
Abstract
Phospholipase D (PLD) produces phosphatidic acid, which is converted to diacylglycerol (DAG) by phosphatidate phosphohydrolase (PAP). Since both these lipid signaling molecules regulate Ca2+-movements, they also influence cardiac contractile function. In this article, we discuss the importance of PLD in relation to the production of lipid signaling molecules and regulation of cardiac function under various pathophysiological conditions such as ischemic heart disease, diabetic cardiomyopathy, and congestive heart failure. In fact, marked alterations in PLD activities have been reported to occur in ischemic heart, diabetic heart, and failing heart. While the mechanisms of changes in PLD activities in heart disease may be of complex nature, oxidative stress seems to play a critical role in the activation of PLD. From the evidence provided it is suggested that impairment in this phospholipid signal transduction pathway results in cardiac dysfunction during the development of different myocardial diseases.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Phospholipase D
- Signal transduction
- Diabetic cardiomyopathy
- Congestive heart failure
- Ischemia-reperfusion injury
- PLD-mediated signal transduction
1 Introduction
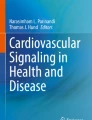
The hydrolysis of phosphatidylcholine (PC) by phospholipase D (PLD) produces phosphatidic acid (PA), which in turn is converted to 1, 2 DAG by the action of phosphatidate phosphohydrolase (PAP) [1, 2]. Both PLD and PAP are thus considered to modulate myocardial levels of PA and DAG. Different hormones such as norepinephrine, endothelin-1, and angiotensin II (Ang II) have been shown to increase formation of PA in cardiomyocytes [3, 4] and stimulate sarcolemmal (SL) and sarcoplasmic reticular (SR) Ca2+-transport systems [5, 6]. Furthermore, PA has been reported to increase the intracellular concentration of free Ca2+ in adult cardiomyocytes and to augment cardiac contractile activity of the normal heart [5, 7]. DAG can also influence cardiac function through phosphorylation of myocardial proteins, including ion channels, via activation of protein kinase C (PKC) isozymes [8]. These PLD-mediatd signal transduction events are summarized in Fig. 23.1.
Two mammalian PLD isozymes, PLD1 and PLD2, have been cloned [9]. While PLD1 is localized to the Golgi apparatus and nuclei [10], PLD2 is the major myocardial PLD isozyme specifically localized to the SL membrane [11]; other subcellular localizations of PLD2 have also been reported [12, 13]. Interestingly, a transient expression of PLD1 during heart development in rats has been demonstrated [14]. In this regard, the level of PLD1 protein increased transiently from 0 to 3 days postpartum and declined gradually beginning 7 days after birth. This suggested that PLD1 protein in the heart is strongly associated with the early postnatal development of the heart in rats [14].
PLD1 requires phosphatidylinositol 4, 5-bisphosphate (PIP2) for its activity, which is stimulated by PKC and Rho small G-protein family members [9, 15–24]. PLD2 also requires PIP2 for its activity [11], but, unlike PLD1, PLD2 is activated by unsaturated fatty acids [2, 16, 17, 25, 26] and is insensitive to the PLD1 activating factors [27]. It should be noted that PLD isozymes contain N-terminal PH (pleckstrin) and PX (phox) homology domains. Both these domains also interact specifically with distinct phosphoinositide ligands [28]. Both the PH and PX domains are important for PLD function by controlling the dynamic association of the enzyme with the plasma membrane. Thus, there are two modes of PLD regulation by phosphoinositides; stimulation of activity mediated by the polybasic domain and dynamic regulation of membrane targeting mediated by the PH and PX domains [28].
Some studies have shown that both receptor- and non-receptor coupled tyrosine kinases are involved in the regulation of PLD activity, in addition to serine/threonine kinases, Ca2+-calmodulin-dependent protein kinase, and cAMP kinases [29–31]. G-proteins, Gα12 and Gα13, have also been reported to activate PLD [32]. Another important regulator of PLD is ARF; ARF directly activates PLD1 and has also been shown to activate PLD2 [25, 33–36]. In fact, PLD2 has been reported to be selectively activated by ARF6 [12]. It is interesting to note that U73122, a known phospholipase C inhibitor, is a potent inhibitor of myocardial PLD by a PIP2-dependent mechanism and thus PLD may be involved in some of the effects ascribed to PLC [37]. While there is some information on the posttranslational mechanisms of regulation of the myocardial PLD isozymes, this is not completely understood.
The increased formation of reactive oxygen species (ROS) is generally associated with oxidative stress and subsequent cardiovascular injury and cardiac dysfunction [38–40]. Since ROS and oxidant molecules such as H2O2 are implicated in the pathogenesis of cardiac dysfunction, this article is intended to describe the role of oxidative stress in relation to myocardial PLD and cardiac dysfunction under different myocardial diseases such as diabetic cardiomyopathy, congestive heart failure, and ischemic heart disease.
