
Abstract
While the treatment results of Hirschsprung’s disease have improved, significant attention is brought to long-term functional, psychosocial, and quality of life issues in children and adults with Hirschsprung’s disease. The overall long-term functional outcome expectancy is relatively optimistic; although many patients have some degree of bowel dysfunction and continence defect, they are able to stay socially continent and report a good quality of life. In contrast, some patients need special bowel management programs to achieve social continence, or some are even left with persistent incontinence and significant psychosocial problems needing additional medical attention. Other long-term problems such as enterocolitis may have a significant impact on long-term functional outcome and quality of life. In this chapter, the long-term outcomes of Hirschsprung’s disease regarding bowel function and continence, enterocolitis, and quality of life are discussed. Furthermore, long-term issues related to specific patient groups, such as syndromic patients and total colonic aganglionosis, are reviewed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
32.1 Introduction
Before the onset of pediatric surgery as an independent specialty and development of modern pediatric surgery, the overall outcome of Hirschsprung’s disease was poor as the disease was fatal in most cases. Along with the development of pediatric surgery, the long-term outcomes of Hirschsprung’s disease have significantly improved following better understanding of the pathophysiology and pathological anatomy of the disease and development of surgical techniques. While the treatment results have improved, significant attention has been brought to long-term functional, psychosocial, and quality of life issues in children and adults with Hirschsprung’s disease. The overall long-term functional outcome expectancy is relatively optimistic; although many patients have some degree of bowel dysfunction and continence defect, they are able to stay socially continent and report a good quality of life [1,2,3]. In contrast, some patients need special bowel management programs to achieve social continence, or some are even left with persistent incontinence and significant psychosocial problems needing additional medical attention [3, 4].
In this chapter, the long-term outcomes of Hirschsprung’s disease regarding bowel function and continence, enterocolitis, and quality of life are discussed. Furthermore, long-term issues related to specific patient groups, such as syndromic patients and total colonic aganglionosis, are reviewed.
32.2 Functional Outcomes
32.2.1 During Childhood
32.2.1.1 Bowel Function
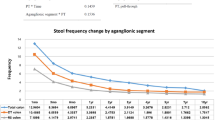
In the majority of studies, the overall bowel function in children with Hirschsprung’s disease is reported to be relatively good although a significant number of patients continue to have problems with bowel function (Table 32.1) [1, 4,5,6,7,8,9]. The bowel function, measured with bowel function score, is clearly worse in children with Hirschsprung’s disease than in healthy controls, but it significantly improves with increasing age [1]. In a Nordic multicenter study [4] in children from 4 to 7 years, 8 to 12 years, and 13 to 17 years who underwent transanal endorectal pull-trough for Hirschsprung’s disease, problems with ability to hold back stools (69% vs 55% vs 22%) and an urge to defecate (38% vs 24% vs 19%) as well as social problems (28% vs 21% vs 19%) were reported in all age groups [4]. After pull-through operation, stooling frequency is generally higher compared to healthy controls but tends to decrease over time, especially during the first 6 months after surgery [1, 10, 11]. Teitelbaum et al. showed that decreasing stooling pattern with good levels of continence was reached after 3 years of follow-up in patients who underwent a primary endorectal pull-through as infants [10]. Similarly, stooling frequency was shown to decrease after both transabdominal (initial average 5/day vs final 2/day) and transanal (5/day vs 2/day) pull-throughs such that by year 7, there was no difference between the groups [11].
32.2.1.2 Constipation
During childhood, constipation is a relatively common problem after pull-through operation for Hirschsprung’s disease as it is reported in 3–36% of patients (Table 32.1) [1, 4,5,6, 8, 9, 12,13,14,15]. Prolonged colonic transition time, abnormal internal sphincter function, or mechanical obstruction such as postoperative stricture or formation of a spur after Duhamel procedure are common causes of constipation [16,17,18]. Constipation is seen significantly more commonly in patients from 4 to 12 years of age compared to adolescents and adults with Hirschsprung’s disease [4]. A significant proportion of children with Hirschsprung’s disease, approximately 30% of patients from 4 to 12 years of age, need diet, laxatives, or enemas to treat the constipation after transanal endorectal pull-through operation [4]. In most cases, however, constipation is manageable with diet changes and oral medication.
