
Abstract
Nonmelanoma (NMSC) are the most common skin cancer in the Western world. Basal cell carcinoma (BCC) account for roughly 80 % of NMSC. BCC are slow growing and rarely aggressive. A variety of treatments exist for the treatment of BCC with conventional surgical excision being the most commonly use method. Other options include Mohs’ surgery, curettage and electrodessication, laser therapies, radiotherapy and a number of topical treatments. Cryosurgery is a potentially under-utilised treatment option that offers the benefit of being less invasive. Cryotherapy is not recommended for lesions that are: morphoeic; have poorly defined margins; recurrent; on the eyelid, nasolabial fold or preauricular region; fixed to deeper structures; have a depth greater than 3 mm. Lesions greater than 2 cm in diameter can be treated segmentally. BCCs that are thick can be debulked with a curette prior to treatment. Common complications include pain, edema and blistering. When BCC lesions are selected carefully treatment outcomes are highly successful.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Nonmelanoma skin cancer (NMSC) are the most common skin cancer in the fair-skin population [1]. Basal cell carcinomas (BCCs) are the most common NMSC. There are a variety of treatment options available for the management of BCC with surgical excision being the most commonly used method. Cryosurgery has been widely available for the treatment of BCCs for the last 20 years, and is a useful alternative to the traditional surgical methods of removal [2]. Cryosurgery has a comparable outcome to conventional surgical excision when lesions are carefully selected and the correct technique is used. It is a less invasive method of treatment with a lower side effect profile and it is well tolerate without anaesthesia.
Description of the Disease
BCCs are the most common malignant neoplasm found in human populations [1]. BCCs constitute roughly 80 % of all non-melanoma skin cancers [3]. The growths are derived from cells originating in the basal layer of the epidermis [1]. Skin directly exposed to sunlight is commonly affected, including skin on the eyelids, the inner canthus and behind the ear.
BCC tumors have a characteristic slow progression. The slow rate of enlargement is due to constant and frequent cell death, whereby dying neoplastic cells undergo shrinkage and necrosis [4]. Extensive cell death causes BCC tumors to be contained within the area of origin [5]. Current estimations indicate that 0.0028–0.1 % of BCCs metastasize [6–8]. Lesions infiltrate tissues with irregular finger-like outgrowths contiguous with the main tumor mass. The malignancy is locally invasive and causes significantly greater morbidity than mortality [8]. Local tissue destruction is the main morbidity that results from BCC and this can impact on the cosmetic appearance or the functional outcome of the location [9].
Nodular BCCs are the most common clinical subtype [10, 11]. Nodular BCCs present as translucent or slightly erythematous papules or nodules with a sharp contour, a smooth margin, and telangiectasia. They commonly occur in sun-exposed areas of the head and neck region. Pigmented BCCs are hyperpigmented nodular BCCs. These lesions exhibit increased melanisation and thus can resemble malignant melanomas. The pigmented BCC has histological features which are similar to the nodular form, but with additional melanin [12].
The superficial subtypes also occur commonly. BCCs of the superficial variety present as well-circumscribed flat lesions with a pearly border [5]. Often there is scaling and crusting. These lesions often occur on the trunk and can resemble eczema [11].
Infiltrative and morpheic BCCs are more aggressive variants and they are less common [13–15]. Morpheic BCCs may present as a depressed white macule or scariform lesion which has a poorly defined border. The morpheic variety of BCCs usually has an aggressive growth pattern. These aggressive variants may invade extensively prior to exhibiting any obvious clinical symptoms.
Therapeutic Alternatives
Surgical Excision
Surgical excision is the most commonly used method of treating BCC. Complete specimens can be sent for histological examination and to assess the adequacy of excision. Primary excision is associated with a high rate of local control and complete excision has a high cure rate [16]. However, conventional surgical excision may not produce a cosmetically attractive outcome, particularly on the face.
Mohs Micrographic Surgery
Another surgical technique that allows for greater histological control is Mohs micrographic surgery. This technique – a microscopically-controlled method of removing skin cancers – is considered the gold standard for treatment of NMSC [16]. It involves excision of the lesion and a surrounding margin of tissue [16]. The tissue is sent for histopathological examination and another excision is undertaken if there are remaining tumor cells [17]. This process is repeated until all of the remaining abnormal cells are removed. This treatment modality is associated with an increased certainty of tumor eradication compared with conventional excision. Traditionally, this surgical option is performed on NMSC lesions occurring on the face. The technique also allows for preservation of non-affected skin and produces a better cosmetic outcome.
