
Abstract
Haptic training in simulation is a rising pedagogical trend in medical education. It is a rather new field that appeared partly because the adage “see one, do one, teach one”, from a mentoring standpoint, is undesirable due to public consideration for patient safety. Teaching strength management for a given procedure is a difficult task. This is not a skill one can retrieve from books or by only “seeing” the procedure. It needs to be experienced by the trainee. For this matter, haptic training on virtual patients offers a good opportunity to tackle this problem at the price of a constant trade-off between what technology can do and the expectation of realism. The technology is expensive, complex to maintain and very specific. Many simulators on the market use low-end devices to maintain the cost and are therefore unable to simulate proper interactions with the virtual patient. The platform presented here is an ecosystem which aims to study how to extend haptic simulations on a broader range of applications. We present an approach using innovative mechatronics, based on purely resistive force, to reach better haptic feedback at lower cost. The system is designed to be compact and safe. It allows strong and high resolution feedback as well as easy integration in existing devices. This technology will help to extend haptic simulations earlier in the curriculum where the resident requires basic hands-on experience.
Supported by ANR SimUSanté and EQUIPEX FIGURES - We thank Az-Eddine Djebara for the organization of the evaluation as well as Pr. Patrick Mertl, the Amiens orthopaedic unit and the Chimère research team.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others

Keywords
1 Training Haptics in Medicine
1.1 Historical Background
The platform presented here originates from the European project SKILLS (FP6) that lasted from 2006 to 2011 in which a surgical platform was specifically designed to provide high fidelity haptic feedback [1]. For this purpose, a 6 dof (degrees of freedom) haptic feedback interface was developed for applications in bone surgery procedures [2]. The platform was tested in several hospitals through a training program on maxillofacial surgery [3]. Since the first prototype, a second version of the platform was developed and delivered to the Facing Faces Institute at the University hospital of Amiens, France. The objective was to integrate the system in a real medical environment to reach a large population of students.
Our investigations showed that providing high fidelity haptic rendering is a key asset to reach stakeholder approbation. There is indeed a strong demand for haptic simulation in medicine but with great expectation on feedback fidelity. However, the price of such robotic systems, like the one developed during the SKILLS project, is very high and the question of the economical model must be addressed either by broadening the range of application or by lowering the cost. The platform had to evolve toward a cheaper and more versatile system while maintaining a high degree of realism. To achieve this goal, it is necessary to open the technology of the platform and to think of the platform as a global research tool in a broader ecosystem.
In order to find a solution to the difficult question of expectation versus cost, we have started investigating the use of a novel haptic technology based on magneto-rheological (MR) fluids. The main idea is to replace a standard electric motor by a purely resistive system to reduce size, cost, and improve security by removing instabilities in the control loop. Such systems may not be applicable to all simulations but are suitable to many of them. Our research program starts with a simple case of only 1 dof : the clinical examination of a knee joint. In the following, we introduce this orthopaedic simulation in Sect. 1.2, hardware in Sect. 2, and we describe the biomechanical simulation of the knee in Sect. 3. A first evaluation of the system was performed in Amiens Hospital and is presented in Sect. 4. Finally, in Sect. 5, we conclude on how the platform will be extended and used in the future.
1.2 Orthopaedic Simulation
Educational resources in the orthopaedic curriculum include lecture courses, academic books, experience in the clinical setting, and experience in the operating theater. Additional knowledge is gained from reading scientific literature in texts and journals, performing dissections on cadavers in the anatomy labs, and from web-based resources. Residency programs have opted to develop ‘skills labs’ where techniques and skills are taught and practised on simulators, bench models, and serious games. The potential benefit these labs offer is increased opportunities for residents to gain familiarity with their working environment and the basic skills, procedures, and techniques in a low-risk, low-cost and easily accessible environments [4, 5]. Simulation in medicine can be defined as “any technology or process that recreates a contextual background in a way that allows a learner to experience mistakes and receive feedback in a safe environment” [6]. The advantages of simulation extend beyond simple technical and procedural skills. Simulation allows trainees to engage with a multi-disciplinary team and focus on individual and team-based cognitive skills including problem solving, decision-making, and team behavior skills [7, 8]. Technological advances in VR immersive environments allow the creation of new learning modalities including 3D vision and haptic (tactile and force) feedback, which are essential in skill learning, retention, and transfer of information to the real world. The anatomy can be re-discovered by learning an active dynamic anatomy, which is much more informative and detailed on osteo-articular displacements in normal and pathological situations [9,10,11], but the literature to date is scarce in this field. Many research programs are oriented in procedural surgical simulation, but very few are involved in the visuo-haptic understanding of the clinical examination of a knee joint.