32.2.1.3 Soiling and Fecal Incontinence
Fecal incontinence and soiling are the major complications after any type of surgery for Hirschsprung’s disease. To maintain normal continence, a preserved sphincter function, rectal reservoir, and anal canal sensation are required. In Hirschsprung’s disease, several components related to the disease and its repair can interfere with the continence mechanism and cause long-term problems with soiling and incontinence. Patients with Hirschsprung’s disease lack normal rectoanal relaxation reflex before and after surgery, consistent with primary defects in the innervation and function of the internal anal sphincter [16, 19]. At pull-through operation, the internal anal sphincter is at least partially interfered, the rectal reservoir is completely or partially lost, and the transitional epithelium responsible for anal sensation may be inadvertently removed. In controlled manometric studies, the resting and maximal anal canal squeeze pressures are significantly lower after Duhamel procedure compared to controls [16, 17]. In Hirschsprung’s disease, the fecal continence is largely dependent on sufficient function of the voluntary sphincters because of the impaired function of the internal sphincter [20].
Overall, soiling or incontinence is reported in 4–77% and 1–63% of children with Hirschsprung’s disease depending on the study population and the used study methods and definitions of soiling and incontinence (Table 32.1) [1, 4,5,6, 8, 9, 12,13,14,15, 21,22,23]. Generally, soiling and incontinence problems seem to decrease from childhood toward adolescence [13, 14, 17, 24].
Kim et al. compared the results of transabdominal (mean age 7 years) and transanal pull-through (mean age 11 years) techniques in a multicenter study, and they found no significant differences in continence scores between the two groups, and the scores did not significantly change with increasing time [11]. Similarly, Neuvonen et al. reported that the type of transanal pull-through (totally transanal or combined) did not significantly influence overall outcome by means of bowel function score [1]. Tannuri et al. compared children who underwent the Duhamel operation to patients with transanal pull-through technique and found similar outcomes according to the fecal continence index [22]. On the other hand, the findings in the large Nordic multicenter study suggested that totally transanal approach is associated with worse outcome than transabdominally or laparoscopically assisted transanal pull-through [4].
32.2.2 Beyond Childhood
32.2.2.1 Bowel Function
Overall, bowel function seems to improve over time when looking at studies showing results 20 years and more after pull-through (Table 32.1) [1, 4, 25]. Neuvonen et al. showed that bowel function score was significantly better after transanal endorectal pull-through in patients more than 18 years of age compared to younger patients [1]. Similar results were reported by Bjornland et al. in a multicenter study after transanal endorectal pull-through, including no social problems related to bowel function in 74%, normal ability to hold back stools in 77%, and mostly or always feeling an urge to defecate in 100% of patients [4]. In contrast, Conway and Granstrom both reported impaired bowel function in adults after Duhamel or Soave pull-through [2, 26]. Although the stooling frequency has been reported to decrease over time during childhood, abnormal stooling frequency persisted in 50% of patients to adulthood [1, 10]. At older age, bowel function seems to be deteriorating as older age predicts poor bowel function [25].
32.2.2.2 Soiling and Fecal Incontinence
Although it is unlikely that surgery-related anatomical defects of anal function that are the cause of fecal incontinence in Hirschsprung’s disease significantly improve over time, the fecal incontinence rate reported by patients seems to diminish after puberty [4, 13, 14, 24]. Several studies have reported that fecal incontinence rate improves with age as problems with fecal continence were more common among toddlers and children and less common in teenagers and adults [1, 13, 14, 17, 24]. In more detail, all aspects of fecal control, including urgency, rectal sensation, ability to hold back defecation, fecal soiling, and fecal accidents, improved to levels that no longer significant differences were detected beyond the age of 18 years compared to healthy controls [1]. Overall, socially disturbing incontinence seems to be relatively uncommon in adults, and it has minor impact on the psychosocial functioning which is likely reflecting the advanced coping and adapting capabilities of adults [2, 15, 25].