2 Impairment of PLD Activities During Diabetes
Oxidative stress has been implicated in the pathogenesis of diabetic cardiomyopathy [41–47]. As a consequence of the effects of oxidative stress on the cardiomyocytes, it would be expected that oxidants and ROS could have an impact on the PLD activity during diabetes. In fact, SL PLD activities have been shown to be significantly depressed in diabetic animals [48, 49], resulting in a marked reduction of PLD-derived PA. It has been suggested that this could lead to an impairment of cardiac function in chronic diabetes [48, 49].
It is pointed out that enhanced tissue Ang II levels have been reported in diabetes and might lead to cardiac dysfunction through oxidative stress [50]. Recently Ang II-induced NADPH oxidase has been shown to be involved in hyperglycemia-induced cardiomyocyte dysfunction, which might play a role in diabetic cardiomyopathy [51] and may be related to impaired PLD activities due to superoxide generation. Impaired PLD activation has been shown to be involved in the damaging effects of oxidative stress in other cells as well. Decreased superoxide generation by neutrophils in insulin-dependent diabetics is, in part, due to impaired activation of PLD [52], and is solely due to high glucose concentrations. The suppressive effect of glucose on diabetic neutrophils is associated with a reduction in PLD activation, which improves when diabetic neutrophils are placed in a normal glucose environment. Glucose causes a reduction in PLD activation, leading to a decrease in second messenger generation and incomplete activation of the respiratory burst [52]. It is interesting to note that we have reported a decrease in the SL amount of PIP2, due to depressed activities of the phosphatidylinositol (PI) kinases in the diabetic heart [53], likely as a result of oxidant-mediated depression in the PI kinase activities [54]. In this regard, the depressed SL PLD activity during diabetes [45, 46] may also be explained on the basis of a reduced SL PIP2 level. While direct information on the redox regulation of PLD isozyme activities and the functional consequences of changes in PLD activities in diabetic cardiomyopathy remains to be established, it is reasonable to assume that the depressed PLD activities in the heart during diabetes may be due to oxidative stress.
3 Abnormal PLD Activities During Cardiac Hypertrophy and Heart Failure
It is well known that heart failure is a major cause for significant morbidity and mortality; however, the pathophysiological events have not been fully elucidated. There is growing evidence that oxidative stress is implicated in the cardiac dysfunction leading to CHF [55–58]. Oxygen-free radicals can affect heart SL [59–62], SR [63], and mitochondrial functions [64], thus affecting signal transduction mechanisms that are possibly involved in cardiac remodeling and subsequent CHF. Since oxidative stress has significant effects on the SL membrane during CHF, it can be assumed that the oxidative stress will also exert detrimental effects on PLD activities.
The mRNA expression levels of both PLD1 and PLD2 have been reported to be markedly enhanced in ventricular pressure-overload hypertrophy subsequent to aortic banding in rats [65]. A similar induction of PLD mRNA and protein expression has also been reported in hypertrophied human hearts of individuals who had died from noncardiac causes [65]. These authors suggested that PLD activation by α-adrenoceptor and PKC plays a significant role in cell signaling in hypertrophy due to pressure overload [65]. Ventricular fibrosis is promoted by many factors that activate PLD and induce cardiac dysfunction and heart failure. In a hypertensive heart failure model using Dahl-Iwai salt-sensitive rats, PLD activity was seen to be increased with progressive ventricular fibrosis, leading to myocardial stiffening and heart failure [66]. Inhibition of PLD activity with administration of N-methylethanolamine decreased collagen content, prevention of myocardial stiffening, attenuation of ventricular hypertrophy as well as hemodynamic deterioration [66].
We have previously shown that PLD activities are differently altered in CHF subsequent to myocardial infarction induced by the occlusion of the coronary artery [67]. While SL PLD1 activity was decreased, an increase in PLD2 activity was observed in the viable left ventricular tissue. Although the specific role of cardiac PLD isozymes is not fully established, an oleate-dependent PLD activity has been shown to be drastically increased during apoptosis of Jurkat T cells [68], whereas increased PLD2 activity has been shown to reduce hypoxia-induced death of PC12 cells [69]; these studies suggest that PLD2 may play a role in cellular apoptosis. It is interesting to note that Ang II activates NADPH oxidase [70, 71], which can be prevented by imidapril, a known angiotensin converting enzyme inhibitor. Activation of the renin-angiotensin system is the hallmark of CHF [72]. In addition, increased myocardial NADPH oxidase activity in CHF has been reported [73, 74]. We have earlier shown that imidapril normalizes the augmented PLD2 activity in CHF [75]. It is possible that this may be due to a blockade of NADPH oxidase and ROS-mediated activation of PLD2. However, while extensive studies need to be conducted to fully determine the functional significance as well as the mechanisms of impaired PLD1 and PLD2 activities in CHF, it is likely that PLD isozymes are altered due to oxidative stress and may influence cardiomyocyte function of the failing heart through impaired Ca2+-handling.