Finally, it is important to draw together the knowledge and quantitative findings that help to explain why certain types of skills are difficult to learn. One of the most important functional features of a simulation training device is the capacity to emulate the procedure to be learned and give detailed, reliable, and valid quantitative measures of performance, i.e. metrics. A simulator without these metric attributes is nothing more than a fancy video game [12].
2 Hardware for Dynamic Anatomy
At this stage, applications are limited to two clinical examinations called the Lachman and Drawer test, consisting in testing the laxity of the cruciate ligaments. Previous studies have already investigated the clinical examination of a knee joint [13] with good results as a pedagogical tool but the phantom-based interaction was using a robot to render the force. Cost is however still a major limitation for the market penetration of these technologies. Heavy robotic systems needed for simulation in orthopaedics where large forces must be managed is neither practical nor economically viable. It is therefore important to investigate alternative technologies in order to make dynamic anatomy for education a reality.
For applications like the Lachman test where the movement is in one direction, applying a force in the opposite direction of the movement is usually enough. This can be achieved using a brake instead of a motor. Haptic feedback applications in virtual reality, especially in medicine, usually require stronger resistive force than driving force. Many papers can be found that use brakes for haptic [14, 15] or prosthetic applications [16], some with hybrid technologies combine an electric motor and a brake [17]. To achieve the required performance in terms of reliability, form factor, range of torque and haptic fidelity, we have chosen a technology based on MR fluid. It provides high torque/weight ratio, low response times and low power. The counter force can be precisely controlled with good linearity and passivity [17, 18]. The device was specifically engineered in our lab for haptic rendering [19, 20]. The MR brake works in rotation with a torque from 10 mN.m to 1.5 N.m and response time below 8 ms. The movement is then transformed into a translation with a pulley and a belt providing a force up to 160 N.
From a mechanical point of view, the movement of the leg is performed with a rotation situated 25 cm below the knee. During the clinical examination, the movement of the knee is neither a translation nor a rotation. Combining the two was considered too expensive to implement and the movement depends too much on the patient physiology. Rotation was a better choice from a mechanical perspective leading to a lighter and more reliable system.
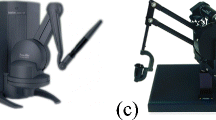
The coupling between the knee and the simulation is done via a USB connection : sensors on the knee send the position of the tibia relative to the femur to the simulation and the simulation returns the force that the brake has to apply. The prototype is shown in Fig. 1.

First prototype of the dynamic anatomy simulator
3 Simulation of the Knee Biomechanics
3.1 Physical Model of the Knee Joint
We simulate the biomechanics of the knee using the SOFA framework [21]. The focus of our simulation is to emphasize the differences between a healthy knee compared to a knee with a broken ligament. The physics of our simulation is thus centered on the ligaments elongation and resistance.
The femur and the duo tibia/fibula are the two articulated rigid bodies of our simulation with a mass and an inertia computed from the shape of our 3D models of the bones. The tibia can move relative to the femur with six degrees of freedom and contacts between the bones are computed as repulsive forces when the two meshes intersect. However, we are mainly interested in two dimensions: the angle of flexion and the translation forward when pulling the tibia during a Lachman test.

Simulation of the fibular collateral ligament. The chain of springs (yellow) is following the deformation of the ligament (orange wireframe) attaching the femur and the fibula (gray) (Color figure online).
