
Abstract
Cannabinoid signaling is believed to decrease anxiety, albeit the conflicting nature of evidence is generally acknowledged. Here we provide a comprehensive overview of available findings by grouping them according to the tools that have been used to modulate cannabinoid signaling. The systemic administration of cannabinoid receptor agonists and antagonists led to the most conflicting findings; such treatments may increase, decrease, or leave anxiety unaffected. In addition, antagonists and agonists had similar effects in many instances including their biphasic effects. The effects of genetic manipulations, cannabinoid synthesis or reuptake inhibition as well as the effects of local brain treatments with cannabinoid ligands appear more consistent. We suggest that systemically administered receptor ligands affect cannabinoid signaling globally and as such lack the spatial and temporal specificity of endocannabinoid signaling. By contrast, gene disruption and the indirect modulation of endocannabinoid availability affect ongoing (natural) processes and lead to more specific and consistent effects. Local brain treatments whit receptor ligands are spatially restricted which increases the consistency of findings, but also reveals that cannabinoids affect anxiety in a brain area-specific manner, which further explains the inconsistency of findings with systemically injected ligands. Environmental conditions have a large impact on effects with all techniques, suggesting that endocannabinoid signaling affects coping with environmental challenges rather than unconditionally decreasing anxiety. The relationship between cannabinoid signaling, anxiety and coping styles is largely understudied, but holds great promise for understanding the roles of cannabinoids in behavioral control and may broaden their therapeutic implications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The totality of scientific evidence obtained so far suggests that cannabinoids do play a role in the inhibitory control of anxiety, but findings are highly contradictory both within and between the techniques employed to manipulate cannabinoid signaling. Inhibition by various means (gene disruption, receptor antagonism) can increase anxiety, decrease anxiety and may be without effect, and the same applies to the enhancement of cannabinoid signaling by cannabinoid receptor agonists, reuptake blockers or by the inhibition of enzymes involved in their degradation. While there seem to be more studies attributing an anxiolytic role to cannabinoids, conflicting evidence is too many to be attributable to experimental error. Contradictions were explained in various ways, and led to several hypotheses. A thorough review of these makes it clear that theoretical approaches are based on partial evidence and none of them is comprehensive enough to create a consistent picture. The goal of the present chapter is to provide a full review of the evidence contained by the PubMed database and to evaluate the reasons of contradictions with the ultimate aim of disentangling the roles played by endocannabinoid signaling in anxiety. We are aware of the fact that neither goal is realistic in absolute terms, because:
-
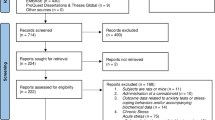
The particularities of the search engine of PubMed do not rule out that some studies remained hidden to this review. The search was performed with the search term “(cannabinoid OR endocannabinoid OR THC OR arachidonoylethanolamide OR anandamide OR AEA OR 2-arachydonoylglycerol OR 2-AG OR WIN 55, 212–2 OR HU 210 OR JWH 133 OR CP 55,940 OR URB 597 OR PF 622 OR PF 3845 OR PF 750 OR JZL 184 OR FAAH OR MAGL OR AM 404 OR AM 1172 OR VDM-11 OR rimonabant OR SR 141716 OR AM 251 OR NESS 0327 OR CB1 KO OR CB2 KO) AND (anxiety OR anxiolytic OR anxiogenic OR anxiolysis OR anxiogenesis or anxious)”. This term resulted in 1017 hits out of which 186 original research studies were identified as relevant for the present study. While the overwhelming majority of studies were likely identified, the database created by this search is probably incomplete. This figure does not include studies on the phytocannabinoid cannabidiolFootnote 1.
-
A full understanding of the role played by endocannabinoids in anxiety may not be achievable at present stage. Reasons are multiple and range from the variability of research techniques and conditions, through species, strain, and even individual differences in the particularities of the endocannabinoid system, to yet unraveled or poorly known epiphenomena of research tools used to manipulate endocannabinoid signaling. In addition to these primarily technical reasons, one cannot rule out that the anxiety-related effects of endocannabinoids are reflections of more general effects on emotions, emotional responsiveness or coping styles. If this was true ‒and many recent findings point to this possibility‒, then the anxiety-related effects of endocannabinoid signaling are inherently complex and condition-dependent, and rule out the possibility of answering simple questions of the type “does endocannabinoid signaling increase or decrease anxiety”?
The next section briefly reviews the main findings of the search described above. This section is free of interpretations or explanations which constitute the subject of the third chapter. The last, concluding section is an attempt to integrate data and views.
Findings
Systemic Effects
Decreased Endocannabinoid Activity
Decreasing endocannabinoid activity via the genetic disruption of the type 1 cannabinoid receptor (CB1R) resulted in an anxious phenotype in most studies employing well-validated tests of anxiety (e.g. the elevated plus-maze, light/dark, social interaction tests [18–25]. The anxiety enhancing effect of CB1R disruption seemed to be specific to young mice in one [26] and to aversive conditions in another study [27]. Two studies did not detect anxiety-like behavior in CB1R knockout (KO) mice tested in the elevated plus-maze [28, 29], while others may suggest that CB1R gene disruption decreases anxiety. For instance, CB1 KO mice showed decreased burying in the shock-prod burying test which was interpreted as an anxiolytic effect [30]. In the cue-induced conditioned fear test, CB1R KO mice did show increased anxiety, but this decreased when mice were socially stressed [29], suggesting that stress exposure paradoxically ameliorates the anxious phenotype of CB1R KOs.
The role of other cannabinoid receptors was poorly studied by transgenic techniques. Two studies suggest that the disruption of the type 2 cannabinoid receptor (CB2R) increases anxiety in the elevated plus-maze [31], light/dark [31] and open-field tests [32]. The disruption of the G protein-coupled receptor 55, a novel cannabinoid receptor [33–35], had no effects on anxiety in the only study available so far [36].
The down-regulation of endocannabinoid signaling by the CB1R antagonist rimonabant (SR141716A) results in biphasic effects. Low doses (0.3–3 mg/kg) reduced anxiety in several models, e.g. the elevated plus-maze [37–39], light/dark [40] and Vogel tests [38], while higher doses (3–10 mg/kg) exerted anxiogenic effects in the elevated plus-maze [28, 41–47], light/dark [48], open-field [28], novelty induced hypophagia [49], elevated T-maze [28], defensive withdrawal [45], social interaction [50] and footshock-induced ultra sound vocalization [51] tests. Such large doses also increased cue-induced conditioned fear after both acute [52] and chronic treatment [29]; in addition, rimonabant inhibited the extinction of this response [53–55]. Rodent findings are supported by human studies, where both acute and chronic treatment with rimonabant exerted anxiogenic effects [56–60].
This ostensibly clear picture is obscured by a large body of conflicting evidence. Firstly, rimonabant did not always produce the effects presented above. Low doses ‒that decreased anxiety in the aforementioned studies‒ were sometimes without effect [28, 38, 61, 62]. High doses ‒anxiogenic in the studies presented above‒ were anxiolytic in the shock prod-burying paradigm [30]. Effects in humans were not replicated either [63]. Secondly, the effects of other antagonists were not always in line with those obtained with rimonabant. For instance, the CB1R blocker AM251 did not show the biphasic effect seen with rimonabant. This antagonist proved to be anxiogenic over a wide range of doses (0.3–8 mg/kg) [21, 25, 50, 64–68]. In addition, AM251 reduced urocortin1 microinjection- and nicotine abstinence-induced anxieties[69, 70]. Other antagonists (AM281, AM4113, and AVE1625) did not affect anxiety [66, 71–73].
Data on CB2R antagonists are sparse. Acute treatment with AM630, a CB2R antagonist, led to anxiogenic effects, while chronic treatment attenuated anxiety in the same paradigm [74].
Taken together, the findings briefly reviewed above are in line with expectations and show that the effects of inhibited endocannabinoid signaling are highly variable (for a summary see Table 4.1).
Increased Endocannabinoid Activity
Similar to the antagonist rimonabant, CB1R agonists have biphasic effects on anxiety. Surprisingly, however, the effects are not only biphasic but entirely similar to those seen with rimonabant (but not other antagonists): low doses decrease, while high doses increase anxiety. Anxiolytic effects were shown for low doses of the phytocannabinoid ∆9-tetrahydrocannabinol (THC; 0.075–2 mg/kg), the endocannabinoid anandamide (AEA; 0.1–1.25 mg/kg) and synthetic cannabinoids (WIN55,212–2: 0.5–3 mg/kg; CP55,940: < 0.1 mg/kg; HU210: 0.01 mg/kg) [21, 43, 53, 65, 67, 68, 75–90]. Higher doses of the same agonists (THC: 2.5–10 mg/kg; AEA: 10 mg/kg; WIN55,212–2: 3–5 mg/kg; CP55,940: > 0.1 mg/kg; HU210: 0.05–0.1 mg/kg) were anxiogenic [40, 44, 71, 78, 83, 89–104]. High doses of THC increased anxiety in humans as well [105–111].
This apparently consistent picture is blurred by a large body of conflicting evidence. Low doses of agonists ‒anxiolytic in the above studies‒ increased anxiety under specific conditions, such as repeated treatments in adults, perinatal administration and in rats that were chronically treated with vehicle before drug administration [112–115]. High doses of CB1R agonists ‒anxiogenic in the above studies—decreased anxiety in cocaine-self-administering subjects, in the 3,4-methylenedioxy-N-methylamphetamine-induced anxiety model, after chronic vehicle pretreatment and in adolescent subjects [116]. The biphasic effect was also overturned by species, strain, gender, and experimental conditions (e.g. enriched environment, treatments received in adolescence) [117]. Additionally, there is a large set of studies, in which doses that effectively altered anxiety in the above studies were without effects [54, 98, 101, 114, 118–123]. Inefficacy was sometimes seen under specific conditions, like stress-induced anxiety [124] or alcohol-withdrawal [125].