Unfortunately, the increasing cost of using Mohs micrographic surgery means that the procedure is usually limited to areas like the face where the cosmetic and functional outcome justifies the cost.
Curettage and Electrodessication
Skin curettes are oval or fenestrated spoons with a sharp cutting edge, usually used combined with an electrosurgical modality [18]. In the treatment of NMSC, electrodessication is used by superficially destroying affected tissue [18]. This technique involves removing cancerous tissue with the curette followed by lightly applying an electrical current to the base to burn any remaining tumor cells. This modality is relatively cheap and easy to perform. The cure rate for primary BCCs treated with this technique has been reported at 92.3 % [19]. A study examining 150 curetted non melanoma skin cancers showed that 76 % left some residual tumor tissue at the surgical margins [20]. Risk of recurrence is much higher with this technique and this is not the treatment of choice for recurrent BCCs [21].
Radiotherapy, Photodynamic, Topical and Laser Treatments
Treatments such as radiotherapy, or using radiation to treat abnormal cells, are reserved for BCCs that cannot be cured with surgical management. Often radiotherapy is used to complement surgical management [22]. Topical treatments like imiquimod (5 % concentration) that stimulate a cell-mediated immune response to cancer cells, have been approved for treatment of BCCs, with an 82 % clearance rate [23].
Photodynamic therapy (PDT) is a technique of using light to activate a photo-sensitizer applied to the skin, which causes formation of reactive oxygen species that destroy tumor-affected cells [24]. A study evaluating nodular BCC treatment using PDT in comparison with surgical excision demonstrated a 76 % clearance rate compared with 96 % respectively [25].
Prior to the introduction of PDT, laser therapies were used. The CO2 laser in particular, was found to be effective using between two and four passes of the laser. These findings were reported in a number of individual case reports and case series [26–28]. Since the introduction of PDT, the use of lasers has become relatively infrequent.
Cryosurgery
Cryosurgery is a method that involves tumor cell destruction by freezing the affected area with vaporizing liquid nitrogen [29]. Tumor cells are sensitive to cryosurgery because of their high water content and high metabolism [30]. Ice forms both extra- and intracellularly. Intracellular ice crystals expand and burst from inside the cell.
Like curettage, cryotherapy is simple and inexpensive; however, it does not allow for tumor margins to be examined under the microscope.
Table 130.1 outlines features to consider when selecting lesions for cryosurgery.
Methodology
Instruments Required
-
Sterile gloves
-
Hand-held cryotherapy unit with various size tips.
-
Antiseptic agents
-
Curette
-
Gauze and bandage
Treatment of Lesions Less Than 2 cm
BCC lesions should have a clearly defined margins. Lesions that do not have a clear border or those that are recurring should be treated using surgical excision. The canister should be full so that the flow of liquid nitrogen is even. For this method the ‘B’ tip should be used.
-
1.
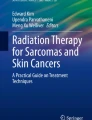
The lesion and an area of 0.5–0.75 cm of normal skin is clearly demarcated with a surgical pen (Fig. 130.1).
Fig. 130.1 
A basal cell carcinoma. An area of 0.5–0.75 cm should be marked around the lesion with surgical pen (Courtesy of Gloria Graham, MD [45])
-
2.
Hold the spray 1 cm away from the lesion at a 90° angle.
-
3.
Spray the center of the lesion until ice forms over the lesion and spreads laterally to the margin (Fig. 130.2)
Fig. 130.2 
Treatment of a basal carcinoma on the left side of the nose. The frield size of ice formation should be held at the marked margin for 30 s (Courtesy of Gloria Graham, MD [45])
-
4.
Maintain the field size of ice formation, at the marked margin, for a total 30 s. The time measured should begin from when ice first forms at the marked margin. At this stage the lesion should be frozen solid and firm on palpation.
-
5.
The area is then thawed out for no less than 60 s. The lesion should be palpated until the lesion softens and the white appearance disappears.
-
6.
Steps 2–4 are repeated.
-
7.
The area is dressed with a potent steroid cream (used twice daily) to prevent inflammation. Oral prednisolone can also be used for 3 days after cryosurgery to prevent post-cryosurgery morbidity. Figure 130.3 demonstrates the end result using this technique.
Fig. 130.3 
Post-operative result of a basal cell carcinoma treated with cryotherapy. Note that there is very minimal scarring (Courtesy of Gloria Graham, MD [45])



Single freeze-thaw cycle may be used, however there is some debate as to the success rate of this method [31]. A study comparing sing and double freeze-thaw cycles demonstrated a 95.3 % cure rate of facial BCC when double freeze-thaw cycle was used compared to 79.4 % cure rate [31]. Effective tissue-destruction occurs with multiple freeze-thaw cycles.