4 Alterations in PLD Activities During Cardiac Ischemia-Reperfusion
A decrease in the blood supply to the heart due to atherosclerosis, thrombosis, or coronary artery spasm is known to induce myocardial ischemia. Although reperfusion of the ischemic myocardium during early stages is essential to prevent cardiac damage, reperfusion of the ischemic heart, after a certain critical period, exerts deleterious effects. These are represented by contractile dysfunction, an increase in infarct size, ultrastructural damage, and changes in myocardial metabolism, which at a later stage leads to cell necrosis [76]. During ischemia, mitochondrial carriers are in a reduced state, due to the degradation of the adenine nucleotide pool. Thus, the interaction of molecular oxygen trapped within the inner membrane of the mitochondria with the leakage of electrons from the respiratory chain leads to the formation of ROS [77]. The deleterious effects of oxidative stress in myocardial I-R are well documented and strongly correlated with cardiac dysfunction [78], a decrease in the antioxidant defense mechanism [79, 80] as well as an increase in lipid peroxidation [80, 81], leading to increased membrane permeability. PLD has been shown in many cases to contribute to the deleterious effects due to oxidative stress in I-R injury. For example, lipid oxidation products such as oxidized LDL have been considered prime candidates for inducing cellular necrosis. Oxidized LDL stimulates PLD [82], implicating a role for PLD in cellular necrosis. Cardiac SL sodium-hydrogen (Na+–H+) exchanger is critical for the regulation of intracellular pH and its activity contributes to I-R injury. Incubation of porcine cardiac SL vesicles with exogenous PLD results in an inhibition of Na+–H+ exchanger [83]. It was concluded that PLD-induced changes in the cardiac SL membrane phospholipid environment alter Na+–H+ exchanger activity.
While some investigators have reported that the activation of PLD is associated with an improvement of post-ischemic functional recovery and attenuation of cellular injury [84], other investigators, as well as work from our laboratory, have found that PLD is not activated in the ischemic heart [85–88]. Furthermore, our studies also revealed that the increase in the SL PLD2 activity in early reperfusion of the 30 min ischemic heart was associated with an increase in V max, indicating that the PLD2 activation may be due to posttranslational modifications as a result of oxidative stress. On the other hand, we have reported that a Ca2+-independent phospholipase A2 (cytosolic PLA2) and subsequent mobilization of the unsaturated fatty acid has been shown to modulate the activity of PLD in heart SL [89]. Interestingly, the cytosolic PLA2 is also activated by H2O2 [90], which could provide a mechanism of an indirect regulation of the SL PLD2 activity by H2O2. It should be noted that we also observed a decrease in the SR PLD2 activity after 5 min of reperfusion. Although the K m value of the SR PLD2 was reduced (increased substrate affinity), the depressed V max value would seem to imply a defect in the catalytic domain of this enzyme; it was suggested that a reversible oxidation may occur since the PLD2 activity was recovered after 30 min reperfusion. In fact, SR PLD activity, in vitro, has been reported to be inhibited by nonradical oxidants, H2O2 and HOCI, through reversible modification of associated thiol groups [18]. Thus, the enzyme may be controlled by the GSH redox status of the cardiac cell. In this regard, in the isolated perfused rabbit heart, an ischemic period results in a progressive reduction of tissue glutathione content and of the GSH/GSSG ratio [91], while post-ischemic reperfusion has been shown to lead to a further decrease in the GSH/GSSG ratio [91]. However, a similar response has also been demonstrated for the SL enzyme [92], which is not consistent with the increase in its activity. This inconsistency could be explained on the basis that the functional thiol groups of the SL PLD2 in the isolated perfused heart are not as readily accessible by oxidants as these are in the isolated SL preparation. Such differences may exist between the sensitivity of the SR and SL PLD to different concentrations of oxidant molecules as well as ROS.