32.3 Enterocolitis
Hirschsprung’s disease-related enterocolitis is a fairly frequent complication that may affect the outcome of patients before and after pull-though procedure. Enterocolitis is reported to occur in 6–50% and 2–35% of Hirschsprung’s disease patients in the pre- and postoperative period [27]. Enterocolitis is a potentially life-threatening complication and late mortalities after pull-through operation are reported to relate to enterocolitis in up to 50% of cases [28, 29]. While any patient with Hirschsprung’s disease is at risk of enterocolitis, there are certain patient groups with significantly increased risk, including patients with Down syndrome, long-segment disease, prior episodes of enterocolitis, and familial history of Hirschsprung’s [30,31,32,33].
Enterocolitis is closely related to overall bowel function. In a recent multicenter study, the history of frequent episodes of enterocolitis was significantly higher in patients who reported soiling often or always compared to those who had soiling never or rarely [4]. In contrast, the overall rates of any soiling or fecal accidents (which included infrequent symptoms) did not differ significantly between patients with persistent enterocolitis compared to enterocolitis-free patients [1].
Hirschsprung’s-related enterocolitis and inflammatory bowel disease have similar clinical symptoms, including diarrhea, hematochezia, and colicky abdominal pain, and both conditions are characterized by an abnormal intestinal mucosal barrier function and alterations in intestinal microbiota [34,35,36,37,38]. Although it still remains unclear whether inflammatory bowel disease and Hirschsprung’s disease have a common etiology, inflammatory bowel disease has been reported to relate to Hirschsprung’s disease [39,40,41]. Both Crohn’s disease and ulcerative colitis are seen in patients with Hirschsprung’s disease, but Crohn’s disease is reported to be more common [40]. Lof Granstrom et al. showed in a nationwide population-based register cohort that the risk for inflammatory bowel disease is significantly increased (OR 4.99) among patients with Hirschsprung’s disease compared to sex- and age-adjusted healthy controls [40]. In a meta-analysis by Nakamura et al., patients with extensive colonic aganglionosis who continued to suffer from enterocolitis after pull-through operation were more susceptible to develop inflammatory bowel disease [34]. In the long-term follow-up, it is important for clinicians to keep in mind that chronic enterocolitis-type symptoms may as well be a sign of inflammatory bowel disease in patients with Hirschsprung’s disease.
32.4 Total Colonic Aganglionosis
Total colonic aganglionosis is a severe form of Hirschsprung’s disease with related significant short- and long-term morbidity, including enterocolitis, perianal excoriation, frequent bowel movements, constipation, soiling, fecal incontinence, metabolic complications, and failure to thrive. Overall, no superior operative approach for total colonic aganglionosis has been confirmed with respect to postoperative morbidity, occurrence of enterocolitis, functional outcome, or mortality [20, 42]. Enterocolitis is a common complication and often a chronic problem in patients with total colonic aganglionosis. The incidence of enterocolitis is significantly higher in patients with total colonic aganglionosis, ranging from 20% to 55%, compared to patients with a rectosigmoid disease [31, 32, 42]. In a recent meta-analysis by Laughlin et al., enterocolitis was the most frequent complication after pull-through arising in 42% of patients with total colonic aganglionosis [43].
Soiling and fecal incontinence are common during childhood and in adults in patients with total colonic aganglionosis. Overall, at least 30–50% of the patients with total colonic aganglionosis suffer from fecal incontinence later in childhood or adolescence [31, 32, 44, 45]. In a meta-analysis by Laughlin et al. with a mean follow-up time of 9.6 years, satisfactory or normal bowel control was reported in 60% of patients with total colonic aganglionosis, while soiling, fecal incontinence, or another poor outcome was found in 34% and 7% requiring a permanent stoma [43]. Surprisingly, in a study by Ludman in patients with total colonic aganglionosis, the continence score was not affected by the length of the aganglionosis or the length of the small bowel resection [23]. The overall mortality rate is reported as high as 20%, with pre-pull-through mortality of 16% and post-pull-through mortality of 6% [43]. Metabolic complications, nutritional deficiencies, growth retardation, and failure to thrive are well-described complications in patients with total colonic aganglionosis, which highlights the need for close multidisciplinary long-term follow-up [45,46,47].