The enhancement of endocannabinoid signaling via the selective blockade of their degrading enzymes is a novel approach for the up-regulation of endocannabinoid activity [126–129]. Endocannabinoids are synthesized “on-demand”; therefore the blockade of their breakdown promotes ongoing signaling processes, i.e. their effects are more specific than those of agonists, which activate cannabinoid receptors throughout the brain. Both genetic and pharmacological blockade of the anandamide metabolizing enzyme, fatty acid amide hydrolase (FAAH), led to anxiolytic effects in a number of reports [43, 46, 67, 71, 86, 100, 126, 128, 130–138]. In other cases, however, no effects were seen either after genetic [139] or pharmacological blockade of FAAH activity [138–140]. FAAH inhibition was anxiogenic in one study [50]. Strong dependence on environmental conditions was reported in two studies [138, 139].
Studies on the specific role of 2-AG signaling were only recently made possible by the synthesis of the first selective, specific monoacylglycerol lipase (MAGL) blocker. This compound decreased anxiety in a number of studies [132, 134, 141, 142]. A few studies suggest that these effects depend on environmental aversiveness, and HPA-axis activity [143, 144].
Endocannabinoid signaling can also be stimulated by the inhibition of endocannabinoid transport. This treatment led to anxiolytic effects in a number of reports [43, 54, 87, 145–148]; no effects were seen in two studies [71, 149].
Taken together, the effects of pharmacological enhancement of endocannabinoid activity have variable effects on anxiety-like behavior. Findings are summarized in Table 4.2.
Local Brain Treatments
Neuron Type-Specific Effects
In this type of studies, transgenic animals were used; the selective disruption of CB1Rs in glutamatergic, dopaminergic and serotonergic neurons all increased anxiety [20, 29, 150]. The same manipulation in GABA-ergic neurons did not cause such changes [29]. One study suggests that cannabinoid signaling in serotonergic neurons ameliorates conditioned fear, despite the fact that the same transgenic animals showed anxiety in the elevated plus-maze [29]. By contrast, dopamine neuron-specific gene disruptions had congruent effects in the social interaction test of anxiety and conditioned fear [150].
Brain Area-Specific Effects
General effects. Blockade of CB1Rs in the brain by the intracerebroventricular injection of the CB1R antagonist AM251 increased anxiety [151], while the enhancement of endocannabinoid activity by FAAH administered via the same route was anxiolytic [133]. The effects of AM251 were reversed in animals treated with corticotrophin releasing hormone and in those submitted to cocaine-withdrawal [151]. Mice expressing CB1Rs only in the dorsal telencephalon showed reduced anxiety compared to CB1R KO mice [152].
Prefrontal cortex. The enhancement of cannabinoid signaling by cannabinoid agonists and FAAH inhibition had biphasic effects in this brain area; small doses decreased, while large doses increased anxiety [153, 154]. The genetic over-expression of the CB1Rs in the same area mimicked the effects of large doses, i.e. it increased anxiety [155]. Thus, the studies performed so far provide a congruent picture. Interestingly, the biphasic effects seen after systemic treatments were replicated by local agonist infusions into the prefrontal cortex. Similar biphasic effects were seldom reported in other brain regions.
Amygdala. We found only one study where local treatments were suggested to cover the whole amygdala; in this case, the cannabinoid agonist arachidonylcyclopropylamide (ACPA) reduced anxiety [156]. This effect was replicated by the infusion of agonists into the basolateral amygdala but not by local treatments targeting specifically the central amygdala. In the former region, agonists (∆9-THC, WIN55,212–2) and N-arachidonoyl-serotonin (a combined FAAH inhibitor/TRPV1 antagonist) reduced anxiety; the effect was valid to certain doses and particular conditions only, but no anxiogenic effects were observed at any dose [153, 157]. It is worth to note that no similar effects were observed with anandamide and pure FAAH inhibitors [158, 159], while ∆9-THC administration into the central amygdala increased anxiety [160].
Cannabinoid antagonists were administered into the basolateral, central, and medial amygdala. In the basolateral amygdala, where agonists decreased anxiety, antagonists increased it [69, 159, 161]; thus, the two types of treatments led to congruent effects in this brain region. In the central amygdala, antagonists (rimonabant, AM251) increased anxiety [161], similar to the agonist ∆9-THC. Thus, in this amygdala region, findings are incongruent. One study suggests that the local disruption of CB1R expression in the medial amygdala decreases anxiety [162].
Taken together, the studies reviewed above suggest that cannabinoid signaling in the basolateral amygdala decreases anxiety. Reports on other amygdalar subregions are disparate, but suggest that the effects of cannabinoid signaling are amygdala subarea-specific.
Hippocampus. Agonists or FAAH inhibitors were infused into the CA1 region in three studies: effects were contrasting as anxiogenic effects [163], no effects [164] or anxiolytic effects [165] were observed. CB1R blockade in the very same brain region either decreased or increased anxiety [163, 166]. In the ventral hippocampus, the enhancement of endocannabinoid signaling by agonists (∆9-THC, high doses), as well as by FAAH or reuptake blockade resulted in anxiogenesis [153, 167, 168], while the blockade of CB1Rs did not affect anxiety [167]. Noteworthy, the effects of ∆9-THC were biphasic, while the effects of reuptake blockade were reversed by stress exposure [153, 167, 168].
Periaqueductal gray. Cannabinoid receptor agonists (2-AG, AEA, ACEA), the blockade of MAGL, as well as the inhibition of cannabinoid reuptake in the dorsal and dorsolateral periaqueductal gray decreased anxiety [141, 169–172]. The CB1R antagonist AM251 was without effect [172]. Except for this latter finding, the anxiolytic roles of cannabinoid signaling in the dorsal/dorsolateral periaqueductal gray appear well supported.
Other brain regions. The local deletion of CB1Rs in the posterior hypothalamus, the paraventricular and supraoptic nuclei increased anxiety [162]. The microinjection of AM251 into the enteropeduncular nucleus also increased anxiety [160].
Conclusions
The number of studies on neuron type-specific and brain area-specific roles of cannabinoid signaling in anxiety are clearly insufficient to draw definite conditions. Nevertheless, the findings obtained so far suggest that cannabinoids have anxiolytic effects in most brain regions. As exception, they appear to have biphasic effects in the prefrontal cortex, and anxiogenic effects in the ventral hippocampus. Data in the dorsal hippocampus and medial amygdala are sparse. Findings appear to be rather congruent in many brain regions, and neuron types. The brain area-specific effects of cannabinoids on anxiety are summarized in Table 4.3.
Interpretation
Clearly, data on the anxiety-related effects of cannabinoids are conflicting, but the thorough overview of the available findings leads to a series of interesting conclusions:
-
The less reliable findings were obtained with cannabinoid agonists and antagonists. The most blatant dissimilarities relate to the biphasic effect of such treatments. Biphasic effects are not particularly unusual in pharmacology, but in the case of cannabinoid ligands, antagonists and agonists have highly similar effect profiles: small doses of both decrease anxiety, while large doses of both increase anxiety. In addition, the largest number of conflicting findings was obtained with these experimental tools.
-
The selective genetic disruption of cannabinoid receptors provided more congruent findings: this procedure increased anxiety in the overwhelming majority reports. One study reported no effects, while another reported context-dependent effects which included anxiogenesis under particular conditions and no effects under other conditions. In addition, one of the reports where anxiolytic effects were observed employed the shock-prod burying paradigm, a mixed anxiety and coping test [173]. Effects on coping will be discussed below. In conclusion, the anxiogenic effects of CB1R disruption is contradicted by one single study, and no effects were obtained in another.
-
Findings obtained with agents that indirectly modulate endocannabinoid signaling (FAAH, MAGL, and reuptake blockers) are not devoid of contradictions, but again the overwhelming majority of findings suggest that such agents decrease anxiety. This statement is supported by 27 studies. Condition-dependent effects were obtained in 4 studies (usually implicating anxiolysis under particular conditions) and no effects were obtained in 3 studies. Anxiogenic effects were obtained in one study only.
-
Local brain treatments with cannabinoid agents provided the most consistent sets of data. There are virtually no contradictions in the case of certain brain areas, while opposing effects are missing in other cases (e.g. discrepancies are between effects and no effects).
The perspective summarized above raise a series of questions; the following sections are attempts to answer them.
Why are the Effects of Receptor Ligands Less Reliable than Those of Indirect Modulators?
The characteristics of endocannabinoid signaling and those of receptor ligands decrease the reliability of the latter as experimental tools. Endocannabinoids are secreted from the post-synaptic membrane and retrogradely inhibit the synaptic neurotransmission that triggered their release [174]. Although a probably low level of tonic activation cannot be excluded, the endocannabinoid signal occurs phasically i.e. when the intensity of anterograde synaptic communication reaches certain levels [175–178]. As such, the main role of endocannabinoid signaling appears to be the blockade of excessive neuronal activation [179].
Agonists overrule this finely tuned mechanism by inhibiting neurotransmission in synapses where this is not justified by its intensity, i.e. where retrograde signaling is not activated under normal conditions. As such, the effects of agonists are broader than those of endocannabinoids, and instead of mimicking natural activity they extend effects to synapses, neurons and brain areas where such activity normally does not take place.
Antagonists on their turn (especially those extensively used in anxiety research), have inverse agonist properties, by which they also overrule the above-described mechanism. Instead of inhibiting endocannabinoid signaling, their inverse agonist effects inhibit neuronal discharges in areas where endocannabinoids are normally not released. Thus, their effects are also extended to synapses, neurons and brain areas where endocannabinoids are not active.
In addition, many of the tools regularly used to affect receptor function affect both CB1Rs and CB2Rs. Originally, this was not perceived as a problem, but relatively recent findings demonstrate that CB2Rs are expressed in the brain and have roles in behavior control [180]. In addition, receptor ligands also bind to other receptors, for instance to the still poorly known “third” cannabinoid receptor as well as to the GPR55 and TRPV1 receptors [181]. Naturally, endocannabinoids also bind to these receptors non-selectively; however, they affect the function of these mechanisms in spatially and temporally selective ways, while exogenous receptor ligands act indiscriminately.
