
Abstract
Neonatal hypertension as a clinical entity has been recognized since the 1970s (Adelman Ped Clin North Am 25(1):99–110, 1978), and yet we still do not have a complete understanding of the physiologic blood pressure changes occurring over the first year of life. Measurement techniques have evolved to less-invasive blood pressure monitoring in a population with increasing complexity related to technologic advances. This chapter will focus on proper assessment of infant blood pressure, expected changes in blood pressure during the first year of life, as well as evaluation, management, and follow-up of neonatal and infant hypertension.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Measurement of Blood Pressure
The gold standard blood pressure measurement technique in neonates is direct intra-arterial monitoring. Common sites for catheterization in neonates are the umbilical artery and radial or posterior tibial arteries, which have all demonstrated comparable blood pressure values in this population [2]. Direct intra-arterial monitoring may be necessary in the most acutely ill neonates although there has been a shift to noninvasive blood pressure monitoring for the majority of the neonates within a neonatal intensive care unit (NICU). Indirect methods for measuring blood pressure include ultrasonic Doppler and oscillometric methods. Palpation and auscultation using a sphygmomanometer are not practical within the NICU setting but may be used in older infants in a clinic setting. Ultrasonic Doppler assessment involves inflation then deflation of a sphygmomanometer with detection of blood flow or motion of the vessel wall with a Doppler device. With experienced users, the systolic blood pressure can easily be detected, but diastolic blood pressure is often unmeasurable. The technique that has become more common within the NICU and follow-up clinics is the oscillometric method. A blood pressure cuff inflates above systolic blood pressure, and then as it deflates, the oscillometric device detects the pressure oscillations within the artery determining the mean arterial pressure (MAP) when the oscillations are maximal. The machine then uses an algorithm specific to each device to calculate systolic and diastolic blood pressure. When oscillometric blood pressures were compared to radial arterial blood pressures in infants and children, there was good correlation between the two methods, and the oscillometric readings were better than values determined by auscultation [3]. Even in premature infants, these noninvasive blood pressures correlate well with intra-arterial monitoring [4].
As each oscillometric blood pressure monitor uses independent algorithms for determination of blood pressure values, several studies have compared multiple devices for accuracy. Dannevig and colleagues compared three monitors: Dinamap Compact™, Hewlett-Packard™ (HP), and Criticare™ models. When compared to intra-arterial blood pressures, they found that the HP model had lower values than invasive monitoring while the Dinamap™ and Criticare™ tended to read higher and that the deviance was dependent on the size of the infant [5]. The HP™ showed lower values in the larger infants, while the Criticare™ and Dinamap™ values were too high in the smallest infants which could lead to under-recognition of hypotension. Another study comparing three oscillometric devices to intra-arterial monitoring found that all three devices overestimated mean blood pressure by 3.3–8.4 mmHg [6]. Oscillometric devices overestimating low blood pressure were confirmed in a study of critically ill premature neonates that showed good correlation of invasive and noninvasive mean blood pressures except when the MAP was less than or equal to 30 mmHg where the oscillometric device readings were too high leading to potential under-recognition of hypotensive events [7].
Other less common methods of blood pressure measurement have been used by practitioners experienced in the techniques. A recent study compared blood pressure values by oscillometry, flush method, and pulse oximetry to Doppler ultrasound and found the best correlation with flush method and pulse oximetry [8]. Another area of debate within some NICU settings is around the use of calf blood pressure measurements. Systolic blood pressure by calf measurements is slightly lower but similar to arm measurements until about 6 months of age when the calf pressures begin to exceed arm blood pressures [9]. Unfortunately, the calf blood pressure values show more variability than arm blood pressures and therefore should only be used in exceptional circumstances when arm blood pressure values are not feasible prior to 6 months of age and not used after 6 months of age.
The state of the infant at the time the blood pressure is being measured is important and can influence the blood pressure value. Early observations of blood pressures in neonates showed that the blood pressure was lower when the neonate was in deep sleep and rose above baseline when crying, being held head up, and during feeding [10]. The elevation of blood pressure with feeding is relatively consistent with an increase of up to 20 mmHg. This observation has been confirmed in more recent studies with neonates within the first days of life having blood pressures increasing significantly during feeding, and the magnitude of elevation may be influenced by the volume of fluid intake within the first few minutes of feeding [11]. In follow-up clinics of infants and children 1–3 years of age, the non-calm state has been associated with significantly higher blood pressures (17–30 mmHg higher) than when the infant is calm [12]. It is sometimes necessary to attempt blood pressures on several occasions or in different settings in order to achieve an accurate calm measurement.
Accurate blood pressure measurement is important in neonates and infants, especially when blood pressure assessment factors into clinical decision making. Some authors suggest that the median of three oscillometric blood pressure measurements should be used [13] while others state that one blood pressure during routine vitals is adequate, in calm healthy term newborns [14]. The cuff size is critically important to accurate blood pressure measurement, and the cuff width/arm circumference ratio should be between 0.45 and 0.70 [15]. Use of a standard protocol for newborn blood pressure measurement has been suggested by Nwankwo and colleagues [16] (see Table 26.1). They found in infants weighing less than 2,500 g, when compared to routine nursing care, standardized blood pressures were significantly lower and showed less variability. In addition, the first blood pressure reading was significantly higher than the third reading. Other than waiting for one and a half hours after a feed or medical intervention to take a blood pressure reading, the protocol is reasonable for use within the NICU setting, especially when clinical assessment and decisions are being based on the blood pressure values.
Factors Influencing Blood Pressure
Various factors, both extrinsic (maternal) and intrinsic (infant), can influence newborn blood pressure values, and while this is discussed in more detail in Chap. 7 on Perinatal Programming, it also deserves brief mention here. Maternal blood pressure and/or hypertension have been related to higher newborn blood pressures in several studies [17–19]. In an early study, a significant correlation was found for blood pressure of maternal-infant pairs after delivery and at 1 year of age [20]. Maternal age has been positively correlated with newborn blood pressure in one study [17] but not consistently in other studies [21, 22]. Maternal diabetes may be related to higher newborn blood pressure especially when born earlier in gestation [19]. The effect of maternal smoking on infant and childhood blood pressure are conflicting, but a more recent birth cohort study demonstrated male infants of maternal smokers had blood pressures more than 8 mmHg higher than maternal nonsmokers, although the increase was not seen in female offspring [23]. The prenatal exposure to “second-hand smoke” seems to lead to alterations in infant circulatory control mechanisms [24]. In a Nigerian study of term neonates, maternal body mass index > 30 and low socioeconomic status were associated with higher newborn systolic blood pressure, although birth weight was still the strongest predictor of neonatal blood pressure [22]. Likely, even maternal nutritional intake has an effect on infant blood pressure, and early findings suggest a u-shaped curve for infant blood pressure at 6 months of age and maternal carbohydrate intake with the highest blood pressures in infants whose mothers’ carbohydrate consumption was in the lowest and highest quartiles of intake [25]. Maternal protein intake does not seem to have the same effect [26].
Perinatal events may also influence newborn blood pressures with the most controversial being antenatal steroids administered during threatened preterm delivery. Antenatal steroids given within 7 days of birth can reduce respiratory distress syndrome, but the effect on newborn blood pressure has been controversial, with some studies finding higher newborn blood pressures [18, 27], while others did not [28, 29]. A recent randomized double-blind, placebo-controlled trial showed no difference in newborn blood pressures in infants that were exposed to repeated doses of prenatal corticosteroids compared to single dose [30]. As antenatal steroids may have an effect on function of the infant hypothalamic-pituitary-adrenal axis, the way in which the placenta handles the steroids seems to also play a role in how steroids may influence infant blood pressure [31]. Maternal hemolysis, elevated liver enzymes, and low platelets or HELLP syndrome have been associated with lower blood pressures in neonates [27]. Even the mode of delivery and type of maternal anesthetic may have an impact on newborn blood pressures, with elective caesarean section and spinal anesthesia being related to lower systolic blood pressures in newborns [21].
The most strongly correlated intrinsic or infant factors consistently associated with newborn blood pressure are birth weight and gestational age. The earlier in gestation that the neonate is born, the lower the expected initial blood pressure values with essentially a linear relationship demonstrating lower newborn blood pressure with lower gestational age [32, 33]. This same relationship has been shown for birth weight and blood pressure as most neonates who are born premature are also born at a low birth weight, but being born small for gestational age may also be associated with lower initial blood pressure values [32–34]. Congenital renal, cardiac, or endocrine anomalies may influence blood pressure and are associated with a higher prevalence of neonatal hypertension. The influence of fluid volume and vasoactive substances on neonatal blood pressure is demonstrated in infant pairs of twin-twin transfusion syndrome where newborn blood pressures in recipients are significantly higher than donors [35]. In fact, 14 % of twin-twin transfusion recipients are hypertensive.
Not surprisingly, genetics also likely plays a role in which infants develop hypertension. Cytochrome P450 CYP2D6 ‘CC’ genotype was associated with increased risk of elevated blood pressure in infants born less than 32 weeks gestation during neonatal and follow-up periods [28]. Likely all these various factors, including antenatal and postnatal exposures, cumulative time with the exposure, gestational age, clinical condition, and genetic predisposition, interact in complex ways to influence neonatal blood pressures.
Normative Data
Day 1 of Life
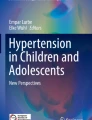
Newborn blood pressure on the first day of life is strongly positively correlated with both birth weight and gestational age. The Philadelphia Neonatal Blood Pressure Study Group clearly demonstrated this correlation when they studied all infants admitted to 14 level III NICUs and analyzed blood pressure values of over 300 infants on day l of life [32]. Their blood pressure nomograms have been the most widely used reference values, but similar to the blood pressure standards used in older children, the preference should be to use reference values determined from stable neonates as a better predictor of what is expected in healthy newborns. A more recent study of almost 400 hemodynamically stable infants has shown a similar correlation of gestational age and birth weight with blood pressure in neonates on day 1 of life, presented with 95 % confidence limits, which may be a better reference for newborn blood pressure values [33] [see Fig. 26.1].

