trends in lower extremity management for ambulatory children with cerebral palsy. Phys. Med. Rehabil. Clin. N. Am. 20, 469–491 (2009)
K. Kong, D. Jeon, Fuzzy control of a new tendon-driven exoskeletal power assistive device, in Proceedings, 2005 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (IEEE, Piscataway, 2005), pp. 146–151
K. Kong, M. Tomizuka, H. Moon, B. Hwang, D. Jeon, Mechanical design and impedance compensation of SUBAR (Sogang University’s Biomedical Assist Robot), in 2008 IEEE/ASME International Conference on Advanced Intelligent Mechatronics, pp. 377–382 (IEEE, Piscataway, 2008)
A.C. Villa-Parra, D. Delisle-Rodríguez, A. López-Delis, T. Bastos-Filho, R. Sagaró, A. Frizera-Neto, Towards a robotic knee exoskeleton control based on human motion intention through EEG and sEMGsignals. Procedia Manuf. 3, 1379–1386 (2015)
R. Sagaro Zamora, Proposal of an assisted-motion system for gait rehabilitation, in International Workshop on Wearable Robotics WEROB2014, Sept 2014
C. Bayón, O. Ramírez, J.I. Serrano, M. del Castillo, A. Moreno, J.M. Belda Lois, I. Martínez-Caballero, S. Lerma Lara, C. Cifuentes G., A. Frizera, E. Rocon, Development and evaluation of a novel robotic platform for gait rehabilitation in patients with cerebral palsy: CPwalker. Robot. Auton. Syst. 91, 101–114 (2017)
S.D. Sierra M., J.F. Molina, D.A. Gomez, M.C. Munera, C.A. Cifuentes, Development of an interface for human-robot interaction on a robotic platform for gait assistance: AGoRA smart walker, in 2018 IEEE ANDESCON, pp. 1–7 (IEEE, Piscataway, 2018)
M. Sánchez-Manchola, D. Gomez-Vargas, D. Casas-Bocanegra, M. Munera, C.A. Cifuentes, Development of a robotic lower-limb exoskeleton for gait rehabilitation: AGoRA exoskeleton, in 2018 IEEE ANDESCON, ANDESCON 2018 - Conference Proceedings (2018), pp. 1–6
M. Sánchez-Manchola, D. Serrano, D. Gómez, F. Ballen, D. Casas, M. Munera, C.A. Cifuentes, T-FLEX: variable stiffness ankle-foot orthosis for gait assistance, in Wearable Robotics: Challenges and Trends (Springer, Cham, 2019), pp. 160–164
D. Casas, M. Gonzalez Rubio, M. Montoya, W. Sierra, L. Rodriguez, E. Rocon, C.A. Cifuentes, Bioinspired hip exoskeleton for enhanced physical interaction, in Converging Clinical and Engineering Research on Neurorehabilitation II. Biosystems & Biorobotics, ed. by J. Ibáñez, J. González-Vargas, J. Azorín, M. Akay, J. Pons (Springer, Cham, 2017), pp. 1497–1501
D. Gomez-Vargas, M.J. Pinto-Betnal, F. Ballén-Moreno, M. Múnera, C.A. Cifuentes, Therapy with t-flex ankle-exoskeleton for motor recovery: a case study with a stroke survivor, in 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob) (2020), pp. 491–496
M.D. Sánchez-Manchola, L.J. Arciniegas Mayag, M. Munera, C.A. Garcia, Impedance-based backdrivability recovery of a lower-limb exoskeleton for knee rehabilitation, in 4th IEEE Colombian Conference on Automatic Control: Automatic Control as Key Support of Industrial Productivity, CCAC 2019 - Proceedings, Medellin (2019), pp. 1–6
S.D. Sierra M., M.F. Jimenez, M.C. Múnera, T. Bastos, A. Frizera-Neto, C.A. Cifuentes, A therapist helping hand for walker-assisted gait rehabilitation: a pre-clinical assessment, in 2019 IEEE 4th Colombian Conference on Automatic Control (CCAC) (2019), pp. 1–6
R.C. Mello, S.D. Sierra, M. Munera, C.A. Cifuentes, M.R.N. Ribeiro, A. Frizera-Neto, Cloud robotics experimentation testbeds: a cloud-based navigation case study, in 2019 IEEE 4th Colombian Conference on Automatic Control (CCAC) (IEEE, Piscataway, 2019), pp. 1–6