32.5 Syndromic Hirschsprung’s Disease
Hirschsprung’s disease has been associated with numerous relatively rare syndromes which further influence the long-term outcome of these patients. Down syndrome, being the most common syndrome related to Hirschsprung’s disease, is found in 2–16% of all patients with Hirschsprung’s disease [30]. Mortality and morbidity rates are higher in Down syndrome patients with Hirschsprung’s compared to non-syndromic patients. The increased mortality rate in Down syndrome patients with Hirschsprung’s is mostly related to the frequent comorbidities, including cardiac anomalies [30, 48]. Postoperative complications, such as enterocolitis, constipation, soiling, and incontinence, are more common in Down patients with Hirschsprung’s compared to non-syndromic patients [30]. Furthermore, the overall functional prognosis is significantly inferior in Down syndrome patients than in non-syndromic Hirschsprung’s disease patients [4, 20, 30]. Down syndrome patients tend to resume bowel control much slower, and many of them, especially those with chronic enterocolitis, suffer from fecal incontinence as adolescents and adults [20]. Catto-Smith et al. reported 87% incidence of fecal incontinence among Down syndrome patients at mean age of 12 years [6].
Hirschsprung’s disease is also known to be associated with more uncommon syndromes such as Shah-Waardenburg syndrome, Mowat-Wilson syndrome, cartilage-hair hypoplasia, and hypoplastic left heart syndrome [20, 49]. Patients with Shah-Waardenburg and Mowat-Wilson syndrome are prone to enterocolitis and develop postoperative bowel control very slowly [20]. Cartilage-hair hypoplasia is a metaphyseal chondrodysplasia with growth failure, impaired immunity, and high incidence of associated Hirschsprung’s disease. Cartilage-hair hypoplasia patients with Hirschsprung’s disease have worse outcome compared to other Hirschsprung’s disease patients, including very high incidence of severe pre- and postoperative enterocolitis and increased mortality rate [50].
32.6 Hirschsprung’s Disease and Cancer
Besides causing Hirschsprung’s disease, the RET proto-oncogene germ line mutations are responsible for the development of multiple endocrine neoplasia type 2 (MEN2A) and familial medullary thyroid carcinoma [51]. The RET mutations are found in up to 50% of the familial and in 15–30% of the sporadic Hirschsprung’s disease cases [52]. On a population-based cohort study from Finland, the risk of medullary thyroid carcinoma, but no other cancers, was found to be increased in patients with Hirschsprung’s disease after mean follow-up of 30 years [53]. Virtanen et al. reported that the medullary thyroid carcinoma-associated RET mutations are restricted to exons 10 and 13 affecting ~5% of unselected adult patients with Hirschsprung’s disease [54]. Based on the known increased risk for medullary thyroid carcinoma, mutation screening for RET exons 10 and 13 may be advisable in patients with Hirschsprung’s disease, not only limited to familial or long-segment diseases [54].
32.7 Quality of Life
Quality of life can be measured in general health-related or symptom-specific measures; both are useful in assessing quality of life of Hirschsprung’s disease patients. Generic quality of life questionnaires, such as PedsQL and SF-36 health survey, help to understand general health and well-being independent of the disease and simultaneously making it possible to compare quality of life between different diseases or to healthy control subjects (Table 32.1). The symptom-specific questionnaires, such as GIQLI and FICQOL, have the advantage of focusing on specific issues relevant to a specific disease (Table 32.1). Assessing the overall quality of life is complex as the relationship between disease-specific functioning and quality of life remains unclear [55]. This highlights the need for longitudinal studies assessing the disease-specific functioning with validated age-specific quality of life questionnaires.
32.7.1 Quality of Life in Children
In contrast to earlier reports that show little or no limitations in quality of life, the recent detailed studies show on average more physical, psychosocial, and overall quality of life problems in children with Hirschsprung’s disease compared to controls, although the effects are small (Table 32.1). Collins et al. reported a good overall quality of life in children with Hirschsprung’s disease at a median age of 6 years but a reduced psychosocial quality of life compared to reference subjects [21]. In contrast, Tannuri et al. reported impaired overall quality of life in children with Hirschsprung’s disease at a median age of 8 years compared to healthy controls [22]. The effect of disease-specific symptoms, such as incontinence, soiling, and constipation, on quality of life varies between different study populations as most studies indicate a significantly reduced quality of life related to these symptoms in comparison to few studies with very little or no association [5, 6, 55, 56]. Interestingly, impaired psychosocial functioning appears to have a stronger effect on quality of life than the disease-specific symptoms [55, 56].