Ischemic preconditioning (IP) involving a brief period of ischemia, prior to a prolonged period of ischemia, has been shown to improve myocardial function and diminishes the infarct size. Activation of PLD due to I-R injury as well as in the preconditioned hearts has been documented [93–95]. Agonists of PLD simulate the effects of IP, whereas the inhibition of PLD blocks the beneficial effects of IP as evidenced by the increased incidence of ventricular arrhythmias [85]. The inhibition of PLD can be seen to reduce the amount of DAG and PA as well as significantly inhibit the stimulation of PKC. Thus, PLD may play a role in the myocardial protection afforded by IP. Indeed, this protective effect may be due to ROS generation during the IP [96, 97], which may also be related to the activation of PLD, thus providing a mechanism of action of IP and protection against I-R injury. In addition, myocardial adaptation to ischemia (IP) is considered to occur through the activation of several tyrosine kinases [98]. The phosphorylation of tyrosine kinases has been shown to be linked with the activation of PLD leading to the activation of multiple kinases [93, 94] including PKC isozymes [99], therefore suggesting that PLD may be a component in the redox signaling designed to protect the heart during IP. While the exact consequences of the changes in PLD1 and PLD2 activities in the heart remain to be determined, PLD isozymes could emerge as an important target for protection against injury during cardiac I-R.
5 Conclusions
From the aforementioned discussion, it is evident that impairment of myocardial PLD activities is associated with cardiac dysfunction under different myocardial diseases, while PLD isozyme specific activation may provide cardioprotection (Fig. 23.2). Although significant advancements have been made, more is required to define the role of PLD in different cardiac pathologies. While oxidative stress appears to be a major factor in causing PLD abnormalities, the targeting of PLD, more specifically, modulation of membrane PA levels, may offer a potential for drug development. Defects in other phospholipid-mediated signaling pathways (PLC and PLA2) are also implicated in different myocardial diseases, and in view of the cross-talk and complexities between these pathways (Fig. 23.3), lipid products generated through their activities may not only alter signal transduction processes, but also modulate the lipid microenvironment of membrane-associated proteins. Thus, alterations in the PLD activities can be seen to influence cardiac function and may constitute additional therapeutic targets for drug discovery [100–102] for the treatment of heart disease due to different etiologies.

Myocardial phospholipase D signal transduction. PLD1 phospholipase D1, PLD2 phospholipase D2, PAP phosphatidate phosphohydrolase, PLC phospholipase C, PKC protein kinase C; +, stimulation

Differential changes and impact of phospholipase D during different cardiac pathologies. PLD phospholipase D

Complexities of phospholipid-mediated signal transduction pathways. PLA 2 phospholipase A2, PLD phospholipase D, PAP phosphatidate phosphohydrolase, PLC phospholipase C, PC phosphatidylcholine, DAG diacylglycerol, PA phosphatidic acid, AA arachidonic acid, PI phosphatidylinositol, PI4P phosphatidylinositol-4 phosphate, PIP 2 phosphatidylinositol,-4,5-bisphosphate, IP 3 inositol-1,4,5-trisphosphate; +, stimulation
References
Exton JH (1994) Phosphatidylcholine breakdown and signal transduction. Biochim Biophys Acta 1212:26–42
Panagia V, Ou C, Taira Y et al (1991) Phospholipase D activity in subcellular membranes of rat ventricular myocardium. Biochim Biophys Acta 1064:242–250
Sadoshima J, Izumo S (1993) Signal transduction pathways of angiotensin II-induced c-fos gene expression in cardiac myocytes in vitro. Roles of phospholipid-derived second messengers. Circ Res 73:424–438
Ye H, Wolf RA, Kurz T, Corr PB (1994) Phosphatidic acid increases in response to noradrenaline and endothelin-1 in adult rabbit ventricular myocytes. Cardiovasc Res 28:1828–1834
Dhalla NS, Xu YJ, Sheu SS et al (1997) Phosphatidic acid: a potential signal transducer for cardiac hypertrophy. J Mol Cell Cardiol 29:2865–2871