A third problem with exogenous ligands is that their brain distribution is not uniform; moreover, different receptor ligands have specific patterns of brain distribution. For instance, two times more WIN55,212–2 was found in the hypothalamus than in the amygdala after the systemic administration of the compound; by contrast, the amounts of the antagonist rimonabant (administered by the same route) were similar in these two brain regions [182]. While the issue remains understudied, the available findings strongly suggest that compound-specific brain distribution patterns constitute an additional confounding factor in the elucidation of the roles of endocannabinoids in behavioral control. Furthermore, cannabinoid receptor ligands may show species- and neuron type-specific ligand sensitivity. Electrophysiological studies showed for instance that WIN-55,212–2 preferentially affected GABA-ergic neurotransmission in mice, while the same compound appeared to affect glutamatergic neurotransmission in rats, which together with species- and neuron type-specific effects of AM251 led to large species differences in the behavioral effects of these ligands and marked differences in their interaction [23].
The use of indirect modulators circumvents most these problems. Metabolic enzyme inhibitors and reuptake blockers enhance and prolong naturally occurring endocannabinoid release. Consequently, the up-regulation of endocannabinoid signaling is restricted to synapses, neurons and brain regions where the system is activated by the behavioral paradigm investigated. The enhanced activation of natural endocannabinoid signaling also eliminates problems related to receptor specificity, brain distribution and ligand sensitivity.
Why are Gene Disruption and Local Treatments More Reliable than Receptor Ligands?
The problems related to the use of receptor ligands are also circumvented by the genetic disruption of the endocannabinoid receptor and by the local brain administration of compounds. The gene disruption technique has its own flaws, among which the development of compensatory mechanisms are believed to have the largest impact on experimental findings. At the same time, however, most of the problems raised by the use of receptor ligands are avoided by this technique. The reason is the spatio-temporal overlap of networks activated by a behavioral context and the lack of receptors in these networks. While receptors are eliminated throughout the brain, the consequences of this are manifested only at those synapses which are activated under the conditions of a particular study. The effects of gene disruption on networks that are unrelated to the context (i.e. are not “working” when a particular behavior is expressed) remain “silent” because they do not contribute to the execution of the behavioral act. Therefore, gene disruption eliminates naturally occurring cannabinoid signaling without having effects on other mechanisms. The same holds true for selectivity: while receptor ligands act on more than one receptor, gene disruptions are selective in this respect. Finally, problems associated by ligand-specific brain distribution patterns and ligand specificity are not present in receptor knockouts, where the ligands are the natural ones, i.e. endocannabinoids.
The local application of receptor ligands involves all the problems associated with direct receptor modulation, but these are spatially restricted, and by this their consequences are minimized. In other words, nonspecific effects at the targeted brain area are not amplified by nonspecific effects at other brain sites. Moreover, local applications eliminate the problem of differential effects exerted in certain brain regions. As shown above, the local administration of cannabinoids results in anxiolysis in some but not all brain regions. Systemically administered cannabinoids activate in parallel biphasic effects in the prefrontal cortex, anxiolytic effects in the amygdala, and anxiogenic effects in the hippocampus, while local administration activate only one of these mechanisms, which leads to clearer findings.
Why are Effects Condition-Dependent?
It is a common observation that the condition of subjects and experimental conditions have a large impact on how cannabinoids affect anxiety; examples were outlined above and will not be reiterated here. One possible interpretation of such condition-dependent effects is that cannabinoids do not affect particular behaviors but affect the way in which the organism responds to challenges, i.e. they affect coping styles. We identified four papers addressing the effects of cannabinoids from this perspective [25, 183–185]. Taken together, these studies suggest that cannabinoids promote active coping, which is associated with anxiolytic-like and antidepressant-like effects in particular tests.
Active and passive coping styles are two distinct behavioral phenotypes which differ in the way challenges are dealt with, and which show a bimodal distribution [186, 187]. Behavior is internally driven and problem oriented in active copers. In contrast, passive copers are governed by environmental stimuli and tend to respond challenges by avoidant behavior. These temporally stable behavioral phenotypes have adaptive significance in animals, while in humans, active (type “A”) and passive (particularly type “C”) coping styles influence disease susceptibility and resilience under adverse conditions [187–189]. Moreover, coping styles are believed to reliably predict disease-induced decreases in quality of life [190, 191]. Consequently, interventions promoting active coping styles -which are associated more favorably with resilience- have been proposed as therapeutic goals for a variety of physical diseases and mental disorders [190, 192, 193]. Thus, the putative effects of endocannabinoid signaling on coping styles are highly relevant from a therapeutic point of view.
The relationships between cannabinoids and coping on one side, and cannabinoids and anxiety on the other side have not been elucidated so far. There are several scenarios that may be considered: (1) cannabinoids affect anxiety in the first place, and promote active coping by decreasing anxiety; (2) cannabinoids affect coping in the first place, and their anxiolytic effects are context-dependent consequences of the shift in coping styles; (3) effects on coping and anxiety are mediated by different cannabinoid-dependent mechanisms that interact under specific conditions.
Conclusions
Overall, the findings suggest that cannabinoid signaling decreases anxiety. The number of conflicting findings is large. A comparison of different technologies demonstrates that the reliability of findings is rather low with receptor ligands (agonists and antagonists). Considerably more consistent findings were obtained with gene knockouts, the indirect enhancement of endocannabinoid signaling (e.g. enzyme inhibitors), and local brain treatments. The anxiolytic effects of cannabinoid signaling are more robustly shown by the latter three as compared with the former approach, but notably, the effects of cannabinoids is not uniform across brain areas. In the prefrontal cortex, biphasic effects were noticed (anxiolysis at low and anxiogenesis at large doses), while in the amygdala and hippocampus cannabinoids seem to decrease and increase, respectively, anxiety-like behavior. The condition of subjects and experimental conditions have a strong impact on the effects of cannabinoids, and this seems to be independent from the technique employed to manipulate endocannabinoid signaling. Recent findings demonstrate that cannabinoids promote a shift from passive to active coping with challenges, which may explain the context-dependence of their anxiety-related effects, and may broaden their therapeutic implications. The relationship and directionality of the triple association between cannabinoid signaling, anxiety and coping styles is largely understudied, but holds great promise for the understanding of the roles of cannabinoids in behavioral control, and the therapeutic potentials of cannabinoid modulators.
Notes
- 1.
This compound has anxiolytic properties [1–14], and as such it is highly relevant to anxiety research in general. However, cannabidiol binds to cannabinoid receptors with very low affinity [15], and its mechanisms are either indirectly related to endocannabinoid signaling [16] or involve direct effects on other neurotransmitter systems [17]. Therefore, data on cannabidiol were not reviewed here.
References
Uribe-Marino A, Francisco A, Castiblanco-Urbina MA, Twardowschy A, Salgado-Rohner CJ, Crippa JA, Hallak JE, Zuardi AW, Coimbra NC. Anti-aversive effects of cannabidiol on innate fear-induced behaviors evoked by an ethological model of panic attacks based on a prey vs the wild snake Epicrates cenchria crassus confrontation paradigm. Neuropsychopharmacology. 2012;37(2):412–21.
Casarotto PC, Gomes FV, Resstel LB, Guimaraes FS. Cannabidiol inhibitory effect on marble-burying behaviour: involvement of CB1 receptors. Behav Pharmacol. 2010;21(4):353–58.
Deiana S, Watanabe A, Yamasaki Y, Amada N, Arthur M, Fleming S, Woodcock H, Dorward P, Pigliacampo B, Close S, Platt B, Riedel G. Plasma and brain pharmacokinetic profile of cannabidiol (CBD), cannabidivarine (CBDV), Delta(9)-tetrahydrocannabivarin (THCV) and cannabigerol (CBG) in rats and mice following oral and intraperitoneal administration and CBD action on obsessive-compulsive behaviour. Psychopharmacology (Berl). 2012;219(3):859–73.
Campos AC, Ferreira FR, Guimaraes FS. Cannabidiol blocks long-lasting behavioral consequences of predator threat stress: possible involvement of 5HT1A receptors. J Psychiatr Res. 2012;46(11):1501–10.
Guimaraes FS, Chiaretti TM, Graeff FG, Zuardi AW. Antianxiety effect of cannabidiol in the elevated plus-maze. Psychopharmacology (Berl). 1990;100(4):558–9.
Resstel LB, Tavares RF, Lisboa SF, Joca SR, Correa FM, Guimaraes FS. 5-HT1A receptors are involved in the cannabidiol-induced attenuation of behavioural and cardiovascular responses to acute restraint stress in rats. Br J Pharmacol. 2009;156(1):181–88.
Campos AC, Guimaraes FS. Evidence for a potential role for TRPV1 receptors in the dorsolateral periaqueductal gray in the attenuation of the anxiolytic effects of cannabinoids. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33(8):1517–21.
Campos AC, de Paula Soares V, Carvalho MC, Ferreira FR, Vicente MA, Brandao ML, Zuardi AW, Zangrossi H, Jr., Guimaraes FS. Involvement of serotonin-mediated neurotransmission in the dorsal periaqueductal gray matter on cannabidiol chronic effects in panic-like responses in rats. Psychopharmacology (Berl). 2013;226(1):13–24.
Guimaraes FS, de Aguiar JC, Mechoulam R, Breuer A. Anxiolytic effect of cannabidiol derivatives in the elevated plus-maze. Gen Pharmacol. 1994;25(1):161–64.
Gomes FV, Resstel LB, Guimaraes FS. The anxiolytic-like effects of cannabidiol injected into the bed nucleus of the stria terminalis are mediated by 5-HT1A receptors. Psychopharmacology (Berl). 2011;213(2–3):465–73.