The two rigid systems are attached by ligaments, whose strength is modeled as a chain of springs. Only the main ligaments assuring the stability of the knee joints are kept: the anterior cruciate, the posterior cruciate, the tibial collateral and the fibular collateral. When the knee moves, the 3D meshes of these ligaments deforms according to an animation skinning based on the bones position and orientation. The intermediate points of the spring chains are constrained by this skinning and deform accordingly (Fig. 2). A constraint is put on the total length of each chain which creates a pulling force when the ligaments are stretched. In the case of a broken ligament simulation, we simply remove this constraint. The power of the constraint can also be modulated to simulate a partial tear of the ligament.
When the tibia is pulled forward for the Lachman test, we can, at each time step of the simulation, note the force applying on the tibia in the axis of its translation. To this force, we add a global affine force, only depending on the tibia translation, to simulate the resistance of all the other tissues (muscles, skin...) to the pulling gesture. The parameters of this affine function are computed so that the total force pulling back the tibia matches the order of magnitude of force measurements made with a GNRB arthrometer [22].
3.2 Mapping of the Simulation
Haptic simulation needs high frame rate and low latency to ensure a good user experience, and running a live physical simulation could slow down the process. Since the input sent by the haptic interface is only two-dimensional (rotation and translation of the tibia), it is possible to create a discretization of all possible inputs, in the range of anatomical limitations, while keeping a fine grain for precision. We thus decided to make a mapping of precomputed outputs of the simulation and then interpolate into this data. Hence, the haptic process is no longer bound to the speed of the physical simulation which is executed offline.
We automatized the simulation to be launched sequentially with a series of different inputs and to register the output force on the tibia depending on these starting conditions. The tibia angle was sampled between 0\(^{\circ }\) (straight leg) and 90\(^{\circ }\) with a step of 10\(^{\circ }\) and its translation between 0 mm and 30 mm with a step of 1.66 mm. Two maps were created and used by the application, one for a healthy knee, another for a broken anterior cruciate ligament.

Testing the prototype at the orthopaedic department of the CHU Amiens, France.
4 First Evaluation
In the user-centered design methodology, a first evaluation of the prototype was organized at the orthopaedic department of the CHU Amiens, France (Fig. 3). The evaluation was performed with a group of 10 orthopaedic surgeons. The panel of expertise was heterogeneous with expert surgeons, interns and medical students.
The evaluation started with a presentation of the purpose of the development and the methodology used for the evaluation. The group was informed that the design followed a user-centered methodology and that the aim was to gather any remarks that would help to improve the design. The methodology was in two sections : one was to gather remarks on the fly during the test of the prototype and the second one was a questionnaire about the quality of the simulator. As some participants did not give their consents relative to the audio and video recording of the evaluation session, the video was restricted to the orthopaedics who gave their consent. Other feedback was gathered through the answers to the questionnaire.
The dynamic haptic simulator of the knee was introduced. The simulation allowed the surgeons to experience two different states of the knee, with cruciate ligament being either broken or healthy. The visual rendering was then presented on a screen. It showed, on demand, the knee and leg according to different viewpoints : whole leg/knee with or without skin, muscles, bones, or ligaments. The visual rendering was linked to the haptic model of the knee.
The prototype was tested by the participants. All feedback converged on the interest of dynamic knee simulation for learning the diagnosis of knee pathology. The need is relative to the Lachman test for the diagnosis of cruciate ligament rupture, but other tests have been mentioned, such as drawer test and the rotational jump test. The interviews indicated the importance of the position, the movements of the hands during the test hands and the feeling of the knee reaction. The latter is described as “feeling the sensation of hard stop” (no ligament rupture) and soft stop (cruciate ligament rupture). The analogy that seems most representative of the feeling of experts is that of a “string being stretched”.