Treatment of Lesions That Are Irregular, Thick or Larger than 2 cm in Diameter
Segmental Therapy
For lesions that are larger than 2 cm or those that are irregular a single spray to the center of the lesion will not be adequate, as the temperatures at the margins may not reach destructive temperatures. Segmental treatment can be used for these types of lesions:
-
1.
Divide the lesion into multiple sections. Areas of no more than 2 cm are recommended so that the whole lesion can be frozen to a satisfactory temperature.
-
2.
Each section is treated using the same methodology outlined for the treatment of lesions less than 2 cm. Each area is treated separately and the field of treatment may overlap.
-
3.
Treatment may occur over two sessions, the second session may occur after 4 weeks
-
4.
Alternatively a portion of the lesion can be treated in one session and remaining treatments treated in a second section. This may help to reduce the severity of the side effects that may occur.
Debulking
Keratin is a poor conductor of cold and as a result thick BCC lesions do not reach satisfactory temperatures sufficient for tumor cell destruction. For BCCs which are large or thick a debulking procedure can be performed using a sharp curette. Recently a study examining 38 patients found that debulking BCCs with radio frequency prior to cryotherapy was also a useful method of debulking lesions, and provided the benefits of less bleeding, decreased procedure time and reduced use of surgical material. Currently, there is no literature comparing efficacy of the two debulking methods with each other [32].
Complications
The most common side effect of cryosurgery is pain [2]. Usually pain occurs in most patients however the severity of pain can vary. In some cases the pain can be so severe patients may have a syncopal episode. Edema and blistering is also a common occurrence. Symptoms are most severe around the eyelids, lips and genitals.
Hypopigmentation is also a common side effect. This loss of pigment is permanent. This side effect is not usually a problem for patients with fair skin. A feathering technique (light spray around the margin after treatment) can be used to disguise the contrast between the hypopigmented and normal skin.
Success Rates
Cure rates are in the order of 92–96 % which is comparable to conventional surgical excision [2]. Recurrence rates have varied in the literature ranging from 0 to 8.2 % [33–43]. A recent study in 2003 examining 12 BCCs, smaller than 1 cm, located on the trunk and arms. The lesions were treated with a single freeze-thaw treatment and were excised and examined histologically. All of the lesions examined had no histologic evidence of the tumor after 1–2 months [43].
Cosmetic results have been shown to be better in conventional surgical treatment compared to cryotherapy [44]. One prospective randomized study compared the cosmetic results of BCC treated with cryosurgery and surgical excision. Cosmetic outcome was evaluated by the patient, a dermatologist, a dermatology nurse, a plastic surgeon and a beautician. The dermatologist, surgeon and nurse all felt that the excision yielded a significantly better cosmetic outcome. The patients felt that the excision produced a better cosmetic result, however the difference between the ratings for both treatments was small. Lastly, the beautician, who was unbiased, had no preference for either procedure.
Conclusions
There are many treatment options available for the treatment of BCC, including surgical excision, Mohs micrographic surgery, curettage and electrodessication and lasers. Cryosurgery is one potentially under-utilised and less invasive option for the treatment of BCC. It is easy to perform in an outpatient setting and offers the benefits of being a fast and cheap procedure to perform. Studies have shown that cryosurgery can be equally as effective as traditional surgical options when the correct technique is used and the lesions are carefully chosen.
References
Crowson AN. Basal cell carcinoma: biology, morphology and clinical implications. Mod Pathol Off J U S Can Acad Pathol Inc. 2006;19 Suppl 2:S127–47.
Sinclair RD, Dawber RP. Cryosurgery of malignant and premalignant diseases of the skin: a simple approach. Australas J Dermatol. 1995;36(3):133–42.
Urbach F. Incidence of nonmelanoma skin cancer. Dermatol Clin. 1991;9(4):751–5.
Kerr JF, Searle J. A suggested explanation for the paradoxically slow growth rate of basal-cell carcinomas that contain numerous mitotic figures. J Pathol. 1972;107(1):41–4.
Dourmishev LA, Rusinova D, Botev I. Clinical variants, stages, and management of basal cell carcinoma. Indian Dermatol Online J. 2013;4(1):12–7.
Mikhail GR, Nims LP, Kelly Jr AP, Ditmars Jr DM, Eyler WR. Metastatic basal cell carcinoma: review, pathogenesis, and report of two cases. Arch Dermatol. 1977;113(9):1261–9.
von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. Report of five cases and review of 170 cases in the literature. J Am Acad Dermatol. 1984;10(6):1043–60.