Granjeiro EM, Gomes FV, Guimaraes FS, Correa FM, Resstel LB. Effects of intracisternal administration of cannabidiol on the cardiovascular and behavioral responses to acute restraint stress. Pharmacol Biochem Behav. 2011;99(4):743–48.
Long LE, Chesworth R, Huang XF, McGregor IS, Arnold JC, Karl T. A behavioural comparison of acute and chronic Delta9-tetrahydrocannabinol and cannabidiol in C57BL/6JArc mice. Int J Neuropsychopharmacol. 2010;13(7):861–76.
Moreira FA, Aguiar DC, Guimaraes FS. Anxiolytic-like effect of cannabidiol in the rat Vogel conflict test. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(8):1466–71.
Soares Vde P Campos AC Bortoli VC Zangrossi H Jr. Guimaraes FS Zuardi AW. Intra-dorsal periaqueductal gray administration of cannabidiol blocks panic-like response by activating 5-HT1A receptors. Behav Brain Res. 2010;213(2):225–29.
Pertwee RG. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. Br J Pharmacol. 2008;153(2):199–215.
Hayakawa K, Mishima K, Hazekawa M, Sano K, Irie K, Orito K, Egawa T, Kitamura Y, Uchida N, Nishimura R, Egashira N, Iwasaki K, Fujiwara M. Cannabidiol potentiates pharmacological effects of Delta(9)-tetrahydrocannabinol via CB(1) receptor-dependent mechanism. Brain Res. 2008;1188:157–64.
Russo EB, Burnett A, Hall B, Parker KK. Agonistic properties of cannabidiol at 5-HT1a receptors. Neurochem Res. 2005;30(8):1037–43.
Derks NM, Pinter O, Zuure W, Ledent C, Watanabe M, Molnar CS, Wei Y, Roubos EW, Wu S, Hrabovszky E, Zelena D, Kozicz T. Cannabinoid modulation of midbrain urocortin 1 neurones during acute and chronic stress. J Neuroendocrinol. 2012;24(11):1447–61.
Hill MN, Hillard CJ, McEwen BS. Alterations in corticolimbic dendritic morphology and emotional behavior in cannabinoid CB1 receptor-deficient mice parallel the effects of chronic stress. Cereb Cortex. 2011;21(9):2056–64.
Jacob W, Yassouridis A, Marsicano G, Monory K, Lutz B, Wotjak CT. Endocannabinoids render exploratory behaviour largely independent of the test aversiveness: role of glutamatergic transmission. Genes Brain Behav. 2009;8(7):685–98.
Haller J, Varga B, Ledent C, Freund TF. CB1 cannabinoid receptors mediate anxiolytic effects: convergent genetic and pharmacological evidence with CB1-specific agents. Behav Pharmacol. 2004;15(4):299–304.
Uriguen L, Perez-Rial S, Ledent C, Palomo T, Manzanares J. Impaired action of anxiolytic drugs in mice deficient in cannabinoid CB1 receptors. Neuropharmacology. 2004;46(7):966–73.
Haller J, Bakos N, Szirmay M, Ledent C, Freund TF. The effects of genetic and pharmacological blockade of the CB1 cannabinoid receptor on anxiety. Eur J Neurosci. 2002;16(7):1395–98.
Martin M, Ledent C, Parmentier M, Maldonado R, Valverde O. Involvement of CB1 cannabinoid receptors in emotional behaviour. Psychopharmacology. 2002;159(4):379–87.
Litvin Y, Phan A, Hill MN, Pfaff DW, McEwen BS. CB1 receptor signaling regulates social anxiety and memory. Genes Brain Behav. 2013;12(5):479–89.
Maccarrone M, Valverde O, Barbaccia ML, Castane A, Maldonado R, Ledent C, Parmentier M, Finazzi-Agro A. Age-related changes of anandamide metabolism in CB1 cannabinoid receptor knockout mice: correlation with behaviour. Eur J Neurosci. 2002;15(7):1178–86.
Haller J, Varga B, Ledent C, Barna I, Freund TF. Context-dependent effects of CB1 cannabinoid gene disruption on anxiety-like and social behaviour in mice. Eur J Neurosci. 2004;19(7):1906–12.
Thiemann G, Watt CA, Ledent C, Molleman A, Hasenohrl RU. Modulation of anxiety by acute blockade and genetic deletion of the CB(1) cannabinoid receptor in mice together with biogenic amine changes in the forebrain. Behav Brain Res. 2009;200(1):60–7.
Dubreucq S, Matias I, Cardinal P, Haring M, Lutz B, Marsicano G, Chaouloff F. Genetic dissection of the role of cannabinoid type-1 receptors in the emotional consequences of repeated social stress in mice. Neuropsychopharmacology. 2012;37(8):1885–1900.
Degroot A, Nomikos GG. Genetic deletion and pharmacological blockade of CB1 receptors modulates anxiety in the shock-probe burying test. Eur J Neurosci. 2004;20(4):1059–64.
Ortega-Alvaro A, Aracil-Fernandez A, Garcia-Gutierrez MS, Navarrete F, Manzanares J. Deletion of CB2 cannabinoid receptor induces schizophrenia-related behaviors in mice. Neuropsychopharmacology. 2011;36(7):1489–1504.
Flake NM, Zweifel LS. Behavioral effects of pulp exposure in mice lacking cannabinoid receptor 2. J Endod. 2012;38(1):86–90.
Ryberg E, Larsson N, Sjogren S, Hjorth S, Hermansson NO, Leonova J, Elebring T, Nilsson K, Drmota T, Greasley PJ. The orphan receptor GPR55 is a novel cannabinoid receptor. Br J Pharmacol. 2007;152(7):1092–101.
Lauckner JE, Jensen JB, Chen HY, Lu HC, Hille B, Mackie K. GPR55 is a cannabinoid receptor that increases intracellular calcium and inhibits M current. Proc Natl Acad Sci USA. 2008;105(7):2699–704.
Sharir H, Abood ME. Pharmacological characterization of GPR55, a putative cannabinoid receptor. Pharmacol Ther. 2010;126(3):301–13.
Wu CS, Chen H, Sun H, Zhu J, Jew CP, Wager-Miller J, Straiker A, Spencer C, Bradshaw H, Mackie K, Lu HC. GPR55, a G-protein coupled receptor for lysophosphatidylinositol, plays a role in motor coordination. PloS ONE. 2013;8(4):e60314.
Rodgers RJ, Haller J, Halasz J, Mikics E. ‘One-trial sensitization’ to the anxiolytic-like effects of cannabinoid receptor antagonist SR141716A in the mouse elevated plus-maze. Eur J Neurosci. 2003;17(6):1279–86.
Griebel G, Stemmelin J, Scatton B. Effects of the cannabinoid CB1 receptor antagonist rimonabant in models of emotional reactivity in rodents. Biol Psychiatry. 2005;57(3):261–67.
Rubio M, Fernandez-Ruiz J, de Miguel R, Maestro B, Michael Walker J, Ramos JA. CB1 receptor blockade reduces the anxiogenic-like response and ameliorates the neurochemical imbalances associated with alcohol withdrawal in rats. Neuropharmacology. 2008;54(6):976–88.
Akinshola BE, Chakrabarti A, Onaivi ES. In-vitro and in-vivo action of cannabinoids. Neurochem Res. 1999;24(10):1233–40.
Takahashi RN, Pamplona FA, Fernandes MS. The cannabinoid antagonist SR141716A facilitates memory acquisition and consolidation in the mouse elevated T-maze. Neurosci Lett. 2005;380(3):270–75.
Huang P, Liu-Chen LY, Kirby LG. Anxiety-like effects of SR141716-precipitated delta9-tetrahydrocannabinol withdrawal in mice in the elevated plus-maze. Neurosci Lett. 2010;475(3):165–68.
Patel S, Hillard CJ. Pharmacological evaluation of cannabinoid receptor ligands in a mouse model of anxiety: further evidence for an anxiolytic role for endogenous cannabinoid signaling. J Pharmacol Exp Ther. 2006;318(1):304–11.
Arevalo C, de Miguel R, Hernandez-Tristan R. Cannabinoid effects on anxiety-related behaviours and hypothalamic neurotransmitters. Pharmacol Biochem Behav. 2001;70(1):123–31.
Navarro M, Hernandez E, Munoz RM, del Arco I, Villanua MA, Carrera MR, Rodriguez de Fonseca F. Acute administration of the CB1 cannabinoid receptor antagonist SR 141716A induces anxiety-like responses in the rat. Neuroreport. 1997;8(2):491–96.
Moise AM, Eisenstein SA, Astarita G, Piomelli D, Hohmann AG. An endocannabinoid signaling system modulates anxiety-like behavior in male Syrian hamsters. Psychopharmacology. 2008;200(3):333–46.
Blasio A, Iemolo A, Sabino V, Petrosino S, Steardo L, Rice KC, Orlando P, Iannotti FA, Di Marzo V, Zorrilla EP, Cottone P. Rimonabant precipitates anxiety in rats withdrawn from palatable food: role of the central amygdala. Neuropsychopharmacology. 2013;38(12):2498–507.
O’Brien LD, Wills KL, Segsworth B, Dashney B, Rock EM, Limebeer CL, Parker LA. Effect of chronic exposure to rimonabant and phytocannabinoids on anxiety-like behavior and saccharin palatability. Pharmacol Biochem Behav. 2013;103(3):597–602.
Gamble-George JC, Conger JR, Hartley ND, Gupta P, Sumislawski JJ, Patel S. Dissociable effects of CB1 receptor blockade on anxiety-like and consummatory behaviors in the novelty-induced hypophagia test in mice. Psychopharmacology (Berl). 2013;228(3):401–9.
Seillier A, Martinez AA, Giuffrida A. Phencyclidine-induced social withdrawal results from deficient stimulation of cannabinoid CB(1) receptors: implications for schizophrenia. Neuropsychopharmacology. 2013;38(9):1816–24.