The dynamic simulator of the knee is considered very accurate for the anterior drawer test when the knee is bent at \(90^{\circ }\). However, the haptic simulator is judged too “lax” for the Lachman test when the Knee is bent at \(20^{\circ }\) and experts do not feel any “hard stop” which indicates the end of the course of the ligament. At the stage of the evaluation, the prototype could not provide the ideal metaphor of a “string being stretched”. The difference may be explained from the fact that the arthrometer used in the definition of the model does not provide a good insight in the clinical examination. The arthrometer explores the joint with a quasi-static displacement and constrains the knee in a strict translation while, for the Lachman test, the surgeons in our studies applied a fast movement, combining a translation and a rotation. Surgeons were not evaluating the overall stiffness but were looking for this feeling of a “hard stop”. However, for the drawer test the movement they applied was actually very similar to what the arthrometer does and they were indeed evaluating the stiffness. This knowledge will be used to refine the model in future works in order to distinguish between the two possible approaches of the examination.
Another interesting fact is that the graphic model is not considered useful by the experts. They indicate that they base their diagnosis solely on the haptic sensation of the behavior of the knee and that they do not rely on vision, which gives them very few diagnostic elements. Young medical students did not express their opinions about the interest of the visual model, but we will have to consider how the visual model could become a pedagogical and evaluation resource.
The answers to the questionnaire indicate that many factors can impact the diagnostic and could be considered in the future versions of the dynamic simulator. Stressed patients may induce wrong diagnostics; athletes are difficult to examine because developed muscles make the leg difficult to examine (heavy and difficult to move); the laxity is also a factor that contributes to make the diagnostics difficult with a risk of false positive.
5 Conclusion
In this document, we presented a first attempt to simulate the haptic clinical examination of the knee with purely resistive actuators. This approach may be a good solution to extend the range of applications of simulation in medical education. The surgeons involved in our first evaluation never mentioned any problems with the fact that the actuation was not dynamic, leading to the conclusion that the omission of motors is a viable solution for this kind of procedure.
The evaluation conducted with the device provided key feedback and gave us better insight of the clinical aspect of the examination. The device turns out to be indeed a great tool to help the surgeon talk about their practice. They all have a different way to do the examination and testing the simulation helps a great deal in defining the common ground of their unsaid sensations.
The second step of our research program is already in the works. It aims at extending the use of the MR brakes to a more complex therapeutic procedure: the reduction of mandibular dislocation. Three brakes will be used to simulate the dynamics of this procedure. At this stage, we will use the platform as a complete research ecosystem. The 6 dof SKILLS platform will be used to evaluate and test the model of the mandible and pedagogical protocol will benefit from both the robotic and the MR based systems leading to a thorough comparison between different technologies.
There is a real benefit in bringing force management training earlier in curriculum. Procedures like the one studied here are often performed in the Emergency Room with young residents. Such simulators will help them practice before having access to the patient. This is important especially for complex, rare, and potentially painful procedures like mandibular dislocation. This is the reason why we introduce the idea of dynamic anatomy as a means to improve the overall expertise of students all along their curriculum.
References
Bouchigny, S., Mégard, C., Gosselin, F., Hoffmann, P., Korman, K.: Designing a VR training platform for surgeons: theoretical framework, technological solutions and results. In: Bergamasco, M., Bardy, B., Gopher, D., (eds.) Skill Training in Multimodal Virtual Environments, p. 199. Taylor and Francis, Bergamasco (2013)