M. Bautista, A. Garzón, S. Sierra Marín, M. Munera, C. Cifuentes G., Integration of a social robot in physical rehabilitation assisted by Lokomat, in X Congreso Iberoamericano de Tecnologías de Apoyo a la Discapacidad IBERDISCAP2019, Buenos Aires (2019), pp. 423–426
S. Hesse, A. Heß, C. Werner, N. Kabbert, R. Buschfort, Effect on arm function and cost of robot-assisted group therapy in subacute patients with stroke and a moderately to severely affected arm: a randomized controlled trial. Clin. Rehabil. 28, 637–647 (2014)
A. Timmermans, R. Lemmens, M. Monfrance, R. Geers, W. Bakx, R. Smeets, H. Seelen, Effects of task-oriented robot training on arm function, activity, and quality of life in chronic stroke patients: a randomized controlled trial. J. Neuroeng. Rehabil. 11, 45 (2014)
W.-w. Liao, C.-Y. Wu, Y.-W. Hsieh, K.-c. Lin, W.-Y. Chang, Effects of robot-assisted upper limb rehabilitation on daily function and real-world arm activity in patients with chronic stroke: a randomized controlled trial. Clin. Rehabil. 26, 111–120 (2011)
J.-C. Fraile, J. Pérez-Turiel, E. Baeyens, P. Viñas, R. Alonso, A. Cuadrado, M. Franco, E. Parra Vidales, L. Ayuso, F. García-Bravo, F. Nieto, L. Lipsa, E2rebot: a robotic platform for upper limb rehabilitation in patients with neuromotor disability. Adv. Mech. Eng. 8, 1–13 (2016)
P. Sale, M. Franceschini, A. Waldner, S. Hesse, Use of the robot assisted gait therapy in rehabilitation of patients with stroke and spinal cord injury. Eur. J. Phys. Rehabil. Med. 48, 111–121 (2012)
C. Senanayake, S. Senanayake, Emerging robotics devices for therapeutic rehabilitation of the lower extremity, in 2009 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (IEEE, Piscataway, 2009), pp. 1142–1147
E. Tsardoulias, P. Mitkas, Robotic frameworks, architectures and middleware comparison. arXiv:1711.06842, Nov 2017
C. Valadao, E. Caldeira, T. Bastos-Filho, A. Frizera-Neto, R. Carelli, A new controller for a smart walker based on human-robot formation. Sensors 16(7), (2016)
M. Sanchez-Villamanan, J. Gonzalez-Vargas, D. Torricelli, J. Moreno, J. Pons, Compliant lower limb exoskeletons: a comprehensive review on mechanical design principles. J. NeuroEng. Rehabil. 16, 55 (2019)
Y. Long, Z.-j. Du, W. Wang, W. Dong, Development of a wearable exoskeleton rehabilitation system based on hybrid control mode. Int. J. Adv. Robot. Syst. 13, 10 (2016)
A. Hasan, Designing and implementing an electronic system to control moving orthosis virtual mechanical system to emulate lower limb. Cogent Eng. 5, 1456632 (2018)
E. Einbinder, T. Horrom, Smart walker: a tool for promoting mobility in elderly adults. J. Rehabil. Res. Dev. 47, xiii–xv (2010)
S. Bradley, C. Hernandez, Geriatric assistive devices. Am. Fam. Physician 84, 405–411 (2011)
A.D.C. Chan, J.R. Green, Smart rollator prototype, in 2008 IEEE International Workshop on Medical Measurements and Applications (IEEE, Piscataway, 2008), pp. 97–100
G. Lacey, S.M. Namara, K.M. Dawson-Howe, Personal adaptive mobility aid for the infirm and elderly blind, in Assistive Technology and Artificial Intelligence (Springer, Berlin, 1998), pp. 211–220
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Sierra M., S.D. et al. (2022). Introduction to Robotics for Gait Assistance and Rehabilitation. In: Interfacing Humans and Robots for Gait Assistance and Rehabilitation. Springer, Cham. https://doi.org/10.1007/978-3-030-79630-3_1
Download citation
DOI: https://doi.org/10.1007/978-3-030-79630-3_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-79629-7
Online ISBN: 978-3-030-79630-3
eBook Packages: EngineeringEngineering (R0)