Patel R, Adsay V, Andea A. Basal cell carcinoma with progression to metastatic neuroendocrine carcinoma. Rare Tumors. 2010;2(1):e8.
Cigna E, Tarallo M, Maruccia M, Sorvillo V, Pollastrini A, Scuderi N. Basal cell carcinoma: 10 years of experience. J Skin Cancer. 2011;2011:476362.
Morgan M. Basal cell carcinoma: variants and challenges. In: Morgan M, Hamill J, Spencer J, editors. Atlas of Mohs and frozen section cutaneous pathology. New York: Springer New York; 2010. p. 79–104.
Carucci JA, Leffell DJ, Pettersen JS. Basal cell carcinoma. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AA, Leffell DJ, Dallas NA, editors. Fitzpatrick’s dermatology in general medicine. 8th ed. New York: McGraw-Hill; 2012.
Karunker I, Morou E, Nikou D, Nauen R, Sertchook R, Stevenson BJ, et al. Structural model and functional characterization of the Bemisia tabaci CYP6CM1vQ, a cytochrome P450 associated with high levels of imidacloprid resistance. Insect Biochem Mol Biol. 2009;39(10):697–706.
Swetter SM, Yaghmai D, Egbert BM. Infiltrative basal cell carcinoma occurring in sites of biopsy-proven nodular basal cell carcinoma. J Cutan Pathol. 1998;25(8):420–5.
Jernbeck J, Glaumann B, Glas JE. Basal cell carcinoma. Clinical evaluation of the histological grading of aggressive types of cancer. Lakartidningen. 1988;85(42):3467–70.
Aasi S, Leffell D, Lazova R. Infiltrative basal cell carcinoma. Atlas of practical Mohs histopathology. New York: Springer; 2013. p. 47–64.
Brightman L, Warycha M, Anolik R, Geroneumus R. Do lasers or topicals really work for nonmelanoma skin cancers? Semin Cutan Med Surg. 2011;30:14–25.
Muhn C, Freiman A, Carey W. Mohs surgery is curettage and electrodessication a thing of the past? Dermatol Rounds. 2003;2(3):1–4.
Sheridan AT, Dawber RP. Curettage, electrosurgery and skin cancer. Australas J Dermatol. 2000;41(1):19–30.
Rowe DE, Carroll RJ, Day Jr CL. Long-term recurrence rates in previously untreated (primary) basal cell carcinoma: implications for patient follow-up. J Dermatol Surg Oncol. 1989;15(3):315–28.
Jih MH, Friedman PM, Goldberg LH, Kimyai-Asadi A. Curettage prior to Mohs’ micrographic surgery for previously biopsied nonmelanoma skin cancers: what are we curetting? Retrospective, prospective, and comparative study. Dermatol Surg Off Publ Am Soc Dermatol Surg [et al]. 2005;31(1):10–5.
Salasche SJ. Status of curettage and desiccation in the treatment of primary basal cell carcinoma. J Am Acad Dermatol. 1984;10(2 Pt 1):285–7.
Mazeron JJ, Chassagne D, Crook J, Bachelot F, Brochet F, Brune D, et al. Radiation therapy of carcinomas of the skin of nose and nasal vestibule: a report of 1676 cases by the Groupe Europeen de Curietherapie. Radiother Oncol J Eur Soc Ther Radiol Oncol. 1988;13(3):165–73.
Geisse J, Caro I, Lindholm J, Golitz L, Stampone P, Owens M. Imiquimod 5% cream for the treatment of superficial basal cell carcinoma: results from two phase III, randomized, vehicle-controlled studies. J Am Acad Dermatol. 2004;50(5):722–33.
Horn M, Wolf P, Wulf HC, Warloe T, Fritsch C, Rhodes LE, et al. Topical methyl aminolaevulinate photodynamic therapy in patients with basal cell carcinoma prone to complications and poor cosmetic outcome with conventional treatment. Br J Dermatol. 2003;149(6):1242–9.
Rhodes LE, de Rie MA, Leifsdottir R, Yu RC, Bachmann I, Goulden V, et al. Five-year follow-up of a randomized, prospective trial of topical methyl aminolevulinate photodynamic therapy vs surgery for nodular basal cell carcinoma. Arch Dermatol. 2007;143(9):1131–6.
Humphreys TR, Malhotra R, Scharf MJ, Marcus SM, Starkus L, Calegari K. Treatment of superficial basal cell carcinoma and squamous cell carcinoma in situ with a high-energy pulsed carbon dioxide laser. Arch Dermatol. 1998;134(10):1247–52.