Xu YJ, Botsford MW, Panagia V, Dhalla NS (1996) Responses of heart function and intracellular free Ca2+ to phosphatidic acid in diabetic rats. Can J Cardiol 12:1092–1098
Xu YJ, Panagia V, Shao Q et al (1996) Phosphatidic acid increases intracellular free Ca2+ and cardiac contractile force. Am J Physiol Heart Circ Physiol 271:H651–H659
Lamers JM, Eskildsen-Helmond YE, Resink AM et al (1995) Endothelin-1-induced phospholipase C β and D and protein kinase C isoenzyme signaling leading to hypertrophy in rat cardiomyocytes. J Cardiovasc Pharmacol 26:S100–S103
Frohman MA, Morris AJ (1999) Phospholipase D structure and function. Chem Phys Lipids 98:127–140
Freyberg Z, Sweeney D, Siddhanta A et al (2001) Intracellular localization of phospholipase D1 in mammalian cells. Mol Biol Cell 12:943–955
Park JB, Kim JH, Kim KY et al (2000) Cardiac phospholipase D2 localizes to sarcolemmal membranes and is inhibited by α-actinin in an ADP-ribosylation factor-reversible manner. J Biol Chem 275:21295–21301
Hiroyama M, Exton JH (2005) Localization and regulation of phospholipase D2 by ARF6. J Cell Biochem 95:149–164
Freyberg Z, Bourgoin S, Shields D (2002) Phospholipase D2 is localized to the rims of the Golgi apparatus in mammalian cells. Mol Biol Cell 13:3930–3942
Moon C, Kim H, Kim S et al (2008) Transient expression of Phospholipase D1 during heart development in rats. J Vet Med Sci 70:411–413
Hammond SM, Jenco JM, Nakashima S et al (1997) Characterization of two alternately spliced forms of phospholipase D1. Activation of the purified enzymes by phosphatidylinositol 4,5-bisphosphate, ADP-ribosylation factor, and Rho family monomeric GTP-binding proteins and protein kinase C-α. J Biol Chem 272:3860–3868
Kim JH, Lee SD, Han JM et al (1998) Activation of phospholipase D1 by direct interaction with ADP-ribosylation factor 1 and RalA. FEBS Lett 430:231–235
Lee TG, Park JB, Lee SD et al (1997) Phorbol myristate acetate-dependent association of protein kinase C α with phospholipase D1 in intact cells. Biochim Biophys Acta 1347:199–204
Liscovitch M, Chalifa V, Pertile P et al (1994) Novel function of phosphatidylinositol 4,5-bisphosphate as a cofactor for brain membrane phospholipase D. J Biol Chem 269:21403–21406
Malcolm KC, Elliott CM, Exton JH (1996) Evidence for Rho-mediated agonist stimulation of phospholipase D in rat fibroblasts. Effects of Clostridium botulinum C3 exoenzyme. J Biol Chem 271:13135–13139
Yamazaki M, Zhang Y, Watanabe H et al (1999) Interaction of the small G protein RhoA with the C terminus of human phospholipase D1. J Biol Chem 274:6035–6038
Nataranjan V, Scribner WM, Vepa S (1996) Regulation of phospholipase D by tyrosine kinases. Chem Phys Lipids 24:103–116
Exton JH (1998) Phospholipase D. Biochim Biophys Acta 1436:105–115
Singer WD, Brown HA, Jiang X, Sternweis PC (1996) Regulation of phospholipase D by protein kinase C is synergistic with ADP-ribosylation factor and independent of protein kinase activity. J Biol Chem 271:4504–4510
Sciorra VA, Hammond SM, Morris AJ (2001) Potent direct inhibition of mammalian phospholipase D isoenzymes by calphostin-c. Biochemistry 40:2640–2646
Hammond SM, Altshuller YM, Sung TC et al (1995) Human ADP-ribosylation factor-activated phosphatidylcholine-specific phospholipase D defines a new and highly conserved gene family. J Biol Chem 270:29640–29643
Dai J, Williams SA, Ziegelhoffer A, Panagia V (1995) Structure-activity relationship of the effect of cis-unsaturated fatty acids on heart sarcolemmal phospholipase D activity. Prostagland Leuk Essent Fatty Acids 52:167–171
Colley WC, Sung TC, Roll R et al (1997) Phospholipase D2, a distinct phospholipase D isoform with novel regulatory properties that provokes cytoskeletal reorganization. Curr Biol 7:191–201
Morris AJ (2007) Regulation of phospholipase D activity, membrane targeting and intracellular trafficking by phosphoinositides. Biochem Soc Symp 74:247–257
Gustavsson L, Moehren G, Torres-Marquez ME et al (1994) The role of cytosolic Ca2+, protein kinase C, and protein kinase A in hormonal stimulation of phospholipase D in rat hepatocytes. J Biol Chem 269:849–859