Neonatal blood pressure on day 1 of life is positively correlated with birth weight (1) and gestational age (2). Systolic (a), diastolic (b), and mean (c) blood pressures are presented with 95 % confidence limits (Reproduced from Pejovic et al. [33] with kind permission from Springer Science + Business Media)
First Days of Life
In very low birth weight infants (VLBW), systolic, diastolic, and mean blood pressure increase by more than 30 % over the first few days of life which demonstrates the physiologic changes that occur as neonates adapt to the ex utero environment [29]. The mechanisms responsible for these dramatic changes are still being determined, but likely involve loss of vasodilator substances important during the in utero environment and maturation of factors controlling vascular tone [29, 36]. The Philadelphia study showed that all infants in the NICU, regardless of gestational age, have a rapid increase in blood pressure over the first 5 days of life with increments around 1.5–2.5 mmHg/day [32]. This differs from healthy term infants on the postnatal ward where blood pressure values are higher on day 2 compared to day 1 of life but not consistently thereafter [37].
First Weeks of Life
In the first weeks of life, the rate of blood pressure change and the length of time over which the blood pressure is rapidly increasing may differ based on gestational age at birth or birth weight. The study by Pejovic and colleagues found that the neonates with the lowest gestational age at birth had the most rapid rate of rise of blood pressure with an average increase in mean blood pressure of 26 % in the first week and 51 % in the first month in infants born at less than 28 weeks gestational age compared to 13 % and 22 % in full-term infants [33]. Another study of stable premature infants showed that the infants born at 28–31 weeks gestational age had a significant increase in blood pressure over the first 2–3 weeks of life, while the infants born at 32–36 weeks gestational age had a rapid increase in blood pressure over only 1 week [38]. The authors suggested that the blood pressure values at the end of the rapid increase were similar to term infants in the first days of life.
These studies are consistent with an earlier study that determined VLBW infants had similar blood pressure values to other NICU graduates at 4 months corrected age despite remaining smaller in length and weight [39]. As blood pressures were not measured between discharge and 4 months of age, we do not know when the catch-up occurred. The appropriateness of weight at birth and blood pressure was assessed in a study of full-term newborns whose birth weights varied from < 2,500 to > 3,500 g [34]. They found that the term infants with the lowest birth weights had the lowest blood pressures initially but then had the most rapid rate of rise of blood pressure so that by 1 month of age, all term infants had similar blood pressures that remained comparable throughout the first year of life. This multitude of variations in blood pressure patterns over the first weeks of life is represented in Fig. 26.2

Illustration of patterns of neonatal blood pressure changes when born at term or premature, extremely premature, or small for gestational age (SGA)
Infant blood pressures have also been described as increasing with postconceptional age (gestational age plus postnatal age) which is now referred to as postmenstrual age. The Philadelphia Study Group developed a clinically useful graphical reference of blood pressure by postconceptual age to be used in neonates after the first day of life while still in the neonatal and early infant period [32]. Recognizing that infant blood pressures over the first 2 weeks are rapidly changing and could influence nomograms by postmenstrual age, we recently derived normative values for infant blood pressures after 2 weeks of life based on current postmenstrual age from the available published literature [40, 41] [see Table 26.2]. 95th and 99th percentiles were calculated as a reference for clinicians to use to determine which infants may require treatment (discussed in more detail later in this chapter).
First Year of Life
Blood pressure changes over the first year of life are less marked than in the newborn period. Blood pressure values increase steadily until 3–6 months of age at which time the values remain stable up to 1 year of age. The most widely used nomograms for infant blood pressure come from the Report of the Second Task Force on Blood Pressure from the 1980s [42] [see Fig. 26.3]. Unfortunately, the infant blood pressures were measured using the Doppler method, which likely provides slightly lower readings than by the oscillometric method commonly used today. As well, the diastolic blood pressures are less likely to be reliably determined with Doppler method so that the number of readings is less than systolic, although this reference still provides data based on the largest number of infants to date (systolic n = 7,643, diastolic n = 3,048). A more recent study of over 400 healthy term infants whose blood pressures were measured by oscillometric method shows a similar trend in blood pressure values over the first year of life [43] [see Fig. 26.4]. The blood pressures were only measured on day 2 of life, at 6 and 12 months of age and therefore do not provide normative data for ages in between, but the advantage is that the blood pressures were measured using the most commonly used method today. Large-scale studies of oscillometric blood pressure values over the first year of life are desperately needed.

Blood pressure percentiles for (a) male infants and (b) female infants from birth to 12 months of age (Reprinted from the Task Force on Blood Pressure Control in Children [42])

Healthy term infant blood pressure values by oscillometric method at 2 days, 6 months, and 12 months of age. Diastolic (blue), mean (red), and systolic (green) values are indicated with the median (horizontal bar) and 5th to 95th percentiles (box) (Reproduced from Kent et al. [43] with kind permission from Springer Science + Business Media)
Definition of Hypertension
Various definitions of infant hypertension have been used since high blood pressure was recognized as an issue in neonates and infants. This has made the comparison of studies and the determination of the incidence of hypertension challenging. Earlier studies used set blood pressure values for all term or preterm infants, but as we now know, values vary based on factors such as gestational age, birth weight, and postnatal age. As studies were published of normative values with percentiles, such as Zubrow and the Philadelphia Neonatal Blood Pressure Study Group or the Second Task Force Report on Blood Pressure, then clinicians applied the concepts used in studies of older children and adopted the 95th percentile blood pressure as the definition of hypertension [32, 42]. Unfortunately, we do not have outcome studies in infants to support or refute the use of this arbitrary definition of hypertension although in the future this may come from the neurocognitive or cardiovascular literature [44, 45]. In addition, the use of antihypertensive medications in the neonatal and infant population is associated with defined risks, and very few studies have been completed on use of blood pressure medications in this population. Therefore, at this time the best recommendation for definition of hypertension in neonates would be blood pressure values consistently above the 95th percentile based on postmenstrual age [41] [see Table 26.2]. In infants, blood pressure values consistently above the 95th percentile based on curves from the Second Task Force on Blood Pressure [see Fig. 26.3] or oscillometric values from the study by Kent and colleagues [see Fig. 26.4] should be considered as hypertension and investigated and managed as appropriate [42, 43].
Incidence of Hypertension
The incidence of hypertension in general healthy newborns is low, likely around 0.2 %, and routine screening of blood pressure is recommended only in infants considered “at risk” which includes NICU graduates, infants with congenital heart or kidney disease, or with other childhood diseases [46, 47]. In one of the first studies of neonatal hypertension, Adelman found an incidence of 2.5 % of NICU infants when hypertension was defined as a blood pressure > 90/60 mmHg in term infants or > 80/45 mmHg in preterm infants [1]. Other NICU studies have found a lower incidence between 0.7 % and 0.8 % [48, 49]. A recent Australian study of all newborns admitted to a tertiary level NICU found an incidence of neonatal hypertension of 1.3 % when more than 2,500 infants were reviewed [18]. The median gestational age of these infants was 34 weeks, and the hypertension was diagnosed on average at postnatal day 5 although the range was 2–144 days. This is similar to an earlier study with a mean age of onset of 11 days suggesting that many infants that will develop hypertension do so within the first 1–2 weeks of life [48]. A recent large database study of more than 120,000 NICU encounters found an incidence of hypertension of 1.7 % in all patients, and 1.0 % after infants with congenital cardiac disorders were excluded [50]. It is interesting that the incidence does not seem to be increasing despite the increasing complexity of patients within the NICU. It may be more likely that the incidence of hypertension in this population will be higher during adolescence and adulthood.
Risk Factors for Hypertension
Various factors have been associated with an increased risk for hypertension in neonates. It is important to recognize that risk factors may not be equivalent to causes of hypertension as the data may come from sources where a primary cause of the hypertension was not able to be determined, as in a database, or multiple factors may have contributed to the development of hypertension in an individual patient. Also, the risk factor itself may not have been the cause of the hypertension but may be a surrogate for the state or condition of the infant. In an earlier study by Singh and colleagues, risk factors for hypertension included use of an umbilical artery catheter (UAC), chronic lung disease, patent ductus arteriosus, and intraventricular hemorrhage [49]. In the Australian study mentioned previously, risk factors for hypertension included acute renal failure, UAC, maternal hypertension, antenatal steroids, and lower gestational age with 76 % of the neonates with hypertension being premature [18]. In the large database study by Blowey and colleagues, the risk of hypertension was higher in infants with acute or chronic renal failure, congenital anomalies of the kidneys and urinary tract, intraventricular hemorrhage, neonatal asphyxia, seizures, necrotizing enterocolitis, UAC, and lower birth weight, and in those infants requiring extracorporeal membrane oxygenation (ECMO) [50]. Hypertension was also more common in infants with a higher severity of illness score, those with more coexisting diagnoses, longer lengths of hospital stay, and in infants that expired before discharge reflecting a more complex and ill population.
Causes of Hypertension
The most common etiologies of neonatal hypertension are renovascular and renal parenchymal disease, accounting for 50 % of cases [49] [see Table 26.3]. The most common renovascular causes include renal artery thrombosis, renal artery stenosis, and renal vein thrombosis (RVT), all of which may be idiopathic but are more often related to use of umbilical catheters. Renal parenchymal causes may be intrinsic conditions such as polycystic kidney disease or renal dysplasia, may be related to urologic abnormalities such as ureteropelvic junction obstruction or obstructive uropathy, may be acquired conditions such as acute tubular necrosis or cortical necrosis, or rarely monogenic forms of hypertension.
The association between UACs and renal artery thrombosis has been recognized for decades [1]. The mechanism is likely related to disruption of the vascular endothelium by the catheter with subsequent development of thrombus and an associated risk of clot extension or release of emboli. The incidence of clot formation associated with umbilical catheters differs widely depending on decade of screening and method of detection. An early study of randomly selected infants found a 95 % incidence of clots associated with low thoracic UACs on aortograms [51]. Seibert and colleagues studied neonates with lower placement of UACs and found 26 % had an aortic thrombus by ultrasound, of which 29 % were asymptomatic, 24 % presented with hematuria, and 24 % had hypertension [52]. A recent Cochrane review of morbidity associated with UAC placement found high-placed UACs were associated with a lower incidence of clinical ischemic complications, but based on limited studies, it seems that hypertension and hematuria do not differ based on catheter position [53].
