
Abstract
Mitochondrial respiratory chain disorders are a heterogeneous group of diseases that clinically involve multiple tissues although they tend to mainly affect nervous system and skeletal muscle. The predominance of neurologic and neuromuscular manifestations in mitochondrial diseases has generally masked the presence of other, but not less important, clinical phenotypes, such as cardiac complications. Nowadays, mitochondrial defects are being increasingly recognized to play an important role in the pathogenesis of a subgroup of cardiomyopathies produced by defects in the energetic metabolism (mitochondrial cardiomyopathies). These diseases can result from mutations in either nuclear or mitochondrial encoded genes although mitochondrial DNA mutations are more frequent. In fact, cardiac conduction abnormalities have been associated with different mtDNA rearrangements. In a same way, sporadic or inherited mutations in mitochondrial DNA specifically in the mitochondrial transfer ribonucleic acid genes (mostly in the tRNALeu(UUR) and tRNAIle) have also been associated with hypertrophic and dilated cardiomyopathy. Mitochondrial diseases caused by mutations in the mitochondrial tRNAVal gene (MT-TV) are not very frequent. However, a relatively high percentage of mutations in this gene have been associated with mitochondrial cardiomyopathy. Besides, functional and molecular analyses suggest that the MT-TV gene should be routinely considered in the diagnosis when there is a high suspicion of mitochondrial cardiomyopathy. Finally, the increasingly importance of the role that this gene has begun to play in the pathophysiology of mitochondrial cardiomyopathies indicates that future studies about the molecular mechanisms that could explain why the cardiomyopathy phenotype appears must be carried out.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Abbreviations
- ARVC:
-
Arrhythmogenic right ventricular cardiomyopathy
- CM:
-
Cardiomyopathy
- CPEO:
-
Chronic progressive external ophthalmoplegia
- DCM:
-
Dilated cardiomyopathy
- HCM:
-
Hypertrophic cardiomyopathy
- MCM:
-
Mitochondrial cardiomyopathy
- MD:
-
Mitochondrial disease
- MELAS:
-
Mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes
- MiMyCa:
-
Maternally transmitted mitochondrial cardiomyopathy and myopathy
- MNGIE:
-
Mitochondrial neurogastrointestinal encephalopathy
- MT-TI:
-
Mitochondrial tRNA isoleucine gene
- MT-TK:
-
Mitochondrial tRNA lysine gene
- MT-TV:
-
Mitochondrial tRNA valine gene
- mtDNA:
-
Mitochondrial DNA
- OXPHOS:
-
Oxidative phosphorylation
- RC:
-
Respiratory chain
- RCM:
-
Restrictive cardiomyopathy
- tRNA:
-
Transfer ribonucleic acid
Key Points
-
Cardiomyopathies are diseases of the myocardium that can be complicated by heart failure, arrhythmias, and sudden death.
-
Mitochondrial cardiomyopathies are a subgroup of cardiomyopathies produced by defects in the energetic metabolism.
-
Cardiac involvement is reported in 20–25 % of patients with mitochondrial disorders.
-
Mitochondrial cardiomyopathies can result from mutations in either nuclear or mitochondrial encoded genes.
-
Mitochondrial tRNALeu, tRNAIle, and tRNAVal are mutational hotspots for mitochondrial cardiomyopathies.
-
Most patients with mutations in the mitochondrial tRNAVal gene (MT-TV) present with a hypertrophic cardiomyopathy.
-
The MT-TV gene should be included in the molecular diagnosis of patients when there is a high suspicion of mitochondrial cardiomyopathy.