Kanaho Y, Nishida A, Nozawa Y (1992) Calcium rather than protein kinase C is the major factor to activate phospholipase D in FMLP-stimulated rabbit peritoneal neutrophils. Possible involvement of calmodulin/myosin L chain kinase pathway. J Immunol 149:622–628
Kiss Z (1992) Differential effects of platelet-derived growth factor, serum and bombesin on phospholipase D-mediated hydrolysis of phosphatidylethanolamine in NIH 3T3 fibroblasts. Biochem J 285:229–233
Kurose H (2003) Gα12 and Gα13 as key regulatory mediator in signal transduction. Life Sci 74:155–161
Lopez I, Arnold RS, Lambeth JD (1998) Cloning and initial characterization of a human phospholipase D2 (hPLD2). ADP-ribosylation factor regulates hPLD2. J Biol Chem 273:12846–12852
Dascher C, Balch WE (1994) Dominant inhibitory mutants of ARF1 block endoplasmic reticulum to Golgi transport and trigger disassembly of the Golgi apparatus. J Biol Chem 269:1437–1448
Rumenapp U, Geiszt M, Wahn F et al (1995) Evidence for ADP-ribosylation-factor-mediated activation of phospholipase D by m3 muscarinic acetylcholine receptor. Eur J Biochem 234:240–244
Shome K, Nie Y, Romero G (1998) ADP-ribosylation factor proteins mediate agonist-induced activation of phospholipase D. J Biol Chem 273:30836–30841
Burgdorf C, Schafer U, Richardt G, Kurz T (2010) U73122, an aminosteroid Phospholipase C inhibitor, is a potent inhibitor of cardiac Phospholipase D by PIP2-dependent mechanism. J Cardiovasc Pharmacol 55:555–559
Kukreja RC, Hess ML (1992) The oxygen free radical system: from equations through membrane-protein interactions to cardiovascular injury and protection. Cardiovasc Res 26:641–655
Singal PK, Khaper N, Palace V, Kumar D (1998) The role of oxidative stress in the genesis of heart disease. Cardiovasc Res 40:426–432
Müller BA, Dhalla NS (2010) Mechanisms of the beneficial actions of ischemic preconditioning on subcellular remodeling in ischemic-reperfused heart. Curr Cardiol Rev 6:255–264
Dhalla NS, Liu X, Panagia V, Takeda N (1998) Subcellular remodeling and heart dysfunction in chronic diabetes. Cardiovasc Res 40:239–247
Mullarkey CJ, Edelstein D, Brownlee M (1990) Free radical generation by early glycation products: a mechanism for accelerated atherogenesis in diabetes. Biochem Biophys Res Commun 173:932–939
Giugliano D, Marfella R, Acampora R et al (1998) Effects of perindopril and carvedilol on endothelium-dependent vascular functions in patients with diabetes and hypertension. Diabetes Care 21:631–636
Jain SK, McVie R, Jaramillo JJ et al (1996) The effect of modest vitamin E supplementation on lipid peroxidation products and other cardiovascular risk factors in diabetic patients. Lipids 31(suppl):S87–S90
Dhalla NS, Pierce GN, Innes IR, Beamish RE (1985) Pathogenesis of cardiac dysfunction in diabetes mellitus. Can J Cardiol 1:263–281
Afzal N, Ganguly PK, Dhalla KS et al (1988) Beneficial effects of verapamil in diabetic cardiomyopathy. Diabetes 37:936–942
Golfman L, Dixon IMC, Takeda N et al (1998) Cardiac sarcolemmal Na+-Ca2+ exchange and Na+-K+ ATPase activities and gene expression in alloxan-induced diabetes in rats. Mol Cell Biochem 188:91–101
Williams SA, Tappia PS, Yu CH et al (1997) Subcellular alterations in cardiac phospholipase D activity in chronic diabetes. Prostagland Leuk Essent Fatty Acids 57:95–99
Williams SA, Tappia PS, Yu CH et al (1998) Impairment of the sarcolemmal phospholipase D-phosphatidate phosphohydrolase pathway in diabetic cardiomyopathy. J Mol Cell Cardiol 30:109–118
Dzau VJ (2001) Tissue angiotensin and pathobiology of vascular disease. Hypertension 37:1047–1052
Privratsky JR, Wold LE, Sowers JR et al (2003) AT1 blockade prevents glucose-induced cardiac dysfunction in ventricular myocytes: role of the AT1 receptor and NADPH oxidase. Hypertension 42:206–212
Ortmeyer J, Mohsenin V (1996) Inhibition of phospholipase D and superoxide generation by glucose in diabetic neutrophils. Life Sci 59:255–262
Tappia PS, Liu SY, Tong Y et al (2001) Reduction of phosphatidylinositol-4,5-bisphosphate mass in heart sarcolemma during diabetic cardiomyopathy. Adv Exp Med Biol 498:183–190
Mesaeli N, Tappia PS, Suzuki S et al (2000) Oxidants depress the synthesis of phosphatidylinositol 4,5-bisphosphate in heart sarcolemma. Arch Biochem Biophys 382:48–56