Renal artery thrombosis is most commonly associated with use of UACs, and infants may present with a sudden increase in blood pressure. The incidence of hypertension in infants with a UAC has been reported between 1.6 % and 8.8 % [18, 49, 50]. In the study by Singh and colleagues, 35 % of hypertensive infants with a UAC had associated thrombocytopenia and 25 % had lower limb ischemia [49]. When investigating for this complication, it is important to realize that when clots are found, they are often extending into or originating from the aorta, but sometimes no clots will be found on imaging when the infant is hypertensive, suggesting either the clot has resolved, emboli occluded peripheral renal arteries, or the UAC caused renal arterial spasm or stenosis [54]. Renal venous thrombosis classically presents with gross hematuria, a palpable abdominal mass, and thrombocytopenia and is often associated with hypertension and acute renal failure. Risk factors for RVT include birth asphyxia, maternal diabetes, hypovolemia, sepsis, and indwelling catheters. Most RVTs present within the first 3 days of life and over 70 % are unilateral with a predominance for the left kidney and male infants [55, 56].
Renal arterial stenosis may be a complication of a UAC, or it may be related to fibromuscular dysplasia, mid-aortic syndrome, or external compression by a mass, or, less commonly in infants, associated with a vasculitis or disease syndrome such as neurofibromatosis or Williams’ syndrome [57] [see Fig. 26.5]. Other uncommon causes associated with renal artery stenosis include congenital rubella syndrome, renal myofibromatosis, and idiopathic arterial calcification of infancy [58–60]. Renal artery stenoses are most commonly unilateral if idiopathic or related to catheters but more commonly bilateral if related to syndromes or other disease processes.

Renal angiogram demonstrating renal artery stenosis of a second-order renal artery branch with poststenotic dilation (Reproduced from Vo et al. [108] with kind permission from Springer Science + Business Media)
In hypertensive neonates within the NICU, between 25 % and 40 % will have a renal abnormality on ultrasound [18, 49]. Lanzarini and colleagues studied nephro-urologic malformations in a tertiary care hospital and found an incidence of 0.89 % in all infants, with almost 20 % of affected neonates developing hypertension during the newborn period [61]. Congenital renal diseases associated with hypertension include polycystic kidney disease (both autosomal dominant and recessive) and renal dysplasia in isolation or associated with urologic abnormalities such as posterior urethral valve or vesicoureteral reflux, renal hypoplasia, multicystic dysplastic kidney, congenital or infantile nephrotic syndrome, and uncommonly renal tubular dysgenesis or atypical hemolytic uremic syndrome. Autosomal recessive polycystic kidney disease is more often presenting during the neonatal period in the recent decades [62] [see Fig. 26.6]. The median age at diagnosis of hypertension in these patients is 16 days old, and hypertension is common in infants also presenting with hyponatremia which may reflect severe tubular dysregulation. The hypertension may be challenging to treat and often requires multiple agents [62]. Even autosomal dominant polycystic kidney disease, where complications are less common during childhood, can cause hypertension in infants less than 1 year of age [63]. Multicystic dysplastic kidneys rarely cause hypertension as they are thought to be nonfunctional but in some cases seem to have just enough renal blood flow or function to cause severe hypertension, likely renin mediated, and in these cases the hypertension resolves after nephrectomy [64]. Renal dysplasia may be associated with hypertension and is common in obstructive uropathies such as posterior urethral value and prune belly syndrome but may not be seen in obstruction due to stones or tumors if the obstruction occurs after completion of renal development. Ureteropelvic junction obstruction has been associated with neonatal hypertension where correction of the abnormality is curative in most although infant pyeloplasty has also been related to a postoperative hyperreninemic hypertension [65]. Other urologic abnormalities associated with infant hypertension include megaureter and neurogenic bladder, often in infants with a meningomyelocele [61, 66].

Renal ultrasound image demonstrating an enlarged echogenic kidney with lack of corticomedullary differentiation and numerous microcysts consistent with autosomal recessive polycystic kidney disease
Acquired renal causes of infant hypertension are less common but may include acute tubular necrosis related to moderate hypoxic, hypotensive, or nephrotoxic injury to the kidneys or if more severe injury, kidneys may develop cortical necrosis. Other acquired causes of renal parenchymal disease and infant hypertension include pyelonephritis, interstitial nephritis, and nephrocalcinosis [48, 67, 68]. Rare heritable forms of hypertension such as Liddle syndrome, apparent mineralocorticoid excess, and glucocorticoid-remediable aldosteronism may present during infancy, and clinical suspicion based on family history and/or suppressed plasma renin is important to diagnose these rare causes as treatments are directed at the specific underlying pathophysiology [69, 70].
Coarctation of the thoracic aorta may present with infantile hypertension and should be suspected in the presence of discrepant arm and leg pulses, perfusion, or blood pressures and a cardiac murmur. Hypertension, as determined by a right upper arm blood pressure measurement, is present in 85 % of children with aortic coarctation and persisted in 38 % of infants after surgical repair [71]. This group is also at risk of restenosis and recurrent hypertension during childhood, and therefore, these children need careful long-term follow-up as systolic blood pressure has been correlated with residual obstruction and may be a clue to persistent stenosis [72]. Patent ductus arteriosus (PDA) as well as closure of the PDA have been associated with neonatal hypertension [1, 49]. The mechanism of the PDA-related hypertension has been suggested to be renal microthrombosis with the PDA as the nidus, while closure of the PDA and hypertension could be related to the use of nonsteroidal anti-inflammatory drugs or the sudden increase in blood volume through the aorta.
ECMO deserves mention as a newer cause of infant hypertension as the technology becomes more widely utilized. An early study showed an incidence of 88 % hypertension in infants on ECMO, when hypertension was defined as systolic blood pressure greater than 90 mmHg, and 44 % of infants developed intraventricular hemorrhage [73]. In this study, 15 % of infants still required some form of antihypertensive medication 1 month after ECMO. Other studies have found the incidence of hypertension to vary between 58 % and 94 %, but fewer hypertensive infants (0–5 %) developed intracranial hemorrhage [74, 75]. A more recent review of 500 neonates treated with ECMO demonstrated that hypertension is the most common cardiovascular complication, occurring in almost 40 % of infants, but when aggressively treated with vasodilators did not adversely affect survival [76]. The mechanisms are thought to involve alterations in the baroreflex and modulation of hormones [77].
Chronic lung disease or bronchopulmonary dysplasia is another common cause of infant hypertension although it may present at neonatal follow-up clinics rather than during NICU admission. Of infants requiring home oxygen therapy for chronic lung disease, the incidence of hypertension during the first year of life has been reported from 12 % to 43 % with an average age of onset of 3.5–5.9 months with approximately half of cases occurring after discharge from the NICU [78–80]. In addition, some infants with chronic lung disease, or at risk of developing chronic lung disease, are treated with corticosteroids or other medications for a period of time which can cause or exacerbate hypertension [81].
Infant hypertension may also be found in disorders of the neurologic and endocrine systems as well as in association with various tumors. Pain and seizures may both lead to elevations in blood pressure, but management should be directed at the underlying stimulus and antihypertensive medications will likely not be necessary [82]. Hypertension occurs in about 3 % of infants with intraventricular hemorrhage [49, 50]. Premature neonates are at particular risk due to the delicate germinal matrix in the brain, and intracranial hypertension may also develop after neonatal asphyxia [83]. Unfortunately, the clinical signs of systemic hypertension and intraventricular hemorrhage may be indistinguishable and include irritability, lethargy, apnea, hypotonia, seizures, and coma [1]. In these situations, appropriate imaging studies may evaluate for central nervous system causes or complications of the high blood pressure.
Although rare, the most commonly associated endocrine etiology for neonatal hypertension is congenital adrenal hyperplasia related to deficiencies in either 11β-hydroxylase or 17α-hydroxylase leading to over production of deoxycorticosterone which has mineralocorticoid activity [84, 85]. Other endocrine causes of hypertension include Cushing’s syndrome, neonatal hyperthyroidism, hyperaldosteronism, and pheochromocytoma [86–89]. Several neoplastic causes of infant hypertension have been recognized including Wilms tumor, neuroblastoma, and mesoblastic nephroma which may all present during infancy [90–94]. The mechanisms for the hypertension may include hyperreninemia related to renal parenchymal compression, renin release by the tumor, compression of the renal vasculature by the mass, or release of catecholamines by the tumor.
Various other causes of neonatal and infant hypertension have been recognized, many of which are iatrogenic. Certain medications or drugs may cause infant hypertension and may be related to maternal ingestion, as in cocaine or heroin abuse, or medications may be prescribed to infants within the NICU for a specific indication [95, 96]. Infants with chronic lung disease may be treated with corticosteroids, caffeine, or theophylline, all of which may lead to hypertension [97, 98]. Vitamin D intoxication has been associated with infant hypertension although it is not clear if this is related to hypercalcemia or some other mechanism [46]. Excess saline administration or salt intake may increase blood pressures in neonates [46, 99]. Total parenteral nutrition has also been related to hypertension with the suspected mechanism either salt and water overload or hypercalcemia. Many of these iatrogenic causes of infant hypertension are based on clinically important indications, but when high blood pressures develop, the risk-benefit ratio must be reevaluated to determine if the medication or agent is still deemed essential.
Diagnostic Evaluation
Many infants with hypertension are asymptomatic, and common symptoms are often nonspecific such as feeding intolerance, vomiting, irritability, or failure to thrive. In those with more obvious symptoms, cardiovascular signs related to the blood pressure can include tachypnea, respiratory distress, and congestive heart failure [1]. In some infants who present with cardiogenic shock, the elevated blood pressure is not detected until after the child is resuscitated and cardiac function improves [100]. Neurologic symptoms may be indistinguishable from intracranial hemorrhage and may include lethargy, apnea, tremors, opisthotonus, facial palsy, hemiplegia, seizures, and coma [1, 101]. Infants may be oliguric or polyuric with renal parenchymal or renovascular abnormalities [46]. Clinical signs and symptoms may provide clues to both the severity and the cause of the elevated blood pressure.