When comparing children and adolescents, children with Hirschsprung’s disease report better quality of life than adolescents. In contrast, adolescents reported less bowel functional problems than children. It seems, that despite less continence problems in adolescents, they are more prone to quality of life problems compared to children [55].
In a study comparing outcomes of children and adolescents with Hirschsprung’s disease or anorectal malformation, the overall quality of life was comparable between the groups [56]. In the same study, both patient groups reported more psychosocial problems in all domains compared to healthy controls [56].
32.7.2 Quality of Life in Adults
In general, adult patients with Hirschsprung’s disease report a good overall quality of life with no significant difference to healthy age-matched reference subjects [2, 25, 57, 58]. However, some patients are left with persistent impaired bowel function, such as soiling and incontinence, significantly impacting their overall and gastrointestinal quality of life [6, 59]. Gunnarsdottir et al. reported a good overall quality of life in adult patients after a Duhamel procedure [60]. In this study young females had lower overall quality of life scores compared to males or older patients [60]. Jarvi and Granstrom both reported a good overall quality of life in adults after Duhamel or Soave procedure, while impaired gastrointestinal function and gastrointestinal quality of life were more common in patients compared to controls [2, 25]. A worrying finding was that in some studies, the degree of impairment of bowel function and symptom-specific quality of life is shown to be associated with increasing age [25, 61]. This is notable as it may have a significant impact on quality of life of older patients with Hirschsprung’s disease and might impact follow-up strategies.
32.7.3 Quality of Life and the Effect of the Extent of Aganglionosis
Overall, patients with more severe forms of Hirschsprung’s disease are more prone to have reduced quality of life compared to patients with shorter segment aganglionosis [44, 60]. A significant number of patients with total colonic aganglionosis have fecal soiling, incontinence, and frequent episodes of enterocolitis extending to adulthood which may have significant psychosocial implications [23, 31, 32, 45, 46]. Gunnarsdottir et al. showed that patients with aganglionosis extending to the right colon had lower overall quality of life than patients with aganglionosis limited to the left colon [60]. Patients with more severe forms of the disease reported lower levels of perceived self-competence and global disease-specific functioning, which in turn predicted overall quality of life, in a study by Hartman et al. [56] Similarly, Ludman et al. showed that patients with total colonic aganglionosis with or without small bowel involvement have more often behavioral and emotional problems compared to patients with rectosigmoid aganglionosis [23].
32.8 Summary
The long-term outcomes of Hirschsprung’s disease have significantly improved following a better understanding of the pathophysiology and pathological anatomy of the disease and development of surgical techniques. While the treatment results have improved, it has become clear that the functional, psychosocial, and quality of life issues in children and adults with Hirschsprung’s disease need specific attention in the long term. Patients with Hirschsprung’s disease are at risk for several complications, including functional and psychosocial issues that are often passed on from childhood to adulthood and may have a significant effect on long-term quality of life. Although symptoms such as constipation, soiling, and fecal incontinence often have a tendency of improving over time, these still are commonly seen in adolescents and adults with Hirschsprung’s disease. All patients with Hirschsprung’s disease need close follow-up during childhood as well as during adulthood.
References
Neuvonen MI, Kyrklund K, Rintala RJ, Pakarinen MP. Bowel function and quality of life after transanal endorectal pull-through for hirschsprung disease: controlled outcomes up to adulthood. Ann Surg. 2017;265(3):622–9.
Granstrom AL, Danielson J, Husberg B, Nordenskjold A, Wester T. Adult outcomes after surgery for hirschsprung’s disease: evaluation of bowel function and quality of life. J Pediatr Surg. 2015;50(11):1865–9.
Wester T, Granstrom AL. Hirschsprung disease-bowel function beyond childhood. Semin Pediatr Surg. 2017;26(5):322–7.
Bjørnland K, Pakarinen M, Stenstrøm P, et al. A nordic multicenter survey of long-term bowel function after transanal endorectal pull-through in 200 patients with rectosigmoid hirschsprung disease. J Pediatr Surg. 2017;52(9):1458–64.