Varga B, Kassai F, Gyertyan I. Interactions of CB1 and mGlu5 receptor antagonists in food intake, anxiety and memory models in rats. Pharmacol Biochem Behav. 2012;103(2):425–30.
Hofelmann D, di Benedetto B, Azad SC, Micale V, Wotjak CT, Rammes G. Lack of interaction of endocannabinoids and 5-HT(3) neurotransmission in associative fear circuits of the amygdala: evidence from electrophysiological and behavioural experiments. Brain Res. 2013;1527:47–56.
Pamplona FA, Prediger RD, Pandolfo P, Takahashi RN. The cannabinoid receptor agonist WIN 55,212–2 facilitates the extinction of contextual fear memory and spatial memory in rats. Psychopharmacology (Berl). 2006;188(4):641–49.
Chhatwal JP, Davis M, Maguschak KA, Ressler KJ. Enhancing cannabinoid neurotransmission augments the extinction of conditioned fear. Neuropsychopharmacology. 2005;30(3):516–24.
Chhatwal JP, Gutman AR, Maguschak KA, Bowser ME, Yang Y, Davis M, Ressler KJ. Functional interactions between endocannabinoid and CCK neurotransmitter systems may be critical for extinction learning. Neuropsychopharmacology. 2009;34(2):509–21.
Van Gaal L Pi-Sunyer X Despres JP McCarthy C Scheen A. Efficacy and safety of rimonabant for improvement of multiple cardiometabolic risk factors in overweight/obese patients: pooled 1-year data from the Rimonabant in Obesity (RIO) program. Diabetes Care. 2008;31(2):229–40.
Dibble CT, Gelfand EV, Cannon CP. Rimonabant: the role of endocannabinoid type 1 receptor antagonism in modulating the weight and lipid profile of obese patients. Curr Atheroscler Rep. 2007;9(5):359–66.
Hollander PA, Amod A, Litwak LE, Chaudhari U. Effect of rimonabant on glycemic control in insulin-treated type 2 diabetes: the ARPEGGIO trial. Diabetes Care. 2010;33(3):605–7.
Doggrell SA. Is rimonabant efficacious and safe in the treatment of obesity? Expert Opin Pharmacother. 2008;9(15):2727–31.
Christensen R, Kristensen PK, Bartels EM, Bliddal H, Astrup A. Efficacy and safety of the weight-loss drug rimonabant: a meta-analysis of randomised trials. Lancet. 2007;370(9600):1706–13.
Lopez-Moreno JA, Gonzalez-Cuevas G, Navarro M. The CB1 cannabinoid receptor antagonist rimonabant chronically prevents the nicotine-induced relapse to alcohol. Neurobiol Dis. 2007;25(2):274–83.
Assareh N, ElBatsh MM, Marsden CA, Kendall DA. The effects of chronic administration of tranylcypromine and rimonabant on behaviour and protein expression in brain regions of the rat. Pharmacol Biochem Behav. 2012;100(3):506–12.
Horder J, Browning M, Di Simplicio M, Cowen PJ, Harmer CJ. Effects of 7 days of treatment with the cannabinoid type 1 receptor antagonist, rimonabant, on emotional processing. J Psychopharmacol. 2012;26(1):125–32.
Rodgers RJ, Evans PM, Murphy A. Anxiogenic profile of AM-251, a selective cannabinoid CB1 receptor antagonist, in plus-maze-naive and plus-maze-experienced mice. Behav Pharmacol. 2005;16(5–6):405–13.
Haller J, Matyas F, Soproni K, Varga B, Barsy B, Nemeth B, Mikics E, Freund TF, Hajos N. Correlated species differences in the effects of cannabinoid ligands on anxiety and on GABAergic and glutamatergic synaptic transmission. Eur J Neurosci. 2007;25(8):2445–6.
Sink KS, Segovia KN, Sink J, Randall PA, Collins LE, Correa M, Markus EJ, Vemuri VK, Makriyannis A, Salamone JD. Potential anxiogenic effects of cannabinoid CB1 receptor antagonists/inverse agonists in rats: comparisons between AM4113, AM251, and the benzodiazepine inverse agonist FG-7142. Eur Neuropsychopharmacol. 2010;20(2):112–22.
Gobira PH, Aguiar DC, Moreira FA. Effects of compounds that interfere with the endocannabinoid system on behaviors predictive of anxiolytic and panicolytic activities in the elevated T-maze. Pharmacol Biochem Behav. 2013;110:33–9.
Cagni P, Barros M. Cannabinoid type 1 receptor ligands WIN 55,212–2 and AM 251 alter anxiety-like behaviors of marmoset monkeys in an open-field test. Behav Brain Res. 2013;240:91–4.
Dono LM, Currie PJ. The cannabinoid receptor CB(1) inverse agonist AM251 potentiates the anxiogenic activity of urocortin I in the basolateral amygdala. Neuropharmacology. 2012;62(1):192–99.
Aydin C, Oztan O, Isgor C. Nicotine-induced anxiety-like behavior in a rat model of the novelty-seeking phenotype is associated with long-lasting neuropeptidergic and neuroplastic adaptations in the amygdala: effects of the cannabinoid receptor 1 antagonist AM251. Neuropharmacology. 2012;63(8):1335–45.
Rutkowska M, Jamontt J, Gliniak H. Effects of cannabinoids on the anxiety-like response in mice. Pharmacol Rep. 2006;58(2):200–06.
Jiang W, Zhang Y, Xiao L, Van Cleemput J, Ji SP, Bai G, Zhang X. Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic- and antidepressant-like effects. J Clin Invest. 2005;115(11):3104–16.
Black MD, Stevens RJ, Rogacki N, Featherstone RE, Senyah Y, Giardino O, Borowsky B, Stemmelin J, Cohen C, Pichat P, Arad M, Barak S, De Levie A, Weiner I, Griebel G, Varty GB. AVE1625, a cannabinoid CB1 receptor antagonist, as a co-treatment with antipsychotics for schizophrenia: improvement in cognitive function and reduction of antipsychotic-side effects in rodents. Psychopharmacology (Berl). 2011;215(1):149–63.
Garcia-Gutierrez MS, Garcia-Bueno B, Zoppi S, Leza JC, Manzanares J. Chronic blockade of cannabinoid CB2 receptors induces anxiolytic-like actions associated with alterations in GABA(A) receptors. Br J Pharmacol. 2012;165(4):951–64.
Fokos S, Panagis G. Effects of delta9-tetrahydrocannabinol on reward and anxiety in rats exposed to chronic unpredictable stress. J Psychopharmacol. 2010;24(5):767–77.
Braida D, Limonta V, Malabarba L, Zani A, Sala M. 5-HT1A receptors are involved in the anxiolytic effect of Delta9-tetrahydrocannabinol and AM 404, the anandamide transport inhibitor, in Sprague-Dawley rats. Eur J Pharmacol. 2007;555(2–3):156–63.
Rubino T, Sala M, Vigano D, Braida D, Castiglioni C, Limonta V, Guidali C, Realini N, Parolaro D. Cellular mechanisms underlying the anxiolytic effect of low doses of peripheral Delta9-tetrahydrocannabinol in rats. Neuropsychopharmacology. 2007;32(9):2036–45.
Harte-Hargrove LC, Dow-Edwards DL. Withdrawal from THC during adolescence: sex differences in locomotor activity and anxiety. Behav Brain Res. 2012;231(1):48–59.
Berrendero F, Maldonado R. Involvement of the opioid system in the anxiolytic-like effects induced by Delta(9)-tetrahydrocannabinol. Psychopharmacology (Berl). 2002;163(1):111–17.
Valjent E, Mitchell JM, Besson MJ, Caboche J, Maldonado R. Behavioural and biochemical evidence for interactions between Delta9-tetrahydrocannabinol and nicotine. Br J Pharmacol. 2002;135(2):564–78.
Spano MS, Fattore L, Cadeddu F, Fratta W, Fadda P. Chronic cannabinoid exposure reduces phencyclidine-induced schizophrenia-like positive symptoms in adult rats. Psychopharmacology (Berl). 2013;225(3):531–42.
Barba-Escobedo PA, Gould GG. Visual social preferences of lone zebrafish in a novel environment: strain and anxiolytic effects. Genes Brain Behav. 2012;11(3):366–73.
Hill MN, Gorzalka BB. Enhancement of anxiety-like responsiveness to the cannabinoid CB(1) receptor agonist HU-210 following chronic stress. Eur J Pharmacol. 2004;499(3):291–95.
Ribeiro A, Ferraz-de-Paula V, Pinheiro ML, Palermo-Neto J. Dose-response effects of systemic anandamide administration in mice sequentially submitted to the open field and elevated plus-maze tests. Braz J Med Biol Res. 2009;42(6):556–60.
Umathe SN, Manna SS, Utturwar KS, Jain NS. Endocannabinoids mediate anxiolytic-like effect of acetaminophen via CB1 receptors. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33(7):1191–99.
Scherma M, Medalie J, Fratta W, Vadivel SK, Makriyannis A, Piomelli D, Mikics E, Haller J, Yasar S, Tanda G, Goldberg SR. The endogenous cannabinoid anandamide has effects on motivation and anxiety that are revealed by fatty acid amide hydrolase (FAAH) inhibition. Neuropharmacology. 2008;54(1):129–40.
Naderi N, Haghparast A, Saber-Tehrani A, Rezaii N, Alizadeh AM, Khani A, Motamedi F. Interaction between cannabinoid compounds and diazepam on anxiety-like behaviour of mice. Pharmacol Biochem Behav. 2008;89(1):64–75.
Panlilio LV, Solinas M, Matthews SA, Goldberg SR. Previous exposure to THC alters the reinforcing efficacy and anxiety-related effects of cocaine in rats. Neuropsychopharmacology. 2007;32(3):646–57.