The infant’s medical history should be reviewed for prenatal exposures, complications of delivery, perinatal course including use of invasive monitoring (umbilical lines), comorbid conditions, and current and previous medications. Family history may be helpful particularly when other newborns have had complications in early life or when there is a history of hypertension at a young age. Fortunately, for infants within the NICU, review of the patient chart often reveals the likely cause or several contributing factors to the development of the hypertension.
The initial step in physical evaluation of the infant is to confirm the blood pressure elevation by using a standardized blood pressure measurement technique [see Table 26.1] and ensuring the proper cuff size is used. Blood pressures and pulses should be assessed in all four limbs with discrepancies suggestive of coarctation, stenoses, or thromboses. The general condition of the infant should be noted including hydration status and dysmorphic features. Further examination should focus on the differential diagnosis [see Table 26.3] as well as looking for signs of end organ damage including cardiac and neurologic abnormalities. Although procedurally challenging, signs of hypertensive retinopathy may be present even in neonates with hypertension [102]. Abdominal examination is critical in these infants and should include inspection, auscultation for bruits, and palpation of the size and symmetry of the kidneys and detection of masses.
Investigations should be tailored to the degree of hypertension and information gathered on history and physical examination. Basic laboratory investigations could include urinalysis, serum electrolytes, blood urea nitrogen, creatinine, and complete blood count [see Table 26.4]. Renal ultrasound with Doppler is a high yield initial investigation in this population. Renal parenchymal abnormalities, such as polycystic kidney disease and renal dysplasia, and structural abnormalities, such as ureteropelvic junction obstruction, are easily diagnosed with basic renal ultrasonography. It is important to note that renal echogenicity and corticomedullary differentiation are relatively increased in neonates [103], and therefore, interpretation should be conducted by radiologists with experience in pediatrics. Renovascular abnormalities may be suspected on ultrasound when there is abnormal renal size or echogenicity, but Doppler imaging is better at identifying a thrombus or stenosis, although lack of vascular anomaly with Doppler ultrasound does not exclude a renovascular cause.
Echocardiography in infants with hypertension may help with diagnosis if cardiac abnormalities are identified but may also demonstrate evidence of target organ damage with left ventricular hypertrophy or congestive heart failure. In infants presenting with heart failure of unknown etiology, hypertension as a cause may be suspected by reduced left ventricle systolic function without chamber enlargement, increased left ventricular mass, diastolic dysfunction without left atrial dilatation, and aortomegaly with Doppler suggestive of increased vascular resistance [104]. Infants may not be hypertensive at presentation when cardiac function is compromised but develop high blood pressure as cardiac function improves, although afterload reduction may improve both blood pressure and cardiac function [104].
Plasma renin or plasma renin activity may be difficult to interpret with limited normal reference values available for neonates. In addition, various measurements have been used including direct renin, plasma renin activity, and active renin mass with differences in normal values for the different assays. A newborn’s renin is higher following a vaginal delivery and higher in preterm than term infants [105, 106]. In term infants, renin is highest in the first 4 days of life and then levels decrease over the following weeks to months to values similar to older children [105]. A suppressed plasma renin may be suggestive of a monogenic form of hypertension, while an elevated renin may suggest a renal stenosis or thrombosis although it is important to note that a normal plasma renin is common even in the presence of a renovascular abnormality so clinicians need to be aware of the limitations of this test [107].
When renovascular hypertension is suspected, angiography may be the best investigation but is not always feasible. A review of renal angiography in a select group of hypertensive children without comorbid conditions revealed that 90 % had a single stenosis with only 25 % in the main renal artery, 50 % in a second order renal artery, and the remainder in more distal branches or accessory vessels indicating the importance of angiography for detection of most renal artery stenoses [108] [see Fig. 26.5]. Digital subtraction angiography is the most accurate for detection of arterial stenoses, and although it is invasive, it may be combined with differential renal vein renin sampling which may be helpful to localize the lesion and guide surgical management [57, 107]. Unfortunately, these procedures require a general anesthetic and may be technically challenging in small infants, and therefore, infants are often managed medically until they achieve a size where the procedure is technically feasible. Other imaging techniques include computed tomography angiography or magnetic resonance angiography, although they are not good at detection of intrarenal vascular anomalies which are often present in infants [103]. Consideration must also be given to a prothrombotic workup in infants with proven thromboses as clotting factor abnormalities are common in infants with renal vein thrombosis regardless of other predisposing perinatal conditions [56, 109].
Management
Hypertensive crises are life-threatening emergencies that require prompt and careful management to avoid complications either of the hypertension or of the treatment and therefore are best managed within an intensive care setting with intravenous (IV) short-acting antihypertensive agents. Blood pressures should be reduced in a slow, controlled manner over days to avoid severe complications of relative hypotension [101]. Several classes of antihypertensive agents have been used in infants for management of severe hypertension including vasodilators, ACE inhibitors, calcium channel blockers, and α- and β-antagonists [see Table 26.5]. Sodium nitroprusside has been used for decades in hypertensive crises and, due to the very short action of the medication, may be easily titrated to the desired effect. With prolonged use, infants need to be monitored for cyanide toxicity which can occur earlier in infants with renal failure. There is one case series of IV enalaprilat use in neonates, but given the high incidence of side effects, importance of the renin-angiotensin-aldosterone system (RAAS) in neonates, and lack of established dose, we cannot endorse its use [110]. Nicardipine, a dihydropyridine calcium channel blocker, has been used safely and effectively in premature and term infants with hypertension but requires administration through a central venous line and should be avoided in perinatal asphyxia [111, 112]. Labetalol is a selective alpha-1-adrenergic antagonist and nonselective beta-adrenergic antagonist that has been used for decades to treat hypertensive crises. The efficacy and safety of IV labetalol is comparable to IV nitroprusside or IV nicardipine in infants less than 24 months of age [113]. Side effects of labetalol included hypoglycemia, bradycardia, and hypotension, although the adverse events were not more common than in the other drug classes, but caution must be used in patients with preexisting brain injury. Esmolol, an IV cardioselective short-acting beta-antagonist, is a newer agent but has been used in children undergoing cardiac surgery for repair of congenital anomalies with good safety and efficacy [114, 115].
Unfortunately, there are occasions when intravenous infusions are not immediately available and other agents must be used. Hydralazine may be given IV or orally with a short onset of action of 5–20 min for IV administration and 20–30 min when given orally. Nifedipine has been studied in infants with hypertensive crises at a dose of 2.5 mg with good effect [116] although caution must be used with this medication as others have found transient neurologic changes in children and small doses require extraction of the liquid from a capsule with estimation of dispensed dose. Isradipine is a newer calcium channel blocker that is being used for acute hypertension as it is available in an immediate release formulation with onset of action of 30–60 min [117, 118]. Other fast-acting medications to consider include oral captopril, clonidine, and minoxidil [47] [see Table 26.5]. Some of these agents may not be available in all countries, so one’s choice of agent may be partly driven by what is available.
As with many medications in pediatrics, most antihypertensive drugs are not approved for use in children, particularly infants, as adequate studies have not been conducted involving this age group [119]. In neonates, the physiology of the immediate postnatal life is very different from older children, and therefore, drug dosages and side effects can be quite different. Many older antihypertensive drugs have been used for decades to treat infant hypertension and are unlikely to be formally studied, but small studies of other antihypertensive medications can be used for guidance when trying to manage infant hypertension. Captopril, a short-acting ACE inhibitor, is much more potent in neonates, and they require a lower dose for clinical effect [see Table 26.5]. Infants may have significant decreases in blood pressure associated with captopril as well as acute renal failure and neurologic consequences [120]. Similar caution should be used for longer-acting ACE inhibitors such as enalapril, lisinopril, and quinapril when used in infants. In addition, we are learning more about the importance of the RAAS during renal development [121], and concern has been raised about persistent use of inhibitors of this developmentally important system in neonates and long-term consequences that have yet to be determined.
Amlodipine, a third-generation dihydropyridine calcium channel blocker, is generally safe and effective for management of childhood hypertension. It can be compounded in a suspension for use in young children and has a long half-life although may need to be dosed twice daily in younger children [122]. Isradipine, a second-generation dihydropyridine calcium channel blocker, has been used in hospitalized neonates, infants, and children with good effect [117, 118]. Dosage based on size produced a relatively larger decrease in blood pressure in the infants compared to older children, but only 1 % of patients developed clinically significant hypotension. Isradipine can be compounded into a stable suspension preparation improving its utility in neonates and infants.
Diuretics are used commonly in NICUs, often for indications other than blood pressure. They have modest effects on blood pressure reduction but may be first-line agents in infants with chronic lung disease or fluid retention. Electrolyte abnormalities are not uncommon and require laboratory monitoring.
Although most antihypertensive medications are not approved for use in infants, physicians have had to treat blood pressure with various agents to prevent the complications of uncontrolled hypertension. Hydralazine has been the most commonly used medication for neonatal hypertension since the 1970s [1]. In an Australian study of neonates with hypertension, 82 % were treated during the initial hospitalization and the most commonly prescribed medications were hydralazine, followed by captopril, labetalol, and atenolol [18]. This is consistent with observed management in the large database study by Blowey and colleagues where vasodilators, primarily hydralazine, were prescribed in 64 % of infants, ACE inhibitors in 51 %, then calcium channel blockers (24 %), alpha- and beta-blockers (18 %), and clonidine (5 %) [50]. Medications were prescribed at a median age of 15 days of life, the median duration was 10 days, and 45 % were treated with two or more drugs [50].
In some cases, surgical or interventional management can be curative for hypertension in infants. For renal artery stenosis, percutaneous transluminal renal angioplasty to correct the stenosis may be curative when the lesion is unilateral and not associated with a systemic disease process although the procedure is technically more difficult in small infants who are often managed medically awaiting further growth [57, 107]. Surgical correction of coarctation of the thoracic aorta improves blood pressure in many but not all infants with this congenital malformation [71]. For infants with tumors such as Wilms tumor, neuroblastoma, and mesoblastic nephroma, surgery usually results in normalization of the blood pressure [90, 92, 94]. Rarely structural or function anomalies of the kidney and urinary tract associated with severe hypertension may require surgery, and it has been reported as curative in some cases of ureteropelvic junction obstruction, multicystic dysplastic kidney, and unilateral renal hypoplasia [64, 67, 123, 124]. In exceptional circumstances, nephrectomy has been used for management of hypertension related to autosomal recessive polycystic kidney disease, which is often difficult to treat in infants, although may become easier with time [125].