Introduction
Cardiomyopathies (CM) are an important and heterogeneous group of diseases. They are defined as diseases of the myocardium with cardiac dysfunction that can be complicated by heart failure, arrhythmias, and sudden death [1]. They are classified into four main different entities: hypertrophic, dilated, restrictive, and arrhythmogenic right ventricular CM/ dysplasia (Fig. 7.1). Hypertrophic cardiomyopathy (HCM) is a clinically heterogeneous but quite common autosomal dominant genetic heart disease that probably is the most frequently occurring CM (estimated prevalence of about 1 of 500 [2–4]). HCM is defined by an unexplained left ventricular hypertrophy usually asymmetrical and that involves the interventricular septum. The clinical pattern is very heterogeneous. In fact, there are a lot of patients without symptoms during their whole life. In some cases HCM may lead to syncope or dysnea, sudden death, or congestive heart failure [1]. Dilated cardiomyopathy (DCM) is the most prevalent cause of congestive heart failure in young patients and besides an important cause of cardiac transplantation. It has an estimated prevalence of 36 of 100,000 in the US [5]. Dilated forms of CM are characterized by ventricular chamber enlargement and systolic dysfunction, thin wall thickness, and depressed left ventricular systolic function [6]. Restrictive cardiomyopathy (RCM) is a rare form of heart muscle disease and a cause of heart failure that is characterized by a pattern of ventricular filling in which increased stiffness of the myocardium causes ventricular pressure to rise with only small increases of volume [7]. Unlike HCM, DCM, and RCM, arrhythmogenic right ventricular cardiomyopathy (ARVC) is an uncommon form of inheritable heart muscle disease (estimated in 1:5,000) [4]. ARVC is defined histologically by the existence of progressive replacement of right ventricular myocardium with adipose and fibrous tissue often confined to a triangle of dysplasia comprising the right ventricular inflow, outflow, and apex [7].

Types of cardiomyopathies. The figure shows schematically different types of cardiomyopathies. HCM Hypertrophic cardiomyopathy, DCM Dilated cardiomyopathy, RCM Restrictive cardiomyopathy, LV Left ventricle (unpublished)
Until now, more than 40 inborn errors in metabolism are reported to cause myocardial abnormalities. They can present with cardiac disease at any moment during life but frequently symptoms and signs of multiorgan system dysfunction appear in infancy or early childhood. Most genetic metabolic CM are inherited as autosomal recessive traits but some of them are X-linked. Another important group of diseases, called mitochondrial cardiomyopathies (MCM), a subgroup of CM produced by defects in the energetic metabolism, can result from mutations in either nuclear or mitochondrial encoded genes, showing the complexity of the inheritance patterns (e.g., maternal, autosomal recessive) [8]. This chapter will focus on MCM caused by mutations in the mitochondrial DNA (mtDNA) with an emphasis on the mitochondrial tRNA mutations and most specifically on mutations identified in the mitochondrial tRNA Valine gene (MT-TV).
Mitochondrial Genetics and Cardiac Disease
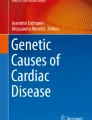
Disorders of energy production are quite common among inborn errors of metabolism. Mitochondrial disorders (MD) are multisystemic diseases that may arise at any age, as a result of dysfunction of the respiratory chain (RC). Clinically, they usually involve multiple tissues although the most frequently and severely affected organs are those that place high demands on aerobic metabolism, such as brain, skeletal muscle, sensory organs, kidney, and cardiac muscle. Myocardium is one of the most energy-demanding tissues in the body because of continuous contractility needed for pumping the blood to the tissues. This energy is mostly supplied by the mitochondrion, the cellular organelle implicated in the generation of energy through the oxidative phosphorylation (OXPHOS). For that reason, it is not surprising that mitochondrial diseases can result in either HCM or DCM. CM usually does not appear as an isolated feature and it is usually a part of a multisystem involvement. As it has been mentioned above MCM can result from inherited or sporadic mutations in mitochondrial (mtDNA) or nuclear DNA. Recent studies have reported a minimum birth prevalence of approximately 1 of 8,000 for mitochondrial disorders caused by mutations in nuclear or mitochondrial genes although mtDNA mutations are more frequent [9, 10]. The human mtDNA is a 16,569 bp double-stranded circular molecule that encodes for 37 genes, 24 of which are involved in the translation mechanism (2 rRNAs and 22 tRNAs) (Fig. 7.2). The 13 remaining genes are responsible for the synthesis of respiratory chain subunits. Functional tRNAs are needed for the translation of these 13 proteins as it is shown by the fact that mutations in mitochondrial tRNA genes are normally associated with combined defects in the respiratory chain complexes [11–14]. However, there are also patients with a mutation in a mitochondrial tRNA gene that causes an isolated deficiency of a complex of the RC [14, 15]. Among the 900 genes that participate in the correct functioning of mitochondria only a few are located in the mtDNA, whereas the rest are encoded in the nucleus. That is the reason why about 50 % of adults and 80–90 % of children suspected to have a mitochondrial disease on the basis of biochemical and/or morphological data remain genetically undiagnosed [16].