Rey AA, Purrio M, Viveros MP, Lutz B. Biphasic effects of cannabinoids in anxiety responses: CB1 and GABA(B) receptors in the balance of GABA-ergic and glutamatergic neurotransmission. Neuropsychopharmacology. 2012;37(12):2624–34.
Marco EM, Perez-Alvarez L, Borcel E, Rubio M, Guaza C, Ambrosio E, File SE, Viveros MP. Involvement of 5-HT1A receptors in behavioural effects of the cannabinoid receptor agonist CP 55,940 in male rats. Behav Pharmacol. 2004;15(1):21–7.
Onaivi ES, Green MR, Martin BR. Pharmacological characterization of cannabinoids in the elevated plus maze. J Pharmacol Exp Ther. 1990;253(3):1002–9.
Trezza V, Campolongo P, Cassano T, Macheda T, Dipasquale P, Carratu MR, Gaetani S, Cuomo V. Effects of perinatal exposure to delta-9-tetrahydrocannabinol on the emotional reactivity of the offspring: a longitudinal behavioral study in Wistar rats. Psychopharmacology (Berl). 2008;198(4):529–37.
Schramm-Sapyta NL, Cha YM, Chaudhry S, Wilson WA, Swartzwelder HS, Kuhn CM. Differential anxiogenic, aversive, and locomotor effects of THC in adolescent and adult rats. Psychopharmacology (Berl). 2007;191(4):867–77.
Page ME, Oropeza VC, Sparks SE, Qian Y, Menko AS, Van Bockstaele EJ. Repeated cannabinoid administration increases indices of noradrenergic activity in rats. Pharmacol Biochem Behav. 2007;86(1):162–68.
Lin HC, Mao SC, Chen PS, Gean PW. Chronic cannabinoid administration in vivo compromises extinction of fear memory. Learn Mem. 2008;15(12):876–84.
Giuliani D, Ferrari F, Ottani A. The cannabinoid agonist HU 210 modifies rat behavioural responses to novelty and stress. Pharmacol Res. 2000;41(1):47–53.
McLaughlin PJ, Lu D, Winston KM, Thakur G, Swezey LA, Makriyannis A, Salamone JD. Behavioral effects of the novel cannabinoid full agonist AM 411. Pharmacol Biochem Behav. 2005;81(1):78–88.
Panlilio LV, Mazzola C, Medalie J, Hahn B, Justinova Z, Drago F, Cadet JL, Yasar S, Goldberg SR. Anandamide-induced behavioral disruption through a vanilloid-dependent mechanism in rats. Psychopharmacology (Berl). 2009;203(3):529–38.
Macri S, Ceci C, Altabella L, Canese R, Laviola G. The Directive 2010/63/EU on animal experimentation may skew the conclusions of pharmacological and behavioural studies. Sci Rep. 2013;3:2380.
Bambico FR, Cassano T, Dominguez-Lopez S, Katz N, Walker CD, Piomelli D, Gobbi G. Genetic deletion of fatty acid amide hydrolase alters emotional behavior and serotonergic transmission in the dorsal raphe, prefrontal cortex, and hippocampus. Neuropsychopharmacology. 2010;35(10):2083–100.
Hill MN, Gorzalka BB. Increased sensitivity to restraint stress and novelty-induced emotionality following long-term, high dose cannabinoid exposure. Psychoneuroendocrinology. 2006;31(4):526–36.
Marin S, Marco E, Biscaia M, Fernandez B, Rubio M, Guaza C, Schmidhammer H, Viveros MP. Involvement of the kappa-opioid receptor in the anxiogenic-like effect of CP 55,940 in male rats. Pharmacol Biochem Behav. 2003;74(3):649–56.
Arnold JC, Dielenberg RA, McGregor IS. Cannabinoids increase conditioned ultrasonic vocalisations and cat odour avoidance in rats: strain differences in drug-induced anxiety. Life Sci. 2010;87(17–18):572–78.
Bambico FR, Nguyen NT, Katz N, Gobbi G. Chronic exposure to cannabinoids during adolescence but not during adulthood impairs emotional behaviour and monoaminergic neurotransmission. Neurobiol Dis. 2010;37(3):641–55.
Morrison PD, Zois V, McKeown DA, Lee TD, Holt DW, Powell JF, Kapur S, Murray RM. The acute effects of synthetic intravenous Delta9-tetrahydrocannabinol on psychosis, mood and cognitive functioning. Psychol Med. 2009;39(10):1607–16.
Martin-Santos R, Crippa JA, Batalla A, Bhattacharyya S, Atakan Z, Borgwardt S, Allen P, Seal M, Langohr K, Farre M, Zuardi AW, McGuire PK. Acute effects of a single, oral dose of d9-tetrahydrocannabinol (THC) and cannabidiol (CBD) administration in healthy volunteers. Curr Pharm Des. 2012;18(32):4966–79.
Karschner EL, Darwin WD, McMahon RP, Liu F, Wright S, Goodwin RS, Huestis MA. Subjective and physiological effects after controlled Sativex and oral THC administration. Clin Pharmacol Ther. 2011;89(3):400–7.
D'Souza DC, Perry E, MacDougall L, Ammerman Y, Cooper T, Wu YT, Braley G, Gueorguieva R, Krystal JH. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology. 2004;29(8):1558–72.
Zuardi AW, Shirakawa I, Finkelfarb E, Karniol IG. Action of cannabidiol on the anxiety and other effects produced by delta9-THC in normal subjects. Psychopharmacology (Berl). 1982;76(3):245–50.
Fusar-Poli P, Crippa JA, Bhattacharyya S, Borgwardt SJ, Allen P, Martin-Santos R, Seal M, Surguladze SA, O'Carrol C, Atakan Z, Zuardi AW, McGuire PK. Distinct effects of {delta}9-tetrahydrocannabinol and cannabidiol on neural activation during emotional processing. Arch Gen Psychiatry. 2009;66(1):95–105.
Bhattacharyya S, Fusar-Poli P, Borgwardt S, Martin-Santos R, Nosarti C, O’Carroll C, Allen P, Seal ML, Fletcher PC, Crippa JA, Giampietro V, Mechelli A, Atakan Z, McGuire P. Modulation of mediotemporal and ventrostriatal function in humans by Delta9-tetrahydrocannabinol: a neural basis for the effects of Cannabis sativa on learning and psychosis. Arch Gen Psychiatry. 2009;66(4):442–51.
Newsom RJ, Kelly SJ. Perinatal delta-9-tetrahydrocannabinol exposure disrupts social and open field behavior in adult male rats. Neurotoxicol Teratol. 2008;30(3):213–219.
Schneider M, Drews E, Koch M. Behavioral effects in adult rats of chronic prepubertal treatment with the cannabinoid receptor agonist WIN 55,212–2. Behav Pharmacol. 2005;16(5–6):447–54.
Malone DT, Jongejan D, Taylor DA. Cannabidiol reverses the reduction in social interaction produced by low dose Delta(9)-tetrahydrocannabinol in rats. Pharmacol Biochem Behav. 2009;93(2):91–6.
Franklin JM, Mathew M, Carrasco GA. Cannabinoid-induced upregulation of serotonin 2A receptors in the hypothalamic paraventricular nucleus and anxiety-like behaviors in rats. Neurosci Lett. 2013;548:165–69.
Biscaia M, Marin S, Fernandez B, Marco EM, Rubio M, Guaza C, Ambrosio E, Viveros MP. Chronic treatment with CP 55,940 during the peri-adolescent period differentially affects the behavioural responses of male and female rats in adulthood. Psychopharmacology (Berl). 2003;170(3):301–08.
Macri S, Lanuzza L, Merola G, Ceci C, Gentili S, Valli A, Macchia T, Laviola G. Behavioral responses to acute and sub-chronic administration of the synthetic cannabinoid JWH-018 in adult mice prenatally exposed to corticosterone. Neurotox Res. 2013;24(1):15–28.
Delatte MS, Paronis CA. Evaluation of cannabinoid agonists using punished responding and midazolam discrimination procedures in squirrel monkeys. Psychopharmacology (Berl). 2008;198(4):521–28.
Klumpers F, Denys D, Kenemans JL, Grillon C, van der Aart J, Baas JM. Testing the effects of Delta9-THC and D-cycloserine on extinction of conditioned fear in humans. J Psychopharmacol. 2012;26(4):471–78.
Pandolfo P, Pamplona FA, Prediger RD, Takahashi RN. Increased sensitivity of adolescent spontaneously hypertensive rats, an animal model of attention deficit hyperactivity disorder, to the locomotor stimulation induced by the cannabinoid receptor agonist WIN 55,212–2. Eur J Pharmacol. 2007;563(1–3):141–48.
Llorente-Berzal A, Fuentes S, Gagliano H, Lopez-Gallardo M, Armario A, Viveros MP, Nadal R. Sex-dependent effects of maternal deprivation and adolescent cannabinoid treatment on adult rat behaviour. Addiction biology. 2011;16(4):624–37.
Higuera-Matas A, Botreau F, Miguens M, Del Olmo N, Borcel E, Perez-Alvarez L, Garcia-Lecumberri C, Ambrosio E. Chronic periadolescent cannabinoid treatment enhances adult hippocampal PSA-NCAM expression in male Wistar rats but only has marginal effects on anxiety, learning and memory. Pharmacol Biochem Behav. 2009;93(4):482–90.
Gonzalez-Cuevas G, Aujla H, Martin-Fardon R, Lopez-Moreno JA, Navarro M, Weiss F. Subchronic cannabinoid agonist (WIN 55,212–2) treatment during cocaine abstinence alters subsequent cocaine seeking behavior. Neuropsychopharmacology. 2007;32(11):2260–66.
Abush H, Akirav I. Cannabinoids ameliorate impairments induced by chronic stress to synaptic plasticity and short-term memory. Neuropsychopharmacology. 2013;38(8):1521–34.