Long-Term Outcome
Few follow-up studies of neonatal hypertension have been published. The review published by Adelman in 1978 of 17 infants with neonatal hypertension found that 13 (76 %) were normotensive off antihypertensive medications by 3–6 months after the onset [1]. Results were similar in a slightly later study of infants hypertensive in the NICU where 56 % were normotensive within the first month of life, 67 % by 6 months of age, and 81 % by 1 year of age [48]. In a recent Australian study of neonates with hypertension, more than 40 % of infants were still receiving antihypertensive medications at discharge and 15 % were still on treatment at follow-up at 3–6 months of age [18].
Attention has been given to certain infant disease states with reported longer-term blood pressure outcomes. While in some conditions the blood pressures improve with time, others are associated with increasing hypertension. Follow-up on infants discharged from the NICU with chronic lung disease has shown that infants with hypertension in the NICU or at follow-up had resolution of the elevated blood pressure at a mean of 7.8 months although the range was less than 1 month to just over 2 years [78]. In children with autosomal recessive polycystic kidney disease who survive the neonatal period, almost 40 % require antihypertensive medications by 1 year, 50 % by 3 years, and 60 % by 15 years of age [125]. Several long-term studies of renal vein thrombosis during infancy have found kidney outcomes are poor regardless of treatment with 66–90 % showing irreversible kidney damage at follow-up and 19–34% of these patients had elevated blood pressure long term [55, 56, 109, 126]. Chronic renal failure was reported in around 30 %, proteinuria in 12 %, and urine-concentrating defects in almost 50 % [109, 126].
Another concern is for the development of hypertension in high-risk infants after discharge from the NICU. Sheftel and colleagues screened infants who were normotensive during the NICU course at follow-up clinics during the first year of life and found 9 % were hypertensive based on three separate systolic blood pressure readings [127]. After extending their cohort and follow-up period, they found 2.6 % were hypertensive at an average follow-up of 19 months [128]. Causes identified included ureteropelvic junction obstruction, renal artery thrombosis, coarctation of the aorta, and neuroblastoma, but no cause was identified in the majority of children. Another study followed up cohorts of VLBW infants at 1, 2, and 3 years of age and found that the observed systolic blood pressure value did not differ between cohorts but that the percentage with blood pressure values exceeding the 95th percentile decreased from 33 % at 1 year to 15 % at 2 years and 8 % at 3 years [129]. A study of genetic and clinical risk factors for infant hypertension found discharge on supplemental oxygen, history of urinary tract infection during NICU, and cytochrome P450 CYP2D6 ‘CC’ genotype to be independent risk factors for elevated blood pressure at NICU follow-up clinics [28].
We should not be surprised that the risks for development of hypertension in this population are likely multifactorial as these infants are often born prior to completion of nephrogenesis and may be susceptible to acute kidney injury from hypoxia, hypotension, and nephrotoxins in addition to a possible genetic predisposition. Following on the early hypothesis by Brenner and colleagues that reduced nephron endowment predisposes to the development of hypertension [130, 131], Rodriguez and colleagues examined renal autopsy specimens from premature and term neonates and found that glomerulogenesis is decreased in all preterm infants and correlates with gestational age [132]. In addition, active glomerulogenesis is absent in longer surviving premature infants and is further inhibited by acute kidney injury. This provides further support to the clinical recommendation that surviving premature infants need long-term follow-up that includes blood pressure assessment.
Neonatal Risk Factors for Later Renal and Cardiovascular Disease
It is becoming more widely recognized that perinatal events may alter risks for renal and cardiovascular disease in adolescence and adulthood. A few comments are included here, but for a more detailed review, see Chap. 7 on Perinatal Programming of Blood Pressure. In particular, there has been much focus recently on prematurity, intrauterine growth restriction, and postnatal weight gain as risk factors for future renal and cardiovascular disease. Although there is still much controversy in the literature regarding which factors have a role and how much of an effect of perinatal factors compared to later health status. Studies that have followed up premature infants through childhood have found an increased incidence of hypertension (7–16 %), chronic renal insufficiency (11 %), and tubular dysfunction (10–15 %) in this population [133, 134]. Using ambulatory blood pressure monitoring (ABPM), it was found that children born prematurely, particularly those that had intrauterine growth restriction, had higher nocturnal blood pressures and reduced dipping compared to controls [135]. Young adults who were born very premature (< 32 weeks) or at very low birth weight (< 1,500 g) have a very high rate of prehypertension (approx. 40 %) and a higher prevalence of hypertension (approx. 10 %) when compared to the general population of a similar age [136]. As discussed above, hypertension may develop in children and adults who were born premature due to a reduced nephron endowment.
Several studies have shown that low birth weight or being born small for gestation age is inversely correlated with blood pressure in childhood and early adulthood and may be related to a higher prevalence of hypertension [137–139]. A large cohort study including almost 30,000 children found that placental ratio percentage, as an indicator of intrauterine growth restriction, was a predictor of elevated blood pressure at 7 years of age while unadjusted birth weight was not [140]. ABPM in children born small for gestation age found blunted circadian and ultradian rhythms in addition to elevated blood pressure demonstrating altered cardiovascular regulation in children born growth restricted [141]. The exact mechanism for the higher cardiovascular risk may differ depending on the etiology as suggested in a 20-year follow-up study of premature neonates where offspring of hypertensive pregnancies showed impaired endothelial function and subclinical atherosclerosis compared to normotensive pregnancy preterm offspring who demonstrated increased aortic stiffness [142]. Differential vascular programming may influence later cardiovascular risks.
The role of early weight gain in later development of cardiovascular disease is still under debate. Studies have shown that accelerated infant weight gain during the first several months of life is related to higher systolic blood pressure during childhood and adolescence, abnormal lipid profile in adolescents, and abnormal glucose metabolism in those children born small for gestational age suggesting effects of both prenatal and early postnatal programming [143, 144]. Another study of children who were born premature also showed that increased weight gain over the first year was associated with a slightly higher systolic blood pressure in childhood, but the weight gain was also associated with improved neurocognition [145]. Exclusive breast feeding of infants has been associated with lower childhood systolic blood pressure with a dose-response relationship in one study [146], while others did not find this association [147, 148] although breast feeding should still be encouraged for all the other health benefits. Several other studies have shown that early postnatal growth has an influence on childhood and early adulthood blood pressures but that the effect is small compared to later childhood growth or adult body mass index [136, 138, 139, 148, 149]. This has lead to the suggestion that the focus shift from perinatal growth to prevention of adiposity from later infancy through childhood as a more effective mechanism to reduce adulthood cardiovascular disease [139].
Conclusions
Neonatal and infant hypertension may be a challenging clinical issue, primarily because we are not certain of the definition of hypertension within this population and limited medication studies are available to guide treatment. Various factors, both intrinsic and extrinsic, can influence neonatal blood pressures with the strongest determinants being birth weight, gestational age, and postmenstrual age. Newer data on normal blood pressure values are available based on stable infants, but larger multicenter studies are needed to confirm and refine these reference values and more accurately determine abnormal values or hypertension. The incidence of neonatal hypertension has remained fairly consistent over the last 30 years at 1–2 % despite changes in the complexity of the neonatal population with new technologic advances. The most common causes of hypertension remain renovascular, commonly related to umbilical catheters, renal parenchymal, coarctation of the aorta, and chronic lung disease although there are newer associations indentified such as ECMO. Most causes can easily be determined by infant history and some basic investigations, and more antihypertensive agents are being trialed or used within this population creating more options for treatment. Most neonatal hypertension will resolve over time although some disease states that may be identified during infancy need long-term follow-up for the development of hypertension or other complications. The exact impact of perinatal events on later renal and cardiovascular disease is still under investigation, but appropriate management of neonatal and infant hypertension is important for both the short- and long-term health of these infants.
Abbreviations
- ABPM:
-
Ambulatory blood pressure monitoring
- ACE:
-
Angiotensin-converting enzyme
- ECMO:
-
Extracorporeal membrane oxygenation
- HP:
-
Hewlett-Packard
- IV:
-
Intravenous
- MAP:
-
Mean arterial pressure
- NICU:
-
Neonatal intensive care unit
- PDA:
-
Patent ductus arteriosus
- RAAS:
-
Renin-angiotensin-aldosterone system
- RVT:
-
Renal vein thrombosis
- UAC:
-
Umbilical artery catheter
- VLBW:
-
Very low birth weight infants
References
Adelman RD. Neonatal hypertension. Pediatr Clin North Am. 1978;25(1):99–110.
Butt WW, Whyte H. Blood pressure monitoring in neonates: comparison of umbilical and peripheral artery catheter measurements. J Pediatr. 1984;105(4): 630–2.
Park MK, Menard SM. Accuracy of blood pressure measurement by the Dinamap monitor in infants and children. Pediatrics. 1987;79:907–14.
Meyer S, Sander J, Graber S, Gottschling S, Gortner L. Agreement of invasive versus non-invasive blood pressure in preterm neonates is not dependent on birth weight or gestational age. J Paediatr Child Health. 2010;46:249–54.
Dannevig I, Dale HC, Liestol K, Lindemann R. Blood pressure in the neonate: three non-invasive oscillometric blood pressure monitors compared with invasively measure blood pressure. Acta Paediatr. 2005;94:191–6.
O’Shea J, Dempsey EM. A comparison of blood pressure measurements in newborns. Am J Perinatol. 2009;26(2):113–6.
Takci S, Yigit S, Korkmaz A, Yurdakok M. Comparison between oscillometric and invasive blood pressure measurements in critically ill premature infants. Acta Paediatr. 2012;101:132–5.
Ribeiro MA, Fiori HH, Luz JH, Piva JP, Ribeiro NM, Fiori RM. Comparison of noninvasive techniques to measure blood pressure in newborns. J Pediatr (Rio J). 2011;87(1):57–72.