Khalil M. Long-term health-related quality of life for patients with hirschsprung’s disease at 5 years after transanal endorectal pull-through operation. Qual Life Res. 2015;24(11):2733–8.
Catto-Smith AG, Trajanovska M, Taylor RG. Long-term continence after surgery for hirschsprung’s disease. J Gastroenterol Hepatol. 2007;22(12):2273–82.
Bai Y, Chen H, Hao J, Huang Y, Wang W. Long-term outcome and quality of life after the swenson procedure for hirschsprung’s disease. J Pediatr Surg. 2002;37(4):639–42.
Moore SW, Albertyn R, Cywes S. Clinical outcome and long-term quality of life after surgical correction of hirschsprung’s disease. J Pediatr Surg. 1996;31(11):1496–502.
Heij HA, de Vries X, Bremer I, Ekkelkamp S, Vos A. Long-term anorectal function after duhamel operation for hirschsprung’s disease. J Pediatr Surg. 1995;30(3):430–2.
Teitelbaum D, Drongowski R, Chamberlain J, Coran A. Long-term stooling patterns in infants undergoing primary endorectal pull-through for hirschsprung’s disease. J Pediatr Surg. 1997;32(7):1049–52.
Kim AC, Langer JC, Pastor AC, et al. Endorectal pull-through for hirschsprung’s disease-a multicenter, long-term comparison of results: transanal vs transabdominal approach. J Pediatr Surg. 2010;45(6):1213–20.
Yang L, Tang S, Cao G, et al. Transanal endorectal pull-through for hirschsprung’s disease using long cuff dissection and short V-shaped partially resected cuff anastomosis: early and late outcomes. Pediatr Surg Int. 2012;28(5):515–21.
Mills JL, Konkin DE, Milner R, Penner JG, Langer M, Webber EM. Long-term bowel function and quality of life in children with hirschsprung’s disease. J Pediatr Surg. 2008;43(5):899–905.
Yanchar NL, Soucy P. Long-term outcome after hirschsprung’s disease: patients’ perspectives. J Pediatr Surg. 1999;34(7):1152–60.
Diseth TH, Bjornland K, Novik TS, Emblem R. Bowel function, mental health, and psychosocial function in adolescents with hirschsprung’s disease. Arch Dis Child. 1997;76(2):100–6.
Heikkinen M, Rintala R, Luukkonen P. Long-term anal sphincter performance after surgery for hirschsprung’s disease. J Pediatr Surg. 1997;32(10):1443–6.
Bjornland K, Diseth TH, Emblem R. Long-term functional, manometric, and endosonographic evaluation of patients operated upon with the duhamel technique. Pediatr Surg Int. 1998;13(1):24–8.
Baillie CT, Kenny SE, Rintala RJ, Booth JM, Lloyd DA. Long-term outcome and colonic motility after the duhamel procedure for hirschsprung’s disease. J Pediatr Surg. 1999;34(2):325–9.
Jarvi K, Koivusalo A, Rintala RJ, Pakarinen MP. Anorectal manometry with reference to operative rectal biopsy for the diagnosis/exclusion of hirschsprung’s disease in children under 1 year of age. Int J Colorectal Dis. 2009;24(4):451–4.
Rintala RJ, Pakarinen MP. Long-term outcomes of hirschsprung’s disease. Semin Pediatr Surg. 2012;21(4):336–43.
Collins L, Collis B, Trajanovska M, et al. Quality of life outcomes in children with hirschsprung disease. J Pediatr Surg. 2017;52(12):2006–10.
Tannuri AC, Ferreira MA, Mathias AL, Tannuri U. Long-term results of the duhamel technique are superior to those of the transanal pullthrough: a study of fecal continence and quality of life. J Pediatr Surg. 2017;52(3):449–53.
Ludman L, Spitz L, Tsuji H, Pierro A. Hirschsprung’s disease: functional and psychological follow up comparing total colonic and rectosigmoid aganglionosis. Arch Dis Child. 2002;86(5):348–51.
Reding R, de Ville de Goyet J, Gosseye S, et al. Hirschsprung’s disease: a 20-year experience. J Pediatr Surg. 1997;32(8):1221–5.