Dhalla NS, Temsah RM, Netticadan T (2000) Role of oxidative stress in cardiovascular diseases. J Hypertens 18:655–673
Dhalla NS, Golfman L, Takeda S et al (1999) Evidence for the role of oxidative stress in acute ischemic heart disease: a brief review. Can J Cardiol 15:587–593
Dhalla NS, Temsah R (2001) Sarcoplasmic reticulum and cardiac oxidative stress: an emerging target for heart disease. Expert Opin Ther Targets 5:205–217
Giordano FJ (2005) Oxygen, oxidative stress, hypoxia and heart failure. J Clin Invest 115:500–508
Kaneko M, Elimban V, Dhalla NS (1989) Mechanism for depression of heart sarcolemmal Ca2+ pump by oxygen free radicals. Am J Physiol Heart Circ Physiol 257:H804–H811
Kaneko M, Beamish RE, Dhalla NS (1989) Depression of heart sarcolemmal Ca2+-pump activity by oxygen free radicals. Am J Physiol Heart Circ Physiol 256:H368–H374
Kaneko M, Lee SL, Wolf CM, Dhalla NS (1989) Reduction of calcium channel antagonist binding sites by oxygen free radicals in rat heart. J Mol Cell Cardiol 21:935–943
Kaneko M, Chapman DC, Ganguly PK et al (1991) Modification of cardiac adrenergic receptors by oxygen free radicals. Am J Physiol Heart Circ Physiol 260:H821–H826
Okabe E, Hess ML, Oyama M, Ito H (1983) Characterization of free radical-mediated damage of canine cardiac sarcoplasmic reticulum. Arch Biochem Biophys 225:164–177
Otani H, Tanaka H, Inoue T et al (1984) In vitro study on contribution of oxidative metabolism of isolated rabbit heart mitochondria to myocardial reperfusion injury. Circ Res 55:168–175
Peivandi AA, Huhn A, Lehr HA et al (2005) Upregulation of phospholipase D expression and activation in ventricular pressure-overload hypertrophy. J Pharmacol Sci 98:244–254
Yamamoto K, Takahashi Y, Mano T et al (2004) N-methylethanolamine attenuates cardiac fibrosis and improves diastolic function: inhibition of Phospholipase D as a possible mechanism. Eur Heart J 25:1221–1229
Dent MR, Singal T, Dhalla NS, Tappia PS (2005) Expression of phospholipase D isozymes in scar and viable tissue in congestive heart failure due to myocardial infarction. J Cell Mol Med 8:526–536
Kasai T, Ohguchi K, Nakashima S et al (1998) Increased activity of oleate-dependent type phospholipase D during actinomycin D-induced apoptosis in Jurkat T cells. J Immunol 161:6469–6474
Yamakawa H, Banno Y, Nakashima S et al (2000) Increased phospholipase D2 activity during hypoxia-induced death of PC12 cells: its possible anti-apoptotic role. Neuroreport 11:3647–3650
Tojo A, Onozato ML, Kobayashi N et al (2002) Angiotensin II and oxidative stress in Dahl Salt-sensitive rat with heart failure. Hypertension 40:834–839
Harrison DG, Cai H, Landmesser U, Griendling KK (2003) Interactions of angiotensin II with NAD(P)H oxidase, oxidant stress and cardiovascular disease. J Renin Angiotensin Aldosterone Syst 4:51–61
Dhalla NS, Shao Q, Panagia V (1998) Remodeling of cardiac membranes during the development of congestive heart failure. Heart Fail Rev 2:261–272
Heymes C, Bendall JK, Ratajczak P et al (2003) Increased myocardial NADPH oxidase activity in human heart failure. J Am Coll Cardiol 41:2164–2171
Li JM, Gall NP, Grieve DJ et al (2002) Activation of NADPH oxidase during progression of cardiac hypertrophy to failure. Hypertension 40:477–484
Yu CH, Panagia V, Tappia PS et al (2002) Alterations of sarcolemmal phospholipase D and phosphatidate phosphohydrolase in congestive heart failure. Biochim Biophys Acta 1584:65–72
Kloner RA, Ellis SG, Lange R, Braunwald E (1983) Studies of experimental coronary artery reperfusion. Effects on infarct size, myocardial function, biochemistry, ultrastructure and microvascular damage. Circulation 68:I8–I15
Freeman BA, Crapo JD (1982) Biology of disease: free radicals and tissue injury. Lab Invest 47:412–426
Ferrari R, Alfieri O, Curello S et al (1990) Occurrence of oxidative stress during reperfusion of the human heart. Circulation 81:201–211
Hasenfuss G, Meyer M, Schillinger W (1997) Calcium handling proteins in the failing human heart. Basic Res Cardiol 92:87–93
Palace V, Kumar D, Hill MF, Khaper N, Singal PK (1999) Regional differences in non-enzymatic antioxidants in the heart under control and oxidative stress conditions. J Mol Cell Cardiol 31:193–202