Map of the human mitochondrial DNA. The human mtDNA is a circular double-stranded molecule with 16,559 base pairs of length. It encodes for 13 subunits of the oxidative phosphorylation system: The mitochondrially encoded NADH dehydrogenase subunits 1, 2, 3, 4, 4 L, 5, 6 (MT-ND1, MT-ND2, MT-ND3, MT-ND4, MT-ND4L, MT-ND5, MT-ND6), the mitochondrially encoded cytochrome c oxidase I, II, and III, (MT-CO1, MT-CO2, MT-CO3), the mitochondrially encoded cytochrome b (MT-CYB), the mitochondrially encoded ATP synthase 6 and 8 (MT-ATP6, MT-ATP8), 2 rRNAs: rRNA12S, and rRNA16S (MT-RNR1, MT-RNR2), and 22 tRNAs. The tRNAVal gene (MT-TV) located between the rRNA12S and rRNA16S is shown (unpublished)
MtDNA mutations obey to different genetic rules than those applied to Mendelian diseases. First of all, mtDNA is maternally inherited. Second, there are multiple copies of mtDNA in each cell. Homoplasmy is the situation in which all mtDNA copies are identical and on the contrary heteroplasmy is described when two or more sequence variants exist in a cell or individual. In fact, when the ratio of mutant to normal mtDNA exceeds a critical threshold, then the respiratory chain function will be impaired and the disease appears. The threshold at which symptoms manifest depends on the tissue involved. Although the presence of heteroplasmy has been a common pathogenic criterion for mitochondrial mutations [13], homoplasmic mutations are being increasingly recognized as causes of MD [13, 17]. Another aspect of the mitochondrial genetics is the mitotic segregation of the multiple copies of mtDNA that explains why the level of mutant mtDNA can change during life.
According to the limited number of reported clinical studies, cardiac involvement is published in 20–25 % of patients with mitochondrial disorders [18–20]. Cardiac manifestations include CM that variably affects the clinical outcome of patients. The course may be stable for many years but rapid deterioration may occur [8]. In spite of the improvement of our knowledge of the molecular mechanisms of these diseases the molecular diagnosis is beginning to have serious implications in the routine management of this type of patients.
tRNA Mutational Spectrum Associated with CM
Mitochondrial diseases (MDs) are a clinically heterogeneous group of disorders caused by dysfunctional mitochondria, the organelles that generate energy for the cell. These diseases can present at any age, and their clinical symptoms reflect a primary defect in tissues with high oxidative demand. Usually, changes in blood parameters such as lactate, pyruvate, carnitine, amino acids, and urine organic acids are described in these disorders as well as deficiencies in enzymes of the RC. Although these diseases can result from mutations in the nuclear genome most of them are caused by mutations in the mtDNA. In spite of the fact that only 10 % of the mtDNA molecule is composed by tRNA genes most of the reported mtDNA mutations associated with MD relies on these genes suggesting that these genes are prone to mutation [17]. This conclusion is also supported by a recent study, in which it is confirmed that mitochondrial tRNA genes are mutational hotspots with a frequency of deleterious mutations (excluding one of the most frequent mutations, the m.3243 A > G) that was almost six times more than that occurring in the protein-coding regions [21]. Until now mutations in all mitochondrial tRNAs have been described associated with several MD (see MITOMAP database: http://www.mitomap.org/). However, the mitochondrial tRNA Leu (MT-TL1), tRNA Lys (MT-TK), and tRNA Ile (MT-TI ) appear to be more susceptible to mutation [22]. In fact, there have been described 35 mutations associated with MD in the MT-TL1, 22 in the MT-TK, and 20 in the MT-TI. By contrast, only three mutations in the mitochondrial tRNA Asp (MT-TD) and two in the mitochondrial tRNA Tyr (MT-TY) have been found.
The predominance of neurologic and neuromuscular manifestations in MD has generally masked the presence of other, but not less important, clinical phenotypes, such as cardiac complications. This may be one of the fact that has prevented the diagnosis of mitochondrial cardiomyopathies (MCMs) [14]. Nowadays, mitochondrial defects are being increasingly recognized to play an important role in the pathogenesis of hereditary cardiomyopathies [8]. Indeed, sporadic or inherited mutations in mitochondrial DNA (mtDNA), specifically in the mtDNA transfer ribonucleic acid (tRNA) genes, or in the nuclear genome, have been associated with hypertrophic and dilated cardiomyopathy [23, 24]. In the same way cardiac conduction abnormalities have also been associated with different mtDNA rearrangements [25].