Alen F, Santos A, Moreno-Sanz G, Gonzalez-Cuevas G, Gine E, Franco-Ruiz L, Navarro M, Lopez-Moreno JA. Cannabinoid-induced increase in relapse-like drinking is prevented by the blockade of the glycine-binding site of N-methyl-D-aspartate receptors. Neuroscience. 2009;158(2):465–73.
Kathuria S, Gaetani S, Fegley D, Valino F, Duranti A, Tontini A, Mor M, Tarzia G, La Rana G, Calignano A, Giustino A, Tattoli M, Palmery M, Cuomo V, Piomelli D. Modulation of anxiety through blockade of anandamide hydrolysis. Nat Med. 2003;9(1):76–81.
Gobbi G, Bambico FR, Mangieri R, Bortolato M, Campolongo P, Solinas M, Cassano T, Morgese MG, Debonnel G, Duranti A, Tontini A, Tarzia G, Mor M, Trezza V, Goldberg SR, Cuomo V, Piomelli D. Antidepressant-like activity and modulation of brain monoaminergic transmission by blockade of anandamide hydrolysis. Proc Natl Acad Sci U S A. 2005;102(51):18620–5.
Piomelli D, Tarzia G, Duranti A, Tontini A, Mor M, Compton TR, Dasse O, Monaghan EP, Parrott JA, Putman D. Pharmacological profile of the selective FAAH inhibitor KDS-4103 (URB597). CNS Drug Rev. 2006;12(1):21–38.
Long JZ, Li W, Booker L, Burston JJ, Kinsey SG, Schlosburg JE, Pavon FJ, Serrano AM, Selley DE, Parsons LH, Lichtman AH, Cravatt BF. Selective blockade of 2-arachidonoylglycerol hydrolysis produces cannabinoid behavioral effects. Nat Chem Biol. 2009;5(1):37–44.
Hill MN, Kumar SA, Filipski SB, Iverson M, Stuhr KL, Keith JM, Cravatt BF, Hillard CJ, Chattarji S, McEwen BS. Disruption of fatty acid amide hydrolase activity prevents the effects of chronic stress on anxiety and amygdalar microstructure. Mol Psychiatr. 2013;18(10):1125–35.
Hermanson DJ, Hartley ND, Gamble-George J, Brown N, Shonesy BC, Kingsley PJ, Colbran RJ, Reese J, Marnett LJ, Patel S. Substrate-selective COX-2 inhibition decreases anxiety via endocannabinoid activation. Nat Neurosci. 2013;16(9):1291–98.
Kinsey SG, O’Neal ST, Long JZ, Cravatt BF, Lichtman AH. Inhibition of endocannabinoid catabolic enzymes elicits anxiolytic-like effects in the marble burying assay. Pharmacol Biochem Behav. 2011;98(1):21–7.
Rossi S, De Chiara V, Musella A, Sacchetti L, Cantarella C, Castelli M, Cavasinni F, Motta C, Studer V, Bernardi G, Cravatt BF, Maccarrone M, Usiello A, Centonze D. Preservation of striatal cannabinoid CB1 receptor function correlates with the antianxiety effects of fatty acid amide hydrolase inhibition. Mol Pharmacol. 2010;78(2):260–68.
Busquets-Garcia A, Puighermanal E, Pastor A, de la Torre R, Maldonado R, Ozaita A. Differential role of anandamide and 2-arachidonoylglycerol in memory and anxiety-like responses. Biol Psychiatry. 2011;70(5):479–86.
Moreira FA, Kaiser N, Monory K, Lutz B. Reduced anxiety-like behaviour induced by genetic and pharmacological inhibition of the endocannabinoid-degrading enzyme fatty acid amide hydrolase (FAAH) is mediated by CB1 receptors. Neuropharmacology. 2008;54(1):141–50.
Cippitelli A, Astarita G, Duranti A, Caprioli G, Ubaldi M, Stopponi S, Kallupi M, Sagratini G, Rodriguez de Fonseca F, Piomelli D, Ciccocioppo R. Endocannabinoid regulation of acute and protracted nicotine withdrawal: effect of FAAH inhibition. PloS ONE. 2011;6(11):e28142.
Cippitelli A, Cannella N, Braconi S, Duranti A, Tontini A, Bilbao A, Defonseca FR, Piomelli D, Ciccocioppo R. Increase of brain endocannabinoid anandamide levels by FAAH inhibition and alcohol abuse behaviours in the rat. Psychopharmacology (Berl). 2008;198(4):449–60.
Haller J, Barna I, Barsvari B, Gyimesi Pelczer K, Yasar S, Panlilio LV, Goldberg S. Interactions between environmental aversiveness and the anxiolytic effects of enhanced cannabinoid signaling by FAAH inhibition in rats. Psychopharmacology. 2009;204(4):607–16.
Naidu PS, Varvel SA, Ahn K, Cravatt BF, Martin BR, Lichtman AH. Evaluation of fatty acid amide hydrolase inhibition in murine models of emotionality. Psychopharmacology. 2007;192(1):61–70.
Zaitone SA, El-Wakeil AF, Abou-El-Ela SH. Inhibition of fatty acid amide hydrolase by URB597 attenuates the anxiolytic-like effect of acetaminophen in the mouse elevated plus-maze test. Behav Pharmacol. 2012;23(4):417–25.
Almeida-Santos AF, Gobira PH, Rosa LC, Guimaraes FS, Moreira FA, Aguiar DC. Modulation of anxiety-like behavior by the endocannabinoid 2-arachidonoylglycerol (2-AG) in the dorsolateral periaqueductal gray. Behav Brain Res. 2013;252:10–7.
Sumislawski JJ, Ramikie TS, Patel S. Reversible gating of endocannabinoid plasticity in the amygdala by chronic stress: a potential role for monoacylglycerol lipase inhibition in the prevention of stress-induced behavioral adaptation. Neuropsychopharmacology. 2011;36(13):2750–61.
Sciolino NR, Zhou W, Hohmann AG. Enhancement of endocannabinoid signaling with JZL184, an inhibitor of the 2-arachidonoylglycerol hydrolyzing enzyme monoacylglycerol lipase, produces anxiolytic effects under conditions of high environmental aversiveness in rats. Pharmacol Res. 2011;64(3):226–34.
Aliczki M, Balogh Z, Tulogdi A, Haller J. The temporal dynamics of the effects of monoacylglycerol lipase blockade on locomotion, anxiety, and body temperature. Behav Pharmacol. 2012;23(4):348–57.
Bortolato M, Campolongo P, Mangieri RA, Scattoni ML, Frau R, Trezza V, La Rana G, Russo R, Calignano A, Gessa GL, Cuomo V, Piomelli D. Anxiolytic-like properties of the anandamide transport inhibitor AM404. Neuropsychopharmacology. 2006;31(12):2652–9.
Bitencourt RM, Pamplona FA, Takahashi RN. Facilitation of contextual fear memory extinction and anti-anxiogenic effects of AM404 and cannabidiol in conditioned rats. Eur Neuropsychopharmacol. 2008;18(12):849–59.
Pamplona FA, Bitencourt RM, Takahashi RN. Short- and long-term effects of cannabinoids on the extinction of contextual fear memory in rats. Neurobiol Learn Mem. 2008;90(1):290–93.
Powers MS, Barrenha GD, Mlinac NS, Barker EL, Chester JA. Effects of the novel endocannabinoid uptake inhibitor, LY2183240, on fear-potentiated startle and alcohol-seeking behaviors in mice selectively bred for high alcohol preference. Psychopharmacology (Berl). 2010;212(4):571–83.
Scherma M, Justinova Z, Zanettini C, Panlilio LV, Mascia P, Fadda P, Fratta W, Makriyannis A, Vadivel SK, Gamaleddin I, Le Foll B, Goldberg SR. The anandamide transport inhibitor AM404 reduces the rewarding effects of nicotine and nicotine-induced dopamine elevations in the nucleus accumbens shell in rats. Br J Pharmacol. 2012;165(8):2539–48.
Terzian AL, Drago F, Wotjak CT, Micale V. The dopamine and cannabinoid interaction in the modulation of emotions and cognition: assessing the role of cannabinoid cb1 receptor in neurons expressing dopamine d1 receptors. Front Behav Neurosci. 2011;5:49.
Kupferschmidt DA, Newman AE, Boonstra R, Erb S. Antagonism of cannabinoid 1 receptors reverses the anxiety-like behavior induced by central injections of corticotropin-releasing factor and cocaine withdrawal. Neuroscience. 2012;204:125–33.
Ruehle S, Remmers F, Romo-Parra H, Massa F, Wickert M, Wortge S, Haring M, Kaiser N, Marsicano G, Pape HC, Lutz B. Cannabinoid CB1 receptor in dorsal telencephalic glutamatergic neurons: distinctive sufficiency for hippocampus-dependent and amygdala-dependent synaptic and behavioral functions. J Neurosci. 2013;33(25):10264–277.
Rubino T, Guidali C, Vigano D, Realini N, Valenti M, Massi P, Parolaro D. CB1 receptor stimulation in specific brain areas differently modulate anxiety-related behaviour. Neuropharmacology. 2008;54(1):151–60.
Rubino T, Realini N, Castiglioni C, Guidali C, Vigano D, Marras E, Petrosino S, Perletti G, Maccarrone M, Di Marzo V, Parolaro D. Role in anxiety behavior of the endocannabinoid system in the prefrontal cortex. Cereb Cortex. 2008;18(6):1292–301.
Klugmann M, Goepfrich A, Friemel CM, Schneider M. AAV-Mediated Overexpression of the CB1 Receptor in the mPFC of Adult Rats Alters Cognitive Flexibility, Social Behavior, and Emotional Reactivity. Front Behav Neurosci. 2011;5:37.
Zarrindast MR, Mahboobi S, Sadat-Shirazi MS, Ahmadi S. Anxiolytic-like effect induced by the cannabinoid CB1 receptor agonist, arachydonilcyclopropylamide (ACPA), in the rat amygdala is mediated through the D1 and D2 dopaminergic systems. J Psychopharmacol. 2011;25(1):131–40.