Gosselin F., Ferlay F., Bouchigny S., Mégard C., Taha F.: Specification and design of a new haptic interface for maxillo facial surgery. In: IEEE International Conference on Robotics and Automation, Shanghai, pp. 737–744 (2011)
Gosselin, F., Bouchigny, S., Mégard, C., Taha, F., Delcampe, P., d’Hauthuille, C.: Haptic systems for training sensorimotor skills: a use case in surgery. Robot. Autonomous Syst. 61(4), 380–389 (2013)
Wolf, B.R., Britton, C.L.: How orthopaedic residents perceive educational resources. Iowa Orthop. J. 33, 185–190 (2013)
Aggarwal, R., et al.: Training and simulation for patient safety. Qual. Saf. Health Care 19(Suppl 2), i34–43 (2010)
Gaba, D.M.: The future vision of simulation in health care. Qual. Saf. Health Care 13(Suppl 1), i2–10 (2004)
Stirling, E.R.B., Lewis, T.L., Ferran, N.A.: Surgical skills simulation in trauma and orthopaedic training. J. Orthop. Surg. Res. 9, 126 (2014). https://doi.org/10.1186/s13018-014-0126-z
Ruikar, D.D., Hegadi, R.S., Santosh, K.C.: A systematic review on orthopedic simulators for psycho-motor skill and surgical procedure training. J. Med. Syst. 42(9), 1–21 (2018). https://doi.org/10.1007/s10916-018-1019-1
Popescu, D., Iacob, R., Laptoiu, D.: Virtual reality in orthopedic surgeons training. Key Eng. Mater. 638, 344–351 (2015)
Lazennec, J., Laudet, C., Guérin-Surville, H., Roy-Camille, R., Saillant, G.: Dynamic anatomy of the acetabulum: an experimental approach and surgical implications. Surg. Radiol. Anat. 19(1), 23–30 (1997). https://doi.org/10.1007/BF01627730
Grow, D.I., Wu, M., Locastro, M.J., Arora, S.K., Bastian, A.J., Okamura, A.M.: Haptic simulation of elbow joint spasticity. In: Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems. Reno, NE, vol. 2008, pp. 475–476 (2008)
Gallagher, A.G., O’Sullivan, G.C.: Fundamentals of Surgical Simulation, p. 31. Springer, London (2012). https://doi.org/10.1007/978-0-85729-763-1
Riener, R., Frey, M., Proll, T., Regenfelder, F., Burgkart, R.: Phantom-based multimodal interactions for medical education and training: the Munich knee joint simulator. IEEE Trans. Inf Technol. Biomed. 8(2), 208–216 (2004)
Senkal, D., Gurocak, H.: Serpentine flux path for high torque MRF brakes in haptics applications. Mechatronics 20(3), 377–383 (2010)
Cinq-Mars, M., Gurocak, H.: Pneumatic actuator with embedded MR-brake for haptics. In: IEEE World Haptics Conference (WHC), Munich, pp. 322–327 (2017)
Bulea, T.C., Kobetic, R., To, C.S., Audu, M.L., Schnellenberger, J.R., Triolo, R.J.: A variable impedance knee mechanism for controlled stance flexion during pathological Gait. IEEE/ASME Trans. Mechatron. 17(5), 822–832 (2012)
Rossa, C., Lozada, J., Micaelli, A.: Design and control of a dual unidirectional brake hybrid actuation system for haptic devices. IEEE Trans. Haptics 7(4), 442–453 (2014)
Rossa, C., Jaegy, A., Lozada, J., Micaelli, A.: Design considerations for magnetorheological brakes. IEEE/ASME Trans. Mechatron. 19(5), 1669–1680 (2014)
Hafez, M., Lozada, J., ECK, L., Changeon, G.: Fluid haptic interface with improved haptic rendering using a torque or load sensor. Patent US9898032B2
Eck, L., Lozada, J., Changeon, G., Hafez, M.: lnterface haptique prenant en compte l’intention d’action de l’utilisateur”. Patent FR14 59187
Allard, J., Cotin, S., Faure, F., Bensoussan, P.J., Poyer, F., Duriez, C., Grisoni, L.: Sofa-an open source framework for medical simulation. In: MMVR 15-Medicine Meets Virtual Reality, vol. 125, pp. 13–18. IOP Press, February 2007
Robert, H., Nouveau, S., Gageot, S., Gagniere, B.: A new knee arthrometer, the GNRB®: experience in ACL complete and partial tears. Orthop. Traumatol. Surg. & Res. 95(3), 171–176 (2009)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this paper

Cite this paper
Bouchigny, S. et al. (2020). A Simulation Platform for Early Haptic Training in Surgical and Medical Education. In: McDaniel, T., Berretti, S., Curcio, I., Basu, A. (eds) Smart Multimedia. ICSM 2019. Lecture Notes in Computer Science(), vol 12015. Springer, Cham. https://doi.org/10.1007/978-3-030-54407-2_22
Download citation
DOI: https://doi.org/10.1007/978-3-030-54407-2_22
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-54406-5
Online ISBN: 978-3-030-54407-2
eBook Packages: Computer ScienceComputer Science (R0)