Based on the prevalence data of mtDNA diseases and the frequency of cardiac involvement, at least 1 in 10–15,000 of the general population will be affected. In 1991, the first mitochondrial DNA (mtDNA) point mutation in the MT-TL1 gene (m.3260A > G) associated with a maternally transmitted MCM and myopathy was identified and the acronym MiMyCa was described [26]. Since then, several mutations in the mtDNA, mostly in mitochondrial tRNA genes have been associated with different MCM phenotypes (HCM and DCM) [25]. These diseases are preferentially linked to mutations in the MT-TL1, and MT-TI genes [8, 27, 28]. The MT-TL1 gene provides instructions for making a specific form of tRNA, present only in mitochondria, called tRNALeu(UUR) and the mitochondrially encoded tRNA isoleucine also known as MT-TI is a tRNA which in humans is encoded by the mitochondrial MT-TI gene. During protein assembly, these molecules attach to the amino acids Leucine and Isoleucine (both branched chain amino acids) and insert it into the appropriate locations in the protein. In Table 7.1 are shown the mutations in the MT-TI and MT-TL1 genes that have been associated with CM. A remarkable fact is that if we consider all the mitochondrial tRNAs the ones with more mutations associated to CM are the mitochondrial tRNALeu, tRNAIle, tRNALys, and tRNAVal (the latter described in more detail in the next section).
Cardiomyopathies Due to Mitochondrial tRNA Val Mutations
The mitochondrially encoded tRNA Valine is a transfer RNA encoded by the mitochondrial MT-TV gene. MT-TV is a 69 nucleotide RNA (located in position 1602–1670 bp of the mtDNA molecule). The tRNAVal attaches to a particular branched chain amino acid, Valine, and inserts it into the suitable locations in many different proteins. The tRNAVal molecule is involved in the assembly of proteins that carry out OXPHOS.
Mitochondrial diseases caused by mutations in the MT-TV gene are not very frequent. In 1996, the first mutation in this gene (m.1642G > A) was described in a patient with a MELAS phenotype (mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes) [29]. Since then, a total of eleven mutations in the MT-TV gene associated with a wide range of phenotypes, including MELAS, Leigh syndrome, CPEO (Chronic progressive external ophthalmoplegia), MNGIE (mitochondrial neurogastrointestinal encephalopathy), or HCM have been identified (Table 7.2).
Five of these mutations (m.1606G > A, m.1607 T > C, m.1630A > G, m.1642G > A, m.1644G > T) were heteroplasmic in all patients studied and three were homoplasmic (m.1624C > T, m.1628C > T, m.1643A > G) (Table 7.2). The m.1659 T > C can also be considered homoplasmic, because in all tissues analysed (blood, muscle, buccal epithelia, and urinary epithelia) the heteroplasmy level was higher than 98 % [22]. The transition (m.1644G > A) was shown both in heteroplasmy (85 %) [30] and homoplasmy [14]. Interestingly, the patient with the m.1644G > A mutation in homoplasmy has a more severe clinical phenotype, including cardiac involvement which was absent in the patient with the mutation in heteroplasmy (Table 7.2). Finally, the heteroplasmy levels of the m.1658 T > C sequence change were not determined in the study, although the electropherogram shows heteroplasmy levels near to 100 % [31].
Only five mutations from the eleven published in the MT-TV gene have already been associated with cardiac conduction abnormalities and HCM within a neurological presentation (m.1624C > T, m.1628C > T; m.1644G > A; m.1644G > T and m.1659 T > C) ([11, 14, 22] (Table 7.2; Fig. 7.3). These data suggest that although the MT-TV gene is not a region prone to mutation compared with other mitochondrial tRNAs, such as MT-TL, MT-TI, and MT-TK, a relatively high percentage of mutations in this gene (45 %: 5/11) are associated with MCM. In consequence, the MT-TV gene should also be included in the molecular diagnosis of patients when there is a high suspicion of MCM [14]. Interestingly, all patients with MT-TV mutations associated with MCM presented with a hypertrophic subtype (Table 7.2).

Schematic representation of the mitochondrial tRNAVal structure. A total of 11 mutations in the MT-TV gene associated with a wide range of phenotypes, including MELAS, Leigh syndrome, CPEO, MNGIE, or HCM have been represented. Mutations specifically associated with CM are highlighted with an asterisk. HCM Hypertrophic cardiomyopathy, MELAS Mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes, CPEO Chronic progressive external ophthalmoplegia, MNGIE Mitochondrial neurogastrointestinal encephalopathy disease (unpublished)
Although the nucleotide changes described in the MT-TV gene associated with HCM were thought to be pathogenic following several molecular criteria only two (m.1624C > T; m.1644G > A) were probed to be pathogenic in functional assays (Table 7.2). The pathogenicity of the m.1624C > T nucleotide change was confirmed by means of transmitochondrial cybrids [32, 33], and a selective reduction of the steady-state mt-tRNAVal level in muscle from the patient harbouring the m.1644G > A transition, supports both the cardiac and the neurological involvement of this mutation [14]. Due to the lack of sample it could not be confirmed whether this mutation may lead to a conformational change or impaired aminoacylation capacity of the mt-tRNAVal [14].