Crapanzano MS, Strong WB, Newman IR, Hixon L, Casal D, Linder CW. Calf blood pressure: clinical implications and correlations with arm blood pressure in infants and young children. Pediatrics. 1996;97:220–4.
Gupta JM, Scopes JW. Observations on blood pressure in newborn infants. Arch Dis Child. 1965;40: 637–44.
Cohen M, Brown DR, Myers MM. Cardiovascular responses to feeding in the neonate during the first four days of life. Early Hum Dev. 1998;50:273–82.
Duncan AF, Rosenfeld CR, Morgan JS, Ahmad N, Heyne RJ. Interrater reliability and effect of state on blood pressure measurements in infants 1 to 3 years of age. Pediatrics. 2008;122:e590–4.
Thoresen M, Cowan F. Dinamap blood pressure measurements in the newborn: how many – what effects? Acta Paediatr. 1992;81:272–3.
Sarici SU, Alpay F, Okutan V, Gokcay E. Is a standard protocol necessary for oscillometric blood pressure measurement in term newborns? Biol Neonate. 2000;77:212–6.
Kimble KJ, Darnall RA, Yelderman M, Ariagno RL, Ream AK. An automated oscillometric technique for estimating mean arterial pressure in critically ill newborns. Anesthesiology. 1981;54:423–5.
Nwankwo MU, Lorenz JM, Gardiner JC. A standard protocol for blood pressure measurement in the newborn. Pediatrics. 1997;99:E10.
Gillman MW, Rich-Edwards JW, Rifas-Shiman SL, Lieverman ES, Kleinman KP, Lipshultz SE. Maternal age and other predictors of newborn blood pressure. J Pediatr. 2004;144:240–5.
Seliem WA, Falk MC, Shadbolt B, Kent AL. Antenatal and postnatal risk factors for neonatal hypertension and infant follow-up. Pediatr Nephrol. 2007;22:2081–7.
Kent AL, Shadbolt B, Hu E, Meskell S, Falk MC, Dahlstrom JE. Do maternal- or pregnancy-associated disease states affect blood pressure in the early neonatal period? Aust N Z J Obstet Gynaecol. 2009; 49(4):364–70.
Zinner SH, Rosner B, Oh W, Kass EH. Significance of blood pressure in infancy. Familial aggregation and predictive effect on later blood pressure. Hypertension. 1985;7:411–6.
Sedaghat N, Ellwood D, Shadbolt V, Kecskes Z, Falk MC, Brussel T, Kent AL. The effect of mode of delivery and anesthesia on neonatal blood pressure. Aust N Z J Obstet Gynaecol. 2008;48:172–8.
Sadoh WE, Ibhanesebhor SE. Predictors of newborn systolic blood pressure. West Afr J Med. 2010;29(2): 86–90.
Geerts CG, Grobbee DE, van der Ent CK, de Jong BM, van der Zalm MM, van Putte-Katier N, Kimpen JL, Uiterwaal CS. Tobacco smoke exposure of pregnant mothers and blood pressure in their newborns: results from the wheezing illnesses study Leidsche Rijn birth cohort. Hypertension. 2007;50: 572–8.
Cohen G, Jeffery H, Lagercrantz H, Katz-Salamon M. Long-term reprogramming of cardiovascular function in infants of active smokers. Hypertension. 2010;55:722–8.
Aaltonen J, Ojala T, Laitnen K, Piirainen TJ, Poussa TA, Isolauri E. Evidence of infant blood pressure programming by maternal nutrition during pregnancy: a prospective randomized controlled intervention study. J Pediatr. 2008;152:79–84.
Huh SY, Rifas-Shiman SL, Kleinman KP, Rich-Edwards JW, Lipshultz SE, Gillman MW. Maternal protein intake is not associated with infant blood pressure. Int J Epidemiol. 2005;34:378–84.
Been JV, Kornelisse RF, Rours IG, Passos VL, De Krijger RR, Zimmermann LJ. Early postnatal blood pressure in preterm infants: effects of chorioamnionitis and timing of antenatal steroids. Pediatr Res. 2009; 66:571–6.
Dagle JM, Fisher TJ, Haynes SE, Berends SK, Brophy PD, Morriss FH, Murray JC. Cytochrome p450 (CYP2D6) genotype is associated with elevated systolic blood pressure in preterm infants after discharge from the neonatal intensive care unit. J Pediatr. 2011;159:104–9.
LeFlore JL, Engle WD, Rosenfeld R. Determinants of blood pressure in very low birth weight neonates: lack of effect of antenatal steroids. Early Hum Dev. 2000;59:37–50.
Mildenhall L, Battin M, Bevan C, Kuschel C, Harding JE. Repeat prenatal corticosteroid doses do not alter neonatal blood pressure or myocardial thickness: randomized, controlled trial. Pediatrics. 2009;123:e646–52.
Stark MJ, Wright IM, Clifton VL. Sex-specific alterations in placental 11B-hydroxysteroid dehydrogenase 2 activity and early postnatal clinical course following antenatal betamethasone. Am J Physiol Regul Integr Comp Physiol. 2009;297:R510–4.
Zubrow AB, Hulman S, Kushner H, Falkner B. Determinants of blood pressure in infants admitted to neonatal intensive care units: a prospective multicenter study. J Perinatol. 1995;15(6):470–9.
Pejovic B, Peco-Antic A, Marinkovic-Eric J. Blood pressure in non-critically ill preterm and full-term neonates. Pediatr Nephrol. 2007;22:249–57.
Lurbe E, Garcia-Vincent C, Torro I, Fayos JL, Aguilar F, de Llano JM, Fuertes G, Redon J. First-year blood pressure increase steepest in low birth weight newborns. J Hypertens. 2007;25:81–6.
Mercanti I, Boivin A, Wo B, Vlieghe V, Le Ray C, Audibert F, Fouron JC, Leduc L, Nuyt AM. Blood pressures in newborns with twin-twin transfusion syndrome. J Perinatol. 2011;31:417–24.
Joppich R, Scherer B, Weber PC. Renal prostaglandins: relationship to the development of blood pressure and concentrating capacity in per-term and full-term healthy infants. Eur J Pediatr. 1979;132: 253–9.
Kent AL, Kecskes Z, Shadbolt V, Falk MC. Normative blood pressure data in the early neonatal period. Pediatr Nephrol. 2007;22:1335–41.
Kent AL, Meskell S, Falk MC, Shadbolt B. Normative blood pressure data in non-ventilated premature neonates from 28–36 weeks gestation. Pediatr Nephrol. 2009;24:141–6.
Georgieff MK, Mills MM, Gomez-Marin O, Sinaiko AR. Rate of change of blood pressure in premature and full term infants from birth to 4 months. Pediatr Nephrol. 1996;10:152–5.
Dionne JM, Abitbol CL, Flynn JT. Hypertension in infancy: diagnosis, management and outcome. Pediatr Nephrol. 2012;27:17–32.
Dionne JM, Abitbol CL, Flynn JT. Erratum to: hypertension in infancy: diagnosis, management and outcome. Pediatr Nephrol. 2012;27:159–60.
National Heart, Lung and Blood Institute, Task Force on Blood Pressure Control in Children. Report of the second task force on blood pressure control in children – 1987. National Institutes of Health; 1987.
Kent AL, Kecskes Z, Shadbolt B, Falk MC. Blood pressure in the first year of life in healthy infants born at term. Pediatr Nephrol. 2007;22:1743–9.
Lande MB, Kaczorowski JM, Aunger P, Schwartz GJ, Weitzman M. Elevated blood pressure and decreased cognitive function among school-age children and adolescents in the United States. J Pediatr. 2003;143:720–4.
Sharma M, Kupferman JC, Brosgol Y, Paterno K, Goodman S, Prohovnik I, Kirkham FJ, Pavlakis SG. The effects of hypertension on the paediatric brain: a justifiable concern. Lancet Neurol. 2010;9:933–40.
Ingelfinger JR. Hypertension in the first year of life. In: Ingelfinger JR, editor. Pediatric hypertension. Philadelphia: WB Saunders; 1982. p. 229–40.
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114: 555–76.
Buchi KF, Siegler RL. Hypertension in the first month of life. J Hypertens. 1986;4:525–8.
Singh HP, Hurley RM, Myers TF. Neonatal hypertension: incidence and risk factors. Am J Hypertens. 1992;5:51–5.
Blowey DL, Duda PJ, Stokes P, Hall M. Incidence and treatment of hypertension in the neonatal intensive care unit. J Am Soc Hypertens. 2011;5(6): 478–83.
Neal WA, Reynolds JW, Jarvis CW, Williams HJ. Umbilical artery catheterization: demonstration of arterial thrombosis by aortography. Pediatrics. 1972;46:6–13.
Seibert JJ, Taylor BJ, Williamson SL, Williams BJ, Szabo JS, Corbitt SL. Sonographic detection of neonatal umbilical-artery thrombosis: clinical correlation. Am J Roentgenol. 1987;148:965–8.
Barrington KJ. Umbilical artery catheters in the newborn: effects of position of the catheter tip (review). Cochrane Database Syst Rev. 2010;1–20.
Plumer LB, Kaplan GW, Mendoza SA. Hypertension in infants – a complication of umbilical arterial catheterization. J Pediatr. 1976;89(5):802–5.
Lau KK, Stoffman JM, Williams S, McCucker P, Brandao L, Patel S, Chan AK. Neonatal renal vein thrombosis: review of the English-language literature between 1992 and 2006. Pediatrics. 2007;120(5): e1278–84.
Kosch A, Kuwertz-Broking E, Heller C, Kurnik K, Schobess R, Nowak-Gottl U. Renal venous thrombosis in neonates: prothrombotic risk factors and long-term follow-up. Blood. 2004;104:1356–60.
Tullus K, Brennan E, Hamilton G, Lord R, McLaren C, Marks SD, Roebuck DJ. Renovascular hypertension in children. Lancet. 2008;371(9622):1453–63.
Menser MA, Dorman DC, Reye RD, Reid RR. Renal-artery stenosis in the rubella syndrome. Lancet. 1966;287(7441):790–2.
Kasaragod AB, Lucia MS, Lum GM, Caldwell S, Stork L, Stenmark KR. Solitary renal myofibromatosis: an unusual cause of infantile hypertension. Pediatrics. 1999;103(5):e66.