Ganon-Elazar E, Akirav I. Cannabinoid receptor activation in the basolateral amygdala blocks the effects of stress on the conditioning and extinction of inhibitory avoidance. J Neurosci. 2009;29(36):11078–88.
John CS, Currie PJ. N-arachidonoyl-serotonin in the basolateral amygdala increases anxiolytic behavior in the elevated plus maze. Behav Brain Res. 2012;233(2):382–88.
Munguba H, Cabral A, Leao AH, Barbosa FF, Izidio GS, Ribeiro AM, Silva RH. Pre-training anandamide infusion within the basolateral amygdala impairs plus-maze discriminative avoidance task in rats. Neurobiol Learn Mem. 2011;95(4):527–33.
Mendez-Diaz M, Caynas-Rojas S, Arteaga Santacruz V, Ruiz-Contreras AE, Aguilar-Roblero R, Prospero-Garcia O. Entopeduncular nucleus endocannabinoid system modulates sleep-waking cycle and mood in rats. Pharmacol Biochem Behav. 2013;107:29–35.
Kamprath K, Romo-Parra H, Haring M, Gaburro S, Doengi M, Lutz B, Pape HC. Short-term adaptation of conditioned fear responses through endocannabinoid signaling in the central amygdala. Neuropsychopharmacology. 2011;36(3):652–63.
Dubreucq S, Kambire S, Conforzi M, Metna-Laurent M, Cannich A, Soria-Gomez E, Richard E, Marsicano G, Chaouloff F. Cannabinoid type 1 receptors located on single-minded 1-expressing neurons control emotional behaviors. Neuroscience. 2012;204:230–44.
Roohbakhsh A, Moghaddam AH, Massoudi R, Zarrindast MR. Role of dorsal hippocampal cannabinoid receptors and nitric oxide in anxiety like behaviours in rats using the elevated plus-maze test. Clin Exp Pharmacol Physiol. 2007;34(3):223–29.
Clarke JR, Rossato JI, Monteiro S, Bevilaqua LR, Izquierdo I, Cammarota M. Posttraining activation of CB1 cannabinoid receptors in the CA1 region of the dorsal hippocampus impairs object recognition long-term memory. Neurobiol Learn Mem. 2008;90(2):374–81.
Hakimizadeh E, Oryan S, Hajizadeh Moghaddam A, Shamsizadeh A, Roohbakhsh A. Endocannabinoid System and TRPV1 Receptors in the Dorsal Hippocampus of the Rats Modulate Anxiety-like Behaviors. Iran J Basic Med Sci. 2012;15(3):795–802.
Zarrindast MR, Nasehi M, Piri M, Bina P. Anxiety-like behavior induced by histaminergic agents can be prevented by cannabinoidergic WIN55,212–2 injected into the dorsal hippocampus in mice. Pharmacol Biochem Behav. 2010;94(3):387–96.
Roohbakhsh A, Keshavarz S, Hasanein P, Rezvani ME, Moghaddam AH. Role of endocannabinoid system in the ventral hippocampus of rats in the modulation of anxiety-like behaviours. Basic Clin Pharmacol Toxicol. 2009;105(5):333–38.
Campos AC, Ferreira FR, Guimaraes FS, Lemos JI. Facilitation of endocannabinoid effects in the ventral hippocampus modulates anxiety-like behaviors depending on previous stress experience. Neuroscience. 2010;167(2):238–46.
Resstel LB, Lisboa SF, Aguiar DC, Correa FM, Guimaraes FS. Activation of CB1 cannabinoid receptors in the dorsolateral periaqueductal gray reduces the expression of contextual fear conditioning in rats. Psychopharmacology. 2008;198(3):405–11.
Casarotto PC, Terzian AL, Aguiar DC, Zangrossi H, Guimaraes FS, Wotjak CT, Moreira FA. Opposing roles for cannabinoid receptor type-1 (CB(1)) and transient receptor potential vanilloid type-1 channel (TRPV1) on the modulation of panic-like responses in rats. Neuropsychopharmacology. 2012;37(2):478–86.
Lisboa SF, Resstel LB, Aguiar DC, Guimaraes FS. Activation of cannabinoid CB1 receptors in the dorsolateral periaqueductal gray induces anxiolytic effects in rats submitted to the Vogel conflict test. Eur J Pharmacol. 2008;593(1–3):73–8.
Moreira FA, Aguiar DC, Guimaraes FS. Anxiolytic-like effect of cannabinoids injected into the rat dorsolateral periaqueductal gray. Neuropharmacology. 2007;52(3):958–65.
De Boer SF Koolhaas JM. Defensive burying in rodents: ethology, neurobiology and psychopharmacology. Eur J Pharmacol. 2003;463(1–3):145–61.
Wilson RI, Nicoll RA. Endogenous cannabinoids mediate retrograde signalling at hippocampal synapses. Nature. 2001;410(6828):588–92.
Di Marzo V De Petrocellis L Bisogno T Melck D. Metabolism of anandamide and 2-arachidonoylglycerol: an historical overview and some recent developments. Lipids. 1999;34 Suppl:S319–25.
Marsicano G, Goodenough S, Monory K, Hermann H, Eder M, Cannich A, Azad SC, Cascio MG, Gutierrez SO, van der Stelt M, Lopez-Rodriguez ML, Casanova E, Schutz G, Zieglgansberger W, Di Marzo V, Behl C, Lutz B. CB1 cannabinoid receptors and on-demand defense against excitotoxicity. Science. 2003;302(5642):84–8.
Adermark L, Lovinger DM. Retrograde endocannabinoid signaling at striatal synapses requires a regulated postsynaptic release step. Proc Natl Acad Sci U S A. 2007;104(51):20564–69.
Lutz B. On-demand activation of the endocannabinoid system in the control of neuronal excitability and epileptiform seizures. Biochem Pharmacol. 2004;68(9):1691–98.
Zanettini C, Panlilio LV, Alicki M, Goldberg SR, Haller J, Yasar S. Effects of endocannabinoid system modulation on cognitive and emotional behavior. Front Behav Neurosci. 2011;5:57.
Onaivi ES, Ishiguro H, Gong JP, Patel S, Perchuk A, Meozzi PA, Myers L, Mora Z, Tagliaferro P, Gardner E, Brusco A, Akinshola BE, Liu QR, Hope B, Iwasaki S, Arinami T, Teasenfitz L, Uhl GR. Discovery of the presence and functional expression of cannabinoid CB2 receptors in brain. Ann NY Acad Sci. 2006;1074:514–36.
Begg M, Pacher P, Batkai S, Osei-Hyiaman D, Offertaler L, Mo FM, Liu J, Kunos G. Evidence for novel cannabinoid receptors. Pharmacol Ther. 2005;106(2):133–45.
Barna I, Till I, Haller J. Blood, adipose tissue and brain levels of the cannabinoid ligands WIN-55,212 and SR-141716A after their intraperitoneal injection in mice: compound-specific and area-specific distribution within the brain. Eur Neuropsychopharmacol. 2009;19(8):533–41.
McLaughlin RJ, Hill MN, Bambico FR, Stuhr KL, Gobbi G, Hillard CJ, Gorzalka BB. Prefrontal cortical anandamide signaling coordinates coping responses to stress through a serotonergic pathway. Eur Neuropsychopharmacol. 2012;22(9):664–71.
Haller J, Aliczki M, Pelczer KG, Spitzer K, Balogh Z, Kantor S. Effects of the fatty acid amide hydrolase inhibitor URB597 on coping behavior under challenging conditions in mice. Psychopharmacology (Berl). 2014;231(3):593–601.
Haller J, Goldberg SR, Pelczer KG, Aliczki M, Panlilio LV. The effects of anandamide signaling enhanced by the FAAH inhibitor URB597 on coping styles in rats. Psychopharmacology (Berl). 2013;230(3):353–62.
Koolhaas JM, Korte SM, De Boer SF, Van Der Vegt BJ, Van Reenen CG, Hopster H, De Jong IC, Ruis MA, Blokhuis HJ. Coping styles in animals: current status in behavior and stress-physiology. Neurosci Biobehav Rev. 1999;23(7):925–35.
Koolhaas JM. Coping style and immunity in animals: making sense of individual variation. Brain Behav Immun. 2008;22(5):662–67.
Kessler RC, Price RH, Wortman CB. Social factors in psychopathology: stress, social support, and coping processes. Annu Rev Psychol. 1985;36:531–72.
Temoshok LR. Complex coping patterns and their role in adaptation and neuroimmunomodulation. Theory, methodology, and research. Ann NY Acad Sci. 2000;917:446–55.
Westerhuis W, Zijlmans M, Fischer K, van Andel J, Leijten FS. Coping style and quality of life in patients with epilepsy: a cross-sectional study. J Neurol. 2011;258(1):37–43.
Pucheu S, Consoli SM, D'Auzac C, Francais P, Issad B. Do health causal attributions and coping strategies act as moderators of quality of life in peritoneal dialysis patients? J Psychosom Res. 2004;56(3):317–22.
Cooke M, Peters E, Fannon D, Anilkumar AP, Aasen I, Kuipers E, Kumari V. Insight, distress and coping styles in schizophrenia. Schizophr Res. 2007;94(1–3):12–22.
Tiemensma J, Kaptein AA, Pereira AM, Smit JW, Romijn JA, Biermasz NR. Coping strategies in patients after treatment for functioning or nonfunctioning pituitary adenomas. J Clin Endocrinol Metab. 2011;96(4):964–71.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Aliczki, M., Haller, J. (2015). Interactions Between Cannabinoid Signaling and Anxiety: A Comparative Analysis of Intervention Tools and Behavioral Effects. In: Campolongo, P., Fattore, L. (eds) Cannabinoid Modulation of Emotion, Memory, and Motivation. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2294-9_4
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2294-9_4
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2293-2
Online ISBN: 978-1-4939-2294-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)