A particular feature of mutations in mitochondrial tRNAs and in mtDNA in general is that a clear correlation between genotype-phenotype does not exit. That means that the same mutations are associated to different clinical phenotypes (clinical heterogeneity) and the same disease is associated with different mutations (genetic heterogeneity). As examples of the clinical heterogeneity, the homoplasmic mutation m.1624C > T in the MT-TV gene can generate from mild to severe phenotypes between the family members [13] or even mutations at the same nucleotide of the MT-TV gene (m.1644G > A and m.1644G > T) result in different phenotypes (Hypertrophic cardiomyopathy plus MELAS or Leigh Syndrome respectively) [11, 30, 34].
There are several explanations for the absence of genotype-phenotype correlation. Among them are the nuclear background, the heteroplasmy levels and its tissue distribution, the mtDNA haplotype, or the total mtDNA copy number [35]. The importance of the nuclear background in the clinical phenotype is highlighted in a recent study, in which the tRNAVal steady-state level in transmitochondrial cybrids carrying the m.1624C > T mutation in homoplasmy (10 % referred to controls) differs significantly of the level observed in muscle biopsy with the same mutation in homoplasmy (<1 % referred to controls) [32]. To date, the most pronounced decrease of the steaty-state mitochondrial tRNAVal in cardiac and in skeletal muscles has been observed in the presence of this mutation associated with infantile and fatal Leigh syndrome together with severe cardiac failure in one of ten children affected [13]. Regarding the quantity of mutant mtDNA, although there are examples of maternally inherited mutations in which the severity of the disease correlates with the number of mutated copies [11], there are also examples in which the level of heteroplasmy do not correlate with the presence or severity of the disease. As an example the mutation m.1630A > G (not associated with a cardiac dysfunction; Table 7.2) has been reported to be in higher levels in a healthy mother (93 % in blood and 98 % in urine) than in her affected daughter (75 % in blood, 95 % in urine, and 60 % in fibroblast) [33].
Pathogenic mutations in mitochondrial tRNAs can alter the secondary structure or change one highly conserved base to another base, abolish the tertiary structure, and lead to dysfunction. Mutations in them affect biogenesis and function of mitochondrial tRNAs by several mechanisms, including transcription, maturation, posttranscriptional modification, structure, stability, aminoacylation, capability of binding to elongation factor thermo-unstable (EF-Tu), and Codon Reading [33, 36].
The pathogenic effect mediated by a structural change is in accordance with the work performed by [37]. In this study they demonstrated that mutations in different mitochondrial tRNAs but at the same position of the cloverleaf originate the same clinical phenotype. For example, mutations located at position 5 of the cloverleaf (m.1606G > A and m.7512 T > C in the MT-TV and MT-TS genes respectively) produce neurological symptoms, myopathy, and hearing loss, and mutations at the position 72 (m.3303C > T and m.8363G > A of the MT-TL1 and MT-TK respectively) are associated with CM. On the contrary, mutations at the same position of the same gene have been reported to be associated with different phenotypes. For example, m.1644G > A and m.1644G > T mutations in the tRNAVal cause different clinical phenotypes, MELAS, or HCM with neurogastrointestinal manifestations in the first case [14, 30] and adult Leigh syndrome in the second case [11, 34].
Regarding the MT-TV gene, its location between the 12S and the 16S ribosomal RNAs could explain by an indirect way how mutations in this gene could originate a pathogenic phenotype. Both rRNAs and the tRNAVal are transcribed as a polycistronic messenger with the posterior cleavage by the RNAse P-like endonuclease [38]. For that reason, it has been hypothesised that mutations in the tRNAVal could interrupt the normal cleavage of the polycistronic messenger and, this could be the reason of the disease. However, in a study performed by [39] with the m.1642G > A mutation, no abnormality in the splicing data was observed. This data suggest that this mechanism by itself cannot explain the observed phenotype.
Due to the fact that the MT-TV gene is being increasingly recognized as cause of MCM, an important effort in improving the knowledge about the molecular mechanisms that could explain the reason why the disease appears must be carried out.