Milner LS, Heitner R, Thomson PD, Levin SE, Rothberg AD, Beale P, Ninin DT. Hypertension as the major problem of idiopathic arterial calcification of infancy. J Pediatr. 1984;105:934–8.
Lanzarini VV, Furusawa EA, Sadeck L, Leone CR, Vaz FA, Kock VH. Neonatal arterial hypertension in nephro-urological malformations in a tertiary care hospital. J Hum Hypertens. 2006;20:679–83.
Guay-Woodford LM, Desmond RA. Autosomal recessive polycystic kidney disease: the clinical experience in North America. Pediatrics. 2003;111:1072–80.
Fick GM, Johnson AM, Strain JD, Kimberling WJ, Kumar S, Manco-Johnson ML, Duley IT, Gabow PA. Characteristics of very early onset autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1993;3:1863–70.
Abdulhannan P, Stahlschmidt J, Subramaniam R. Multicystic dysplastic kidney disease and hypertension: clinical and pathological correlation. J Pediatr Urol. 2011;7:566–8.
Gilboa N, Urizar RE. Severe hypertension in the newborn after pyeloplasty of hydronephrotic kidney. Urology. 1983;22(2):179–82.
Oliveira EA, Diniz JS, Rabelo EA, Silva JM, Pereira AK, Filgueiras MT, Soares FM, Sansoni RF. Primary megaureter detected by prenatal ultrasonography: conservative management and prolonged follow-up. Int Urol Nephrol. 2000;32:13–8.
Munoz AI, Baralt JF, Melendez MT. Arterial hypertension in infants with hydronephrosis. Am J Dis Child. 1977;131:38–40.
Schell-Feith EA, Kist-van Holthe JE, van Zwieten PH, Zonderland HM, Holscher HC, Swinkels DW, Brand R, Berger HM, van der Heijden BJ. Preterm neonates with nephrocalcinosis: natural course and renal function. Pediatr Nephrol. 2003;18:1102–8.
Assadi FK, Kimura RE, Subramanian U, Patel S. Liddle syndrome in a newborn infant. Pediatr Nephrol. 2002;17:609–11.
Ingelfinger JR. The molecular basis of pediatric hypertension. Pediatr Clin North Am. 2006;53: 1011–28.
Smith Maia MM, Cortex TM, Parga JR, de Avila LF, Aiello VD, Barbero-Marcial M, Ebaid M. Evolution aspects of children and adolescents with surgically corrected aortic coarctation: clinical, echocardiographic, and magnetic resonance image analysis or 113 patients. J Thorac Cardiovasc Surg. 2004;127:712–20.
O’Sullivan JJ, Derrick G, Darnell R. Prevalence of hypertension in children after early repair of coarctation of the aorta: a cohort study using casual and 24 hour blood pressure measurement. Heart. 2002;88:163–6.
Sell LL, Cullen ML, Lerner GR, Whittlesey GC, Shanley CJ, Klein MD. Hypertension during extracorporeal membrane oxygenation: cause, effect, and management. Surgery. 1987;102:724–30.
Boedy RF, Goldberg AK, Howell CG, Hulse E, Edwards EG, Kanto WP. Incidence of hypertension in infants on extracorporeal membrane oxygenation. J Pediatr Surg. 1990;25(2):258–61.
Heggen JA, Fortenberry JD, Tanner AJ, Reid CA, Mizzell DW, Pettignano R. Systemic hypertension associated with venovenous extracorporeal membrane oxygenation for pediatric respiratory failure. J Pediatr Surg. 2004;39:1626–31.
Becker JA, Short BL, Martin GR. Cardiovascular complications adversely affect survival during extracorporeal membrane oxygenation. Crit Care Med. 1998;26:1582–6.
Buckner PS, Maidens JM, Finer NN. Characterization of the neonatal heart rate baroreflex during and after ECMO. Early Hum Dev. 1993;32:49–61.
Anderson AH, Warady BA, Daily DK, Johnson JA, Thomas MK. Systemic hypertension in infants with severe bronchopulmonary dysplasia: associated clinical factors. Am J Perinatol. 1993;10(3):190–3.
Abman SH, Warady BA, Lum GM, Koops BL. Systemic hypertension in infants with bronchopulmonary dysplasia. J Pediatr. 1984;104(6):928–31.
Alagappan A, Malloy MH. Systemic hypertension in very low-birth weight infants with bronchopulmonary dysplasia: incidence and risk factors. Am J Perinatol. 1998;15(1):3–8.
Stark AR, Carlo WA, Tyson JE, Papile L, Wright LL, Shankaran S, Donovan EF, Oh W, Rauer CR, Saha S, Poole K, Stoll BJ. Adverse effects of early dexamethasone treatment in extremely-low-birth-weight infants. N Engl J Med. 2001;344:95–101.
Perlman JM, Volpe JJ. Seizures in the preterm infant: effects on cerebral blood flow velocity, intracranial pressure, and arterial blood pressure. J Pediatr. 1983;102(2):288–93.
Kaiser AM, Whitelaw AG. Hypertensive response to raised intracranial pressure in infancy. Arch Dis Child. 1988;63:1461–5.
Minouni M, Kaufman H, Roitman A, Morag C, Sadan N. Hypertension in a neonate with 11β-hydroxylase deficiency. Eur J Pediatr. 1985;143: 231–3.
Parsa AA, New MI. Low-renin hypertension of childhood. Endocrinol Metab Clin North Am. 2011;40:369–77.
Klevit HD, Campbell RA, Blair HR, Bongiovanni AM. Cushing’s syndrome with nodular adrenal hyperplasia in infancy. J Pediatr. 1968;68(6): 912–20.
Schonwetter BS, Libber SM, Jones MD, Park KJ, Plotnick LP. Hypertension in neonatal hyperthyroidism. Am J Dis Child. 1983;137:954–5.
Malagon-Rogers M. Non-glucocorticoid-remediable aldosteronism in an infant with low-renin hypertension. Pediatr Nephrol. 2004;19:235–6.
Kumar M, Kumar V, Talukdar B, Mohta A, Khurana N. Cushing syndrome in an infant due to cortisol secreting adrenal pheochromocytoma: a rare association. J Pediatr Endocrinol Metab. 2010;23(6):621–5.
Sheth KJ, Tang TT, Blaedel ME, Good TA. Polydipsia, polyuria, and hypertension associated with renin-secreting Wilms tumor. J Pediatr. 1978;92(6):921–4.
Tsuchida Y, Shimizu K, Hata J, Honna T, Nishiura M. Renin production in congenital mesoblastic nephroma in comparison with that in Wilms’ tumor. Pediatr Pathol. 1993;13:155–64.
Sellden H, Kogner P, Sollevi A. Adenosine for pre-operative blood pressure control in an infant with neuroblastoma. Acta Anaesthesiol Scand. 1995;39:705–8.
Shinohara M, Shitara T, Hatakeyama S, Suzuki N, Maruyama K, Kobayashi T, Tsuchida Y. An infant with systemic hypertension, renal artery stenosis, and neuroblastoma. J Pediatr Surg. 2004;39:103–6.
Miller OF, Kolon TF. Hyperreninemia and congenital mesoblastic nephroma: case report and review of the literature. Urology. 2000;55(5):775. xxv-xxvii.
Horn PT. Persistent hypertension after prenatal cocaine exposure. J Pediatr. 1992;121:288–91.
Dube SK, Jhaveri RC, Rosenfeld W, Evans HE, Khan F, Spergel G. Urinary catecholamines, plasma renin activity and blood pressure in newborns: effects of narcotic withdrawal. Dev Pharmacol Ther. 1981;3(3):83–7.
Takeuchi T, Tanaka D, Saikawa N, Satoh H, Iwasaki J, Inoue M, Narui K, Iikura Y. Changes of the physiological parameters of very low-birth weight infants with chronic lung disease treated with dexamethasone. Pediatr Int. 2002;44:122–6.
Cannon ME, Twu BM, Yang CS, Hsu CH. The effect of theophylline and cyclic adenosine 3′,5′-monophosphate on renin release by afferent arterioles. J Hypertens. 1989;7:569–76.
Pomeranz A, Dolfin T, Korzets A, Eliakim A, Wolach G. Increased sodium concentrations in drinking water increase blood pressure in neonates. J Hypertens. 2002;20:203–7.
Kovacikova L, Kunovsky P, Skrak P, Havviar D, Martanovic P. Renovascular hypertension in infant presenting with cardiogenic shock. Pediatr Emerg Care. 2005;21(5):322–4.
Deal JE, Barratt TM, Dillon MJ. Management of hypertensive emergencies. Arch Dis Child. 1992;67: 1089–92.
Skalina ME, Kliegman RM, Fanaroff AA. Epidemiology and management of severe symptomatic neonatal hypertension. Am J Perinatol. 1986; 3(3):235–9.
Roth CG, Spottswood SE, Chan JC, Roth KS. Evaluation of the hypertensive infant: a rational approach to diagnosis. Radiol Clin North Am. 2003;41:931–44.
Peterson AL, Frommelt PC, Mussatto K. Presentation and echocardiographic markers of neonatal hypertensive cardiomyopathy. Pediatrics. 2006;118:e782–5.
Kruger C, Rauh M, Dorr HG. Immunoreactive renin concentrations in healthy children from birth to adolescence. Clin Chim Acta. 1998;274:15–27.
Richer CH, Hornych H, Amiel-Tison C, Relier JP, Giudicelli JF. Plasma renin activity and its postnatal development in preterm infants. Biol Neonate. 1977;31:301–4.
Deal JE, Snell MF, Barratt TM, Dillon MJ. Renovascular disease in childhood. J Pediatr. 1992;121:378–84.
Vo NJ, Hammelman BD, Racadio JM, Strife CF, Johnson ND, Racadio JM. Anatomic distribution of renal artery stenosis in children: implications for imaging. Pediatr Radiol. 2006;36:1032–6.
Marks SD, Massicotte MP, Steele BT, Matsell DG, Filler G, Shah PS, Perlman M, Rosenblum ND, Shah VS. Neonatal renal venous thrombosis: clinical outcomes and prevalence of prothrombotic disorders. J Pediatr. 2005;146:811–6.