Jarvi K, Laitakari EM, Koivusalo A, Rintala RJ, Pakarinen MP. Bowel function and gastrointestinal quality of life among adults operated for hirschsprung disease during childhood: a population-based study. Ann Surg. 2010;252(6):977–81.
Conway SJ, Craigie RJ, Cooper LH, et al. Early adult outcome of the duhamel procedure for left-sided hirschsprung disease – a prospective serial assessment study. J Pediatr Surg. 2007;42(8):1429–32.
Frykman PK, Short SS. Hirschsprung-associated enterocolitis: prevention and therapy. Semin Pediatr Surg. 2012;21(4):328–35.
Swenson O, Sherman JO, Fisher JH, Cohen E. The treatment and postoperative complications of congenital megacolon: a 25 year followup. Ann Surg. 1975;182(3):266–73.
Pini Prato A, Rossi V, Avanzini S, Mattioli G, Disma N, Jasonni V. Hirschsprung’s disease: what about mortality? Pediatr Surg Int. 2011;27(5):473–8.
Friedmacher F, Puri P. Hirschsprung’s disease associated with down syndrome: a meta-analysis of incidence, functional outcomes and mortality. Pediatr Surg Int. 2013;29(9):937–46.
Wildhaber BE, Teitelbaum DH, Coran AG. Total colonic hirschsprung’s disease: a 28-year experience. J Pediatr Surg. 2005;40(1):203–6; discussion 206.
Menezes M, Pini Prato A, Jasonni V, Puri P. Long-term clinical outcome in patients with total colonic aganglionosis: a 31-year review. J Pediatr Surg. 2008;43(9):1696–9.
Dong Q, Li G, Dong J. Identification of risk factors for postoperative recurrent hirschsprung associated enterocolitis. J Pediatr Surg. 2018.
Nakamura H, Lim T, Puri P. Inflammatory bowel disease in patients with hirschsprung’s disease: a systematic review and meta-analysis. Pediatr Surg Int. 2018;34(2):149–54.
Nakamura H, Tomuschat C, Coyle D, O’Donnel A, Lim T, Puri P. Altered goblet cell function in hirschsprung’s disease. Pediatr Surg Int. 2018;34(2):121–8.
Prideaux L, Kang S, Wagner J, et al. Impact of ethnicity, geography, and disease on the microbiota in health and inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(13):2906–18.
Frykman P, Nordenskjöld A, Kawaguchi A, et al. Characterization of bacterial and fungal microbiome in children with hirschsprung disease with and without a history of enterocolitis: a multicenter study. PLoS One. 2014;10(4):e0124172.
Neuvonen MI, Korpela K, Kyrklund K, Rintala RJ, Pakarinen MP. Intestinal microbiota in hirschsprung disease. J Pediatr Gastroenterol Nutr. 2018; epub ahead of print.
Sherman JO, Snyder ME, Weitzman JJ, et al. A 40-year multinational retrospective study of 880 swenson procedures. J Pediatr Surg. 1989;24(8):833–8.
Lof Granstrom A, Amin L, Arnell H, Wester T. Increased risk of inflammatory bowel disease in a population-based cohort study of patients with hirschsprung disease. J Pediatr Gastroenterol Nutr. 2018;66(3):398–401.
Levin DN, Marcon MA, Rintala RJ, Jacobson D, Langer JC. Inflammatory bowel disease manifesting after surgical treatment for hirschsprung disease. J Pediatr Gastroenterol Nutr. 2012;55(3):272–7.
Marquez TT, Acton RD, Hess DJ, Duval S, Saltzman DA. Comprehensive review of procedures for total colonic aganglionosis. J Pediatr Surg. 2009;44(1):257–65; discussion 265.
Laughlin DM, Friedmacher F, Puri P. Total colonic aganglionosis: a systematic review and meta-analysis of long-term clinical outcome. Pediatr Surg Int. 2012;28(8):773–9.
Roorda D, Witvliet MJ, Wellens LM, et al. Long-term outcome and quality of life in patients with total colonic aganglionosis in the Netherlands. Colorectal Dis. 2018;20(8):719–26.