Conclusions
Mitochondrial dysfunction frequently affects the heart and can produce both hypertrophic and dilated CM. CM are among the most severe presentations of OXPHOS with a relatively high morbidity and mortality. Due to the fact that genetics and biochemical aspects of the mitochondrion and mitochondrial disorders are beginning to be better understood, the pathophysiologic features of the mitochondrial heart disease are also becoming to be understood.
In spite of the improvement of our comprehension of the molecular mechanisms of these diseases the molecular diagnosis is beginning to have serious repercussions in the routine management of these patients. Indeed, an appropriate diagnosis of a mitochondrial cardiomyopathy could have not only important clinical implications but also could open new possibilities towards the development of potential future therapeutic strategies for these diseases which at this moment only have palliative therapeutic approaches.
The discovery that the MT-TV gene is another mutational hotspot for MCM will allow physicians to offer better genetic counselling. However more exhaustive sequencing strategies that involve the use of next generation sequencing will be needed to identify new molecular genetic causes in patients with MCM.
References
Charron P. Clinical genetics in cardiology. Heart. 2006;92:1172–6.
Maron BJ, Gardin JM, Flack JM, et al. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the cardia study. Coronary artery risk development in (young) adults. Circulation. 1995;92:785–9.
Maron BJ, Spirito P, Roman MJ, et al. Prevalence of hypertrophic cardiomyopathy in a population-based sample of American Indians aged 51 to 77 years (the strong heart study). Am J Cardiol. 2004;93:1510–4.
Maron MS, Olivotto I, Zenovich AG, et al. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114:2232–9.
Sugrue DD, Rodeheffer RJ, Codd MB, et al. The clinical course of idiopathic dilated cardiomyopathy. A population-based study. Ann Intern Med. 1992;117:117–23.
Hughes SE, McKenna WJ. New insights into the pathology of inherited cardiomyopathy. Heart. 2005;91:257–64.
Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies: a position statement from the european society of cardiology working group on myocardial and pericardial diseases. Eur Heart J. 2008;29:270–6.
Lev D, Nissenkorn A, Leshinsky-Silver E, et al. Clinical presentations of mitochondrial cardiomyopathies. Pediatr Cardiol. 2004;25:443–50.
Chinnery PF, Elliott HR, Hudson G, et al. Epigenetics, epidemiology and mitochondrial DNA diseases. Int J Epidemiol. 2012;41:177–87.
Schaefer AM, McFarland R, Blakely EL, et al. Prevalence of mitochondrial DNA disease in adults. Ann Neurol. 2008;63:35–9.
Chalmers RM, Lamont PJ, Nelson I, et al. A mitochondrial DNA tRNA(val) point mutation associated with adult-onset leigh syndrome. Neurology. 1997;49:589–92.
Horvath R, Bender A, Abicht A, et al. Heteroplasmic mutation in the anticodon-stem of mitochondrial tRNA(val) causing MNGIE-like gastrointestinal dysmotility and cachexia. J Neurol. 2009;256:810–5.
McFarland R, Elson JL, Taylor RW, et al. Assigning pathogenicity to mitochondrial tRNA mutations: when “definitely maybe” is not good enough. Trends Genet. 2004;20:591–6.
Arredondo JJ, Gallardo ME, Garcia-Pavia P, et al. Mitochondrial tRNA valine as a recurrent target for mutations involved in mitochondrial cardiomyopathies. Mitochondrion. 2012;12:357–62.
Da Pozzo P, Cardaioli E, Malfatti E, et al. A novel mutation in the mitochondrial tRNA(pro) gene associated with late-onset ataxia, retinitis pigmentosa, deafness, leukoencephalopathy and complex i deficiency. Eur J Hum Genet. 2009;17:1092–6.
Berardo A, Musumeci O, Toscano A. Cardiological manifestations of mitochondrial respiratory chain disorders. Acta Myol. 2011;30:9–15.
DiMauro S, Schon EA. Mitochondrial DNA mutations in human disease. Am J Med Genet. 2001;106:18–26.
Holmgren D, Wahlander H, Eriksson BO, et al. Cardiomyopathy in children with mitochondrial disease; clinical course and cardiological findings. Eur Heart J. 2003;24:280–8.
Scaglia F, Towbin JA, Craigen WJ, et al. Clinical spectrum, morbidity, and mortality in 113 pediatric patients with mitochondrial disease. Pediatrics. 2004;114:925–31.