Wells TG, Bunchman TE, Kearns GL. Treatment of neonatal hypertension with enalaprilat. J Pediatr. 1990;117(4):664–7.
Milou C, Debuche-Benouachkou V, Semana DS, Germain JF, Gouyon JB. Intravenous nicardipine as a first-line antihypertensive drug in neonates. Intensive Care Med. 2000;26:956–8.
Flynn JT, Mottes TA, Brophy PD, Kershaw DB, Smoyer WE, Bunchman TE. Intravenous nicardipine for treatment of severe hypertension in children. J Pediatr. 2001;139(1):38–43.
Thomas CA, Moffett BS, Wagner JL, Mott AR, Feig DI. Safety and efficacy of intravenous labetalol for hypertensive crisis in infants and small children. Pediatr Crit Care Med. 2011;12:28–32.
Wiest DB, Garner SS, Uber WE, Sade RM. Esmolol for the management of pediatric hypertension after cardiac operations. J Thorac Cardiovasc Surg. 1998;115:890–7.
Tabbutt S, Nicolson SC, Adamson PC, Zhang X, Hoffman ML, Wells W, Backer CL, McGowan FX, Tweddell JS, Bokesch P, Schreiner M. The safety, efficacy, and pharmacokinetics of esmolol for blood pressure control immediately after repair of coarctation of the aorta in infants and children: a multicenter, double-blind, randomized trial. J Thorac Cardiovasc Surg. 2008;138:321–8.
Lopez-Herce J, Dorao P, de la Oliva P, Delgado MA, Martinez MC, Ruza F. Dosage of nifedipine in hypertensive crises of infants and children. Eur J Pediatr. 1989;149:136–7.
Miyashita Y, Peterson D, Rees JM, Flynn JT. Isradipine for treatment of acute hypertension in hospitalized children and adolescents. J Clin Hypertens. 2010;12:850–5.
Flynn JT, Warnick SJ. Isradipine treatment of hypertension in children: a single-center experience. Pediatr Nephrol. 2002;17:748–53.
Flynn JT. Successes and shortcomings of the food and drug modernization act. Am J Hypertens. 2003;16(10):889–91.
Perlman JM, Volpe JJ. Neurologic complications of captopril treatment of neonatal hypertension. Pediatrics. 1989;83:47–52.
Lacoste M, Cai Y, Guicharnaud L, Mounier F, Dumez Y, Bouvier R, Dijoud F, Gonzales M, Chatten J, Delezoide AL, Daniel L, Joubert M, Laurent N, Aziza J, Sellami T, Amar HB, Jarnet C, Frances AM, Daikha-Dahmane F, Coulomb A, Neuhaus TJ, Foliguet B, Chenal P, Marcorelles P, Gasc JM, Corvol P, Gubler MC. Renal tubular dysgenesis, a not uncommon autosomal recessive disorder leading to oligohydramnios: role of the renin-angiotensin system. J Am Soc Nephrol. 2006;17:2253–63.
Flynn JT, Pasko DA. Calcium channel blockers: pharmacology and place in therapy of pediatric hypertension. Pediatr Nephrol. 2000;15:302–16.
Susskind MR, Kim KW, King LR. Hypertension and multicystic kidney. Urology. 1989;34(6):362–6.
Tokunaka S, Takamura T, Osanai H, Yachiku S, Hashimoto H, Mori Y. Severe hypertension in infant with unilateral hypoplastic kidney. Urology. 1987;29(6):618–20.
Roy S, Dillon MJ, Trompeter RS, Barratt TM. Autosomal recessive polycystic kidney disease: long-term outcome of neonatal survivors. Pediatr Nephrol. 1997;11:302–6.
Mocan H, Beattie TJ, Murphy AV. Renal venous thrombosis in infancy: long-term follow-up. Pediatr Nephrol. 1991;5:45–9.
Sheftel DN, Hustead V, Friedman A. Hypertension screening in the follow-up of premature infants. Pediatrics. 1983;71:763–6.
Friedman AL, Hustead VA. Hypertension in babies following discharge from a neonatal intensive care unit. Pediatr Nephrol. 1987;1:30–4.
Duncan AF, Heyne RJ, Morgan JS, Ahmad N, Rosenfeld CR. Elevated systolic blood pressure in preterm very-low-birth-weight infants ≤ 3 years of life. Pediatr Nephrol. 2011;26:1115–21.
Brenner BM, Garcia DL, Anderson S. Glomeruli and blood pressure: less of one, more the other? Am J Hypertens. 1988;1:335–47.
Mackenzie HS, Lawler EV, Brenner BM. Congenial oligonephropathy: the fetal flaw in essential hypertension? Kidney Int. 1996;49(Supp55):S30–4.
Rodriguez MM, Gomez AH, Abitbol CL, Chandar JJ, Duara S, Zilleruelo GE. Histomorphometric analysis of postnatal glomerulogenesis in extremely preterm infants. Pediatr Dev Pathol. 2004;7:17–25.
Kist-van Halthe JE, van Zwieten PH, Schell-Feith EA, Zonderland HM, Holscher HC, Wolterbeek R, Veen S, Frolich M, van der Heijen BJ. Is Nephrocalcinosis in preterm neonates harmful for long-term blood pressure and renal function? Pediatrics. 2007;119(3):468–75.
Washburn LK, Nixon PA, O’Shea TM. Follow-up of a randomized, placebo-controlled trial of postnatal dexamethasone: blood pressure and anthropometric measurements at school age. Pediatrics. 2006;118: 1592–9.
Bayrakci US, Schaefer F, Duzova A, Yigit S, Bakkaloglu A. Abnormal circadian blood pressure regulation in children born preterm. J Pediatr. 2007;151:399–403.
Keijzer-Veen MG, Finken MJ, Nauta J, Dekker FW, Hille ET, Frolich M, Wit JM, van der Heijden AJ. Is blood pressure increased 19 years after intrauterine growth restriction and preterm birth? A prospective follow-up study in the Netherlands. Pediatrics. 2005;116:725–31.
Hovi T, Andersson S, Raikkonen K, Strang-Karlsson S, Jarvenpaa AL, Eriksson JG, Pesonen AK, Heinonen K, Pyhala R, Kajantie E. Ambulatory blood pressure in young adults with very low birth weight. J Pediatr. 2010;156:54–9.
Law CM, Shiell AW, Newsome CA, Sydall HE, Shinebourne EA, Fayers PM, Martyn CN, de Swiet M. Fetal, infant, and childhood growth and adult blood pressure. Circulation. 2002;105:1088–92.
Jones A, Charakida M, Falaschetti E, Hingorani AD, Finer N, Masi S, Donald AE, Lawlor DA, Smith GD, Deanfield JE. Adipose and height growth through childhood and blood pressure status in a large prospective cohort study. Hypertension. 2012;59:919–25.
Hemachandra AH, Klebanoff MA, Duggan AK, Hardy JB, Furth SL. The association between intrauterine growth restriction in the full-term infant and high blood pressure at age 7 years: results from the collaborative perinatal project. Int J Epidemiol. 2006;35:871–7.
Wolfenstetter A, Simonetti GD, Poschl J, Schaefer F, Wuhl E. Altered cardiovascular rhythmicity in children born small for gestational age. Hypertension. 2012;60:865–70.
Lazdam M, de la Horra A, Pictcher A, Mannie Z, Diesch J, Trevitt C, Kylintireas I, Contractor H, Singhal A, Lucas A, Neubauer S, Kharbanda R, Alp N, Kelly B, Leeson P. Elevated blood pressure in offspring born premature to hypertensive pregnancy: is endothelial dysfunction the underlying vascular mechanism? Hypertension. 2010;56:159–65.
Belfort MB, Rifas-Shiman SL, Rich-Edwards J, Kleinman KP, Gillman MW. Size at birth, infant growth, and blood pressure at 3 years of age. J Pediatr. 2007;151(6):670–4.
Fabricius-Bjerre S, Jensen RB, Faerch K, Larsen T, Molgaard C, Michaelsen KF, Vaag A, Greisen G. Impact of birth weight and early infant weight gain on insulin resistance and associated cardiovascular risk factors in adolescence. PLoS One. 2011;6(6): e20595.
Belfort MB, Martin CR, Smith VC, Gillman MW, McCorkick MC. Infant weight gain and school-age blood pressure and cognition in former preterm infants. Pediatrics. 2010;125:e1419–26.
Lawlor DA, Riddoch CJ, Page AS, Andersen LB, Wedderkopp N, Harro M, Stansbie D, Davey SG. Infant feeding and components of the metabolic syndrome: findings from the European Youth Heart Study. Arch Dis Child. 2005;90:582–8.
Fall CH, Borja JB, Osmond C, Richter L, Bhargava K, Martorell R, Stein AD, Varros FC, Victora CG. Infant-feeding patterns and cardiovascular risk factors in young adulthood: data from five cohorts in low- and middle-income countries. Int J Epidemiol. 2001;40:47–62.
Joglekar C, Fall CH, Deshpande VU, Joshi N, Bhalerao A, Solat V, Deokar TM, Chougule SD, Leary SD, Osmond C, Yajnik CD. Newborn size, and childhood growth, and cardiovascular disease risk factors at the age of 6 years: the Pune Maternal Nutrition Study. Int J Obes. 2007;31(10):1534–44.
Tilling K, Davies N, Windmeijer F, Kramer MS, Bogdanovich N, Matush L, Patel R, Smith GD, Ben-Shlomo Y, Martin RM. Is infant weight associated with childhood blood pressure? Analysis of the Promotion of Breastfeeding Intervention Trial (PROBIT) cohort. Int J Epidemiol. 2011;40:1227–37.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Dionne, J.M. (2013). Neonatal and Infant Hypertension. In: Flynn, J., Ingelfinger, J., Portman, R. (eds) Pediatric Hypertension. Clinical Hypertension and Vascular Diseases. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-62703-490-6_26
Download citation
DOI: https://doi.org/10.1007/978-1-62703-490-6_26
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-62703-489-0
Online ISBN: 978-1-62703-490-6
eBook Packages: MedicineMedicine (R0)