Escobar MA, Grosfeld JL, West KW, et al. Long-term outcomes in total colonic aganglionosis: a 32-year experience. J Pediatr Surg. 2005;40(6):955–61.
Hoehner JC, Ein SH, Shandling B, Kim PC. Long-term morbidity in total colonic aganglionosis. J Pediatr Surg. 1998;33(7):961–5; discussion 965.
Urla C, Lieber J, Obermayr F, et al. Surgical treatment of children with total colonic aganglionosis: functional and metabolic long-term outcome. BMC Surg. 2018;18(1):58–018.
Quinn FM, Surana R, Puri P. The influence of trisomy 21 on outcome in children with hirschsprung’s disease. J Pediatr Surg. 1994;29(6):781–3.
Ahola JA, Koivusalo A, Sairanen H, Jokinen E, Rintala RJ, Pakarinen MP. Increased incidence of hirschsprung’s disease in patients with hypoplastic left heart syndrome – a common neural crest-derived etiology? J Pediatr Surg. 2009;44(7):1396–400.
Makitie O, Heikkinen M, Kaitila I, Rintala R. Hirschsprung’s disease in cartilage-hair hypoplasia has poor prognosis. J Pediatr Surg. 2002;37(11):1585–8.
Asai N, Jijiwa M, Enomoto A, et al. RET receptor signaling: dysfunction in thyroid cancer and hirschsprung’s disease. Pathol Int. 2006;56(4):164–72.
Amiel J, Lyonnet S. Hirschsprung disease, associated syndromes, and genetics: a review. J Med Genet. 2001;38(11):729–39.
Pakarinen MP, Rintala RJ, Koivusalo A, Heikkinen M, Lindahl H, Pukkala E. Increased incidence of medullary thyroid carcinoma in patients treated for hirschsprung’s disease. J Pediatr Surg. 2005;40(10):1532–4.
Virtanen VB, Pukkala E, Kivisaari R, et al. Thyroid cancer and co-occurring RET mutations in hirschsprung disease. Endocr Relat Cancer. 2013;20(4):595–602.
Hartman EE, Oort FJ, Aronson DC, Sprangers MA. Quality of life and disease-specific functioning of patients with anorectal malformations or hirschsprung’s disease: a review. Arch Dis Child. 2011;96(4):398–406.
Hartman EE, Oort FJ, Sprangers MA, et al. Factors affecting quality of life of children and adolescents with anorectal malformations or hirschsprung disease. J Pediatr Gastroenterol Nutr. 2008;47(4):463–71.
Onishi S, Nakame K, Kaji T, et al. The bowel function and quality of life of hirschsprung disease patients who have reached 18 years of age or older - the long-term outcomes after un... - PubMed - NCBI J Pediatr Surg. 2017;52(12):2001–5.
Heikkinen M, Rintala R, Louhimo I. Bowel function and quality of life in adult patients with operated hirschsprung’s disease. Pediatr Surg Int. 1995;10:342–4.
Ieiri S, Nakatsuji T, Akiyoshi J, et al. Long-term outcomes and the quality of life of hirschsprung disease in adolescents who have reached 18 years or older – a 47-year single-institute experience. J Pediatr Surg. 2010;45(12):2398–402.
Gunnarsdottir A, Sandblom G, Arnbjornsson E, Larsson LT. Quality of life in adults operated on for hirschsprung disease in childhood. J Pediatr Gastroenterol Nutr. 2010;51(2):160–6.
Hartman EE, Oort FJ, Visser MR, et al. Explaining change over time in quality of life of adult patients with anorectal malformations or hirschsprung’s disease. Dis Colon Rectum. 2006;49(1):96–103.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Mutanen, A., Pakarinen, M.P., Rintala, R.J. (2019). Long-Term Outcome and Quality of Life After Treatment of Hirschsprung’s Disease. In: Puri, P. (eds) Hirschsprung's Disease and Allied Disorders. Springer, Cham. https://doi.org/10.1007/978-3-030-15647-3_32
Download citation
DOI: https://doi.org/10.1007/978-3-030-15647-3_32
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-15646-6
Online ISBN: 978-3-030-15647-3
eBook Packages: MedicineMedicine (R0)