Limongelli G, Tome-Esteban M, Dejthevaporn C, et al. Prevalence and natural history of heart disease in adults with primary mitochondrial respiratory chain disease. Eur J Heart Fail. 2010;12:114–21.
Tang S, Wang J, Zhang VW, et al. Transition to next generation analysis of the whole mitochondrial genome: a summary of molecular defects. Hum Mutat. 2013;34:882–93.
Blakely EL, Poulton J, Pike M, et al. Childhood neurological presentation of a novel mitochondrial tRNA(val) gene mutation. J Neurol Sci. 2004;225:99–103.
Hirano M, Davidson M, DiMauro S. Mitochondria and the heart. Curr Opin Cardiol. 2001;16:201–10.
Papadopoulou LC, Sue CM, Davidson MM, et al. Fatal infantile cardioencephalomyopathy with COX deficiency and mutations in SCO2, a COX assembly gene. Nat Genet. 1999;23:333–7.
Marin-Garcia J, Ananthakrishnan R, Goldenthal MJ, et al. Biochemical and molecular basis for mitochondrial cardiomyopathy in neonates and children. J Inherit Metab Dis. 2000;23:625–33.
Zeviani M, Gellera C, Antozzi C, et al. Maternally inherited myopathy and cardiomyopathy: association with mutation in mitochondrial DNA tRNA(Leu)(UUR). Lancet. 1991;338:143–7.
Marin-Garcia J, Goldenthal MJ, Ananthakrishnan R, et al. The complete sequence of mtDNA genes in idiopathic dilated cardiomyopathy shows novel missense and tRNA mutations. J Card Fail. 2000;6:321–9.
Wahbi K, Larue S, Jardel C, et al. Cardiac involvement is frequent in patients with the m.8344A > G mutation of mitochondrial DNA. Neurology. 2010;74:674–7.
Taylor RW, Chinnery PF, Haldane F, et al. Melas associated with a mutation in the valine transfer RNA gene of mitochondrial DNA. Ann Neurol. 1996;40:459–62.
Tanji K, Kaufmann P, Naini AB, et al. A novel tRNA(val) mitochondrial DNA mutation causing MELAS. J Neurol Sci. 2008;270:23–7.
Yan N, Cai S, Guo B, et al. A novel mitochondrial tRNA(val) t1658c mutation identified in a CPEO family. Mol Vis. 2010;16:1736–42.
Rorbach J, Yusoff AA, Tuppen H, et al. Overexpression of human mitochondrial valyl tRNA synthetase can partially restore levels of cognate mt-tRNAVal carrying the pathogenic C25U mutation. Nucleic Acids Res. 2008;36:3065–74.
Glatz C, D'Aco K, Smith S, et al. Mutation in the mitochondrial tRNA(val) causes mitochondrial encephalopathy, lactic acidosis and stroke-like episodes. Mitochondrion. 2011;11:615–9.
Mostafaie N, Rossmanith W, Hombauer H, et al. Mitochondrial genotype and risk for Alzheimer's disease: Cross-sectional data from the vienna-transdanube-aging “vita” study. J Neural Transm. 2004;111:1155–65.
Sacconi S, Salviati L, Gooch C, et al. Complex neurologic syndrome associated with the G1606A mutation of mitochondrial DNA. Arch Neurol. 2002;59:1013–5.
Zhang AM, Bandelt HJ, Jia X, et al. Is mitochondrial tRNA(phe) variant m.593 t > c a synergistically pathogenic mutation in chinese LHON families with m.11778 g > a? PLoS One. 2011;6:e26511.
Schon EA, Bonilla E, DiMauro S. Mitochondrial DNA mutations and pathogenesis. J Bioenerg Biomembr. 1997;29:131–49.
Doersen CJ, Guerrier-Takada C, Altman S, et al. Characterization of an RNase p activity from HeLa cell mitochondria. Comparison with the cytosol RNase p activity. J Biol Chem. 1985;260:5942–9.
de Coo IF, Sistermans EA, de Wijs IJ, et al. A mitochondrial tRNA(val) gene mutation (G1642A) in a patient with mitochondrial myopathy, lactic acidosis, and stroke-like episodes. Neurology. 1998;50:293–5.
Silvestri G, Santorelli FM, Shanske S, et al. A new mtDNA mutation in the tRNA(leu(UUR)) gene associated with maternally inherited cardiomyopathy. Hum Mutat. 1994;3:37–43.