Meerson FZ, Kagan VE, Kozlov Yu P et al (1982) The role of lipid peroxidation in pathogenesis of ischemic damage and the antioxidant protection of the heart. Basic Res Cardiol 77:465–485
Natarajan V, Scribner VM, Hart CM, Parthasarathy S (1995) Oxidized low density lipoprotein-mediated activation of phospholipase D in smooth muscle cells: a possible role in cell proliferation and atherogenesis. J Lipid Res 36:2005–2016
Goel DP, Vecchini A, Panagia V, Pierce GN (2000) Altered cardiac Na+/H+ exchange in Phospholipase D-treated sarcolemmal vesicles. Am J Physiol Heart Circ Physiol 279:H1179–H1184
Tosaki A, Maulik N, Cordis G et al (1997) Ischemic preconditioning triggers phospholipase D signaling in rat heart. Am J Physiol Heart Circ Physiol 273:H1860–H1866
Bruhl A, Faldum A, Loffelholz K (2003) Degradation of phosphatidylethanol counteracts the apparent phospholipase D-mediated formation in heart and other organs. Biochim Biophys Acta 1633:84–89
Bruhl A, Hafner G, Loffelholz K (2004) Release of choline in the isolated heart, an indicator of ischemic phospholipid degradation and its protection by ischemic preconditioning: no evidence for a role of phospholipase D. Life Sci 75:1609–1620
Kurz T, Kemken D, Mier K et al (2004) Human cardiac phospholipase D activity is tightly controlled by phosphatidylinositol 4,5-bisphosphate. J Mol Cell Cardiol 36:225–232
Asemu G, Dent MR, Singal T et al (2005) Differential changes in phospholipase D and phosphatidate phosphohydrolase activities in ischemia-reperfusion of rat heart. Arch Biochem Biophys 436:136–144
Liu SY, Tappia PS, Dai J et al (1998) Phospholipase A2-mediated activation of phospholipase D in rat heart sarcolemma. J Mol Cell Cardiol 30:1203–1214
Sapirstein A, Spech RA, Witzgall R, Bonventre JV (1996) Cytosolic phospholipase A2 (PLA2), but not secretory PLA2, potentiates hydrogen peroxide cytotoxicity in kidney epithelial cells. J Biol Chem 271:21505–21513
Ferrari R, Ceconni C, Curello S et al (1991) Oxygen free radicals and myocardial damage: protective role of thiol-containing agents. Am J Med 91:95S–105S
Gilbert HF (1984) Redox control of enzyme activities by thiol/disulfide exchange. Methods Enzymol 107:330–351
Moraru II, Popescu LM, Maulik N et al (1992) Phospholipase D signaling in ischemic heart. Biochim Biophys Acta 1139:148–154
Cohen MV, Liu Y, Liu GS et al (1996) Phospholipase D plays a role in ischemic preconditioning in rabbit heart. Circulation 94:1713–1718
Trifan OC, Popescu LM, Tosaki A et al (1996) Ischemic preconditioning involves phospholipase D. Ann NY Acad Sci 793:485–488
Lecour S, Rochette L, Opie L (2005) TNFα-induced cardioprotection. Cardiovasc Res 65:239–243
Tritto I, Ambrosio G (2001) Role of oxidants in the signaling pathway of preconditioning. Antioxid Redox Signal 3:3–10
Armstrong SC (2004) Protein kinase activation and myocardial ischemia/reperfusion injury. Cardiovasc Res 61:427–436
Eskildsen-Helmond YE, Gho BC, Bezstarosti K et al (1998) Exploration of the possible roles of phospholipase D and protein kinase C in the mechanism of ischemic preconditioning in the myocardium. Ann NY Acad Sci 793:210–225
Tappia PS (2007) Phospholipid-mediated signaling systems as novel targets for treatment of heart disease. Can J Physiol Pharmacol 85:25–41
Tappia PS, Singal T (2008) Phospholipid-mediated signaling and heart disease. Subcell Biochem 49:299–324
Tappia PS, Dent MR, Dhalla NS (2008) Oxidative stress and redox regulation of phospholipase D in myocardial disease. Free Radic Biol Med 41:349–361
Acknowledgment
Infrastructural support was provided by the St. Boniface Hospital Research Foundation.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Tappia, P.S., Dhalla, N.S. (2014). Alterations in Phospholipase D During the Development of Myocardial Disease. In: Tappia, P., Dhalla, N. (eds) Phospholipases in Health and Disease. Advances in Biochemistry in Health and Disease, vol 10. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0464-8_23
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0464-8_23
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0463-1
Online ISBN: 978-1-4939-0464-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)