Nouri K, Chang A, Trent JT, Jimenez GP. Ultrapulse CO2 used for the successful treatment of basal cell carcinomas found in patients with basal cell nevus syndrome. Dermatol Surg Off Publ Am Soc Dermatol Surg [et al]. 2002;28(3):287–90.
Fader DJ, Lowe L. Concomitant use of a high-energy pulsed CO2 laser and a long-pulsed (810 nm) diode laser for squamous cell carcinoma in situ. Dermatol Surg Off Publ Am Soc Dermatol Surg [et al]. 2002;28(1):97–9.
Neville JA, Welch E, Leffell DJ. Management of nonmelanoma skin cancer in 2007. Nat Clin Pract Oncol. 2007;4(8):462–9.
Ermertcan AT, Hellings PW, Cingi C. Nonmelanoma skin cancer of the head and neck: nonsurgical treatment. Facial Plast Surg Clin North Am. 2012;20(4):445–54.
Mallon E, Dawber R. Cryosurgery in the treatment of basal cell carcinoma. Assessment of one and two freeze-thaw cycle schedules. Dermatol Surg Off Publ Am Soc Dermatol Surg [et al]. 1996;22(10):854–8.
Goncalves JC, Martins C. Debulking of skin cancers with radio frequency before cryosurgery. Dermatol Surg Off Publ Am Soc Dermatol Surg. 1997;23(4):253–6.
Lindgren G, Larko O. Long-term follow-up of cryosurgery of basal cell carcinoma of the eyelid. J Am Acad Dermatol. 1997;36(5 Pt 1):742–6.
Jaramillo-Ayerbe F. Cryosurgery in difficult to treat basal cell carcinoma. Int J Dermatol. 2000;39(3):223–9.
Nordin P, Larko O, Stenquist B. Five-year results of curettage-cryosurgery of selected large primary basal cell carcinomas on the nose: an alternative treatment in a geographical area underserved by Mohs’ surgery. Br J Dermatol. 1997;136(2):180–3.
Kuflik EG, Gage AA. The five-year cure rate achieved by cryosurgery for skin cancer. J Am Acad Dermatol. 1991;24(6 Pt 1):1002–4.
Nordin P. Curettage-cryosurgery for non-melanoma skin cancer of the external ear: excellent 5-year results. Br J Dermatol. 1999;140(2):291–3.
Kuflik EG, Gage AA. Recurrent basal cell carcinoma treated with cryosurgery. J Am Acad Dermatol. 1997;37(1):82–4.
Biro L, Price E. Cryosurgical management of basal cell carcinoma of the eyelid: a 10-year experience. J Am Acad Dermatol. 1990;23(2 Pt 1):316–7.
Fraunfelder FT, Zacarian SA, Wingfield DL, Limmer BL. Results of cryotherapy for eyelid malignancies. Am J Ophthalmol. 1984;97(2):184–8.
Kuflik EG. Cryosurgery for basal-cell carcinomas on the wings of the nose and in the nasolabial folds. J Dermatol Surg Oncol. 1981;7(1):23–5.
Zacarian SA. Cryosurgery of cutaneous carcinomas. An 18-year study of 3,022 patients with 4,228 carcinomas. J Am Acad Dermatol. 1983;9(6):947–56.
Giuffrida TJ, Jimenez G, Nouri K. Histologic cure of basal cell carcinoma treated with cryosurgery. J Am Acad Dermatol. 2003;49(3):483–6.
Thissen MR, Nieman FH, Ideler AH, Berretty PJ, Neumann HA. Cosmetic results of cryosurgery versus surgical excision for primary uncomplicated basal cell carcinomas of the head and neck. Dermatol Surg Off Publ Am Soc Dermatol Surg [et al]. 2000;26(8):759–64.
Graham GF. Cryosurgery. In: Nouri K, Skin Cancer. New York: McGraw-Hill Companies Inc.: 2008. p. 534.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag London
About this chapter
Cite this chapter
Perera, E., Sinclair, R. (2016). Basal Cell Carcinoma. In: Abramovits, W., Graham, G., Har-Shai, Y., Strumia, R. (eds) Dermatological Cryosurgery and Cryotherapy. Springer, London. https://doi.org/10.1007/978-1-4471-6765-5_130
Download citation
DOI: https://doi.org/10.1007/978-1-4471-6765-5_130
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-6764-8
Online ISBN: 978-1-4471-6765-5
eBook Packages: MedicineMedicine (R0)