Goldstein JD, Shanske S, Bruno C, et al. Maternally inherited mitochondrial cardiomyopathy associated with a C-to-T transition at nucleotide 3303 of mitochondrial DNA in the tRNA(leu(UUR)) gene. Pediatr Dev Pathol. 1999;2:78–85.
Ciafaloni E, Ricci E, Shanske S, et al. Melas: clinical features, biochemistry, and molecular genetics. Ann Neurol. 1992;31:391–8.
Goto Y, Horai S, Matsuoka T, et al. Mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS): a correlative study of the clinical features and mitochondrial DNA mutation. Neurology. 1992;42:545–50.
Hiruta Y, Chin K, Shitomi K, et al. Mitochondrial encephalomyopathy with A to G transition of mitochondrial transfer RNA(Leu(UUR)) 3,243 presenting hypertrophic cardiomyopathy. Intern Med. 1995;34:670–3.
Gerbitz KD, Paprotta A, Jaksch M, et al. Diabetes mellitus is one of the heterogeneous phenotypic features of a mitochondrial DNA point mutation within the tRNALeu(UUR) gene. FEBS Lett. 1993;321:194–6.
Mariotti C, Tiranti V, Carrara F, et al. Defective respiratory capacity and mitochondrial protein synthesis in transformant cybrids harboring the tRNA(Leu(UUR)) mutation associated with maternally inherited myopathy and cardiomyopathy. J Clin Invest. 1994;93:1102–7.
Hayashi J, Ohta S, Kagawa Y, et al. Functional and morphological abnormalities of mitochondria in human cells containing mitochondrial DNA with pathogenic point mutations in tRNA genes. J Biol Chem. 1994;269:19060–6.
Taniike M, Fukushima H, Yanagihara I, et al. Mitochondrial tRNA(ile) mutation in fatal cardiomyopathy. Biochem Biophys Res Commun. 1992;186:47–53.
Perli E, Giordano C, Tuppen HA, et al. Isoleucyl-tRNA synthetase levels modulate the penetrance of a homoplasmic m.4277 T > C mitochondrial tRNA(ile) mutation causing hypertrophic cardiomyopathy. Hum Mol Genet. 2012;21:85–100.
Giordano C, Perli E, Orlandi M, et al. Cardiomyopathies due to homoplasmic mitochondrial tRNA mutations: Morphologic and molecular features. Hum Pathol. 2013;44(7):1262–70.
Merante F, Myint T, Tein I, et al. An additional mitochondrial tRNA(ile) point mutation (A-to-G at nucleotide 4295) causing hypertrophic cardiomyopathy. Hum Mutat. 1996;8:216–22.
Casali C, Santorelli FM, D'Amati G, et al. A novel mtDNA point mutation in maternally inherited cardiomyopathy. Biochem Biophys Res Commun. 1995;213:588–93.
Chamkha I, Mkaouar-Rebai E, Aloulou H, et al. A novel m.3395A > G missense mutation in the mitochondrial ND1 gene associated with the new tRNA(ile) m.4316A > G mutation in a patient with hypertrophic cardiomyopathy and profound hearing loss. Biochem Biophys Res Commun. 2011;404:504–10.
Tanaka M, Ino H, Ohno K, et al. Mitochondrial mutation in fatal infantile cardiomyopathy. Lancet. 1990;336:1452.
Santorelli FM, Mak SC, Vazquez-Acevedo M, et al. A novel mitochondrial DNA point mutation associated with mitochondrial encephalocardiomyopathy. Biochem Biophys Res Commun. 1995;216:835–40.
Tiranti V, D'Agruma L, Pareyson D, et al. A novel mutation in the mitochondrial tRNA(val) gene associated with a complex neurological presentation. Ann Neurol. 1998;43:98–101.
Acknowledgments
This work was supported by grants of the Center for Biomedical Research on Rare Diseases (CIBERER), Instituto de Salud Carlos III (grants PI 07/0167, PI 10/0703 to R.G. and PI06/0205, PS09/00941 to B.B.) and Comunidad de Madrid (grant number S2010/BMD-2402).
Conflict of Interest
The authors report no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Gallardo, M.E., Galera, T., Garesse, R., Bornstein, B. (2015). Mitochondrial tRNA Valine in Cardiomyopathies. In: Rajendram, R., Preedy, V., Patel, V. (eds) Branched Chain Amino Acids in Clinical Nutrition. Nutrition and Health. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-1914-7_7
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1914-7_7
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-1913-0
Online ISBN: 978-1-4939-1914-7
eBook Packages: MedicineMedicine (R0)